
Abstract
The prone position is often used for patients with adult respiratory distress syndrome and specific surgical postures. When performing venous cannulation in this position, it is important to have a structured review to introduce the available major veins and ultrasound-guided procedure. In this review, we discuss the techniques of ultrasound-guided cannulation and provide insights into various aspects, including the anatomical locations of veins, vein sizes, placement techniques, surrounding structures at risk, and reported experiences with catheter placements. Eight major veins can be accessed in the prone position: the internal jugular vein, external jugular vein, brachiocephalic vein, basilic vein, mid-thigh femoral vein, popliteal vein, posterior tibial vein, and small saphenous vein. To minimize the risk of venous thromboembolism, the ratio of catheter diameter to vessel diameter should be less than 0.67. The review also presents the minimal requirement of venous diameter for different catheters in a tabulated form. For larger veins, real-time ultrasound guidance with the long-axis view/in-plane technique is suggested, while for smaller vessels, the short-axis view/out-of-plane technique is recommended. The review includes sonographic illustrations of the two techniques and surrounding arteries and nerves for the eight major veins. The aim of this review is to help clinicians assess the eight major veins and safely insert various types of catheters for patients in the prone position.
Keywords
Introduction
The prone positioning technique has important applications in critical care and surgical procedures. First, a prone position (PP) can improve oxygenation by reducing ventilation–perfusion mismatch. 1 PP has demonstrated positive impacts on patients requiring mechanical ventilator support for managing acute respiratory distress syndrome (ARDS). 2 PP could reduce the mortality risk of patients with moderate-to-severe ARDS, 3 and a prolonged PP duration of more than 24 h may be required to extend the benefits.4,5 Second, placing patients in the PP during anesthesia is crucial to facilitate operative access for various surgical procedures. 6 Therefore, the establishment of venous access in the PP becomes a critical issue. There are a limited number of single case reports or case series present in the current literature. To the best of our knowledge, few articles have presented a structured discussion of venous catheterization in the PP. In this article, we aim to review and summarize the accessible veins, their anatomy, sonographic guidance techniques, relevant structures to be aware of, and experiences with venous catheter placements in the PP.
Real-Time Ultrasound Guidance
Using real-time ultrasound guidance for the insertion of venous catheters not only improves the success rates but also reduces the risk of complications, especially in cases where conventional methods, such as the anatomical landmark technique, pose challenges for insertion. The application of ultrasound guidance is effective in decreasing the occurrence of complications during catheter placement, including arterial puncture, hematoma formation, and hemothorax.7–13 Given the anatomical inversion in the PP and the occasional need to access deep veins, real-time ultrasound guidance is recommended for placing venous catheters.
Steps of Ultrasound-Guided Placement of a Venous Catheter
Selection of the Ultrasound Probe
The choice of an appropriate probe is crucial for successful placement. For this exploration, a linear, high-frequency probe is selected. In this context, higher frequencies enhance resolution, but they come with a trade-off, as they can lead to a reduction in the tissue penetration depth.14–16
Choosing an Appropriate Vein
Before selecting a vein, the surrounding structures such as arteries and nerves should be verified, and thrombosis should be ruled out. Distinguishing between arteries and veins can be accomplished by gently compressing the blood vessels, observing the vessel direction and pulsatility using the color Doppler mode, and differentiating them based on the wave pattern in the pulse wave Doppler mode.17–19 After choosing the vein, attention must be paid to its size, as reducing blood flow can potentially induce venous stasis. The catheter size in relation to the vein is particularly impactful, especially in peripherally inserted central catheters (PICCs). 20 An optimal cutoff point with high sensitivity and specificity to minimize the risk of venous thromboembolism was identified at a cross-sectional area of the catheter-to-vein ratio of 45%.21–24 Using the formula for the area of a circle, the ratio of catheter diameter to vessel diameter should be less than 0.67, which is calculated as follows: Area = r² × π (“r” is the radius). R² × π × 0.45 > r² × π, 0.45 > (r/R)², 0.67 > r/R (r: catheter radius, R: blood vessel radius) (Table 1).25,26
Comparison of Catheter Size with the Smallest Feasible Blood Vessel Diameter.
Real-Time Ultrasound Guidance
Reverberation Artifacts
Reverberation artifacts can obscure the needle dimensions and sometimes significantly distort the entire image. Understanding and accurately interpreting these artifacts are essential for safe medical practice. Identifying the needle, especially the needle tip, during ultrasound-guided interventions is crucial. Ensuring the precise location of the needle tip is essential for safe and successful venous catheter placement. 27 The details in Figure 1 include hazardous structures around the blood vessel, symptoms of accidental injury, and sonographic illustrations.
This figure describes the structures around the blood vessel that require attention and their relative positions in the prone position (the green dot corresponds to the direction of the ultrasound probe in the other figures).
In-Plane Technique
The two basic methods for vascular access are as follows: the in-plane and out-of-plane techniques; each has its own advantages and limitations.28–32 With long-axis view showing the longitudinal image of the vessel, the in-plane technique involves keeping the entire needle shaft and the complete course of the target vessel visible on the ultrasound screen throughout the procedure. Sustained visualization of the needle is crucial during in-plane puncture, particularly when the primary risk is penetrating the vein's posterior wall. However, challenges arise when dealing with small vessels, making it difficult to consistently maintain the position of the probe along the optimal plane.17,18
Out-of-Plane Technique
Conversely, an out-of-plane puncture may be preferable when dealing with small target vessels or when the vital structures are closely situated to the target vessel.14,33–36 In out-of-plane puncture with a cross-sectional image of the vessel (short-axis view), research comparing the effectiveness of the dynamic needle tip positioning (DNTP) technique with that of the angle-distance (AD) technique is limited. No significant variations were noted in the first-pass success rate, whether or not posterior wall puncture of the vessel was involved, or in the overall success rate within the first 10 min between the DNTP and AD groups. However, it was observed that the cannulation time was longer and the incidence of posterior wall puncture was lower in the DNTP group. 37
Introduction to the Individual Veins
Internal Jugular Vein
Anatomy
The internal jugular vein (IJV) descends within the carotid sheath and joins the subclavian vein behind the clavicle's sternal end, creating the brachiocephalic vein. In addition, a communication between the IJV and external jugular vein (EJV) may be present. The thoracic duct opens near the junction of the left subclavian and IJVs. 38
Tips for Vascular Access
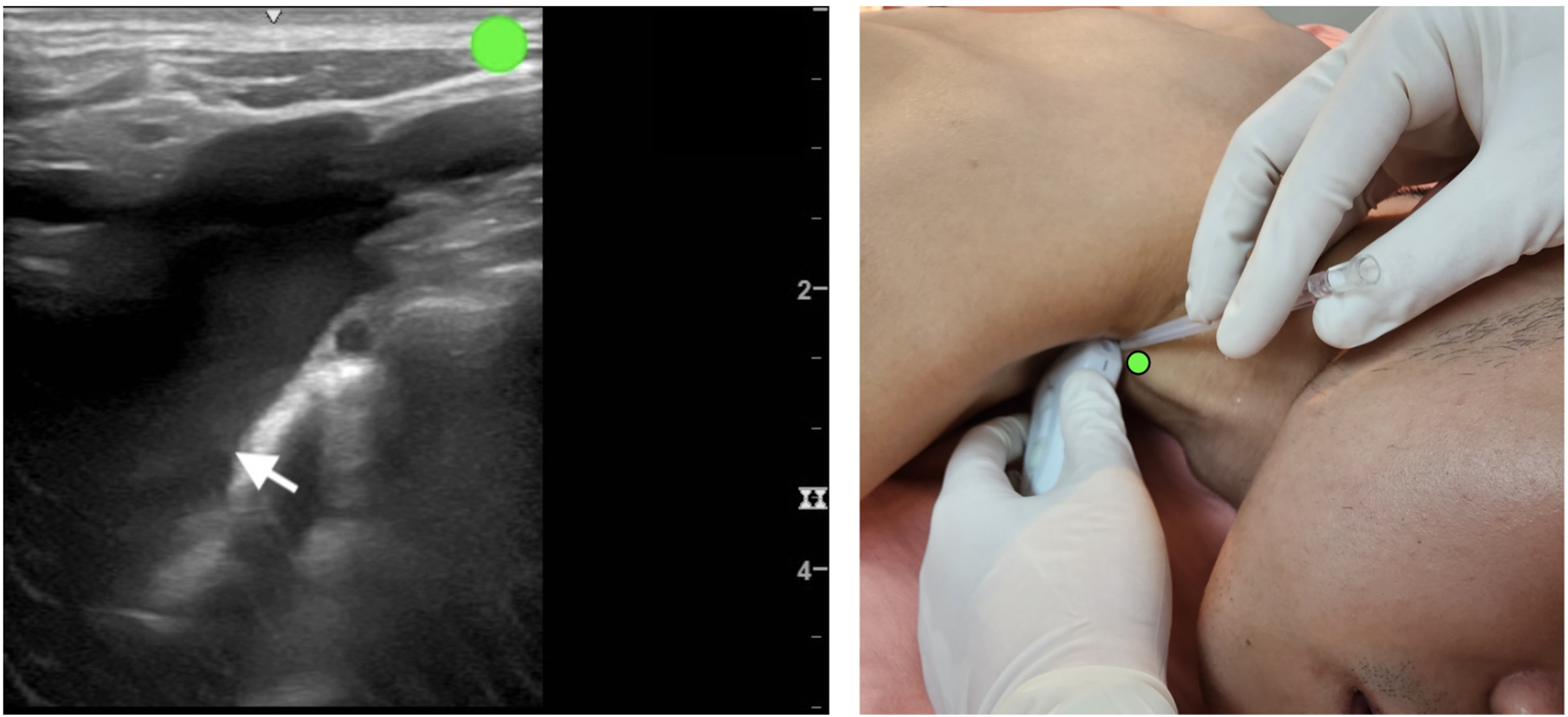
The preferred positioning method involves a slight elevation of the trunk with a pillow, neck extension, application of traction over the ipsilateral shoulder using an adhesive tape, and tilting the bed to a 15° Trendelenburg position. 39 The probe is positioned perpendicular to the posterior margin of the sternocleidomastoid, and the IJV is identified on the basis of its medial location. 40 It is important to note that in the PP, the phrenic nerve and brachial plexus follow the needle insertion pathway.41,42 A previous study comparing the positioning of the IJV in the supine position and PP indicated that, in the supine position, the IJV is lateral to the carotid artery, requiring needle entry from the anterior wall. However, in PP, the IJV is more superficially situated to the carotid artery, necessitating needle entry from the lateral wall, thereby posing an increased risk of arterial puncture. 43 Therefore, ultrasound examination is essential to identify the position of the needle tip and avoid unnecessary damage, especially after the needle has entered the blood vessel, to carefully avoid piercing through the posterior wall of the vessel and causing nerve injury (Figure 2).
The ultrasound probe is positioned in the out-of-plane short-axis (upper image) and in-plane long-axis (lower image) views and placed on the mid-right neck area in the prone position. The white and black arrows indicate the internal jugular vein and internal carotid artery, respectively. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
The diameter of the right IJV was 17 ± 5 mm (mean ± standard deviation [SD]), whereas those of the left IJV was 14 ± 5 mm (mean ± SD) in 190 outpatient adults. 44 This site represents the most easily approachable major vein. Therefore, during dialysis catheter placement in a PP, choosing to prioritize placement at this site is an option.
Previous Reported Clinical Experience
For Emergent Conditions
The adoption of PP during surgery due to procedural requirements has been mentioned multiple times. In cases of sudden massive bleeding, performing an urgent central venous catheterization (CVC) on the IJV in the PP, accompanied by substantial fluid infusion, is feasible.43,45 Although there is no literature comparing the time required for IJV cannulation between the supine position and PP, based on the author's personal experience, the speed of CVC placement in the PP with ultrasound guidance does not show a significant extension as compared with the supine position. In 2023, data obtained from three patients with coronavirus disease 2019 (COVID-19) and ARDS who were placed in the PP because of low oxygen levels showed that one patient even had a peri-arrest period. Nevertheless, despite these challenges, CVC placement was successfully performed in the PP. 39
For the Dialysis Catheter
In Salik et al's study, CT scans obtained from 30 patients revealed that the placement of a dialysis catheter in the left IJV results in the following two additional sharp angulations compared with the placement on the right side: an average of 117° between the left internal jugular and brachiocephalic veins, an average of 116° between the left brachiocephalic vein and superior vena cava, and an average of 106° as the left brachiocephalic vein traverses the aorta and left brachiocephalic artery. Therefore, the hemodialysis catheter passing through these angles may be more prone to contact with the vascular wall, causing endothelial irritation. 46 A previous study revealed that COVID-19 patients with ARDS placed in the PP had a right-sided dialysis catheter inserted to facilitate continuous renal replacement therapy, which remained in use for 5 days. 47 In 2023, a report documented 33 ARDS patients undergoing IJV insertion in the PP; of these, 32 patients received a dialysis catheter and four patients received a CVC. Two patients developed pneumothorax, with no instances of arterial puncture. Given that the entry point is more cranial than the supine central approach, a longer pathway is required, typically around 20 and 24 cm for the right and left sides, respectively. 40 Due to the angle, the right internal jugular vein is often a better choice. In our clinical experience, we have also found that inserting a dialysis catheter in the PP often results in smoother blood flow on the right side during hemodialysis. It is important to note that in the PP, the patient's left and right sides are opposite to those of the practitioner. Therefore, it is essential to confirm the difference between the ultrasound probe's orientation and the actual direction before proceeding with the procedure.
External Jugular Vein
Anatomy
The structure descends obliquely from the mandibular angle to the midclavicle, traversing superficially over the sternocleidomastoid and reaching the root of the neck. At this point, it crosses the deep fascia and terminates in the subclavian vein, positioned laterally or anteriorly to the anterior scalene muscle. It is enveloped by the platysma, superficial fascia, and skin, with the deep cervical fascia separating it from the sternocleidomastoid. 38
Tips for Successful Vascular Access
Placing the patient in the Trendelenburg position enhances the cross-sectional area of the veins. 48 Due to the shallow position of the vein, if the vein is visible to the naked eye, ultrasound guidance may not be necessary for placement. If ultrasound guidance is required, we recommend that the probe should be in very light contact with the skin, and the needle should be kept as flat as possible to avoid piercing the posterior wall of the vessel and causing a hematoma (Figure 3).
The ultrasound probe is positioned in the out-of-plane short-axis (upper image) and in-plane long-axis (lower image) views and placed on the mid-right neck area in the prone position. The white arrow indicates the external jugular vein. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
A previous study evaluating 61 septic adult patients in intensive care units using an ultrasound device revealed that the average diameter of the external jugular vein is within the range of 0.25 ± 0.05 cm (mean ± SD). 49 This site commonly allows for the insertion of a large-bore intravenous catheter and facilitates CVC placement into the central vein.
Previous Clinical Experience
The central venous catheter can be inserted along the EJV into the IJV. A previous study collected data from 563 patients placed in the supine position, of whom 411 successfully underwent catheter placement into the central vein using the EJV route. No life-threatening complications were reported in this cohort. 50 Another study reported that during anesthesia in the PP, EJV cannulation with ultrasound guidance can be accomplished very quickly. 51
Brachiocephalic Vein
Anatomy
The subclavian vein traverses over the first rib, entering the root of the neck. Typically, the subclavian vein converges with the IJV posterior to the sternoclavicular joint, forming the brachiocephalic vein. The right brachiocephalic vein descends nearly vertically to the sternal end of the first costal cartilage, where it merges with the left brachiocephalic vein, giving rise to the superior vena cava. 46
Tips for Successful Vascular Access
A linear probe was positioned in the supraclavicular fossa, parallel to the medial end of the clavicle, while the patient was in the PP. 52 Careful attention to aseptic techniques is crucial in this scenario. Numerous structures in this area require consideration. Ultrasound is not effective in detecting the thoracic catheters, but special attention must still be paid to the potential risk of thoracic duct injury leading to lymphorrhagia, particularly when accessing the left brachiocephalic vein junction. 53 Care should be taken to prevent pleural puncture, as it can result in pneumothorax or hemothorax. Pleural puncture is recognized as a significant complication of brachiocephalic vein catheterization. 54 The phrenic nerve traverses the thoracic cavity behind the subclavian vein, and injury to this nerve can affect the patient's respiratory function. 55 The vagus nerve is situated posteromedially to the venous angle, where the left subclavian vein joins the left IJV 56 Figure 4). We recommend using the in-plane technique for accessing this vessel because it allows for better placement of the ultrasound probe and makes it easier to visualize the surrounding structures.
The ultrasound probe is positioned in the in-plane long-axis view and placed on the lower-right neck area in the prone position. The white arrow indicates the brachiocephalic vein. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
The mean cross-sectional diameter of the left peripheral brachiocephalic vein is 11 ± 5.2 mm (mean ± SD) in 30 adult patients suspected of having pulmonary embolism. 46 Owing to its large vein diameter, it is suitable for the placement of various catheters.
Previous Reported Clinical Experience
In 2023, Kumar and Amarjeet highlighted that, even in the prone surgical position with hypotension, CVC rescue can be performed through the brachiocephalic vein. 52 These authors have also frequently administered CVC in emergencies and found it to be a straightforward and expedient insertion site.
Basilic Vein
Anatomy
The basilic vein originates medially within the dorsal venous network of the hand. It travels posteromedially in the forearm, angling forward to the anterior surface below the elbow, where it penetrates the deep fascia and merges with the median cubital vein. The basilic vein then ascends superficially between the biceps and pronator teres, ultimately forming the axillary vein at the lower border of the teres major. 38
Tips for Successful Vascular Access
Placing a basilic vein PICC in the PP is feasible and using the short-axis-out-of-plane approach at a 45° angle enhances the smoothness of the placement process. 57 However, the median, ulnar, medial brachial cutaneous, and medial antebrachial cutaneous nerves are close to the basilic vein in the arm's proximal part, so caution is required to prevent nerve injury58–60 (Figure 5).
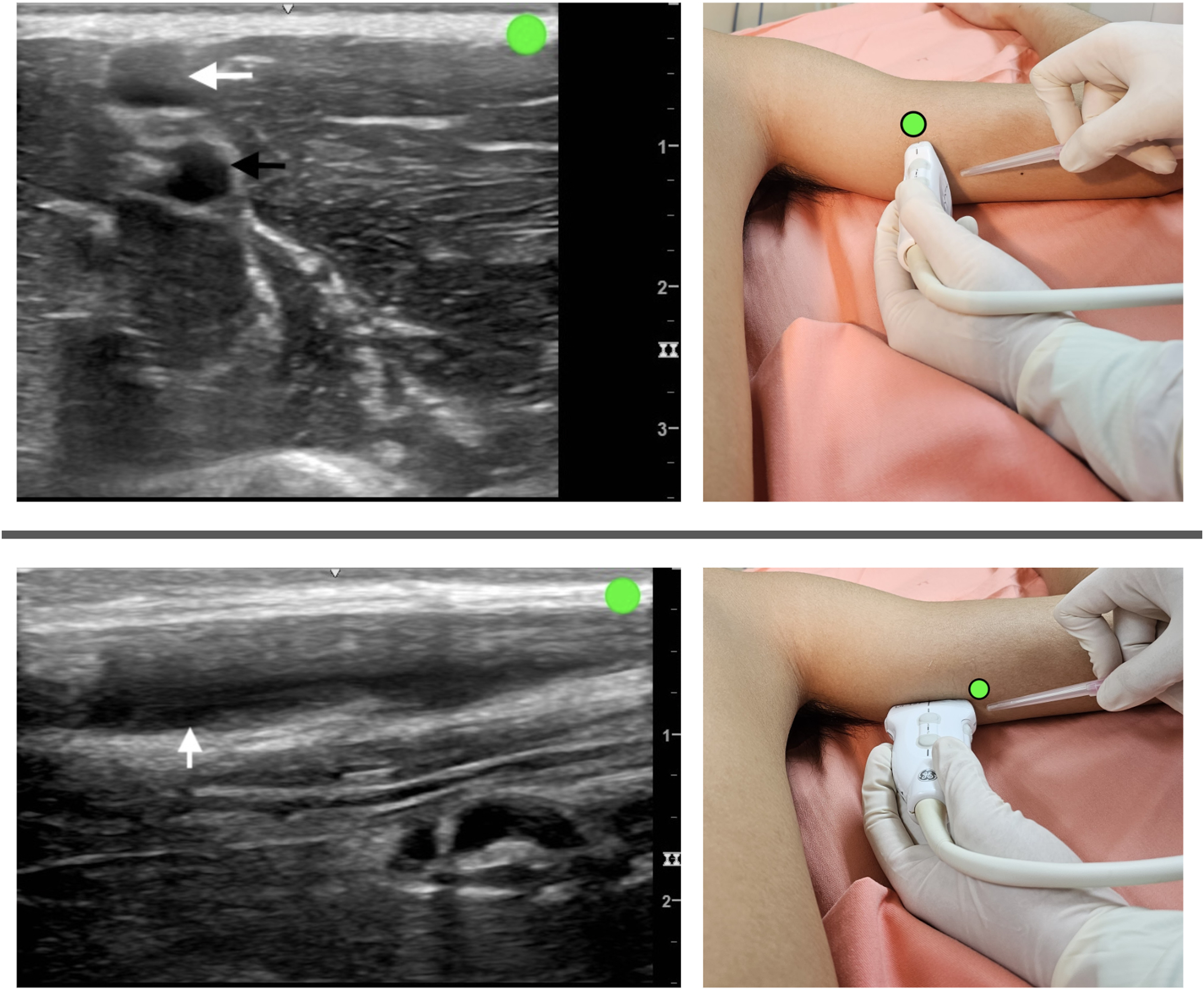
The ultrasound probe is positioned in the out-of-plane short-axis (upper image) and in-plane long-axis (lower image) views and placed on the right arm in the prone position. The white arrow indicates the basilic vein, and the black arrow indicates the brachial artery. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
In 50 cadavers, it was found that the diameters of the basilic vein in the right and left upper limbs are 3.32 ± 0.1 mm and 3.32 ± 0.09 mm (mean ± SD), respectively. 61 Owing to the size of the basilic vein, it can be used for large-bore intravenous catheters, midline catheters, and PICC placements.
Previous Reported Clinical Experience
In a report in 2023, for PP in patients with ARDS, IJV is unavailable due to the presence of an extracorporeal membrane oxygenation cannula. As an alternative, the basilic vein PICC was ultimately chosen as the route for administering inotropic agents. 62 Due to the shallow position and ease of access of the vein in this area, establishing a large-bore intravenous catheter for fluid administration here is a quick and safe option.
Mid-Thigh Femoral Vein
Anatomy
The femoral vein travels alongside its corresponding artery, starting at the adductor opening as a continuation of the popliteal vein and concluding behind the inguinal ligament as the external iliac vein. In the distal adductor canal, the vein is situated posterolateral to the femoral artery. Moving more proximally within the canal and into the distal femoral triangle, the vein is positioned posterior to the artery. Finally, at the base of the triangle, the vein is located medial to the artery. 38
Tips for Successful Vascular Access
As the femoral vein, femoral artery, and saphenous nerve advance toward the distal end of the thigh, they gradually come together to create the adductor canal. The adductor canal's proximal end is near the mid-thigh. Hence, special care is needed when inserting a venous catheter into the femoral vein below the mid-thigh because the nerves and arteries are more concentrated at this point. 63 At the inguinal ligament, the femoral vein is situated medially to the femoral artery. As one progresses toward the distal end, the femoral vein transitions to the posterior side of the femoral artery 64 (Figure 6). Precisely because of the anatomical position, we believe that placing an intravenous catheter in the mid-thigh femoral vein is easier in the PP compared to the supine position.
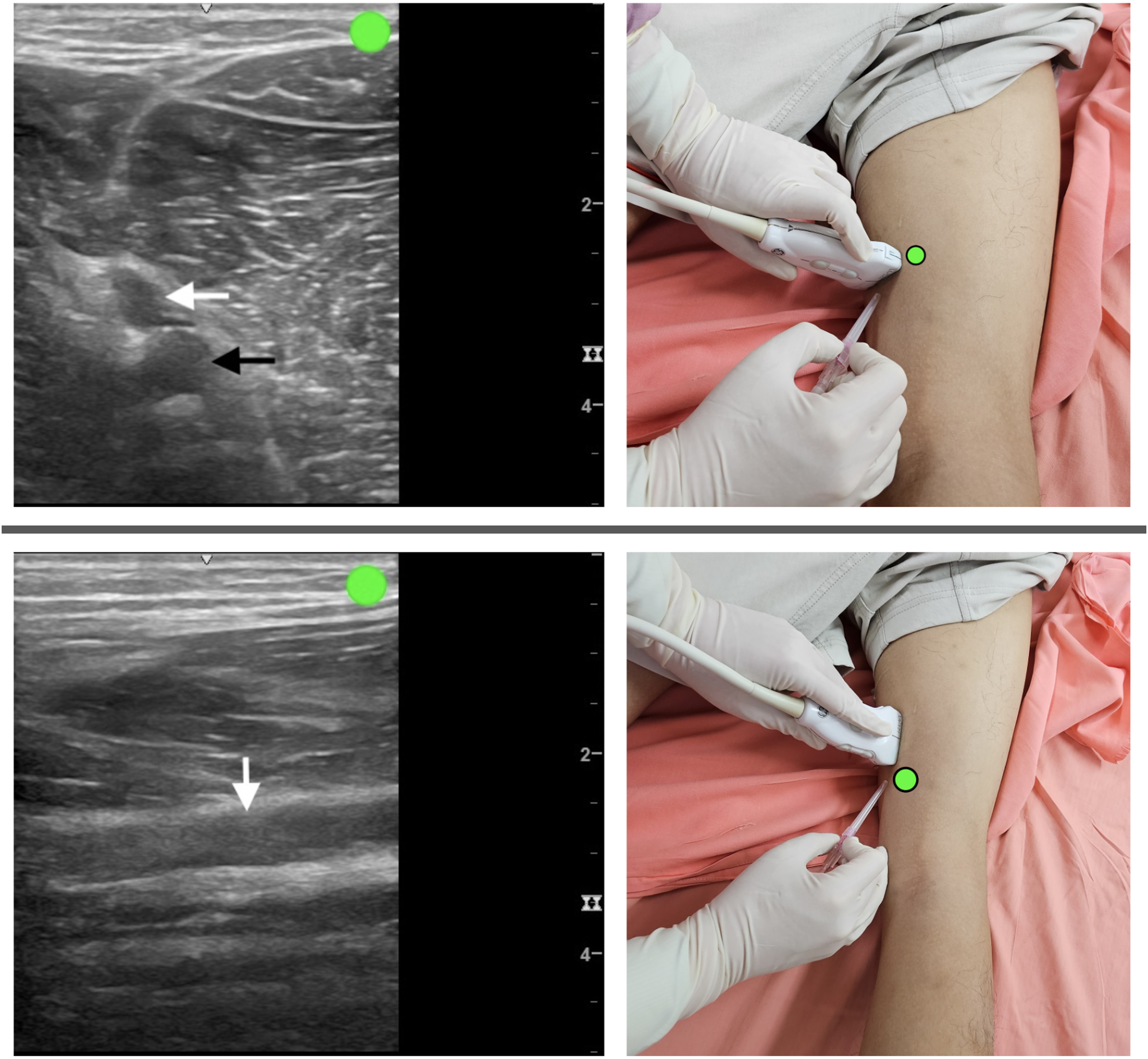
The ultrasound probe is positioned in the out-of-plane short-axis view (upper image) and in-plane long-axis view (lower image) and placed on the right mid-thigh in the prone position. The white arrow indicates the femoral vein, and the black arrow indicates the femoral artery. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
In 82 healthy adult Caucasians, the distal section of the femoral vein, approximately 20 cm distal to the orifice of the deep femoral vein, has a diameter of 8.6 ± 1.8 mm (mean ± SD). 65 Although there are few cases of intravenous catheter placements at this location, due to the larger diameter, this site can be considered for the placement of a dialysis catheter, CVC, midline catheter, or PICC.
Previous Reported Clinical Experience
In 2022, Ostroff et al described a patient with severe COVID-19-related ARDS placed in the PP. Owing to extensive systemic edema, a 55-cm long PICC was inserted into the femoral vein at the upper mid-thigh. The probe was positioned on the thigh's inner side, approximately 6 cm deep, and placement was performed using a short-axis out-of-plane approach. 66
Popliteal Vein
Anatomy
The popliteal vein ascends through the popliteal fossa, reaching the opening in the adductor magnus, where it transforms into the femoral vein. 38
Tips for Successful Vascular Access
For the relative positioning of the popliteal vein and popliteal artery, starting from the femorotibial joint space and moving toward the proximal end, the vein tends to shift posteriorly and laterally to the artery. However, in the femorotibial joint space, the artery often lies in front (deep) of the vein, with an overlap of approximately 75%–100%. Therefore, it is crucial to use ultrasound guidance to carefully confirm the needle position and prevent inadvertent arterial puncture. 67 The shape of the sciatic nerve in the popliteal fossa can be round, triangular, or elliptical, and it appears as a hyperechoic structure. 68 The sciatic nerve bifurcates into the tibial and common peroneal nerves within the popliteal fossa. The popliteal artery is situated anterior to the popliteal vein and anteromedial to the tibial nerve. The common peroneal nerve courses more laterally in the popliteal fossa. 69 During injection, extra caution is required because the nerves are superficial to the veins, minimizing the risk of nerve injury Figure 7).
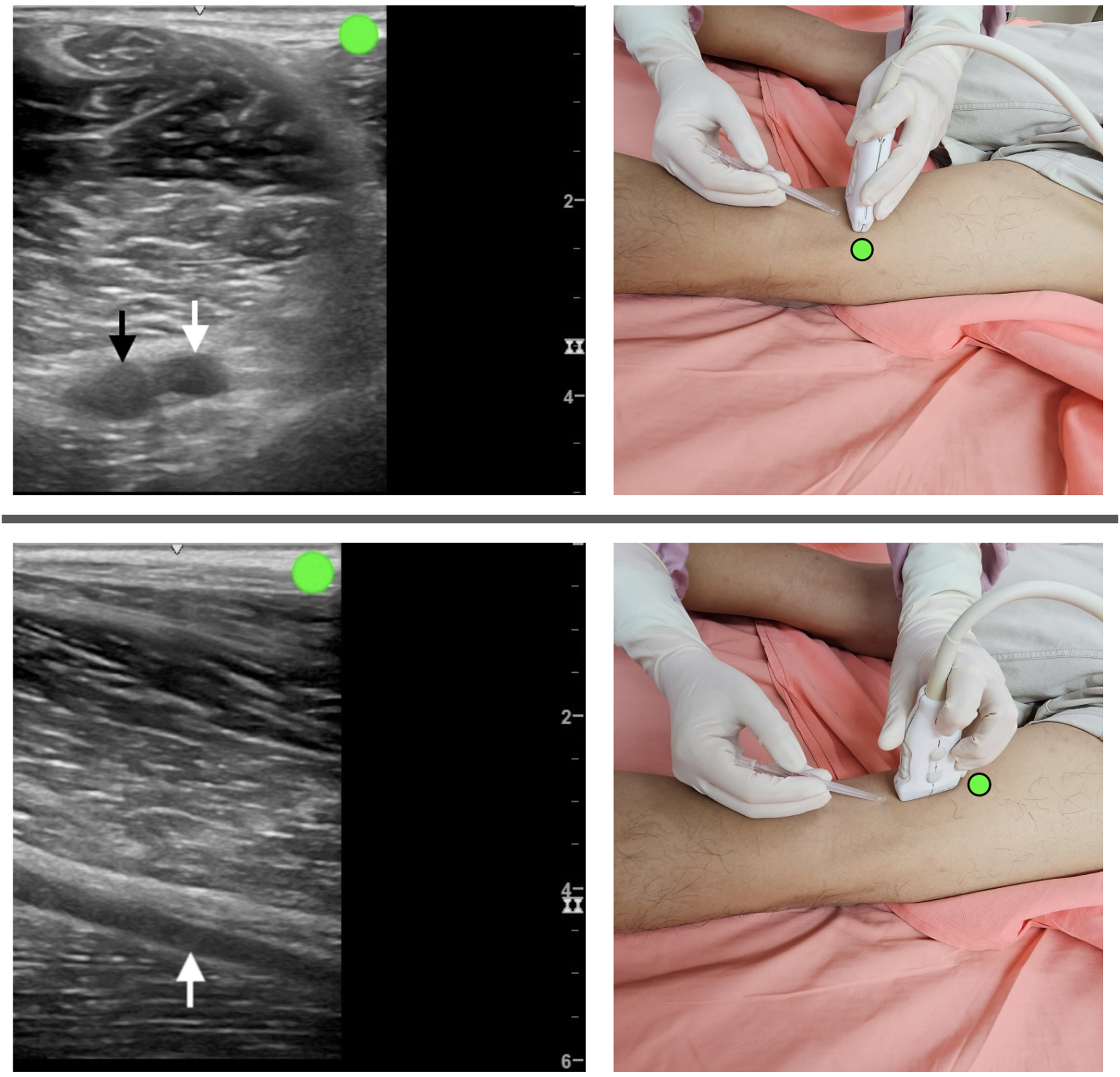
The ultrasound probe is positioned in the out-of-plane short-axis view (upper image) and in-plane long-axis view (lower image) and placed on the right lower thigh in the prone position. The white arrow indicates the popliteal vein, and the black arrow indicates the popliteal artery. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
In 132 legs from Korean and Thai cadavers, the diameter of the popliteal vein is 7.42 ± 1.21 mm (mean ± SD). 70 Catheters, such as CVC and dialysis catheters, can be placed in this location. Owing to the vein's large diameter, midline catheter, PICC, and intravenous catheter are all considered viable options.
Previous Reported Clinical Experience
A previous report demonstrated the successful placement of a CVC through the popliteal vein in a patient undergoing emergent surgery for intracerebral hemorrhage while in the PP. 71 In another COVID-19 patient complicated by ARDS was positioned prone, due to an urgent requirement for hemodialysis, a 50-cm dialysis catheter was inserted into the popliteal vein, and blood flow during the sessions consistently ranged from 300 to 400 mL/min. 72 Therefore, when in the PP and when facing difficulties in establishing a blood dialysis route, the popliteal vein can serve as an alternative option. 73
Since the popliteal vein is often narrower than the mid-thigh femoral vein, but the mid-thigh femoral vein is deeper, when placing an intravenous catheter in the PP, if the mid-thigh femoral vein is approachable, we recommend prioritizing the mid-thigh femoral vein to reduce the incidence of venous thrombosis.
Posterior Tibial Vein
Anatomy
The posterior tibial veins are formed by the convergence of the medial and lateral plantar veins. They ascend deep to the flexor retinaculum and posterior to the medial malleolus, accompanying the posterior tibial artery. 38
Tips for Successful Vascular Access
The posterior tibial artery is situated in front of the posterior tibial vein and runs parallel to the posterior tibial nerve.69,74 Therefore, precaution should be taken during a venous catheter insertion to avoid arterial puncture and nerve injury (Figure 8).
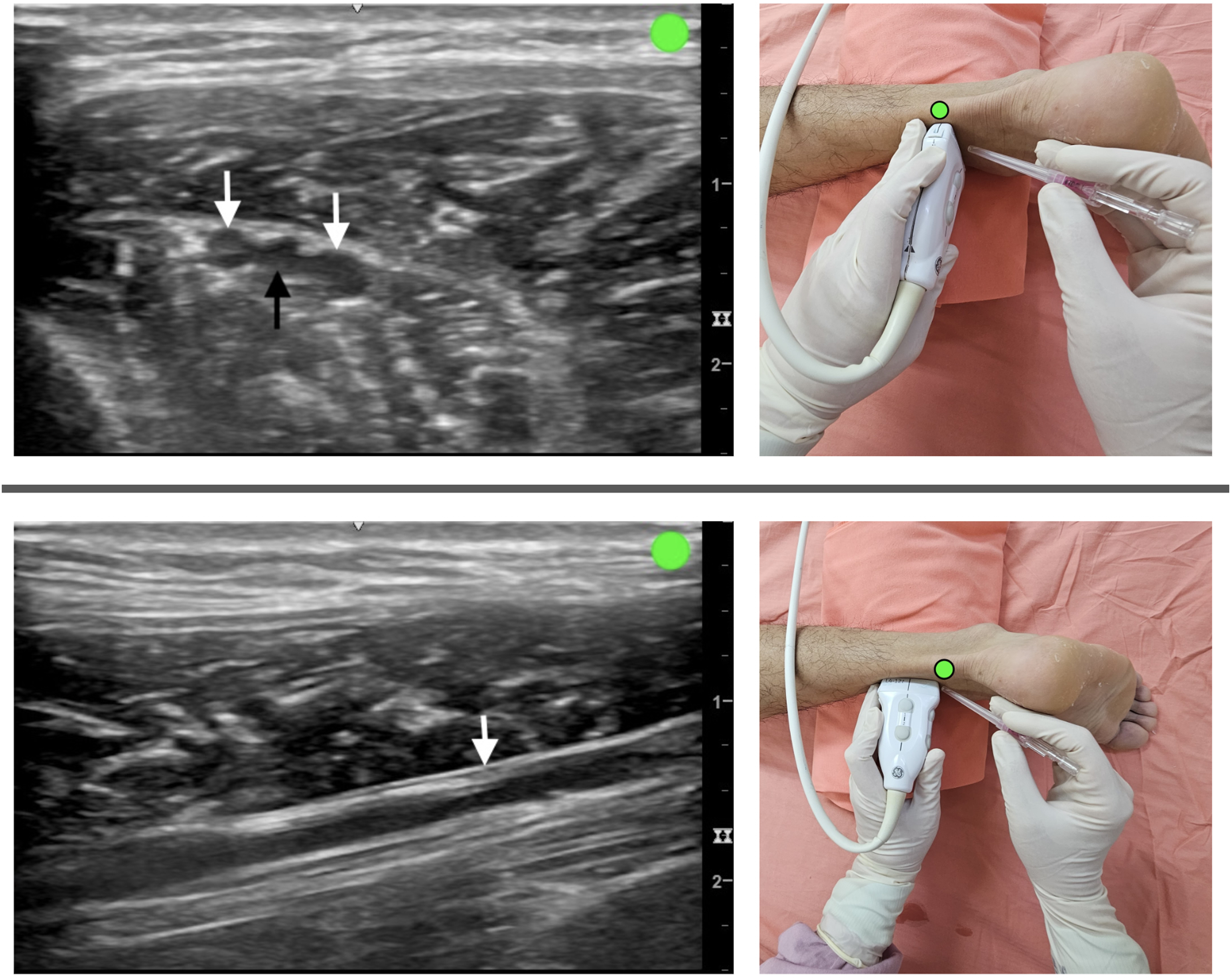
The ultrasound probe is positioned in the out-of-plane short-axis view (upper image) and in-plane long-axis view (lower image) and placed on the right ankle in the prone position. The white arrow indicates the posterior tibial vein, and the black arrow indicates the posterior tibial artery. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
In 132 legs from Korean and Thai cadavers, the diameter of the distal posterior tibial vein is 3.43 ± 1.24 mm (mean ± SD). 70 Intravenous catheters are placed multiple times in patients in the PP; however, due to the presence of smaller vessels in this area, it is less suitable for the placement of larger-diameter catheters.
Previous Reported Clinical Experience
The posterior tibial vein approach for catheter-directed thrombolysis for treating iliofemoral and femoropopliteal deep vein thromboses has been reported for years. 75 Therefore, it can be inferred that catheter placement through the posterior vein for infusion is feasible.
Small Saphenous Vein
Anatomy
The small saphenous vein originates behind the lateral malleolus as a continuation of the lateral marginal vein. In the calf's lower third, it travels along the lateral side of the calcaneal tendon, is positioned on the deep fascia, and is covered solely by subcutaneous tissue and skin. Curving medially to reach the calf's midline, it perforates the deep fascia, ascending on the gastrocnemius, only becoming visible between the deep fascia and gastrocnemius gradually, approximately at the junction of the calf's middle and proximal thirds. Continuing its ascent, it passes between the heads of the gastrocnemius and proceeds to its termination in the popliteal vein. 38
Tips for Successful Vascular Access
The sural nerve ascends directly to the lateral side of the vein, which typically runs on and then beneath the muscular fascia before reaching its endpoint. 76 The separation between the sural nerve and small saphenous vein measures 4.06 ± 1.8 and 3.4 ± 1.4 mm at the distal 50% and 25% points of the total leg length, respectively. 77 To prevent sural nerve injury, avoiding needle insertion in the lower 1/3 segment of the leg is advisable 78 (Figure 9).
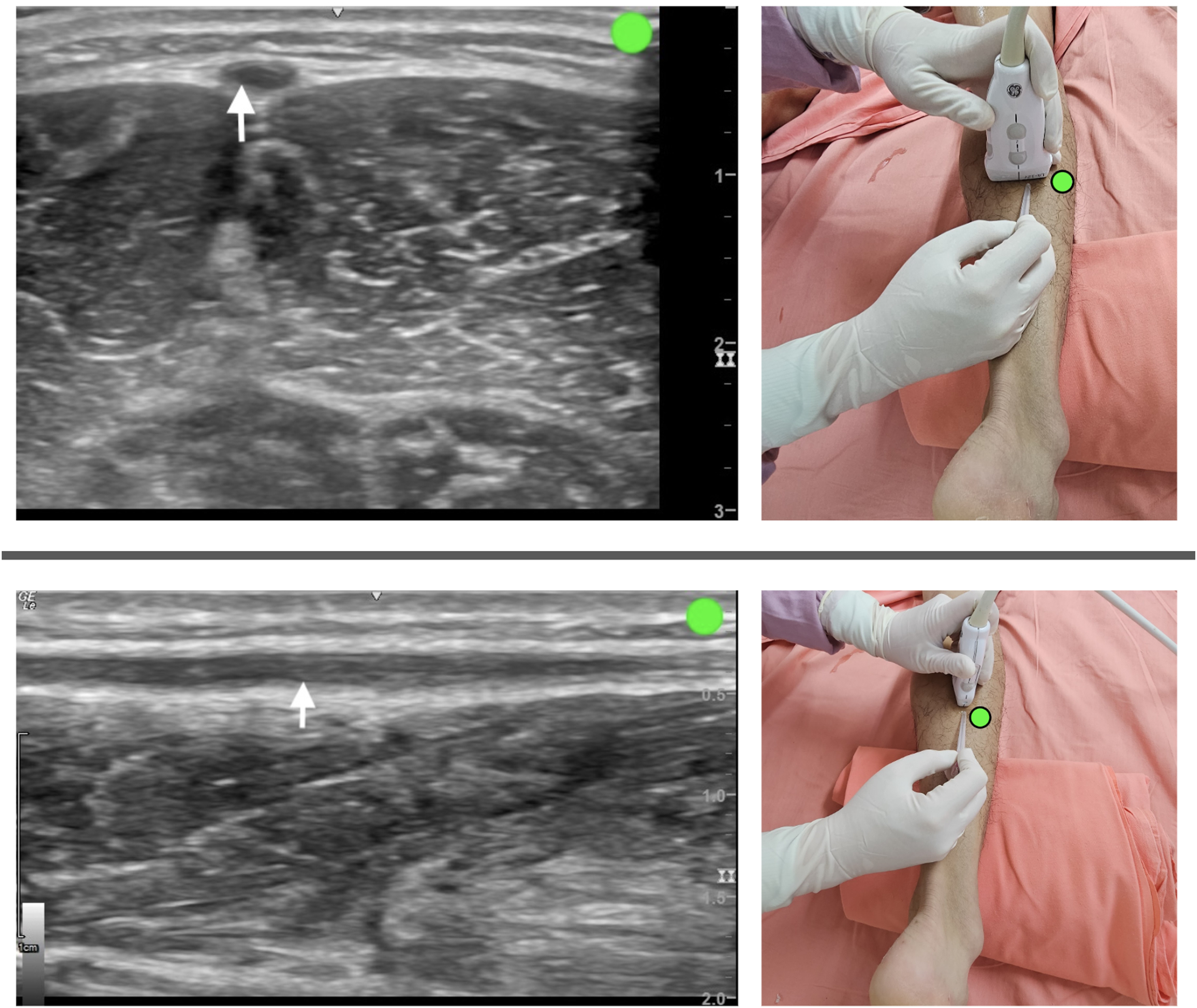
The ultrasound probe is positioned in the out-of-plane short-axis view (upper image) and in-plane long-axis view (lower image) and placed on the right calf of the leg in the prone position. The white arrow indicates the small saphenous vein. The green dot indicates the direction of the ultrasound probe.
Venous Diameter
In 132 legs from Korean and Thai cadavers, the diameter of the distal posterior tibial vein is 3.1 ± 1.3 mm (mean ± SD). 70 Although the vein is relatively small at this location, only allowing for the insertion of an intravenous catheter, its shallow depth and easy needle access allows for a convenient and rapid approach.
Previous Reported Clinical Experience
A patient underwent emergent spine surgery because of trauma. While in the PP, an 18-gauge intravenous catheter was urgently inserted on the lateral side of the mid-calf under ultrasound guidance. Therefore, this approach is considered an option for urgent intravenous access in patients placed in the PP. 79
Conclusion
The PP is frequently used for patients with severe ARDS and surgical positioning requirements. However, physicians may not be familiar with venous catheterization in this position. Our structured review provides a summary of the major accessible veins, anatomy, venous sizes, vascular access tips, and literature experience. Due to the anatomical positioning and mirror-image effect in the PP, it is recommended to use real-time ultrasound guidance to avoid unnecessary damage to surrounding nerves and arteries. We suggest using the long-axis view/in-plane technique for larger veins and the short-axis view/out-of-plane technique for smaller vessels. When selecting catheters, it is important to adhere to the principle that the ratio of catheter diameter to vessel diameter should be less than 0.67 to minimize the risk of venous thromboembolism.
Given the difficulty of the approach and the risk of complications, we recommend prioritizing the use of the IJV in the upper limb and the mid-thigh femoral vein in the lower limb. For dialysis catheters, the right IJV can be prioritized. When placing PICC lines, the basilic vein is recommended, while smaller intravenous catheters can often be placed in more superficial veins, such as the EJV, basilic vein, posterior tibial vein, and small saphenous vein. However, the above should be guided by individual patient variations and circumstances. Practitioners should still be mindful of selecting the best vessel for the intended purpose using ultrasound guidance for catheter placement in the PP.
Footnotes
Abbreviations
Authors’ Contributions
All authors were involved in the study design. KP and KH performed the review of literatures. TC and YC contributed to writing the manuscript. KP drafted and KH supervised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.