
Abstract
Background
Acute kidney injury (AKI) is associated with high morbidity and mortality in critically ill patients. Multicenter analyses describing the epidemiology of AKI in the cardiac intensive care unit (CICU) are scarce. Here, we describe the prevalence, predictors, and outcomes associated with AKI in a contemporary multicenter CICU population.
Methods
The Critical Care Cardiology Trials Network (CCCTN) is a collaboration of CICUs in North America coordinated by the TIMI Study Group (Boston, MA). We evaluated patient and hospital-level outcomes as a function of creatinine-only Kidney Disease: Improving Global Outcomes (KDIGO) AKI stage within the CCCTN registry. Logistic regression was used to assess associations with in-hospital mortality.
Results
Among 21 603 admissions, the overall prevalence of AKI was 23.7%, which was composed of KDIGO stage 1: 12.7%, stage 2: 1.7%, and stage 3: 9.2%. A higher prevalence and severity of AKI were seen in patients with baseline kidney disease, hypertension, or diabetes and in admissions with heart failure, cardiogenic shock, and cardiac arrest (P < .001 for all). There was a stepwise increase in hospital mortality across AKI stages (stage 1: 23%, stage 2: 39%, stage 3: 42%; P < .0001). The increased risk of death associated with progressive AKI stage persisted after multivariate adjustment (adjusted OR: stage 1: 2.1, stage 2: 3.7, stage 3: 3.4).
Conclusions
AKI occurs in 1 in 4 admissions to the CICU, and a higher AKI stage is incrementally associated with in-hospital mortality, highlighting a need to develop strategies to mitigate AKI and its complications.
Keywords
Key Points
1-in-4 CICU admissions developed acute kidney injury, and approximately 9%, or one-in-ten admissions, will develop severe kidney injury.
Over half of patients with stage III AKI needed renal replacement therapies.
Stage III AKI is associated with more than 40% total in-hospital mortality.
Introduction
Acute kidney injury (AKI) is common in critically ill patients with cardiovascular disease.1,2 High variability in the reported prevalence of AKI likely reflects differences in patient population, type of intensive care unit (ICU), concomitant diagnoses, overall severity of illness, and the definition of AKI.3–6 AKI is an important manifestation of end-organ dysfunction, and its presence is associated with poor prognosis.6–10 The epidemiologic data regarding AKI in cardiac ICU (CICU) patients are limited and derived primarily from retrospective single-center studies that may not sufficiently represent the broader CICU population.10–14 Moreover, published data regarding risk factors, admission diagnoses, ICU resource utilization, and hospital mortality in patients who develop AKI in the CICU are scarce.
The Critical Care Cardiology Trials Network (CCCTN) Registry is a multi-center, prospective registry of CICU admissions in North America. The CCCTN Registry has been leveraged to describe the utilization and outcomes of acute renal replacement therapy (RRT) in CICU patients, observing high in-hospital mortality in patients requiring RRT.11,15 In the present analysis, we sought to examine the full range of acute kidney dysfunction in this population and better characterize the prevalence and risk of mortality across the spectrum of AKI severity.
Methods
Study Population
The CCCTN is a research network of predominantly American Heart Association Level 1 CICUs; 42 centers contributed data to this analysis. The methods of the CCCTN Registry have been reported.16,17 Participating centers capture all consecutive medical CICU admissions during 2-month annual collection cycles. In addition, some centers contribute all consecutive admissions year-round. All available data from 2017 to 2022 were included in this analysis. The TIMI Study Group (Boston, MA) is the coordinating center and provides scientific oversight to the network. Local institutional review boards approved the CCCTN Registry protocol and waiver of informed consent at each participating site.
Data Collection
We assigned a modified Kidney Disease: Improving Global Outcomes (KDIGO) AKI stage during the CICU stay based on baseline (first collected at CICU admission) and peak serum creatinine during the CICU stay or need for new renal replacement therapy (RRT) based on the following creatinine-only criteria: Stage 0: no AKI; Stage 1: increase of creatinine ≥1.5× to <2× of baseline or change of >0.3 mg/dL from baseline; Stage 2: Increase of creatinine ≥2× to <3× of baseline; Stage 3: increase of creatinine ≥3× from baseline, >4 mg/dL at any point, or initiation of RRT during CICU stay; urine output data were not available and could not be used to assign AKI stage.12,18 The KDIGO classification used for this data is described in detail in Supplemental Table S1. Regardless of CKD history, Staging AKI used the same criterion: the absolute change in serum creatinine from baseline to peak during the CICU stay. We excluded all patients with a history of end-stage kidney disease (ESKD) and patients for whom an admission (baseline) serum creatinine level was unavailable. Sequential organ failure assessment (SOFA) scores during the first 24 h after CICU admission are captured for all patients. 19 We elected to use the SOFA score in this study because it was uniformly collected across all CCCTN sites and was used in our risk-adjusted models.
Data Analysis
All descriptive analyses were stratified by KDIGO criteria. Descriptive statistics were presented as median with interquartile range (IQR) for continuous outcomes and frequency with percentage for categorical outcomes. Testing for the significance of differences between study groups was based on nonparametric tests unless otherwise stated. The association of hospital mortality with categorical AKI stages was assessed by estimating odds ratios using logistic regression adjusting for baseline covariates. Those baseline covariates included age, sex, history of CKD, history of heart failure, cardiac arrest at CICU admission, shock at CICU admission, prior percutaneous coronary intervention (PCI), invasive mechanical ventilation, mechanical circulatory devices, and a maximum number of inotropes/vasopressors for shock management. The association of hospital mortality with continuous predictors, including serum creatinine, was evaluated by fitting flexible logistic regressions with natural cubic splines of the continuous predictor variables. We performed a multivariable logistic regression using backward model selection (α = 0.05) to identify independent predictors of AKI. Candidate covariates included age, sex, race, body mass index, history of diabetes mellitus, hypertension, heart failure, severe liver disease, severe valvular heart disease, initial diagnosis of ACS, cardiac arrest prior to or at admission, cardiogenic shock, invasive mechanical ventilation, and SOFA score. We also conducted a sensitivity analysis with mechanical circulatory support (MCS) as a candidate predictor. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC).
Results
Among a total of 22 869 medical CICU admissions, we excluded 1202 admissions with end-stage kidney disease (ESKD) and 64 admissions for whom baseline serum creatinine was unknown. Among 21 603 eligible admissions, the median age was 67 years (25th - 75th percentiles: 56-76 years), 63.4% were males, and 70.4% were Caucasian. The most common primary admission diagnoses were acute coronary syndrome (ACS; 31.7%), shock (27.5%), heart failure (19.6%), and cardiac arrest (11.2%).
Comparison of Admissions with and Without Acute Kidney Injury
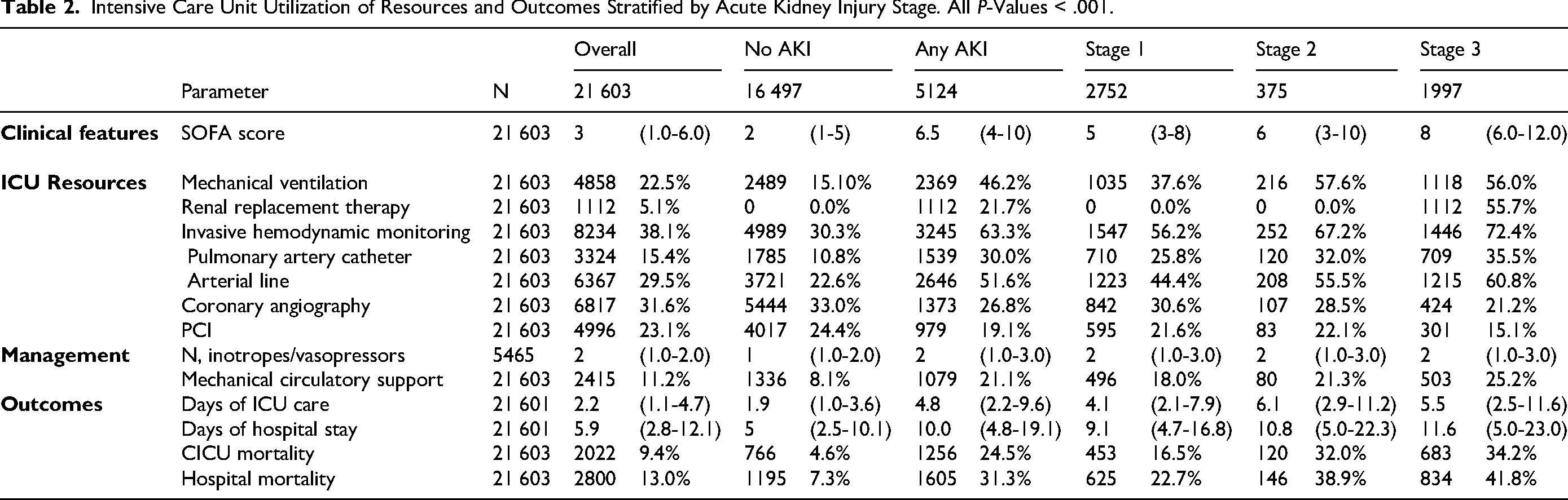
A total of 5124 (23.7%) admissions met the criteria for AKI during the CICU stay (Figure 1). Admissions with any AKI more frequently had comorbid hypertension, heart failure, diabetes mellitus, coronary artery disease, and chronic kidney disease as compared to admissions without AKI (Table 1). Admissions with any AKI were more commonly admitted with heart failure and cardiogenic shock and less often admitted with ACS, as compared to admissions with no AKI (Figure 2A). More PCI procedures were performed in admissions with no AKI compared to admissions with AKI. In contrast, any AKI was associated with more mechanical ventilation, invasive hemodynamic monitoring, and more use of mechanical circulatory support devices (Table 2).
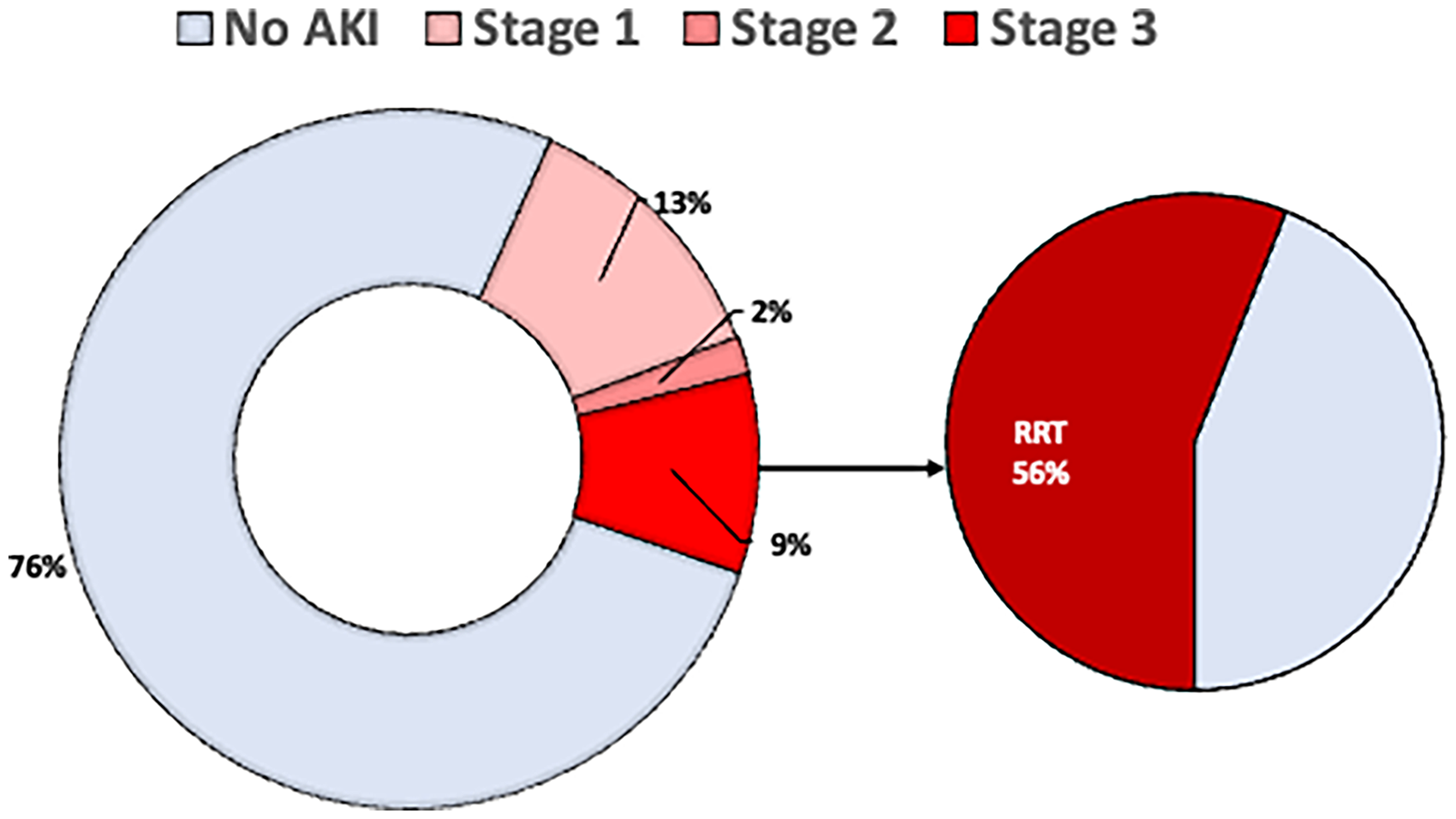
Percent stages of Kidney Disease Improving Global Outcomes (KDIGO) acute kidney injury (AKI) in all admissions. A total of 21 603 admissions were included in this study.
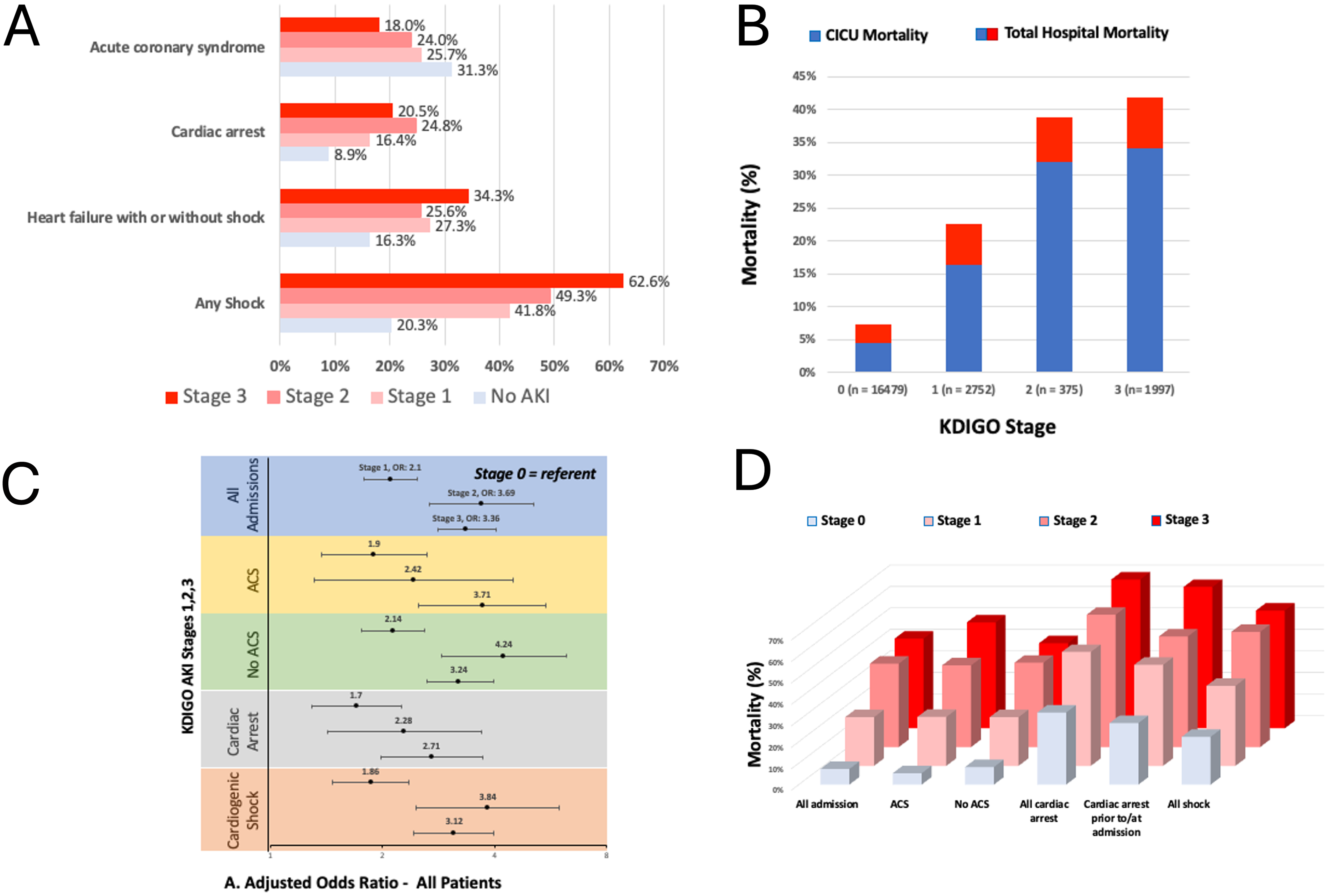
A. The proportion of admissions with select diagnoses stratified by acute kidney injury stage (AKI). B. Relationship between acute kidney injury stage and mortality for all admissions. CICU, Cardiac Intensive Care Unit; KDIGO, Kidney Disease Improving Global Outcomes. C. Adjusted odds ratios for hospital mortality by categorical acute kidney stage are presented among all admissions and within subgroups based on admission diagnosis. The logistic regression model includes covariates of age, sex, co-morbid chronic kidney disease, comorbid heart failure, cardiac arrest or shock before admission, prior percutaneous intervention, use of invasive mechanical ventilation, mechanical support device, and number of vasoactive agents administered for shock. ACS, Acute Coronary Syndrome; KDIGO, Kidney Disease Improving Global Outcomes. D. Hospital mortality stratified by acute kidney injury stage and admission diagnoses. ACS, Acute Coronary Syndrome.
Demographics Stratified by Acute Kidney Stage. All Values are Reported in Median (25th-75th Percentiles) or N, % Where Appropriate. Percentages are Reported per Acute Kidney Injury (AKI) Stage.
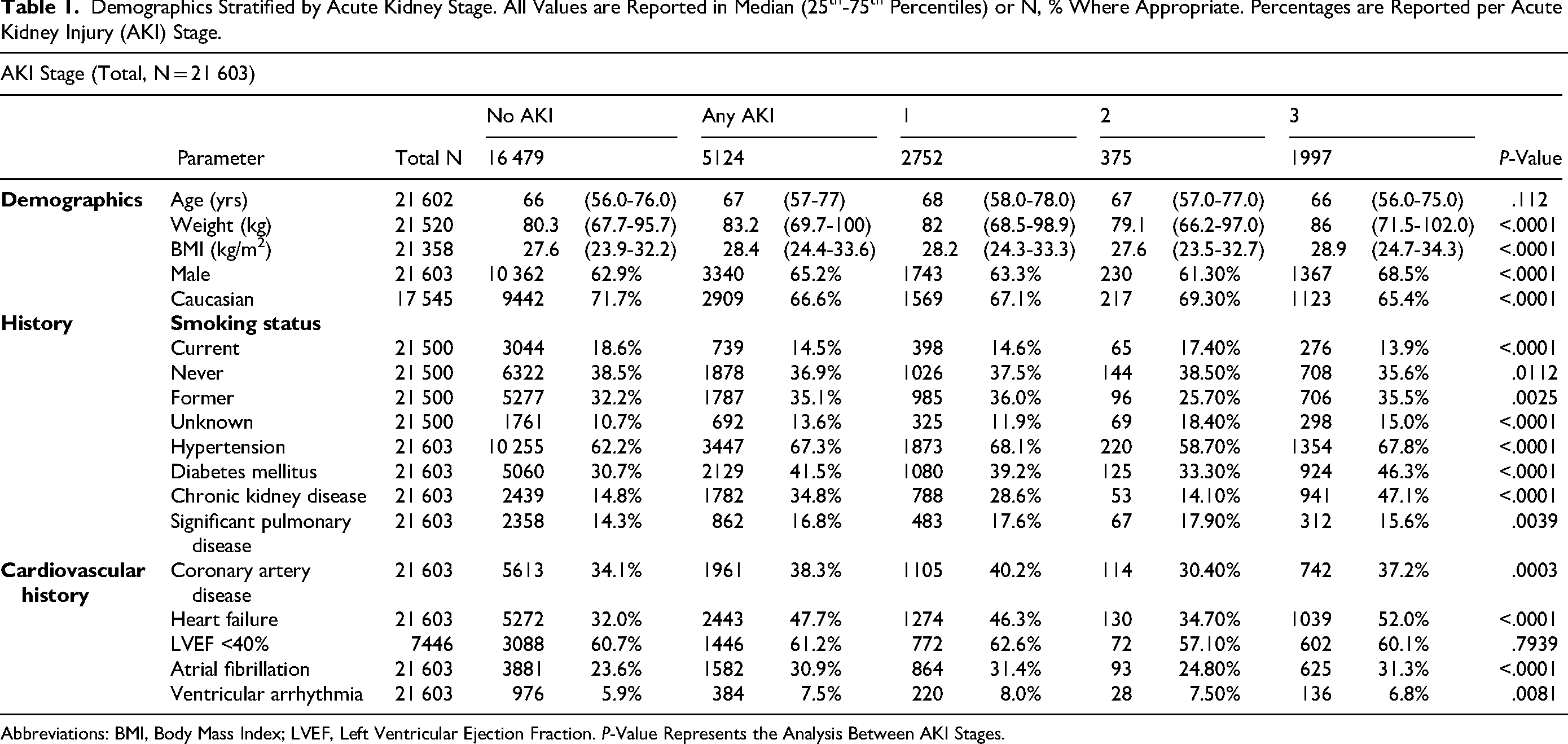
Abbreviations: BMI, Body Mass Index; LVEF, Left Ventricular Ejection Fraction. P-Value Represents the Analysis Between AKI Stages.
Intensive Care Unit Utilization of Resources and Outcomes Stratified by Acute Kidney Injury Stage. All P-Values < .001.
Outcomes by KDIGO Stage
Among the 5124 admissions that met criteria for AKI diagnosis, 2752 (12.7%) admissions had stage 1 AKI, 375 (1.7%) admissions had stage 2 AKI, and 1997 (9.2%) admissions had stage 3 AKI. Renal replacement therapy was used in approximately 5% (N = 1112) of all CICU admissions (ie, AKI-D), and over half of patients with stage 3 AKI. The baseline characteristics stratified by the KDIGO stage are shown in Table 1. The median baseline creatinine in all patients was 1.1 mg/dL (1.0-2.0 mg/dL), with a stepwise association in peak creatinine at each KDIGO stage: stage 0: 1.1 mg/dL (0.9-1.5), stage 1: 1.9 mg/dL (1.5-2.5), stage 2: 2.6 mg/dL (1.9-3.1), and stage 3: 4.5 mg/dL (3.5-5.7). Compared to stage 1 AKI, admissions with stage 3 AKI had higher rates of co-morbid diabetes mellitus, chronic kidney disease, heart failure, and were more frequently admitted with more cardiac arrest, heart failure, cardiogenic shock, and general medical problems in patients with cardiac disease. More admissions with stage 1 AKI presented with ACS compared to stage 3 AKI (Figure 2A). Table 3 reports admission diagnoses and risk of AKI stratified by the KDIGO stage. Compared to admissions with stage 1 AKI, those with stage 3 AKI underwent less PCI but had increased mechanical ventilation, invasive hemodynamic monitoring, and mechanical circulatory support device utilization (Table 2). Admissions with stage 3 AKI had higher SOFA scores, ICU days, and hospital length of stay as compared to stage 1 AKI. Higher serum lactate and both lower hemoglobin and pH were also associated with a higher KDIGO stage (
Distribution of Acute Kidney Injury KDIGO Stages among Cases with Select Admission Diagnoses.

Independent Predictors of AKI
Using a multivariable logistic regression analysis with backward selection (α = 0.05), several factors were independently associated with AKI development (Table 4). The strongest predictor was severity of illness as demonstrated by the SOFA score (excluding kidney components, OR 2.13 per 4-point increase, 95% CI 2.02-2.24, P < .001). Invasive mechanical ventilation (OR 2.10, 95% CI 1.9-2.32, P < .001), history of heart failure (OR 1.44, 95% CI 1.22-1.56), diabetes mellitus (OR 1.33, 95% CI 1.22-1.44), cardiogenic shock at admission (OR 1.33, 95% CI 1.22-1.46), higher body mass index (OR 1.12 per 7 kg/m2 increase, 95% CI 1.08-1.16), and hypertension (OR 1.12, CI 1.03-1.22) were also independently associated with AKI development. Non-white race was also associated with a higher risk of AKI development (Black vs White: OR 1.38, 95% CI 1.26-1.52; Other vs White: OR 1.45, 95% CI 1.27-1.66). A sensitivity analysis that included MCS as a candidate predictor yielded similar results, with MCS as an independent predictor of AKI development (Supplement Table S3)
Multivariable Logistic Regression for AKI.
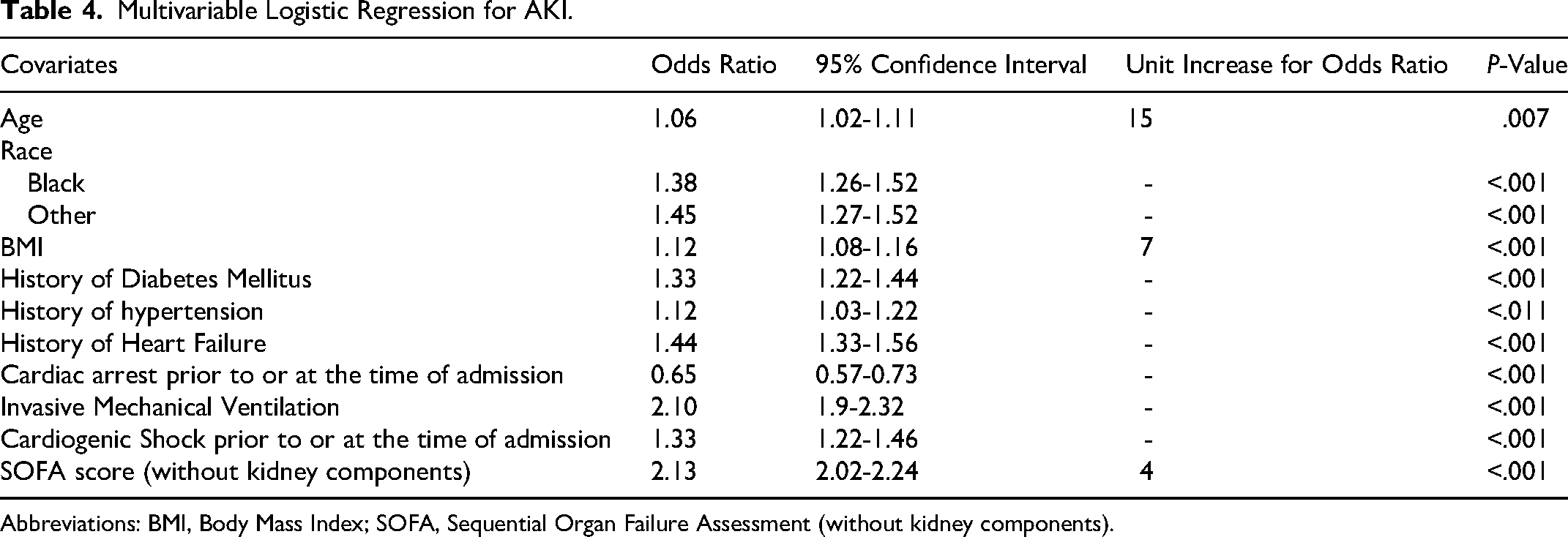
Abbreviations: BMI, Body Mass Index; SOFA, Sequential Organ Failure Assessment (without kidney components).
Mortality in Patients with AKI in the CICU
There were 2800 (13.0%) in-hospital deaths in this cohort, including a 9.4% CICU mortality rate. There was a stepwise graded relationship between stages of AKI and hospital mortality (P < .001; Figure 2B). The risk of in-hospital death exceeded 40% for admissions that developed stage 3 AKI. Approximately one in four admissions with AKI died during the hospitalization as compared to 4.6% of patients without AKI (P < .0001). In the overall population, the adjusted odds of death increased stepwise by stage of AKI (Figure 2C). This pattern was consistent among admissions with and without ACS, cardiac arrest, or shock (Figure 2D). The probability of in-hospital death increased with rising percentage change in creatinine from baseline to peak (Figure 3). A stepwise relationship was noted between in-hospital and CICU death and increased per baseline changes in eGFR (Supplemental Figure S1). Sensitivity analyses among admissions with a baseline eGFR ≥ 60 mL/min/1.73 m2 demonstrated similar findings (Supplemental Figure S2).
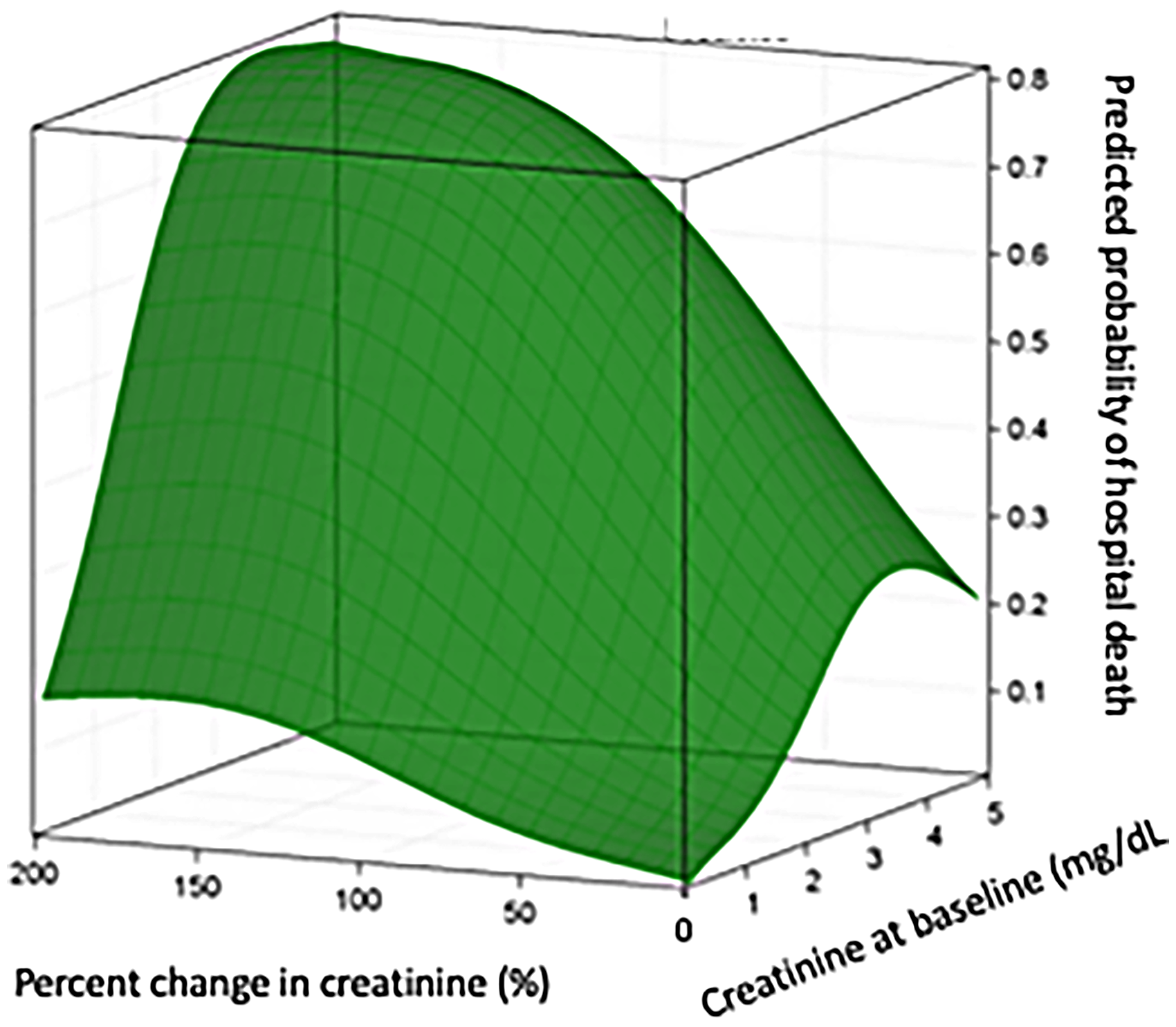
Spline association of probability of hospital death versus percent change in creatinine from baseline to worst creatinine.
Discussion
We aimed to address the knowledge gap regarding the epidemiology and outcomes of AKI in the contemporary CICU using the multicenter CCCTN Registry. We found that AKI developed during the CICU stay in approximately one-quarter of admissions to the CICU, and 9% of admissions developed Stage 3 AKI, among whom 56% received RRT (ie, AKI-D). Admissions with more severe AKI had longer CICU and hospital lengths of stay, more acidemia, increased lactate, higher SOFA scores, and a greater need for advanced ICU therapies. We observed a graded stepwise association between AKI stage and in-hospital mortality, with a 42% absolute risk of in-hospital death among patients with Stage 3.
Prevalence of AKI in the CICU and Association with Admission Diagnoses
Prior retrospective single-center studies reported a prevalence of AKI during CICU stay and hospitalization ranging between 30-50%, including 15% having stages 2 and 3 AKI.9,12,20 We demonstrate a total prevalence approaching 24% during CICU stay, with approximately 11% having stages 2 and 3 AKI. Interestingly, few patients met criteria for stage 2 AKI, implying that many such patients ultimately progressed to stage 3 AKI. While we did not have data regarding the prevalence of AKI during the entire hospital stay, presumably, this proportion may be even higher. Our study provides a more comprehensive assessment of this epidemiology within North America's largest dedicated prospective registry of CICU patients.
The prevalence of AKI in CICU admissions is limited to single-center studies. Jentzer and colleagues found a higher prevalence of AKI, but as in our analysis, more patients with stage 3 AKI were admitted with heart failure, cardiac arrest, and shock. 12 Similarly, in our analysis, underlying chronic kidney disease, admission diagnosis of a general medical problem with underlying cardiac disease, shock, cardiac arrest, and heart failure were more prevalent in stage 3 AKI. Our study builds on prior studies by demonstrating that approximately one in three admissions with cardiogenic shock, cardiac arrest, or heart failure develop stage 3 AKI. These studies emphasize the importance of AKI as a component of multi-organ failure in critically ill CICU patients, commonly associated with shock and respiratory failure.
AKI in the CICU likely reflects multiple mechanisms that vary by diagnosis. In patients with cardiogenic shock or acute decompensated heart failure, the mechanism of AKI could be related to decreased renal perfusion and increased renal venous congestion (ie, cardiorenal physiology) in addition to various neurohormonal activation pathways and exposure to various medications (ie, diuretics). 21 In cardiac arrest patients, AKI could be from global ischemic or reperfusion injury. 22 In patients with infections or acute inflammatory states, kidney injury may result from tubular necrosis in the setting of systemic inflammation and hemodynamic instability. 23 In patients with ACS undergoing coronary angiography, intra-arterial contrast injections may contribute to kidney injury. Our multivariable analysis of AKI predictors supports a multi-mechanistic framework for the development of AKI, where the strongest independent predictors were markers of acute illness severity (ie, SOFA score and mechanical ventilation), while established risk factors for kidney injury (ie, diabetes, hypertension, obesity, and heart failure) were also independently retained in the model. This pattern suggests that AKI in the CICU arises principally from acute hemodynamic and inflammatory insults superimposed on reduced baseline renal reserve, rather than any single mechanistic entity. Our results may further explain the diagnosis specific variations in the Aki epidemiology observed in this cohort.
Independent Predictors of AKI in the CICU
To our knowledge, this is the first multicenter logistic analysis to identify independent predictors of AKI in the CICU. The SOFA score (excluding kidney components) and mechanical ventilation were the strongest predictors of AKI, underscoring the role of multiorgan dysfunction and illness severity in driving AKI. In a sensitivity analysis, MCS was also independently associated with AKI development. 24
Stages of AKI and Associations with Outcomes
Our findings are consistent with prior retrospective studies that demonstrate that higher stages of AKI are associated with worse prognosis (ie, longer hospital/CICU length of stay, higher rates of mortality). In a study by Holland and colleagues, AKI was associated with an 85% higher risk of death among CICU patients. 20 Our data extend upon these results by categorizing the risk of mortality by AKI stage, revealing a 1.9-fold higher mortality risk for mild (stage 1) AKI and 3.7-fold higher risk for all admissions with stage 3 AKI. In admissions with an initial eGFR ≥60 mL/min/1.73 m2, there is a four times higher risk of death with stage 3 AKI. Admissions with normal eGFR who develop stage 3 AKI after presenting with acute coronary syndrome, cardiogenic shock, and cardiac arrest have a three to six times higher risk for death. These novel data suggest that stage 3 AKI portends high mortality in all patients admitted to the CICU, especially those with ACS, cardiac arrest, and shock. This finding is consistent with our prior analysis from the CCCTN Registry, showing poor outcomes in patients who required RRT (a group that accounted for more than half of our Stage 3 AKI patients). 15 Notably, Stage 3 AKI patients, those meeting creatinine criteria, and those requiring RRT, may represent a more severely ill subgroup. A dedicated analysis comparing the outcomes between RRT and non-RRT stage 3 AKI patients warrants further investigation.
While the prevalence of AKI in the broader cohort of patients with ACS is well-established, the available evidence on AKI in patients with ACS in the CICU is limited. 8 Jentzer and colleagues demonstrated that the prevalence of AKI was lowest in CICU patients with ACS when compared to other admission diagnoses. 12 A prior study demonstrated a 15.8% incidence of AKI in unselected patients with ACS (including those without critical illness) and found that AKI was associated with an increased risk of mortality. 8 We demonstrate that approximately one in five patients with ACS develop any AKI, which is lower than in prior CICU studies but exceeds the broader cohort of ACS patients. 8 The prevalence of stage 3 AKI is approximately 6% in the ACS subgroup. However, Stage 3 AKI increases the risk of death by over six-fold in these patients. The use of coronary angiography and PCI did not appear to be associated with a higher prevalence of AKI; indeed, these procedures were utilized less often in patients who developed severe AKI, which could represent reverse causation. Although we lack information on the etiology of AKI, the lack of an association between coronary angiography and PCI with AKI would seem to argue against contrast-associated AKI being the predominant mechanism of AKI in our CICU patients. Mechanisms of AKI in the CICU population are complex and typically multi-factorial, with acute tubular necrosis from hypotension/hypoperfusion, renal vasoconstriction, neurohormonal modification, nephrotoxic drugs, and venous congestion often each playing a role.8,25,26 Given the associations between circulatory failure and cardiac arrest, the core causes likely include hypoperfusion and cardiorenal mechanisms. The potential effects of PCI or coronary angiography on AKI cannot be further elucidated from our study due to limited sample size, unknown timing/duration of the procedure, and lack of information regarding contrast-agent use.
Limitations
This study has several limitations. The most significant limitation of this analysis is that historical outpatient creatinine is not collected in the registry. This limitation could have reduced our sensitivity for AKI that was present on CICU admission, leading our findings to be a conservative estimate of the prevalence of AKI. Co-morbid CKD was noted to be close to 35% in admissions with AKI; however, the severity of prior CKD is not collected in this registry. In addition, urine output is not collected and, therefore, cannot be used as an additional criterion for the KDIGO stage, as urine output is known to be complementary to creatinine changes for identifying AKI and determining AKI prognosis. Because urine output and outpatient baseline creatinine values were unavailable, we defined AKI using the trajectory of creatinine during the CICU stay, with admission creatinine as baseline compared to peak creatinine. However, several other studies have similarly used admission creatinine as a baseline marker and demonstrated changes in creatinine as markers of AKI to define the modified KDIGO stages.12,27 Furthermore, we focused only on AKI development during the CICU stay. We cannot comment on late AKI occurring during hospitalization after CICU discharge, a time period that accounted for many cases in some studies. Finally, some patients may have died before meeting the criteria for AKI.12,28 While the large, prospective multicenter cohort comprising the CCCTN Registry is an important strength of our analysis, the registry composition of primarily Level 1 CICUs from the United States and Canada may limit the ability to generalize to other healthcare settings, countries, or underrepresented regions.
Conclusions
In a large registry of tertiary and quaternary hospital centers, we observed that AKI occurs in one in four CICU admissions, and over thirty percent of admissions with shock, cardiac arrest, or heart failure develop Stage 3 AKI during the CICU stay. Stage 3 AKI is associated with a three-to-four-fold increase in the risk of hospital death. These data suggest that strategies to mitigate the risk of AKI and its harmful consequences in the CICU are needed. Further research to understand the mechanisms and therapies for AKI in CICU patients is also warranted to identify treatments that may reduce the risk of adverse outcomes in patients with AKI.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261440201 - Supplemental material for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network
Supplemental material, sj-docx-1-jic-10.1177_08850666261440201 for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network by Narayana Sarma V. Singam, MD, Mitchell Padkins, MD, Alexander I. Papolos, MD, Benjamin B. Kenigsberg, MD, David Berg, MD, MPH, Jason N. Katz, MD, Sean van Diepen, MD, MSc, Alexandra K. Steverson, MD, MPH, Scott W. Rose, MD, Jeffrey Wang, MD, Erin A. Bohula, MD, DPhil, Jeong-Gun Park, PhD, David A. Morrow, MD, MPH, Gregory W. Barsness, MD, and Jacob Colin Jentzer, MD in Journal of Intensive Care Medicine
Supplemental Material
sj-tiff-2-jic-10.1177_08850666261440201 - Supplemental material for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network
Supplemental material, sj-tiff-2-jic-10.1177_08850666261440201 for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network by Narayana Sarma V. Singam, MD, Mitchell Padkins, MD, Alexander I. Papolos, MD, Benjamin B. Kenigsberg, MD, David Berg, MD, MPH, Jason N. Katz, MD, Sean van Diepen, MD, MSc, Alexandra K. Steverson, MD, MPH, Scott W. Rose, MD, Jeffrey Wang, MD, Erin A. Bohula, MD, DPhil, Jeong-Gun Park, PhD, David A. Morrow, MD, MPH, Gregory W. Barsness, MD, and Jacob Colin Jentzer, MD in Journal of Intensive Care Medicine
Supplemental Material
sj-tiff-3-jic-10.1177_08850666261440201 - Supplemental material for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network
Supplemental material, sj-tiff-3-jic-10.1177_08850666261440201 for Acute Kidney Injury and Outcomes in the Cardiac Intensive Care Unit: Insights from the Critical Care Cardiology Trials Network by Narayana Sarma V. Singam, MD, Mitchell Padkins, MD, Alexander I. Papolos, MD, Benjamin B. Kenigsberg, MD, David Berg, MD, MPH, Jason N. Katz, MD, Sean van Diepen, MD, MSc, Alexandra K. Steverson, MD, MPH, Scott W. Rose, MD, Jeffrey Wang, MD, Erin A. Bohula, MD, DPhil, Jeong-Gun Park, PhD, David A. Morrow, MD, MPH, Gregory W. Barsness, MD, and Jacob Colin Jentzer, MD in Journal of Intensive Care Medicine
Footnotes
Contributions
Narayana Sarma V. Singam MD – Conceptualizing, methodology, writing – original draft, visualization
Mitchell Padkins MD – writing – review and editing
Alexander I. Papolos MD - writing – review and editing
Benjamin B. Kenigsberg MD - writing – review and editing
David Berg MD MPH - writing – review and editing
Jason N. Katz MD - writing – review and editing, supervision
Sean van Diepen MD MSc - writing – review and editing, supervision
Alexandra K. Steverson - writing – review and editing
Scott W. Rose MD - writing – review and editing
Jeffrey Wang M, - writing – review and editing
Erin A. Bohula MD DPhil - writing – review and editing
Jeong-Gun Park PhD – Data curation, formal analysis
David A. Morrow MD MPH, - Methodology, writing-original draft, supervision
Gregory W. Barsness MD - writing-review and editing, supervision
Jacob Colin Jentzer MD - Methodology, writing-original draft, supervision
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Berg and Dr Morrow are members of the TIMI Study Group, which has received institutional research grant support through Brigham and Women's Hospital from Abbott Laboratories, Abiomed, Amgen, Anthos Therapeutics, Arca Biopharma, AstraZeneca, Daiichi-Sankyo, Intarcia, Janssen, Merck, Novartis, Pfizer, Poxel, Quark Pharmaceuticals, Regeneron, Roche Diagnostics, Siemens, and Zora Biosciences. Dr Berg has received honoraria from the Medical Education Speakers Network and USV Private Limited; consulting fees from AstraZeneca, MobilityBio, Pfizer, and Youngene Therapeutics; and serves on clinical endpoint committees for studies sponsored by Beckman Coulter, Kowa Pharmaceuticals, and Tosoh Biosciences. Dr Morrow has received consulting fees from Abbott Laboratories, InCarda, Merck, Novartis, Regeneron, and Roche Diagnostics.
Dr Singam is a co-founder and co-owner of High Enroll LLC; this submission has no direct conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.