
Abstract
Background
Bicaval dual lumen cannula (DLC) is gaining popularity in veno-venous extracorporeal membrane oxygenation (V-V ECMO) for having less recirculation and facilitating mobilization. It is usually inserted under fluoroscopic or transesophageal echocardiographic guidance to prevent potentially fatal complications. Thus, their utilization was limited during the COVID-19 outbreak due to stringent quarantine policy and manpower shortage, especially when emergency insertion was required.
Purpose
To describe our experience on DLC insertion using transthoracic echocardiography alone during the pandemic, with a focus on safety considerations by using detail step-by-step procedural guide.
Outcome
Four patients were performed V-V ECMO using the transthoracic echocardiographic-guided DLC cannulation technique during the fifth wave of the COVID-19 outbreak, with no cannulation-related complications.
Conclusion
Transthoracic echocardiographic guidance for DLC insertion is feasible and probably safe with a detailed guide, which can be adopted as a supplementary tool during future endemic outbreaks.
Keywords
Introduction
Veno-venous extracorporeal membrane oxygenation (V-V ECMO) is widely used for respiratory failure that is refractory to conventional treatment. It may serve as a bridge to recovery or lung transplant. V-V ECMO involves the drainage of deoxygenated venous blood, which is returned to the same venous compartment after passing through a blood pump and oxygenator where oxygenation and carbon dioxide removal take place. 1 In traditionally, a two-cannulae technique is utilized, whereby the drainage cannula is inserted via the femoral vein into the inferior vena cava (IVC), and the return cannula is inserted into the internal jugular vein (IJV), femoral or subclavian veins. However, this technique may reduce the efficacy of gaseous exchange due to recirculation and limit patients from early mobilization and rehabilitation.2,3 The bicaval dual lumen cannula (DLC) aims to alleviate these limitations. The first DLC was first developed and used in neonates in the 1980s. 4 The Avalon Elite DLC was marketed in Europe and incorporated into the practice of adult ECMO since 2008. In 2018, the Crescent bicaval DLC (MC3, Dexter, MI) was approved by FDA for prolonged use with V-V ECMO. Proper insertion and precise positioning of the cannula are the most important part for the safety and optimal functioning of the DLC.
Currently, fluoroscopic and transesophageal echocardiographic (TEE)-guided insertion of DLC are the most common techniques being reported in literature5–7 and are recommended by the Extracorporeal Life Support Organization guidelines. 1 Other centres have also reported the use of mobile x-ray to guide insertion of DLC. 8 In this case report, we would like to report our experience and safety tips on the use of transthoracic echocardiography (TTE)-guided insertion of DLC during the COVID-19 pandemic when fluoroscopic and TEE services were limited.
Case Presentation
A 49-year-old man was admitted to hospital with a 4-day history of fever and shortness of breath. He had a history of IgA nephropathy and was on long-term steroid therapy. A sample from bronchoalveolar lavage confirmed a diagnosis of Pneumocystis jirocevii pneumonia and sulfamethoxazole was started. He developed progressive respiratory failure, requiring intubation and prone ventilation on day 10 of admission. Clindamycin and Caspofungin were administrated in view of possible sulfamethoxazole resistance. He deteriorated further on day 12, with a P/F ratio of 117, and V-V ECMO was initiated.
In view of his immunocompromised status, a 26Fr Crescent bicaval DLC (MC3, Dexter, MI) was inserted in the right IJV to facilitate early mobilization. However, the hospital infection control advisory board recommended against the transferal of the patient to the radiology fluoroscopy suite amid the fifth wave of COVID-19 outbreak. Urgent TEE service was also not available due to manpower shortage. Therefore, we decided to insert the DLC at the bedside under TTE guidance.
A 5Fr vascular sheath was inserted into the right IJV, followed by the introduction of a J-tip 0.035inch diameter, guidewire (Maquet, Rastatt, Germany) through the sheath. The distance from the IJV sheath to the subxiphoid region was estimated and confirmed by visualizing the tip of the guidewire in the IVC by subxiphoid view (Figure 1), taking note that extra length may suggest the guidewire looping within the heart. This was further confirmed by apical or/and subxiphoid four-chamber views, parasternal short axis view of aortic root and right ventricular inflow view. The insertion of guidewire can be further facilitated by obtaining the TTE bicaval view if the body habitus allows. 9 If resistance was encountered, the guidewire was withdrawn and the above steps repeated. After visualizing the guidewire in the IVC, it is advanced 10 cm to prevent dislodgement into the hepatic vein upon cannula insertion. With continuous monitoring of the guidewire position using the subxiphoid view, serial percutaneous dilation was performed and the DLC was inserted into the IVC.
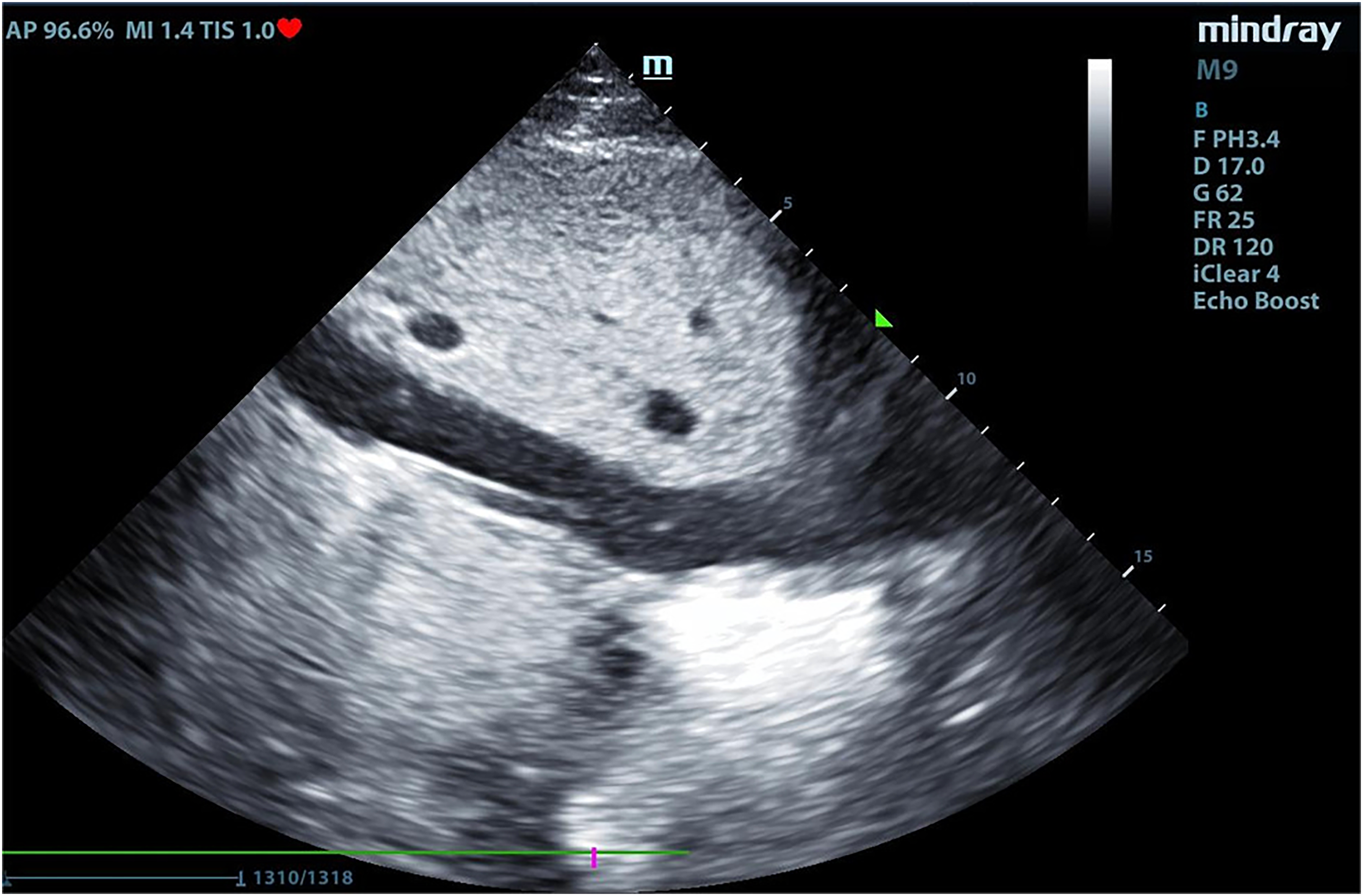
Ultrasonographic image in subxiphoid view shows the position of the guidewire in the IVC. IVC, inferior vena cava.
The optimal position of the DLC required the reinfusion port opening to be directed at the right atrium. According to manufacturer's information, the length from the reinfusion port to the tip of cannula is 9.3 cm (Figure 2). Anatomically, the length between the opening of SVC and IVC was estimated to be about 3.2 cm. 10 With this information, the DLC was advanced 7 cm from the opening of the IVC guided by abdominal ultrasonography (Figure 3), with the resultant reinfusion port opening to be positioned within the right atrium. The DLC was then rotated so that the arm of the return cannula was pointing medially at the 10 o’clock position when viewing craniocaudally. ECMO was initiated at both blood flow and fresh gas flow of 3.5 L/min. Doppler ultrasound was used to ensure the ECMO blood flow was directed towards the tricuspid valve. Distinctive colour difference between the drainage and return cannulae and the mixed venous oxygen saturation (SvO2) reading on the ECMO console can be used to exclude recirculation at the bedside. Chest radiograph can be deployed to confirm the orientation of the DLC (Figure 4).
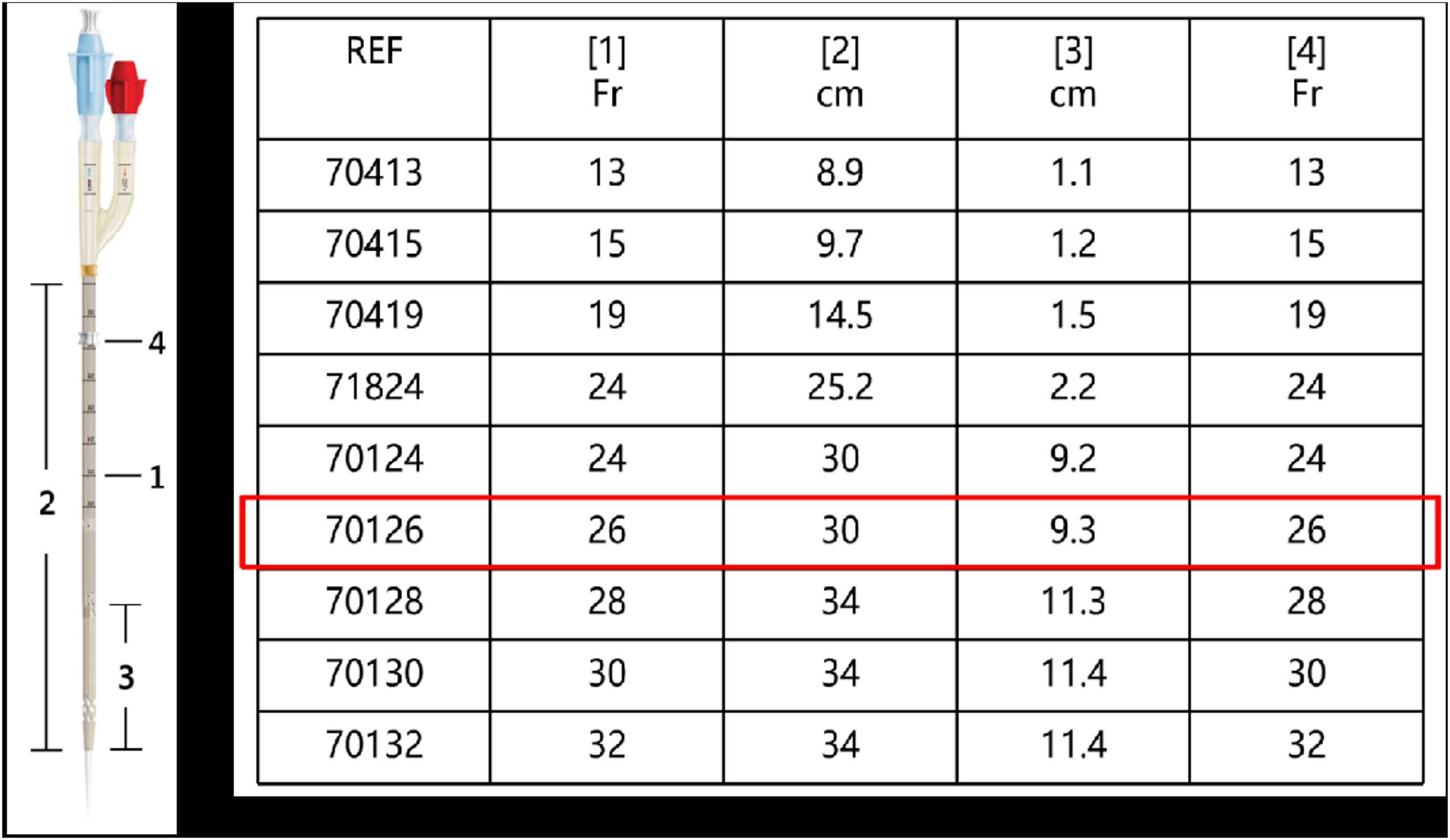
Configuration of the 26Fr crecent bicaval DLC. DLC, dual lumen cannula.
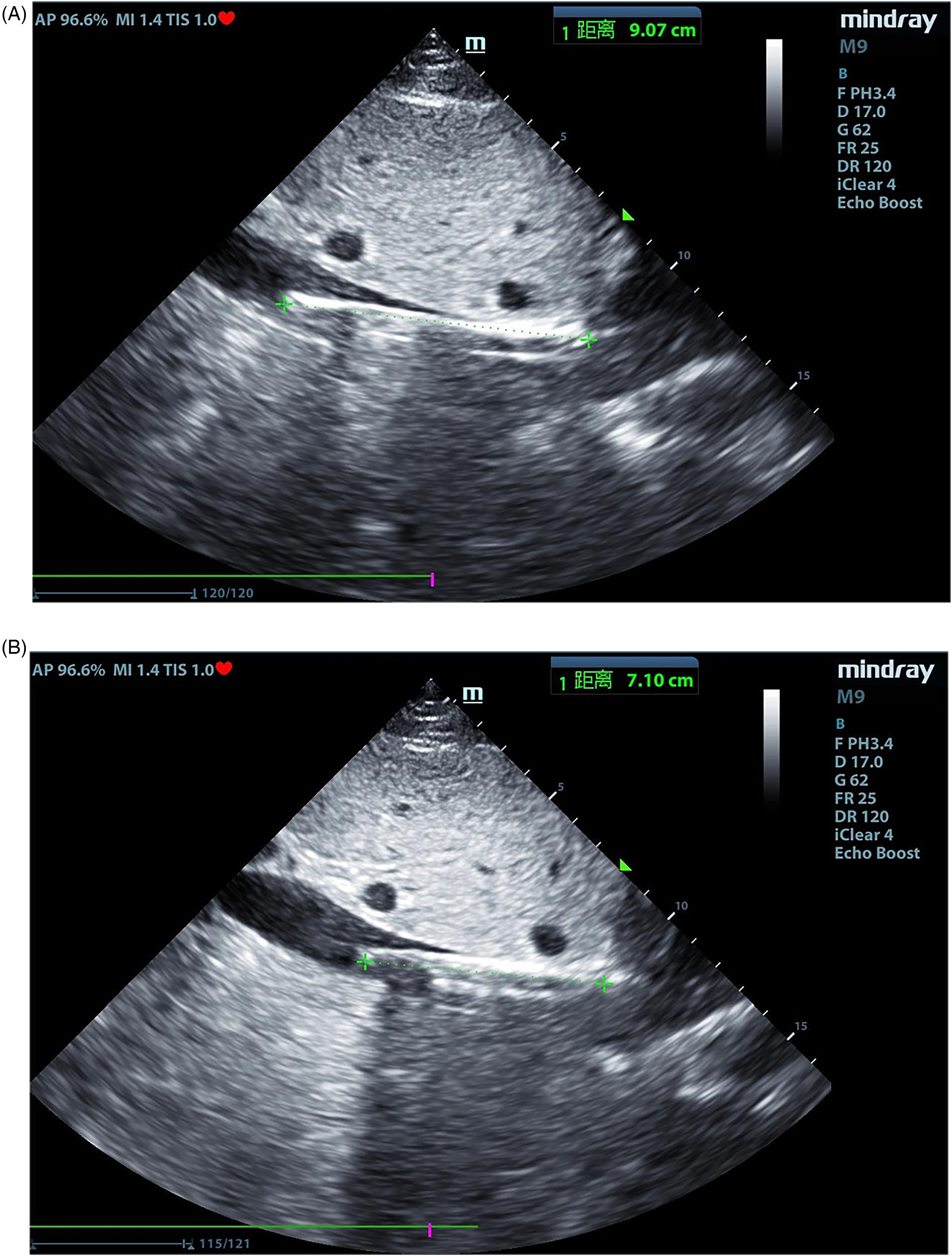
Ultrasonographic image in subxipoid view shows the manipulation of the cannula. The cannula was initially inserted at 9 cm.
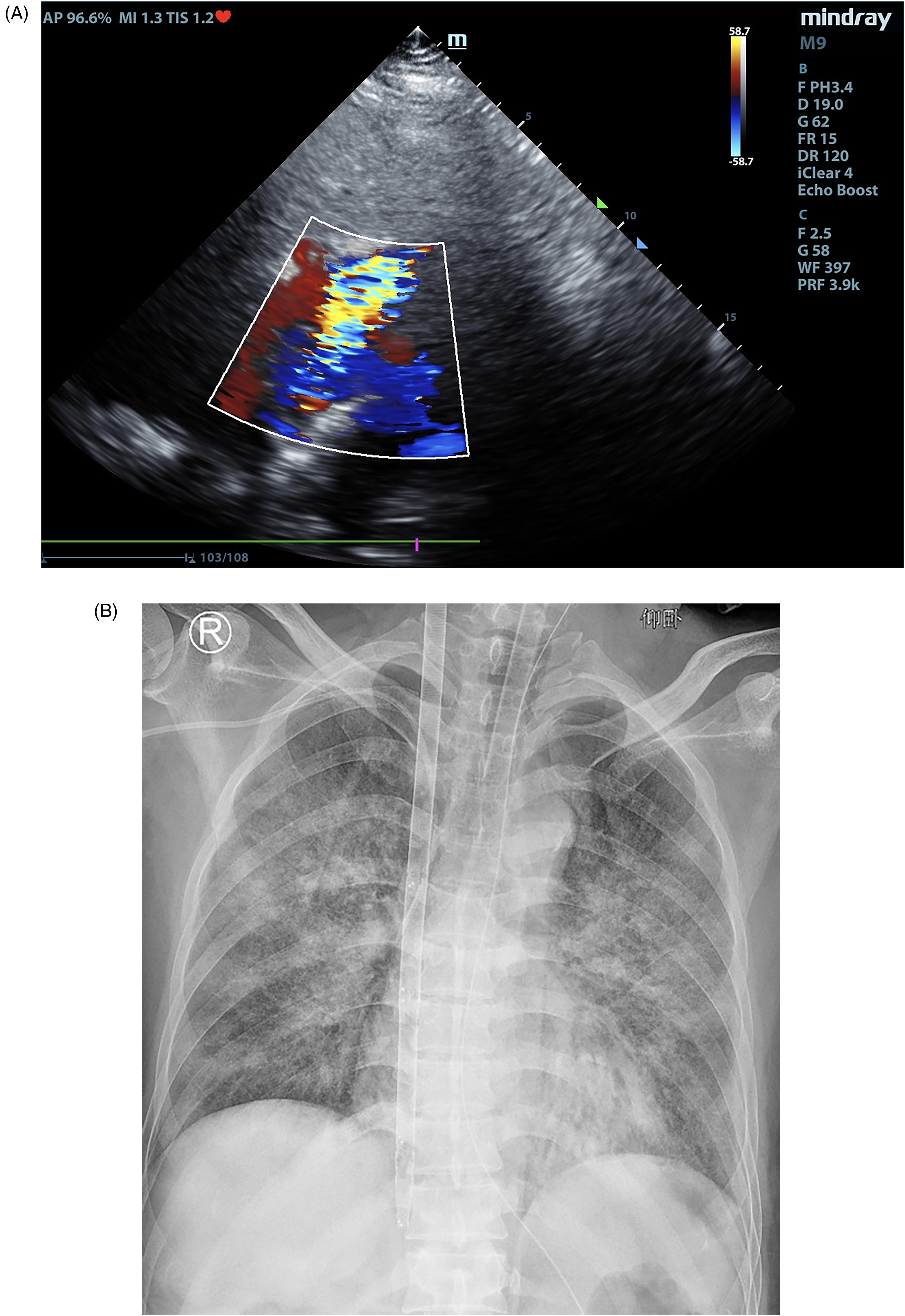
The cannula was withdrawn until the distance from the open of IVC to the tip was about 7 cm. Ultrasonographic image obtained in a subxiphoid four-chamber view shows the blood flow towards the tricuspid valve. IVC, inferior vena cava.
We have performed TTE-guided DLC cannulation for four patients requiring V-V ECMO during the fifth wave of COVID-19. All patients were critically ill with low P/F requiring urgent cannulation. There were no cannulation-related complications. In our experience, we have not aborted any procedure by adopting this technique. The characteristics of the patients are listed below in Table 1.
Characteristics of Four Patients with DLC V-V ECMO.
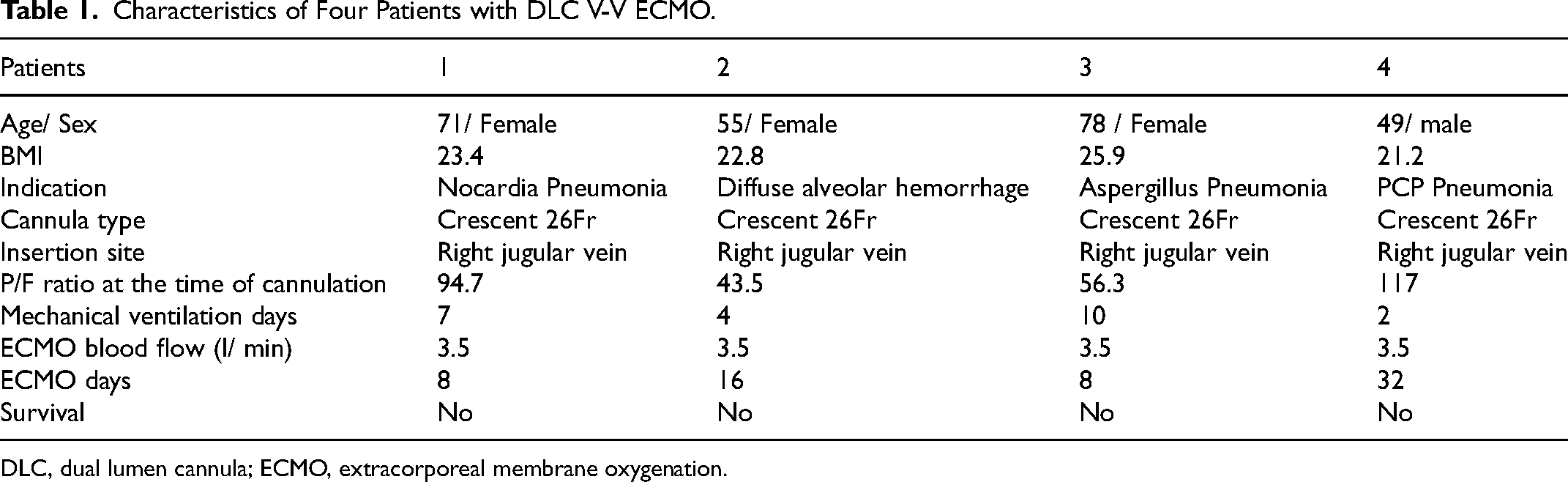
DLC, dual lumen cannula; ECMO, extracorporeal membrane oxygenation.
Discussion
To our knowledge, this is the largest case series reporting DLC insertion entirely guided by TTE, which showing this approach is consistently applicable when the technical aspects during insertion is protocolized. Le et al. reported one patient successfully cannulated with such approach during COVID-19 outbreak with similar technique. 9 An institutional protocol has been developed to ensure steps are properly followed during cannulation (Table 2).
Institutional Step-by-Step Guide for TTE-Guided DLC Cannulation/.
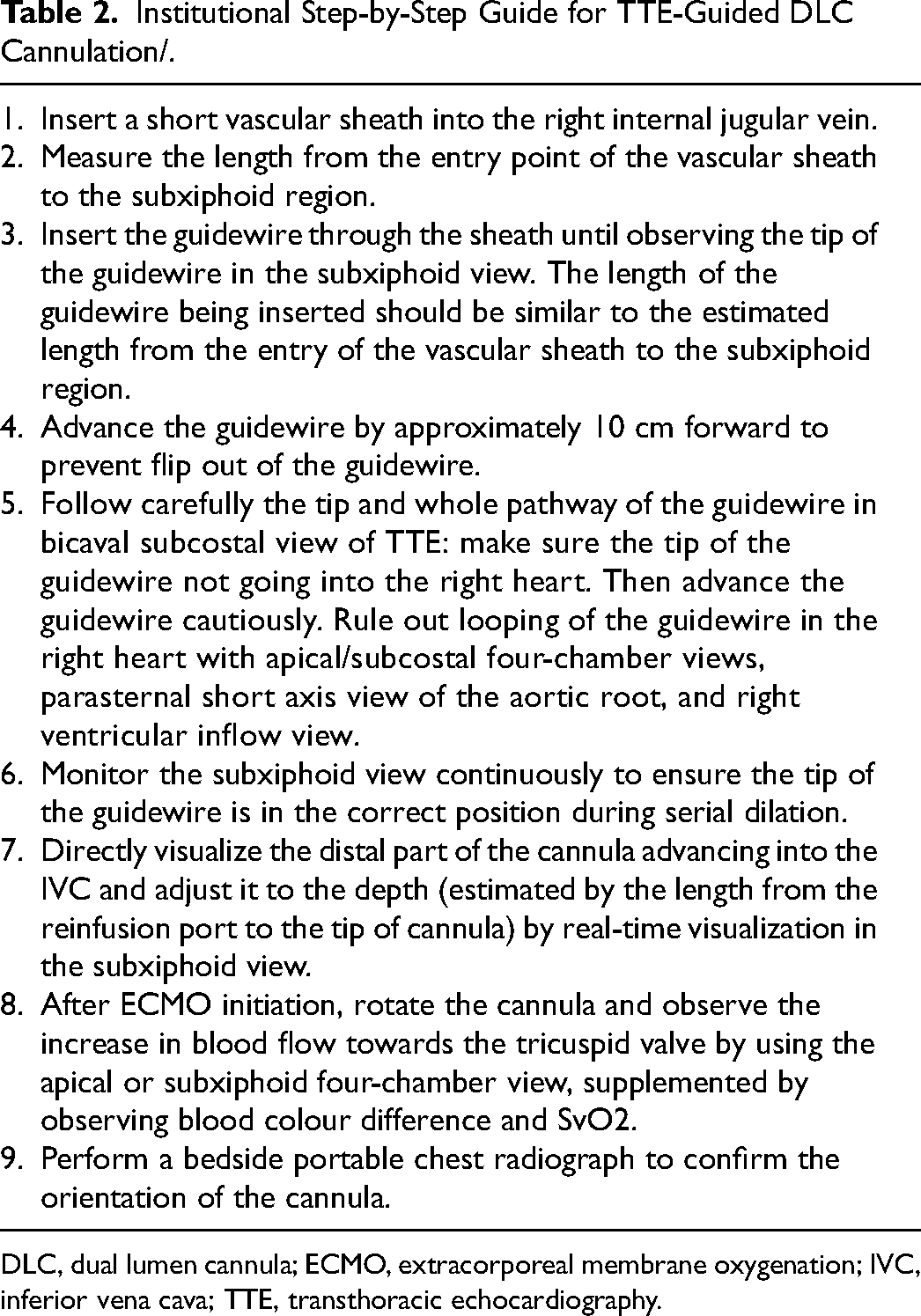
DLC, dual lumen cannula; ECMO, extracorporeal membrane oxygenation; IVC, inferior vena cava; TTE, transthoracic echocardiography.
TTE is readily available in all ICU and most ICU specialists can perform good quality TTE, whereas TEE requires advanced training. Moreover, patients requiring V-V ECMO are often unstable, and transferal outside of ICU is not favourable. The ability to use transthoracic echocardiogram to guide double lumen cannula insertion thus provides an alternative for these patients, especially at a time of disease outbreak, and routine workflow and resource allocation are jeopardized.
Nonetheless, there are several limitations of this technique. Firstly, TTE image quality can be affected by body habitus, especially in obese and mechanically ventilated patients, whenever in doubt, mobile X-ray would be useful to confirm the guidewire straightening as described by Uemura et al.11 Secondly, the operators are experienced in ECMO cannulation making this technique not generalizable. Thirdly, in our experience, the time required for manipulating the guidewire into the IVC can be lengthy. The implications of these limitations are twofold: it required careful monitoring of vital signs during the procedure, and the readiness for alternative cannulation plan should this technique fail. Lastly, direct visualization of the outflow jet from reinfusion port directed towards the tricuspid valve by TTE will depend on image quality. As a result, blood colour difference, SvO2 and CXR are essential as supplementary tools to assess the degree of recirculation.
Conclusions
In conclusion, the case series described the technique and feasibility of using TTE in DLC insertion that can be adopted in future endemic as a supplementary tool when there are restrictions on manpower and patient transfer. We still recommend the use of fluoroscopy/TEE-guided insertion technique as standard practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.