
Abstract
Background
For some liver transplant recipients, elevated lactate after transplantation is associated with early allograft dysfunction (EAD). Determining which patients with elevated lactate will develop EAD is a challenge because lactate can accumulate due to increased production, decreased hepatic clearance, or both. Intravenous fluid administration may be beneficial for patients with elevated lactate who have insufficient intravenous circulating vascular volume, or it may result in vascular volume overload and allograft injury from congestion for patients who have adequate perfusion and no signs of shock. We hypothesized that in absence of other signs of shock, intravenous fluid administration would not be associated with improved graft function for patients with elevated post-transplant lactate.
Methods
We performed a single-center cohort study of living donor liver transplant recipients between March 2009-June 2018 (n = 197). We categorized the study population based on the highest lactate in the first 6 h of the post-transplant ICU stay (Group 1: < 3 mmol/L; Group 2: 3-6 mmol/L and Group 3: > 6 mmol/L). Our primary exposure was post-transplant ICU intravenous fluid administration and primary outcome was EAD.
Results
Sixty- four (32.5%) patients developed EAD: 24 (26.7%) in Group 1, 21 (29.6%) in Group 2 and 19 (52.8%) in Group 3. Within group 2, there was no difference between EAD and non-EAD patients in baseline characteristics, vasopressor use at two hours, or urine output. In a linear mixed model in Group 2 patients, there was a significant difference in the mean fluid intake during the first 36 h of ICU stay for those who developed EAD compared to those who did not (EAD: 826 ± 56 ml vs non-EAD: 680 ± 39 ml respectively, p = 0.03).
Conclusion
Our results show that elevated lactate after liver transplant is frequently caused by decreased lactate clearance. Following liver transplantation, intensivists should interpret elevated lactate levels in clinical context before administering intravenous fluids.
Background
In some liver transplant recipients, elevated lactate after transplantation is associated with early allograft dysfunction (EAD), primary graft non-function (PNF), and increased mortality.1-4 Following transplant, lactate usually peaks at reperfusion with a gradual decline to normal over the next several hours. 1 Intensive care providers may interpret persistently elevated post-liver transplant lactate levels as markers of tissue hypoperfusion and subsequently administer intravenous fluids to increase cardiac output. Unfortunately, elevated postoperative lactate may also be a marker of delayed graft function rather than systemic hypoperfusion,1,3,5-7 particularly in the setting of graft size mismatch.2,8,9 Understanding how to interpret elevated lactate levels after transplant therefore has high clinical relevance, as treatment with intravenous fluids will be beneficial or detrimental depending on the underlying reason. We hypothesized that in the absence of signs of hemodynamic compromise, intravenous fluid resuscitation would not be associated with improved graft function for patients with elevated lactate levels following liver transplantation.
Methods
Study Design and Population
The study was approved by the University of Pittsburgh human subjects review board under approval number STUDY19080302 (formerly PRO13060220). We performed a single-center cohort study using a clinical registry of adult living donor liver transplant (LDLT) recipients at UPMC between March 2009 and June 2018. Follow-up data was available for all patients through April 2020. We adhered with the STROBE reporting guidelines.
Data Collection
We used separate inpatient and outpatient electronic medical records (EMR) to collect relevant clinical information. Using the outpatient EMR we obtained donor and recipient demographics, laboratory values, vasopressor use, postoperative complications, re-operation, transplant variables, survival, and follow-up after transplant. Using the inpatient EMR we obtained a record of fluid input and output following the transplant, laboratory values at the time of operation, and immediate postoperative laboratory values to calculate the model for end-stage liver disease score (MELD) scores.
Our primary outcome measure was EAD, which we defined as the presence of one or more of the following variables: (i) serum bilirubin ≥10 mg/dL on postoperative day 7, (ii) an international normalized ratio ≥1.6 on postoperative day 7; (iii) an alanine or aspartate aminotransferase of >2000 IU/L within the first 7 postoperative days. 10 We defined primary graft nonfunction as irreversible failure of graft requiring re-transplantation or patient death with in 7 days after the transplant.
We defined three categories of early post-operative lactate (low, intermediate, and high) to evaluate the association between lactate level, fluid administration, and graft function in clinically meaningful groups. We used the highest post-transplant lactate value in the first 6 h of the intensive care unit stay: group 1: Lactate < 3 mmol/L; group 2: Lactate 3–6 mmol/L; and group 3: Lactate >6 mmol/L.
We evaluated the association between EAD and the amount of fluid administered within first 36 h for all three groups.
We defined the start of post-operative period from when patients arrived in the intensive care unit. We included fluid input, fluid output, and vasopressor data in increments of six hours, for the first 36 h of ICU admission. The volume of blood products administered was included in fluid balance. We obtained patient input and output data for crystalloids administered, blood products administered, urine output, ultrafiltrate, use of norepinephrine and vasopressin directly from the electronic medical records. We classified patients as not being on vasopressors post-operatively if all vasopressors were weaned off within the first two hours of arriving in the ICU.
Statistical Methods
We used ANOVA and Chi-Square tests to evaluate baseline characteristics across the groups. We applied savage multi-sample tests for nonparametric data when appropriate. We used linear mixed models to examine trends in mean lactate levels, fluid intake, and output during the first 36-h of the ICU stay, and a Bonferroni correction for multiple comparisons. All tests of statistical significance were two-tailed tests and used an alpha of less than 0.05 for single comparisons and downward adjusted for multiple comparisons.
We hypothesized that in the absence of hypotension, fluid resuscitation would not be associated with improved EAD for patients with elevated lactate levels following liver transplantation. We used SAS version 9.4 (SAS Institute, Cary, NC) and R version 3.6.0 to perform the analyses.
Results
A total of 210 patients underwent LDLT and were admitted to the ICU between March 2009 and June 2018. Thirteen patients could not have their ICU records linked at the time of study and were excluded from the study, resulting in a final cohort of 197 patients.
Baseline Patient Characteristics and Clinical Outcomes of the Whole Cohort
There was a total of 197 patients in the study with a mean age of 56 years, of whom 79 (40.1%) were female. Among the study participants, one hundred and eight seven (96.9%) reported the white race, and 11 (5.6%) patients had a history of prior transplant. Average MELD at the time of transplantation was 16 (12-20), and the median graft weight (GW) to recipient weight (RW) ratio was 1.1 (0.9-1.3). The median highest lactate in the first six hours post-transplant was 3.4 (2.2-5.5) mmol/L. One hundred and forty-six (74.1%)) patients were either never on vasopressor or weaned from vasopressors within the first two hours from time zero. (Table 1)
Baseline Demographics of the Whole Cohort (n = 197).
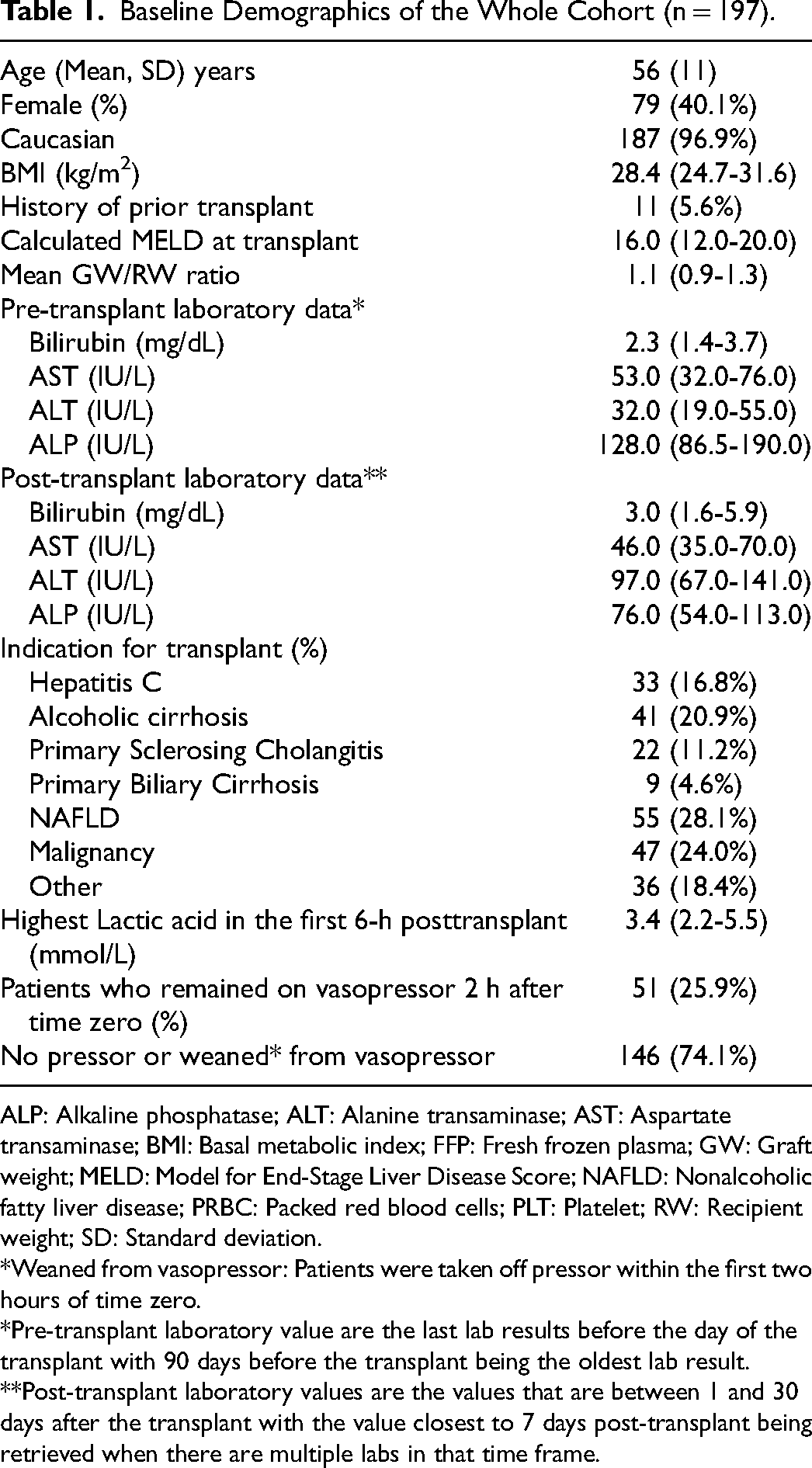
ALP: Alkaline phosphatase; ALT: Alanine transaminase; AST: Aspartate transaminase; BMI: Basal metabolic index; FFP: Fresh frozen plasma; GW: Graft weight; MELD: Model for End-Stage Liver Disease Score; NAFLD: Nonalcoholic fatty liver disease; PRBC: Packed red blood cells; PLT: Platelet; RW: Recipient weight; SD: Standard deviation.
*Weaned from vasopressor: Patients were taken off pressor within the first two hours of time zero.
*Pre-transplant laboratory value are the last lab results before the day of the transplant with 90 days before the transplant being the oldest lab result.
**Post-transplant laboratory values are the values that are between 1 and 30 days after the transplant with the value closest to 7 days post-transplant being retrieved when there are multiple labs in that time frame.
No patients developed primary graft non-function (0%), and 64 (32.5%) developed EAD. 53 (26.9%) patients underwent re-operation in one month, and 30 (15.3%) patients had biliary complications. The median post-transplant hospital length of stay was 11.0 (7.0-22.0) days
Clinical Outcomes of the Whole Cohort (%).
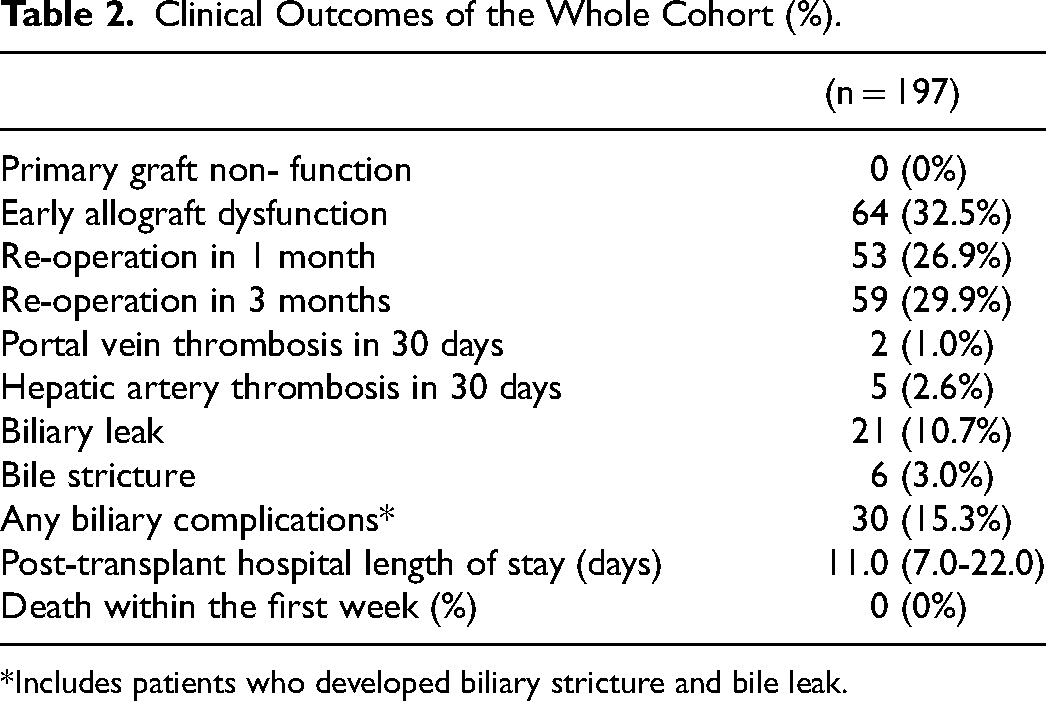
*Includes patients who developed biliary stricture and bile leak.
Patient Characteristics and Fluid Balance in Lactate-Based Groups
Ninety (45.7%) of the patients had a maximum lactate <3 mmol/L, 71 (36%) patients had a maximum lactate between 3–6 mmol/L and 36 (18.3%) patients had a maximum lactate >6 mmol/L. There was no significant difference in the history of prior transplants, MELD at the time of transplant, or median GW/RW ratio between the groups (p-value >0.05
Baseline Demographics of Different Lactate Groups.
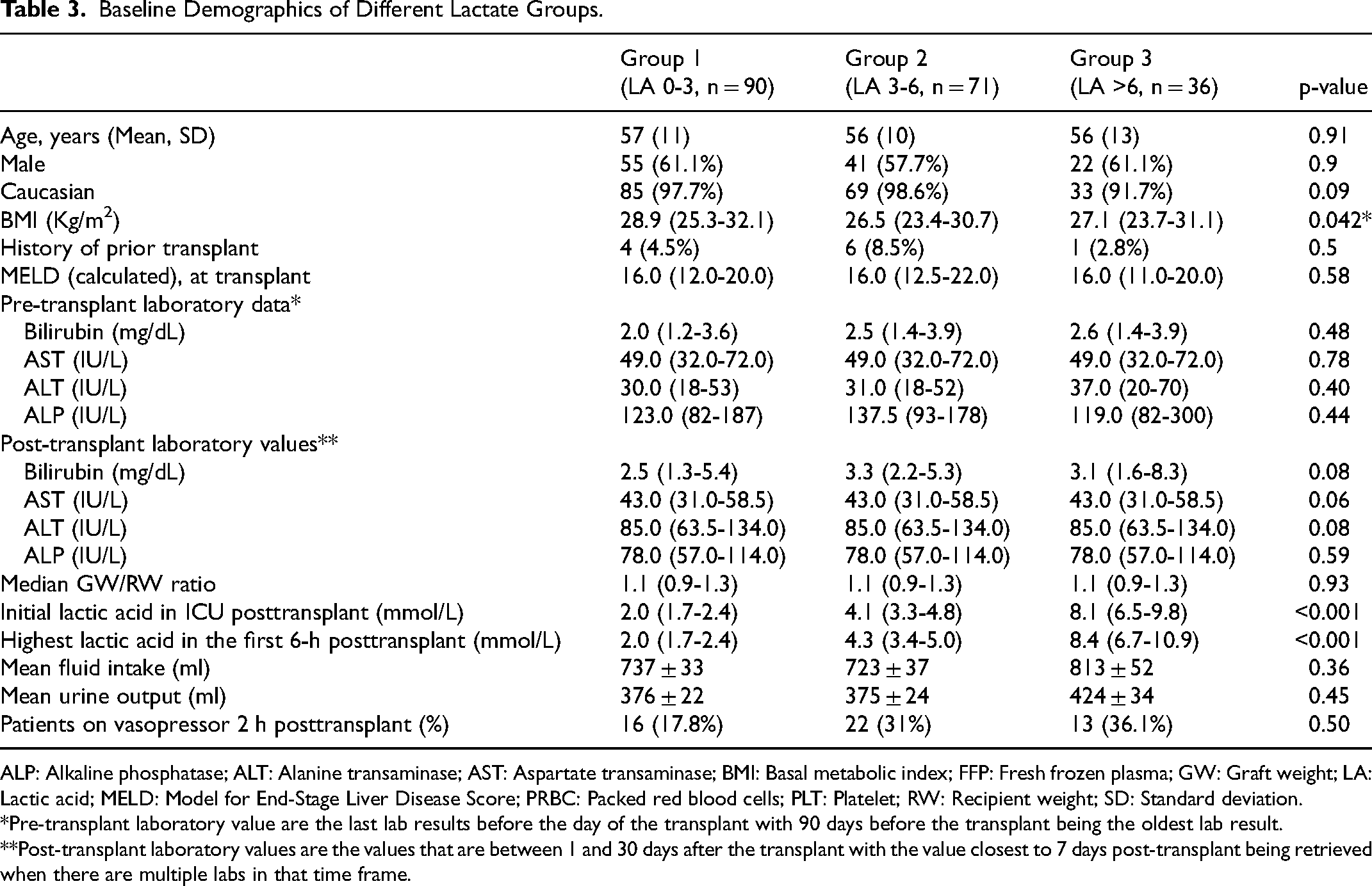
ALP: Alkaline phosphatase; ALT: Alanine transaminase; AST: Aspartate transaminase; BMI: Basal metabolic index; FFP: Fresh frozen plasma; GW: Graft weight; LA: Lactic acid; MELD: Model for End-Stage Liver Disease Score; PRBC: Packed red blood cells; PLT: Platelet; RW: Recipient weight; SD: Standard deviation.
*Pre-transplant laboratory value are the last lab results before the day of the transplant with 90 days before the transplant being the oldest lab result.
**Post-transplant laboratory values are the values that are between 1 and 30 days after the transplant with the value closest to 7 days post-transplant being retrieved when there are multiple labs in that time frame.
In a linear mixed model, mean intravenous fluid volumes administered over 36-h were not significantly different between groups (Group 1:737 ± 33 ml; Group 2:723 ± 37 ml and Group 3:813 ± 52 ml, p = 0.36). (Table 3)
However, Group 3 patients received a higher amount of fluid between the 6- and 12-h mark as compared to the other two groups during the same period (Bonferroni adjusted p-value = 0.03) (Figure 1).
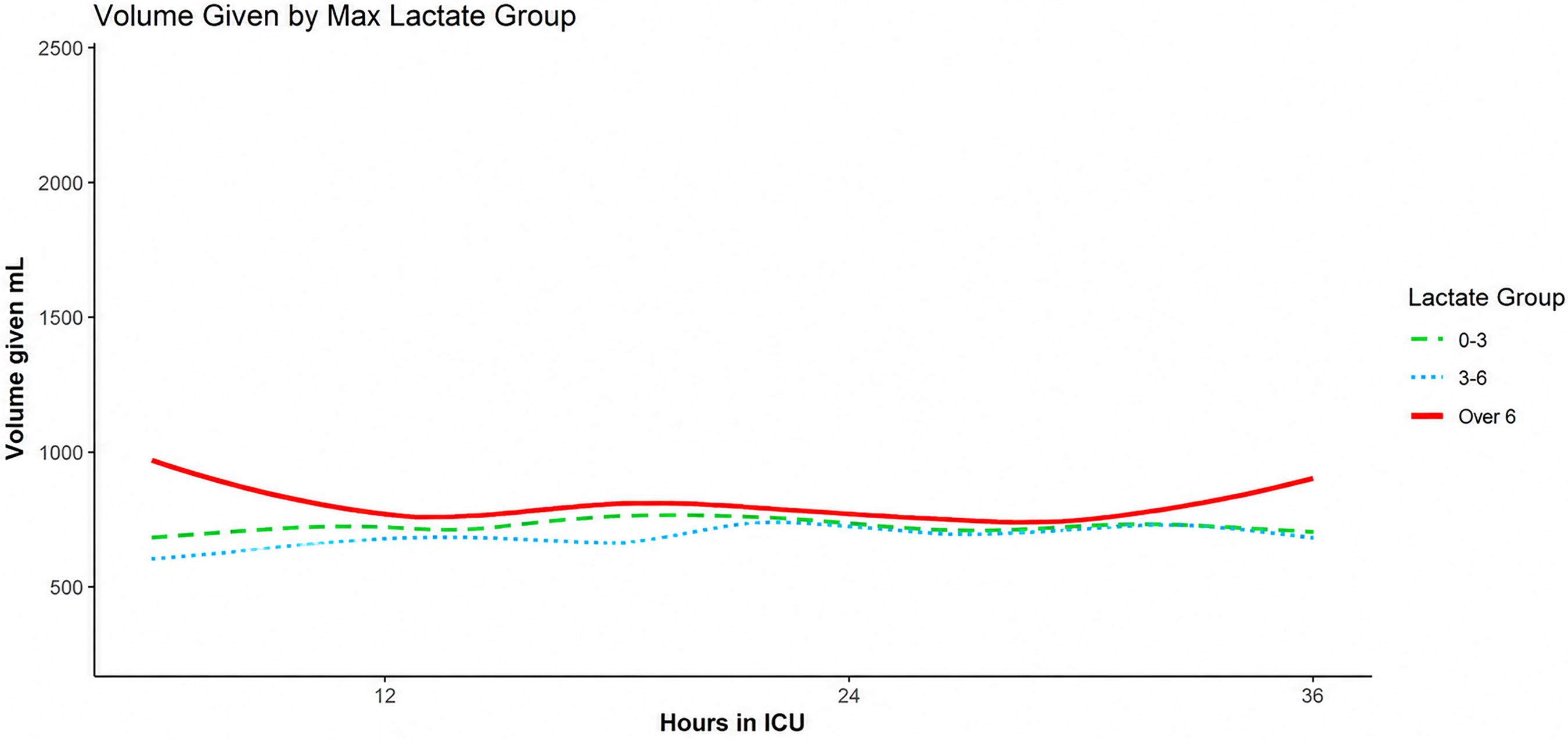
Comparison of fluid intake volume over time between the three lactate-based groups.
The mean overall fluid output was not significantly different between groups over 36 h [Group 1: 376 ml ± 22 ml, Group 2:375 ± 24 ml, and Group 3: 424 ± 34 ml (p = 0.45)]. Group 3 patients had higher urinary output between 6–12-h mark as compared to the other two groups during the same period (Bonferroni adjusted p-value = 0.017) (Figure 2
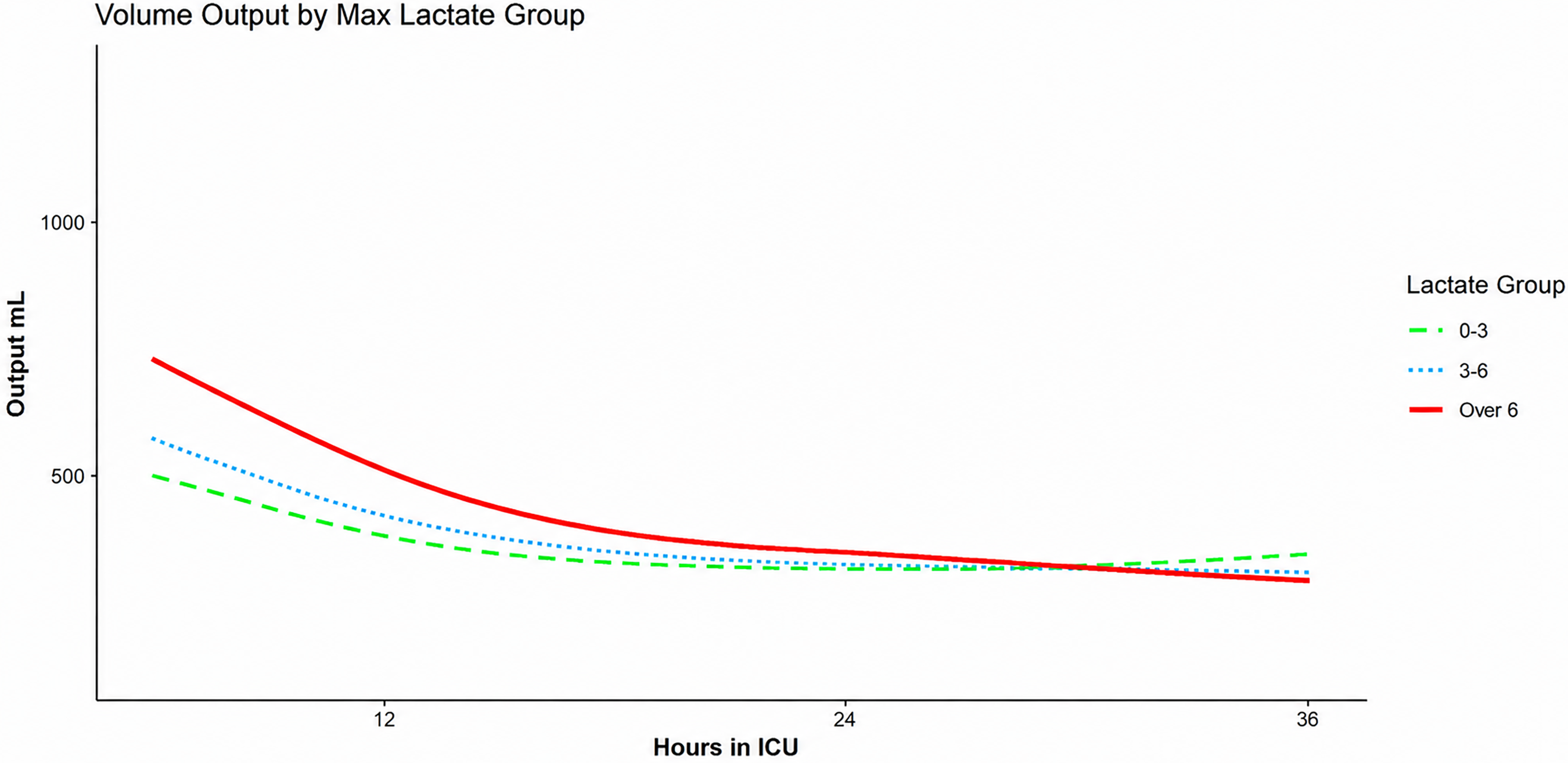
Comparison of urinary output volume over time between the three lactate-based groups.
Clinical Outcomes
The incidence of EAD was more common in Group 3 [19 (52.8%) patients] as compared to Group 1 [24 (26.7%) patients] and Group 2 [ 21 (29.6%) patients, p = 0.015] as was re-operation at 1-month and three months. (Table 4)
Clinical Outcomes of Different Groups.
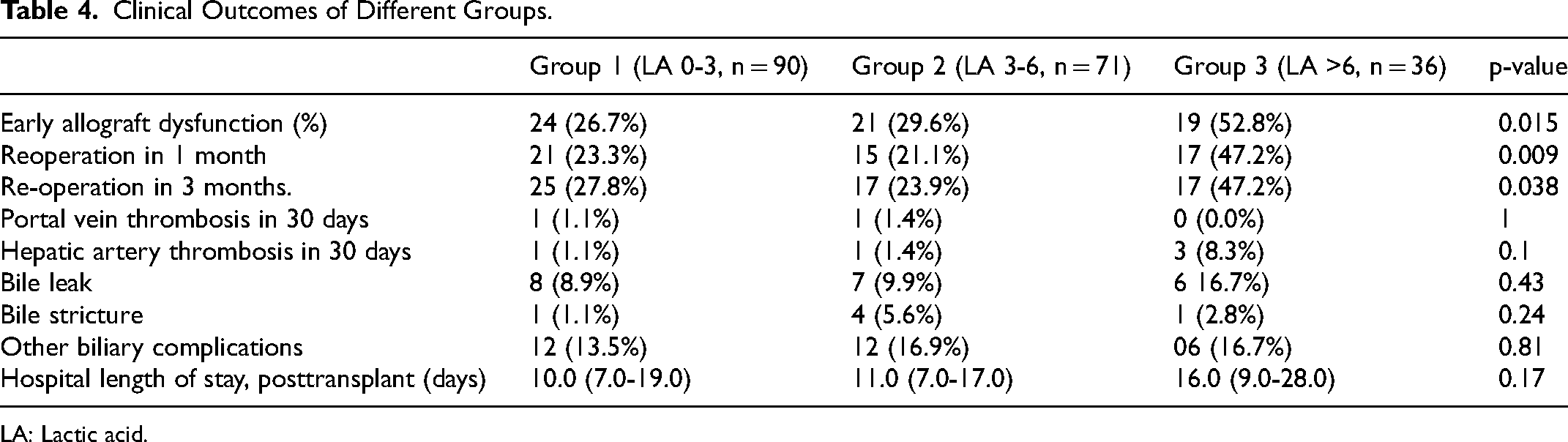
LA: Lactic acid.
There was no significant difference in biliary complications or length of post-transplant hospital stay between the three groups [Length of stay, Group 1: 10.0 (7.0-19.0) days, Group 2: 11.0 (7.0-17.0) days, Group 3: 16.0 (9.0-28.0) days, p = 0.17].
Patient Characteristics and Fluid Balance in Group 2
There were a total of 71 patients in the intermediate lactate group (Lactate: 3-6 mmol/L), out of which 21 (29.6%) had EAD. Comparing EAD to non-EAD patients within this group, there was no difference in baseline characters, including prior transplant [EAD: One (4.8%) patient versus Non-EAD: Five (10.0%) patients], MELD at transplant [EAD: 16.0 (14.0-19.0) versus Non-EAD: 16.0 (11.0-22.0)] or median GW/RW ratio [EAD: 1.0 (0.9-1.1) versus Non-EAD: 1.2 (0.9-1.4)] (p-value for all variable > 0.05) (Supplement Table 1). There was no significant difference in the number of patients on vasopressors after two hours between the two groups. [EAD: Nine (43%) patients versus non-EAD: 13 (26%) patients, p = 0.11].
In a linear mixed model, there was a significant difference in the mean fluid intake during the first 36 h of ICU stay for those who developed EAD compared to those who did not (EAD: 826 ± 56 ml vs Non-EAD: 680 ± 39 ml respectively, p = 0.03) (Figure 3).
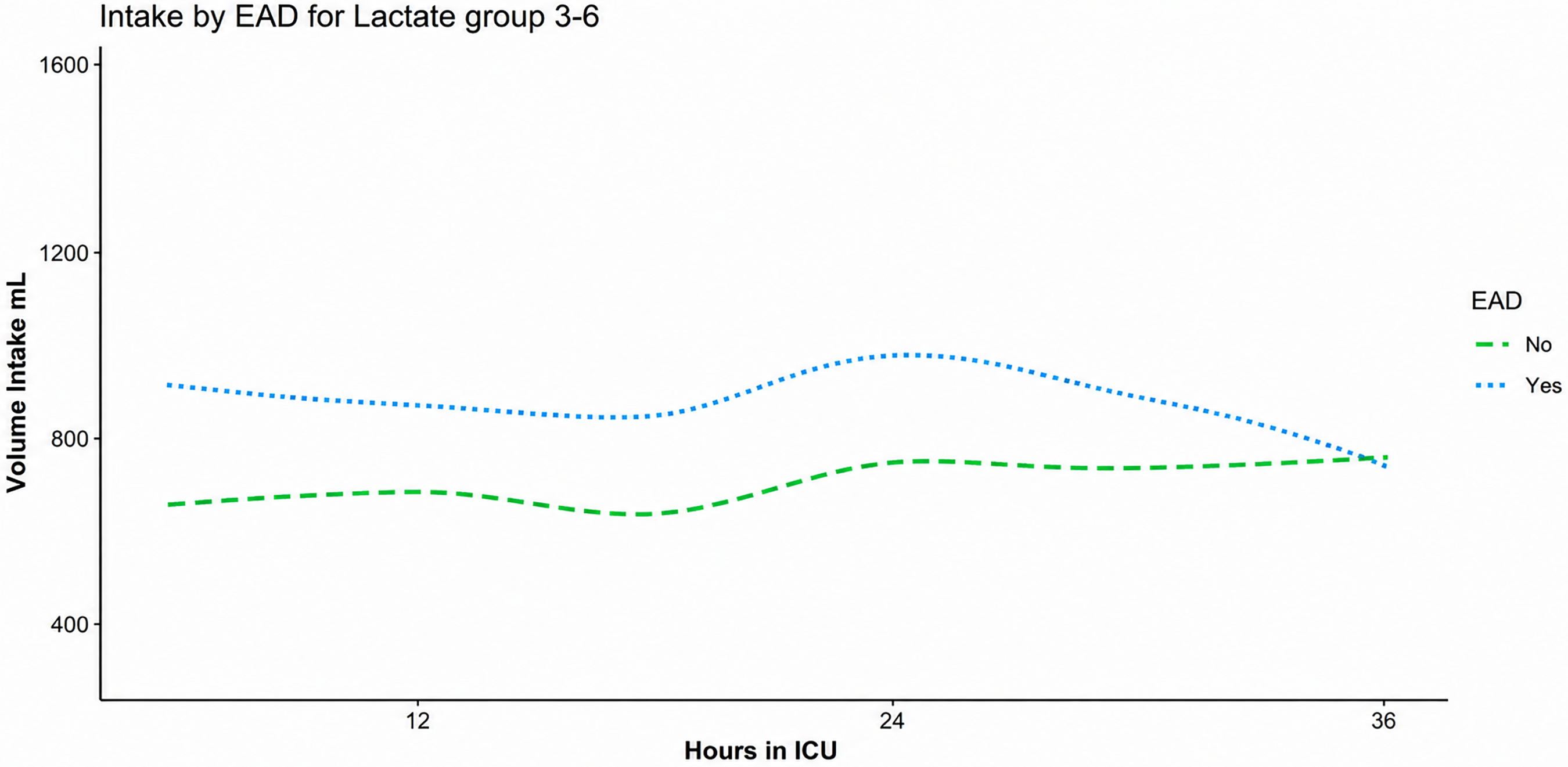
Comparison of fluid intake volume over time between EAD and non-EAD patients in Group 2. EAD: Early allograft dysfunction.
Those in the EAD group received, on average, 146 ml more volume than the Non-EAD group. There was no statistical difference in mean urine output during the ICU period between EAD and non-EAD group (EAD: 324 ± 43 ml vs Non-EAD: 394 ± 29 ml, p = 0.18) (Supplement Fig 1). Other than EAD, there was no significant difference in measured clinical outcomes between the two groups, including re-operation at one month or three months (p-value for all variables > 0.05). (Supplement Table 2) We also found a 20% increase [95% CI: 3%–40%] in the odds of EAD for every 500 ml of volume given during the ICU stay (p-value = 0.02) even after controlling for vasopressor use. (Supplement table 3; Supplement Figure 2). Vasopressor use was not a predictor of a higher probability of EAD for the same volume of fluid given (p = 0.24). Vasopressor use was also not a significant predictor of EAD (p = 0.4).
Discussion
In our retrospective study of living donor liver transplant patients (LDLT), the incidence of EAD was higher in the group with a post-transplant lactate level of >6 mmol/L as compared to the patients with lactate of less than 6 mmol/L. There was no difference in MELD at transplant, graft weight recipient weight ratio, mean fluid intake, and output in the first 36 h of ICU admission or number of patients on vasopressors after the first two hours of ICU admission between the three lactate-based groups. Our study suggests that persistently elevated post-transplant lactate in LDLT patients is frequently a marker of graft dysfunction. Intensive care providers should interpret elevated lactate in the setting of other clinical factors before administering intravenous fluids
After categorizing our study population into three groups based on the highest post-transplant lactate level, there was no difference in baseline characteristics between groups for MELD score, GW/RW ratio, and vasopressor dependence after two hours of ICU admission. (Table 3). Additionally, fluid intake and urine output were also not different between these groups. Prior studies have reported elevated lactate and slow lactate clearance after liver transplant as a marker of graft dysfunction rather than of state of shock.1,35-7 Transplant patients with small for size grafts also have higher lactate and slow lactate clearance following the transplantation.2,8,11 Elevated post-transplant lactate is associated with poor graft and host outcomes in multiple prior studies.1-3,5,6 In our study, the rate of EAD was highest in Group 3 (Lactate >6 mmol/L) as compared to the other two groups. (Table 4
We performed a sub-group analysis of patients with intermediate post-transplant lactate levels (Group 2: Lactate: 3-6 mmol/L) by dividing the cohort into EAD and non-EAD groups. There were no differences in baseline characteristics, including a recipient age, history of prior transplant, MELD score, GW/RW ratio, and the number of patients on vasopressor at two hours after the ICU presentation. Interestingly, patients who developed EAD in Group 2 had a higher mean fluid intake during the first 36 h of ICU stay, and the fluid intake was independent of vasopressor use. We also found a 20% increased risk of developing EAD with every 500 ml of fluid administered in Group 2 patients. These findings, though intriguing, should be interpreted with caution given the retrospective nature of our study.
Our study certainly has its limitations. First, our study was single center and may not generalize to all living donor liver transplant recipients. Second, we did not collect information on the patient blood pressure and heart rate. However, we used vasopressor dependence after two hours of ICU admission as a surrogate marker of significant hemodynamic compromise. Third, our cohort included patients who underwent LDLT over ten years, during which there were changes in surgical and fluid management practices at some hospitals. Our surgical team has mostly remained the same during this time, and fluid administration for LDLT patients has also broadly remained stable at our institute, as shown in supplement figure 3.
Our results suggests that elevated lactate after liver transplant is often caused by decreased lactate clearance, rather than organ hypoperfusion. Intensive care providers should interpret elevated post-transplant lactate level in the setting of other clinical information such as hypotension before administering intravenous fluids.
Conclusion
In LDLT patients elevated lactate level in immediate post-op period without other signs of shock is often reflective of graft dysfunction rather than shock state. Management of these patients should not automatically include fluid resuscitation.
Supplemental Material
sj-docx-1-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-1-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-2-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-3-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-3-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-4-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-4-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-5-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-5-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-6-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-6-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-7-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-7-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-8-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-8-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-9-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-9-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-10-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-10-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-11-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-11-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-12-jic-10.1177_08850666251406213 - Supplemental material for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience
Supplemental material, sj-docx-12-jic-10.1177_08850666251406213 for Association Between Post-Operative Serum Lactate, Fluid Administration, and Outcome in Living Donor Liver Transplant Recipients: A Ten-Year Experience by Nauman Farooq, David J. Wallace, Dana R. Jorgensen, David T. Huang, Abhinav Humar and Ali Al-Khafaji in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.