
Abstract
Purpose
Postextubation dysphagia (PED) can lead to prolonged tube feeding, but risk factors associated with prolonged tube feeding in this population are largely unknown. The purpose of this study was to identify factors independently associated with prolonged tube feeding in adult inpatients who required intubation and mechanical ventilation.
Materials and Methods
Retrospective observational cohort study in a dataset of 1.3 million inpatients. Extubated adults without preventilation dysphagia or tube feeding who underwent instrumental swallowing assessment were included. To characterize factors independently associated with prolonged tube feeding, we compiled a set of potential factors, completed factor selection using a random forest algorithm, and performed logistic regression.
Results
In total, 206 of 987 (20.9%) patients had prolonged tube feeding. The regression model produced an area under the curve of 0.79. Factors with the greatest influence on prolonged tube feeding included dysphagia with thickened liquids, dysphagia with soft/solid foods, preadmission weight loss, number of intubations, admission for neurologic disorder, and hospital of admission.
Conclusions
Several factors predicted prolonged tube feeding after extubation. The strongest were some, but not all, aspects of swallowing function and clinical practice pattern variability. Clinical decision-making should consider bolus-specific data from instrumental swallowing evaluation rather than binary presence or absence of dysphagia.
Introduction
Swallowing difficulty after endotracheal intubation and ventilation, known as postextubation dysphagia (PED), is common. 1 PED is associated with numerous negative outcomes, including tracheal aspiration of food and/or liquid, increased risk of pneumonia, and mortality.2,3 Nasogastric or gastrostomy feeding tubes are sometimes used for an extended time after extubation to reduce the risk of prandial aspiration by eliminating the need for oral and pharyngeal swallowing. However, prolonged tube feeding has been associated with delayed hospital discharge, increased risk of aspiration pneumonia, pressure sores, and death in some populations.4,5 Further, the presence of a nasogastric feeding tube can negatively influence swallowing in recently extubated patients. 6 Thus, while tube feeding is an important tool in aiding recovery from critical illness, return to oral nutrition as soon as possible could reduce negative outcomes associated with prolonged tube feeding. Many clinical indications for initiation of tube feeding exist, but factors associated with prolonged tube feeding following extubation are poorly described.
Although PED is recognized as one risk factor for prolonged tube feeding, other factors warrant investigation, including severity of PED, underlying comorbidities, and the initial condition necessitating intubation, as well as demographic factors and variation in practice. Identification of factors associated with prolonged tube feeding could improve prognostic accuracy, and aid clinicians in mitigating factors associated with prolonged intubation. The objective of this study was to identify factors that independently contributed to prolonged tube feeding after extubation in adults who required mechanical ventilation. We hypothesized that admission diagnosis and underlying comorbidities would be the strongest predictors of prolonged tube feeding.
Methods
Patient Population and Design
We performed a large, retrospective observational cohort study of inpatients treated at 12 hospitals in the Midwest United States, with the primary goal of examining factors that were independently associated with prolonged tube feeding following endotracheal intubation and mechanical ventilation. This study was approved by the University of Minnesota Institutional Review Board (STUDY00014868).
We included patients ≥18 years of age, who were admitted to the hospital between January 2011 and August 2022, and who had undergone intubation, mechanical ventilation, and subsequent successful extubation. To ensure that objective swallowing data could be taken into account, we applied an additional inclusion criteria that patients had completed a modified barium swallow study (MBSS) or a flexible endoscopic evaluation of swallowing (FEES) with a Penetration-Aspiration Scale 7 score for at least 1 bolus type following extubation. In the event that patients were intubated and ventilated multiple times in a single hospital admission, the final instance of intubation and ventilation was used for analysis (n = 2600) to most accurately represent time since extubation. Patients were excluded if they had a history of dysphagia (ICD-10 codes R13.1-R13.19, 1.4%), or if they had tube feeding (order for tube feeding placement, or nutritional order for tube feeding, 24.6%) within 2 years prior to hospital admission. (Supplemental Information e-Figure 1).
Statistical Analyses
To characterize factors independently associated with prolonged tube feeding, 93 potential factors and covariates were identified. We compared these factors in patients with and without prolonged tube feeding in univariate analysis using χ2 tests for categorical variables, Student's t-tests for continuous variables, and Kruskal-Wallis rank sum tests when continuous variables were non-normally distributed. We addressed missingness of these factors with multiple imputations using chained equations, and completed factor selections using a Random Forest algorithm. We then performed logistic regression to determine association with prolonged tube feeding, using factors identified as most-important by the Random Forest algorithm as statistical co-variates to adjust for other potentially significant factors.
Variable Selection and Modeling
Following imputation, a random forest algorithm was optimized and used for variable selection.8,9 The 30 variables from the random forest algorithm with the greatest mean decrease in Gini coefficient were selected as predictor variables for logistic regression. Model performance was assessed with R2, area under the curve, and Brier Scores. Assumptions of logistic regression were assessed using residual plots and multicollinearity of the model was assessed using variance inflation factors. All statistical analysis was performed using R statistical software (v 4.1.2).
Extensive sensitivity analyses were performed to assess the robustness of the findings. These included the implementation of a full model without variable selection, use of a proxy outcome, and exploration of different feature selection combinations. To comprehensively examine all available variables and capture their relationships, we implemented a full model without feature selection. This approach allowed us to analyze the complete set of variables, providing a robust benchmark for evaluating the impact of feature selection techniques. As a proxy outcome, we defined prolonged tube feeding using a median split for a total duration of postextubation tube feeding. The median threshold for prolonged tube feeding was greater than 4 days. In addition, we explored various combinations of feature selection using the random forest and Gini coefficients. This involved comparing the performance of the top 10, top 30, and top 50 selected features. After careful evaluation, the top 30 features yielded the most clinically and statistically meaningful results.
Primary Outcome and Factor Selections
The primary outcome of this study was prolonged tube feeding. Prolonged tube feeding was defined as the use of nasogastric or gastric tube feeding occurring within 24-h prior to hospital discharge. We compiled a list of 93 factors for predicting prolonged tube feeding, including those identified as significant predictors for PED in 2 or more peer-reviewed publications, 10 patient-related factors that were expected to impact the risk of prolonged tube feeding, and swallowing variables. PED-associated variables included duration of intubation, number of intubations, and individual components of the Acute Physiology and Chronic Health Evaluation-II (APACHE-II) score. Patient-related variables included preadmission Elixhauser comorbidities, 11 admission medication class mappings based on the Veterans Health Administration National Drug File, 12 demographic factors, specific diagnoses likely to influence tube feeding (eg, pancreatitis, small bowel procedures, colon procedures), hospital of admission, and consultation to palliative care and comfort care, which could influence patient/family decisions regarding feeding tube placement. We chose a nonacademic, level-III trauma center with the largest number of beds as the reference level hospital of admission, as it is likely to most closely represent patient and provider demographics in the Midwest United States. Swallowing variables included: normal versus abnormal swallow function (1) with thin liquids, (2) with slightly, mildly, or moderately thickened liquids, (3) with purees, and (4) with soft solids and solids during the first MBSS or FEES following extubation. For each of these bolus textures and consistencies, we operationally defined normal swallow as a Penetration-Aspiration Scale scores of 1 or 2, and abnormal as scores of 3 or higher.
The proportion of missingness was assessed for all predictor variables (Supplemental Information e-Table 3). Variables with more than 40% missingness were removed from consideration. Missing data were imputed for continuous variables using predictive mean matching. 13 Missing data were imputed for categorical variables using polynomial regression. In order to balance computational resources and statistical rigor, imputations were run for 5 iterations. All imputations were performed using fully conditional specifications and implemented by the Multivariate Imputation by Chained Equations 14 package in R statistical software (v 4.1.2). Following imputation, the variables were subjected to variable selection.
Results
After the application of inclusion and exclusion criteria, we analyzed data from 987 patients who had been extubated (Flow Diagram Supplemental Information e-Figure1). Of these, 206 (20.9%) had prolonged tube feeding. Patients who had prolonged tube feeding were 35.4% female (n = 73), consistent with literature suggesting increased risk of PED in males. 15 Patients with prolonged tube feeding were 85.9% White race (n = 177), and had a median age of 65.5 years (interquartile range 56.3-74.0 years; Table 1; Supplemental Information e-Table 1).
Characteristics of Patients who did and did not Have Prolonged Tube Feeding.
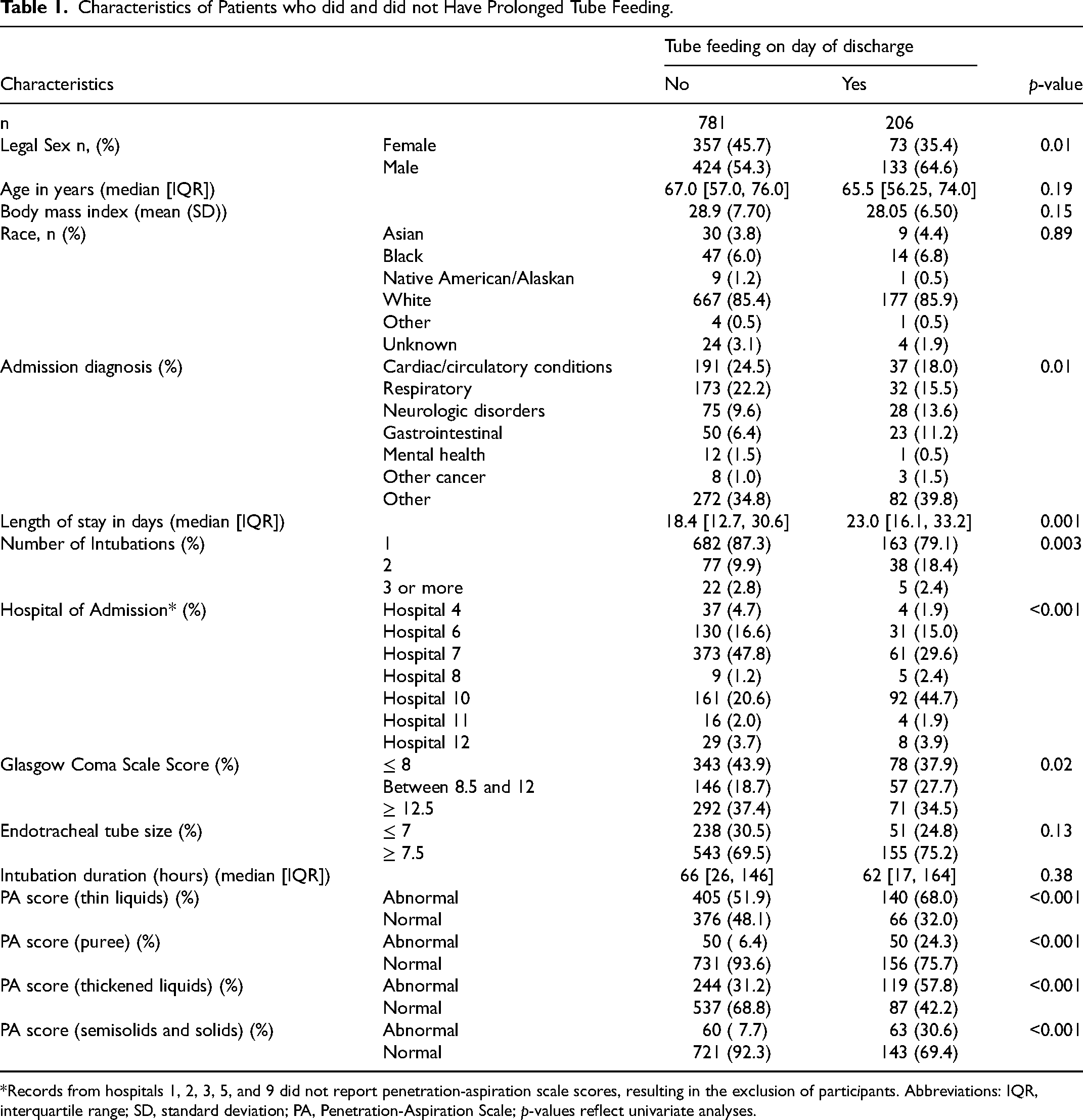
*Records from hospitals 1, 2, 3, 5, and 9 did not report penetration-aspiration scale scores, resulting in the exclusion of participants. Abbreviations: IQR, interquartile range; SD, standard deviation; PA, Penetration-Aspiration Scale; p-values reflect univariate analyses.
Among variables identified by the random forest algorithm as the most important contributors to prolonged tube feeding (Figure 1), the greatest risk (Figure 2) of prolonged tube feeding was independently associated with: Hospital 8 as the hospital of admission (reference level: Hospital 7; OR 4.45, 95% CI: 1.22-16.28), dysphagia with soft or solid foods (OR: 4.19; 95% CI: 2.23-7.88); Hospital 10 as the hospital of admission (reference level: Hospital 7; OR 3.24, 95% CI: 2.0-5.25); 2 intubations (reference level 1 intubation; OR: 2.1; 95% CI: 1.22-3.65); neurological admission diagnosis (OR 1.96, 95% CI: 1.07-3.58); and dysphagia with thickened liquids (OR 1.81, 95% CI: 1.16-2.82). A listing of characteristics of the hospitals included in analysis (eg, number of beds, level of trauma center) can be found in Supplementary Information e-Table 2.
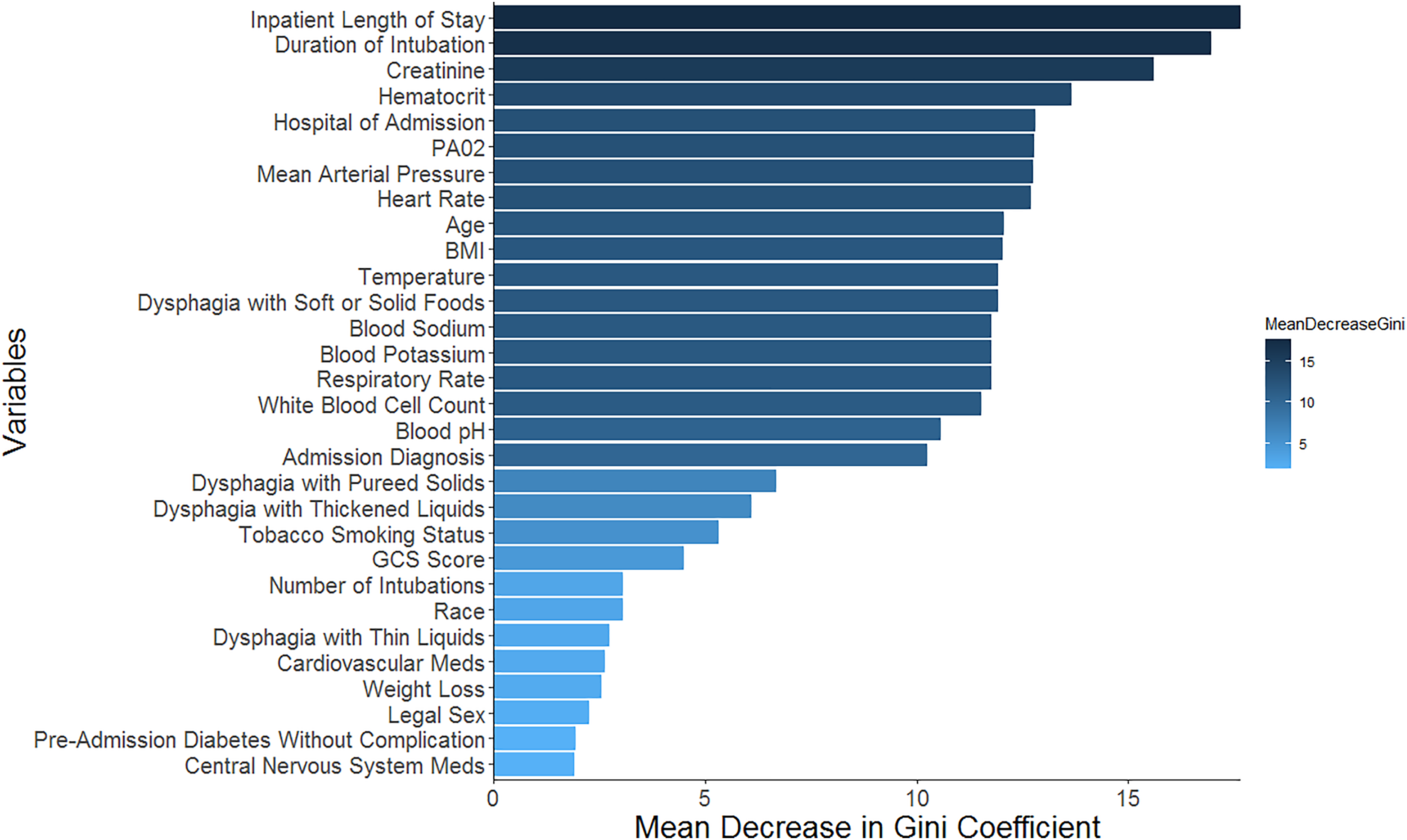
Variables identified by the random forest algorithm as having the greatest contribution to the prediction of prolonged tube feeding. These variables were supplied to the logistic regression model.
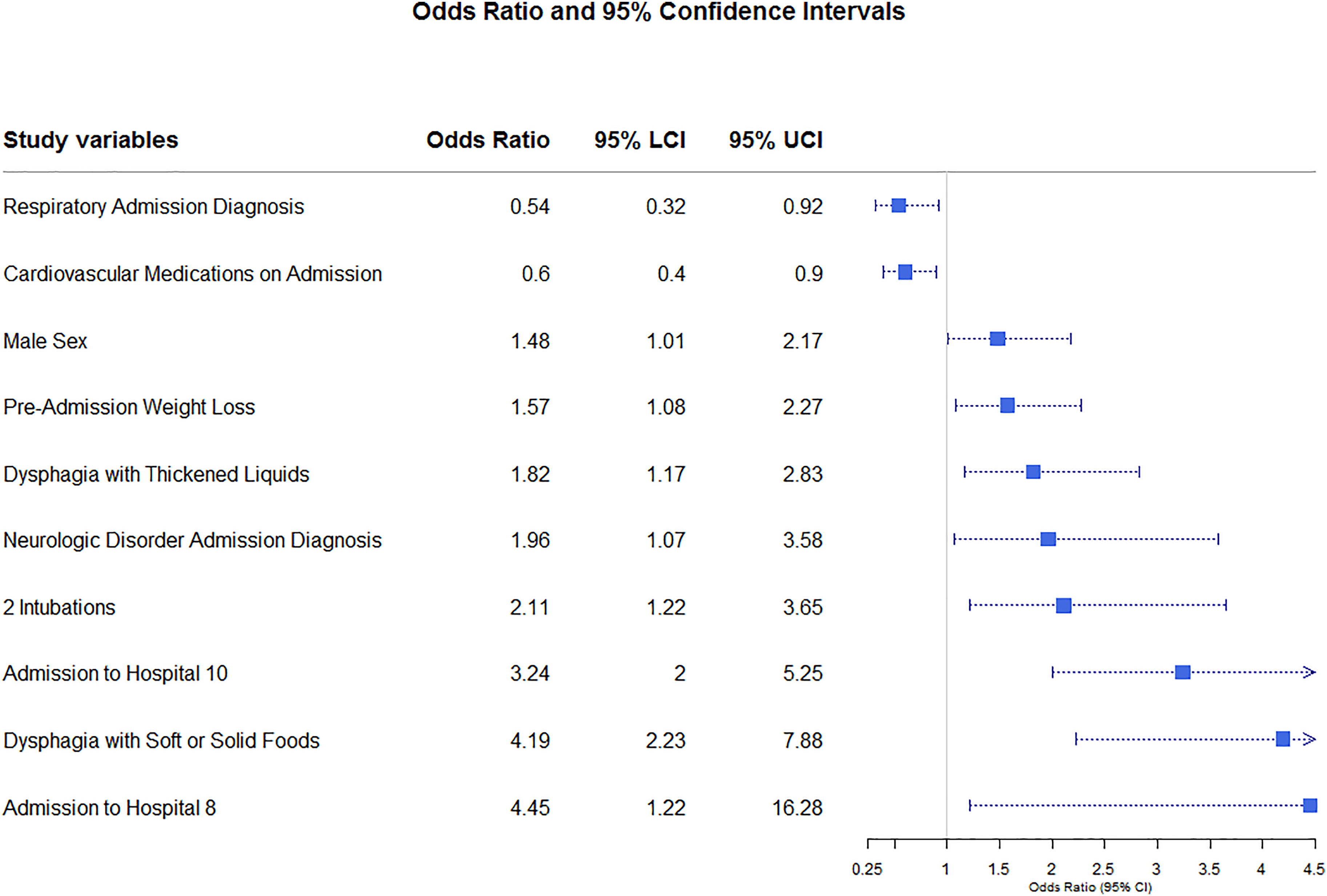
Odds ratio and 95% confidence intervals for predictors of prolonged tube feeding. Abbreviations: LCI, lower confidence interval; UCI, upper confidence interval.
The logistic regression model produced an area under the receiver operating curve 0.79 (79%). Brier score estimated an accuracy of the model as 0.13. R2 indicated that 19% of the observed variability in the outcome was explained by the predictors.
Sensitivity Analyses
After redefining prolonged tube feeding using total postextubation duration of tube feeding, 514 patients had postextubation tube feeding greater than the median duration (4 days) (AUROC of 0.74, R2 of 0.14, and Brier score of 0.21). The strongest predictors of having greater than the median duration of postextubation tube feeding were dysphagia with thickened liquids, Glasgow Coma Scale Score between 8.5 and 12, blood pH levels, and hospital of admission.
When using our primary definition of prolonged tube feeding and assessing full model performance without variable selection, we observed area under the receiver operating curve of 0.81, R2 of 0.23, and Brier Score of 0.12. The strongest predictors of prolonged tube feeding with the full model using the primary definition of prolonged tube feeding were dysphagia with soft or solid foods, hospital of admission, 2 intubations, admission for neurologic disorder, preadmission weight loss, and dysphagia with thickened liquids.
When we removed all variables with greater than 10% missingness prior to imputation, we observed an area under the receiver operating curve of 0.79, R2 of 0.19, and Brier Score of 0.13. The strongest predictors of prolonged tube feeding with in this model were hospital of admission, dysphagia with soft or solid foods, admission for a neurological disorder, 2 intubations, preadmission weight loss, and male sex. Dysphagia with thickened liquids was also a significant predictor of prolonged tube feeding, but to a slightly lesser degree than in the primary model. These analyses indicate general agreement with our primary model.
Discussion
Return to oral nutrition following endotracheal intubation is an important aspect of recovery from critical illness.15,16 The purpose of this study was to characterize factors that were independently associated with prolonged tube feeding in adult inpatients who required intubation and mechanical ventilation. In this large study of patients with a wide variety of admission diagnoses, ages and clinical characteristics, specific aspects of swallow function and hospital of admission were the strongest independent predictors of prolonged tube feeding. These findings did not support our hypothesis that admission diagnosis and premorbid conditions would be the strongest predictors of prolonged tube feeding.
There are 2 key findings from this study. The first is that different types of swallow impairment had different effects on the risk for prolonged tube feeding. Our findings are consistent with the literature17,18 in that swallowing disruption, broadly speaking, is associated with prolonged tube feeding, and in that factors associated with risk of PED (admission diagnosis, premorbid conditions, male sex, number of intubations) were also independent predictors of prolonged tube feeding in the current study.3,10,15,19,20 Interestingly, neither duration of intubation nor endotracheal tube size were independent predictors for prolonged tube feeding, despite the fact that both have been associated with risk of PED in the literature. 10 A possible explanation for this discrepancy is that not all types of swallowing impairment in our study were significantly predictive of prolonged tube feeding, suggesting that results obtained from swallowing evaluation should not be aggregated and interpreted in a binary manner. For example, in other studies, patients who demonstrate tracheal aspiration with thin liquids are often reported to have “failed” a MBSS or a FEES, 21 and these individuals are categorized in a binary manner as having PED in most research literature. In the current study, however, we observed that abnormal swallowing with thin liquids (including tracheal aspiration) had a limited association with prolonged tube feeding. Conversely, impaired swallowing function with thickened liquids and/or with soft solids resulted in a significant increase in the risk of prolonged tube feeding. A binary definition of PED would have obscured these results. A thorough instrumental swallowing assessment that includes investigation of multiple viscosities across multiple trials is time consuming to analyze and interpret and can be resource-intensive for both patients and clinicians. However, lack of this knowledge may lead to unnecessarily prolonged or inappropriately abbreviated tube feeding. Further investigation of factors that would prospectively identify at-risk individuals could ultimately lead to a clinical decision support system prompting more in-depth swallow assessment.
Consideration of specific swallowing physiology measures is also likely to further inform the risk of prolonged tube feeding. For example, laryngeal visualization could help to identify potential mechanisms of PED, such as impaired airway protection due to vocal fold immobility or reduced laryngeal sensitivity and associated airway protective reflexes. 22 Likewise, quantification of swallowing kinematics, 23 such as anterior-posterior tongue pressure, pharyngeal response time, hyolaryngeal elevation and anterior excursion, and duration and extent of upper esophageal sphincter opening could aid in both understanding of physiologic mechanisms of PED, and could shed light on why swallowing impairment with thickened liquids and solids, but not thin liquids or purees, result in increased risk of prolonged tube feeding. While these data were not available in the current data set because laryngeal exams were only completed on a small subset of patients and because swallowing kinematic measures are only rarely reported in clinical contexts, these data should be considered in future prospective investigations.
The second key finding is that variation in clinical practice across hospitals may account for a great degree of variability in outcomes for patients who have prolonged tube feeding following extubation. Even when controlling for all other clinical and demographic factors, dysphagia with thickened liquids and dysphagia with soft/solid foods, admission site was associated with differences in risk of prolonged tube feeding. Admission to the 2 hospitals associated with increased risk of prolonged tube feeding (hospital 8 and hospital 10) differed substantially in size (153 beds and 743 beds, respectively) and in Trauma Care Categorization (level III and level II, respectively). This implies that clinical practice patterns, rather than objective interpretation of clinical data, may have a disproportionate impact on risk for prolonged tube feeding. The development of clinical decision support systems could help to improve patient outcomes by appropriately reducing prolonged or abbreviated tube feeding.
Limitations
The primary limitation of this study is its retrospective nature. Dysphagia determination was made by diagnosis codes, but identification of dysphagia by codes alone may be an underestimate. 24 The decision of a medical team to order an instrumental swallowing assessment (MBSS or FEES) may have resulted in selection bias, with those who were suspected to have swallowing impairment being more likely to receive an instrumental swallow assessment. In addition, exclusion of patients who were not referred for a MBSS or FEES may have excluded sicker patients who were unable to participate in these procedures. We attempted to control for this by controlling for each element of the APACHE-II, but the potential for introduction of possible selection bias remains. The study period also includes patients from the coronavirus disease 2019 (COVID-19) pandemic period, but we did not perform a subanalysis of the COVID-era to account for variations in clinical practices. Such limitations will be addressed in future studies as they are beyond the scope of the current manuscript.
Prospective validation of the model developed in this work will be important for future clinical translation. While a considerable strength of this study is the use of multiple types of swallowing data as predictive factors for assessment of the risk of prolonged intubation, these data were flattened to produce a binary of normal versus abnormal swallowing for each of the liquid and solid textures considered. Greater nuance in swallowing data, such as the degree of postswallow pharyngeal residue and other measures of swallowing efficiency, would likely improve the predictive capacity of these models.
Conclusion
Several factors predicted prolonged tube feeding after extubation. Specific aspects of swallowing function and clinical practice pattern variability were among the strongest predictors. Clinical decision-making for individuals with uncertain prognosis for prolonged tube feeding following extubation will likely benefit from the consideration of data obtained from thorough instrumental swallowing evaluation. Future work should assess predictive factors for other consequences of PED and tube feeding, such as aspiration pneumonia, hospital readmission, and mortality.
Supplemental Material
sj-docx-1-jic-10.1177_08850666241258960 - Supplemental material for Independent Risk Factors for Prolonged Tube Feeding After Endotracheal Intubation and Ventilation
Supplemental material, sj-docx-1-jic-10.1177_08850666241258960 for Independent Risk Factors for Prolonged Tube Feeding After Endotracheal Intubation and Ventilation by Prajwal M. Pradhan, Schelomo Marmor, Christopher Tignanelli, Stephanie Misono and Jesse Hoffmeister in Journal of Intensive Care Medicine
Footnotes
Author Contributions
Prajwal M. Pradhan, MPH1,2, Schelomo Marmor, PhD2,3,4, Christopher Tignanelli, MD, MS2,4, Stephanie Misono, MD, MPH2,5 and Jesse Hoffmeister, PhD5
PMP made substantial contributions to the conception and design of the work, analysis, and interpretation of data for the work; drafting the work and reviewing it critically for important intellectual content; final approval for the version to be published; accountable for all aspects of the work ensuring that questions related to the accuracy and integrity of any part of the work will be appropriately investigated and resolved. S Marmor made substantial contributions to the conception and design of the work, acquisition, analysis, and interpretation of data for the work; drafting the work and reviewing it critically for important intellectual content; final approval for the version to be published; accountable for all aspects of the work ensuring that questions related to the accuracy and integrity of any part of the work will be appropriately investigated and resolved. CT made substantial contributions to the conception and design of the work, acquisition, analysis, and interpretation of data for the work; critically reviewing the work for important intellectual content; final approval for the version to be published; accountable for all aspects of the work ensuring that questions related to the accuracy and integrity of any part of the work will be appropriately investigated and resolved. S Misono made substantial contributions to the conception and design of the work, interpretation of data for the work; critically reviewing the work for important intellectual content; final approval for the version to be published; accountable for all aspects of the work ensuring that questions related to the accuracy and integrity of any part of the work will be appropriately investigated and resolved. JH made substantial contributions to the conception and design of the work, analysis, and interpretation of data for the work; drafting the work and reviewing it critically for important intellectual content; final approval for the version to be published; accountable for all aspects of the work ensuring that questions related to the accuracy and integrity of any part of the work will be appropriately investigated and resolved.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Dystonia Coalition through the National Institutes of Health (NIH) office of Rare Diseases Research in the National Center for Advancing Translational Sciences, the National Institute of Neurological Disorders and Stroke (NS065701, TR001456, and NS116025), from the NIH National Institute on Deafness and Other Communication Disorders (grant K23DC016335).
Ethical Approval
This study was approved by the University of Minnesota Institutional Review Board (STUDY00014868).
Guarantor
All authors are equally responsible for all content of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.