
Abstract
Graft versus host disease (GVHD) in acute and chronic forms is a frequent post-transplant complication and seen in 50% of patients in acute and up to 70% cases in chronic GVHD setting. Patients with multiorgan involvement and those who are steroid refractory, frequently present with complications arising from this post-transplant complication. These GVHD patients are frequently managed in the Intensive care unit for treatment of air leaks, effusions, management of hypoxemia due to lung GVHD or infections. Close coordination between hematologists and Pulmonary medicine specialists is critical for timely management of these complications to improve patient outcomes.
Introduction
Allogenic hematopoietic cell transplantation (allo-HCT) is an established form of immunotherapy and is a curative treatment modality for both malignant (ie acute leukemia, aggressive lymphoma) and nonmalignant hematologic disorders (ie bone marrow failure syndromes, metabolic disorders, immunodeficiency syndromes and hemoglobinopathies). 1 In the United States, approximately 8000 allo-HCTs are done annually, and acute myeloid leukemia (AML) is the leading indication for HCT based on the most recent data from the Center for International Blood and Marrow Transplant Registry (CIBMTR; Figure 1). In patients undergoing HCT, the main causes of treatment failure beyond Day +100 are relapse of primary malignancy or non-relapse mortality (NRM) due to opportunistic infections or graft-versus-host disease (GVHD). Patients with lung GVHD and infectious complications resulting in sepsis frequently need ICU care and given underlying comorbid conditions and immunocompromised status, the mortality in this high-risk group remains high. 2 GVHD is a multisystem alloimmune-mediated disorder seen in the post-HCT setting in more than 50% of patients undergoing HCT. This post-HCT complication was previously defined temporally with acute GVHD (aGVHD) developing within the first 100 days, and chronic GVHD (cGVHD) defined as occurring after Day +100 post-HCT. With a better understanding of disease biology, this temporal definition has given way to a newer classification based on presenting clinical symptoms. 3 In aGVHD, patients present with skin (manifested as maculopapular erythematous skin rash), gastrointestinal (with symptoms of nausea, vomiting or diarrhea) or hepatic (elevated bilirubin or transaminitis) involvement, with most patients having multiorgan involvement. Risk factors for developing aGVHD include use of peripheral blood stem cell (PBSC) grafts, HLA disparity, utilization of unrelated donors, myeloablative conditioning regimens, older age of donor or recipient and female donor to male recipient. 3 Chronic GVHD manifests as a multisystem alloimmune disorder with an inflammatory component (oral ulcerations, scleritis, skin rash) or with fibrotic manifestations in the skin (scleroderma), lungs (bronchiolitis obliterans syndrome), or joints (decreased range of movement). Patients oftentimes also present with chronic dry mouth, dry eyes (sicca syndrome), nail dystrophy, dysphagia (due to esophageal stricture), weight loss and failure to thrive due to malabsorption resulting from exocrine pancreatic insufficiency. 3 Patients with cGVHD frequently have multiple organ involvement. Occasionally, patients may have manifestations of both acute and chronic GVHD and are classified as having overlap syndrome. 4 Based on data from the CIBMTR, the incidence of aGVHD is approximately 40–60% with current GVHD prophylaxis regimens comprising of a calcineurin inhibitor (cyclosporine or tacrolimus) and methotrexate. 5 Chronic GVHD is the leading cause of non-relapse mortality (NRM) in patients who are long-term survivors after allo-HCT and is seen in up to 50–70% of transplant survivors.6,7 Recent data suggests that the clinical outcomes (overall survival, NRM and relapse rates) of patients transplanted in a more recent era (2013-2017) are improved compared to an earlier era (2003-2007) due to improvements in donor selection, GVHD prophylaxis/treatments, and advancements in supportive care practices. 8 The prevalence of cGVHD in United States is estimated to be approximately 14,000 cases, of which 40% patients have severe cGVHD and ≥ 4 organ involvement at the time of diagnosis.9,10 The common risk factors associated with the development of cGVHD include the use of unrelated donor transplants, increasing recipient age, HLA disparity, female donor to male recipient, use of myeloablative conditioning and the use of PBSC as the graft source. 11 With improvements in supportive care practices and decline in incidence of relapse and NRM, the population at risk for developing cGVHD is now higher as more patients are long term survivors post HCT. 12 Additionally, older patients are now being considered eligible for allo-HCT due to the adoption of reduced-intensity conditioning regimens (RIC), this trend will result in more cases of cGVHD as older age is considered a risk factor for cGVHD. 13 A recent CIBMTR analysis of 26,563 allo-HCT recipients over three time periods showed that in the most recent era from 2004–2007, the incidence of cGVHD at the 1-year mark was higher compared to earlier years. 14 These trends suggest that there will be a continued increase in the number of patients who are long-term survivors of allo-HCT and require management of late complications including cGVHD. Not only does cGVHD contribute to an increase in mortality, but these patients also have a poor quality of life, psychosocial issues and increased resource utilization resulting in increased healthcare costs.15,16 As the prevalence of long-term survivors post-HCT increases, it is anticipated that more patients with advanced cGVHD will require ICU management mainly for management of respiratory failure or sepsis. 17
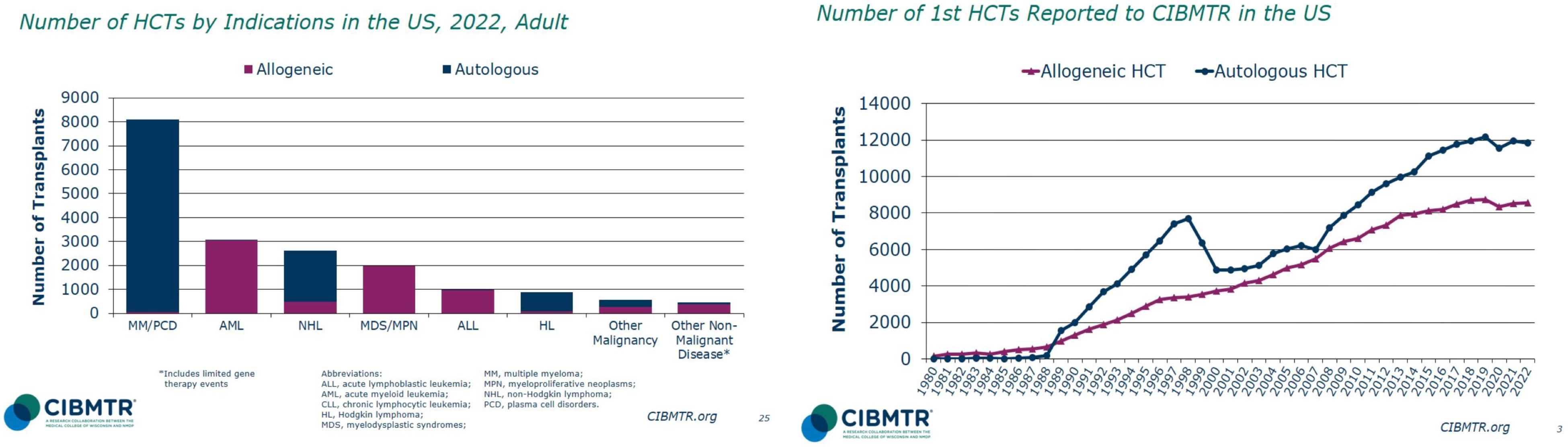
Data from CIBMTR showing indications (left) and trends in utilization of allo-HCT over time.
The pathophysiology of cGVHD can be described as a multisystem fibro-inflammatory disorder, which involves epithelial tissues and the lymphohematopoietic system. 18 Previously, cGVHD was classified as limited or extensive based on the severity and number of organs involved. 19 The development of NIH consensus criteria in 2005 (updated in 2014) has streamlined the classification of cGVHD using a grading system to assess patient symptom presentation and a response criterion to evaluate progress on long-term follow-up.20,21 In the NIH grading system, eight organs (skin, eyes, gastrointestinal tract, mouth, genital tract, lungs, liver, joints fascia) are scored for severity of GVHD manifestations based on the classification of mild to moderate or severe cGVHD symptoms, which is predictive of overall survival. 22 The NIH classification allows comparison of patient outcomes across multiple centers and guides management and response assessment of patients on treatment. 3 Most patients with cGVHD can be managed as outpatient with a combination of corticosteroids and novel second-line agents, but certain manifestations of GVHD require patients to be cared for in a more acute setting with escalation of care to the intensive care unit (ICU). Such conditions include: i) respiratory failure arising from severe lung GVHD requiring noninvasive or invasive ventilation ii) severe GI aGVHD causing hypotension due to GI bleed or electrolyte abnormalities and dehydration from fluid losses iii) atypical pulmonary infections (viral, bacterial or fungal) caused by prolonged exposure to immunosuppressive therapy causing respiratory distress and requiring diagnostic procedures as bronchoscopy and microbiologic evaluation of lavage fluid iv) air leak arising from severe BOS requiring placement of chest tubes and oxygen therapy. 17 In this review, we will cover ICU management of common complications arising from GVHD post allo-HCT focusing mainly on the pulmonary system.
Pathophysiology of GVHD
Our understanding regarding the biology of acute and chronic GVHD is derived mainly from mismatched mouse transplantation models that provides insights into the development and evaluation of GVHD and provides a model for testing new therapeutic agents before clinical use. 18 These murine models show that the development of GVHD in recipient mice can be divided into three distinct phases. The early phase involves the activation of donor CD4 T-cells upon contact with antigen presenting cells (APCs: dendritic cells, monocytes, macrophages, and B cells). The donor T-cell activation by host antigens presented by APCs is initiated by tissue damage by conditioning regimen that releases damage associated molecular patterns (DAMPS: ATP, uric acid, IL-33) and pathogen associated molecular patterns (PAMPs: bacteria, viruses, fungi). 23 Epithelial damage from the conditioning regimen releases soluble inflammatory mediators (ATP, uric acid, interleukin-33, and Lipopolysaccharide) that activates APC to present host antigens to donor T-cells. 24 Endothelial damage due to intimal arteritis leads to reduced microvascular density, which predisposes to subsequent fibrotic manifestations of cGVHD. In the second (inflammatory) phase of cGVHD, alloreactive B- and T-cells primed by APCs proliferate and expand towards Type-1 (Th-1), Type-2 (Th-2), and Type-17 (Th-17) helper T-cells.25,26 The inflammatory milieu is maintained by secretions of proinflammatory cytokines by CD4 positive T-cells which have previously escaped immune regulation. In the lymphoid follicles, these T-helper cells produce interleukin-21 leading to formation of germinal centers and expansion of B-cell clones. 27 Damage to the thymic epithelium from conditioning regimen and the reactive T-cells results in loss of regulatory T/B cells causing loss of peripheral tolerance. 28 In the final phase of GVHD, there is activation of fibroblasts by platelet-derived growth factor alpha and transforming growth factor beta secreted by macrophages resulting in production of collagen in the extracellular matrix resulting in sclerosis. 29 Unregulated immunoglobulin production by B-cells driven by B-cell activating factor results and pathogenic immunoglobulin deposition in organs contribute to organ damage and fibrosis.
Prevention of GVHD:
All patients undergoing HCT require GVHD prophylaxis prior to infusion of stem cell graft to prevent GVHD. The combination of calcineurin inhibitors (CNI) and methotrexate (MTX) 45 mg/m2 is the current standard in patients undergoing allo-HCT in both reduced-intensity (RIC) or myeloablative (MAC) conditioning. 30 The incidence of aGVHD and cGVHD remains high with this prophylactic regimen (∼40-60%), and MTX use is associated with an increased incidence of mucositis (occasionally requiring intubation for airway protection) and delayed neutrophil engraftment. Hence, attempts have been made to add novel agents such as mycophenolate mofetil (MMF) or sirolimus in combination with CNI to improve clinical outcomes.31,32 At our center, tacrolimus and sirolimus-based prophylaxis (T/S) is standard in both the RIC and MAC setting based on the promising results seen in Phase 2 studies with good disease control long term.33,34 However, cGVHD rates remain high and attempts have been made to improve the composite outcome of 1-year GRFS (GVHD and relapse-free survival) with newer strategies. 35 Promising newer strategies to reduce cGVHD incidence include incorporation of post-transplant cyclophosphamide, antilymphocyte globulin, CTLA-4 antagonists, use of bone marrow graft, and ex-vivo graft engineering.35–40 Novel GVHD prophylaxis strategies currently in clinical trials may influence natural history and lower the incidence of cGVHD in the future.
Treatment of GVHD
Corticosteroids remain the therapy of choice in both aGVHD and cGVHD.41,42 In milder forms (Grade 1-2) of aGVHD, topical steroids may be used to successfully manage aGVHD. However, for more severe forms (Grade 3-4) of aGVHD, systemic corticosteroids such as methylprednisolone 1–2 mg/kg/day is recommended. 43 Patients who respond to frontline corticosteroids within 1–2 weeks typically have a good prognosis and, in many cases, steroids may gradually be tapered off after adequate clinical response is achieved. Serum biomarkers have been developed that are predictive of NRM and allows for better risk stratification, and patient counseling. 44 Clinical grading based on site and extent of organ involvement can also be used to classify patients as high versus low risk. Novel trials are in development that offer immunotherapy combination to high-risk patients. 45 Ruxolitinib, a JAK-STAT inhibitor, has been used successfully to control symptoms in patients who are deemed steroid-refractory. In a large randomized phase 3 study, ruxolitinib was associated with superior overall response rates (ORR 49% vs 25%) compared to best available therapy (BAT) resulting in its FDA approval in this setting. 46
Corticosteroids (prednisone 1 mg/kg/day or equivalent dose of alternative steroids) are also recommended as frontline therapy for patients with a new diagnosis of moderate to severe cGVHD. 42 Patients with cGVHD are graded based on severity of organ involvement (score 0-3) in the NIH consensus criteria. 21 Approximately, half of patients will respond to upfront therapy with steroids, but those who remain steroid-refractory (SR) or steroid-dependent (SD) require second and/or third-line therapies. Currently, there are three FDA approved drugs in this setting that inhibit alloreactive T-cells by inhibiting JAK-STAT (ruxolitinib), ROCK-2 (belumosudil) or BTK/ITK (ibrutinib) pathways with ORR of 60–75%.47–49
Complications of GVHD Requiring ICU Care:
Pulmonary cGVHD/BOS is a distinct form of cGVHD which is seen in less than 10% of patients undergoing allo-HCT, and is associated with disproportionately large mortality in HCT patients. 50 The 5-year OS is now improved to 40% in BOS patients due to improved understanding of its pathophysiology, availability of newer treatment options, and more awareness of screening pulmonary function tests (PFTs) which may allow for earlier diagnosis of BOS and intervention. 51 BOS primarily results from immune cell-mediated damage to the small bronchioles leading to fibrotic occlusion and airway obstruction. 52
Diagnosis of BOS: This requires the following physiologic and radiographic criteria: i) New onset obstructive airway defect defined as an FEV1 < 75% of predicted ii) FEV1:FVC ratio of < 0.70; or below 90% confidence iii) absence of infection; iv) evidence of airtrapping identified by an inspiratory/expiratory noted on high resolution CT scan or pulmonary function testing.residual volume (RV) > 120% or RV/total lung capacity exceeding the 90% confidence interval.21,53 Newer guidelines do not require the presence of air trapping at diagnosis, as this is a late finding and lung biopsy is rarely required for diagnosis as non-invasive testing with PFTs, CT-imaging in an approproate clinical setting is sufficient to make a diagnosis of BOS.50,53 Patients with extrapulmonary restriction due to scleroderma, myopathy (GVHD-induced or steroid myopathy), or polyneuritis may present with extrapulmonary restriction and occasionally make it difficult to distinguish from BOS. 54 Serial PFTs and the measurement of maximum inspiratory pressures (MIP) and expiratory pressure may help with the diagnosis of respiratory muscle weakness arising from muscle weakness (myositis, steroid-induced myopathy) or neuropathy. PFTs in patients with BOS shows a progressive decline in FEV1, FEV1/FVC ratio on spirometry and flattening of expiratory limb of flow volume loop (Figure 2). 55
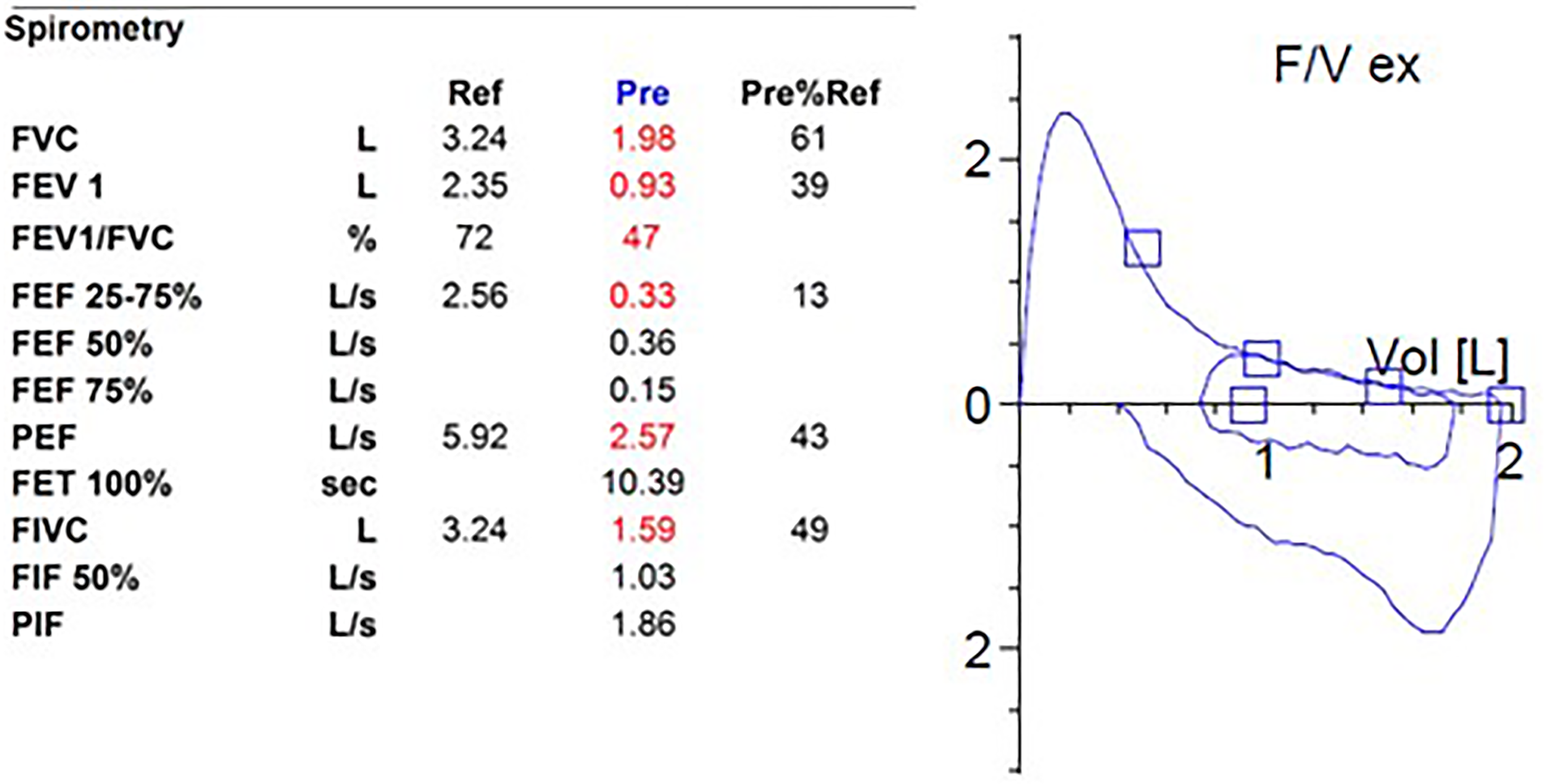
Pulmonary function testing showing reduction in FEV1 and FEV1/FVC rations in patients with BOS.
Differential diagnosis: Conditions that can present with progressive dyspnea post-HCT should be ruled out, which include: opportunistic lung infections, cryptogenic organizing pneumonia (COP), radiation fibrosis, idiopathic pneumonia syndrome (IPS) and exacerbation of underlying asthma or chronic obstructive pulmonary disease (COPD). Decline in FEV1 is seen in asthma, but this is reversible with bronchodilators, in contrast to BOS, wherein the decline in FEV1 is fixed. Patients with COP respond very well to the initiation of systemic corticosteroids, in contrast to BOS, where clinical responses are slow. 53 IPS is a pulmonary complication that can develop in up to 10% of patients in the first four months after allo-HCT. Diagnosis requires evidence of alveolar injury as noted by multifocal opacities on CT chest, hypoxemia manifested by increased alveolar arterial gradient or need for supplemental oxygen and absence of documented lower respiratory tract infection is negative bronchoscopy/BAL. Treatment is by using immunosupression with high-dose steroids and etanercept. 56 COPD also presents with a decline in FEV1, but patients typically have this condition prior to transplant. Prior to the diagnosis of BOS, pulmonary infections need to be ruled out using imaging and invasive tests such as bronchoscopy. Patients with clincial diagnosis of BOS should have serial PFTs from previous evaluations documenting slope of decline in FEV1. During acute decompensation and ICU transfer, PFTs have limited applicability and patients are too sick to perfom these tests and the findings may be altered by added conditions such as congestive heart failure (CHF), infection, and etc.
Natural History and phenotypes in BOS: Pathological review of surgical lung biopsy specimens obtained from patients with BOS reveals obliterative bronchiolitis and fibrosis resulting in luminal narrowing and obliteration. 52 Risk factors for the development of BOS include : busulfun-based conditioning, ABO-mismatch HCT, peripheral stem cell transplant, unrelated donor transplant, respiratory viral infections, older age at transplant, and poor baseline lung function. 52 Patients with BOS may exhibit distinct clinical courses, including those with a slow decline in lung function versus those with a rapid decline in FEV1, defined as those who develop BOS within six months of HCT or demonstrate a decline in FEV1 of 25% within three months of BOS diagnosis. 52 Cheng et al described the natural history of lung function decline in 36 patients in the FAM cohort (fluticasone, azithromycin, montelukast) versus 46 patients who developed BOS post-HCT, but were not treated with FAM. 57 In both cohorts, the overall trajectory of FEV1 showed consistent decline in the preceding six months prior to BOS diagnosis, which continued post-diagnosis as well. Additional PFT parameters, such as FVC and FEF25–75, also declined in BOS patients. Poor survival was associated with diagnosis of BOS within 1-year post-HCT, FEV1 < 44% or FVC <67% and use of myeloablative regimens for HCT. Similar findings were reported in a larger subset of 1461 patients who underwent HCT at an academic center, of which 95 patients (6%) eventually developed BOS. 58 In this study, patients with a rapid initial 25% decline in FEV1 within the first three months after diagnosis of BOS had significantly worse lung function and poorer OS compared to patients with a more gradual initial decline in lung function.
Another form of lung dysfunction called chronic lung allograft dysfunction (CLAD) is seen frequently (30%) after lung transplantation. 59 Two distinct CLAD phenotypes are described, which include obliterative bronchiolitis (OB) and restrictive allograft syndrome (RAS or rCLAD). 60 Similar to the clincial syndrome of BOS noted post-allo-HCT, OB is characterized by an obstructive pattern on PFTs and air trapping on CT scan. RAS/rCLAD is manifested by restrictive pattern on PFTs, pleuroparenchymal pulmonary infiltrates on CT scan and fibroelastosis on lung biopsy. Patients with RAS/rCLAD have a worse prognosis with median OS of 6–18 months compared to 3–5 months after diagnosis of OB. Presence of bronchiectasis in patients with OB/BOS is associated with adverse clinical outcomes due to more infectious complications and airway colonization with Pseudomonas aeruginosa in patients with bronchiectasis. 56 Similar association of bronchiectasis and poor OS in BOS post-HCT is lacking, but it is possible that post- allo-HCT development of bronchiectasis may be associated with gram-negative bacilli and atypical mycobacterial colonization in allo-HCT recepients. 57 Recognizing CLAD is important in patients who receive solid organ HCT pre- or post-allo-HCT.61,62
Prevention and Treatment: A large randomized prospective study was conducted in 465 HCT patients to evaluate azithromycin prophylaxis in preventing BOS post-HCT by assigning patients to receive either azithromycin 250 mg 3 times a week or placebo for two years at the initiation of the conditioning regimen (ALLOZITHRO Trial) which was based on a prior successful Phase 2 study. 63 Unfortunately, this trial was negative and in fact was associated with increased mortality in patients randomized to the azithromycin group. Thus, the approach of azithromycin prophylaxis is currently not recommended in post-allo-HCT setting. 64
Treatment of patients who are diagnosed with BOS post-HCT requires initiation of systemic immunosuppression with systemic and inhaled medications . A Phase 2 open-label study showed that patients with BOS treated with the FAM (
When admitted to the ICU due to respiratory complications, patients with pulmonary GVHD/BOS invariably require augmented respiratory support due to poor baseline reserve . Studies have demonstrated that 15% of patients who undergo alloHCT and develop acute respiratory distress syndrome (ARDS) with or without BOS, have a high mortality rate of 50–70%.72,73 A recent report reviewed the outcomes of 70 patients who needed ICU care post allo-HCT patients, the most comon cause for ICU transfer post HCT was sepsis (50%) followed by respiratory failure(20%) and neurologic symptoms (20%) and half of the patients required mechanical ventilator support. The 30 day mortality of allo-HCT patients admitted to ICU was 48% and 1 year OS 16%, indicating that few patients survive long term in this setting. 74 Etilogy of respiratory failure is infectious pneumonia in majority of cases which could be secondary to bacterial, viral or fungal pathogens . Non infectious causes of respiratory failure include engraftment syndrome (11%), IPS (7.5%), diffuse alvelolar hemorrhage(4%), BOS (8%) and COP 2%. 75 Prior to requiring mechanical ventilation, many patients in the ICU setting are provided with supplemental respiratory and oxygenation support via high flow oxygen or non-invasive postive pressure ventilation (NIPPV). Historically, early initiated NIPPV was thought to be associated with decreased rates of progression to needing invasive mechanical ventilation and improved survival. 76 Newer data is inconclusive on the benefit of NIPPV, results demonstrating possibe increased mortality. 77 Due to the difficulty in delivering uniformly controlled tidal volumes with NIPPV and generation of high-delivered tidal volumes by the patient, there is a higher rate of NIPPV failure. 78 It is hypothesized that high-delivered tidal volumes leads to lung injury and potentiates respiratory failure. Moreover, recent studies indicate an increased role of high-flow nasal oxygen. NIPPV has not been demonstrated to have survival benefit over high-flow nasal oxygen in immunocompromised patients, including those who were HCT recipients.78,79
HCT patients, particulary those with pulmonary GVHD, who progress to needing invasive mechanical ventilation have high mortality.72,80 Ventilator strategies for these patients mirror those of non-HCT patients, with particular emphasis placed on preventing ventilator-induced lung injury. In patients with severe pulmonary GVHD, a volume-limited mode of ventilation is favored given the presence of airflow limitation. Ventilator settings and mode selection should be tailored to each patient's unique clinical situation, but general goals of low tidal volume for lung protection, avoidance of over oxygenation, and appropriate use of positive end-expiratory pressure depending on the underlying etiology of the patient's respiratory failure should be prioritized.
Pediatric studies have shown poor outcomes for patients admitted to the ICU for acute respiratory failure post-HCT due to the multiple etiologies (BOS, DAH, engraftment syndrome, COP) and requiring mechanical ventilation. Survival in these patients is poor with high mortality rates ranging from 24–40%. 81 Multivariate analysis showed that the requirment of renal replacement therapy, CMV viremia, and severe hypoxemia is associated with increased ICU mortality in pediatric patients with pulmonary complications. Studies looking at the outcomes of patients with post-HCT BOS in adults are lacking, however, outcomes of patients who are transferred to the ICU in the peri-transplant period shows similar high 90-day mortality of approximately 50% in single-center studies. 74 In these settings, it may be appropriate to have a discussion with patient and family regarding palliation and symptom control rather than mechanical ventilation given the poor data regarding long-term survival in intubated patients. A frank and compassionate discussion with family member(s) regarding prognosis and expectations for successful extubation and rehabilitation needs to be done at the time of transfer to the ICU. A discussion between the patient and care providers ahead of time and having an advanced directive ready before any clinical deterioration occurs may help prevent instituting care that may be eventually futile. Tools are now availabe to help guide such discussions with critically ill patients in the ICU. 82
Diagnosis of Lower Respiratory Tract Infections in Patients with cGVHD
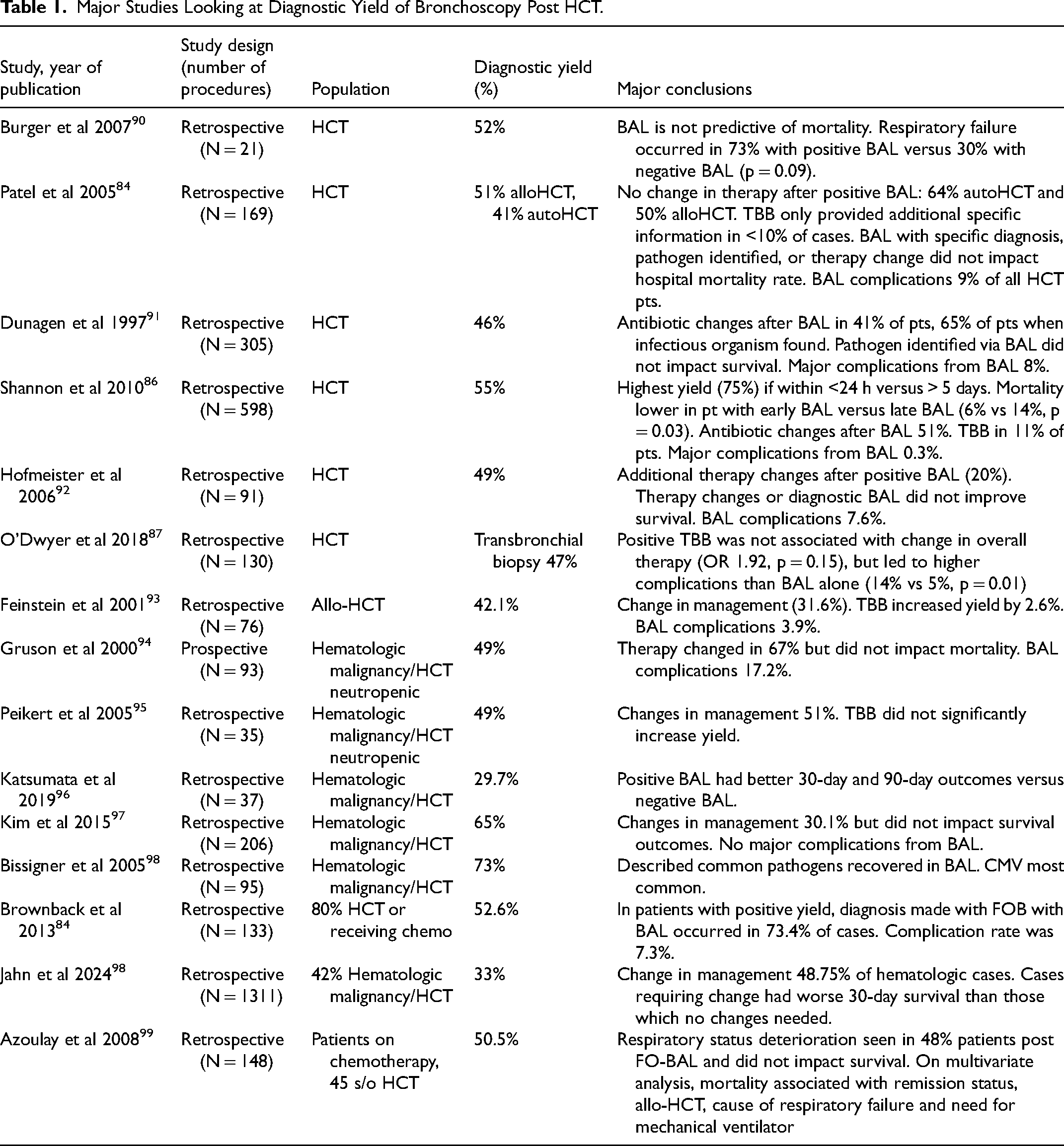
The predominant cause of respriatory failure in patients with cGHVD requiring ICU admission is infection. Pulmonary infection has a considerable effect on mortality in alloHCT recipients. A prospective study investigating the epidemiology, etiology, and outcome of pneumonia in all alloHCT recipients (with and without cGVHD) demonstrated that the 1-year probability of survival was 82.7% without the presence of pneumonia and decreased to 47.4% among those who had at least one episode of pneumonia. 83 Bronchosopic evaluation for the cause of respiratory infection remains an investigative mainstay. However, there is a wide discrepancy in the published diagnostic yield of a bronchoalveolar lavage (BAL) ranging on average from 30–65% (Table 1). BAL yields a diagnosis in half of the cases when done in alloHCT recipients and adding transbronchial biopsy adds to additional information in < 10% cases, thus for most patients, a bronchioloalveolar lavage (BAL) may be sufficient for microbiologic diagnosis. 84 Diagnostic yield has been correlated with specific morphology of the pulmonary lesions seen on radiographic studies. Consolidative infiltrates and tree-in-bud infiltrates (see Figure 3) have higher associated BAL diagnostic yield when compared to reticular or nodular infiltrates. 85 Early BAL performed within four days of presenation of respiratory symptoms was associated with a 2.5-fold higher yield than those performed after four days of presentation. Moreover, diagnostic yield was 75% when performed within 24 h of clinical presentation. 86 We recommed testing for i) respiratory virus pathogens using commercially available rapid screening tests (eg BioFireRP2.1 PCR), which tests for common respiratory pathogens such as adenovirus, coronaviruses, SARS-CoV-2, human metapneumovirus, human rhinovirus/enterovirus, influenza A and B, parainfluenza viruses (1, 2, 3, and 4), respiratory syncytial virus, bordetella pertussis, bordetella parapertussis, chlamydophila pneumoniae, and mycoplasma pneumoniae ii) culture, gram stain, and cytology iii) HSV, CMV PCR, pneumocysticis jiroveci qPCR and DFA and MTB PCR iv) fungal pathogens including mucor PCR and aspergillus galactomannan antigen testing. Additional tests may be added to BAL fluid based on geographic location or specific exposures in consultation with infectious disease specialists. The addition of a traditional transbronchial biopsy (TBB) has not been associated with an improved diagnostic yield for infectious processes, but has demonstrated a role in identifying non-infectious pulmonary complications and impacting the initiation of corticosteroid therapy.87,88 TBB also carries an increased procedural risk due to the potential of pneumothorax and the possibility of bleeding in this thrombocytopenic patient population. In the ICU setting, BAL had a diagnostic yield of 27% and resulted in management change in only 38% of patients who were immuncompromised, with a majority of the patients possessing an underlying hematologic malignancy or were post-HCT. Bronchoscopic intervention was also associated with worsening respiratory status in 11% of patients and associated with higher ICU and in-hospital mortality with rates approaching 50%. 89 Therefore, the pursuit of brochoscopy in ICU patients should be a considered decision with emphasis on identifying if and how it will impact treatment and management decisions.

Consolidative peripheral opacities seen in HCT patient, these tend to have higher yield from BAL.
Major Studies Looking at Diagnostic Yield of Bronchoscopy Post HCT.
In order to increase the diagnostic accuracy of bronchoscopy and BAL, cell free DNA analysis is currently being evaluated like the Karius test. 100 In a study of 257 patients, where standard testing was unable to make a microbial diagnosis in patients with pneumonia who underwent diagnostic bronchoscopy and BAL evaluation, the use of the Karius test increased the probability of microbial diagnosis by another 20%. More widespread adoption of DNA-based testing such as universal PCR may also increase diagnostic yield in patients where current tests are unable to determine etiology of infections. 101
Recently, there has been advancement in the fields of bronchoscopy and interventional pulmonology with the introduction of robotic assisted bronchoscopy. These robotic systems allow for increased precison and targeting of peripheral pulmonary lesions and promote stability during biopsy. 102 Currently, there are three FDA-approved robotic bronchoscpy systems. Primarily developed for peripheral biopsy of lesions suscpicious for solid organ malignancy, the advantages offered by robotic assisted bronchoscopy can be extrapolated to the HCT population in the diagnostic work-up of pulmonary lesions suspicious for infectious or inflammatory etiology. Biopsies performed with increased proximity to the target lesion can be hypothesized to have increased diagnostic yield when compared to traditional TBB. Morever, intraoperative confirmation of the biopsy tool being close to the lesion can be obtained with augmented fluoroscopy or Cone-Beam CT. In addition, BAL can be performed via robotic-assisted bronchoscopy allowing sampling from an optimized, locoregional position in close vicinity to the target lesion. It is theorized that this improved positioning could lead to an increased diagnostic yield. It is important to note that currently no retrospective or prospective studies have been performed investigating the use of robotic-assisted bronchoscopy in the HCT patient population for idenftification of infectious or inflammatory etiologies of pulmonary lesions. Likewise, there have been no studies to date studying whether robotic-assisted bronchoscpy is associated with increased diagnostic yield or therapeutic benefit when compared to traditional bronchoscopy with BAL and/or TBB. There are currently no guidelines regarding which point in a patient's work-up for pulmonary lesions robotic-assisted bronchoscopy should be used. It is also important to take into consideration bleeding risk and pneumothorax risk in the HCT population, given an increased incidence of thrombocytopenia and potentially lower pulmonary reserve, particularly in patients with pulmonary GVHD.
A rare complication of late pulmonary cGVHD is spontaneous thoracic air leakage syndrome, which is the presence of extra-alveolar air including spontaneous pneumothorax, pneumomediastinum, pneumopericardium, and subcuteanous/interstitial emphysema. 103 The reported incidence of spontaneous thoracic air leakage syndrome is only 0.83%-2.3%. 104 Though these occurrences are likely secondary to archictecural distortion of the lung parenchyma, pleura and airways; they may also be secondary to the violation of these anatomical structures by invasive infectious organisms. Pneumothorax as result of cGVHD falls under the classifcation of spontaneous secondary pneumothorax (SSP) which is a pneumothorax due to underlying lung disease. SSP is associated with more challenging management and increased morbidity and mortality. 105 Air leak is unlikely to spontaneously resolve in patients with SSP and the symptoms related to pneumothorax are greater in this patient population due to their underlying lung disease. Patients with pulmonary GVHD should have their pneumothoraces managed according to standard guidelines established for all SSPs.
Initial management of a patient with SSP depends on their clinical symptoms and the radiographic size of the pneumothorax.105,106 Small bore chest tube placement is advised, particulary in the setting of clinical symptoms and pneumothorax size >2 cm. 105 Smaller pneumothoraces, in the absence of clinical symptoms, can be monitored in the hospital setting with oxygen treatment, or if symptoms are present, can be considered for needle aspiration versus chest tube placement.105,106 Those patients with increased respiratory compromise being considered for mechanical ventilation may benefit from larger size chest tube placement due to the concern for large airway leak due to positive airway pressure. 106 Figure 4 displays a patient presenting with a pneumothorax with improvement after the placement of a chest tube.
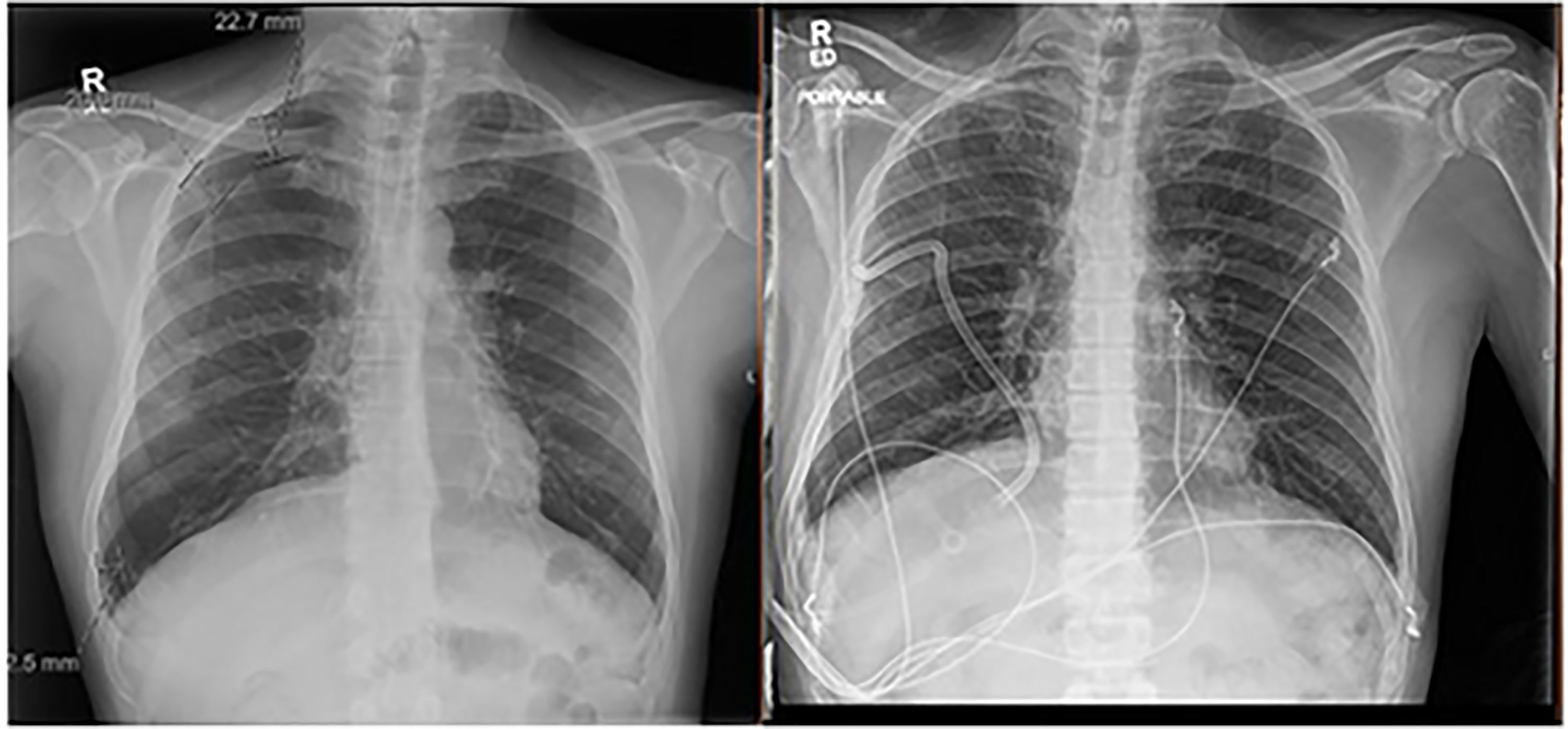
Patient with lung GVHD presenting with dyspnea and Chest X ray showed right sided pneumothorax (left panel) that improved with placement pf chest tube and re-expansion of underlying lung (right panel).
Patients with SSP with a persistent air leak or inadequate lung re-expansion despite chest tube intervention should be considered for additional treatment including medical or surgical chemical pleurodesis or video assisted thoracoscopic surgery (VATS) with pleurectomy and pleural abrasion.105,106 However, given these patients’ underlying respiratory insufficiency, they are occasionally not candidates for invasive interventions. Other techniques to treat persistent air leaks include autologous blood patch pleurodesis, sealants, and spigots/coils have been described. 107 Moreover, in the past few years, increasingly minimally invasive techniques to address persistent air leaks have been developed, including the use of bronchial valves. 108 These valves are placed bronchoscopically, and allow for unidirectional airflow preventing air entry during inspiration, but allowing expiratory airflow. 109 A large reterospective single-center study published their results on the efficacy of bronchial valves, with over 68% of patients having SSPs, demonstrated successful closure of persistent air leaks with chest tube removal in 80% of patients. 108 Other smaller retrospective studies have demonstrated resolution of persistent air leaks in almost 90% of patients. 107 Prospective studies are currently underway to further clarify use of bronchial valves in the treatment of persistent air leaks. There is currently no published experience of the use of bronchial valves in patients with pulmonary GVHD, but given their success in other causes of SSPs, they should be considered as a treatment strategy in patients with pulmonary GVHD with pneumothorax complicated by persistent air leaks. The majority of studies looking at the implications of endbronchial valve placement are related to bronchoscopic lung volume reduction. In several studies, a low infection risk has been identified and ranges from 1.7–3%. Though an immuncomprised patient with pulmonary GVHD is at higher risk of developing a pulmonary infection, the placement of broncial valves is temporary. The benefit of resolving a patient's persistent air leak despite other more conservative methods needs to be considered, especially if leading to prolonged ICU stay. In the presence of existing pulmonary infection, the placement of bronchial valves should be avoided.
Another cause of significant respiratory morbidity in patients with pulmonary GVHD is the development of pleural and pericardial effusions. Depending on the size and laterality of the pleural effusions, they can cause significant respiratory failure leading to ICU admission. In a recent reterospective study in patients who had undergone HCT, 9.9% of patients developed a pleural effusion where prior studies have described an incidence of pleural effusion as high as 16%. 110 Etiology of pleural effusion in HCT varies, and also depends on duration of time that has elapsed since undergoing HCT. Though volume overload and infection are predominant causes of pleural effusions throughout a patient's transplant course, the presence of pleural effusion due to GVHD and malignancy increases 100 days status post-HCT. 111 Pleural effusion secondary to cGVHD is related to pleural involvement with serositis. The majority of these patients usually have significant cGVHD, often with multiorgan involvement, prior to the development of a pleural effusion. Figure 5 illustrates a patient with cGVHD presenting with a signficiant pleural effusion. Often, the onset of pleural effusion coincides with development of a pericardial effusion and ascites as well. 111
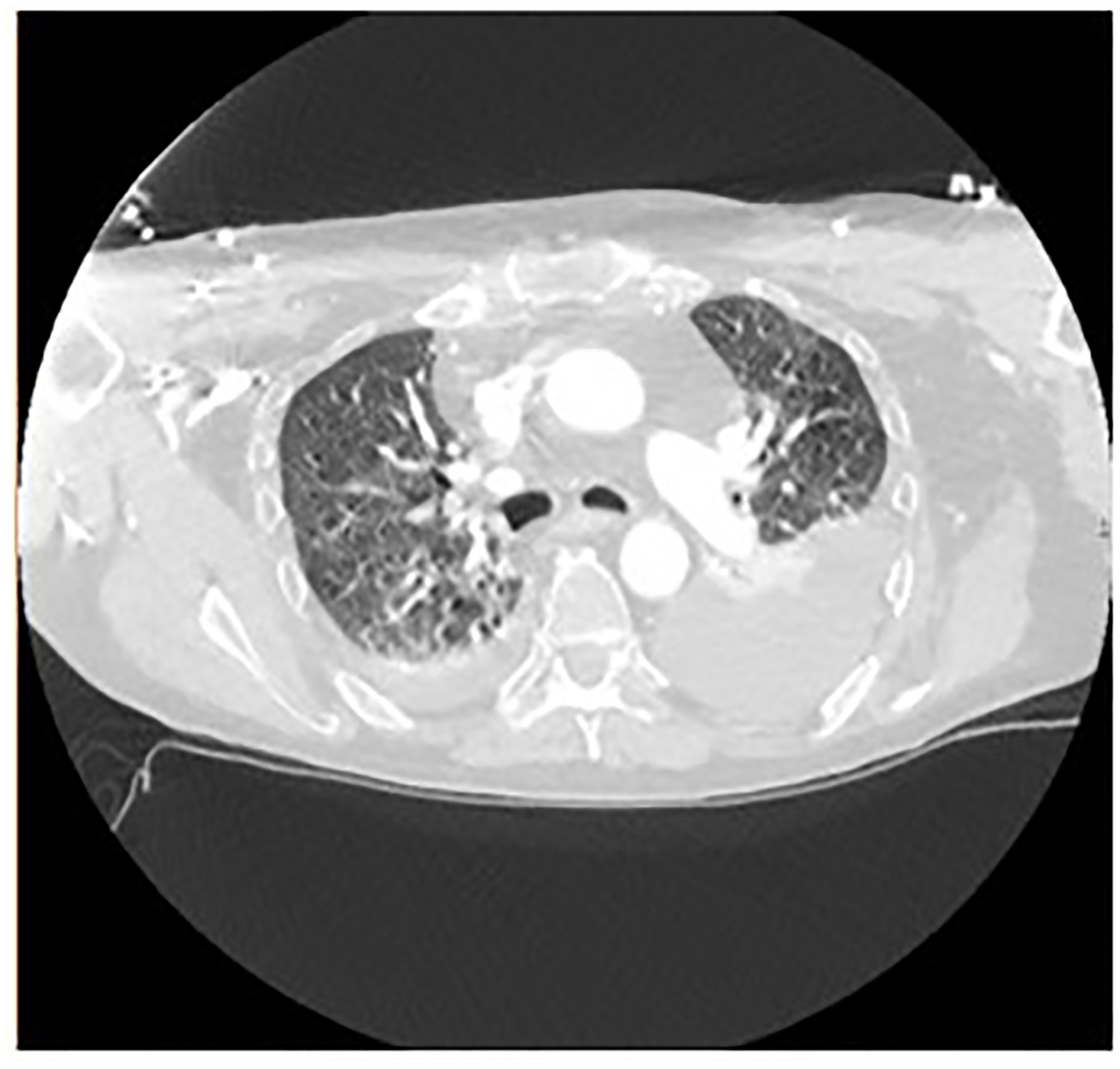
Patient with cGVHD presenting with moderately large left pleural effusion.
To determine the etiology and provide symptomatic relief, a thoracentesis should be promptly performed when safe to do so after managing any presenting thrombocytopenia or coagulopathy. Determination of whether the pleural fluid is a transudate or exudate should be made, most often by Light's criteria. 112 Further pleural fluid analysis should also include cell count and differential, microbiology cultures and cytology. Other correlating laboratory and radiographic studies should also be performed based on the patient's clinical scenario and suspected cause of pleural effusion to help clarify an etiology. Depending on the etiology and re-accumulation rate, placement of an indwelling pleural catheter(s) can be considered. Though not well described in the literature, medical or surgical thoracoscopy can be considered for diagnostic purposes if a thoracentesis does not yield a diagnosis. Similarly, pleurodesis could also be considered in select cases for refractory pleural effusion.
Similar to pleural effusions, pericardial effusions are a rare, but potentially life-threatening complication of HCT. Patients identified with pericardial effusion usually require prompt ICU management, especially in the setting of cardiac tamponade physiology. GVHD can lead to pericardial serositis in HCT patients, with a recent reterospective review by Azoulay et al describing the incidence to be 3.1% in the HCT population. 113 Depending on the patient's hemodynamic stabilty and the presence of cardiac tamponade, prompt treatment with pericardiocentesis or pericardial window should be undertaken. Often, when a percardiocetensis is performed, a pericardial drain is placed to help prevent re-accumulation. When the pericardial effusion is suspected to be secondary to cGVHD, immunosuppressive treatment should also be started. 113
Conclusion
Graft-versus-host disease remains a very common problem post allo-HCT. Approximately 40% patients develop acute and 50–70% of the patients will develop cGVHD post allo-HCT. Patients who fail frontline treatment with corticosteroids present with multiorgan involvement and require many lines of treatment for disease control. Corticosteroids still remain the first line therapy for both aGVHD and cGVHD. Patients failing corticosteroids can now consider recent FDA approved therapies available for the management of cGVHD. Availability of approved therapies and the improvement in supportive care practices has improved overall survival and quality of life in patients with cGVHD post-HCT. Patient with GVHD frequently require co-management with pulmonary medicine for i) diagnosis of lower respiratory tract infections ii) management of lung GVHD/BOS iii) management of complications arising from cGVHD including respiratory failure(due to infections,IPS,DAH, septic shock) and need for mechanical ventilation, management of air leaks and pleuropericardial effusions. Timely referral to the appropriate specialists is crucial in the symptom management and overall improvement in survival outcomes for GVHD in ICU patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.