
Abstract
Background and Purpose
Mechanical ventilation (MV) occurs in a substantial subset of acute ischemic stroke (AIS) hospitalizations and is associated with worse outcomes, including prolonged hospital stay. Large national studies evaluating clinical predictors of MV and comparing regression with machine learning–based risk stratification in AIS remain limited. We examined clinical factors associated with MV in AIS and compared logistic regression with gradient-boosting approach for early respiratory risk stratification.
Methods
We analyzed 949,916 AIS hospitalizations from National Inpatient Sample (2016–2022). MV was identified using ICD-10 procedure codes and stratified by duration (<24 h, 24–96 h, >96 h). Demographics, comorbidities, treatment variables, and hemorrhagic transformation were compared between MV and non-MV groups. Multivariable logistic regression identified factors associated with MV. A simplified Ventilation Risk Score (sVRS) was derived from clinically relevant variables. Logistic regression and extreme gradient boosting (XGBoost) were trained on an 80/20 split and validated against a prolonged MV (>24 h) outcome. Model performance was assessed using AUC, Brier score, calibration, and SHAP analyses.
Results
MV occurred in 9.7% of hospitalizations; 83.7% were prolonged (>24 h). MV patients were younger and had higher prevalences of congestive heart failure, COPD, atrial fibrillation, chronic kidney disease, coagulopathy, liver disease, and hemorrhagic transformation (15.7% vs. 4.6%, P < .001). Endovascular thrombectomy was more frequent among MV patients and associated with shorter MV duration. The sVRS stratified patients into low-, intermediate-, and high-risk groups with MV rates of 3.65%, 9.25%, and 28.7%, respectively. Logistic regression achieved AUCs of 0.706 (all MV) and 0.711 (prolonged MV); XGBoost achieved 0.716 and 0.721. SHAP analyses identified coagulopathy, age, liver disease, congestive heart failure, and thrombectomy as top predictors.
Conclusion
MV identifies a clinically distinct AIS subgroup with greater comorbidity burden, higher hemorrhagic transformation rates, and longer hospitalizations. The sVRS provides graded, robust risk stratification supporting its use for early respiratory risk assessment in AIS.
Keywords
Introduction
Mechanical ventilation (MV) is often required in patients with acute ischemic stroke (AIS) and signifies a transition from isolated cerebral injury to systemic physiological compromise. Reported MV rates range from 6% to 20%, and the need for MV is consistently associated with longer hospitalizations, increased complications, and significantly higher mortality.1‐3 Patients may require ventilatory support because of impaired consciousness, aspiration, airway obstruction, respiratory muscle failure, or hemodynamic instability. Additionally, MV is frequently used to facilitate neurointerventional procedures such as mechanical thrombectomy, which has become central to contemporary AIS management. 4
Despite the clinical importance of MV in AIS, studies evaluating associated clinical characteristics have been limited. Earlier population-based work demonstrated that MV is linked to markedly increased mortality and resource utilization,2,3 while more recent multicenter cohorts have examined long-term outcomes, including one-year survival among ventilated stroke patients.5,6 Other studies have focused on prolonged ventilation in patients undergoing endovascular therapy. 7 However, comprehensive, contemporary analyses using nationally representative data to characterize factors associated with MV across the broader AIS population remain sparse.
Multiple comorbidities may contribute to respiratory failure in AIS, including congestive heart failure, chronic lung disease, atrial fibrillation, chronic kidney disease (CKD), coagulopathy, and hepatic dysfunction. Obesity-related abnormalities—such as impaired respiratory mechanics, reduced ventilatory reserve, and hypoventilation—may further increase the risk of MV in susceptible individuals.8‐10 Although such conditions are common in AIS patients, the degree to which they collectively influence MV risk in real-world practice is not well defined.
Prediction models for prolonged ventilation have been developed in other critical care settings, including after cardiac surgery11,12 and in general critical illness, 13 yet a practical, AIS-specific bedside tool to estimate the likelihood of requiring MV does not exist. Machine learning (ML) methods may provide complementary insights beyond traditional approaches by capturing nonlinear interactions among clinical variables, but their use in AIS respiratory risk prediction remains limited.
Using a large, nationally representative cohort of AIS hospitalizations from 2016–2022, we aimed to (1) characterize demographic and clinical differences between AIS patients who did and did not require MV; (2) identify variables associated with MV; (3) develop a simplified Ventilation Risk Score (sVRS) using clinically relevant predictors; and (4) compare the predictive performance of logistic regression with a gradient-boosting model. Our goal is to provide an updated, data-driven framework to support practical respiratory risk assessment in AIS.
Methods
This retrospective observational study used data from the National Inpatient Sample (NIS), Healthcare Cost and Utilization Project (HCUP), from 2016 through 2022. The NIS is a stratified all-payer inpatient database representing approximately 20% of U.S. hospitalizations and enables generation of national estimates through discharge sampling weights. All analyses followed HCUP methodological guidance.
Hospitalizations with a principal diagnosis of AIS were identified using ICD-10-CM codes I63.x and I66.x. Patients aged 18 to 90 years were included to minimize misclassification at extreme ages. Exclusions were applied for missing age, sex, discharge disposition, or invalid sampling weights. After all exclusions, the final analytic cohort included 949,916 unweighted AIS hospitalizations, representing approximately 4.7 million weighted discharges. MV was identified using ICD-10-PCS procedure codes 5A1935Z (<24 h), 5A1945Z (24–96 h), and 5A1955Z (>96 h). Any occurrence of these codes during hospitalization classified the encounter as MV-positive.
Demographic variables included age, sex, and race/ethnicity. Comorbidities were selected a priori based on physiologic plausibility and existing literature linking them to respiratory failure or critical illness in stroke populations. Specifically, conditions known to impair cardiopulmonary reserve (congestive heart failure [CHF], chronic obstructive pulmonary disease [COPD], atrial fibrillation, CKD), alter coagulation or hepatic function (coagulopathy, liver disease), or independently increase critical care risk (cancer, obesity, diabetes) were included. Cancer was identified using ICD-10-CM codes for malignant neoplasms (C00–C99), in situ neoplasms (D00–D09), and neoplasms of uncertain behavior (D37–D48). Immunocompromised states, restrictive lung disease, and neuromuscular disease were not included as separate variables due to heterogeneous ICD-10 coding patterns in administrative data that would limit reliable identification across years and institutions. All comorbidities were derived using ICD-10-CM definitions consistent with Elixhauser and Charlson classification systems. Hemorrhagic transformation (HT) was identified by the presence of secondary ICD-10-CM codes I61.x or I62.x in the AIS cohort. Treatment exposures were defined as intravenous thrombolysis (ICD-10 3E033 series) and mechanical thrombectomy (03CG3ZZ, 03CG4ZZ, 03CK3ZZ, 03CK4ZZ, 03CL3ZZ, 03CL4ZZ). Because treatment patterns can correlate with severity, these variables were analyzed strictly as treatment exposures and not as surrogates for stroke severity. Hospital region was categorized as Northeast, Midwest, South, or West. Length of stay (LOS) was calculated directly from discharge records.
Missing data for age, sex, discharge disposition, and sampling weights were excluded before cohort construction in accordance with HCUP guidelines. Variables with rare missingness (<1%), such as race, were retained in their recorded form without imputation. All multivariable and machine learning analyses were performed on complete-case data.
Descriptive statistics compared MV and non-MV groups. Categorical variables were evaluated using chi-square tests and continuous variables using t-tests or survey-weighted means. All comparisons in Table 1 are reported with P-values; significance was defined as P < .05.
Baseline Demographic, Clinical, and Treatment Characteristics Among Acute Ischemic Stroke Patients Stratified by Mechanical Ventilation Status. Values are Presented as Number (Percentage) or Mean (SD).
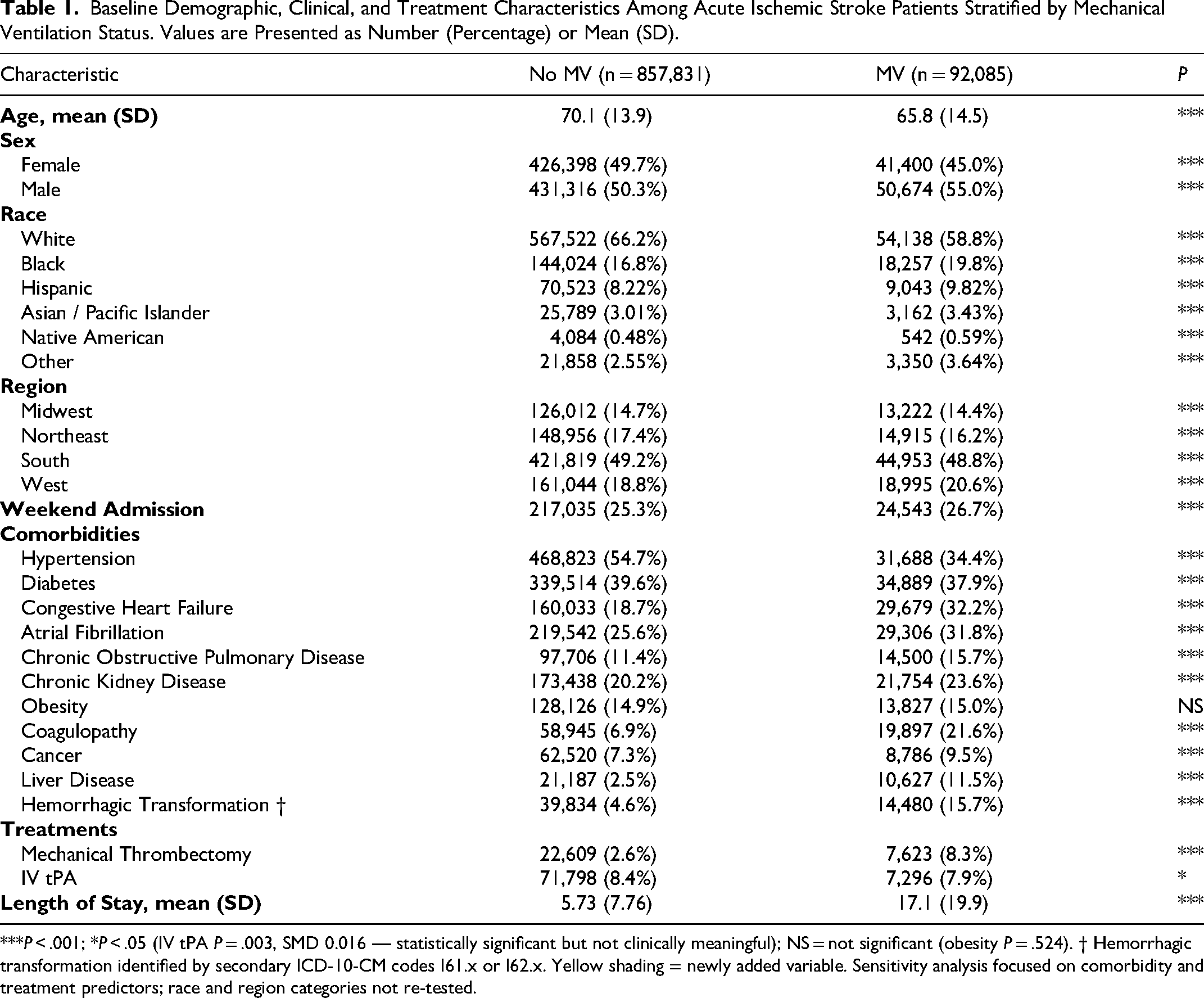
***P < .001; *P < .05 (IV tPA P = .003, SMD 0.016 — statistically significant but not clinically meaningful); NS = not significant (obesity P = .524). † Hemorrhagic transformation identified by secondary ICD-10-CM codes I61.x or I62.x. Yellow shading = newly added variable. Sensitivity analysis focused on comorbidity and treatment predictors; race and region categories not re-tested.
A multivariable logistic regression model was developed to estimate associations between clinical characteristics and MV. Predictors were selected a priori based on physiologic plausibility and existing literature. Adjusted odds ratios with 95% confidence intervals were reported.
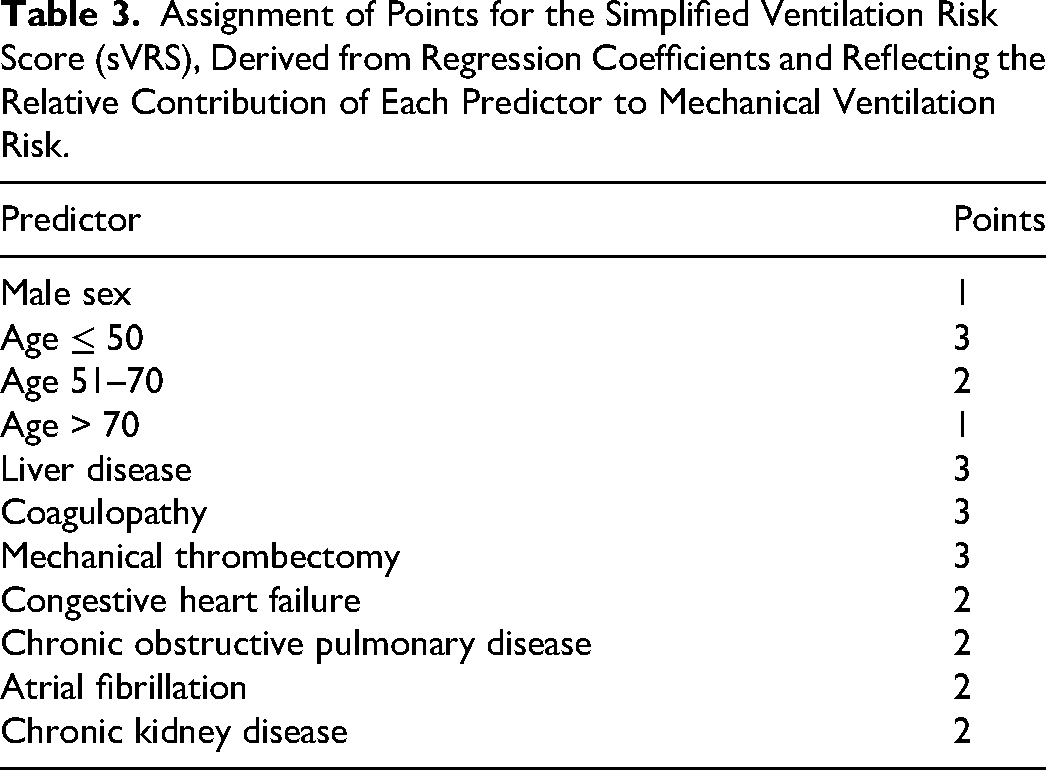
A simplified Ventilation Risk Score (sVRS) was derived from the logistic regression coefficients. Each β-coefficient was divided by the smallest clinically meaningful coefficient and rounded to the nearest integer. The total score was categorized into low-, intermediate-, and high-risk groups. Observed MV frequencies were computed for each category.
To address the clinical distinction between procedural and respiratory failure-related MV, a pre-specified sensitivity analysis was performed restricting the outcome to prolonged MV (>24 h), defined by codes 5A1945Z and 5A1955Z. This analysis included both logistic regression and XGBoost models, and results were compared with the primary (all MV) models. Additionally, an exploratory analysis examined the association between sVRS risk group and MV duration category, and a thrombectomy subgroup analysis assessed MV duration distribution and comorbidity profile differences between thrombectomy and non-thrombectomy MV patients.
Two supervised machine learning models were developed: logistic regression with regularization and gradient-boosted decision trees (XGBoost). The dataset was randomly split into a training set (80%) and a testing set (20%). Hyperparameters were optimized using five-fold cross-validation. Model performance was evaluated using the AUC, Brier score, and calibration characteristics. Feature contributions for XGBoost were assessed using Shapley additive explanations (SHAP).
All analyses were performed in R version 4.5.2 using the tidyverse, tidymodels, xgboost, SHAPforxgboost, and survey packages. Analytic code is available from the authors upon reasonable request. The NIS contains fully de-identified data and does not constitute human subjects’ research.
Results
Cohort Characteristics
The final analytic cohort included 949,916 AIS hospitalizations, of which 92,085 (9.7%) required MV and 857,831 (90.3%) did not. Of the 92,085 MV patients, 15,026 (16.3%) had short-duration MV (<24 h), 31,566 (34.3%) had intermediate duration (24–96 h), and 45,493 (49.4%) had prolonged MV (>96 h). In total, 77,059 patients (83.7% of all MV cases) had prolonged MV lasting more than 24 h. MV patients were younger (mean 65.8 ± 14.5 years vs 70.1 ± 13.9 years) and more frequently male (55.0% vs 50.3%).
Comorbidity burden was substantially higher among MV patients (Table 1). Coagulopathy occurred in 21.6% of MV encounters versus 6.9% of non-MV encounters, and liver disease in 11.5% versus 2.5%. CHF was present in 32.2% of MV cases versus 18.7% of non-MV cases, atrial fibrillation in 31.8% versus 25.6%, COPD in 15.7% versus 11.4%, and CKD in 23.6% versus 20.2%. HT was identified in 15.7% of MV patients compared with 4.6% of non-MV patients (P < .001; SMD 0.373), representing more than a threefold difference. Diabetes (37.9% vs 39.6%) and obesity (15.0% vs 14.9%, P = .524) differed minimally between groups. Mechanical thrombectomy was more common among MV cases (8.3%) compared with non-MV cases (2.6%). Length of stay differed substantially: MV cases averaged 17.1 ± 19.9 days compared with 5.73 ± 7.76 days in non-MV cases.
Predictors of Mechanical Ventilation
Multivariable logistic regression results are presented in Table 2. Liver disease demonstrated the strongest association with MV (adjusted OR 3.43; 95% CI 3.34–3.52; P < .001), followed by mechanical thrombectomy (adjusted OR 3.29; 95% CI 3.19–3.38; P < .001) and coagulopathy (adjusted OR 2.84; 95% CI 2.79–2.89; P < .001). CHF was associated with nearly double the odds of MV (adjusted OR 1.83; 95% CI 1.80–1.86; P < .001). COPD (adjusted OR 1.42), atrial fibrillation (adjusted OR 1.41), CKD (adjusted OR 1.10), and cancer (adjusted OR 1.10) were significant contributors (all P < .001). Age was inversely associated with MV (adjusted OR 0.977 per year; P < .001). Obesity demonstrated minimal clinical effect (adjusted OR 0.87; P < .001).
Adjusted Odds Ratios from Multivariable Logistic Regression Evaluating Demographic, Clinical, Comorbidity, and Treatment Predictors of Mechanical Ventilation in Acute Ischemic Stroke.
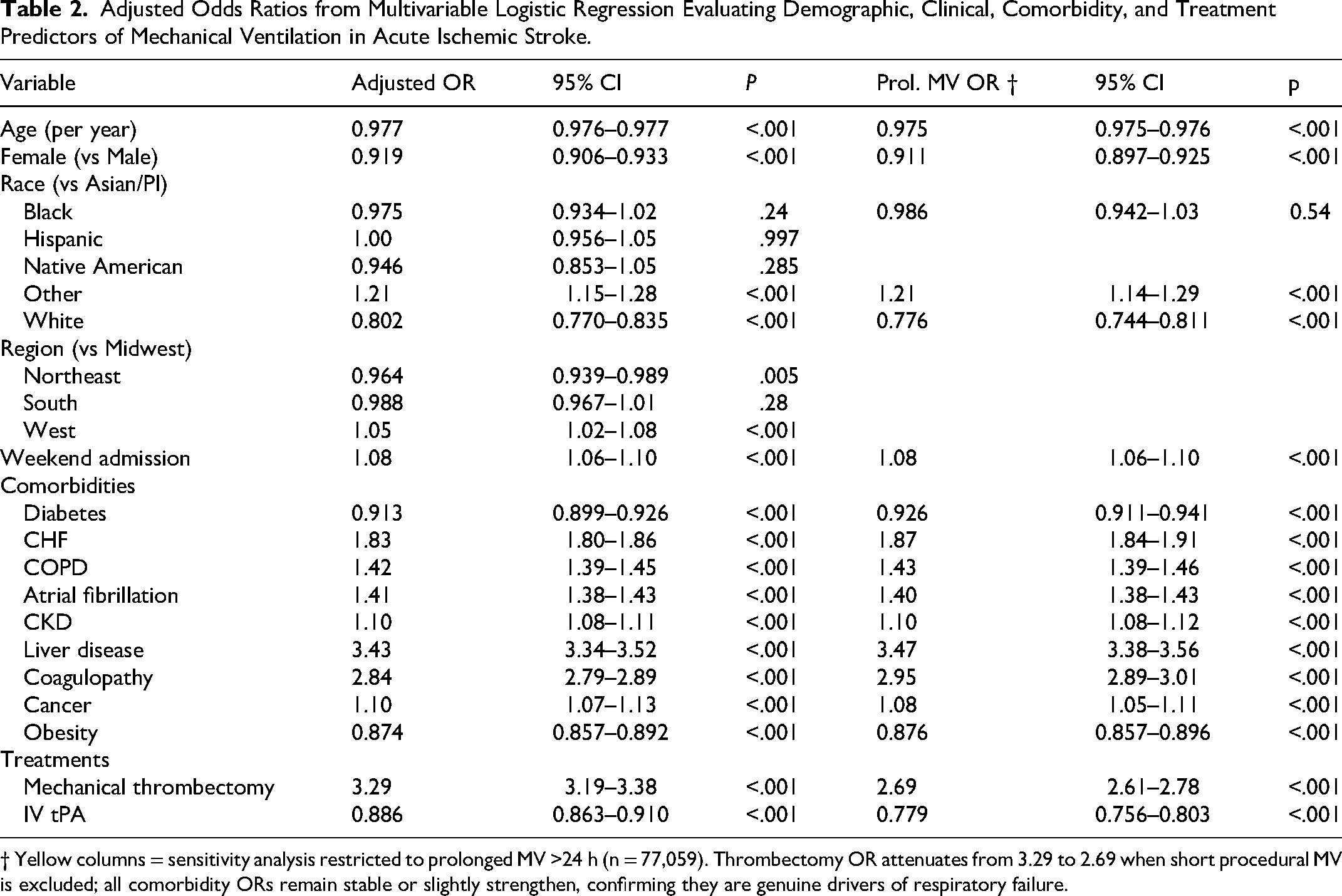
† Yellow columns = sensitivity analysis restricted to prolonged MV >24 h (n = 77,059). Thrombectomy OR attenuates from 3.29 to 2.69 when short procedural MV is excluded; all comorbidity ORs remain stable or slightly strengthen, confirming they are genuine drivers of respiratory failure.
Simplified Ventilation Risk Score (sVRS)
The sVRS was constructed from regression coefficients (Table 3). The sVRS demonstrated clear stratification of MV probability (Table 4): MV occurred in 3.65% of patients in the low-risk category (sVRS <5), 9.25% in the medium-risk category (sVRS 5–11), and 28.7% in the high-risk category (sVRS ≥12), representing an approximately eightfold difference between low- and high-risk groups.
Assignment of Points for the Simplified Ventilation Risk Score (sVRS), Derived from Regression Coefficients and Reflecting the Relative Contribution of Each Predictor to Mechanical Ventilation Risk.
Stratification of Acute Ischemic Stroke Patients by Simplified Ventilation Risk Score (sVRS) Showing Score Thresholds, Mechanical Ventilation Rates, and the Number of Patients in Each Risk Group.
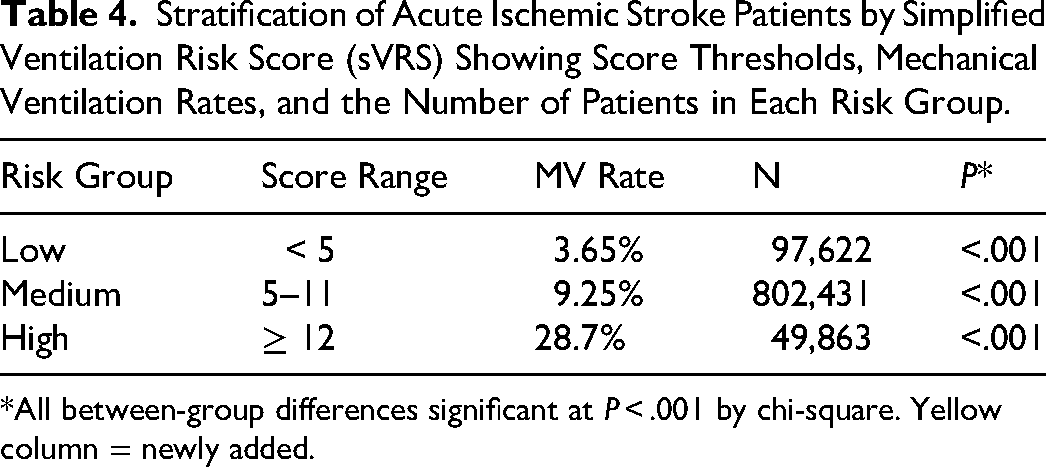
*All between-group differences significant at P < .001 by chi-square. Yellow column = newly added.
An exploratory analysis examined the association between sVRS risk group and MV duration among ventilated patients (Table 5). Prolonged MV rates followed the same graded pattern: 2.78% in the low-risk group, 7.70% in the medium-risk group, and 25.1% in the high-risk group. Among patients who received MV, the proportion with prolonged ventilation (>24 h) increased with sVRS tier: 76% in the low-risk group, 83% in the medium-risk group, and 87% in the high-risk group. This gradient suggests that the sVRS not only identifies patients at risk for intubation but also associates with the duration of respiratory dependency.
Exploratory Analysis: Association Between sVRS Risk Group and MV Duration Among Ventilated Patients, with Overall and Prolonged MV Rates by Risk Group.

Duration column percentages reflect distribution among MV patients within each risk group. Among MV patients, proportion with prolonged MV (>24 h): Low 76%, Medium 83%, High 87%. New exploratory analysis added in revision.
Thrombectomy Subgroup Analysis
Among the 92,085 MV patients, thrombectomy and non-thrombectomy patients showed distinct MV duration profiles. Among non-thrombectomy MV patients (n = 84,462), 15.4% had short-duration MV (<24 h), 33.8% intermediate, and 50.8% prolonged (>96 h). Among thrombectomy MV patients (n = 7,623), 26.1% had short-duration MV, 39.8% intermediate, and 34.1% prolonged, confirming that thrombectomy patients are disproportionately represented among short-duration MV cases, consistent with peri-procedural intubation (chi-square p < 2.2 × 10−16). However, 73.9% of thrombectomy-MV patients still had prolonged MV (>24 h). Thrombectomy-MV patients also had substantially lower rates of liver disease (3.6% vs 12.3%) and coagulopathy (14.8% vs 22.2%) compared with non-thrombectomy MV patients, suggesting distinct mechanistic pathways to intubation in these subgroups (Figure 1).
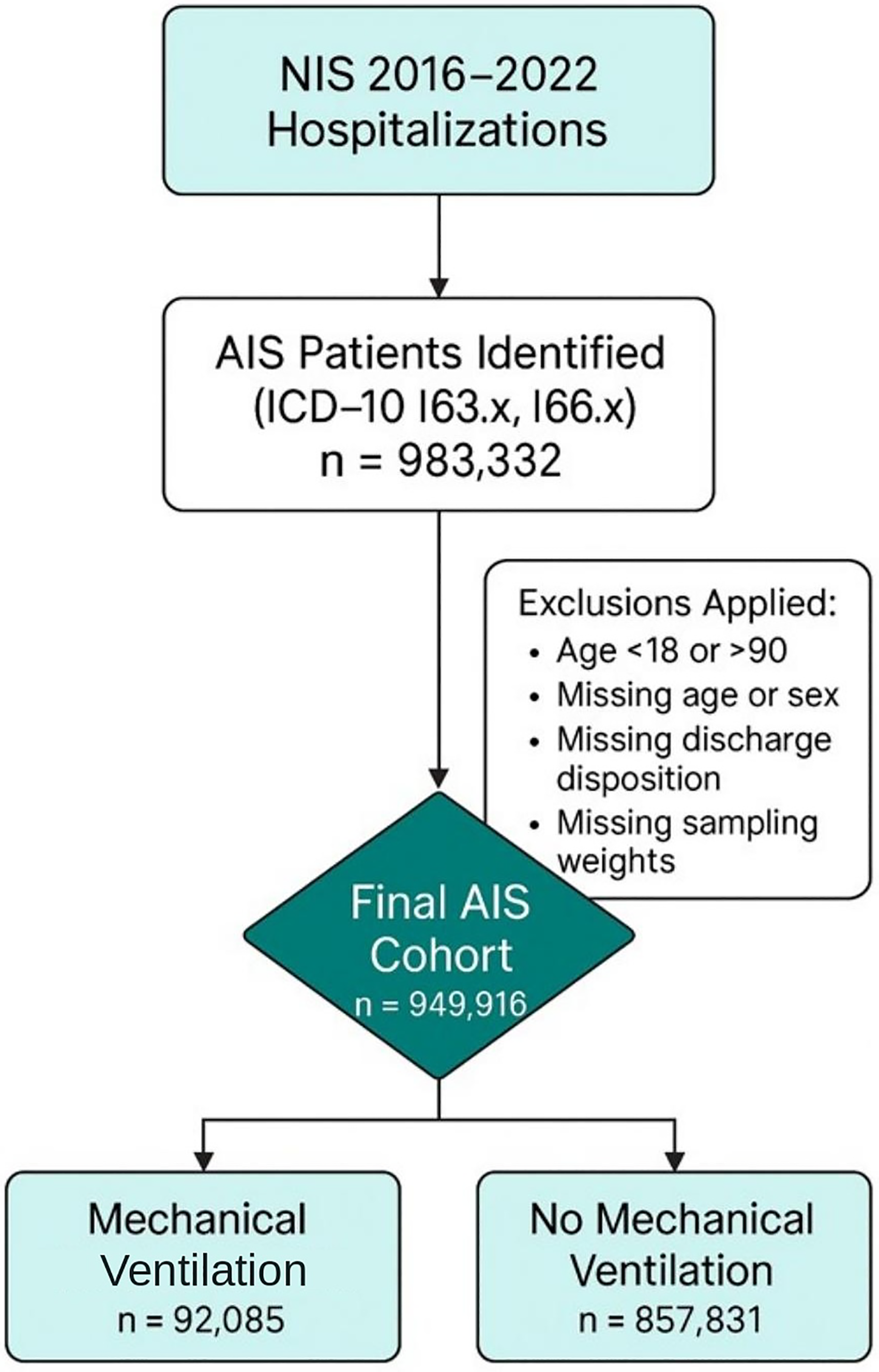
Flowchart depicting selection of the AIS cohort and classification by receipt of mechanical ventilation in the National Inpatient Sample, 2016–2022.
Sensitivity Analysis: Prolonged MV Outcome
When the outcome was restricted to prolonged MV (>24 h; n = 77,059), all comorbidity predictors remained significant and their associations were stable or slightly strengthened: liver disease OR 3.47 (95% CI 3.38–3.56), coagulopathy OR 2.95 (95% CI 2.89–3.01), CHF OR 1.87 (95% CI 1.84–1.91), COPD OR 1.43, atrial fibrillation OR 1.40, CKD OR 1.10 (all P < .001). The thrombectomy OR attenuated from 3.29 (all MV) to 2.69 (95% CI 2.61–2.78; P < .001) in the prolonged MV model, consistent with partial confounding by short peri-procedural intubation. These findings confirm that the comorbidity predictors in the sVRS are robust drivers of true respiratory failure rather than procedural artifacts.
Model Performance and Machine Learning
Logistic regression achieved an AUC of 0.706 for the primary (all MV) outcome. XGBoost demonstrated slightly higher discrimination with an AUC of 0.716 and exhibited smoother calibration. Brier scores were 0.081 (logistic) and 0.080 (XGBoost). In the prolonged MV sensitivity analysis, AUCs improved modestly: logistic regression AUC 0.711 and XGBoost AUC 0.721, consistent with improved predictor specificity for true respiratory failure. Both models showed acceptable agreement between predicted and observed MV risk across all deciles of predicted probability (Figure 2).
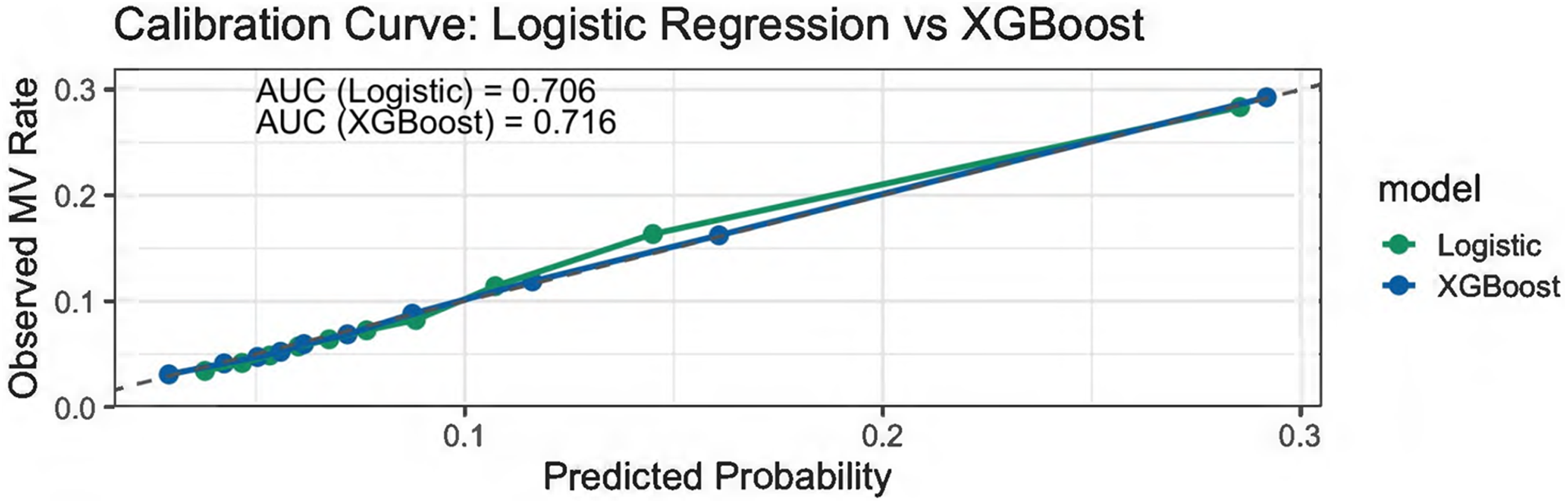
Calibration performance of logistic regression and XGBoost models for predicting early mechanical ventilation in acute ischemic stroke. Calibration curves were generated using deciles of predicted probability, comparing observed and expected MV rates. Both models show strong agreement with the ideal reference line, with XGBoost providing slightly superior discrimination (AUC 0.716) relative to logistic regression (AUC 0.706).
SHAP analysis identified coagulopathy, age, liver disease, CHF, and thrombectomy as the strongest contributors to predicted MV probability (Supplementary Figures 1 and 2). The close correspondence between SHAP results and logistic regression findings reinforces the robustness of the predictor set.
Discussion
MV in AIS marks a pivotal inflection point that reflects the convergence of neurologic injury with systemic physiologic vulnerability.1‐3,14,15 Using a large, contemporary, nationally representative cohort, we show that nearly one in ten patients hospitalized with AIS requires MV, reinforcing prior observations that this is a common and clinically consequential event in stroke care.2,3,5 Ventilated and non-ventilated patients represent two distinct clinical phenotypes characterized by markedly different comorbidity profiles, treatment exposure, and hospital trajectories.
The principal finding of this study is that AIS patients who require MV differ fundamentally from those who do not, with markedly higher systemic comorbidity burden and treatment exposure. Liver disease, coagulopathy, CHF, COPD, atrial fibrillation, CKD, and mechanical thrombectomy emerged as the strongest predictors of MV. Importantly, HT was present in 15.7% of MV patients compared with 4.6% of non-MV patients—a more than threefold difference—underscoring the interplay between cerebrovascular injury severity and respiratory vulnerability. These associations persisted after multivariable adjustment, reinforcing the central role of systemic vulnerability in respiratory failure during AIS hospitalization. Our findings extend earlier population-based studies1‐3 by identifying specific identifiable clinical predictors in the modern endovascular era.5‐7
Mechanical thrombectomy was among the strongest treatment-related predictors of MV. Our subgroup analysis clarifies the nature of this association: thrombectomy patients had a higher proportion of short-duration MV (<24h: 26.1% vs 15.4%), consistent with peri-procedural airway protection; however, 73.9% of thrombectomy-MV patients still had prolonged MV (>24 h), and thrombectomy remained strongly associated with prolonged MV (OR 2.69) in the sensitivity analysis. Notably, thrombectomy-MV patients had substantially lower rates of liver disease and coagulopathy compared with non-thrombectomy MV patients, suggesting that neurologic severity and anesthetic exposure—rather than systemic comorbidity—are the dominant drivers of intubation in this subgroup. Prior studies have documented outcomes and indications for MV in stroke patients, including the impact of anesthetic and procedural management on respiratory trajectories.16,17 Our findings should not be interpreted as suggesting that thrombectomy causes respiratory failure; rather, they identify thrombectomy patients as a high-risk subgroup in whom anticipatory respiratory planning is particularly valuable.
To translate these findings into a clinically actionable framework, we developed the sVRS derived from regression coefficients of routinely available clinical variables. The sVRS demonstrated robust and graded risk stratification with nearly an eightfold difference in MV rates between low- and high-risk groups. A key finding of the sensitivity analysis is that the sVRS stratification is maintained when the outcome is restricted to prolonged MV (>24 h): low 2.78%, medium 7.70%, high 25.1%. Furthermore, higher sVRS scores associate with greater proportions of prolonged ventilation among those who are intubated (76% in low vs 87% in high risk), suggesting that the score may also have utility in anticipating tracheostomy need in future prospective studies.
Machine learning models demonstrated modestly higher discrimination compared with traditional logistic regression, while showing substantial concordance in predictor importance. Discrimination improved slightly when restricted to prolonged MV (logistic AUC 0.711; XGBoost AUC 0.721), consistent with the hypothesis that the core predictors are more specific for true respiratory failure than for brief procedural intubation. SHAP analyses consistently identified the same core clinical variables as dominant contributors, reinforcing biological plausibility.18‐21 Machine learning serves not as a replacement for traditional modeling but as a complementary strategy that supports validation and robustness testing.
The sVRS is constructed entirely from variables routinely available at hospital admission, making it well suited for early risk stratification before overt respiratory failure develops. Early recognition of high-risk patients may facilitate anticipatory ICU triage, prompt neurocritical care involvement, and earlier goals-of-care discussions. At a systems level, the ability to stratify ventilatory risk early aligns with efforts to optimize resource utilization in high-acuity neurocritical care environments.22‐25
Limitations
This study has limitations inherent to administrative data. The NIS does not capture granular neurologic severity measures, such as the NIH Stroke Scale. Critically, the NIS does not provide information on infarct location, volume, or territory involvement. Stroke location and size are well-established determinants of impaired consciousness and aspiration risk, and their absence is an important limitation. Future prospective studies incorporating neuroimaging data should evaluate whether infarct topography and volumetric burden independently predict MV risk and improve sVRS performance. The NIS also lacks detailed information regarding the timing, indications, or clinical context surrounding MV initiation, and does not capture granular procedural or ventilatory management data. As with all observational analyses, residual confounding is possible and causal relationships cannot be inferred. Despite these limitations, the NIS remains uniquely suited for evaluating relatively infrequent yet clinically meaningful outcomes at a national level when analyses adhere to established methodological guidance. 26
Conclusions
In summary, this study identifies a distinct clinical phenotype associated with the need for MV in AIS and translates these findings into a simple, interpretable risk stratification tool. MV occurs in approximately one in ten AIS hospitalizations and identifies patients with substantially higher comorbidity burden, longer hospitalization, and a higher prevalence of HT. The sVRS demonstrated robust, graded risk stratification across low-, intermediate-, and high-risk groups, with nearly an eightfold difference in MV rates, and higher sVRS scores were associated with greater proportions of prolonged ventilation. Sensitivity analyses restricting the outcome to prolonged MV (>24 h) confirmed the stability and biological plausibility of the identified predictors. Future work should focus on prospective validation of the sVRS in emergency department and neurocritical care cohorts, and on integrating neuroimaging and physiologic variables to enhance predictive precision.
Supplemental Material
sj-tif-1-jic-10.1177_08850666261452639 - Supplemental material for Early Risk Stratification for Mechanical Ventilation in Acute Ischemic Stroke: Development and Validation of a Simplified Clinical Score
Supplemental material, sj-tif-1-jic-10.1177_08850666261452639 for Early Risk Stratification for Mechanical Ventilation in Acute Ischemic Stroke: Development and Validation of a Simplified Clinical Score by Mian Urfy and Mariam Tariq Mir in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666261452639 - Supplemental material for Early Risk Stratification for Mechanical Ventilation in Acute Ischemic Stroke: Development and Validation of a Simplified Clinical Score
Supplemental material, sj-docx-2-jic-10.1177_08850666261452639 for Early Risk Stratification for Mechanical Ventilation in Acute Ischemic Stroke: Development and Validation of a Simplified Clinical Score by Mian Urfy and Mariam Tariq Mir in Journal of Intensive Care Medicine
Footnotes
Ethical Considerations and Consent to Participate
This study used de-identified, publicly available data from the NIS. Institutional review board approval and informed consent were waived.
Author Contributions
Mian Urfy: Conceptualization; study design; data analysis and interpretation; development of the simplified Ventilation Risk Score; manuscript drafting; critical revision for important intellectual content; supervision.
Mariam Tariq Mir: Data interpretation; literature review; manuscript drafting; critical revision for important intellectual content.
All authors approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This study was conducted using the NIS, a publicly available, de-identified database developed by the Agency for Healthcare Research and Quality. Institutional review board approval and informed consent were not required.
Authorship Confirmation
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. The final manuscript was reviewed and approved by all authors.
Reporting Guidelines
This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The completed EQUATOR checklist is provided as supplementary material.
Prior Publication and Exclusivity
This manuscript has not been published previously and is not under consideration for publication elsewhere.
Artificial Intelligence–Assisted Technology
Artificial intelligence–assisted technologies were used only for limited editorial refinement and language clarity. All analyses, interpretation, and final content decisions were performed by the authors, who take full responsibility for the integrity and originality of the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.