
Abstract
Background
Dexmedetomidine is a first-line sedative in intensive care unit (ICU) patients. Dexmedetomidine has a high hepatic extraction ratio, where clearance is primarily determined by hepatic blood flow. In cirrhosis, hepatic blood flow is reduced, and reduced dexmedetomidine clearance may confer increased susceptibility to cardiovascular adverse effects. Drug-induced hypotension can complicate diagnosis and treatment for the ICU-based clinician. This study's objective was to evaluate clinically significant cardiovascular adverse drug reactions (CS CV-ADRs) according to liver disease severity, stratified by the Albumin-Bilirubin (ALBI) grade, in patients with cirrhosis.
Methods
This retrospective, observational, case-control study using inverse probability of treatment weighting with the propensity score assessed adults at an academic medical center in Detroit, Michigan, from July 2018 through June 2023. Critically ill patients with cirrhosis receiving intravenous dexmedetomidine in an ICU were included. Patients experiencing a CS CV-ADR within 24 h of dexmedetomidine initiation were cases and those without a CS CV-ADR were controls. The primary outcome was incidence of CS CV-ADRs stratified by liver disease severity. A CS CV-ADR included a hemodynamic event and clinically relevant intervention each within 60 minutes. A multivariable regression was used to identify predictors of CS CV-ADRs.
Results
A total of 95 cases and 95 controls were included. The median (IQR) time to CS CV-ADR was 2.4 h (1.3-9.8). Liver disease severity was stratified using the ALBI Grade, ranging from ALBI Grade 1 (least severe) to Grade 3 (most severe) disease. ALBI Grade 3 was significantly associated with increased odds of CS CV-ADRs (Adjusted OR 2.25; 95% CI [1.47-3.46]).
Conclusions
Increasing liver disease severity according to ALBI Grade was associated with greater odds of CS CV-ADRs in critically ill patients with cirrhosis receiving dexmedetomidine. ALBI Grade may be an objective tool for predicting adverse effects of dexmedetomidine or development of dose adjustments for liver dysfunction.
Introduction
Dexmedetomidine is a first-line sedative in critically ill patients. 1 Dexmedetomidine is a potent alpha-2 adrenoceptor agonist, and related side effects can include hypotension and bradycardia. 2 Dexmedetomidine effects are concentration-dependent, and after initial increases in systemic vascular resistance, bradycardia may also occur, which may culminate in hypotension via catecholamine suppression. 2 Based on these concentration-dependent effects, individuals with diminished dexmedetomidine metabolism may be more likely to experience cardiovascular instability related to dexmedetomidine.
Dexmedetomidine has a high hepatic extraction ratio (hepatic extraction ratio = 0.7; range = 0-1). 2 Hepatic extraction ratio describes drug removal following passage through the liver, comparing entry and exit serum concentrations. 3 High hepatic extraction ratio drugs (extraction ratio > 0.6) are primarily blood flow-dependent, where the major determinant of medication clearance is blood flow. 3 Hepatic blood flow is reduced in cirrhosis, leading to elevations in plasma concentration for high hepatic extraction ratio drugs. 3 Reductions in both protein binding and cytochrome P450 activity are observed in cirrhosis and may further contribute to medication accumulation. 3 Dexmedetomidine's manufacturer notes that clearance decreases in hepatic impairment and to consider hepatic dose reduction, but provides no specific hepatic dysfunction threshold for reduced dosing. 4 Pharmacokinetic data corroborates this, showing an approximately two-fold reduction in dexmedetomidine clearance and three-fold increase in half-life in severe hepatic failure. 5 Experts have noted a lack of clear and consistent guidance for clinicians and an urgent unmet need for standardized assessment of drug dosing in cirrhosis. 6
The Child-Pugh score (Figure 1), developed for prognostication in cirrhosis, contains five variables and has been used to describe hepatic dose adjustments.7,8 Subjective variables (ascites, encephalopathy), potential for imprecision with transforming continuous into categorical data (albumin, bilirubin, INR), and insufficient validation are noted concerns.3,9 Additionally, Child-Pugh's cut-points may not accurately translate the magnitude of liver dysfunction. 9 To address these limitations, the Albumin-Bilirubin (ALBI) Grade (Figure 1) was proposed as a novel hepatic disease severity assessment. 9 Containing only objective variables (albumin and bilirubin), ALBI demonstrates broad prognostic value in chronic liver diseases and may be more sensitive throughout liver disease progression versus Child-Pugh.10–13 ALBI has been shown to detect smaller changes in hepatic dysfunction than the Child-Pugh and MELD scores and can detect worsening liver function sooner than MELD in early cirrhosis. 10 Numerous reports exist detailing that ALBI predicts mortality as well as, or better, than MELD and Child-Pugh in populations with cirrhosis of varying etiology. 10 ALBI has also predicted drug clearance, validating the hypothesized mechanism (reduced hepatic blood flow) for increased effects of high extraction ratio drugs.14,15
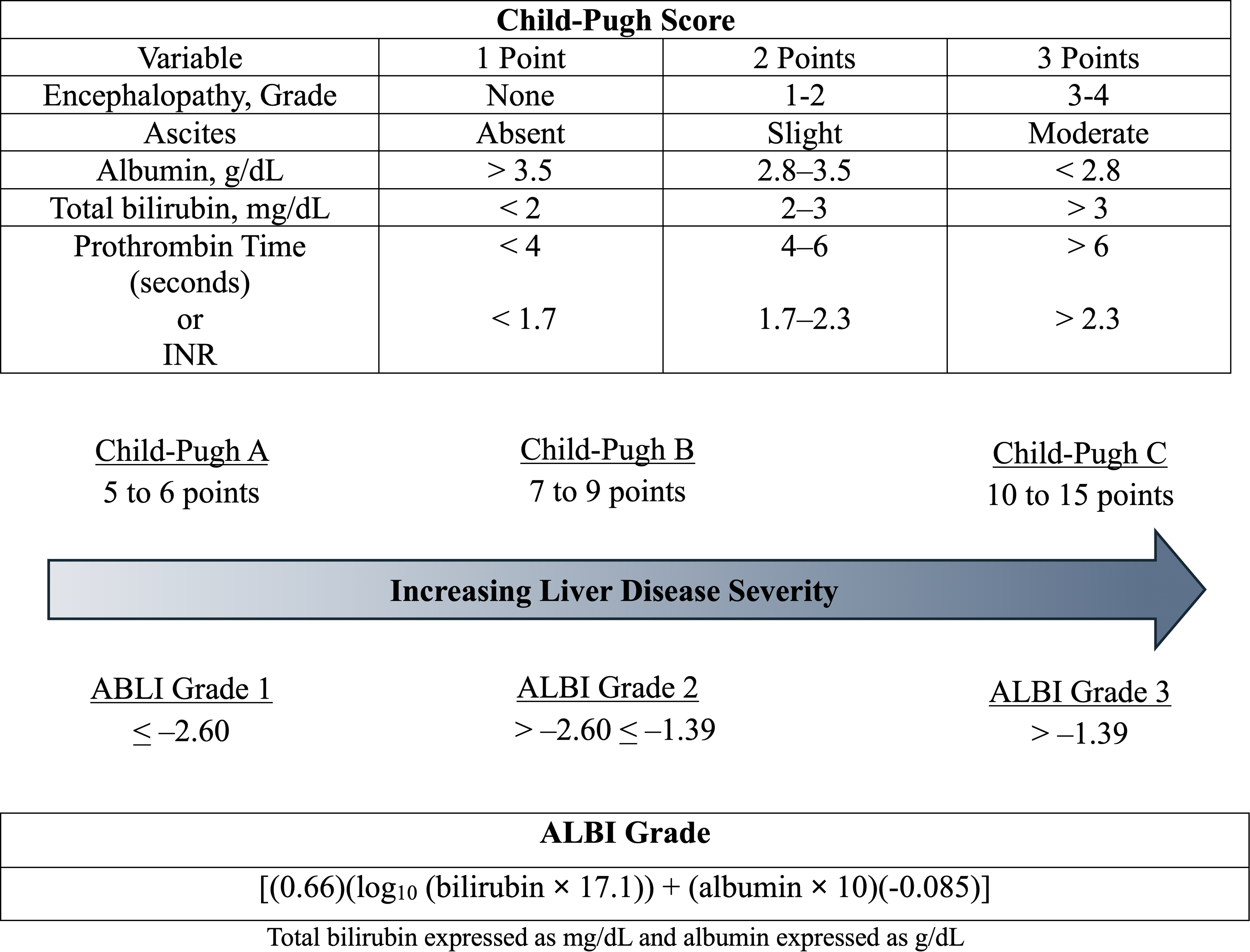
The Child-Pugh score and the ALBI grade.
It remains unclear what degree of hepatic insufficiency confers increased susceptibility to dexmedetomidine's hemodynamic adverse effects. While the ideal method for characterizing liver dysfunction severity is debatable, there is substantial evidence suggesting ALBI may be the optimal tool. 10 Experts suggest that, given its simplicity, ALBI may be well-suited for the bedside clinician given ease of use and ability to identify hepatic deterioration as it evolves. 10 Further, applying ALBI to predict adverse effects with a high hepatic extraction ratio drug is a previously undescribed approach. The purpose of this investigation is to describe the incidence of clinically significant cardiovascular adverse drug reactions (CS CV-ADRs) in patients with cirrhosis receiving dexmedetomidine stratified by ALBI Grade.
Materials and Methods
This was a retrospective, observational, propensity-adjusted, case control study conducted at an 877-bed, quaternary, academic medical center in Detroit, Michigan. Patients greater than or equal to 18 years of age were included if they received dexmedetomidine as an intravenous (IV) infusion in any intensive care unit (ICU) from July first, 2018 - June 30th, 2023, for light sedation or alcohol withdrawal, and had a cirrhosis diagnosis based on International Classification of Diseases 9 or 10 codes. Cirrhosis diagnosis was confirmed by chart review of patient past medical history and other objective data points were collected from the electronic medical record. Patients were excluded if they were pregnant, incarcerated, cognitively impaired, had mechanical circulatory support devices, pacemakers, previous heart transplant, or were undergoing targeted temperature management. This manuscript was conducted in accordance with the STROBE checklist (Appendix A).
The primary outcome was the incidence of CS CV-ADRs stratified by ALBI Grade. A CS CV-ADR was defined as: systolic blood pressure (SBP) < 90 mm Hg, mean arterial pressure (MAP) < 60 mm Hg, or heart rate < 55 beats per minute (BPM) plus one clinically relevant intervention within 60 minutes of the hemodynamic event defined as: crystalloid fluid bolus ≥ 250 mL, addition of a vasopressor, tapering dexmedetomidine faster than institutional protocol, increase in vasopressors by ≥ 10 mcg/min norepinephrine equivalents, switching sedatives, atropine administration, or discontinuation of agents that slow atrioventricular nodal conduction (beta blockers, calcium channel blockers, digoxin, amiodarone). The hemodynamic parameters were derived from precedent described in similar literature, and the clinically relevant intervention parameters based on expert opinion.
16
CS CV-ADRs were examined from the initiation of the dexmedetomidine until reaction occurred (cases), with an observation duration of up to 24 hours if no reaction occurred (controls). The ALBI Grade is calculated as follows with total bilirubin expressed as mg/dL and albumin expressed as g/dL: [(0.66)(log10 (bilirubin
Cases were defined as those experiencing a CS CV-ADR within 24 hours of dexmedetomidine infusion. Controls were those that did not experience a CS CV-ADR in the first 24 hours. Inverse probability of treatment weighting (IPTW) with the propensity score was applied to mitigate potential confounders of hemodynamic instability. 17 Variables used in the propensity scoring model included low baseline hemodynamic values, age, weight at admission, and cardiac ICU admission. Low baseline hemodynamics were defined as any of the following (individually or in combination): SBP < 100 mm Hg or MAP < 70 mm Hg or HR < 70 BPM. These variables were selected for the propensity model to offset confounding, as patients with low hemodynamic values at baseline would be more likely to meet the prespecified hemodynamic threshold, advanced age may predispose to hypotension in the ICU, increases in weight may yield larger dexmedetomidine exposure, and cardiac ICU patients may be more sensitive to drugs that impact the cardiovascular system. Data nearest to dexmedetomidine administration was used to calculate SOFA score. For MELD 3.0 scoring, data was used at ICU admission.
Data was extracted from the electronic medical record via manual chart review. Data was analyzed using chi-squared, Fisher's exact test, student's T-test, or Mann-Whitney U, depending on data type and distribution. Results are presented as unadjusted and adjusted odds-ratios (ORs and AdjORs). Multivariable logistic regression was performed using backwards, stepwise, conditional methods with a removal criteria p-value of < 0.2. The Naranjo Adverse Drug Reaction and Probability Score was computed among cases by two separate investigators. If discrepancies were noted in the categorization of probability scores, the investigators reviewed cases together to develop a conclusion. 18 Previous literature reported worsening of cardiovascular SOFA subscores in 23% of patients receiving dexmedetomidine and internal data estimated dexmedetomidine-mediated hypotension in 56.8% of cirrhosis patients. 16 Differences in treatment effect were truncated to clinically reasonable values. Assuming an incidence of 23% in the controls and 45% in the cases, a sample size of 190 patients was required for 90% power.
Results
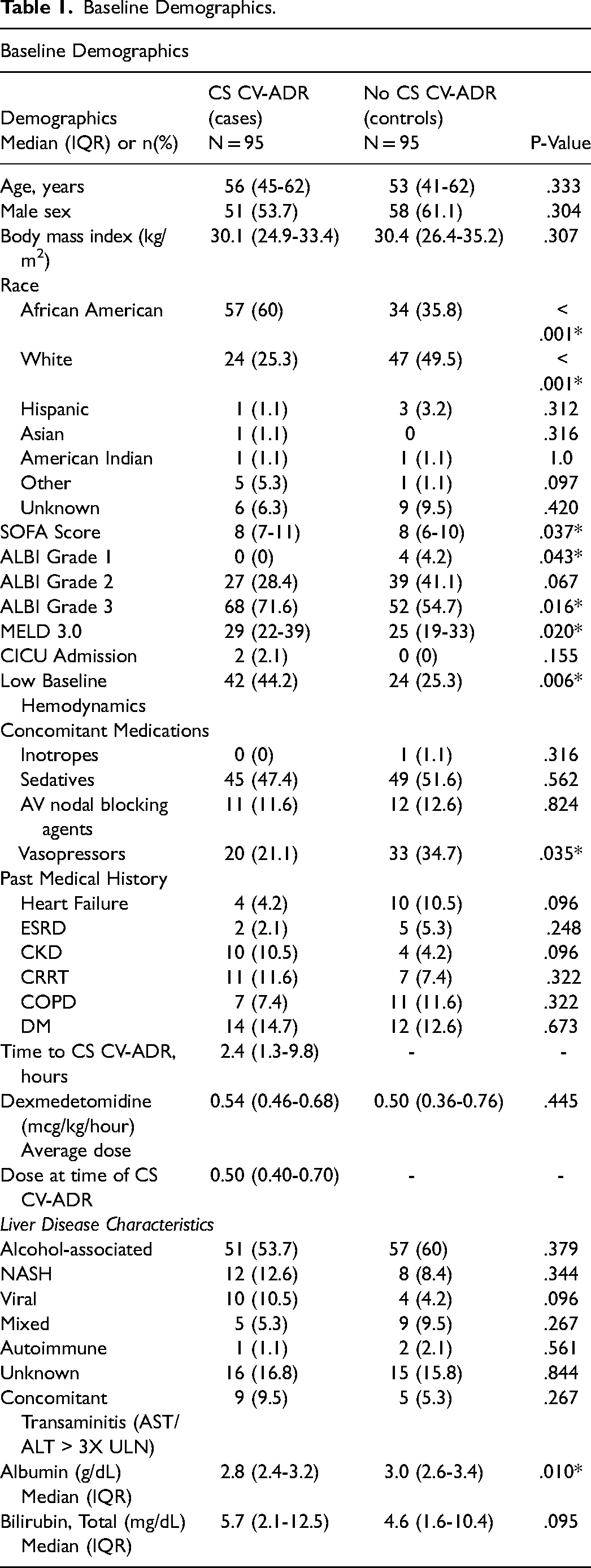
A total of 333 patients were screened, 143 excluded, and 190 included. Patient baseline characteristics are shown in Table 1. Most exclusions were due to not having cirrhosis (n = 66, 46%), not being in the ICU (n = 23, 16%) or not receiving dexmedetomidine while in the ICU (n = 30, 21%) (Figure 2). There were 95 cases and 95 controls included the analysis. A majority of the population was male (n = 109, 57.4%), with a median SOFA score of 8 (6-10), and primary cirrhosis etiology as alcohol-associated (n = 108, 57%). Median MELD 3.0 score was higher among cases compared to controls [29 (22-39) versus 25 (19-33); p = .020). Low baseline hemodynamic values were noted more among cases (44.2% vs 25.3%; p = .006). Cases were also less likely to be on concomitant vasopressor therapy at baseline compared to controls (21.1% vs 34.7%; p = .035). Among cases, the median time to CS CV-ADR was 2.4 hours (1.3-9.8).
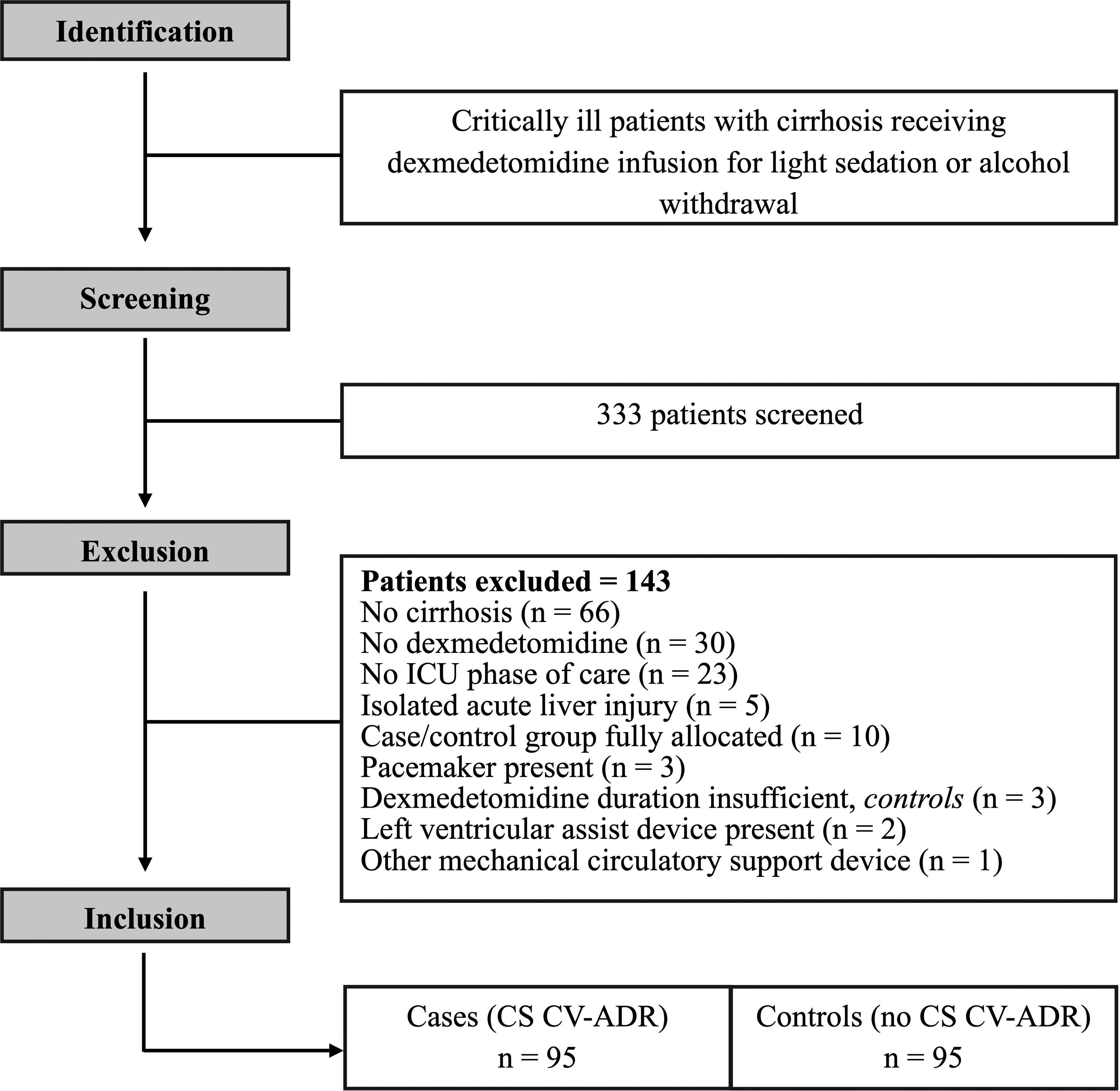
Patient inclusion flowchart.
ALBI Grade 3, representing the most severe liver dysfunction, was associated with increased odds of CS CV-ADRs (AdjOR 2.25; 95% CI [1.47-3.46]) (Table 2). Given minimal representation of ALBI Grade 1, for comparisons, ALBI Grade 1 patients were included with ALBI Grade 2 patients. ALBI Grade 1-2, representing lesser severity liver dysfunction, was a protective factor and associated with reduced rates of CS CV-ADRs (AdjOR 0.44; 95% CI [0.29-0.68]; p < .001). Among patients not experiencing a CS CV-ADR (n = 95), there were 59 (62%) patients with isolated hemodynamic ADRs. There were no significant differences in rates of isolated hemodynamic ADRs (Table 2), but there were proportionally more events as ALBI Grade increased (ALBI Grade 1-2 = 42.4%, ALBI Grade 3 = 57.6%; p = NS).
Baseline Demographics.
CS CV-ADRs and Isolated Hemodynamic ADRs Stratified by ALBI Grade.
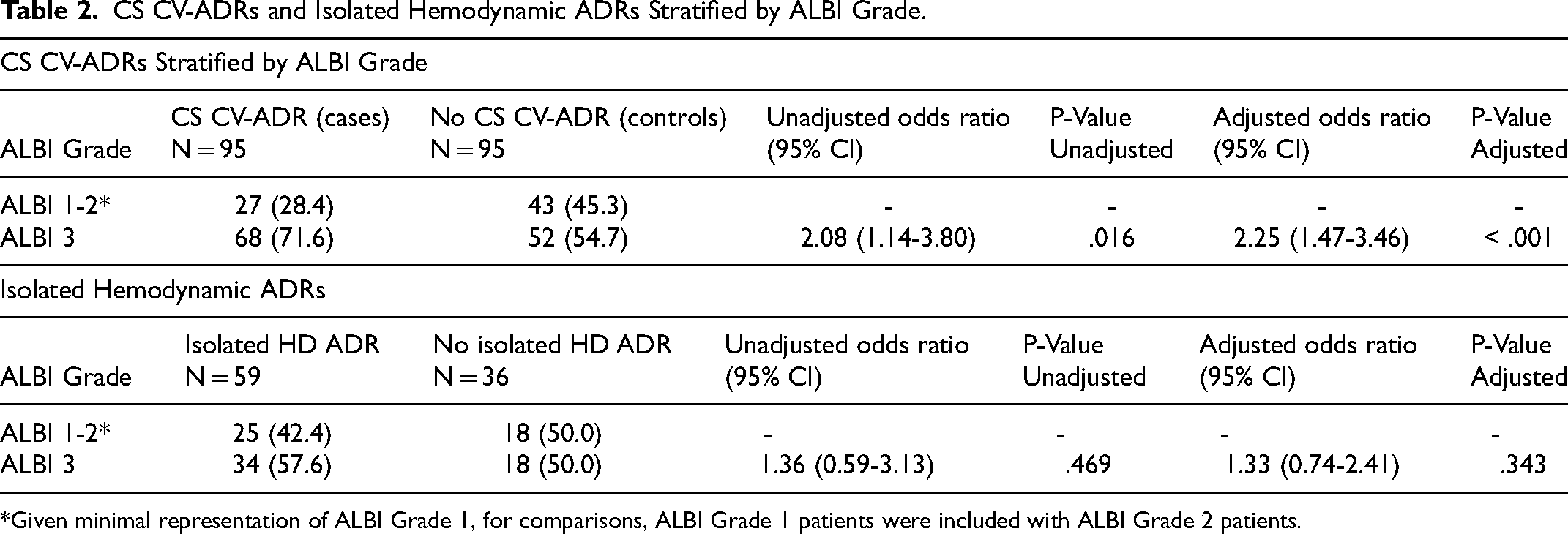
*Given minimal representation of ALBI Grade 1, for comparisons, ALBI Grade 1 patients were included with ALBI Grade 2 patients.
Multivariable Logistic Regression.
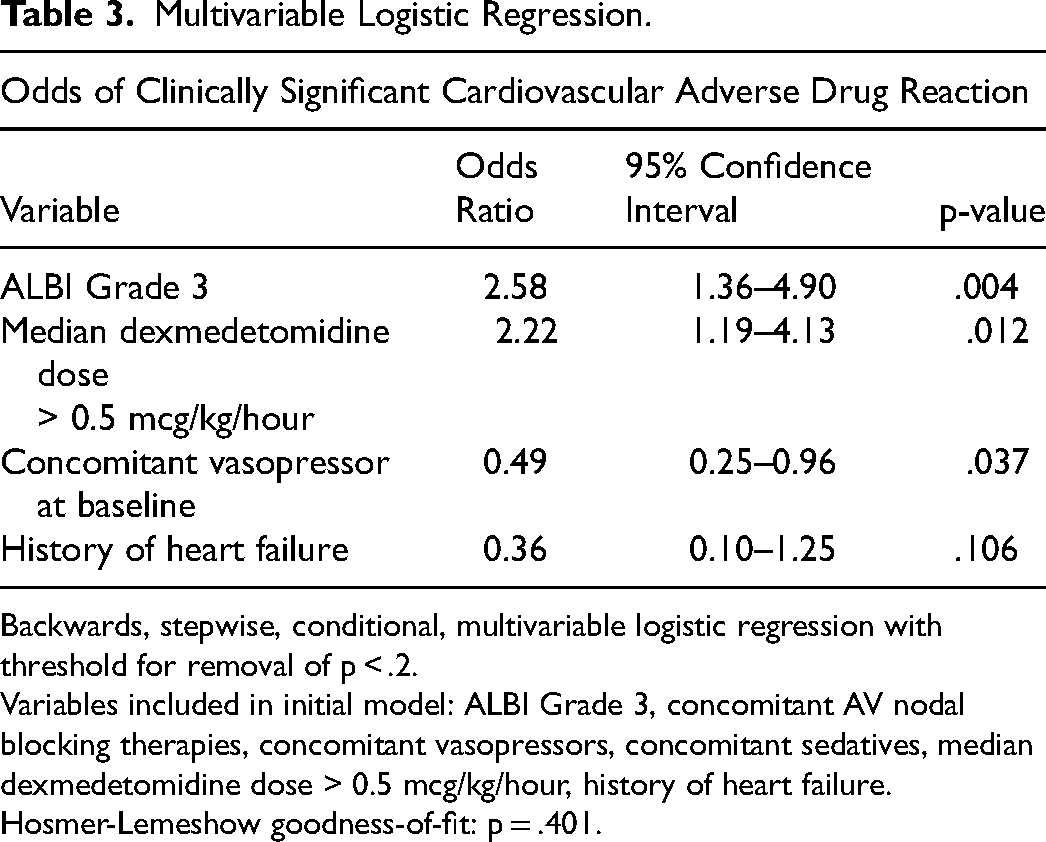
Backwards, stepwise, conditional, multivariable logistic regression with threshold for removal of p < .2.
Variables included in initial model: ALBI Grade 3, concomitant AV nodal blocking therapies, concomitant vasopressors, concomitant sedatives, median dexmedetomidine dose > 0.5 mcg/kg/hour, history of heart failure.
Hosmer-Lemeshow goodness-of-fit: p = .401.
According to multivariable logistic regression (Table 3), independent predictors of developing CS CV-ADRs were ALBI Grade 3 (OR 2.58; 95% CI [1.36-4.90]; p = .004) and median dexmedetomidine dose > 0.5 mcg/kg/hour (OR 2.22; 95% CI [1.19-4.13]; p = .012). This model also identified concomitant vasopressor at baseline (OR 0.49; 95% CI [0.25-0.96]; p = .037) as a protective factor against developing CS CV-ADRs. Among those experiencing a CS CV-ADR, Naranjo Adverse Drug Probability classified 61 CS CV-ADRs as “probably” and 34 as “possibly” related to dexmedetomidine. 18
Discussion
CS CV-ADRs were significantly greater with worsening liver disease, defined by ALBI Grade, in patients with cirrhosis receiving dexmedetomidine. This relationship was non-linear, with a substantially different risk profile when moving from ALBI Grades 1 or 2 to ALBI Grade 3 liver disease. Patients with ALBI Grade 3 receiving dexmedetomidine had more than two-fold odds of experiencing a CS CV-ADR compared to those with less severe disease. The median 2.4-hour CS CV-ADR onset among cases demonstrates need for vigilance alongside potential pre-emptive dose individualization.
Dexmedetomidine is a common sedative and cirrhosis has increased markedly over the last several decades. 19 Concerningly, epidemiologic studies noted a 74.5% increase in liver cirrhosis prevalence from 1990 to 2017. 19 If these trends continue, clinicians might anticipate increased rates of cirrhosis across all phases of care. Moreover, drug induced cardiovascular instability is burdensome. An ICU-based point prevalence study estimated drug-induced hypotension occurs in up to 23% of critically ill patients, where improper dosing (56.9%) is among leading causes. 20 The differential diagnosis for hypotension in a critically ill patient is broad and can implicate serious medical conditions. When the hypotension is drug-induced, particularly if unrecognized, patients may be exposed to tests and/or interventions that place them at additional risk or delay treatment of the index condition. For this reason, prevention of drug-induced hypotension is essential. Defining at-risk patients using ALBI Grade and culprit drug therapies through pharmacokinetic properties may help minimize drug-induced adverse events in patients with cirrhosis.
These findings highlight the potential role of ALBI Grade as a surrogate to predict increases in therapeutic or adverse effects for high hepatic extraction ratio drugs in cirrhosis.3,10 Other studies assessing dexmedetomidine's hemodynamic impact in mixed ICU populations without cirrhosis have reported median time to hemodynamic instability of approximately 4 hours. 16 The present finding of 2.4 hours to CS CV-ADR appears to be consistent with the notion of the cirrhosis population being at risk due to a two-fold reduction in dexmedetomidine clearance noted previously. 5 Considering literature has shown correlation in drug clearance with liver dysfunction according to ALBI Grade, it is likely that reduced clearance drives these research findings. 14 Given ALBI Grade objectivity and use of common lab values, integration into electronic clinical decision support tools may help identify patients where alternative sedation or tailored dexmedetomidine dosing should be considered. Beyond dexmedetomidine, high hepatic extraction ratio drugs used for pain, agitation, and delirium in the ICU include fentanyl, ketamine, morphine, and propofol.21–23 ICU-based clinicians are lacking specific hepatic dose recommendations for these therapies. The present proof-of-concept study using ALBI Grade may reflect a new strategy to predict adverse responses, and potentially identify dosing thresholds, in patients with hepatic failure when manufacturer guidance does not exist or is unclear.
Strengths of this study include the case-control design and IPTW to diminish confounding. The primary confounder at greatest risk of impacting results is classification bias around CS CV-ADR definitions among patients with baseline low hemodynamics. The IPTW model was primarily pursued to counterbalance this, such that patients with lower baseline hemodynamics were balanced between the two groups, given low baseline hemodynamics may be collinear with hepatic dysfunction severity. The relatively similar odds ratios and confidence intervals of the primary endpoint in adjusted and unadjusted analyses favors that the findings are unlikely due to chance. Despite this, the confidence intervals remain wide, and quantifying the precise increase in odds of CS CV-ADRs would likely require a larger and more homogeneous population. Limitations include potential incomplete specification of the IPTW model, which operates under the assumption that all relevant confounders are identified and included. Additionally, measurement of albumin, which is an acute phase reactant and a component of the ALBI Grade, raises questions about optimal timing of ALBI Grade assessment. With no standard of care for timing of ALBI Grade assessment, the present investigation used albumin and bilirubin at the time point closest to dexmedetomidine initiation as the patient may be expected to experience the pharmacodynamic effects of hypoalbuminemia at this time. The definition of a CS CV-ADR is somewhat arbitrary as there is no validated definition. The present definition was modeled off similar literature alongside expert opinion regarding bedside interventions that would be considered clinically significant for the ICU-based clinician. 16 The observation that concomitant vasopressors at baseline was significantly greater in the control group might suggest potential masking of CS CV-ADRs through slow upwards titration of vasopressors that did not reach the magnitude and timing definitions for a significant event. Moreover, vasopressor use at baseline was a protective factor in multivariable logistic regression, which supports potential masking. If this was the case, it is possible that the burden of CS CV-ADRs using the current study definition might be an underestimate. Of note, a previously published study was used to constitute a 10 mcg/min norepinephrine equivalent as a clinically significant increase. 24 Finally, the population in this study is primarily medical ICU, making these findings less generalizable to other relevant ICU populations.
Conclusions
In critically ill patients with cirrhosis, ALBI Grade 3 was independently associated with developing a CS CV-ADR within 24 hours of initiating dexmedetomidine. Assessment of ALBI Grade may be considered to guide individualized dexmedetomidine use in critically ill patients with cirrhosis. Future research is needed to assess impact of applying ALBI Grade with intent to reduce CS CV-ADRs and define evidence-based dose adjustments in cirrhosis.
Supplemental Material
sj-doc-1-jic-10.1177_08850666251408751 - Supplemental material for Critically Ill Patients with Severe Cirrhosis Receiving Dexmedetomidine at a Higher Risk of Cardiovascular Instability: Application of an Objective Novel Cirrhosis Scoring System
Supplemental material, sj-doc-1-jic-10.1177_08850666251408751 for Critically Ill Patients with Severe Cirrhosis Receiving Dexmedetomidine at a Higher Risk of Cardiovascular Instability: Application of an Objective Novel Cirrhosis Scoring System by Emma Kabalka, Zachary Smith, Geneva Tatem and Benjamin August in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge Michael Veve, Pharm.D., MPH, for contributions to methodology and analysis and Kristin Griebe, Pharm.D., BCPS, BCCCP, for data retrieval and expertise.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.