
Abstract
Background
Distinguishing surgical intensive care unit (ICU) patients with ongoing bleeding who require hemorrhage control interventions (HCI) can be challenging. Guidelines recommend risk-stratification with clinical variables and prediction tools, however supporting evidence remains mixed.
Methods
This retrospective study evaluated adult patients admitted to the surgical ICU with concern for ongoing hemorrhage under our institution's “Hemorrhage Watch” (HW) protocol and aimed to derive a clinical prediction model identifying those needing HCI with serial vital signs (VS) and serum biomarkers. The HW protocol included ICU admission followed by a 3-h observation period with VS monitoring every 15 min and hourly biomarkers. The primary outcome was the need for HCI (operative and endovascular interventions) within nine hours of ICU arrival. Secondary outcomes included in-hospital mortality, blood transfusions, and ICU and hospital length-of-stay. A clinical prediction model was developed by utilizing the variables most associated with HCI in a best subsets regression, which was subsequently internally validated using a Bootstrap algorithm.
Results
305 patients were identified for inclusion and 18 (5.9%) required HCI (3 operative, 15 endovascular). The median age was 70 years (IQR 54, 83), 60% had traumatic injuries, and 73% were enrolled from the emergency department. Blood product transfusion and mortality were similar between the HCI and no-HCI groups. Our analysis demonstrated that a model based on the minimum hemoglobin (9.9 vs 8.1 g/dL), minimum diastolic (57 vs 53 mm Hg) and systolic blood pressures (105 vs 90 mm Hg), and minimum respiratory rate (15 vs 18) could predict HCI with an area under the Receiver Operating Characteristics curve (AUROC) of 0.87, outperforming the Shock Index (SI) (AUROC = 0.64).
Conclusions
In this study of surgical ICU patients with concern for ongoing bleeding, a prediction model using serial VS and biomarkers outperformed the SI and may help identify those requiring HCI.
Introduction
Hemorrhage is the leading cause of preventable death in trauma patients, and post-operative bleeding is associated with increased morbidity, mortality, and resource utilization.1,2 For this reason, patients with concern for life-threatening hemorrhage are often admitted to the intensive care unit (ICU) where monitoring allows for the early detection of ongoing hemorrhage, resuscitative measures, and hemorrhage control interventions (HCI). 3 Continuous hemodynamic monitoring, frequent laboratory measurements, and scoring systems are all recommended to identify hemorrhage under the most recent European Guidelines on the Management of Bleeding and Coagulopathy Following Trauma. 4 However, distinguishing patients in need of HCI in the ICU remains challenging. 5
Numerous studies have investigated the use of clinical variables, including vital signs (VS) and serum biomarkers, to identify life-threatening hemorrhage over the past two decades. 6 Despite widespread adoption, research examining their utility has yielded inconsistent results and their impact on decision-making remains controversial.7–11 Similarly, serial measurements of these variables have produced mixed results.12–17 Considering this, scoring systems such as the Shock Index (SI) have also been developed to predict major hemorrhage in trauma and post-operative patients.16,18–21 Yet, a meta-analysis conducted by Carsetti et al concluded that the SI “may have a limited role as the sole tool to predict” the need for massive transfusion, while another by Gianola et al advocated for its use.22,23
Currently, evidence supporting the use of VS, biomarkers, and scoring systems to identify ongoing hemorrhage in patients admitted to the ICU for monitoring after initial resuscitations is lacking. Further, practice remains largely guided by literature predicting the need for massive transfusion, rather than the need for operative or endovascular procedures.24–28 To improve outcomes for patients with major hemorrhage at our institution, in 2017 a “Hemorrhage Watch” (HW) protocol was implemented, where patients with concern for ongoing hemorrhage after their initial resuscitation were admitted to the surgical ICU for observation. Through an investigation of this protocol and cohort, we aimed to identify clinical variables associated with HCI and derive a prediction model that can help distinguish surgical ICU patients requiring HCI.
Materials and Methods
Selection and Description of Participants
This was a retrospective study of post-operative and trauma patients determined to be at risk for ongoing hemorrhage and admitted to the surgical ICU following initial resuscitations at a single Level 1 Trauma Center between August 2017 and March 2022. In August of 2017, as part of a quality improvement initiative identifying preventable adverse outcomes resulting from hemorrhage, a “Hemorrhage Watch” protocol was implemented. This protocol consisted of admission to the surgical ICU, with VS assessments every 15 min and hourly complete blood counts and blood gas samples for a 3-h period. Concern for ongoing hemorrhage was established by CT imaging suggesting active bleeding or at the discretion of the treating surgeon based on clinical findings (ie bloody surgical drains, oozing from membranes, unstable VS). Importantly, surgical ICU clinicians were instructed to document the term “Hemorrhage Watch” in the patient chart when implementing the protocol. With data obtained during the 3-h monitoring period, the surgical and ICU teams could choose to pursue an HCI (operative or endovascular) or discontinue the protocol and continue regular ICU care.
All adult patients aged ≥18 years and admitted to the surgical ICU between August 2017 and March 2022 were screened for inclusion in the study. Using automated electronic medical record (EMR) searches for the combination keywords “hemorrhage” AND “watch”, patients undergoing the HW protocol were identified for inclusion in the study. Patients not possessing this combination of keywords within the EMR were excluded from the study. A sample of 100 cases were reviewed at random to confirm the accurate identification of HW patients and demonstrated perfect inclusion. The HW start time was defined as the surgical ICU arrival time and confirmed by the documentation of VS every 15 min within 15 min of the arrival time. Exclusion criteria included the lack of VS or biomarker measurements in at least two instances, given the purpose of serial monitoring was to construe the changes in these measurements observed by clinicians.
Data electronically extracted from the EMR and Trauma Registry included demographic information, VS, serum biomarkers, imaging reports, therapeutic interventions, and operative and procedure notes. Biomarker data specifically included hourly CBC and blood gases collected via the HW protocol, as well as other laboratory measurements collected as part of routine ICU care and cited in the literature as predictors of hemorrhage. Please see Supplement sTable 1 for a complete list of serum biomarkers. A secure private data storage platform was used for data compilation and maintenance. This study was approved by the Northwell Health Institutional Review Board (IRB) with a waiver of informed consent (IRB number: 220244, IRB title: Serial Chemical Biomarkers and Vital Sign Measurements and the Need for Operative or Interventional Radiology Management in Surgical ICU Patients with Ongoing Hemorrhage, IRB approval date: April 4, 2022). Procedures were conducted in accordance with the ethical standards of our institutional committee responsible for human experimentation and the principles reported by the Declaration of Helsinki.
The primary outcome was the use of HCI, including operative and endovascular procedures, within nine hours of ICU arrival. This timeframe was chosen due to prior literature reporting increased morbidity beyond a 6-to-12-h mark in trials of non-operative management in trauma.29,30 Operative procedures were deemed HCI if performed for hemostatic control and endovascular procedures were deemed HCI if angioembolization was performed. These procedures were identified through a manual review of operative and endovascular notes by a surgical intensivist and trauma surgeon (DJ, EK), and reviewers were blinded to predictor variables. In cases of disagreement, the two discussed and converged on a single outcome. Secondary outcomes included blood transfusions, in-hospital mortality, and ICU and hospital length-of-stay.
Data Processing and Relevant Variables
The clinical variables initially investigated as predictors for HCI included VS and biomarker measurements. To construct an HCI prediction model, several derived variables were additionally created using the VS and laboratory serial measurements obtained over the 3-h HW observation period. These included minimum systolic blood pressure (minSBP), maximum respiratory rate (maxRR), minimum pulse pressure (minPP), minimum hemoglobin (minHb), etc Using these values, delta variables were additionally calculated, as fluctuations in variable measurements over the 3-h observation period may suggest both the use of interventions (ie blood transfusions) or clinical deterioration due to hemorrhage. These included: DeltaSBP = maxSBP − minSBP, DeltaHR = maxHR − minHR, etc Both the initial Diastolic Shock Index (DSI) and Systolic Shock Index (SSI) were calculated using the first recorded systolic blood pressure (SBP0), diastolic blood pressure (DBP0), and heart rate (HR0) in each time-series using the following formulas: SSI = HR0/SBP0 and DSI = HR0/DBP0. A novel Dynamic Systolic Shock Index (DynamicSSI) and Dynamic Diastolic Shock Index (DynamicDSI) were additionally created and calculated using the following equations: DynamicSSI = maxHR/minSBP and DynamicDSI = maxHR/minDBP.
Statistical Analysis and Model Development
Descriptive statistics including frequencies and proportions for categorical variables and mean (standard deviation) and median (interquartile range) for continuous variables were used to describe the study sample. Characteristics of patients requiring HCI and those who did not were compared using Wilcoxon rank sum, t, chi-square, and Fisher's exact tests. An initial pool of clinically relevant variables (including the serum biomarkers and constructed variables described above) considered for inclusion in the model was established through literature review and expert consensus. Variables missing in no more than 20% of patients were excluded and no imputation method was used. Please see Supplement sTable 1 for a comprehensive list of biomarkers collected in the study as well as missing data.
Subsequently, variables were screened individually for association with HCI and noted when the test produced a p statistic <0.1. Maximum and delta derived variables for all lab results were dropped from the pool due to co-linearity with the minimum variables. This co-linearity is owed to the fact that lab readings were more sparse than VS and showed little variation between patients. Hemoglobin trends were additionally removed from the analysis due to a lack of linearity over time. All variables missing in no less than 20% of patients and evaluated for inclusion in the prediction model are reported in Supplement sTable 2 . Twelve variables ultimately met inclusion criterion and were selected for use during model development. An all-possible subset selection procedure was applied during model development, where 212 models including every possible combination of relevant variables was computed. From this exhaustive set we found the model with the smallest possible Akaike information criterion. The final model included the variables: MinHb, MinRR, MinSBP and MinDBP. A receiver operating characteristic (ROC) analysis was used to quantify model discrimination, and an ordinary bootstrapping algorithm with 10,000 synthetic replicates with replacement was run to assess optimism and provide internal validation for the model. Bootstrap output was then used to compute distributions and bias-corrected and accelerated (BCA) confidence intervals for the model parameters, as well as an optimism-corrected AUROC. The area-under ROC curve (AUROC) was finally compared to the AUROC of the previously described “Shock Index” in the same cohort. All statistical analyses were conducted using Python™3.1 software in conjunction with SciPy and R V4.1.2 and R suite V2022.12.0.31–34
Results
Patient Demographics
Between August 2017 and March 2022, 407 patients with concern for ongoing hemorrhage after initial resuscitations were enrolled in HW. After excluding patients with missing data, 305 patients were available for the final analysis and model development (Figure 1). The median age was 70 years (IQR 54, 83), 51% (157/305) were male, and 68% (197/291) were White. 60% (182/305) had hemorrhage secondary to trauma, while the remaining 40% (123/305) had hemorrhage due to post-operative or other etiologies. Regarding demographic distributions pertaining to outcomes of interest, a higher proportion of Black (10%) and Asian (11%) patients were found to undergo HCI when compared with White (3%) patients. The proportion of trauma patients undergoing HCI was also found to increase as Injury Severity Scores (ISS) (9 vs 19; p = 0.034) and APACHE (58 vs 64; p = 0.167) scores increased. In patients not undergoing HCI, 8% (median 350 ml; IQR 300, 600) received packed red blood cells (PRBCs) in the four hours preceding ICU admission, compared to 22% (median 300 ml; IQR 275, 300) in those undergoing HCI. Demographic variables are presented in Table 1.
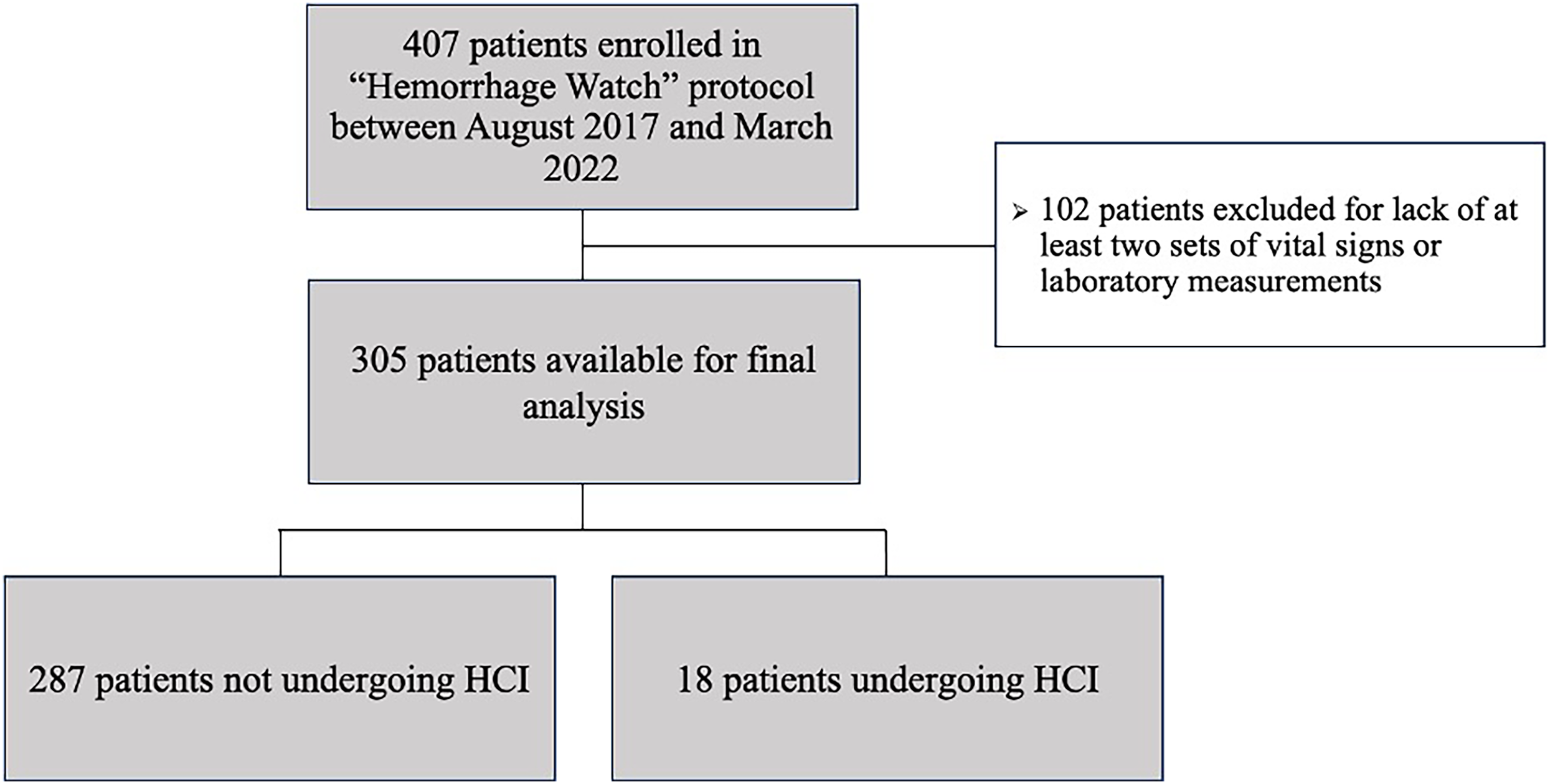
Consort diagram.
Baseline Patient Characteristics.
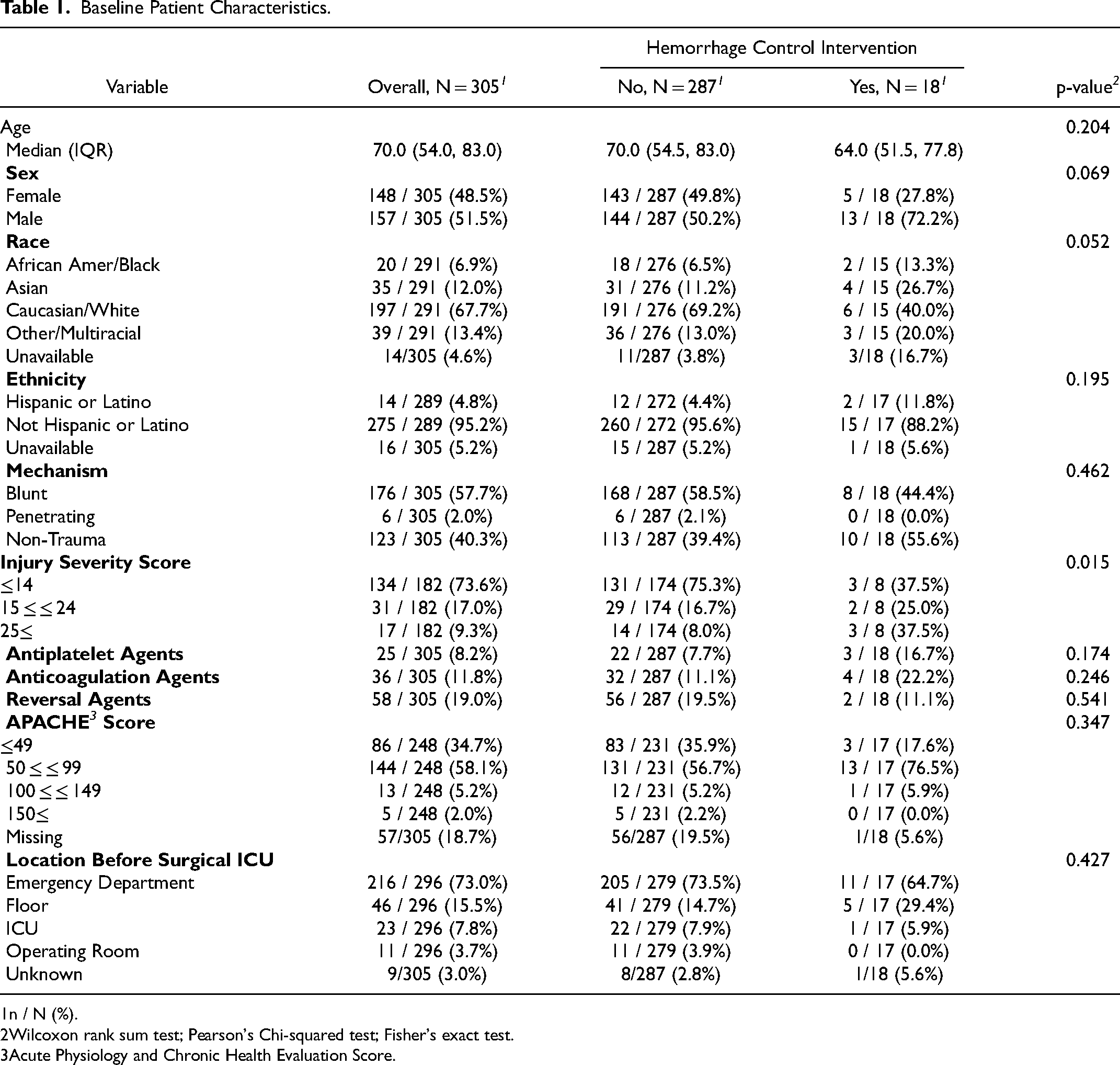
n / N (%).
Wilcoxon rank sum test; Pearson's Chi-squared test; Fisher's exact test.
Acute Physiology and Chronic Health Evaluation Score.
Outcomes
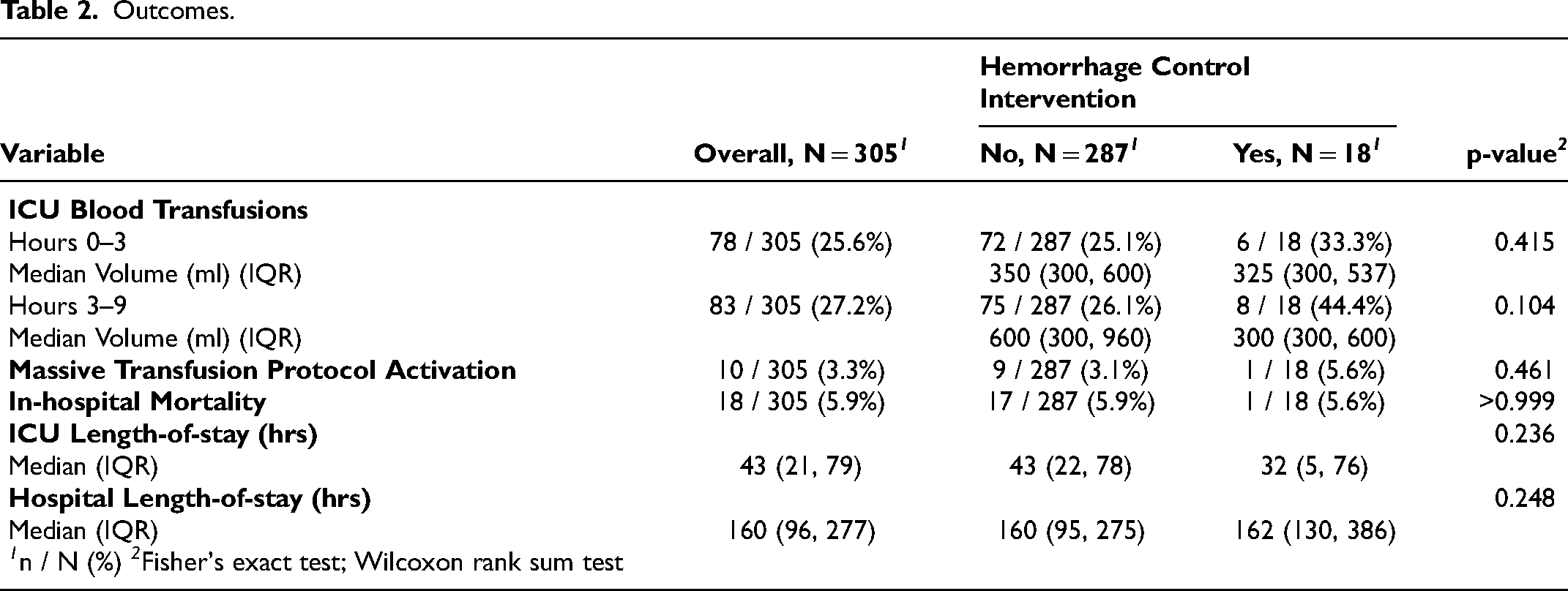
In total, 18 (5.9%) patients received HCI within nine hours of ICU arrival. 17% (n = 3) of these patients were managed operatively and 83% (n = 15) with endovascular procedures. For those undergoing HCI, the median time to an HCI was 5 h and 39 min (IQR 3:29, 7:04). The median time to an endovascular procedure was 5 h and 43 min (IQR 3:48, 7:06), compared to 5 h and 3 min (IQR 2:35, 6:59) with operative interventions (p = 0.52). The overall mortality rate was 5.9% (18/305) and in those undergoing HCI it was 5.6% (1/18). Of the 18 patients experiencing in-hospital mortality, 1 (5.6%) was determined to be secondary to hemorrhage and this patient had refused HCI. The median time to death after SICU arrival was 9 days and 18 h (IQR 7d 20hrs, 18d 18hrs). The most immediate death occurred 10 h after SICU arrival, however the remainder occurred greater than 4 days after arrival. The median ICU and hospital length-of-stay were not significantly different between groups. In patients not undergoing HCI, 25.1% received PRBCs during the 3-h HW observation period and 26.1% received PRBCs in the six hours after. In patients undergoing HCI, these values were 33.3% and 44.4%, respectively. Outcome data is presented in Table 2.
Outcomes.
Variables and Clinical Characteristics
Several variables were evaluated for their ability to distinguish patients requiring HCI. Overall, patients undergoing HCI were found to have a significantly different minSBP, maxRR, DynamicSSI, and minPP. The minSBP (90 vs 105 mm Hg) had the strongest association with HCI, followed by the minPP (34 vs 42 mm Hg) and maxRR (35 vs 31 breaths per minute). Among biomarker measurements, the minHb (8.15 vs 9.90 g/dL) had the strongest association. All patient clinical variables considered for application in the model (p < 0.1) are presented in Table 3.
Three-Hour Monitoring Variables Used in the Hemorrhage Control Intervention Prediction Model Development.
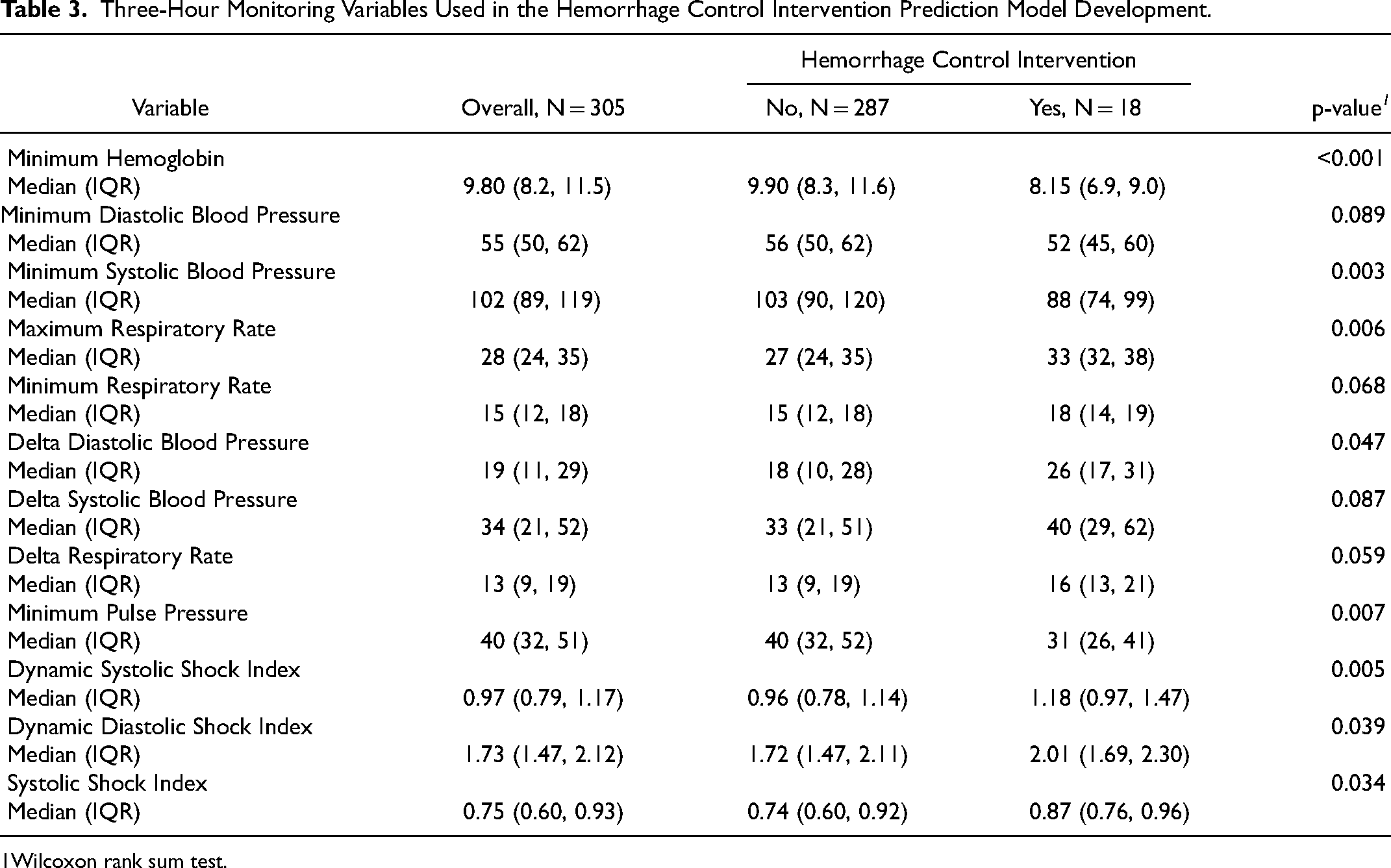
Wilcoxon rank sum test.
Using the variables obtained over the 3-h HW observation period, an HCI prediction model was created and optimized to distinguish patients requiring HCI. The final prediction model utilized minDBP, minSBP, minRR, and minHb. It should be noted that even though the minDBP was lower in the HCI cohort, the regression fit assigned this variable a positive coefficient. After direct inspection it was determined that the minDBP and minSBP interacted within the model, in that HCI were more likely in patients with a higher minDBP in the setting of a low minSBP. This interaction led us to consider minPP as a variable, but the minSBP/minDBP pair yielded a model with similar ROC value, and lower Akaike information.
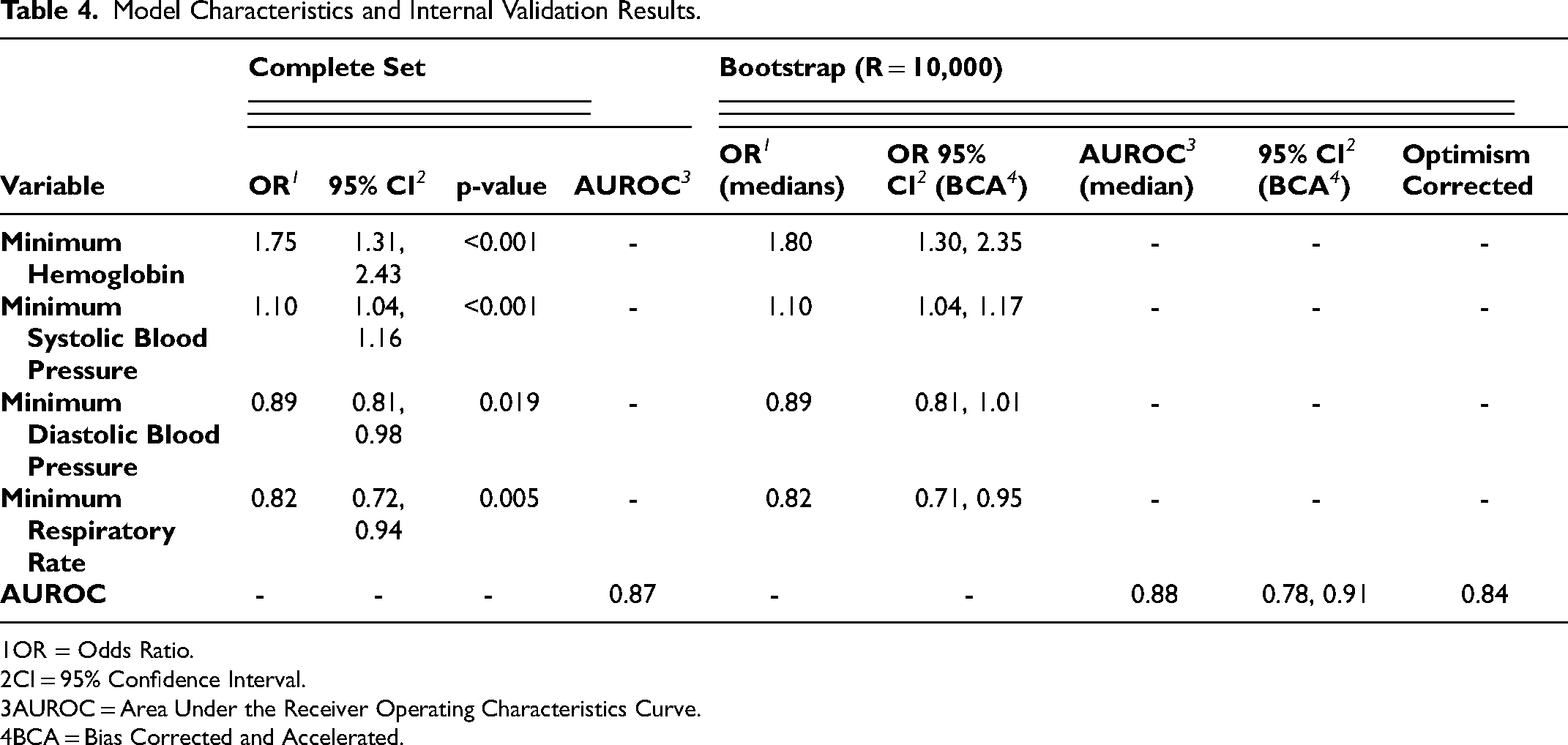
The derived model ultimately predicted the need for HCI in our cohort with an AUROC of 0.87. A point on the ROC curve selected under a maximum sum criterion yielded a sensitivity of 88.9% and specificity of 74.5%. A post-hoc sample size calculation with 80% power resulted in a minimum of N = 180 subjects, of which 19 are positives. The ROC curves for the HCI prediction model and SI are shown in Figure 2. Odds ratios with 95% confidence intervals, and bootstrap estimates for model variables and the AUROC statistic are reported in Table 4. Supplement sFigure 1 additionally displays the model's ROC curve alongside the variables having strong associations with HCI (ie DynamicSSI, DynamicDSI, minPP, and maxRR).
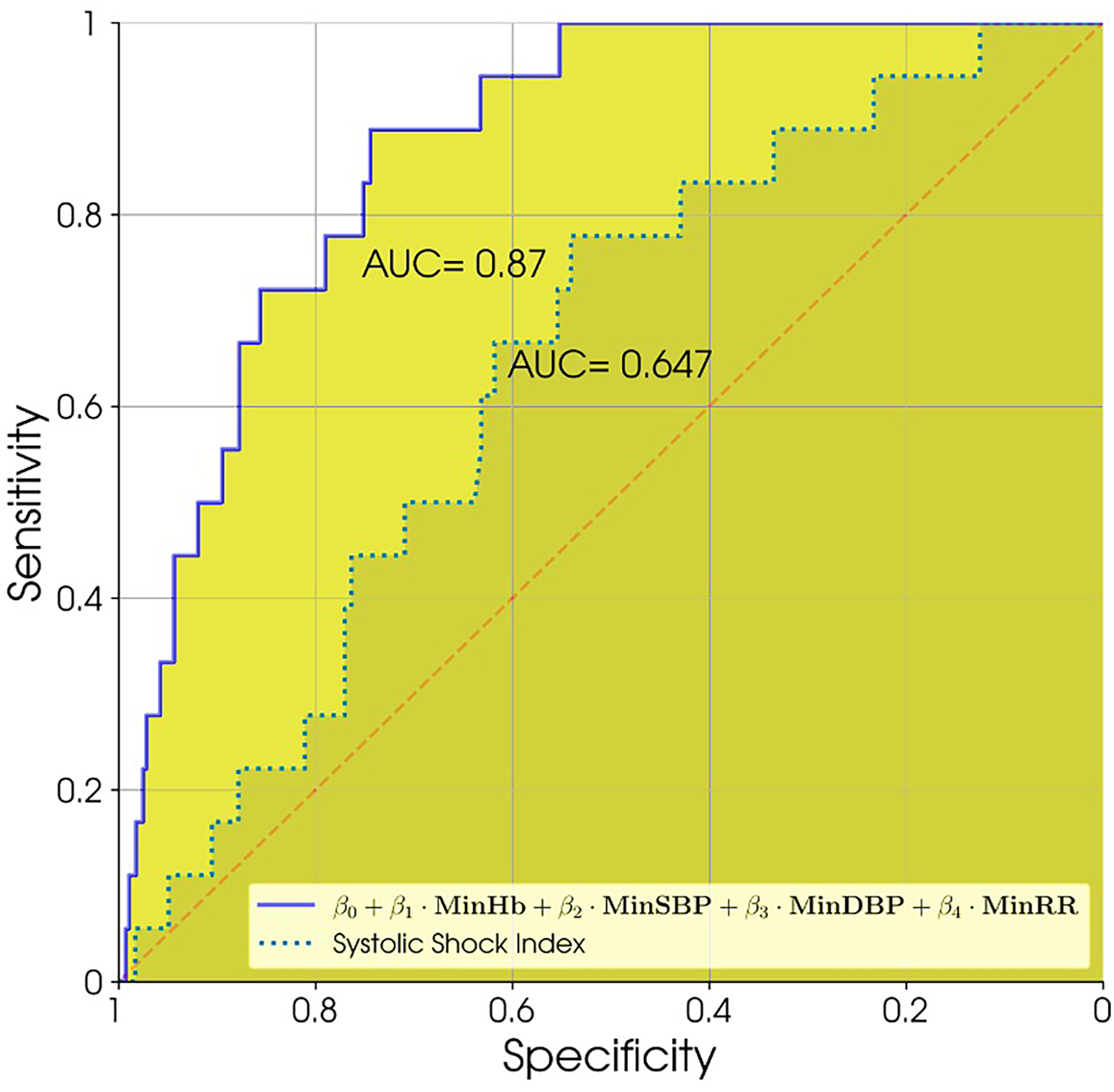
Receiver operating characteristics curves for the computed hemorrhage control intervention prediction model versus systolic shock Index.
Model Characteristics and Internal Validation Results.
OR = Odds Ratio.
CI = 95% Confidence Interval.
AUROC = Area Under the Receiver Operating Characteristics Curve.
BCA = Bias Corrected and Accelerated.
Discussion
In this study of patients admitted to the surgical ICU with concern for ongoing hemorrhage following initial resuscitations under our HW protocol, which included serial VS and biomarkers, the minHb, minSBP, maxRR, and minPP had the strongest associations with the requirement for HCI. Notably, this finding suggests that minimum and maximum values obtained over a period of observation may be able to assist in the identification of those at risk for ongoing bleeding. When applying variables obtained over the 3-h observation period in a derived clinical model, the need for HCI could be predicted with a sensitivity of 88.9% and a specificity of 74.5%. Bootstrap validation additionally produced parameter estimates and confidence intervals in good agreement with those of the model, with an optimism corrected AUROC of 0.84. When compared to the Shock Index, touted in the most recent European Guidelines to help identify severe hemorrhage, our derived model demonstrated superior discriminatory value.
Regarding outcomes, although patients undergoing HCI received blood transfusions more frequently, this difference was not found to be statistically significant. Additionally, only 27% of patients in our cohort received PRBCs in the nine hours following the HW start time, and even less required HCI (5.9%). These low HCI rates bring attention to the screening process for ICU monitoring for hemorrhage, and whether many patients could be safely observed outside the ICU remains an important question. To address this issue, we derived a prediction model using readily available VS and biomarker variables to identify patients in need of HCI. The strength of this model was found to be in part related to the interaction between the minDBP and minSBP within it, as their relationship improved its discriminatory value significantly - even more so than the minPP. Further, while the minDBP and minRR were not strongly associated with HCI in our initial analysis, it should be noted that these factors improved the predictive value of the model during development. Interestingly, it was specifically an elevated minRR, representing an increase in the lowest documented respiratory rate obtained over the 3-h observation period, which was incorporated into the final model. Although an elevated maximum respiratory rate is often referenced as an indicator of severe hemorrhage, the concept of an elevated minimum respiratory rate (minRR) is less intuitive and may warrant investigation as a predictor of adverse outcomes in future studies. This is particularly true given the increasing ability to obtain comprehensive monitoring data using modern EMRs.
Evidence regarding scoring systems and prediction models to risk–stratify ICU patients for ongoing hemorrhage is currently limited, and prior research has focused largely on the need for massive transfusion rather than HCI.35–37 Additionally, although scoring systems predicting the need for HCI in specific populations have been investigated, their application in the ICU where the causes of bleeding can be diverse is lacking.38–43 Previously, Pasquale et al developed a predictive model using continuous VS monitoring and biomarkers which could predict the need for greater than three units of PRBCs within 24 h in post-operative ICU patients (AUROC = 0.93). 35 Kang et al also demonstrated that machine learning could predict the need for hemorrhage control procedures and transfusion volumes greater than 1500 ml (AUROC = 0.74). 36 Our model builds upon this existing literature and brings attention to the feasibility of models identifying patients requiring HCI for ongoing hemorrhage with readily available clinical variables. This model also more directly addresses the “post-initial resuscitation” phase in patients who were deemed at risk for ongoing hemorrhage. This closely resembles a real-life scenario that surgeons and intensivists must face regularly.
The application of predictive models like this one to identify ongoing hemorrhage following initial resuscitations has several immediate clinical benefits. While blood transfusions are associated with potential harms and resource utilization, HCI are arguably more resource intensive and carry greater harms. Therefore, it is imperative to focus our attention on identifying patients requiring HCI more accurately and expeditiously. Next, given the complexities inherent in HCI implementation, including the need to prepare an operating room or activate off-site staff, an accurate and parsimonious prediction model could shorten the time to lifesaving HCI and potentially avoid “cautionary” team activations. Lastly, a predictive model which uses fewer datapoints and is reliable in patient populations with diverse sources of bleeding, from trauma to post-surgical, would be valuable in both ICU and non-ICU settings. A strategy like this could help identify patients requiring intensive care, while also discriminating patients at low risk for bleeding who may be safely monitored outside the ICU.
Overall, with an increasing utilization of predictive models to assist ICU providers with clinical decision making in recent years, analyses similar to this are likely to become more prevalent.44–49 Future research will focus on the validation of our prediction model and monitoring its use for safety in patient populations less represented in our cohort (ie penetrating trauma). Eventually, external validation at other institutions could improve our model's predictive accuracy. Additionally, with only a small proportion of patients in our cohort undergoing HCI, variables that could help select patients who can be safely observed outside the ICU must be investigated. Ultimately, we hope that the incorporation of this model into the EMR will assist in the identification of patients at risk for bleeding, while improving both patient outcomes and resource allocation.
Limitations
This study has several important limitations. First, both enrollment in our HW protocol and the use of HCI were at the discretion of the attending intensivist physician, albeit often in conjunction with the surgeon or interventional radiologist, allowing for selection biases related to variable practice patterns. The retrospective nature of the study additionally limits the ability to determine precisely when and on what basis decisions to intervene were made. The finding of higher ISS and APACHE scores in patients undergoing HCI argues that this was in fact a sicker cohort, however this point remains a limitation none-the-less. Second, the results should be interpreted within the context of our patient population at a single, Level-1 trauma center, with an elderly cohort demonstrating a high rate of blunt traumatic injuries. These characteristics may limit generalizability and require replication in alternative and larger sample sizes. Third, the protocol in our study was implemented following initial resuscitations outside the ICU, and therefore these results are not meant to influence care of patients outside of ICU settings, such as in initial emergency department resuscitations. Fourth, the retrospective nature of the study resulted in missing information, most notably regarding APACHE scores, VS, and biomarker variables, and this may have influenced the study's outcomes. It is possible that the severity of illness and time required to document VS every 15 min made compliance challenging, and this must be addressed in future studies. Importantly, this was considered during model development and to enhance reliability only variables with high response rates could remain in the model. Fifth, although there has been a growing body of evidence surrounding the use of thromboelastography in hemorrhage, testing was not available at our institution until 2020 and therefore it was not included in our protocol. 49 Finally, it should be noted that the rate of HCI in our cohort is relatively low, and the results of the study should be interpreted with this in mind. Future research will be required to evaluate the model's application in larger sample sizes to fully establish its discriminatory value, while also ensuring its calibration through external validation.
Conclusion
In this study of surgical ICU patients suspected of ongoing hemorrhage following initial resuscitations, the minHb, maxRR, minSBP, and minPP were found to be associated with the need for HCI. Using readily available clinical variables obtained over a 3-h observation period, it was feasible to derive a prediction model which could discriminate patients requiring HCI which outperformed the SI. Further research is needed to confirm this model's value and compare its use to existing hemorrhage prediction models, including the SI.
Supplemental Material
sj-docx-1-jic-10.1177_08850666241312614 - Supplemental material for A Combined Model of Vital Signs and Serum Biomarkers Outperforms Shock Index in the Prediction of Hemorrhage Control Interventions in Surgical Intensive Care Unit Patients
Supplemental material, sj-docx-1-jic-10.1177_08850666241312614 for A Combined Model of Vital Signs and Serum Biomarkers Outperforms Shock Index in the Prediction of Hemorrhage Control Interventions in Surgical Intensive Care Unit Patients by John P. Forrester, Manuel Beltran Del Rio, Cristine H. Meyer, Samuel P. R. Paci, Ella R. Rastegar, Timmy Li, Maria G. Sfakianos, Eric N. Klein, Matthew E Bank, Daniel M. Rolston, Nathan A Christopherson and Daniel Jafari in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666241312614 - Supplemental material for A Combined Model of Vital Signs and Serum Biomarkers Outperforms Shock Index in the Prediction of Hemorrhage Control Interventions in Surgical Intensive Care Unit Patients
Supplemental material, sj-docx-2-jic-10.1177_08850666241312614 for A Combined Model of Vital Signs and Serum Biomarkers Outperforms Shock Index in the Prediction of Hemorrhage Control Interventions in Surgical Intensive Care Unit Patients by John P. Forrester, Manuel Beltran Del Rio, Cristine H. Meyer, Samuel P. R. Paci, Ella R. Rastegar, Timmy Li, Maria G. Sfakianos, Eric N. Klein, Matthew E Bank, Daniel M. Rolston, Nathan A Christopherson and Daniel Jafari in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
The authors would like to thank the clinical and research staff at North Shore University Hospital and the Northwell Health Trauma Institute for their contributions to the care of these patients and the conduction of this study.
Author Contributions
John Forrester, DO: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Visualization; Writing – original draft; Writing – review & editing.
Manuel Beltran Del Rio, PhD: Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Visualization; Writing – original draft.
Ella Rastegar, BS: Conceptualization; Writing – original draft; Writing – review & editing.
Cristine Meyer, MPH: Conceptualization; Data curation; Methodology; Resources; Writing – review & editing.
Maria Sfakianos, MD: Conceptualization; Investigation; Methodology; Supervision; Writing – review & editing.
Samuel Paci, MD: Data curation; Writing – review & editing.
Eric Klein, MD: Conceptualization; Investigation; Methodology; Supervision; Writing – review & editing.
Matthew Bank, MD: Conceptualization; Investigation; Methodology; Supervision; Writing – review & editing)
Timmy Li, PhD (Methodology; Supervision; Writing – review & editing.
Daniel Rolston, MD, MPH: Conceptualization; Investigation; Methodology; Supervision; Writing – review & editing.
Nathan A Christopherson, DNP, MBA, MSN, RN: Conceptualization; Supervision; Writing – review & editing.
Daniel Jafari, MD, MPH: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Visualization; Writing – original draft; Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Northwell Health Institutional Review Board (IRB) with a waiver of informed consent (IRB number: 220244, IRB title: Serial Chemical Biomarkers and Vital Sign Measurements and the Need for Operative or Interventional Radiology Management in Surgical ICU Patients with Ongoing Hemorrhage, IRB approval date: April 4, 2022). Procedures were conducted in accordance with the ethical standards of our institutional committee responsible for human experimentation and the principles reported by the Declaration of Helsinki.
Consent to Participate
This study was approved by the Northwell Health Institutional Review Board (IRB) with a waiver of informed consent.
Consent for Publication
Not applicable.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interest
Daniel Jafari Received funding from the Zoll Foundation. Daniel Rolston received funding from Flosonics.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.