
Abstract
Background
Persistent vasopressor requirements are a common reason for delayed liberation from the intensive care unit (ICU) and adjunct oral agents are sometimes used to hasten time to vasopressor discontinuation. We sought to describe the use of droxidopa for vasopressor weaning in critically ill patients with prolonged hypotension.
Materials and Methods
This retrospective, single-arm, observational study included adult patients admitted to an ICU at two academic centers between 06/2016–07/2023 who received droxidopa for vasopressor weaning. Patients who received droxidopa prior to admission or for another indication were excluded. The primary outcome was time to vasopressor discontinuation, defined as when vasopressors were stopped and remained off for at least 24 h. Secondary outcomes included rates of tachycardia and hypotension post-initiation, norepinephrine equivalents pre- and post-initiation, concomitant oral agent use, and dosing. A subgroup analysis was conducted in patients receiving droxidopa via feeding tubes.
Results
A total of 30 patients met inclusion criteria. Median age was 62 years old, 12 (40%) were female, and 73% were in a cardiac/cardiac surgical ICU. Patients were on vasopressors for a median of 16 days prior to droxidopa initiation. Median (IQR) time to vasopressor discontinuation was 70 h (23-192) and norepinephrine equivalents decreased immediately after initiation (0.08 vs 0.02 mcg/kg/min, p < 0.001). MAP increased after droxidopa initiation (68.8 vs 66.5 mm Hg, p = 0.008) while heart rates were unchanged (86 vs 84 BPM, p = 0.37) after initiation. Patients who weaned from vasopressors within 72 h versus longer than 72 h after droxidopa initiation were more likely to be on lower norepinephrine equivalents prior to initiation (0.05 vs 0.12 mcg/kg/min, p = 0.013). Feeding tube administration did not impact time to vasopressor discontinuation (p = 0.93).
Conclusions
Droxidopa may be considered an adjunct therapy for vasopressor weaning. Effects were similar when analyzing patients receiving droxidopa via feeding tube.
Introduction
Patients with critical illness admitted to the intensive care unit (ICU) frequently require intravenous vasopressors for the management of hypotension. 1 Periodically, prolonged courses of intravenous vasopressors even after resolution of critical illness may be necessary, resulting in prolonged ICU admissions. 2 Adjunctive oral vasoactive agents such as midodrine have been used off-label as a means to facilitate intravenous vasopressor weaning in this subset of patients. Midodrine, an oral alpha1 adrenergic receptor agonist, has been shown to cause modest increases in supine and standing blood pressure measurements and is commonly utilized off-label in ICU patients for the facilitation of vasopressor weaning. Trials evaluating its use for this indication, however, suggest that its use may not reduce the duration of vasopressor therapy or length of ICU admission.3,4
Droxidopa is an alternative oral vasoactive agent which is a prodrug of norepinephrine and is approved for use in neurogenic orthostatic hypotension (nOH). While commonly initiated in the outpatient setting, one small study reported the successful use of droxidopa in severely ill, hospitalized patients with underlying nOH. 5 The authors concluded that droxidopa initiation in these patients was safe and effective, with sustained benefit beyond hospitalization. Given its success in inpatients with nOH, droxidopa has been considered in the ICU to hasten vasopressor weaning in critically ill patients refractory to other oral vasoactive medications such as midodrine. Currently, there is limited data on the utilization of droxidopa as an adjunct agent in this subset population. This study aimed to describe the use of droxidopa for vasopressor weaning in a mixed population of critically ill adults, including its effects on hemodynamics, vasopressor doses, and time to liberation from intravenous vasopressors.
Materials and Methods
This was a multicenter retrospective cohort study conducted at two tertiary academic medical centers: Massachusetts General Hospital and Brigham and Women's Hospital, both in Boston, MA. Patients admitted to any ICU at either hospital that were administered droxidopa between June of 2016 and July of 2023 were screened for inclusion. Patients were eligible for inclusion if they were over the age of 18, received intravenous vasopressors, and received droxidopa for vasopressor weaning. Patients were excluded if they were prescribed droxidopa prior to admission or received droxidopa for an indication other than assistance with vasopressor weaning. The study was reviewed by the Massachusetts General Brigham Institutional Review Board and was deemed exempt.
Data Collection
Data were extracted from the electronic medical record and enterprise data warehouse and entered into a common REDCap instrument.6,7 Data collected included baseline demographics, admission details, indication for vasopressor therapy, administration time and dosing of all droxidopa doses administered during the ICU stay, and hourly vital signs collected during the ICU stay. Blood pressures were primarily captured from automated blood pressure cuffs, but blood pressures collected from arterial lines were also collected. Details on vasopressor and inotropic support were also collected, including which vasopressors and inotropes were administered to the patient during their ICU stay, norepinephrine equivalent doses, and which other adjunctive vasoactive medications (midodrine, pseudoephedrine, fludrocortisone, or pyridostigmine) patients received. Ephedrine was not used in this cohort. Norepinephrine equivalents were calculated using the equation proposed by Kotani and colleagues: norepinephrine (mcg/kg/min) + epinephrine (mcg/kg/min) + 0.001 * dopamine (mcg/kg/min) + 0.06 * phenylephrine (mcg/kg/min) + 2.5 * vasopressin (U/min). 8 Angiotensin II was not available at either institution during any of the study period.
Outcomes
The primary outcome was the time from droxidopa initiation to vasopressor discontinuation. Vasopressor discontinuation was defined as the time when all vasopressors were stopped and remained off for at least 24 h after droxidopa initiation. Secondary outcomes included rates of tachycardia and hypotension after droxidopa initiation compared to the 24 h prior to initiation, mean norepinephrine equivalents pre- and post-initiation, adjunct oral agent use, and droxidopa dosing. Differences in rates of tachycardia (HR >100 bpm) and hypotension (MAP <65 mm Hg) were calculated as the percent of hourly vital sign measurements that met the criteria for tachycardia or hypotension in the 24 h preceding droxidopa initiation compared to the percent of hourly measurements meeting the criteria during either the 7 days after droxidopa was initiated or until droxidopa was discontinued, whichever came first. Changes in norepinephrine equivalents were calculated in the 24 h prior to droxidopa initiation and the 24 h after droxidopa was initiated.
Because the droxidopa package insert recommends against opening capsules and suggests capsules should be swallowed whole, an a priori subgroup analysis was planned to evaluate the differences in outcomes between patients who received droxidopa via a feeding tube (ie, the capsule was opened for administration) compared to patients who received the capsule whole. 9 Patients who had a feeding tube (orogastric, nasogastric, gastrostomy, or jejunostomy) in place while receiving droxidopa were considered to have received droxidopa via feeding tube, while patients without a feeding tube present were considered to have received the capsule whole. Standard administration technique was to mix the content of the capsule in 10 mL of water, administer via the feeding tube, and flush with 10–20 mL of water. Tube feeding was assumed to have been continued prior to administration, but this could not be reliably confirmed with the available data.
Statistical Analysis
Data were summarized using descriptive statistics, including means (standard deviation), median (interquartile range), or percents as appropriate. Differences in paired continuous variables were compared using the Wilcoxson matched pairs or paired student's t test, as appropriate, and unpaired data were compared using the Mann-Whitney U test or student's t test. Differences in categorical variables were compared using Mantel Haenszel test or Chi Squared test, as appropriate. Time to vasopressor discontinuation was assessed using survival plots constructed using the ggsurvfit package. An alpha level of 0.05 was considered significant. Statistical analysis was conducted using R, version 4.1.2. (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 44 patients received droxidopa in any ICU across both institutions during the study period of which 30 met inclusion criteria (Figure 1). Baseline demographics are summarized in Table 1; 12 (40%) patients were female, the median age was 62 years old, and 22 (73%) were admitted to a cardiac or cardiac surgical ICU. The most common admission diagnoses were acute coronary syndromes (20%) and valvular diseases (16.7%), and cardiogenic or mixed shock states were the most common indication for vasopressor therapy (33.3%). Droxidopa capsules were opened and administered via feeding tube in 21 (70%) of patients. The median hospital length of stay was 63 days and ICU length of stay was 44 days. Overall, 47% of patients experienced in-hospital mortality.
CONSORT Inclusion Flow Diagram.
Baseline Demographics.
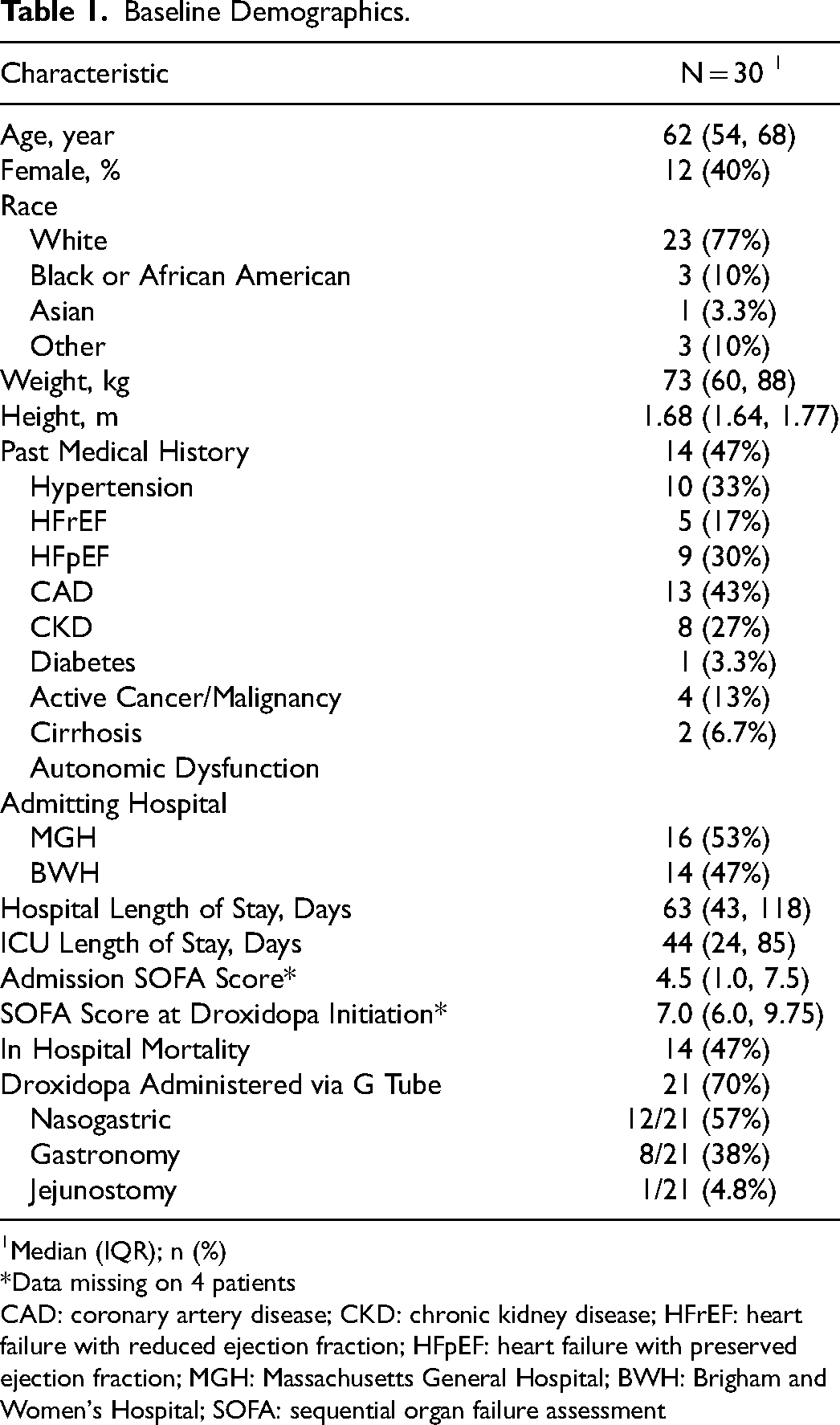
Median (IQR); n (%)
Data missing on 4 patients
CAD: coronary artery disease; CKD: chronic kidney disease; HFrEF: heart failure with reduced ejection fraction; HFpEF: heart failure with preserved ejection fraction; MGH: Massachusetts General Hospital; BWH: Brigham and Women's Hospital; SOFA: sequential organ failure assessment
Patients were on vasopressors for a median of 16 days (IQR 10-27) prior to droxidopa initiation. Adjunct agent use was common prior to droxidopa initiation: 27 (90%) patients received midodrine (median dose 90 mg/day), seven (23.3%) received fludrocortisone (median dose 0.2 mg/day), twelve (40%) received pseudoephedrine (median dose 150 mg/day), and one (3.3%) received pyridostigmine (60 mg/day) in the 24 h preceding droxidopa initiation (Table 2). The most frequent starting dose of droxidopa was 100 mg every 8 h. The median norepinephrine equivalent dose at the time of droxidopa initiation was 0.06 mcg/kg/min (IQR 0.03, 0.14). After droxidopa initiation, 25 (83.3%) patients continued midodrine, 10 (33.3%) continued pseudoephedrine, 5 (16.7%) continued fludrocortisone, and none continued pyridostigmine.
Vasopressors were weaned off within 7 days of droxidopa initiation in 19 (70.3%) patients. Three patients had vasopressors stopped shortly or immediately before droxidopa initiation and were not included in this percent calculation and one patient transitioned to hospice care within 7 days of initiation and vasopressor discontinuation was not counted as successful. The median time to vasopressor discontinuation in all patients (including those weaned off after 7 days of therapy) was 70 h (IQR 34, 192), Figure 2. The median daily dose of droxidopa at the time of vasopressor discontinuation was 600 mg/day (IQR 300, 1125) and the maximum daily dose was 2400 mg/day. Mean norepinephrine equivalents were 0.08 mcg/kg/min in the 24 h prior to droxidopa initiation and 0.02 mcg/kg/min in the 24 h after initiation (p < 0.001).

Time to Successful Vasopressor Weaning. Time to vasopressor discontinuation after droxidopa initiation. Three of the 30 patients had vasopressors discontinued immediately preceding the first droxidopa dose administration and thus are not included in the survival curve. Patients who died or transitioned to comfort measures or hospice prior to successful vasopressor discontinuation are censored (crossmark).
Vasopressor titrations are depicted in Figure 3. Mean HR was 84 BPM prior to and 86 BPM (p = 0.37) after initiation and mean MAP was 66.5 mm Hg and 68.8 mm Hg (p = 0.008) prior to and after droxidopa initiation, respectively. 13% and 18% of HRs were >100 BPM pre- and post-initiation (p = 0.35) and 43% and 33% of MAPs were <65 mm Hg pre- and post-initiation (p = 0.023), respectively. Median ICU length of stay prior to droxidopa initiation was 28 days (IQR 15, 52) and median time to transfer out of the ICU was 16 days (IQR 6, 36) after droxidopa initiation. Of the 16 patients surviving to hospital discharge, five (31.3%) were prescribed droxidopa at discharge. We additionally screened for patients whose droxidopa was discontinued but then re-initiated for recurrent hypotension. Of the 30 patients, 6 (20%) resumed droxidopa after initial discontinuation due to recurrent hypotension. The median time to re-initiation was 24 days (IQR 7-36); the remainder of patients either maintained on droxidopa up to or after discharge or did not require re-initiation after discontinuation.
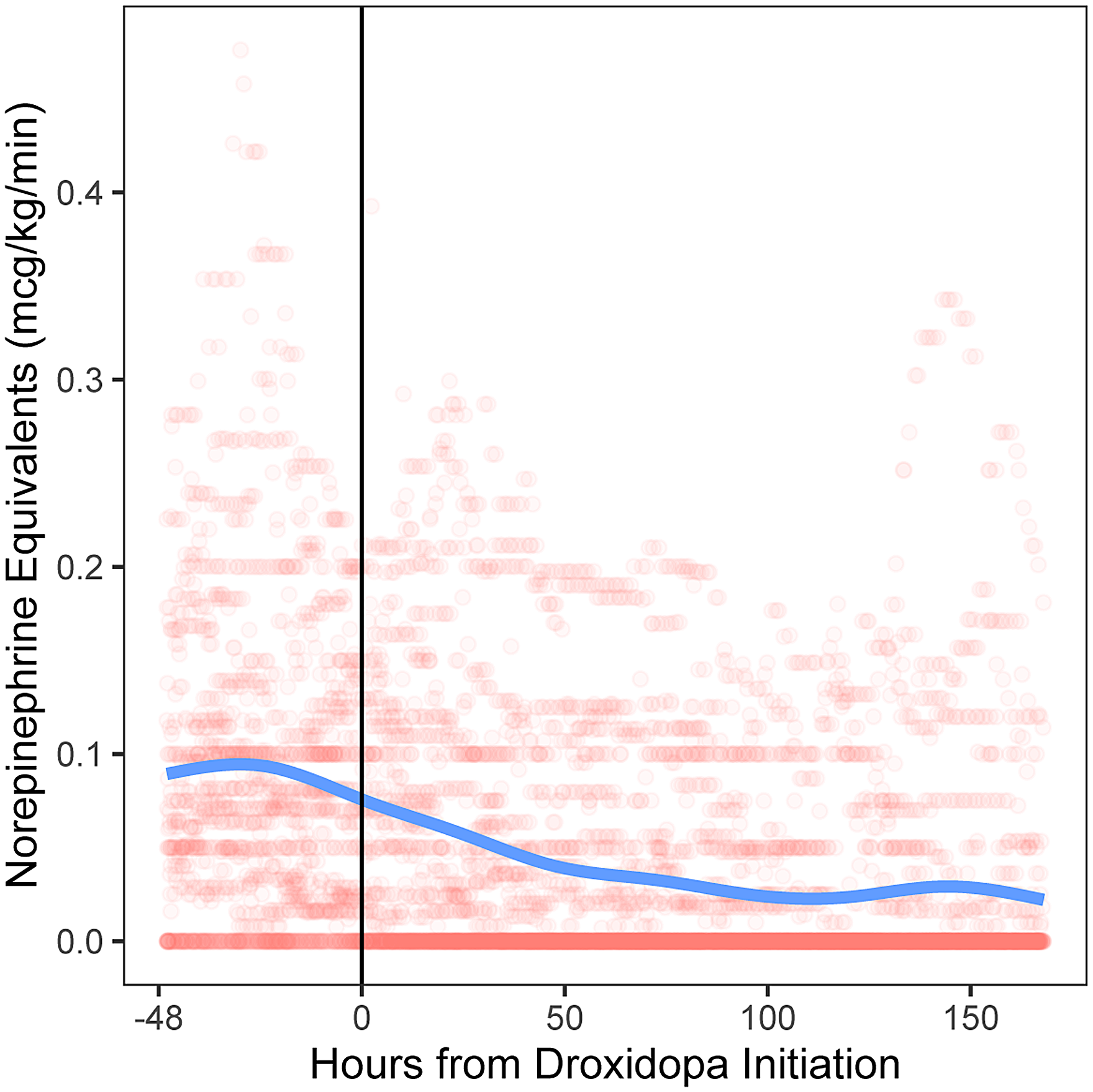
Vasopressor Titration After Droxidopa Initiation. The hourly norepinephrine equivalents for each hour in the 48 h preceding droxidopa initiation and up to 7 days after droxidopa initiation were calculated for each patient. Each dot represents an individual patient's norepinephrine equivalent dose at each hour; some jitter was introduced to prevent excessive stacking. After vasopressors were discontinued, patients were considered to be on a norepinephrine equivalent of 0 mcg/kg/min (increasing density of dots at 0 represents patients successfully weaning off vasopressors and staying off vasopressors). The solid vertical line at time 0 represents the relative time of the first droxidopa dose administration for each patient. The solid trend line represents a smoothed estimate of the overall vasopressor trajectory before and after droxidopa was initiated.
Time to event analysis demonstrated a flattening of the slope of the line at 72 h after droxidopa, suggesting patients who would successfully wean off vasopressors with the addition of droxidopa would be most likely to do so within 72 h of initiation. To identify whether any phenotypic differences existed between patients who successfully weaned off vasopressors within 72 h of droxidopa initiation (“responders”) and those who did not (“non-responders”), patients were dichotomized by whether vasopressors were weaned to off within 72 h or not. A total of 16 (53.3%) patients were responders; baseline characteristics between groups are summarized in Table S1. Responders were overall similar to non-responders but had numerically lower ICU (37 vs 58 days, p = 0.52) and hospital (62 vs 93 days, p = 0.42) lengths of stay and in-hospital mortality (31% vs 64%, p = 0.07). Droxidopa responders had similar SOFA scores as non-responders at the time of droxidopa initiation (8 vs 6, p = 0.72).
Responders were on vasopressors for a similar duration of time prior to droxidopa initiation (16 vs 18 days, p = 0.42) but were on lower norepinephrine equivalents at the time of droxidopa initiation (0.05 vs 0.12 mcg/kg/min, p = 0.013). Non-responders were more likely to start droxidopa at 200 mg every 8 h (29% vs 0%, p = 0.037), while all responders started at 100 mg every 8 h. Responders remained on lower doses; median daily droxidopa dose at the time of vasopressor discontinuation was 300 mg (IQR 300-600 mg) for responders and 1200 mg (IQR 1050-1575 mg) for non-responders (p < 0.001). Use and doses of other adjunctive meds were similar between responders and non-responders, except fewer responders were on fludrocortisone prior to initiation (6.3% vs 42.9%, p = 0.03). Median time from droxidopa initiation to ICU transfer was shorter in responders (8.6 vs 41.7 days, p = 0.046), but this was no longer significant when time to ICU transfer was assessed from vasopressor discontinuation (7.8 vs 15.1 days, p = 0.12), Figure 4.
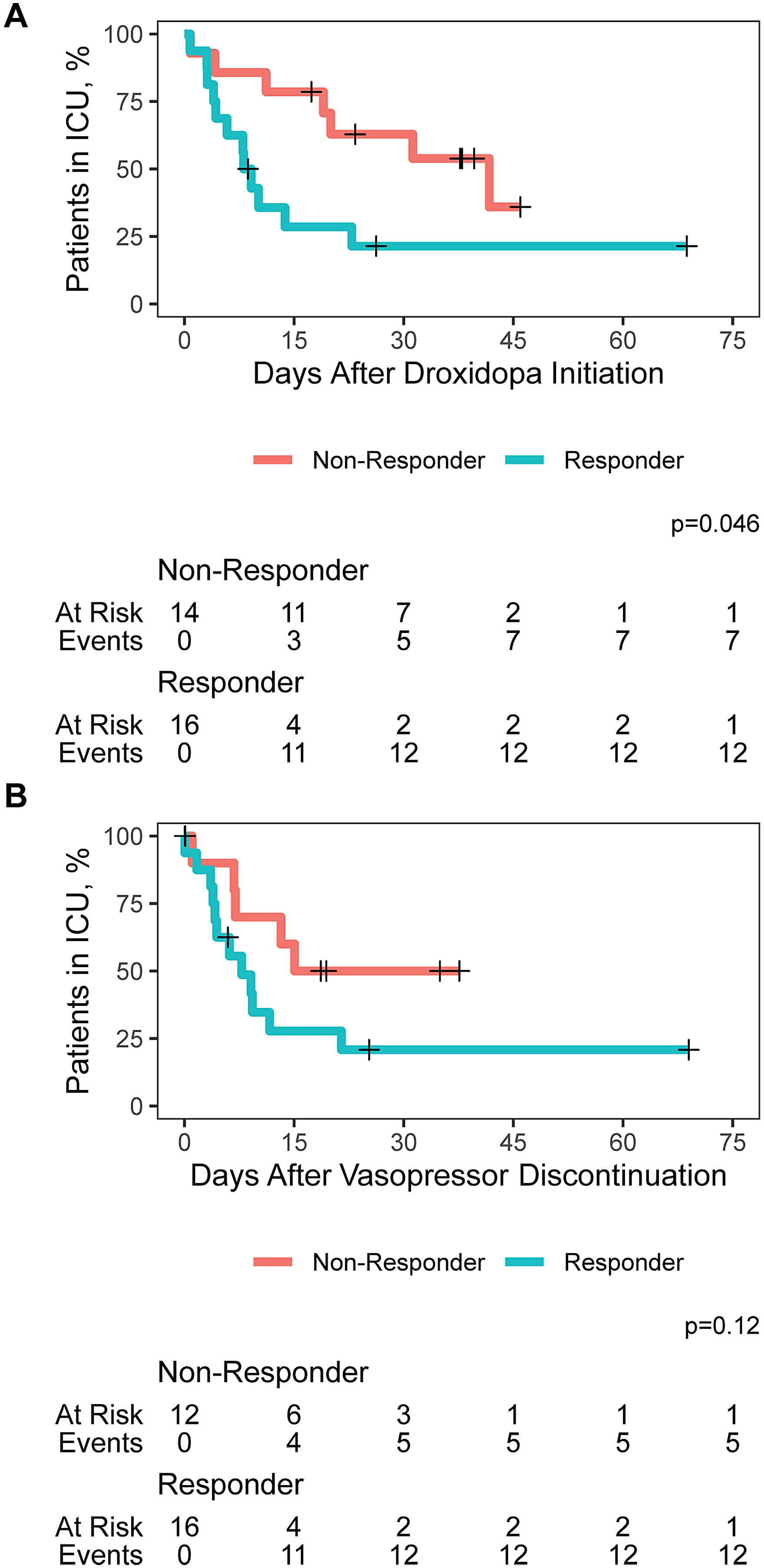
Time to ICU Transfer After Droxidopa Initiation or Vasopressor Discontinuation. Time to ICU transfer, calculated as time from droxidopa initiation (A) and time from vasopressor discontinuation (B) between responders and non-responders. Patients who experienced in-hospital mortality in the ICU or who experienced mortality within 8 h of ICU transfer were censored (crossmark). Median time to ICU transfer was significantly shorter for responders after droxidopa initiation (8.6 vs 41.7 days, p = 0.046) but not from vasopressor discontinuation (7.8 vs 15.1 days, p = 0.12).
Outcomes were similar in patients who received droxidopa via feeding tube. Time to vasopressor discontinuation was 70 h (IQR 31, 175) hours (p = 0.93 vs non-GT administration), mean norepinephrine equivalents were 0.08 mcg/kg/min in the 24 h prior to droxidopa initiation and 0.02 mcg/kg/min in the 24 h after initiation (p < 0.001), and rates of pre- and post-initiation tachycardia (17% vs 22%, p = 0.43) and hypotension (29% vs 19%, p = 0.14) were consistent with those who received the capsule whole. Time to vasopressor discontinuation between patients who received droxidopa via feeding tube versus whole capsule are depicted in Figure S1.
Discussion
In this multicenter, retrospective, single-arm observational study of 30 critically ill patients who experienced persistent hypotension and prolonged need for vasopressors, vasopressors were discontinued within a week of droxidopa initiation in 70.3% of patients and after a median of 70 h overall. Vasopressor discontinuation was successful despite a median time on vasopressors of 16 days prior to initiation and most patients already having failed other adjunct agents including midodrine, fludrocortisone, or pseudoephedrine. The median droxidopa dose at the time of vasopressor discontinuation was 600 mg/day, but some patients did exceed the package label recommended maximum dose of 1800 mg/day and received up to 2400 mg/day at the time of vasopressor discontinuation. 9 In the immediate period after droxidopa initiation, norepinephrine equivalents decreased, MAP increased, and heart rate remained unchanged. Administration via GT did not affect the likelihood of response. This suggests droxidopa may be a viable adjunct option for vasopressor weaning in critically ill patients who are persistently hypotensive requiring vasopressors despite the use of traditional adjunct agents including midodrine, although exact treatment effect cannot be confirmed in the absence of a comparison group.
Vasopressor and Adjunct Agent Use.
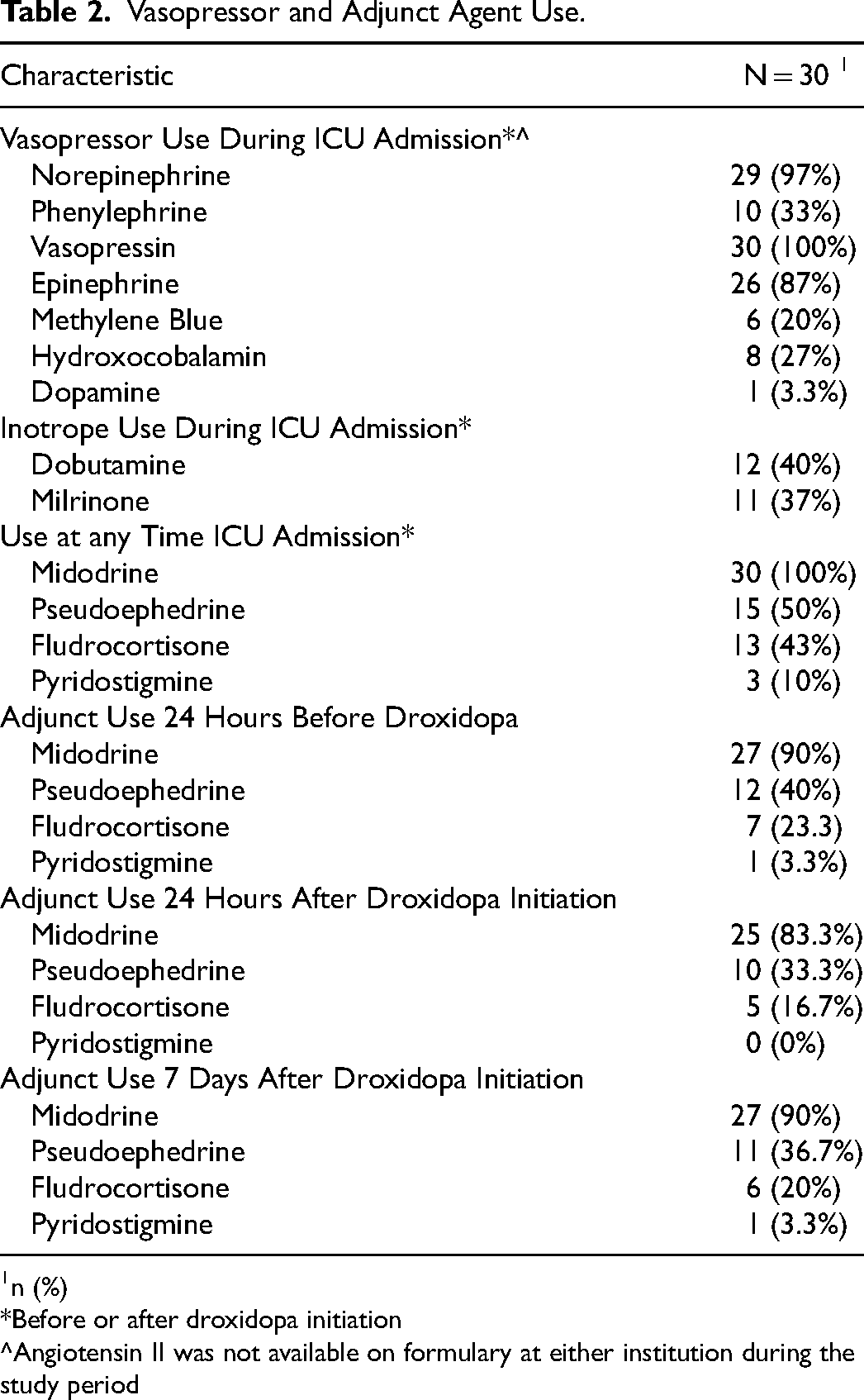
n (%)
Before or after droxidopa initiation
Angiotensin II was not available on formulary at either institution during the study period
Droxidopa is a prodrug of norepinephrine which is converted to norepinephrine by dopamine-beta-hydroxylase both peripherally and centrally.10,11 It was approved for the treatment of nOH after the results of the NOH301 trial revealed that droxidopa, when titrated to individual response, significantly improved both supine blood pressure and quality of life metrics in 162 in patients with nOH. 11 It has durable effectiveness as demonstrated in an open-label extension trial of 114 patients with nOH where no signs of tachyphylaxis or loss of treatment effect were observed over 12 weeks. 12 It has been successfully utilized for patients with nOH secondary to a variety of etiologies including amyloidosis, autoimmune autonomic neuropathy, multiple system atrophy, and pure autonomic failure. Initiation has occurred both outpatient and inpatient; consistent response to droxidopa was observed in a series of 46 patients who underwent droxidopa up titration in the inpatient setting compared to what is expected of outpatient initiation, demonstrating that acutely ill patients may benefit from the therapy as much as outpatients. 5
The consistent dose-response relationship and relatively low rate of adverse effects has sparked interest in the use of droxidopa for weaning vasopressors in patients in the ICU. Midodrine, which is similarly approved for symptomatic OH, has been studied as an oral vasopressor-weaning in two randomized controlled trials – the MIDAS trial and the MAVERIC trial – and a third trial, the LIBERATE trial, is underway.3,4,13 Other adjunctive agents, including fludrocortisone, pyridostigmine, and pseudoephedrine, have also been trialed for this indication after extrapolation from experience in patients with OH.14,15 While adjunctive use of oral vasopressors for intravenous vasopressor weaning has mixed results, they are often trialed in patients with persistent hypotension in the ICU as a means to accelerate liberation from the ICU. Our cohort, who had been continuously on intravenous vasopressors for a median of 16 days prior to droxidopa initiation, is representative of a population where acceleration of vasopressor discontinuation would be particularly beneficial for ICU liberation.
Droxidopa, as a norepinephrine prodrug, may offer distinct advantages over midodrine, a direct alpha1 adrenoreceptor agonist, for this indication. Patients may experience dose-limiting bradycardia from midodrine due to autonomic reflex effects from the unopposed alpha agonism. In the MIDAS trial, bradycardia occurred significantly more often in the patients who were randomized to midodrine versus placebo (7.6% vs 0%, p = 0.02), although this was not seen in the MAVERIC study. Midodrine dosing in each study was fixed and low, however, at 10–20 mg every 8 h, which limits conclusions given dosing should be titrated to individual effect and effective doses may exceed 120 mg/day.16–18 Droxidopa has not been associated with bradycardia and in our cohort, heart rates did not significantly change after initiation (84 vs 86 BPM, p = 0.37), although high use of midodrine may have blunted tachycardia. Droxidopa also has a wider dosing range than midodrine, and our cohort demonstrates that most patients only required one dose up-titration (from 100 mg every 8 h to 200 mg every 8 h prior to vasopressor discontinuation) and few patients required titration beyond the package label recommended maximum dose, while exceeding maximum dose recommendations is standard for midodrine. The median daily dose of midodrine patients in our cohort received prior to initiating droxidopa, 90 mg, exceeds the maximum recommended dose of 30 mg. 19
The role of droxidopa as an adjunct for vasopressor weaning has only been described in one other small cohort and select case reports.20–22 The only retrospective cohort evaluating droxidopa as an adjunct for refractory hypotension described 45 patients with refractory hypotension after cardiac surgery who received droxidopa, atomoxetine, or both for hypotension that was refractory to midodrine and/or intravenous vasopressors. Twenty-seven of the 45 patients received droxidopa, and only 16 of the 27 were on intravenous vasopressors when droxidopa was initiated. Median time to vasopressor discontinuation was 8 days for patients who received droxidopa alone and 13.9 days in patients who received both droxidopa and atomoxetine. 20 This time to vasopressor discontinuation is much longer than the median 70 h in our cohort and may be explained by higher severity of illness, worse underlying cardiac function, or medication underdosing.
Interestingly, in our cohort, if patients did not wean off vasopressors by 72 h, time to discontinuation was significantly delayed, if they were discontinued at all. We characterized patients who discontinued vasopressors within 72 h of droxidopa initiation as “responders” and those who weaned off after 72 h or did not wean successfully as “non-responders.” Median time to discontinuation in responders was 22 h, and responders tended to be on lower doses of norepinephrine equivalents than non-responders (0.05 vs 0.12 mcg/kg/min, p = 0.013). Patients with nOH with elevated plasma norepinephrine concentrations are less likely to respond to droxidopa, so this may explain why droxidopa had little additive effects in patients already on higher doses of norepinephrine. 23 In patients whose blood pressures already require reasonably high doses of norepinephrine, droxidopa is unlikely to provide additive benefit. It may be possible that responders had lower severity of critical illness and may have weaned from vasopressors independent of droxidopa, although responders had similar SOFA scores both at admission and at the time of droxidopa initiation. The observation that higher baseline norepinephrine equivalent requirements led to a shallower slope of time to discontinuation is an important consideration when considering when to initiate droxidopa. Responders were also able to transfer out of the ICU sooner than non-responders, although the difference in time to ICU transfer was not significant after removal of immortal time bias by calculating from the time of vasopressor discontinuation.
We observed that over 30% of patients surviving to discharge continued droxidopa after hospital admission. This is consistent with a cohort of patients started on midodrine for vasopressor weaning, where 311 of 909 (34%) patients started on midodrine in the ICU continued midodrine at hospital discharge. 24 Continuation of ICU-initiated therapies in the outpatient setting is common; this has also been described with antipsychotics 25 and acid-suppressive therapy. 26 While we did not assess duration of outpatient use, this redemonstrates that transitions of care are an important opportunity to ensure that therapies initiated in the ICU are appropriate to continue after admission.
There are several limitations to this study. Given the numerous factors that influence hemodynamics in the ICU, it is not possible to definitively know whether droxidopa, versus another factor, influenced the changing doses and eventual discontinuation of vasopressors. Additionally, the lack of a comparison group limits our ability to make claims about effect and vasopressor discontinuation may have occurred without droxidopa. We were unable to find a sufficient usual care population which appropriately matched the complexity of the baseline characteristics of our population which would allow us to compare treatment effects of droxidopa versus usual care. Retrospective comparative studies of agents used to wean vasopressors are challenging because of the inherent immortal time bias with patients who did not require adjunct agents to wean vasopressors, so this limitation is difficult to overcome. We believe the temporal relationship between droxidopa initiation and decreasing vasopressor doses may suggest a relationship between droxidopa and successful weaning. Because nearly all patients were on additional adjunctive agents, however, it is not possible to disentangle the effects of droxidopa versus another agent on vasopressor doses. Lastly, we did not include acquisition price in our analysis. A barrier to droxidopa has historically been its high cost; average wholesale price for droxidopa can range from $23.33 to $48.73 per 100 mg capsule at the time of writing, translating to an estimated daily cost of $70-$146 at the median dose of 300 mg/day for responders and potentially exceeding $500/day at the dose of 1200 mg/day seen in non-responders. We did not include this in our analysis, however, because contract acquisition costs will vary substantially from institution to institution, making conclusions about cost difficult to translate across centers. Droxidopa is now available off-patent which may improve acquisition costs over time. Lastly, the period of enrollment eligibility was wide, and treatment paradigms in shock may have changed between 2016 and 2024. The majority (20 of 30 patients) were treated after 2022, however, and so the period of enrollment is unlikely to significantly influence the likelihood of droxidopa to influence vasopressor weaning.
Conclusion
Droxidopa added as an adjunct vasoactive agent for vasopressor weaning was associated with successful vasopressor discontinuation within a week of initiation in 70.3% of patients with a median time to discontinuation of 70 h. In patients without adequate response to midodrine or other common adjunctive agents, droxidopa could be considered to assist in vasopressor weaning. Further prospective, randomized studies should evaluate the role of droxidopa in vasopressor weaning in critically ill patients against usual care.
Supplemental Material
sj-docx-1-jic-10.1177_08850666241270089 - Supplemental material for Droxidopa for Vasopressor Weaning in Critically Ill Patients with Persistent Hypotension: A Multicenter, Retrospective, Single-Arm Observational Study
Supplemental material, sj-docx-1-jic-10.1177_08850666241270089 for Droxidopa for Vasopressor Weaning in Critically Ill Patients with Persistent Hypotension: A Multicenter, Retrospective, Single-Arm Observational Study by Andrew J Webb, Gianna LH Casal, Kelly A Newman, Justin R Culshaw, Kalynn A Northam, Edmond J Solomon, Sarah M Beargie, Riley B Johnson, Natasha D Lopez, Bryan D. Hayes and Russel J. Roberts in Journal of Intensive Care Medicine
Footnotes
Conflict of Interest Statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.J. Webb accepts consulting fees from Acasti Pharma, Inc. The remaining authors do not have conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.