
Abstract
Objectives
To determine whether a nurse practitioner and physician assistant (NP/PA)-led rapid staffing. Model in the cardiac surgical intensive care unit (ICU) can optimize resource utilization without compromising safety or increasing hospital length of stay (LoS).
Design
Retrospective observational cohort study comparing before-and-after implementation of an NP/PA-led rapid recovery pathway.
Setting
A large tertiary referral academic cardiac surgery ICU.
Participants
There were 116 patients in the prerapid recovery cohort and 153 in the postimplementation rapid recovery phase.
Interventions
Low-risk cardiac surgery patients were selected for postoperative care by an NP/PA-led ICU staffing model.
Measurements and Main Results
Mean hospital LoS in the prerapid recovery cohort was 5.7 days compared to 5.2 days in the rapid recovery pathway cohort (P = .02). Thirty-day hospital readmission in the prerapid recovery pathway cohort was 7.8% compared with 2.0% in the rapid recovery cohort (P = .04). The ICU readmission rate for prerapid recovery cohort was 4.3%, while the rapid recovery percentage was 2.0% (P = .30).
Conclusions
Overall, implementation of an NP/PA-led postcardiac surgical ICU team (rapid recovery pathway) was associated with similar ICU LoS, hospital LoS, ICU readmission rates, 30-day readmission rates, and no significant signal of increased adverse events or safety concerns.
Introduction
Contemporary cardiovascular surgery comprises a broad spectrum of surgical complexity and patient acuity. Depending on the surgical procedure and a patient's preoperative medical complexity, the required postoperative course can be relatively uncomplicated and at least partially protocolized. Recently there has been added emphasis on the cost-effectiveness of surgical treatments, including concerns about inpatient staffing constraints and the rising costs of inpatient hospital care. 1
At our institution, a rapid recovery pathway was conceived and designed to select adult cardiovascular surgery patients expected to have an uncomplicated intensive care unit (ICU) course. Therefore, we reasoned that the traditional ICU staffing model which was historically used to care for all cardiovascular surgery patients (including patients requiring postoperative mechanical circulatory support, advanced mechanical ventilator management, frequent blood transfusions, and/or complex immunosuppression therapies) may not be required for patients who are relatively stable postoperatively. For example, a healthy 60-year-old patient undergoing an elective and uncomplicated Bentall procedure likely would not require the same ICU resources as a 75-year-old medically complex patient undergoing a third-time redo-mitral and tricuspid valve replacement. With this premise in mind, we created a new nurse practitioner and physician assistant (NP/PA)-led postoperative ICU staffing model for the subset of cardiovascular surgery patients who met inclusion criteria. We performed an observational study to examine the outcomes of the new NP/PA-led rapid recovery pathway and used a historical cohort of patients who also would have met inclusion criteria for the rapid recovery pathway.
Methods
We performed a retrospective observational cohort study comparing patients 18 years and older who were enrolled in a new postoperative rapid recovery pathway, and a historical cohort of patients who met inclusion criteria for the postoperative rapid recovery pathway (but were not enrolled in the pathway because it had not yet been launched). Demographic data, procedure type, ICU complications, and postoperative outcomes were collected, summarized, and compared between the 2 cohorts. The study was approved by the institutional review board (IRB 24-001784).
Setting
The study was performed at a tertiary referral medical center with a robust cardiovascular surgery program routinely completing more than 2500 cardiac surgical cases each year. Postoperatively, all cardiovascular surgical procedures for adult patients who require cardiopulmonary bypass or extracorporeal membrane oxygenation are admitted to a 32-bed closed cardiovascular surgical ICU (CVS ICU). The adult CVS ICU has been a closed unit for more than 10 years and is staffed by a team of dedicated anesthesiologist intensivists and CVS-trained NPs/PAs 24 h a day. ICU admission was required for all patients requiring mechanical ventilation, new noninvasive positive pressure ventilation (NIPPV) (ie, not home NIPPV settings), hemodynamic instability (heart rate <50 or >120 bpm, mean arterial pressure <60 mmHg, or systolic blood pressure <90 or >150 mmHg), vasoactive infusions, need for more than 4 L/min supplemental oxygen to maintain SpO2 > 92%, respiratory rate <8 or >24 breaths/min, and temporary epicardial pacing wire-dependent heart rhythms.
Rapid Recovery Pathway and Staffing Details
The inclusion and exclusion criteria for the rapid recovery pathway are outlined in Table 1. The primary discrete differences in the rapid recovery pathway (compared to the traditional ICU pathway) were (i) admission by an NP/PA-led multidisciplinary ICU team and (ii) admission to a prespecified subsection of the cardiovascular surgical ICU (geographically separate from the highest-acuity subsection of the ICU where mechanical circulatory support is managed). Although the rapid recovery pathway team was an NP/PA-led ICU team, there was an ICU physician immediately available for consultation as needed. Criteria for mandatory ICU physician consultation are outlined in Table 2. In other words, although the intensivist physician was not directly supervising rapid recovery pathway patients, an intensivist physician was in-house and immediately available at all hours in case clinical deterioration resulted in a patient “falling off” the rapid recovery pathway. The subset of NP/PAs who volunteered to cover the rapid recovery pathway had >1 year of experience in cardiac surgical critical care (range 4–11 years, median 7.5 years). The initial cohort consisted of 6 NPs and 2 PAs. No additional training was required before working in the rapid recovery pathway. ICU staffing prior to implementation of the rapid recovery pathway consisted of 1 NP/PA paired with 1 critical care physician to cover an 8-bed pod of the CVS ICU. The staffing ratio during the preimplementation period and postimplementation period were both 1 : 8 (1 NP/PA per 8 patients). During the postimplementation period of the rapid recovery pathway, the NP/PA led multidisciplinary bedside rounds for patients in the rapid recovery pathway, and the ICU physician was involved if there was concern that the patient was meeting exclusion criteria for the rapid recovery pathway.
Rapid Recovery Pathway Patient Selection Criteria.
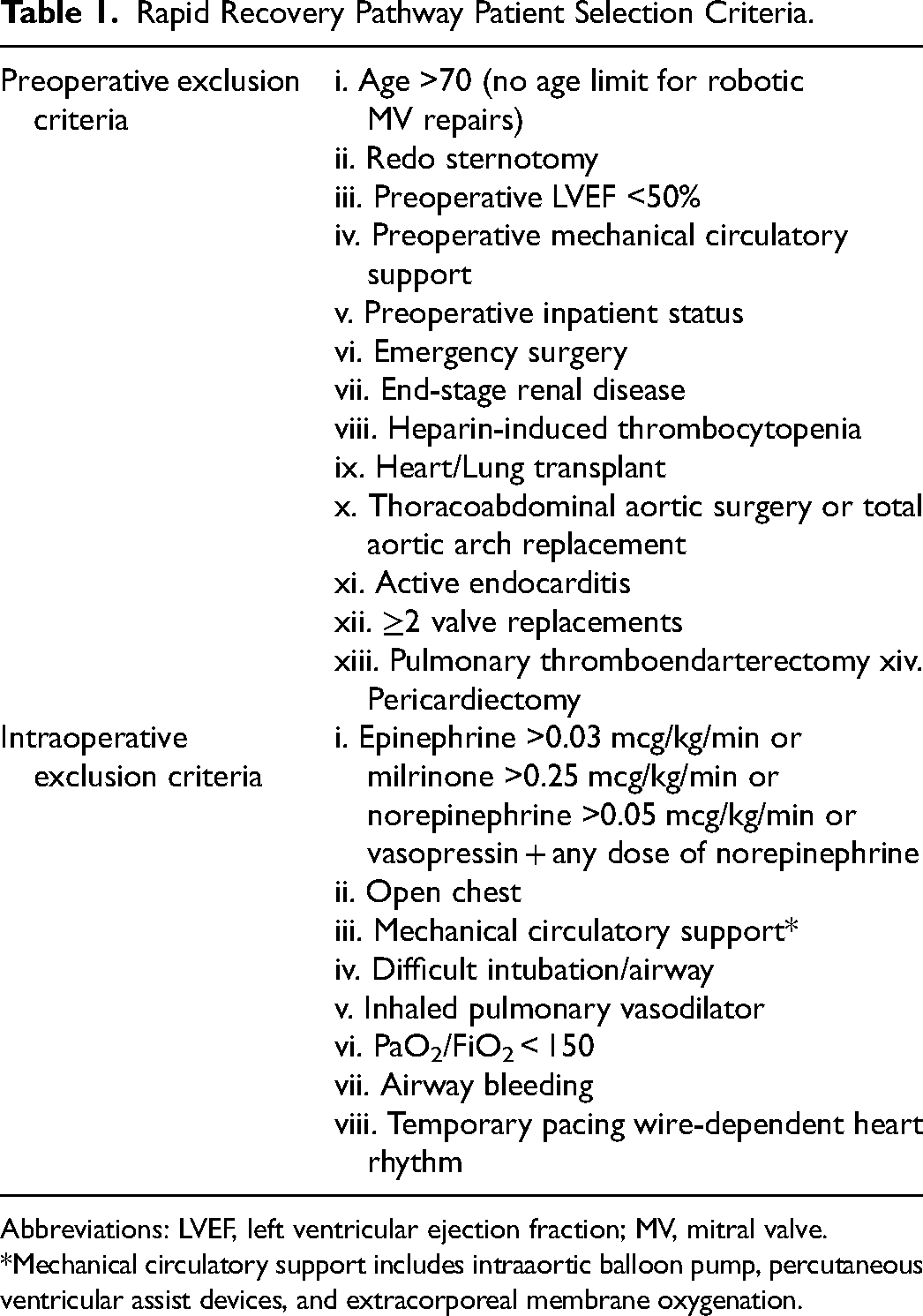
Abbreviations: LVEF, left ventricular ejection fraction; MV, mitral valve.
*Mechanical circulatory support includes intraaortic balloon pump, percutaneous ventricular assist devices, and extracorporeal membrane oxygenation.
Criteria for Removal From Rapid Recovery Pathway.
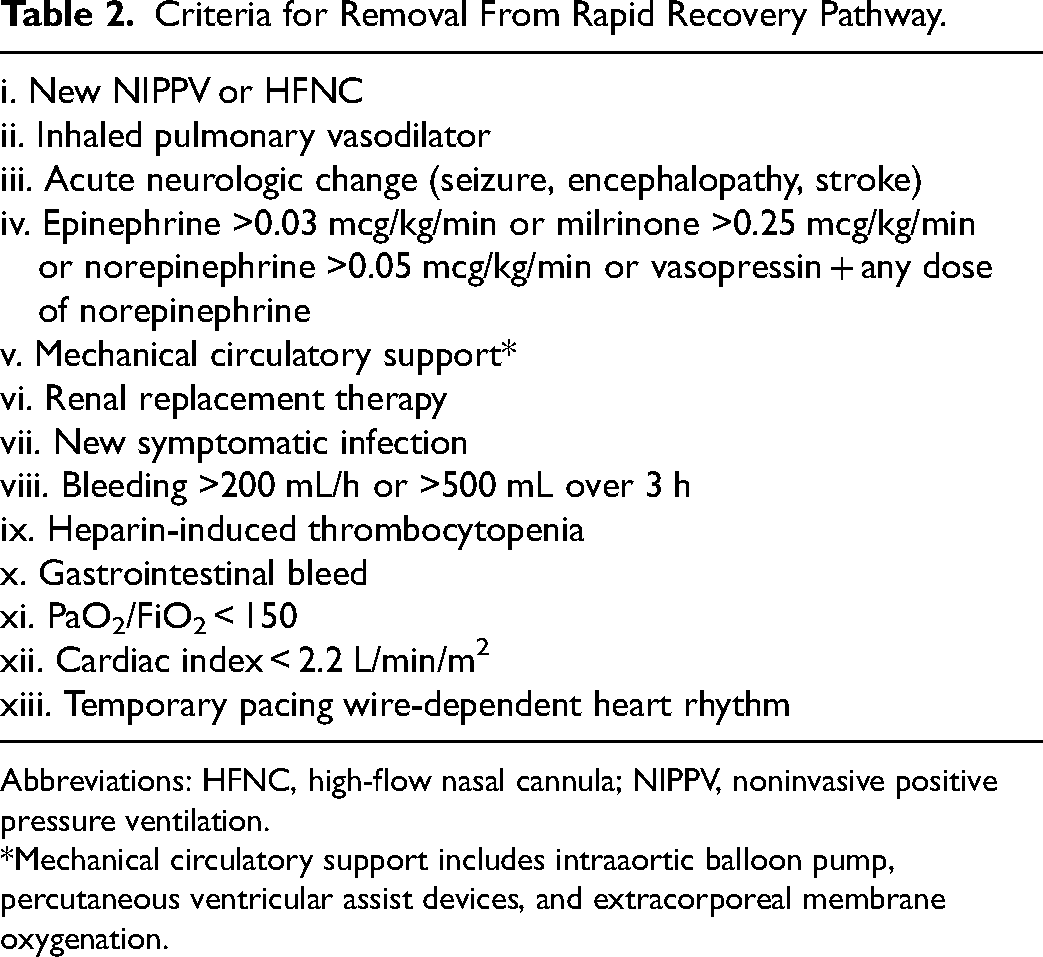
Abbreviations: HFNC, high-flow nasal cannula; NIPPV, noninvasive positive pressure ventilation.
*Mechanical circulatory support includes intraaortic balloon pump, percutaneous ventricular assist devices, and extracorporeal membrane oxygenation.
Statistical Analysis
Summary statistics were performed and presented as counts and proportions for categorical variables and medians and interquartile ranges (IQRs) for continuous variables. The primary outcome was hospital length of stay (LoS), chosen as an overall marker of quality of care, given the fact that any complications or safety events (even if not explicitly captured in our data review) during patient admission would certainly result in prolonged hospital LoS. A comparison of categorical variables was completed with the chi-square test (or the Fisher exact test if <5 observations), and for continuous variables with nonparametric data distribution and small sample size, the Mann–Whitney U test was performed. The threshold for statistical significance was defined as P < .05. Statistical analyses were performed with BlueSky Statistics v10.3 (BlueSky Statistics).
Results
After exclusions for lack of research consent (MN Research Authorization) and intraoperative exclusion criteria (Table 1), 116 adult patients were included in the historical “pre-rapid recovery pathway” cohort, and 153 patients were included in the postimplementation “rapid recovery pathway” cohort. Patient screening and ultimate inclusion are detailed in Figure 1. The “pre-rapid recovery pathway” cohort timeframe was March 13, 2023–May 12, 2023. “Pre-rapid recovery pathway” data were collected and used by our clinical leadership team to determine whether to formally launch the “rapid recovery pathway” later that year, which explains the time lag between the 2 cohorts. During the rapid recovery pathway timeframe (October 2, 2023–February 29, 2024), 957 index cardiovascular surgical procedures were completed at the study institution. Therefore, the proportion of index cardiovascular surgical procedures that were admitted to the postoperative ICU on the rapid recovery pathway was 16.0% (153 of 957 patients). Excluding the 133 emergency cases and 48 transplants, the proportion of routine cardiovascular surgical procedures that were admitted to the postoperative ICU on the rapid recovery pathway was 19.7% (153 of 776 patients).
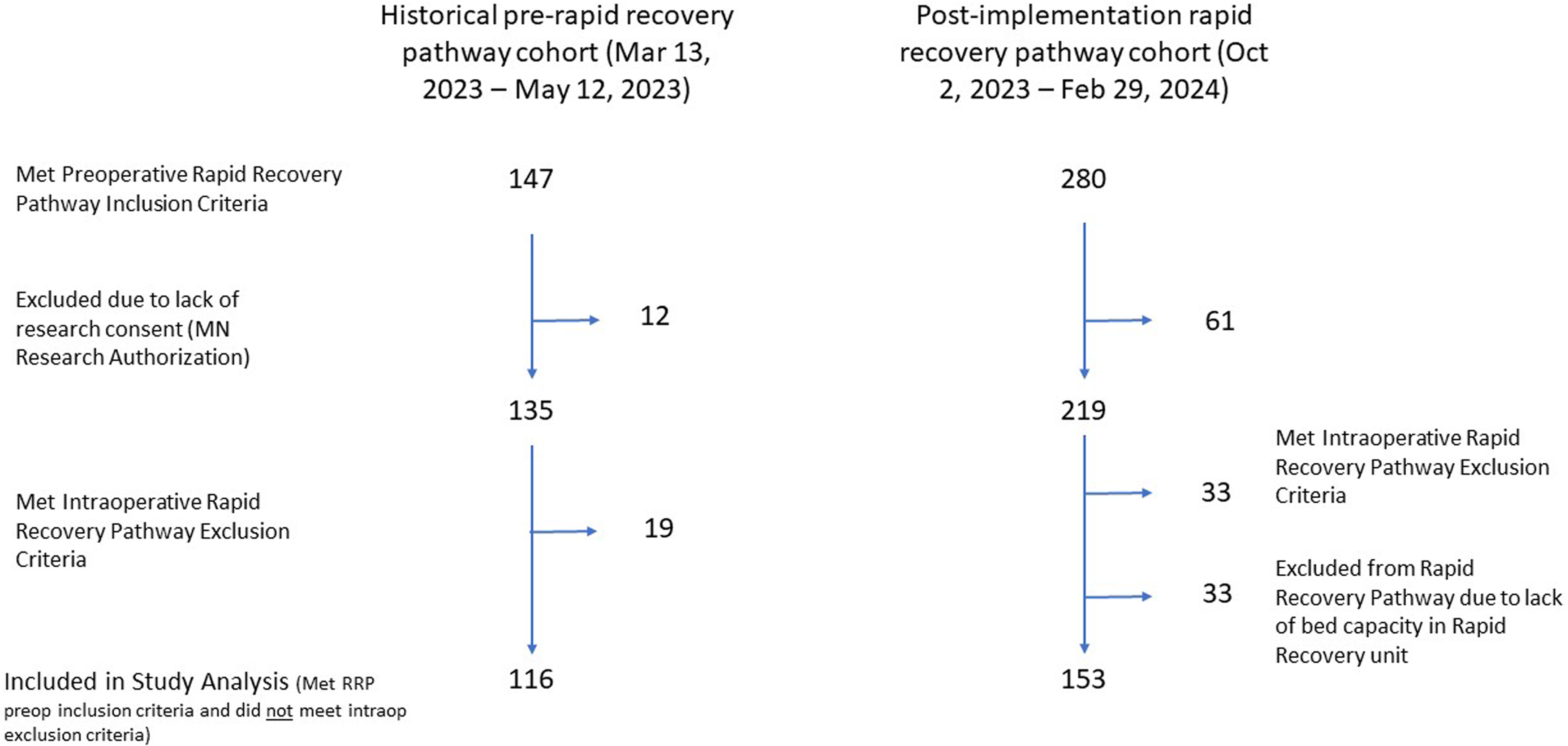
Study enrollment flowchart.
Summary and comparison of demographic data for patients who met preoperative criteria for inclusion in the rapid recovery pathway and did not meet any intraoperative exclusion criteria are detailed in Table 3. No statistically significant differences were found between the baseline characteristics of the preimplementation and postimplementation cohorts. Summary and comparison of outcome data for patients who met preoperative criteria for inclusion in the rapid recovery pathway and did not meet any intraoperative exclusion criteria are detailed in Table 4. No baseline patient demographics were statistically significantly different between the 2 cohorts. The only outcome variables with a statistically significant difference between the 2 cohorts were hospital LoS and 30-day readmission rates, both of which were lower in the rapid recovery pathway cohort. The hospital LoS was a median of 5 days in both cohorts, but the mean (range) for the preimplementation cohort was 5.7 days (3–29) versus 5.2 days (2–28) in the rapid recovery pathway cohort, suggesting a slightly shorter total hospital LoS in the rapid recovery pathway cohort. Table 5 outlines the proportion of those who met preoperative inclusion criteria (Table 1), the proportion excluded due to intraoperative exclusion criteria (Table 1), and the proportion of patients who were admitted to the ICU as rapid recovery patients but later met rapid recovery pathway exclusion criteria (Table 2).
Patient demographics.
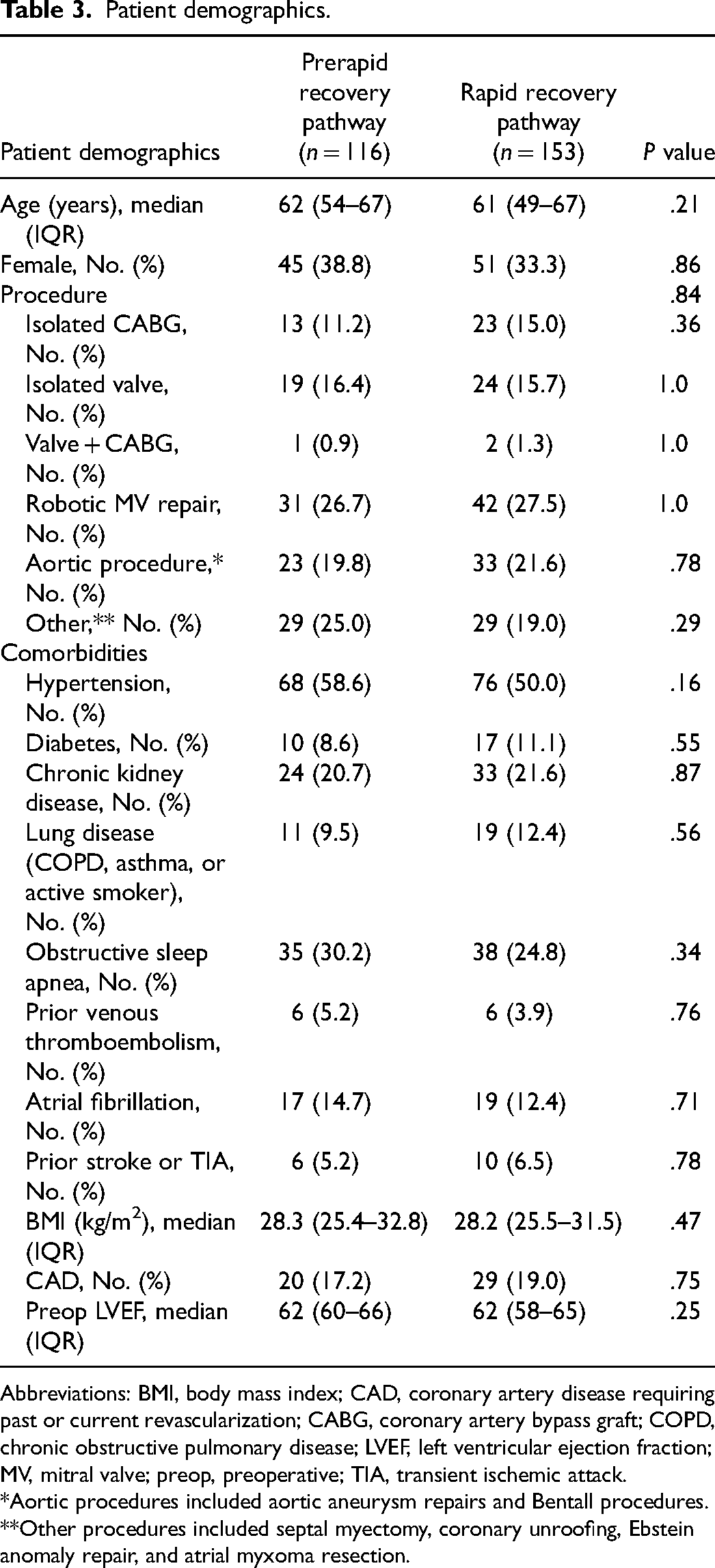
Abbreviations: BMI, body mass index; CAD, coronary artery disease requiring past or current revascularization; CABG, coronary artery bypass graft; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; MV, mitral valve; preop, preoperative; TIA, transient ischemic attack.
*Aortic procedures included aortic aneurysm repairs and Bentall procedures.
**Other procedures included septal myectomy, coronary unroofing, Ebstein anomaly repair, and atrial myxoma resection.
Patient outcomes.
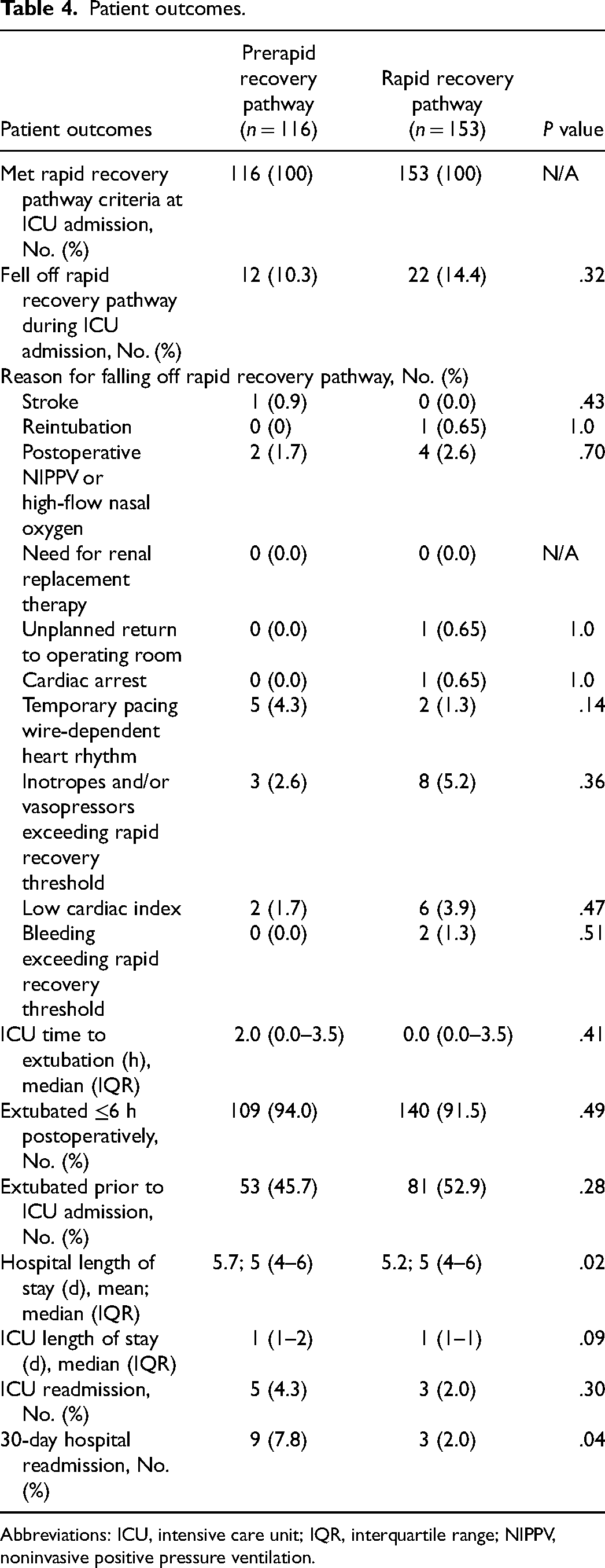
Abbreviations: ICU, intensive care unit; IQR, interquartile range; NIPPV, noninvasive positive pressure ventilation.
Selection of Rapid Recovery Pathway Patients.
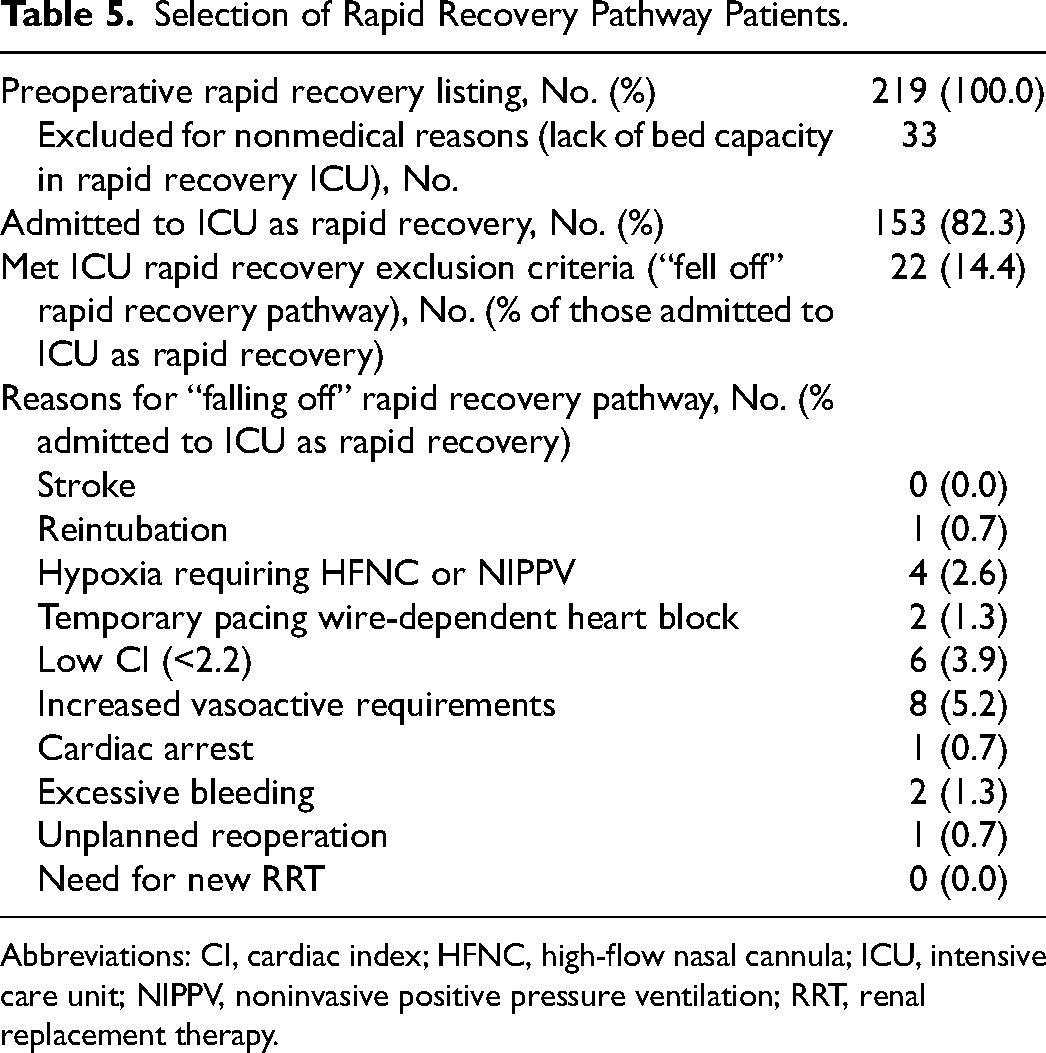
Abbreviations: CI, cardiac index; HFNC, high-flow nasal cannula; ICU, intensive care unit; NIPPV, noninvasive positive pressure ventilation; RRT, renal replacement therapy.
Patients Who “Fell Off” the Rapid Recovery Pathway
Of the 153 patients admitted to the ICU on the rapid recovery pathway, 22 patients (14.4%) “fell off” the pathway (met predefined criteria that required a physician intensivist consultation). Reasons for “falling off” the pathway are summarized in Table 4. There were no deaths. The median hospital LoS in this subgroup was 6 days (IQR, 6–7) and the median ICU LoS was 2 days (IQR, 2–3.75). The patient who suffered a cardiac arrest from sudden-onset ventricular tachycardia shortly after ICU admission to the NP/PA-led team had no neurologic insult, was discharged alive, and had no ICU readmission or 30-day hospital readmission. A thorough review of this case demonstrated that the cause of the arrest (acute coronary occlusion) could not be attributed to the ICU care team model, and as designed, the full extent of ICU resources (including the physician intensivist) was immediately called to the bedside by the NP/PA-led team.
Discussion
This study describes the implementation and outcomes of a novel NP/PA-led postcardiac surgical ICU team and demonstrates the safety and efficiency of such a model for appropriately selected adult cardiac surgery patients. Although the name chosen for the new NP/PA-led ICU care was rapid recovery pathway, the overarching intent was not focused on dismissing patients from the hospital more quickly. The primary intent of the rapid recovery pathway was to more responsibly allocate resources to patients under our care. This is a critical distinction, because the primary motivators for this practice change were to (i) deploy our critical resources where they would have the most impact and (ii) avoid any negative safety impacts (intended or otherwise) on our patients. The name rapid recovery pathway was chosen because, for the general audience, it had more positive connotations than other names we had contemplated. For example, efficient staffing model or streamlined staffing model may have suggested that necessary resources were diverted from the care of the patients in this pathway, when in fact concrete steps were taken to ensure immediate availability of the full ICU repertoire to maintain our high safety standards for all of our ICU patients. Although somewhat limited by sample size, our data reported here demonstrate the safety of the NP/PA-led coverage model for appropriately selected cardiovascular surgical ICU patients. In our cardiac surgical practice, ∼19.7% of listed surgery patients met the criteria for postoperative rapid recovery pathway admission. Considering the high complexity of cases (including multiple redo surgeries) at our institution, other cardiac surgical centers may encounter a higher proportion of listed surgery patients who meet our selection criteria for postoperative rapid recovery pathway admission.
A sizeable body of literature is accumulating to support the value of incorporating NP/PA staff into acute care and intensive care settings, including positive impacts on safety and quality metrics, continuity of care, and patient satisfaction. 2 However, few publications to date offer data specifically pertaining to the transition of surgical ICU care from a physician-led model to an NP/PA-led model. A survey of 965 cardiac surgical centers published in 2020 described how postoperative ICU staffing models vary throughout the US. 3 The majority (47%) of cardiothoracic ICUs were “open” (covered by cardiac surgeons who were not assigned to primarily cover the ICU), and PAs were the primary after-hours clinicians in 44% of the cardiothoracic ICUs. In a similar study performed in Canadian cardiac surgical ICUs, 26% were semiopen (a dedicated intensivist was staffing the ICU for <7 days per week) and 70% were closed ICUs, but did not specifically report on the presence of NP/PA staff in the ICU. 4 In our study, the baseline (nonrapid recovery) and rapid recovery pathway ICU coverage models are both in the context of a closed ICU (covered by dedicated intensivists) who are also in-house during all hours of the day. Again, although the physician intensivist was not directly supervising the care of rapid recovery pathway patients, a physician intensivist was always available and in-house if any clinical deterioration occurred prompting “falling off” the rapid recovery pathway.
A recent publication describing a fast-track pathway of care for carefully selected low-risk cardiac surgery patients is a retrospective single-center study by Haunschild et al. 5 Adult patients undergoing elective Bentall procedures were either selected for conventional postoperative care (direct admission to the CVS ICU) or fast-track care (admission to an anesthesiologist-staffed postanesthesia care unit [PACU]) before transfer to a common intermediate care unit. Propensity score matching was performed before comparison of the traditional and fast-track cohorts. The fast-track cohort had a shorter duration of postoperative mechanical ventilation and shorter ICU/PACU duration. There was no difference in hospital LoS or 30-day mortality.
A report of a carefully selected cohort of patients who were only selected for fast-track status (discharge from ICU on postoperative day 0) after ICU admission showed favorable safety outcomes. 6 It should be noted that this study's results were impacted by selection bias and, unlike our study, did not study any changes in the postoperative staffing model. A randomized trial of fast-track cardiac surgery focused primarily on the impact of intraoperative anesthetic management on postoperative outcomes of cardiac surgery patients. 7 This study enrolled only patients undergoing elective coronary artery bypass grafting (CABG). In the fast-track group, the mean ICU admission-to-extubation time was 4.1 h, and the mean hospital LoS was 7.6 days. These studies are distinct from what was investigated in our study—specifically, our study focused primarily on the postoperative ICU staffing model, rather than intraoperative management or postoperative protocols.
A descriptive study of implementation of an NP/PA ICU staffing model in a mixed medical–surgical ICU in the Netherlands showed how NP/PA staff can reduce physician intensivist and resident physician workload. 8 In contrast to our study, the NP/PA staff in the Dutch study was trained to place invasive lines (arterial lines and central venous catheters) independently. Another retrospective cohort study from Taiwan described the addition of NPs to an open surgical ICU. 9 This study described an effort to introduce NPs to help the practice cope with resident work-hour restrictions and is not a direct comparison to our study. In a study of Japanese surgical ICUs, Mori et al 10 described the outcomes associated with integration into their practice. The new surgical staffing model changed from physician intensivist only to a physician intensivist-plus-NP model, and this change was associated with a reduction in ICU LoS but no change in hospital LoS or mortality. A non-ICU study described the impact of changing a non-ICU inpatient staffing model to include PAs in addition to physicians. 11 In this study, a combined physician–PA inpatient staffing model was associated with a reduction in median hospital LoS and no change in 30-day readmission, compared to the historical physician-only staffing model. A recent review outlined the growing presence and considerations regarding how best to integrate NPs and PAs into medical cardiac ICU practices. 12
Our study is limited by its retrospective and observational design. There is inherent selection bias with this design, but a comparison of baseline demographics and procedures showed no clear differences between the cohorts.
Footnotes
Acknowledgments
The Scientific Publications staff at Mayo Clinic provided copyediting support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.