
Abstract
Impaired GI tract function is a common and often underappreciated symptom in the Medical Intensive Care Unit (MICU). The most visible manifestation of this dysfunction is reduced bowel movements. The occurrence of impaired GI function is associated, both independently and in association with delayed enteral feeding, with increased length of stay, morbidity and mortality. We report on a process implementation project conducted at a single academic center designed to: (I) increase visibility of bowel movement charting and (II) transition from a reactive to a proactive laxative administration regimen for prophylaxis against MICU associated constipation. Scheduled laxatives, polyethylene glycol and sennoside-docusate, were added to the MICU admission orderset and bowel movement charting was moved to a more readily accessible flowsheet in the electronic medical record. Six months of pre-intervention and post-intervention admissions to the MICU were reviewed to determine patient demographics, admitting diagnosis, Sequential Organ Failure Assessment (SOFA) score, laxative utilization, and time to first bowel movement. Following implementation of these changes, prophylactic laxative utilization significantly increased (p < .001) driven largely by the agents included in the orderset. This was associated with a decrease in MICU length of stay by an average of 21 h (p = .006) and median time to first bowel movement by 4 h (p = .026), but no changes in incidence of impaired transit (as defined by greater than 72 h without a bowel movement). This data represents an exciting first step in the use of mixed agent prophylactic laxative regimens.
Keywords
Background
The Medical Intensive Care Unit (MICU) is the appropriate level of care for patients who are critically ill from a variety of underlying pathologies. It is typical for these patients to receive both ventilatory support with invasive ventilation as well as circulatory support, both chemically and occasionally mechanically. Dysfunction of multiple organ systems, both at time of admission and during the MICU course is common. Often underappreciated is dysfunction in the gastrointestinal (GI) tract, however, emerging data suggests that GI tract impairment has significant impacts on both morbidity and the overall MICU course.1–4
Constipation, defined by the American College of Gastroenterology (ACG) and American Gastroenterological Association (AGA), is generally referred to as bowel movements occurring less than three times weekly. 5 Within the critical care space, the European Society of Intensive Care Medicine (ESICM) defines constipation as greater than or equal to three days between bowel movements.6,7 Related to this definition is the concept of Impaired GI Transit (IGT) seen within the critically ill, namely, the generalized motility disorders that accompany critical illness.7–12 Current understanding of the pathophysiology of IGT is limited and, likely, is due to the overlap of stress response and inflammation, pharmacologic effects, biophysical changes associated with mechanical ventilation, and other yet to be identified factors.1,7,9 Impaired movement of contents in all portions of the GI tract has been observed in the critically ill and while the pathology seems to be shared, the clinical presentation of these dysfunctions remains different.9,13,14 Understanding of this condition is further limited by the variety of definitions which have been used in the literature as well as lack in standardized approach to diagnosis and management.9–12 Delayed gastric emptying (ie, gastroparesis) typically presents with feeding intolerance, nausea/vomiting and impaired small intestine motility (ie, ileus), and may cause abdominal distension and pain. These symptoms may go unnoticed in the intubated and sedated patient.1,7,9,11,13
The most common clinically observed symptom is delayed bowel movements, which, while not providing specific localization of the dysmotility, indicate impaired GI tract function. It is estimated that up to 80% of patients admitted to the ICU experience constipation or some other impaired GI function.2,8–10,12,15 Incidence of constipation or IGT has been associated with a number of problematic clinical outcomes: increased length of stay, increased mechanical ventilation requirement, increased rates of infection, delirium, and possibly mortality.2,16 In spite of these severe consequences, this condition remains common owing to lack of agreement on diagnosis and treatment. Typical treatment options are laxative agents (including osmotic, stimulant, and lubricant), promotility agents (eg, metoclopramide, erythromycin, neostigmine), and peripherally acting mu-opioid antagonists (PAMORAs). 17 There have been several trials comparing prophylactic and treatment strategies of laxative administration. Seminal work has shown that administration of either polyethylene glycol or lactulose is more effective than placebo in preventing delayed defecation in critically ill patients. 18 However, results from meta-analyses are mixed with some showing overall reduction in constipation or delayed defecation and others showing no differences.1,16,19 Though, it is worth noting that most of the trials included in the meta-analyses have used lactulose, which is associated with a number of side effects. Few, if any, include stimulant laxatives.
We present a process improvement study designed to reduce IGT and improve patient outcomes in the MICU with key interventions: (I) increase visibility of bowel movement documentation for clinicians and (II) implement a prophylactic two agent laxative regimen pre-ordered at the time of MICU admission. The choice of a two agent regimen was based on ACG guidelines on treatment of chronic constipation and AGA guidelines on opioid induced constipation. To our knowledge, this is the first reported protocol using scheduled osmotic and stimulant laxatives simultaneously. This single center study was designed as a proof of concept and exploration of the ways to mitigate IGT, in accordance with SQUIRE guidelines.
Methods
Participants
The population under study were adults older than 18 years of age admitted to the Medical Intensive Care Unit (MICU) at a single academic hospital for a total of 12 months. Six months pre-intervention (September 2022-March 2023) and six months post-intervention (September 2023-March 2024). Variables recorded were: age, sex, admitting diagnosis, Sequential Organ Failure Assessment (SOFA) score at admission, admission date and time, MICU length of stay (LOS) and medication administration information. Data was collected retrospectively, stored securely, and analyzed in a de-identified fashion. The interventions outlined below were exempted from informed consent by the Institutional Review Board at University of Connecticut Health Center, IRB number: 24X-008-2.
Interventions
The primary intervention implemented was incorporating scheduled laxative agents into the admission orders for the MICU. The standardized admission orders used at our institution were edited to include an osmotic (polyethylene glycol) and stimulant (sennoside-docusate) laxative ordered in a scheduled fashion for all patients (Figure 1A). Previously, no laxatives were part of the order set. Admitting providers were able to hold or discontinue laxatives at their discretion and patients were able to refuse laxative agents. When this was clinically appropriate (eg, in the setting of GI bleeding, diarrhea, or strict NPO status) these instances were accounted for in laxative use calculations. In addition, the charting of bowel movements was made more visible (Figure 1B). The critical care context of the EPIC (Verona, Wisconsin, USA) electronic medical record at our institution contains an “ICU provider flowsheet” with essential data for MICU rounding. Last charted bowel movement was added to this flowsheet.
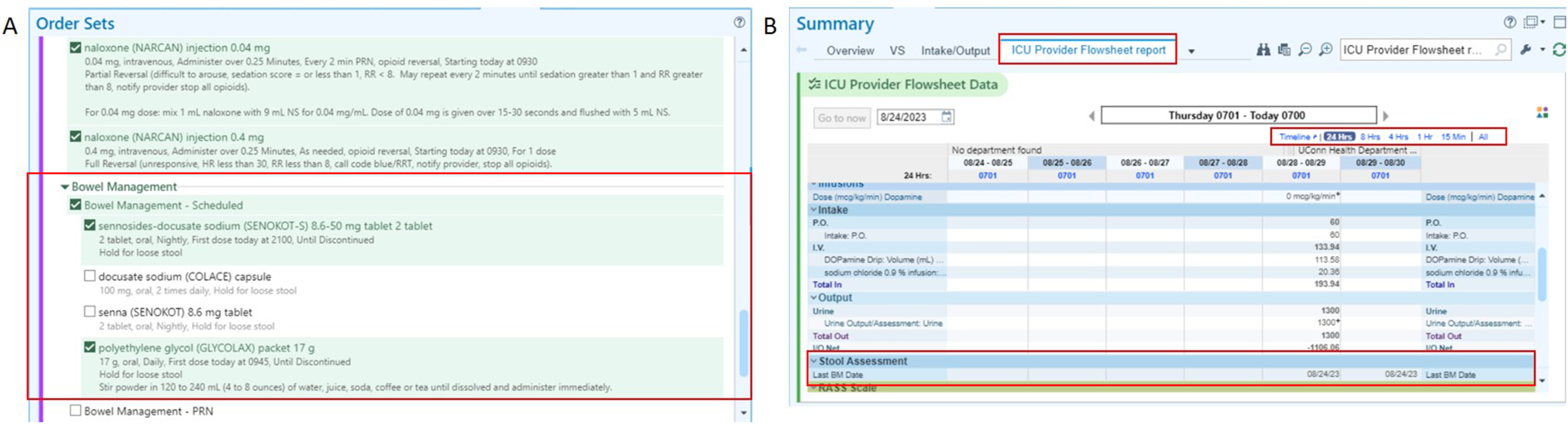
Updated order set in electronic medical record. (A) The primary intervention implemented was a pre-selected laxative regimen of scheduled polyethylene glycol and sennoside-docusate within the admission order set for the medical ICU. Providers needed to de-select these agents if laxatives were contraindicated for patients. (B) Additional intervention included increased visibility of bowel movement charting for providers.
Statistical Analysis
Descriptive statistics were calculated for demographic variables. All continuous variables were compared using Student's t Test of mean or Wilcoxon Signed Rank Test where not normally distributed. Categorical variables were compared using X2 test or Fisher's exact test, if the count was less than or equal to 5. Pearson's correlation was used to assess for relationship between time to first bowel movement and time to first laxative administration. An alpha value of 0.05 was used for significance. To detect a doubling in the rates of utilization at 80% power, 33 instances would be needed in each group. Time durations were calculated using the lubridate package in R Statistical Software. 20 Data was analyzed using both R Statistical Software (Vienna, Austria) and GraphPad Prism 10.1 for Windows (GraphPad Software, Boston, MA).
Results
ICU Population
Between September 1, 2022 and March 1, 2023, the pre-intervention time frame, 464 admissions were identified longer than 12 h. During the post intervention time frame (September 1, 2023-March 1, 2024), 494 admissions were identified. Both groups showed similar distributions of sex, age, admitting diagnosis, vasopressor use, ventilator status, and severity of illness assessed by SOFA score at admission (Table 1).
Group Characteristics and Comparison of Laxative use.
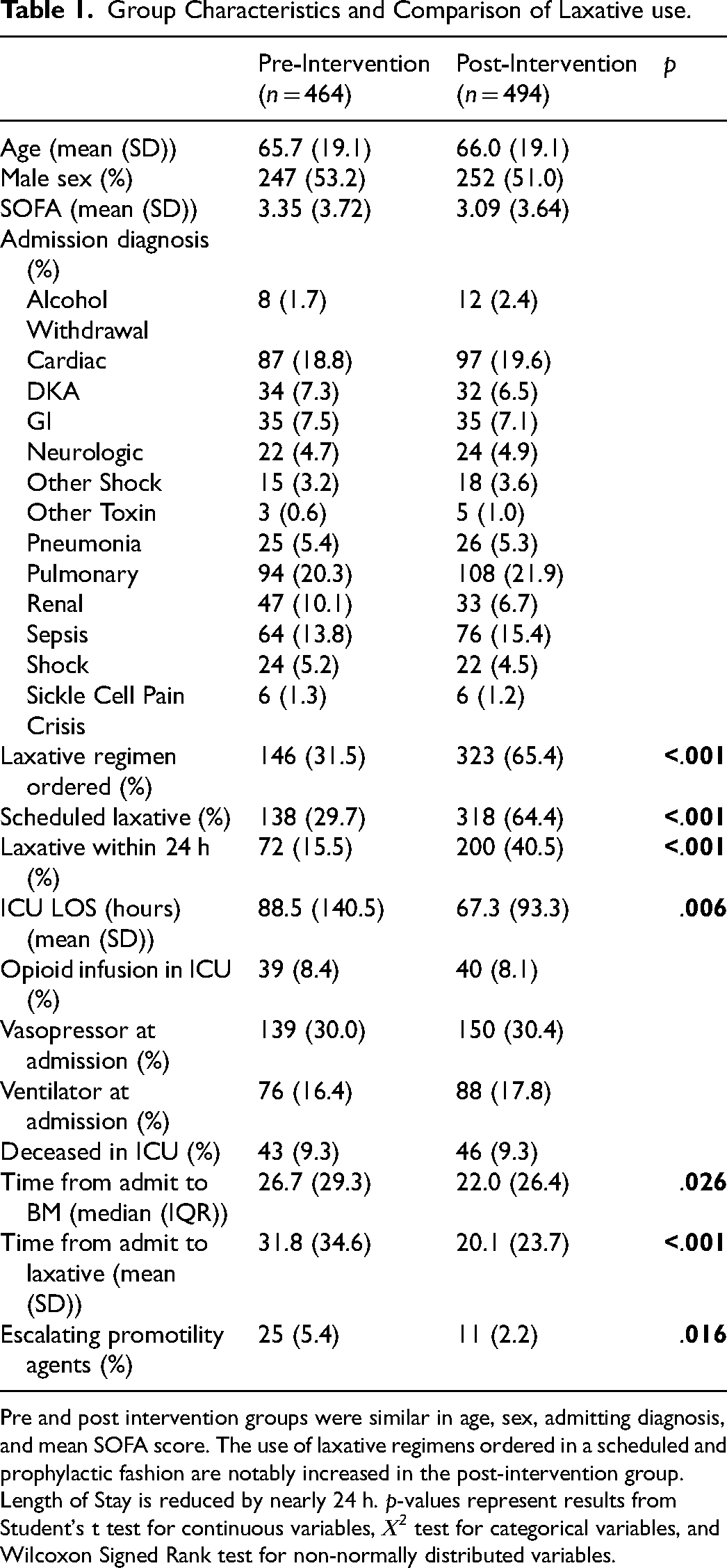
Pre and post intervention groups were similar in age, sex, admitting diagnosis, and mean SOFA score. The use of laxative regimens ordered in a scheduled and prophylactic fashion are notably increased in the post-intervention group. Length of Stay is reduced by nearly 24 h. p-values represent results from Student's t test for continuous variables, Χ2 test for categorical variables, and Wilcoxon Signed Rank test for non-normally distributed variables.
Laxative use Patterns
Pre-intervention laxative use patterns showed low utilization of laxatives, with only 31.5% of admissions having laxatives ordered. Notably, even fewer were administered in a prophylactic fashion with average time to first administration being over 31 h and 15% receiving laxatives within 24 h of admission (Table 1). Following implementation of the interventions, laxative orders increased over twofold to 65% of admissions, with nearly triple the rate of laxatives being used prophylactically (40.5%, Table 1). There was also a significant reduction in the time elapsed to first laxative administration (mean difference = 11.6 h, t = 3.54, df = 196, p < .001). The change in usage occurred quickly after implementation of the interventions and was sustained throughout the period under study (Figure 2A–C).
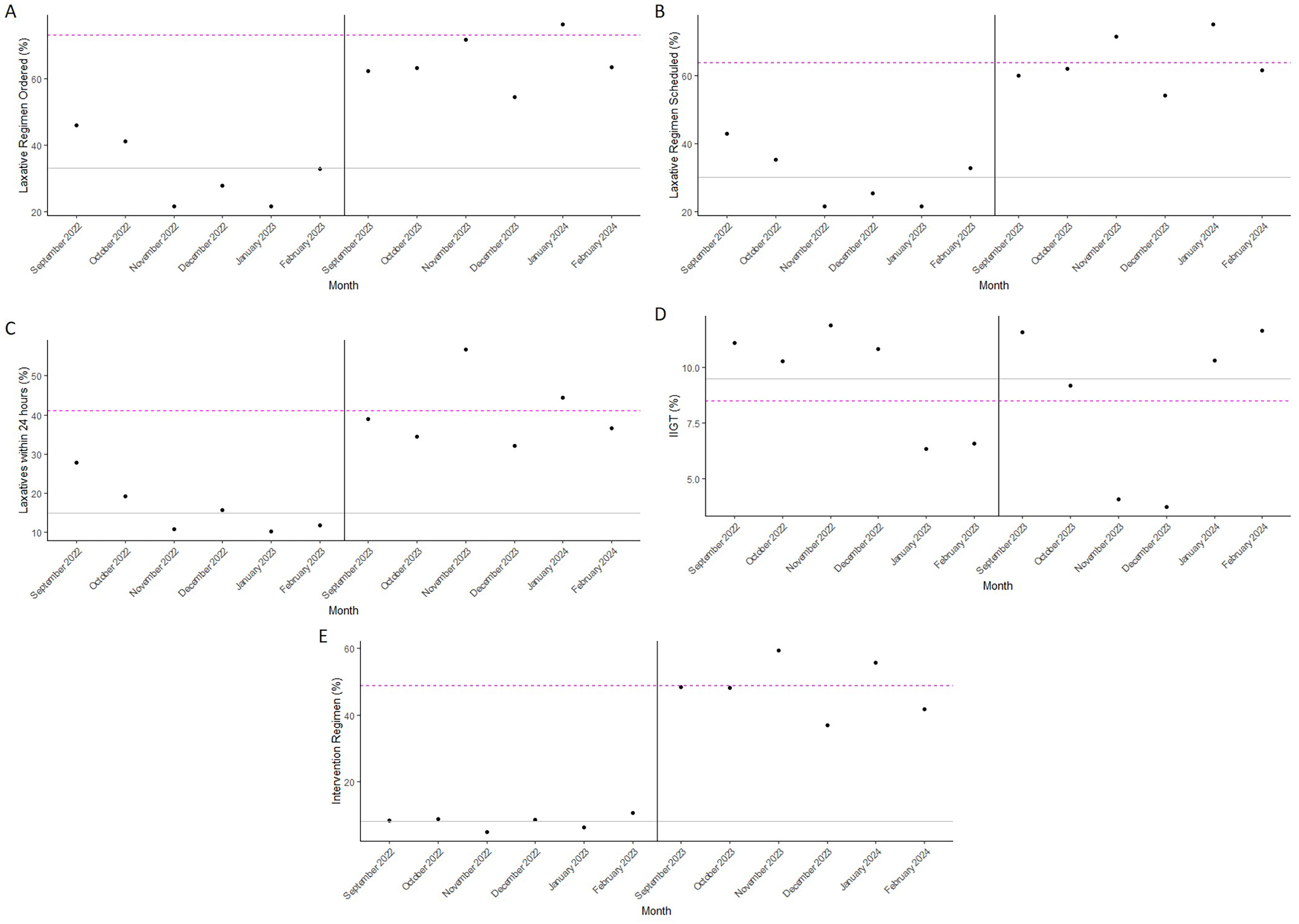
Run charts. For all: Vertical line denotes pre (left) and post (right) intervention times. Grey lines (solid horizontal lines) denote pre-intervention average and magenta lines (dashed lines) denote post-intervention average. (A) Run chart of percentage of patients admitted to the ICU with laxative regimen ordered, showing immediate increase in utilization following start of intervention and consistent increased usage. (B) Not only are more laxatives ordered, but rapidly being ordered in a scheduled rather than an as needed fashion. (C) With increased scheduled laxatives, there is a decrease in the time taken to administer the first laxative dose. (D) While the incidence of ICU associated Impaired GI Transit (IIGT) decreased post-intervention, this was not consistent throughout the months under study. November and December 2023 showed rates below 5%, the lowest seen in the time under study, but this was not sustained throughout. (E) Intervention regimens notably increased post-intervention.
Not only were more laxative agents used and the time to administration decreased, the types of laxatives utilized post-intervention also showed a shift. Agents included within the order set, polyethylene glycol and sennoside-docusate, as individual components (X2 = 125, df = 1, p < .001 and X2 = 124, df = 1, p < .001, respectively) and their combination (X2 = 150, df = 1, p < .001) increased post-intervention. Additionally, bisacodyl suppository usage decreased post-intervention (X2 = 6.4, df = 1, p = .01) (Table 2). Most significantly, escalating laxative agents and other promotility agents (eg, polyethylene glycol colonoscopy preparations in the absence of planned procedures, single time suppositories or enemas, or magnesium citrate), showed marked decrease following implementation of intervention (X2 = 5.4, df = 1, p = .02).
Laxative Agents Used pre and Post Intervention.
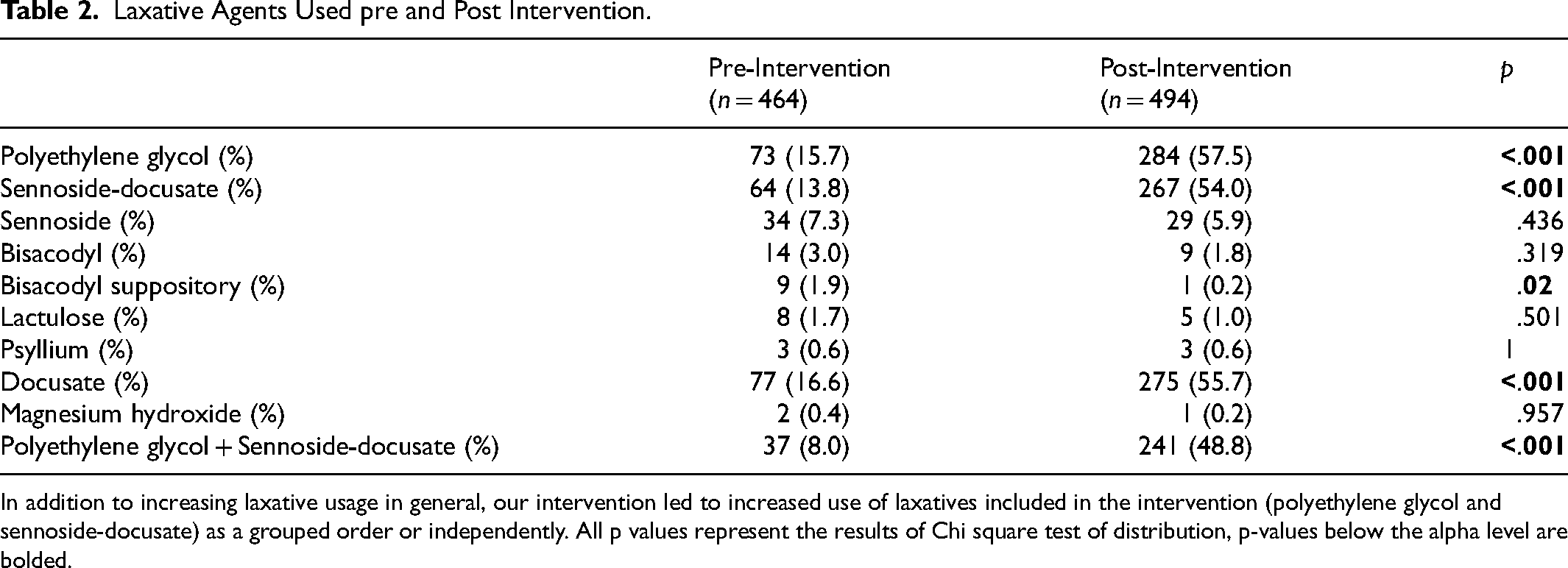
In addition to increasing laxative usage in general, our intervention led to increased use of laxatives included in the intervention (polyethylene glycol and sennoside-docusate) as a grouped order or independently. All p values represent the results of Chi square test of distribution, p-values below the alpha level are bolded.
MICU Length of Stay
Prior to intervention length of stay averaged 88.5 h (SEM 6.5), with significant variability in length of stay. Following implementation of intervention, mean length of stay decreased by nearly one day (mean difference = 21.2 h, t = 2.74, df = 798, p = .006) (Table 1). Accounting for laxative regimens that were held appropriately, this difference is preserved (mean difference = 20.8 h, t = 2.51, df = 779, p = .012).
Bowel Movements and Incidence of Impaired GI Transit
Time to first bowel movement in the ICU prior to intervention showed great variability. In the pre-intervention period, the median time to first bowel movement was 26 h. Following intervention, there was a reduction in time to first bowel movement by approximately 4 h (W = 105,060, p = .026). Interestingly, there were no observed differences in incidence of impaired GI transit, defined as no bowel movement within 72 h of ICU admission, between pre and post intervention timepoints overall (X2 = 0.714, df = 1, p = .398) or when excluding participants with appropriately held laxative regimens (X2 = 0.887, df = 1, p = .346). This is also true for selected subgroups of participants on ventilators (X2 = 0.012, df = 1, p = .912), vasopressors (X2 = 1.75, df = 1, p = .186), and opioid infusions (X2 = 0, df = 1, p = 1) (Table 3).
Incidence of ICU Constipation.

There are no differences in incidence of impaired GI transit in the pre and post intervention groups. Data is displayed as incidents over total individuals with percentages in parentheses, p values represent the results of X2 tests.
Notably, a positive linear correlation exists between the time to first bowel movement and time to administration of laxative agent (Figure 3). This is a moderate positive relationship in the pre-intervention group (r = 0.42, p < .0001), but a weak positive correlation in the post-intervention group (r = 0.12, p < .05).
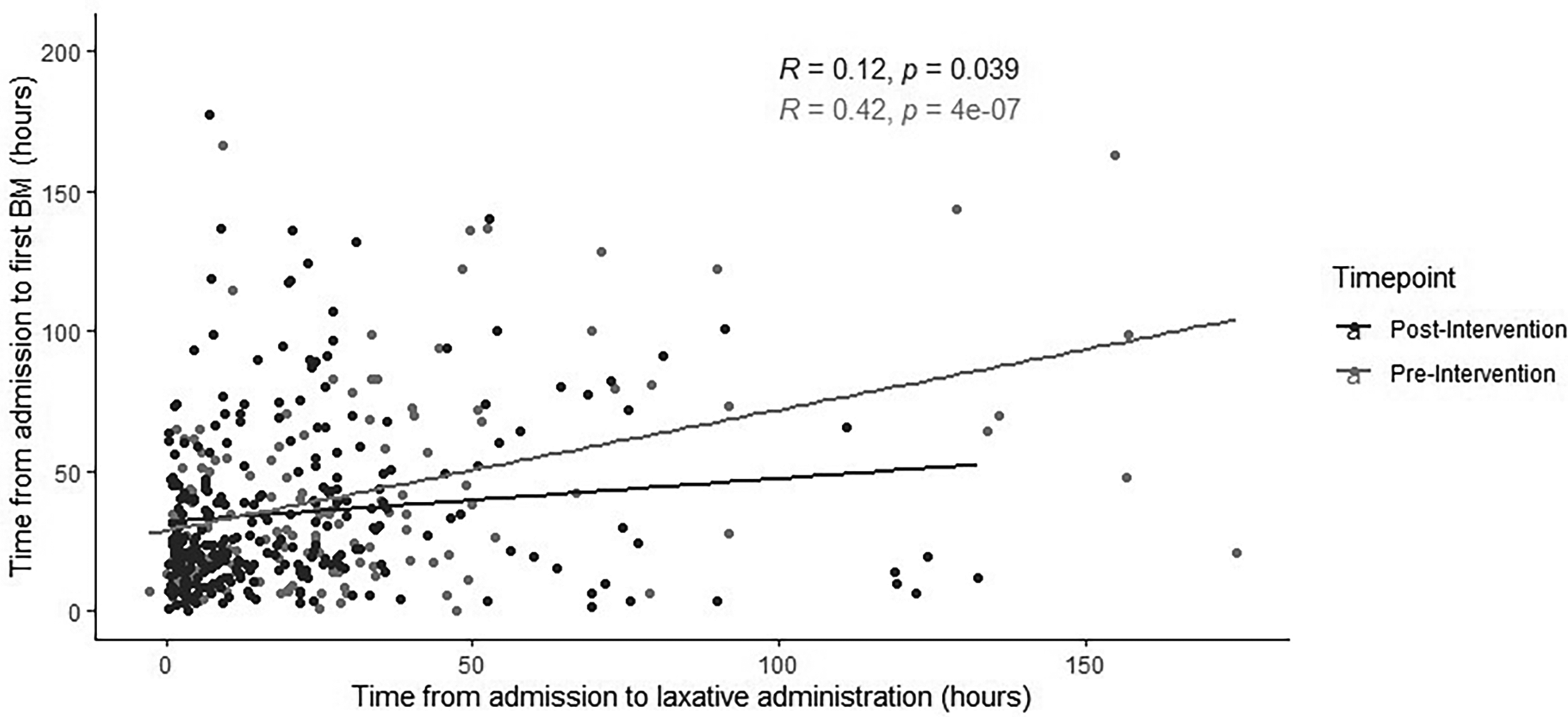
Time to First Bowel Movement is Correlated to Time to Laxative Administration. the Time to First Bowel Movement (BM) in the MICU is Directly Correlated to the Time to First Laxative Administration. the Correlation Shows Moderate Strength in the Pre-Intervention Group but a Weak Strength in the Post-Intervention Group.
Discussion
We have shown that simply increasing visibility of bowel movement charting and implementing pre-ordered laxative agents is sufficient to increase utilization of laxative agents and timeliness of laxative administration, thereby supporting early constipation prophylaxis. Prior work has shown that prophylactic dosing of laxatives is associated with reduced organ dysfunction without overall decrease in mortality, as well as a trend towards reducing length of stay.3,11,21,22 Consistent with these findings, our population demonstrated significant reduction in MICU length of stay.
It is worth noting that the overall use of laxative agents increased following implementation of our protocol, led primarily, but not exclusively, by our targeted agents (ie, polyethylene glycol and sennoside-docusate). The rise in administration from 31.5% to 65% reflects strong adoption of the protocol and integration into routine care. Increased laxative usage occurred quickly after implementation and was sustained throughout the study period. Though increased usage falls below universal usage, this is explained by the ability of providers to discontinue these orders and for admitted individuals to refuse these medications. These improvements combined with the significant decrease in time to first administration highlight both the feasibility and durability of the intervention, features that demonstrate its ability to easily be implemented at additional ICUs.
Furthermore, use of rescue therapies (eg, bisacodyl suppositories, enemas) and escalating promotility agents declined post-intervention. This suggests that early, structured bowel management may decrease the need for more invasive therapies, aligning with patient comfort while optimizing healthcare resources.
A reduction in median time to first bowel movement was also observed, which was positively correlated with laxative administration prior to the intervention (r = 0.42), potentially indicating that earlier initiation of laxatives may promote GI transit. Although this association weakened post-intervention (r = 0.12), this may reflect the increasing influence of patient-specific factors on bowel function once early administration of laxatives becomes standard. Given that total gastrointestinal transit is highly variable in the healthy ambulatory population, it is more than likely that this variability will be accentuated by critical illness. It is also likely that there are a number of currently undefined factors which contribute to interindividual variations in total gastrointestinal transit in the MICU. This illustrates a barrier of protocol-driven prophylaxis in its ability to overcome the complex, multifactorial nature of dysmotility in critically ill patients.
We also observed a notable reduction in MICU length of stay by nearly one full day. However, similar to previously published studies, there was no corresponding reduction in incidence of delayed defecation. This may be explained by many factors. First, the lack of consensus regarding definition of impaired defecation in the ICU may play a role.3,8,9 We used the commonly agreed upon duration of 72 h however, this may not be sufficient to capture the true GI dysfunction present in critical illness. Additionally, delayed defecation alone may not be sufficient to capture the spectrum of GI dysfunction. Indeed, a multitude of factors influence the duration of MICU admission including illness severity, therapeutic interventions, hospital census among others. It is worth noting that pre and post intervention groups had equivalent illness severity (as assessed by admission SOFA score), age, sex distribution, and admitting diagnosis. Moreover, both groups entered the MICU with similar distributions of therapeutic interventions, having nearly equal rates of ventilator, vasopressor, and opioid infusion. It would be tempting to consider that the reduced length of stay was due to unequal numbers of deaths in each of the groups, however, this was not the case. All other factors being equal, the only significant change between pre and post intervention groups was the implementation of these laxative agents. There may still be other unmeasured factors, however, for the major predictors of MICU length of stay, no convincing differences exist between our groups. Anecdotally, return of bowel function is often of interest to clinicians and facilitating this with laxatives may be a potential driver of reduced length of stay acting outside of a biological mechanism. Further study is required to understand the psychology of clinicians in this regard. Nonetheless, the reduction in both MICU length of stay and the need for rescue promotility agents suggests that our intervention meaningfully influenced the clinical outcome of MICU length of stay. While constipation may not have met the strict ESICM definition, the GI dysfunction seen within the MICU and potentially ameliorated by prophylactic laxative regimens may still be clinically significant.
There are some limitations with our study. The laxative regimen of polyethylene glycol and sennoside-docusate was selected based on general guidelines for treatment of constipation in the ambulatory setting as no guidelines for the treatment of this condition in the inpatient population exist at the time of writing, but may not be the ideal regimen for critically ill patients. Additionally, imprecision in documentation of bowel movements may have introduced measurement bias. Moreover, as a single-center study generalizability is limited. Multi-center evaluations are warranted to validate these findings and identify patient-specific characteristics that may affect outcomes, such as ethnic and socioeconomic differences. Furthermore, outcomes may have been influenced by unmeasured confounders, such as diet, mobility, or concurrent medications. Future research should explore patient-centered outcomes including patient discomfort, the presence of ileus, and the need for diagnostic abdominal imaging.
Footnotes
Acknowledgements
The authors would like to acknowledge critical assistance from Sean Johnston, Rosemary Swanke, and Joseph Bahgat in the implementation of this project.
Author Contributions
CJC: Conceived project, designed protocol, compiled and analyzed data and manuscript; RH: Compiled and analyzed data and manuscript; RF: Supervised manuscript creation and assisted in project conception.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.