
Abstract
We greatly appreciate the comments of Rakovich and Kurz regarding our recently published article. In our correspondence, we clarify several issues raised by the authors regarding the definition, pathophysiology and management of necrotizing lung infections (NLI) in patients requiring VV-ECMO support for severe respiratory failure. We emphasize that there is currently no universally accepted radiological definition or volumetric cut-off for necrotizing pneumonia. Our study intentionally used a broader CT-based definition encompassing necrotizing pneumonia, lung abscess and necrotizing cavitation to capture the clinically relevant spectrum of destructive pulmonary complications observed in critically ill ECMO patients. Following the authors’ suggestion, we additionally re-analysed our cohort using a proposed threshold of >50% non-enhancing consolidated parenchyma, with 55% of patients still fulfilling these criteria. We further clarify that our cohort consisted primarily of patients with severe ARDS requiring ECMO support in whom NLI developed as a complication of extensive pre-existing lung injury, rather than as the primary cause of refractory hypoxemia. The high proportion of viral pneumonia, particularly COVID-19, concomitant thromboembolic events, corticosteroid exposure and severe ventilation/perfusion abnormalities likely contributed to the high incidence of necrotic complications observed in our cohort. Finally, we agree that surgical intervention should remain a last-resort strategy in these patients and provide additional clinical data regarding surgically treated patients to better illustrate the severity of disease and indications for operative management.
Keywords
To the Editor
We would like to thank Dr Rakovich and Dr Kurz for their thoughtful and insightful comments on our recently published article and are delighted that our data have raised interest and constructive remarks. We appreciate the opportunity to clarify observations addressed in their correspondence.
We acknowledge the authors’ concern regarding the definition of necrotizing pneumonia (NP) and its potential impact on the reported incidence of necrotising lung infections (NLI). We would like to emphasise that there is no universally accepted radiological definition or threshold percentage of affected parenchyma for NP, with most severe forms affecting >50% of lobe historically regarded as pulmonary gangrene.1-3 We adopted a radiological definition encompassing NP, lung abscess and necrotizing cavitation based on CT findings such as low post-contrast attenuation and non-enhancing parenchyma as described in Methods. Regarding the comment on Table 3, we acknowledge authors’ objection that extent of consolidation was reported, which may not correlate to the degree of necrotic volume. With regard to this issue and authors’ suggestion that area of non-contrast enhancement within a consolidated lobe of >50% would be a more reasonable cut-off for severe NP, we re-analysed our data to conclude that 21 (55%) patients would fulfil these proposed criteria. However, as NP remains an ill-defined entity, we reported as stated that ‘NP of variable extent was documented in the majority of patients (89.5%)’ and as clearly outlined in the article our patients spanned over the entire spectrum of NLI from single lung abscess to severe diffuse NP/pulmonary gangrene with extensive cavitations and there was considerable overlap between different NLI entities in majority of patients as is common in clinical practice.
With regard to the second remark raising the question about recalcitrant respiratory failure in these patients, we would like to clarify and emphasise that as stated in the article we report a cohort of patients that required ECMO treatment due to severe ARDS (P/F ratio < 70 mm Hg, Murray score 3.3) of different etiologies who had concurrent severe organ failure (median SOFA 10, median APACHE II 19). Only a smaller proportion of patients (23.7%) had some form of NLI documented before ECMO start and majority developed NLI during ECMO run as a complication of pre-existing extensive parenchymal lung damage that required ECMO treatment in the first place. We report a cohort of ECMO patients where NLI development was a subsequent complication and not a primary cause for hypoxic lung failure necessitating ECMO support. We hope this clarifies authors’ concern with regard to this issue.
Related to previous issue is also elucidation that high proportion of necrosis and secondary pulmonary complications we report for the first time in such a cohort of severely ill patients is most likely attributed to severe parenchymal lung damage caused by primary causative agent (viral pneumonia in majority of our patients), high proportion of corticosteroid use (50%) and severe ventilation/perfusion mismatch attributable also to high percentage of PE events, especially in COVID-19 patients.
The authors raised concerns regarding surgical interventions in these patients. We must commend the authors and would like to express our agreement with their view and current literature1-4 as we aim to avoid surgical interventions in our practice and surgery is used as last resort only. We report 5 patients with surgical intervention in our cohort with dismal outcomes. We would like to emphasise that surgery was attempted as last resort strategy in an attempt to manage secondary complications in all of these patients and we report their characteristics (Table 1, Figure 1) to provide a clearer insight into their condition and to justify this strategy.
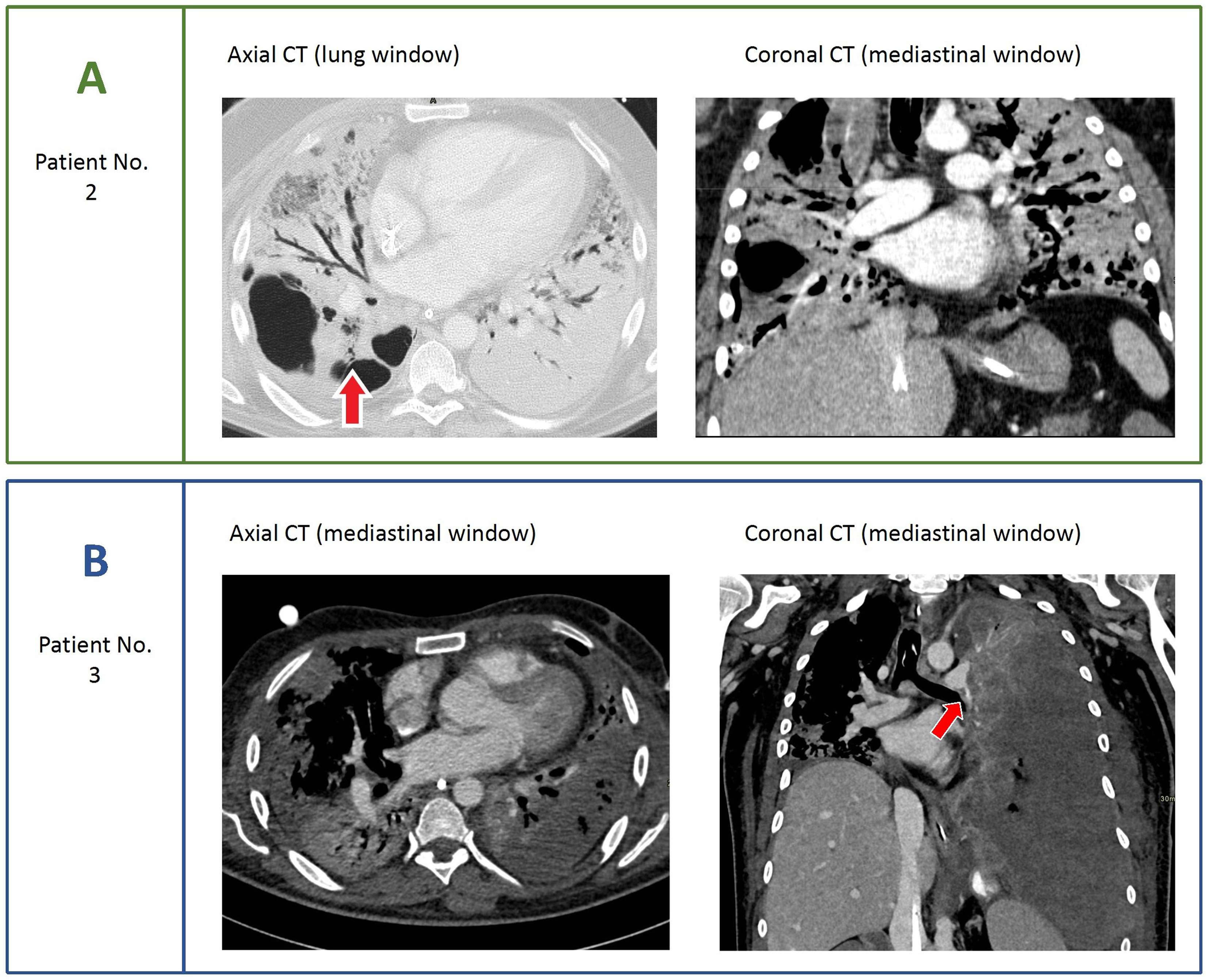
Representative chest CT findings of two patients with severe necrotizing lung infections on ECMO support requiring surgical interventions. Panel A (Patient 2): Chest CT scan with axial and coronal views demonstrating areas of necrotising pneumonia involving all three right lung lobes, as well as extensive areas of dense consolidation with bronchiectasis in the left lung. The red arrow indicates one of multiple bronchopleural fistulae in the right lung. Panel B (Patient 3): Chest CT scan with axial and coronal views demonstrating necrotising pneumonia affecting the parenchyma of the entire left lower lobe, as well as smaller areas of the inferior lingula, right middle lobe, and right lower lobe. Note the presence of pulmonary embolism in the left descending pulmonary artery (red arrow). Surgical intervention was warranted because of a large acute left-sided haemothorax with pronounced mass effect and haemodynamic instability of the patient.
Characteristics of Patients Requiring Surgical Interventions.
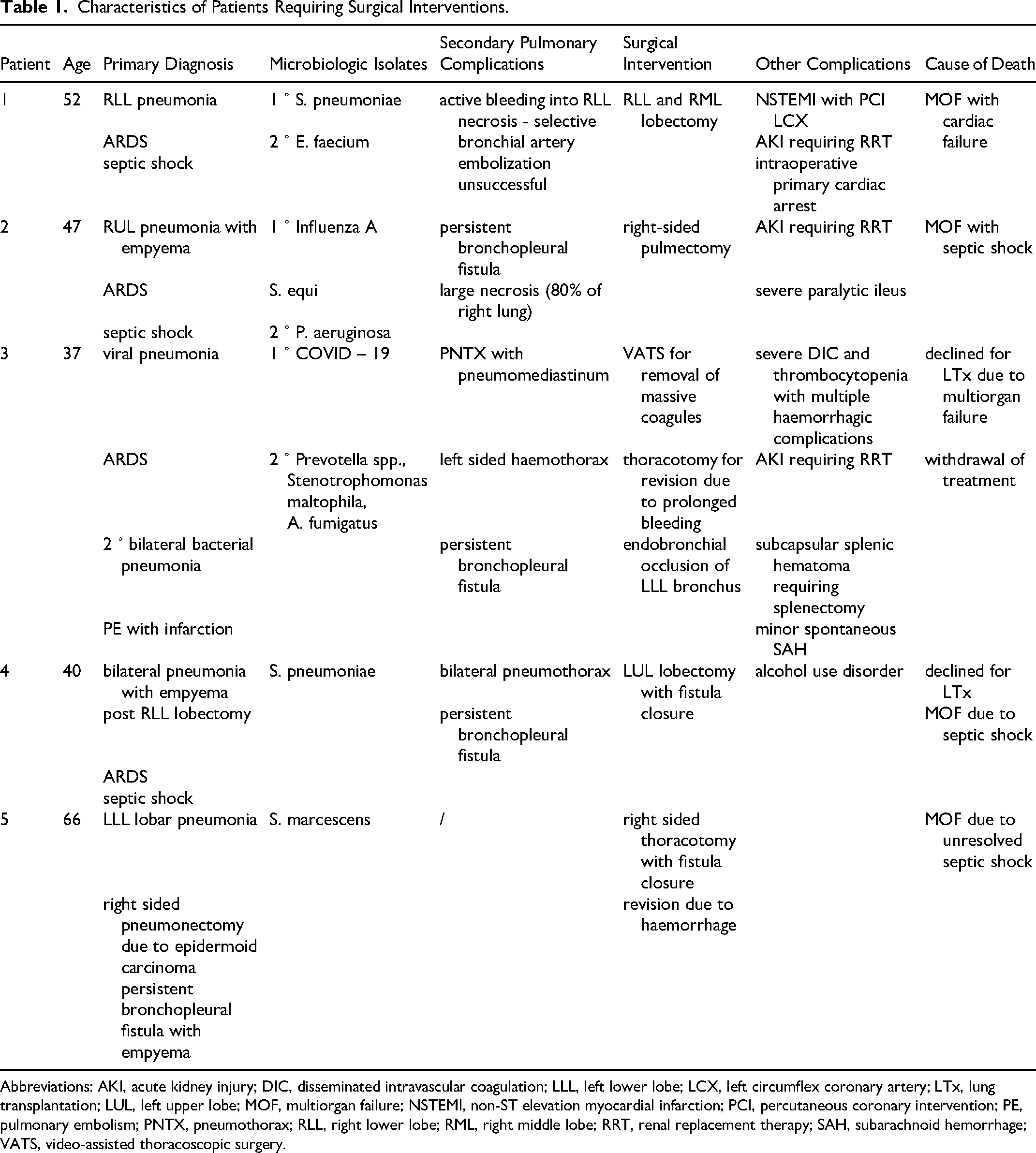
Abbreviations: AKI, acute kidney injury; DIC, disseminated intravascular coagulation; LLL, left lower lobe; LCX, left circumflex coronary artery; LTx, lung transplantation; LUL, left upper lobe; MOF, multiorgan failure; NSTEMI, non-ST elevation myocardial infarction; PCI, percutaneous coronary intervention; PE, pulmonary embolism; PNTX, pneumothorax; RLL, right lower lobe; RML, right middle lobe; RRT, renal replacement therapy; SAH, subarachnoid hemorrhage; VATS, video-assisted thoracoscopic surgery.
We hope that we have adequately addressed authors’ comments. Furthermore, we hope that our report emphasises sufficiently that despite the cumulative burden of severe ARDS, multiple organ dysfunction, ECMO support and NLI complications a non-negligible proportion of patients survived to hospital discharge.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.