
Abstract
It seems logical to divide the macrocirculation into systemic and pulmonary circulation, but it is rare in clinical practice to further subdivide microcirculation into systemic and pulmonary microcirculation. Both systemic and pulmonary microcirculations play important roles in the development and progression of critical illness. Therefore, targeting the overall microcirculation status for clinical treatment may overlook the heterogeneity of different critically ill patients. It seems unavoidable to further subdivide the microcirculation, so this review explains the differences in structure, function, blood flow regulation, and other important aspects between systemic and pulmonary microcirculation, systematically presenting the concept of “double microcirculation.” At the same time, to refine the critical care treatment and even improve the prognosis of critically ill patients, we further propose and explain the treatment key points based on “double microcirculation protection.”
Keywords
Introduction
Critically ill patients often exhibit abnormal microcirculation. However, due to the mismatch between macrocirculation and microcirculation hemodynamics, attention is frequently focused solely on the microcirculation, which may not always provide an accurate and effective assessment of the patient's condition. 1 Consequently, there has been an increasing recognition of the importance of considering microcirculation in critically ill patients in recent years, leading to the development of numerous microcirculation-oriented treatment strategies.2,3 Despite these advancements, the mortality for critical illnesses such as sepsis remains high. 4 Dobson et al 5 recently proposed that sepsis treatment should be grounded in a systematic pathophysiological mechanism. This theory has stimulated our thinking and offered a new research direction and therapeutic concept.
We often divide the macrocirculation into systemic and pulmonary circulation, and there are obvious differences between the two at the macro level. Interestingly, while in the past we tended to describe and target the microcirculation as a whole for clinical treatment guidance, recent years have seen a deeper understanding and exploration, leading to a trend of further refinement in the microcirculation.6,7 Experts are increasingly recognizing that pulmonary microcirculation may possess distinct functions and features. Schneider et al 8 subdivided microcirculation into systemic and pulmonary microcirculation in 1968 when exploring meconium embolism. Subsequently, Doerschuk et al 9 compared the adhesion of neutrophils and endothelial cells (ECs) in pulmonary microcirculation versus systemic microcirculation of rabbits, confirming organ-specificity within the microvasculature likely due to differential responses of pulmonary and systemic ECs to the same stimulus. It is reasonable to infer that critical illnesses may lead to dysfunction within more specific subtypes of the microcirculation, thus necessitating a more systematic treatment strategy. Therefore, based on the development of understanding of microcirculation in critically ill patients in recent years, this review emphasizes the importance of subdividing microcirculation into pulmonary and systemic components while advocating the treatment key points of “double microcirculation protection” to enhance critical care efficiency and improve patient prognosis.
Common Abnormalities of Systemic and Pulmonary Microcirculation in Critically Ill Patients
The microcirculatory dysfunction commonly observed in critically ill patients has been extensively emphasized and thoroughly discussed. As a systemic condition, microcirculatory dysfunction may affect multiple organs, such as the lung, kidney, liver, stomach, intestine, and brain. 10 Compared with microcirculation in other organs, pulmonary microcirculation has more unique properties. For example, the dual systems (pulmonary and bronchial) blood supply and direct oxygen diffusion from the airways make the pulmonary microcirculation uniquely tolerant to ischemia and hypoxia. 11 Therefore, it is essential to explore the impact of critical illness on systemic and pulmonary microcirculation separately.
Systemic Microcirculation
Taking sepsis and septic shock as examples, most discussions are based on systemic microcirculation, and it is believed that the change of microcirculation has far-reaching significance and is a key factor in the pathogenesis of critical illnesses. 12 While discussions have primarily focused on sepsis, it is noteworthy that other critical diseases can also result in abnormal microcirculation. Recent research by Merdji et al 13 comprehensively describes the relationship between cardiogenic shock and microcirculatory perfusion dysfunction, highlighting that the prognosis is closely related to microcirculation rather than macrocirculation. Trauma patients are also very common in the intensive care unit (ICU), and microcirculatory dysfunction is now recognized as a key pathogenic mechanism of the disease progression, even related to multiple organ dysfunction syndrome. This research result also suggests that interventions to preserve microcirculation and ensure adequate oxygen delivery will likely yield positive effects. 14 In addition, the unique systemic circulation characteristics of critically ill patients may also be an important factor in causing microcirculatory dysfunction. Critically ill patients often exhibit a high cardiac drive state in the early stages of the disease, leading to alterations in both macrocirculation and microcirculation. For instance, septic shock frequently presents with normal or high cardiac output (CO) and oxygen delivery, with normal systemic and local blood flow; however, it may still manifest microcirculatory dysfunction, resulting in insufficient tissue perfusion. One potential mechanism underlying this phenomenon is the accelerated red blood cell (RBC) flow rate induced by the high cardiac drive, resulting in reduced oxygen dissociation efficiency in the microcirculation. Research on septic rats demonstrated that high cardiac drive caused an increase in capillary RBC average flow rate by about 17%. 15 The study of Edul et al 16 partially supported this hypothesis: septic shock often has a marked high CO and low systemic vascular resistance and is related to increased RBC flow rate in the microcirculation, but some small vessels also show slow perfusion velocity, which may suggest the heterogeneity of blood flow in septic shock. However, some microvascular also exhibited slow perfusion, indicating potential blood flow heterogeneity during septic shock. Unfortunately, there are still few high-quality clinical studies to confirm the statement that critically ill patients have increased RBC flow rates. 17 A study involving septic shock patients did not reveal a significant increase in RBC flow rate; nevertheless, considering that the study mainly encompassed patients with normal CO, it cannot be ruled out that those with high CO might experience higher RBC flow rates. 18 Koning et al 19 also noted an increase in RBC flow rate among patients with cardiopulmonary bypass; however, the pathophysiology of such patients was not the same as that of patients with septic shock.
Pulmonary Microcirculation
Pulmonary microcirculation abnormalities can easily occur, whether influenced by systemic macrocirculation and microcirculation or by the unique respiratory characteristics of critically ill patients. Critically ill patients are prone to cardiac function abnormalities, leading to a mismatch between left and right cardiac function that may increase pressure in the left atrium and pulmonary veins, thereby raising pulmonary microcirculation hydrostatic pressure. 20 Elevated pulmonary vascular hydrostatic pressure can increase the permeability of the alveolar-capillary membrane, ultimately causing pulmonary congestion and edema. Additionally, septic shock patients often experience increased CO, which can lead to elevated pulmonary blood flow rate and volume, further increasing pulmonary vascular hydrostatic pressure and transvascular pressure. This result is similar to the perspective of Jozwiak et al, 21 who state that higher CO leads to greater volume in the pulmonary blood vessels to elevate hydrostatic pressure, while extravascular lung water (EVLW) increases with volume expansion at the same permeability. Simultaneously, higher transvascular pressure can damage ECs of pulmonary microcirculation while also increasing permeability significantly, greatly increasing the risk of pulmonary edema and impacting lung compliance and gas exchange function. 22 Pan et al 23 confirmed that high CO increases EVLW and exacerbates pulmonary edema; interestingly, EVLW is decreased in cardiogenic shock patients. Furthermore, under conditions ensuring tissue perfusion is maintained appropriately, reducing CO may reduce the severity of pulmonary edema while improving patient prognosis. Moreover, critically ill patients often exhibit high respiratory drive, a unique respiratory state that significantly impacts pulmonary microcirculation. High respiratory drive can augment transpulmonary pressure in critically ill patients suffering from conditions such as acute respiratory distress syndrome (ARDS), potentially resulting in excessive lung distension and heightening the risk of barotrauma and volutrauma during ventilation. 24 It is crucial to recognize that excessive inspiratory effort may be accompanied by a decrease in alveolar pressure, even falling below the level of positive end-expiratory pressure (PEEP), particularly when airway resistance increases. 25 The decreased alveolar pressure may elevate transcapillary pressure across pulmonary microvessels, exacerbating pulmonary edema. 26 Furthermore, a rapid decrease in alveolar pressure can also damage pulmonary ECs and alveolar epithelial cells, undermining the integrity of the pulmonary vascular-alveolar barrier and increasing permeability within the pulmonary microcirculation, ultimately leading to pulmonary interstitial edema. 27
The Concept of “Double Microcirculation”
The widespread involvement of systemic and pulmonary microcirculation in critical illnesses manifests their huge contributions to the occurrence and development of critical illnesses. This understanding has also promoted continuous exploration of microcirculation changes in critical illnesses in recent years. The update of related concepts and the rapid development of monitoring technologies have made bedside assessment of microcirculation an integral part of clinical practice. Although there is still a lack of technology and equipment to assess pulmonary microcirculation at the bedside visually, some laboratory results still show differences between systemic and pulmonary microcirculation. For example, by assessing the subpleural alveolar microcirculation using sidestream dark field imaging, He et al 28 found high PEEP would damage both systemic and pulmonary microcirculation; however, the improvement in pulmonary microcirculation after fluid therapy was much weaker than in systemic microcirculation. This difference also suggests that assessing the condition based on the whole microcirculation can no longer meet the needs of precision intervention in clinical practice, which may also be one of the reasons why the mortality of critically ill patients remains difficult to decrease significantly. 4 Therefore, it is necessary to classify microcirculation further based on its homogeneity and heterogeneity in a detailed and reasonable manner. The terms “systemic microcirculation” and “pulmonary microcirculation” have been proposed for a long time. However, high-quality research and systematic theories supporting the detailed microcirculation classification still need improvement. 8 Therefore, this review will provide theoretical support for “double microcirculation” by explaining systemic and pulmonary microcirculation from the perspective of structure, function, blood flow regulation, and other aspects (Table 1).
Comparison of Pulmonary and Systemic Microcirculation.
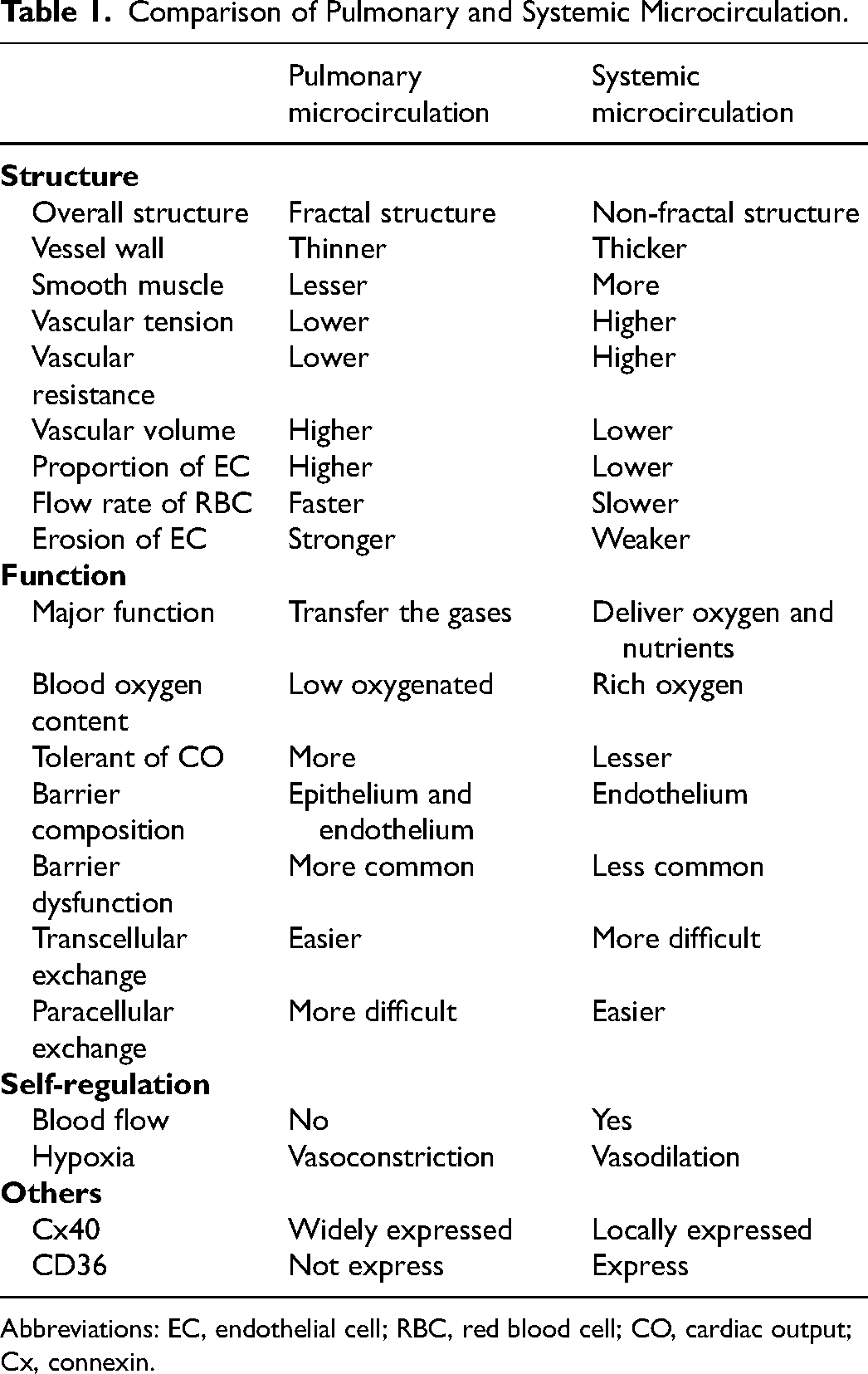
Abbreviations: EC, endothelial cell; RBC, red blood cell; CO, cardiac output; Cx, connexin.
Structure
The maturation of pulmonary microvessels is one of the few lung development processes that persist into young adulthood, suggesting the importance and complexity of pulmonary microcirculation. 29 The structure of the pulmonary circulation is very distinctive, and the pulmonary vessels form a complete vascular tree by repeatedly adding branches at the end of each branch, so the pulmonary circulation is considered a fractal structure. 30 This unique structure creates as much surface area as possible within a limited volume while minimizing the blood flow and power consumption required for pulmonary microcirculation perfusion. 31 Correspondingly, the structure of this vascular tree will also have the disadvantage of unequal blood flow distribution. 32 Therefore, it is crucial to ensure the matching of ventilation and perfusion in the pulmonary microcirculation to achieve effective gas exchange. Pulmonary circulation has thinner vessel walls and much less smooth vascular muscles than systemic circulation. Even muscular arteries with more smooth muscle still have thinner walls than systemic arteries of the same diameter, so the underlying vascular tension is relatively weak. 33 The walls of pulmonary capillaries are thinner and consist of a single layer of ECs. 34 The normal pulmonary vascular resistance is approximately one-tenth that of the systemic circulation, potentially due to the high levels of endogenous vasodilators and low production of vasoconstrictors. 35 Therefore, pulmonary microcirculation operates as a low-resistance, high-volume system, whereas systemic microcirculation is characterized by high resistance and low volume. Interestingly, the thickness of the pulmonary capillary wall varies. 33 For example, the part of the alveolar-capillary wall responsible for gas exchange can be thinned, basically consisting of only the alveolar epithelium facing the gas side, the endothelium on the blood side, and a single layer of basement membrane between the two, only 20–30 nm thick. At the same time, the cell contents and nucleus are transferred to the “thick” side wall at the non-gas exchange. 33 Pulmonary microcirculation is the primary site for gas exchange between the alveoli and the blood. The thickness of the microvascular membrane and vascular perfusion are crucial for maintaining normal gas exchange. 36 Both systemic and pulmonary microcirculation are primarily composed of ECs. However, the proportion of ECs is greater in pulmonary microcirculation. The microvascular membrane in pulmonary microcirculation is thicker, the flow rate of RBC is faster, and the erosion of ECs occurs at a higher rate in this area.37,38 The endothelial glycocalyx plays an important role in ensuring the integrity of pulmonary microvessels, and the concentration of degradation products (such as syndecan-1 and hyaluronic acid) is closely related to the severity degree of pulmonary microcirculation injury.39,40 In addition, compared with systemic microcirculation, pulmonary microvascular ECs contain abundant pores, mediating the active transport of specific molecules from blood vessels to the interstitial space. Therefore, it is easy to see that the systemic microcirculation is structurally very different from the pulmonary microcirculation.
Function
Pulmonary microcirculation is also functionally unique, with clear differences from systemic microcirculation. The main function of systemic microcirculation is to deliver oxygen and nutrients to organs and tissues, while the main function of pulmonary microcirculation is to facilitate the transfer of gases across the alveolar-capillary membrane while limiting waste products from entering the lungs.41,42 The pulmonary micro-arteries carry a mixture of venous blood, and deoxygenated blood flows from the pulmonary artery through the alveolar-capillary units, where extensive gas exchange occurs, and gradually returns to the left atrium via the pulmonary micro-veins before being gradually distributed to the systemic microcirculation. The close contact between the pulmonary artery and the trachea highlights the relationship between ventilation and perfusion and plays a decisive role in the normal function of the lungs. Therefore, although the systemic and pulmonary vessels have similar histological arrangements, the two circulatory systems also have unique functional attributes and characteristics. For example, the pulmonary microcirculation is more tolerant of large fluctuations in CO, thus ensuring that blood pressure does not change significantly and maintaining its low-resistance, high-compliance feature. 35 Interestingly, this feature reduces the ECs in the pulmonary vasculature from experiencing shear stress and injury, thereby greatly reducing the incidence of atherosclerosis, which is extremely important. 43 Pulmonary microcirculation also filters blood, removes microemboli, and regulates the metabolic regulation of various vasoactive substances. 35 Furthermore, compared with the systemic large vessels and microvessels, maintaining a complete barrier has a more important physiological significance in pulmonary microcirculation. The alveolar epithelium and vascular endothelium together form a unique dual-layer barrier structure, effectively preventing alveolar and interstitial edema formation. The pulmonary microcirculation has a stronger limitation on the exudation of fluid and proteins in the vessel lumen, aiming to minimize edema in the alveoli and interstitium, which is of great importance for maintaining the effective gas exchange in the pulmonary microcirculation. 44 The more tightly packed vascular barrier in the pulmonary microcirculation makes it a preferred site for transcellular action, ensuring continuous transcellular exchange between the vasculature and the interstitium, of course, with correspondingly weaker paracellular exchange compared to the systemic microcirculation. 45 Moreover, the tight arrangement of pulmonary ECs also means that various mediators, toxins, and pathogens often cause damage to the pulmonary vascular barrier function. 46 Therefore, the importance of protecting or restoring the endothelial barrier function of the pulmonary microcirculation in acute and chronic diseases is often greater than that of the systemic microcirculation, as it is a highly relevant and urgent clinical need of critically ill patients. 47 Interestingly, the lung is uniquely composed of two circulations: systemic circulation and pulmonary circulation. 48 The systemic circulation supplies oxygenated blood to the large airways and pleura, while the pulmonary circulation supplies deoxygenated blood to the pulmonary tissue for gas exchange. The different physiological functions of these circulations and the different cell populations in each circulation cause ECs to play unique and different roles. 48 Schupp et al 48 studied multiple species using lung scRNAseq data sets. They discovered two distinguishable capillary EC populations, dividing them into aerocyte ECs participating in gas exchange and common capillary ECs. Unlike all other types of vascular endothelium, aerocytes ECs lack some major components of the Weibel-Palade body, a characteristic of vascular ECs. They also found pulmonary vein ECs in the lung parenchyma, systemic vein ECs in the respiratory tract, and visceral pleura. 48 The result also confirmed the difference and uniqueness of pulmonary and systemic microcirculation, which strongly supports the concept of “double microcirculation.”
Blood Flow Regulation
Due to differences in structure and function, pulmonary and systemic microcirculation also exhibit significant differences in blood flow regulation. Each organ in the systemic microcirculation has unique requirements for blood flow: Due to the relatively distant vertical distances between organs, in order to effectively distribute blood flow to the corresponding vascular network, the systemic vessels not only need a high-pressure gradient but also need to have strong self-regulation ability, thus accurately controlling the vascular resistance to maintain adequate blood pressure and flow. 35 In contrast, pulmonary circulation and microcirculation cannot actively regulate the total blood flow because they need to accommodate the blood volume pumped by the heart. 35 However, it is worth noting that pulmonary microcirculation in adults is more susceptible to the influence of external factors such as CO, body position, gravity, and respiration. 41 At the same time, because the pulmonary tissue is adjacent to it very closely, the pulmonary microcirculation is often affected by specific vascular wall pressure (whether from alveoli or pulmonary tissue), meaning that each segment of the vessel (except for the parts that serve as blood and gas exchange cavities) reacts uniquely to the hemodynamics.35,41 Even more interesting is that the pulmonary vessels uniquely respond to hypoxia. The systemic circulation, including the brain, causes vasodilation in hypoxia, but the pulmonary circulation is the only exception. The pulmonary circulation has a vasoconstrictive response to hypoxia, stimulating pulmonary artery contraction. 49 Although it is currently believed that this response mainly occurs in pulmonary arterioles with a diameter less than 500μm, studies have shown that this response can also be observed in pulmonary microcirculation: The pulmonary microvessels contract markedly due to local low oxygen levels in the alveoli and blood, causing a reduction in local microcirculation blood flow, thereby ensuring adequate blood flow in the oxygenated regions of the microcirculation. 50 In addition, the pressor response caused by acute hypoxia is quickly reversed after improved oxygenation. In contrast, chronic hypoxia stimulation leads to remodeling of pulmonary microcirculation, resulting in increased resistance and pressure. 51
Others
The differences between pulmonary and systemic microcirculation exist in many aspects. For example, pulmonary microcirculation has a unique phenotype and specific molecules distinct from systemic microcirculation. The ECs of both systems have significant differences in cell surface markers and responses to growth factors. Three types of connexin (Cx), Cx37, Cx40, and Cx43, are expressed in pulmonary ECs, while Cx40 is highly expressed in pulmonary ECs and only expressed in small arteries in the systemic circulation. 52 Cxs are often closely related to vascular barrier function: Studies have found that pulmonary microvascular barrier dysfunction after lipopolysaccharide stimulation is closely related to the loss of Cx40. 53 Therefore, the difference in Cx expression between pulmonary and systemic microcirculation also reflects the difference in barrier function. Also, the white blood cells that adhere and migrate in different vascular ECs depend on different adhesion molecules and chemokines, indicating that pulmonary and systemic microcirculation also have differences. 54 At the same time, the degree of response of cell adhesion molecules to pro-inflammatory mediators is significantly different between the vasculature beds of the systemic and pulmonary circulation. For example, Eppihimer et al 55 found that the expression levels of E-selectin and P-selectin in the pulmonary and systemic circulations and their expression changes in response to inflammatory stimulation are completely different. Furthermore, the ECs between pulmonary and systemic microcirculation are also different, and the heterogeneity can lead to selective infections in various organs. For example, the unique expression of CD36 in the brain and skin of the systemic microcirculation can lead to malaria-infected RBCs selectively adhering to these organs rather than the pulmonary microcirculation or other organs. 56
It is necessary to further refine the overall concept of microcirculation because of the significant differences in structure and function between pulmonary and systemic microcirculation. Based on the detailed and systematic theoretical support above, the “double microcirculation” concept is proposed in this review. This concept will promote the systematic typing of microcirculation, improve clinical treatment strategies, and ultimately improve patient outcomes.
Treatment key Points of “Double Microcirculation Protection”
It is well known that interventions aimed at improving macrocirculation have unpredictable effects on microcirculation. However, microcirculation is closely related to critically ill patients’ prognosis. De Backer et al 57 proposed that changes in microcirculatory perfusion, rather than macrocirculation parameters such as mean arterial pressure (MAP) or CO, can predict mortality during a severe infection. Therefore, one suggestion is to use peripheral tissue perfusion assessment indicators such as capillary refill time (CRT), skin mottling score, and skin temperature gradient, representing the overall microcirculation, for risk stratification and managing critically ill patients. 58 Unfortunately, interventions guided by the overall microcirculation have not shown a clear improvement in the prognosis of critically ill patients, for example, the ANDROMEDA-SHOCK study, which found that CRT-guided resuscitation strategies had no advantage in reducing mortality in septic shock patients. 59 One of the important reasons for the negative results may be that assessing the overall microcirculation still needs to be sufficiently detailed and precise. At the same time, based on the concept of “double microcirculation,” it is necessary to further refine clinical treatment perspectives to the level of systemic and pulmonary microcirculation. Therefore, this review summarizes and proposes the treatment key points aimed at protecting systemic and pulmonary microcirculation, which may be of great importance and value for refining the management of critically ill patients and improving their prognosis (Table 2).
Treatment key Points of “Double Microcirculation Protection”.
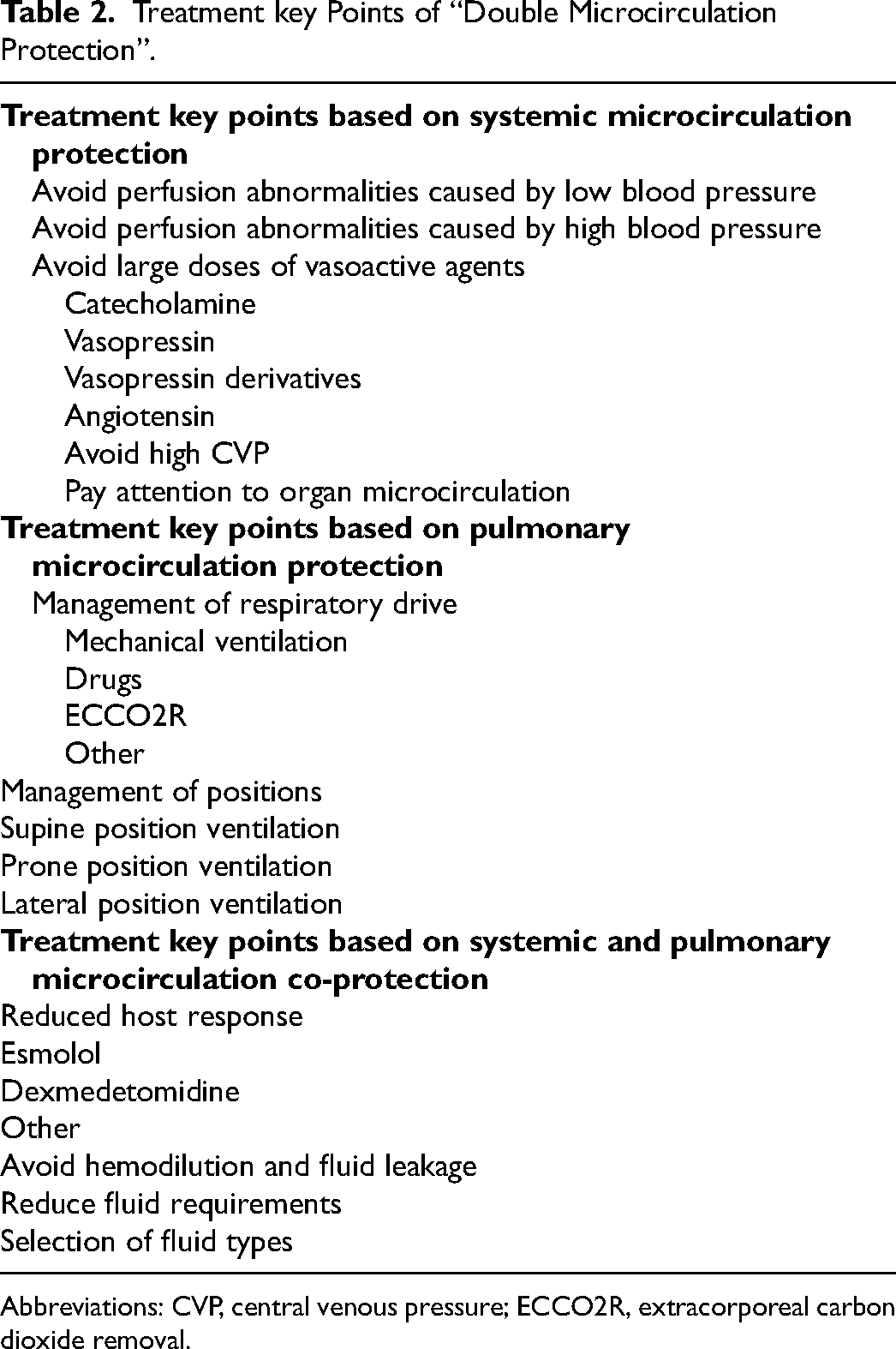
Abbreviations: CVP, central venous pressure; ECCO2R, extracorporeal carbon dioxide removal.
Treatment key Points Mainly Based on Systemic Microcirculation Protection
Avoid Perfusion Abnormalities Caused by Low or High Blood Pressure
Pulmonary microcirculation has a high tolerance to ischemia, so changes in blood pressure to a certain extent have relatively little impact on pulmonary microcirculation. 11 Unlike pulmonary microcirculation, the management of systemic microcirculation should ensure adequate perfusion of all organs, which means that maintaining appropriate blood pressure is often the core requirement of critical care treatment. However, there is currently a lack of high-quality evidence on specific blood pressure targets. 60 Hypotension may cause insufficient systemic microcirculation perfusion, so maintaining appropriate arterial pressure seems necessary. For example, one of the important components of sepsis management is preventing hypotension; the international guidelines for sepsis recommend maintaining MAP > 65mm Hg (higher for elderly and cardiovascular disease patients). 61 The findings of Maheshwari et al 62 support this recommendation, as they found that a decrease in MAP in septic patients was associated with an increased risk of in-hospital mortality and renal injury. Acute myocardial infarction patients should also avoid excessively low blood pressure, and international guidelines recommend the use of positive inotropic drugs and vasoactive agents to maintain circulatory perfusion and protect organ function (although no specific hemodynamic targets are mentioned). 63 Ameloot et al 64 demonstrated in patients with acute myocardial infarction who experienced cardiac arrest followed by shock that, compared with MAP > 65mm Hg, maintaining MAP between 80 and 100mm Hg in the first 36 h after ICU admission was associated with lower high sensitivity cardiac troponin T, suggesting that raising MAP would improve microcirculation and reduce myocardial injury. Avoiding excessively low blood pressure may be beneficial for improving systemic microcirculation. A prospective study including 13 septic shock patients found that maintaining MAP ≥ 65mm Hg improved microvascular function and was associated with a lower lactate concentration; unfortunately, there was considerable variability in microvascular responses among patients, which may have affected the conclusions of this study to some extent. 65
It is easy to understand why avoiding excessively low blood pressure is important, but whether raising blood pressure can be beneficial is still controversial. For example, raising MAP also increases left ventricular afterload, which may impair cardiac function and reduce CO. 66 Moreover, the positive inotropic drugs and vasoactive agents used to raise MAP theoretically increase afterload, heart rate, and contractile work, leading to an increase in myocardial oxygen consumption. 67 The comparison between hypertension and hypotension is also controversial in clinical trials, with most trials not reaching consistent conclusions.68,69 The impact of high blood pressure on systemic microcirculation is also controversial; for example, previous studies have found that raising MAP to 85mm Hg does not significantly improve overall oxygen metabolism and skin microcirculation blood flow.70,71 Dubin et al 72 also found that raising MAP from 65 to 85mm Hg could not improve the severe changes in sublingual microcirculation in septic shock patients, which even caused a decrease in capillary perfusion density, suggesting that unquestioningly increasing blood pressure was not an appropriate way to improve microcirculation perfusion, and might even be harmful to some patients. It is uncertain whether different blood pressure targets can benefit selected patient populations; one reason may be the heterogeneity of microcirculation conditions. Therefore, effectively evaluating the microcirculation of patients and carrying out guided, accurate management of blood pressure is still a huge challenge in critical care treatment.
Avoid Large Doses of Vasoactive Agents
To prevent microcirculatory hypoperfusion due to hypotension, vasoactive agents are often used in critical care treatment. 73 While these drugs are crucial for life-saving interventions in certain scenarios, it is undeniable that they may concomitantly reduce blood flow to systemic microvessels and cause various adverse effects. 74 For instance, as the dose of vasoactive agents increases, it is correlated with a heightened incidence of atrial fibrillation. 75 Regrettably, clinicians frequently underestimate these potential risks. 76 Current clinical guidelines recommend norepinephrine (NE) as the first-line vasoactive agent for the management of septic shock. 77 NE is an α1 and β1 receptor agonist, enhancing vascular tone and myocardial contractility. It appropriately addresses hypotension resulting from reduced venous return, myocardial dysfunction, and decreased vascular tone. 78 However, merely increasing the dosage of NE is neither a safe nor effective strategy. Studies have demonstrated that NE does not improve microcirculatory perfusion in the cerebral cortex and kidneys.79,80 Furthermore, in the management of patients with critical illness and metabolic acidosis, the administration of a single large dose of NE is ineffective in improving patient prognosis. 81 Additionally, large doses of NE may be harmful; studies indicated that NE doses higher than 1.0 µg/kg/min are strongly associated with a mortality exceeding 80%. 82 Large doses of NE may damage the macrocirculation, significantly reduce CO, and increase arterial stiffness. 83 Concurrently, NE may induce constriction of microvessels, resulting in abnormal microcirculatory perfusion, thereby exacerbating organ dysfunction and ischemia, ultimately leading to the deterioration of patient conditions. 84 Poterman et al 85 reported that NE impaired peripheral tissue perfusion and oxygenation in anesthetized patients. Similarly, Kindermans et al 83 showed that NE may reduce tissue perfusion.
In addition, although pulmonary microcirculation is rarely considered when adjusting the blood pressure target, this should not ignore the effect of vasoactive agents on it. For example, high doses of catecholamines may cause decreased oxygenation by altering pulmonary microcirculation perfusion. 86 Attention should also be paid to the different effects of vasoactive agent types on pulmonary microcirculation. Several studies have confirmed that angiotensin II may improve the oxygenation of patients based on mechanisms such as adjusting pulmonary microcirculation blood flow distribution or producing anti-inflammatory effects.87-91 In addition, the unique characteristic of hypoxic pulmonary vasoconstriction may result in different responses of pulmonary microcirculation to vasoactive agents under different oxygenation conditions. For example, under normal oxygen conditions, pulmonary microcirculation is more sensitive to angiotensin II than systemic microcirculation 92 ; however, hypoxia modifies the intrapulmonary effects of angiotensin II, as first reported by Cargill et al, 93 alveolar hypoxemia attenuates the pulmonary vasoconstriction effects of angiotensin II. Due to the current difficulty in adjusting vasoactive agents usage through timely and effective pulmonary microcirculation assessment, this section is not the focus of this review.
The potential adverse effects of administering large doses of single catecholamines on systemic microcirculation are well-documented. One proposed solution is to minimize the dosage of vasoactive agents to the greatest extent feasible. While acute severe hypotension in critically ill patients is strongly associated with poor prognosis, this does not mean that vasoactive agents must be used to normalize blood pressure. Implementing permissible hypotension strategies, predicated on ensuring adequate microcirculatory perfusion and appropriate restriction of vasoactive agents, is of significant value. 3 An alternative approach involves combining catecholamine with non-catecholamine vasoactive agents, thereby minimizing the continuous administration of a single high-dose vasoactive agent. Vasopressin derivatives and angiotensin are commonly used non-catecholamine vasoactive agents, exhibiting effects comparable to those of NE, which can significantly reduce the requirement for NE and aid in maintaining blood pressure.94,95 While this reduction in NE dosage may not necessarily lower 28-day mortality, it can potentially decrease the risk of certain complications.95,96 Consider the use of pituitrin: Although the combination of NE with pituitrin has no significant advantage over NE alone in decreasing mortality, organ dysfunction, or the incidence of serious adverse events, it may reduce the need for renal replacement therapy in patients with acute kidney injury (AKI).96,97 Furthermore, the combination of NE and pituitrin has been shown to lower the risk of atrial fibrillation induced by NE alone, potentially contributing to a reduction in mortality. 98 It is important to note, however, that non-catecholamine vasoactive agents have been associated with adverse effects such as digital necrosis and visceral ischemia. 99 Therefore, it is necessary to choose whether to apply non-catecholamines more carefully and find an appropriate balance between catecholamines and non-catecholamines. 100
Avoid High Central Venous Pressure (CVP)
CVP influences the driving force of systemic circulation, defined as the difference between mean systemic filling pressure and CVP, and impacts the perfusion pressure and flow of systemic microcirculation, which serves as the endpoint of venous return. 101 In a study conducted in 2013, Vellinga et al 102 explored the relationship between CVP and systemic microcirculation in sepsis patients. Their findings indicated that compared with CVP ≤ 12mm Hg, CVP > 12mm Hg was associated with a significant reduction in the microvascular flow index (MFI) and the proportion of perfused small vessels; CVP > 12mm Hg was identified as the only significant predictor of a microvascular MFI < 2.6. This finding suggests that high CVP may play a crucial role in the dysfunction of systemic microcirculation. The impact of high CVP on systemic microcirculation is further evidenced by its influence on the perfusion and function of various organs. Wang et al 103 demonstrated that maintaining a continuous CVP > 8mm Hg in sepsis patients was associated with increased levels of total bilirubin, lactate, and Sequential Organ Failure Assessment scores, as well as a decreased oxygenation index, compared to CVP < 8mm Hg. The findings indicate that high CVP significantly impacts the perfusion and function of the liver, kidneys, and lungs. The effect of high CVP alone on pulmonary microcirculation may be relatively insignificant, but there may be a pathological mechanism of volume overload behind it, which leads to increased leakage of pulmonary microcirculation and affects lung function. The content of fluid leakage is described in detail below.
In addition, it is well known that early right ventricular diastolic dysfunction is a critical factor contributing to postoperative increases in creatinine levels and AKI. However, it is noteworthy that the primary mechanism underlying this phenomenon is excessively high CVP rather than inadequate CO, as previously widely believed. 104 The influence of high CVP on systemic microcirculation ultimately affects patient prognosis. Xiao et al 105 recently confirmed that high CVP not only significantly increased the risk of AKI in septic shock patients but also worsened the prognosis. Therefore, under the principle of systemic microcirculation protection, minimizing high CVP whenever feasible is imperative. In clinical practice, once adequate tissue perfusion is achieved, it is crucial to avoid unnecessary high CVP. Efforts should be directed towards identifying and maintaining the lowest and most appropriate CVP as much as possible and minimizing the duration of high CVP. This approach aims to reduce venous return resistance, enhance organ microcirculation, and improve patient prognosis. 3
The Budding of Organ Microcirculation
The progression of theoretical concepts can occasionally surpass the advancements in technology and equipment. Limited by the level of technology and equipment, the evaluation and monitoring of systemic microcirculation in clinical practice still need to be improved. Nevertheless, the theoretical framework of systemic microcirculation has shown a trend of organ microcirculation. Significant attention has been directed towards the issues related to organ dysfunction and compromised microcirculation in critically ill patients. Impaired microcirculation results in hypoxemia and functional deterioration of organs and is correlated with increased mortality.12,57 Simultaneously, advancements in theoretical understanding have prompted further research into the microcirculation of specific organs. Cerebral microcirculation exhibits a distinctive ultrastructure, establishing a close relationship between the microvessels and the corresponding neurons. 106 Given that the total cross-sectional area of cerebral micro-arteries significantly exceeds that of the major arteries, increased cerebral vascular resistance resulting from cerebral vasoconstriction and microvascular thrombosis can impact local cerebral microcirculation and frequently exacerbate neurological outcomes.107,108 Furthermore, early recirculation therapy can improve certain aspects of cerebral microcirculation perfusion but may not fully restore all microcirculatory pathways. This incomplete restoration, the no-reflow phenomenon, is closely associated with poor patient prognosis.109,110 Renal microvascular dysfunction and hypoxia frequently result in AKI. For instance, hemorrhagic shock can lead to reduced renal perfusion, manifesting as decreased blood flow in both the renal cortex and medulla.111,112 Evidence indicates that hemodynamic alterations in renal microcirculation occur in sepsis-induced AKI, characterized by microvascular constriction and hypoperfusion, which contribute to both direct and indirect renal damage. 113 Critical illnesses instances of sepsis frequently coincide with hepatic dysfunction and are correlated with increased mortality. 114 The pathophysiological mechanisms underlying liver failure are poorly understood; however, disruptions in hepatic microcirculation, rather than macrocirculation, and resultant hypoperfusion may play a critical role. 115 For instance, Wu et al 116 utilized laser speckle contrast imaging to demonstrate that hepatic microcirculatory dysfunction emerged 12 h after sepsis and progressively deteriorated. This dysfunction was attributed to interactions between neutrophils and ECs, microthrombosis, and vascular leakage. Furthermore, dysfunction of the intestinal microcirculation is a critical determinant of mortality in critically ill patients, which should not be ignored. 117 Several factors influence the sensitivity and distinctiveness of the intestinal microcirculation. Initially, the parallel arrangement of arteries and veins within the intestinal villi creates a unique anatomical structure that reduces oxygenation in the proximal lumen area of the intestine and is susceptible to microcirculatory perfusion. 118 Consequently, impaired intestinal microcirculation can readily impair the barrier function, facilitating the translocation of intestinal bacteria to other organs.119,120 Concurrently, the gut microbiota and endotoxins may independently induce intestinal mucosal barrier dysfunction, further impacting intestinal microcirculation.121,122 Therefore, based on the close relationship between organ function and organ microcirculation, as well as the unique characteristics of organ microcirculation, it is not difficult to see that further subdivision of systemic microcirculation according to organ-specific orientation is a valuable way, and the budding of organ microcirculation is born (Figure 1).
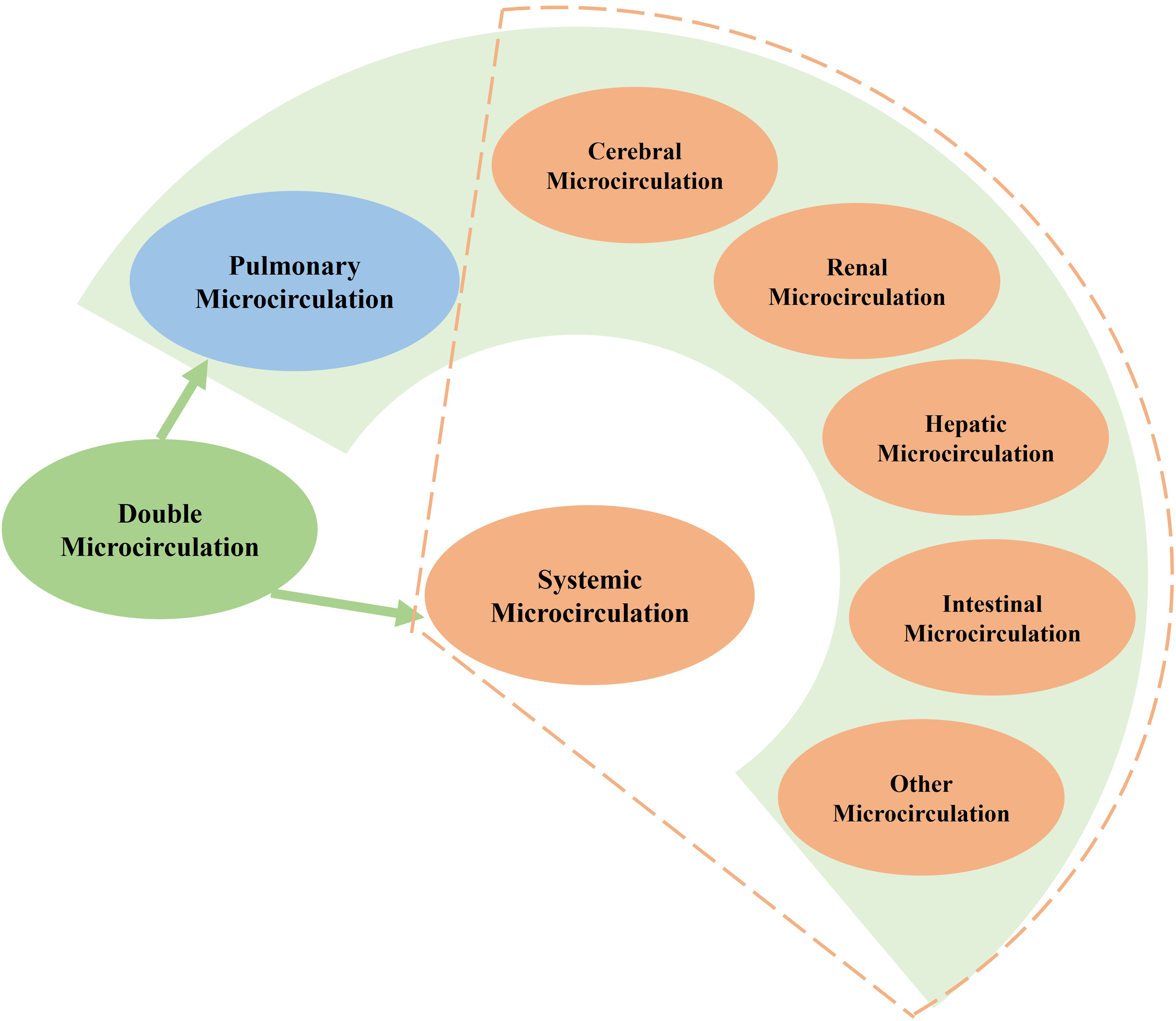
Double microcirculation refers to the pulmonary microcirculation and systemic microcirculation, and systemic microcirculation can be further subdivided into cerebral microcirculation, renal microcirculation, hepatic microcirculation, intestinal microcirculation, and other organ microcirculation according to the different characteristics of each organ.
Treatment key Points Mainly Based on Pulmonary Microcirculation Protection
Management of Respiratory Drive
The impact of respiratory drive on pulmonary microcirculation is huge, so paying attention to and strengthening the management of respiratory drive from the perspective of pulmonary microcirculation protection is necessary. The optimal target and safe upper limit of respiratory drive may vary from patient to patient, depending on factors such as the severity of lung injury, diaphragm injury, and the level of the host response.24,123 However, targeting the physiological level of the respiratory drive may reduce the lung and diaphragm injury caused by the abnormal respiratory drive and even improve the prognosis of critically ill patients. Mechanical ventilation is one of the commonly used ways to manage respiratory drive in clinical practice, which can directly affect the main determinants of respiratory drive, such as PaO2, PaCO2, and the mechanical deformation of the lung and chest wall, through unique ways, such as changing the level of PEEP. 124 Increasing inspiratory support reduces respiratory motivation but has a much smaller effect on respiratory rate.125,126 It is worth noting that if respiratory drive abnormalities are caused by factors such as stress, pain, and chest or nervous system disorders, mechanical ventilation alone may not be effective, and medication or other methods should be considered for management. Some drugs can manage respiratory drive by regulating the input signals of the respiratory or even directly affecting the respiratory center. 127 It is important to note the different effects of several commonly used drugs: Remifentanil, an opioid, which mainly affects respiratory frequency; Propofol and benzodiazepine drugs, which tend to affect respiratory amplitude; Neuromuscular blockers, which do not directly control respiratory drive, can reduce the mechanical work of respiratory muscles.128-130 However, the adverse effects of these drugs should not be ignored, and their long-term use should be minimized and closely monitored. In addition, the emerging extracorporeal carbon dioxide removal (ECCO2R), which reduces the level of ventilation by reducing the amount of carbon dioxide removed through the lung, is not only suitable for lung protective ventilation in patients with low tidal volume induced hypoxia failure and respiratory acidosis but has also been shown to reduce respiratory drive in patients with ARDS and acute exacerbation of chronic obstructive pulmonary disease. 131 Of course, ECCO2R does not change the level of neural drive in the brain, and its safety still requires further validation.
Management of Positions
The distribution of blood flow in the lungs of critically ill patients is affected by various factors such as position, gravity, mechanical ventilation, and local lung injury. Of these, the change in position has a particularly significant impact on adult pulmonary microcirculation. 35 The effects of position on pulmonary microcirculation are not fully understood. However, existing research results suggest that position may have a significant impact on the clinical treatment of critically ill patients, especially those with ARDS.132,133 Long-term supine position ventilation injuries pulmonary microcirculation, causing alveolar collapse in gravity-dependent areas, compression atelectasis, and pulmonary edema, thereby worsening hypoxemia. 134 In contrast, prone position ventilation (PPV) can change the gradient of thoracic pressure and improve the abnormal distribution of pulmonary lesions, facilitating the drainage of secretions from collapsed alveoli and improving blood perfusion, thereby greatly promoting alveolar reexpansion and achieving significant improvement in lung ventilation. 135 A recent meta-analysis by Liao et al 136 confirms that PPV can significantly improve the oxygenation index, reduce mechanical ventilation duration, shorten the ICU stay, and even reduce in-hospital mortality. Early and long-term use of PPV protects pulmonary microcirculation and improves lung ventilation, which will be a key factor in improving the prognosis of critically ill patients. In addition, some studies have explored the effects of lateral positioning on pulmonary microcirculation blood flow. For example, Wieslander et al 137 used magnetic resonance imaging technology to evaluate the pulmonary artery and vein blood flow of 10 healthy subjects in the lateral position. The study found that compared to the supine position, the blood flow to the gravity-dependent area in the lateral position increased by about 25%, and the vessels of the non-gravity-dependent area were significantly expanded. Furthermore, the study suggests that the mechanism of improving lung ventilation by lateral positioning is similar to that of PPV: the healthy side lung tissue bears the main pressure, and the pressure on the affected side is greatly reduced, thereby improving the uneven distribution of pulmonary lesions, redistributing the pulmonary blood flow to the gravity-dependent area, correcting the pulmonary ventilation/perfusion ratio, increasing the oxygenation index, and the infection is controlled.
Treatment key Points Based on Systemic and Pulmonary Microcirculation co-Protection
Reduced Host Response
The host response is often caused by infection, tissue injury, and others through pathogen-associated molecular patterns and damage-associated molecular patterns pathways acting on pattern recognition receptors, triggering a wide range of interconnected but different immune, inflammatory, coagulation, and neuroendocrine responses in multiple systems.138,139 The concept of the host response was first proposed in the 2016 international guidelines for sepsis and has since received widespread attention during the coronavirus disease 2019 pandemic before being further elaborated in a review by Arina et al in 2021.138,140,141 The host response has a significant impact on systemic and pulmonary microcirculation. For example, when the host response is enhanced, the sympathetic nervous system is activated, leading to arrhythmia or impaired contractile function in the heart, the main target of sympathetic nerve stimulation, which reduces CO and ultimately causes reduced blood flow and impaired perfusion in the systemic and pulmonary microcirculation.142,143 Furthermore, the autonomic nervous system (ANS) plays an important role in regulating inflammatory responses and maintaining host homeostasis. In contrast, the dysregulated host response often leads to ANS disorders, which directly cause myocardial injury, endothelial injury, microvascular thrombosis, and other adverse reactions, resulting in microcirculation dysfunction. 144 Therefore, managing the host response may also be an important part of double microcirculation protection. In clinical practice, the host response can be managed by controlling the sympathetic nerve and regulating ANS. For example, Morelli et al 145 demonstrated that esmolol effectively controls heart rate and reduces ineffective cardiac work while ensuring CO, thereby improving double microcirculation perfusion and even improving the prognosis of critically ill patients. 145 Similarly, dexmedetomidine can also significantly reduce the impact of the host response on the ANS, thereby improving cardiac function, increasing vascular tension, enhancing the effect of NE pressor and reducing its dosage, and ultimately playing a role in stabilizing the hemodynamics of macrocirculation and double microcirculation. 146
Avoid Hemodilution and Fluid Leakage
The current understanding of fluid administration has entered an era characterized by efficacy selection; that is, the fluid should be regarded as a drug possessing both therapeutic benefits and potential adverse effects. 147 Notably, the negative impact of hemodilution on systemic and pulmonary microcirculation cannot be overlooked. 148 Hemodilution naturally lowers the hematocrit level, which may reduce the oxygen-carrying capacity of the blood and subsequently impair the delivery of oxygen to tissues. Although compensation can be achieved by increasing CO and enhancing tissue oxygen uptake efficiency, this compensatory mechanism is extremely constrained in cases of severe hemodilution. 149 Hemodilution adversely impacts organ microcirculation, leading to organ dysfunction. For instance, studies have demonstrated that the hematocrit level below 20% due to hemodilution is strongly associated with cerebral damage. 150 Additionally, hemodilution can induce heterogeneity in renal microcirculatory perfusion, exacerbating hypoxia in both the renal cortex and medulla. 151 Furthermore, the intestinal microcirculation necessitates a slightly elevated hematocrit compared to the normal range. Consequently, severe hemodilution can easily lead to intestinal ischemia and compromise the integrity of the intestinal barrier.152,153 Additionally, hemodilution may result in a reduced proportion of perfused small vessels, a decline in hemoglobin concentration, and even tissue edema. These changes collectively increase the diffusion distance for oxygen within the microvessels, thereby reducing gas exchange efficiency. 154 Therefore, it is easy to see that hemodilution significantly impacts both systemic and pulmonary microcirculation.
Fluid therapy, or hemodilution, induces cytokine activation and impairs the microcirculatory endothelial glycocalyx. 147 Furthermore, hemodilution reduces coagulation factors and anticoagulant proteins, which results in endothelial activation and coagulation dysfunction, ultimately contributing to endothelium-dependent thrombosis and inflammatory responses.155,156 These processes collectively lead to injury of ECs in the systemic and pulmonary microcirculation, compromise barrier function, and cause leakage of intravascular fluid, resulting in edema within the extravascular tissue space. The impact of fluid leakage on systemic and pulmonary microcirculation is significant and detrimental. For example, substantial fluid leakage in the pulmonary microcirculation can result in a pronounced increase in EVLW, thereby exacerbating the decline in oxygenation. 157 Similarly, fluid leakage can adversely affect renal microcirculation, leading to conditions such as renal interstitial edema, significantly elevating the likelihood of requiring renal replacement therapy, and may even cause irreversible renal damage. As demonstrated in the study by Messmer et al, 158 the administration of large fluid transfusions in sepsis patients is significantly correlated with an elevated risk of AKI and respiratory failure, which subsequently impacts patient prognosis. Consequently, avoiding excessive hemodilution and fluid leakage benefits systemic and pulmonary microcirculation.
Fluid resuscitation, guided by the principle of systemic and pulmonary microcirculation co-protection, is more suitable for clinical resuscitation objectives and ensures accurate fluid administration to prevent secondary damage to organ microcirculation. For instance, bedside ultrasound can provide a more accurate assessment of pulmonary exudation and renal blood flow, thereby avoiding the risk of organ microcirculation damage due to fluid overload. 159 Chen et al 160 recently provided a systematic demonstration of the substantial value of contrast-enhanced ultrasound in assessing renal microcirculation and guiding hemodynamic therapy. Furthermore, it is essential to consider the critical role of fluid type in managing hemodilution and fluid leakage in critically ill patients. International guidelines recommend crystalloid, particularly balanced salt solutions, as the preferred resuscitation fluids for sepsis patients. 161 However, the adverse effects associated with the extensive administration of crystalloid, including hemodilution, endothelial damage, and increased vascular permeability, cannot be ignored. 162 Conversely, albumin and fresh frozen plasma (FFP) have demonstrated the potential to reduce fluid requirements, repair endothelial glycocalyx, and enhance vascular barrier function.163-165 The beneficial impact of albumin and FFP on microcirculation has garnered increasing attention, prompting a gradual shift in clinical practice preferences regarding fluid selection.
Conclusion
The understanding of microcirculation has advanced into a more specific and detailed phase characterized by systemic and pulmonary microcirculation. This review first elucidates the profound impact of critical diseases on systemic and pulmonary microcirculation, highlighting the crucial role in the pathogenesis of critical illnesses. Subsequently, it establishes a systematic theoretical framework for “double microcirculation” by elaborating on the differences in structure, function, blood flow regulation, and others between systemic and pulmonary microcirculation from several important perspectives. Finally, based on this novel concept, we propose treatment key points to protect double microcirculation to enhance management practices for critically ill patients and potentially improve their prognoses. Additionally, this review briefly describes the unique characteristics and distinctions of microcirculation across various organs while reasonably concluding that exploring organ microcirculation will emerge as a significant research direction within critical care.
Footnotes
Abbreviations
Acknowledgements
Not applicable.
Authors’ Information
Not applicable.
Author Contributions
Guangjian Wang and Xiaoting Wang conceived the manuscript. Guangjian Wang drew the figure and drafted the manuscript. Hui Lian, Xiaoting Wang, Qingyu Deng, Jie Wang, and Qian Zhang revised the manuscript together. Hui Lian and Xiaoting Wang co-directed and reviewed the final manuscript. All authors read and approved the final manuscript.
Availability of Data and Material
Not applicable.
Consent for Publication
Not applicable.
CRediT Authorship Contribution Statement
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National High Level Hospital Clinical Research Funding (2022-PUMCH-B-026). Beijing natural Science Foundation (7232126).