
Abstract
Objective
Mechanically ventilated sepsis patients have a high mortality rate. This retrospective cohort study aimed to investigate the impact of dexmedetomidine on the clinical prognosis of mechanically ventilated sepsis patients and to analyze its correlation with local pulmonary inflammation and oxidative stress status.
Methods
Patients admitted between January 2022 and December 2025 who met the Sepsis 3.0 diagnostic criteria and received invasive mechanical ventilation for over 24 h were included. Based on whether dexmedetomidine was administered within 72 h of sepsis diagnosis, patients were divided into a dexmedetomidine-exposed group (DEX group) and a non-exposed group (Non-DEX group). The primary outcome was 28-day mortality risk. Secondary outcomes included duration of mechanical ventilation, length of ICU stay, and total hospital stay. By measuring levels of tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), malondialdehyde (MDA), and superoxide dismutase (SOD) in bronchoalveolar lavage fluid (BALF), the local pulmonary inflammatory and oxidative stress status were assessed. Kaplan-Meier survival curves, multivariable Cox regression models, and other methods were used to analyze the association between dexmedetomidine exposure and clinical outcomes, as well as local pulmonary inflammation and oxidative stress status.
Results
A total of 168 patients were included (58 in the DEX group, 110 in the Non-DEX group), with an overall 28-day mortality rate of 57.14% (51.72% in DEX group vs 69.09% in Non-DEX group). The median survival time was 31 days in the Dex group and 23 days in the Non-Dex group. The death risk in the Non-Dex group was 1.627 times that of the Dex group. After adjusting for confounding factors such as baseline Sequential Organ Failure Assessment (SOFA) score, shock status, and blood lactate level, dexmedetomidine use was independently associated with a reduced 28-day mortality risk (Hazard Ratio [HR] = 0.65, 95% CI: 0.46-0.79, P = 0.00362). There was no significant difference in mechanical ventilation time between the two groups (P = 0.2217), but the DEX group had longer ICU and total hospital stays (P = 0.015, 0.0484, respectively). Analysis of BALF samples showed that TNF-α, IL-6, and MDA levels were significantly lower, while SOD activity was significantly higher in the DEX group (all P < 0.05).
Conclusion
In mechanically ventilated sepsis patients, dexmedetomidine exposure was independently associated with reduced 28-day mortality risk. The survival benefit may be related to the alleviation of local pulmonary inflammation and oxidative stress, with improvements in BALF biomarkers providing direct evidence. The study suggests that dexmedetomidine may have a dual role of sedation and potential organ protection for the high-risk population.
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. 1 The Sepsis 3.0 definition emphasizes not only the presence of infection but also highlights the complex pathophysiological processes occurring during the host response. Uncontrolled inflammatory response, accompanied by oxidative stress, immune dysregulation, and sympathetic nervous system hyperactivation induced by the inflammatory storm, are core pathological features of sepsis progression.2,3 These pathophysiological mechanisms could lead to cellular and tissue damage, immune dysfunction, and may ultimately progress to multiple organ dysfunction syndrome (MODS). 2 Due to its complex pathogenesis, rapid progression, and numerous complications, the morbidity and mortality rates of sepsis remain high. 4 Although early diagnostic capabilities and treatment strategies have improved in recent years with a deeper understanding of sepsis pathophysiology, the lack of specific treatments targeting the core pathological processes and the strong disease heterogeneity mean that sepsis remains a critical global public health challenge.
Among the organ dysfunctions caused by sepsis, the lung is one of the earliest and most commonly affected organs. Globally, there are at least 20 million sepsis patients annually, of whom over 20% require mechanical ventilation, with mortality rates exceeding 40% in this subgroup. 5 Sepsis-associated lung injury is a key factor leading to respiratory failure, prolonged mechanical ventilation, and poor prognosis. Mechanical ventilation itself can cause barotrauma and volutrauma, exacerbating lung injury. The interaction between excessive pulmonary inflammatory response and oxidative stress leads to alveolar-capillary barrier disruption, pulmonary edema, and impaired gas exchange. 6 Therefore, analgesia and sedation are not only essential for ensuring patient tolerance of mechanical ventilation but are also crucial components of the multidimensional management of sepsis.7–9
Dexmedetomidine is a selective α2-adrenergic receptor agonist with sedative, analgesic, and sympatholytic effects, widely used for endotracheal intubation in surgical patients under general anesthesia and for sedation in mechanically ventilated patients.10–13 Beyond its traditional sedative role, preclinical studies have demonstrated its unique potential for multi-organ protection. 14 Animal experiments have shown that dexmedetomidine may attenuate severe systemic inflammation, encephalitis, and neurocognitive impairment induced by sepsis, 15 and exhibit protective effects on the heart, 16 liver, 17 and kidneys. 18 Regarding lung protection, dexmedetomidine could mitigate lipopolysaccharide-induced acute lung injury in septic mice through multiple pathways, including anti-inflammatory, antioxidant, and anti-apoptotic mechanisms. 19 Although preclinical studies confirmed the anti-inflammatory, antioxidant, and anti-apoptotic organ-protective properties of dexmedetomidine in septic animal models, its clinical benefits in sepsis patients remain unclear, with conflicting conclusions in related studies.20–22 The reasons may include: 1. Strong heterogeneity of sepsis and lack of studies on specific subgroups; 2. Existing clinical evidence primarily focuses on systemic indicators, such as peripheral blood inflammatory levels, duration of mechanical ventilation, and patient mortality, lacking direct assessment of local pathophysiological status in specific populations and target organs.
Leveraging the hospital's sepsis data platform and acute lung injury biobank, this study designed a retrospective cohort study targeting the high-risk population of mechanically ventilated sepsis patients. We hypothesized that the clinical effects of dexmedetomidine in these patients are related to its impact on pulmonary inflammation and oxidative stress response. To test this hypothesis, the study innovatively analyzed bronchoalveolar lavage fluid to directly measure levels of pulmonary inflammatory and oxidative stress markers, preliminarily validating the association between drug effects and core pathophysiological changes in lung tissue. The findings are expected to provide evidence for the role of dexmedetomidine in sepsis-induced lung injury, offer a reference for precise sedation therapy in these patients, and guide efforts to improve the clinical prognosis of mechanically ventilated sepsis patients.
Materials and Methods
General Information
Case Selection
This was a retrospective cohort study approved by the hospital's Medical Ethics Committee (Ethics Approval No.: PJ2025-08-09). Sepsis patients receiving mechanical ventilation at the First Affiliated Hospital of Anhui Medical University between January 2022 and December 2025 were included, resulting in a final cohort of 168 patients.
Inclusion Criteria
Sepsis diagnosis meeting the 2016 Sepsis 3.0 definition and diagnostic criteria;
Requirement for invasive mechanical ventilation with a duration exceeding 24 h;
Age 18 years or older.
Exclusion Criteria
Hospital stay less than 72 h;
Patients with second-degree or higher atrioventricular block;
Patients with severe bradycardia (heart rate less than 50 beats per minute);
Pregnant patients.
Research Methods
Patient Grouping
Patients were grouped based on whether they received dexmedetomidine treatment within 72 h after sepsis diagnosis: the Dexmedetomidine-Exposed Group was defined as patients who received dexmedetomidine within the time window, regardless of concomitant use of other sedatives; the Non-Exposed Group consisted of patients who never received dexmedetomidine during hospitalization and received other sedative drugs within the aforementioned 72-h window.
Primary Disease Treatment
All patients received comprehensive treatment for sepsis, including adequate source control, antibiotic therapy, fluid resuscitation for patients with hypoperfusion, and vasoactive drugs to maintain hemodynamic stability. Mechanically ventilated patients were managed with controlled or assisted ventilation modes, with plateau pressure limited to below 35 cm H₂O and positive end-expiratory pressure (PEEP) titrated to maintain optimal oxygen saturation.
Collection of Bedside Bronchoalveolar Lavage Fluid
Utilizing the hospital's sepsis data platform and acute lung injury biobank, we collected fiberoptic bronchoalveolar lavage fluid (BALF) samples. Patients were placed in the supine position, adequately sedated and analgesicized pre-procedure, pre-oxygenated with pure oxygen for 10–15 min, with continuous monitoring of vital signs including fingertip oxygen saturation. The fiberoptic bronchoscope was introduced via the endotracheal tube or tracheostomy tube. After the tip reached the right middle lobe or the more severely affected lobe, 20 ml of sterile saline was injected in aliquots and aspirated. The lavage and aspiration steps were repeated until a total of 50 ml was recovered or a total of 100 ml was instilled. The collected BALF was centrifuged at 1200 × g for 10 min. The supernatant was frozen at −80 °C for subsequent batch analysis.
Outcome Measures
Primary outcome measure: 28-day mortality risk after sepsis diagnosis.
Secondary outcome measures: Hospital length of stay, ICU length of stay, duration of mechanical ventilation.
Measurement of BALF inflammatory factors and oxidative stress indicators (if multiple bronchoscopies were performed, the specimen obtained 48 h to 1 week after sedative use was selected): To account for potential variability in collection timing, the exact time from sedative initiation to BALF collection (in hours) was recorded for each patient. This variable was included as a covariate in sensitivity analyses to adjust for its potential confounding effect. Levels of tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), malondialdehyde (MDA), and superoxide dismutase (SOD) in BALF were measured using commercial kits (COIBO Biotechnology, China). Briefly, following the kit instructions, a double-antibody sandwich enzyme-linked immunosorbent assay (ELISA) was employed. BALF was added to microplate wells coated with specific antibodies. Horseradish peroxidase-labeled detection antibodies were then added and incubated to form antibody-antigen-enzyme-antibody complexes. After washing, 3,3′,5,5′-tetramethylbenzidine solution was added to react with horseradish peroxidase for color development. Optical density was measured at 450 nm using a spectrophotometer. Finally, biomarker concentrations in BALF were calculated based on standard curves. Each sample was assayed in triplicate, and the average of three independent experiments was taken as the final concentration.
Other clinical data: Age, sex, comorbidities, infection site, oxygenation index after sepsis diagnosis, blood lactate level, white blood cell count, C-reactive protein (CRP) level, procalcitonin (PCT) level, and baseline Sequential Organ Failure Assessment (SOFA) score (calculated and scored by retrospectively reviewing case data based on SOFA scoring guidelines).
Handling of Missing BALF Data
Among the 168 included patients, 8 (4.8%) had missing BALF specimens due to logistical reasons (eg, bronchoscopy not performed due to hemodynamic instability or technical failure). Little's MCAR test indicated that the missingness was completely at random (χ2 = 6.32, df = 8, P = 0.61). To handle missing values while preserving statistical power, multiple imputation was performed using the fully conditional specification (FCS) method in SPSS version 26.0.
The imputation model included the following auxiliary variables: age, sex, SOFA score, shock status, oxygenation index (PaO₂/FiO₂), vasopressor use, mechanical ventilation parameters (PEEP, plateau pressure), CRP, PCT, white blood cell count, 28-day mortality status, ICU length of stay, dexmedetomidine group assignment, and the other three BALF biomarkers when imputing a specific marker. Twenty imputed datasets were generated with 10 iterations each, and convergence was confirmed by visual inspection of trace plots. For continuous variables (TNF-α, IL-6, MDA, SOD), linear regression was used after log transformation to approximate normality; for binary variables, logistic regression was used. Between-group comparisons (DEX vs non-DEX) were performed on each imputed dataset using the Mann-Whitney U test, and results were pooled according to Rubin's rules.
To assess the robustness of the imputation results, two sensitivity analyses were conducted: (1) a complete-case analysis excluding the 8 patients with missing BALF, and (2) a worst-case scenario imputation assuming missing not at random (MNAR) by adding a shift of +0.5 standard deviation to imputed values in the non-DEX group. Both analyses yielded results consistent with the primary imputation analysis.
Statistical Analysis
Sample Size Estimation
As a retrospective analysis, the study retrieved case data from the available records in the hospital's Health Information System (HIS) and the internal sepsis data platform.
Data Processing and Analysis
All data analyses were performed using SPSS software (version 26.0). For missing values of key variables, if the missing rate was ≥20%, the variable was excluded from the analysis. For continuous variables with a missing rate <20%, multiple imputation was used. All continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed variables are presented as mean ± standard deviation, and between-group comparisons were made using independent samples t-tests. Non-normally distributed variables are presented as median (interquartile range, IQR) [M (p25, p75)], and between-group comparisons were made using the Mann-Whitney U test. Categorical variables are presented as frequency (percentage). Between-group comparisons were made using Pearson's chi-square test or Fisher's exact test, depending on expected frequencies. For repeated measures data, if normality and sphericity assumptions were met, repeated measures analysis of variance was used; otherwise, the Friedman test was used. When overall comparisons showed statistical significance, post-hoc pairwise comparisons were performed using the Bonferroni correction. All statistical tests were two-sided. A P-value < 0.05 was considered statistically significant, and 95% confidence intervals were reported for main parameters.
The primary outcome of this study was 28-day mortality risk. Between-group comparisons of mortality risk were performed using Kaplan-Meier survival curves to plot cumulative risk, and the log-rank test was used to assess statistical differences. A Cox proportional hazards regression model was used to evaluate the association between dexmedetomidine treatment and 28-day mortality risk. To control for the influence of potential confounding factors such as disease severity (eg, shock) and comorbidities on outcomes, the analysis was adjusted by including covariates. Model construction followed a principle of first univariate, then multivariate analysis: variables with P < 0.05 in univariate analysis were initially included in the multivariable model, followed by variable selection using backward stepwise regression to identify independent influencing factors for the final model. Before modeling, multicollinearity among variables was diagnosed by calculating variance inflation factors.
To address the potential time-dependent bias due to varying timing of dexmedetomidine initiation within the 72-h exposure window, two sensitivity analyses were performed. First, a landmark analysis was conducted at 48 h after sepsis diagnosis, excluding patients who died within this period (n = 12). Dexmedetomidine exposure was then redefined as initiation within the first 48 h, and the 28-day mortality risk was re-evaluated using the same multivariable Cox model. Second, a time-dependent Cox proportional hazards model was fitted, wherein dexmedetomidine exposure was treated as a time-varying covariate. Patients contributed unexposed person-time from sepsis diagnosis until the time of first dexmedetomidine administration, after which they contributed exposed person-time. The results of these sensitivity analyses were compared with the primary analysis to assess the robustness of the findings. To address the potential risk of overfitting given the events-per-variable (EPV) ratio of approximately 6.6, we performed additional sensitivity analyses. First, a LASSO-penalized Cox regression model with 10-fold cross-validation was fitted using the same candidate variables. The optimal penalty parameter λ was selected by minimizing the partial likelihood deviance. Second, bootstrap internal validation with 500 resamples was conducted to estimate the optimism-corrected C-index of the final model. Third, a reduced Cox model including only pre-specified key covariates (age, SOFA score, shock, malignancy, and group assignment) was also fitted as a parsimonious alternative.
Additional Analyses
Considering the observational nature of this study, we also performed a post hoc sensitivity analysis using inverse probability of treatment weighting (IPTW) based on propensity scores to further reduce potential confounding. Propensity scores were estimated using a logistic regression model including baseline covariates with P < 0.10 in Table 1 (malignancy, CRP, chronic liver/renal disease, and pulmonary infection site). The IPTW-adjusted Cox proportional hazards model was then applied to evaluate the association between dexmedetomidine exposure and 28-day mortality.
Baseline Characteristics Between two Groups.
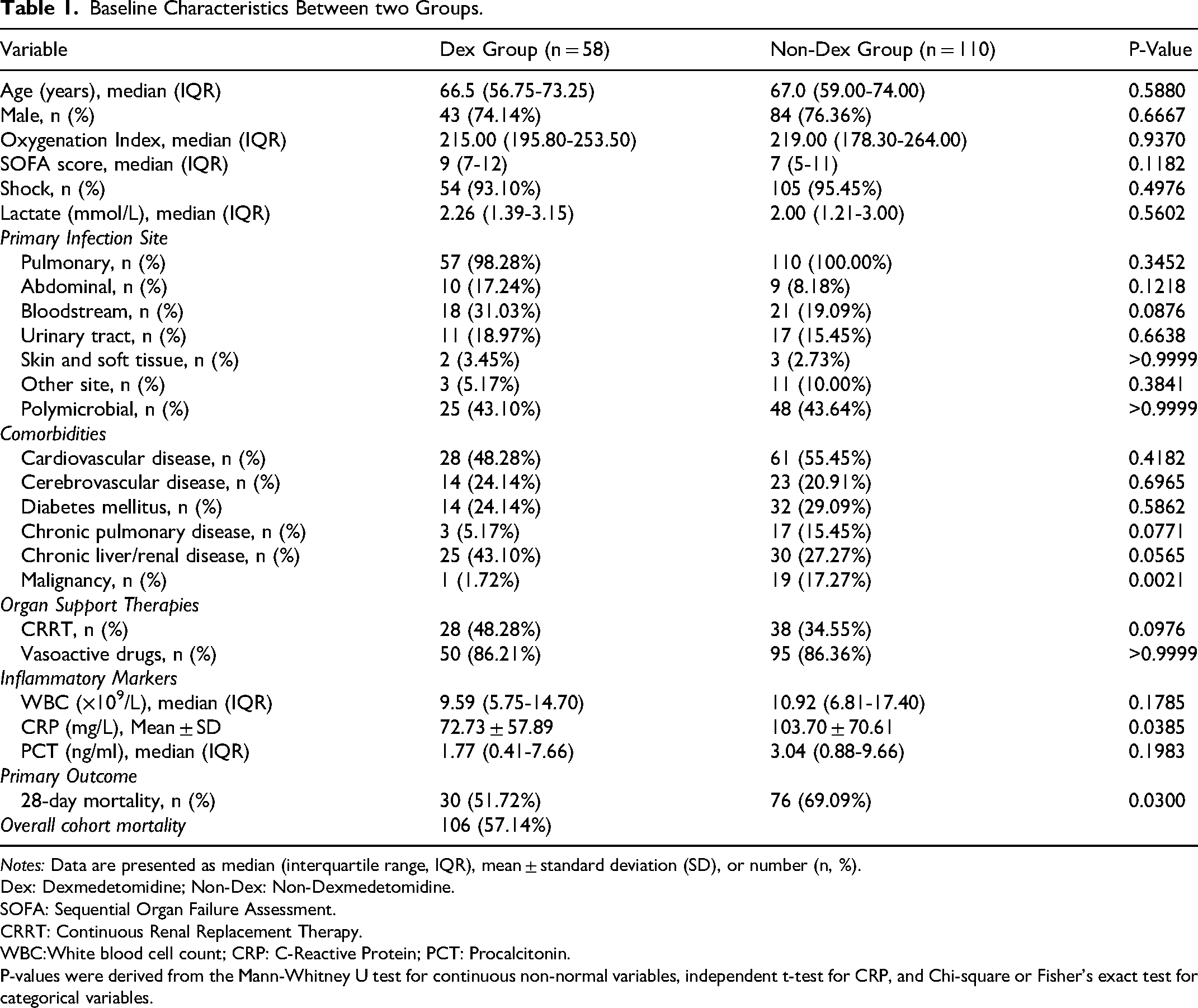
Notes: Data are presented as median (interquartile range, IQR), mean ± standard deviation (SD), or number (n, %).
Dex: Dexmedetomidine; Non-Dex: Non-Dexmedetomidine.
SOFA: Sequential Organ Failure Assessment.
CRRT: Continuous Renal Replacement Therapy.
WBC:White blood cell count; CRP: C-Reactive Protein; PCT: Procalcitonin.
P-values were derived from the Mann-Whitney U test for continuous non-normal variables, independent t-test for CRP, and Chi-square or Fisher's exact test for categorical variables.
Results
The final sample size for this study was 168 patients. During the study period, a total of 1039 sepsis patients were admitted to the ICU (diagnoses included: sepsis, septicemia, septic shock, infectious shock). Among them, 217 patients who received mechanical ventilation for over 24 h met the inclusion criteria. From these, 49 patients were further excluded. Specifically: 14 patients who did not receive dexmedetomidine or any other sedative within 72 h of sepsis diagnosis; 13 patients who received dexmedetomidine but for less than 24 h; 11 patients who survived less than 72 h after sepsis diagnosis; 5 patients with second- or third-degree atrioventricular block; 3 patients with severe bradycardia; and 3 pregnant patients. Ultimately, 168 eligible patients were identified, including 58 in the dexmedetomidine group and 110 in the non-dexmedetomidine group. The detailed patient screening process is shown in Figure 1.
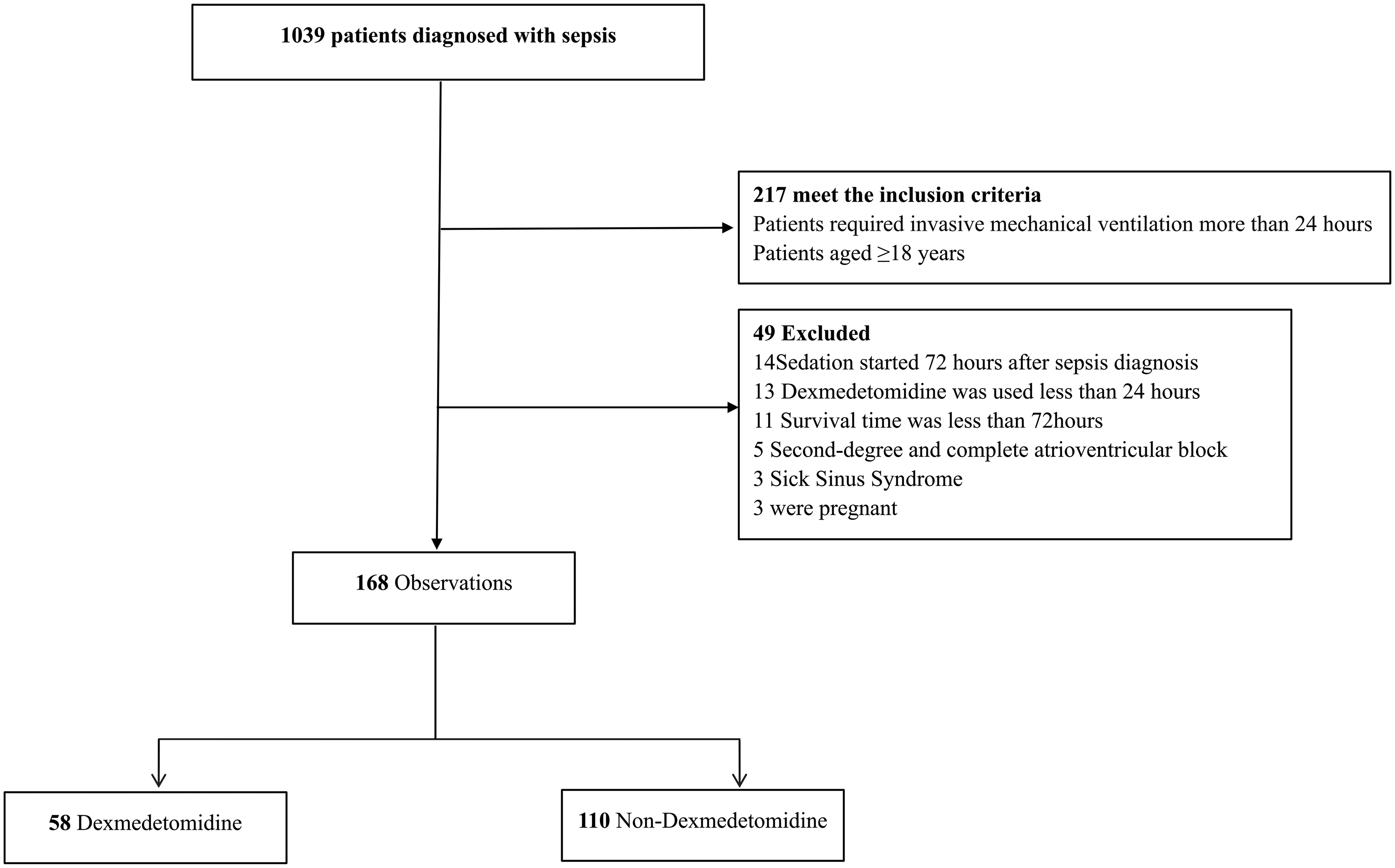
Patient Screening Flowchart.
Baseline Characteristics of the Two Groups
Comparison of Baseline Characteristics Between Groups
There were 28 missing items for SOFA scores. Multiple imputation was performed based on SOFA scoring guidelines combined with age, Glasgow Coma Scale score, oxygenation index, shock status, vasopressor use, mechanical ventilation status, and continuous renal replacement therapy (CRRT) status. The missing proportion for baseline data such as CRP and PCT was less than 20%. After imputation, all data fell within normal ranges.
Table 1 presents the baseline characteristics of the study population. The dexmedetomidine group included 58 patients, and the non-dexmedetomidine group included 110 patients. There were no significant differences in most baseline variables between the two groups, except for malignancy and CRP.
Dexmedetomidine Dosing, Exposure Characteristics, and Timing of Initiation
Among the 58 patients in the DEX group, dexmedetomidine was administered as a continuous intravenous infusion in 53 patients (91.4%) and as intermittent boluses in 5 patients (8.6%). The median infusion duration was 4.0 days (IQR: 2.0-7.0 days). The median maintenance dose was 0.4 μg/kg/h (IQR: 0.3-0.6 μg/kg/h). The median cumulative dose was 38.4 μg/kg (IQR: 19.2-67.2 μg/kg). Twelve patients (20.7%) received an initial loading bolus of 0.5–1.0 μg/kg over 10 min.
Regarding the timing of initiation, the median time from sepsis diagnosis to first dexmedetomidine administration was 14.5 h (IQR: 6.0-34.0 h). Initiation occurred within the first 24 h in 42 patients (72.4%), between 24–48 h in 11 patients (19.0%), and between 48–72 h in 5 patients (8.6%).
Based on chart review, the primary clinical indications for dexmedetomidine initiation were: (1) early sedation to facilitate mechanical ventilation tolerance in 46 patients (79.3%), typically requiring deeper sedation (RASS −3 to −5) in combination with other sedatives; and (2) later use for weaning or extubation in 12 patients (20.7%), aiming to facilitate ventilator liberation and prevent delirium.
Comparison of Primary Outcome Measures Between Groups
Survival Risk Analysis
This study included 168 mechanically ventilated sepsis patients. During the 28-day follow-up period, 106 deaths occurred (see Table 1), resulting in an all-cause mortality rate of 57.14%. The 28-day mortality rate was 51.72% in the dexmedetomidine group, lower than the 69.09% in the non-dexmedetomidine group. Survival analysis (Figure 2) showed a significant difference in cumulative mortality risk between the two groups (log-rank test, P = 0.0165). The median survival time was 31 days in the Dex group and 23 days in the Non-Dex group. The death risk in the Non-Dex group was 1.627 times that of the Dex group.
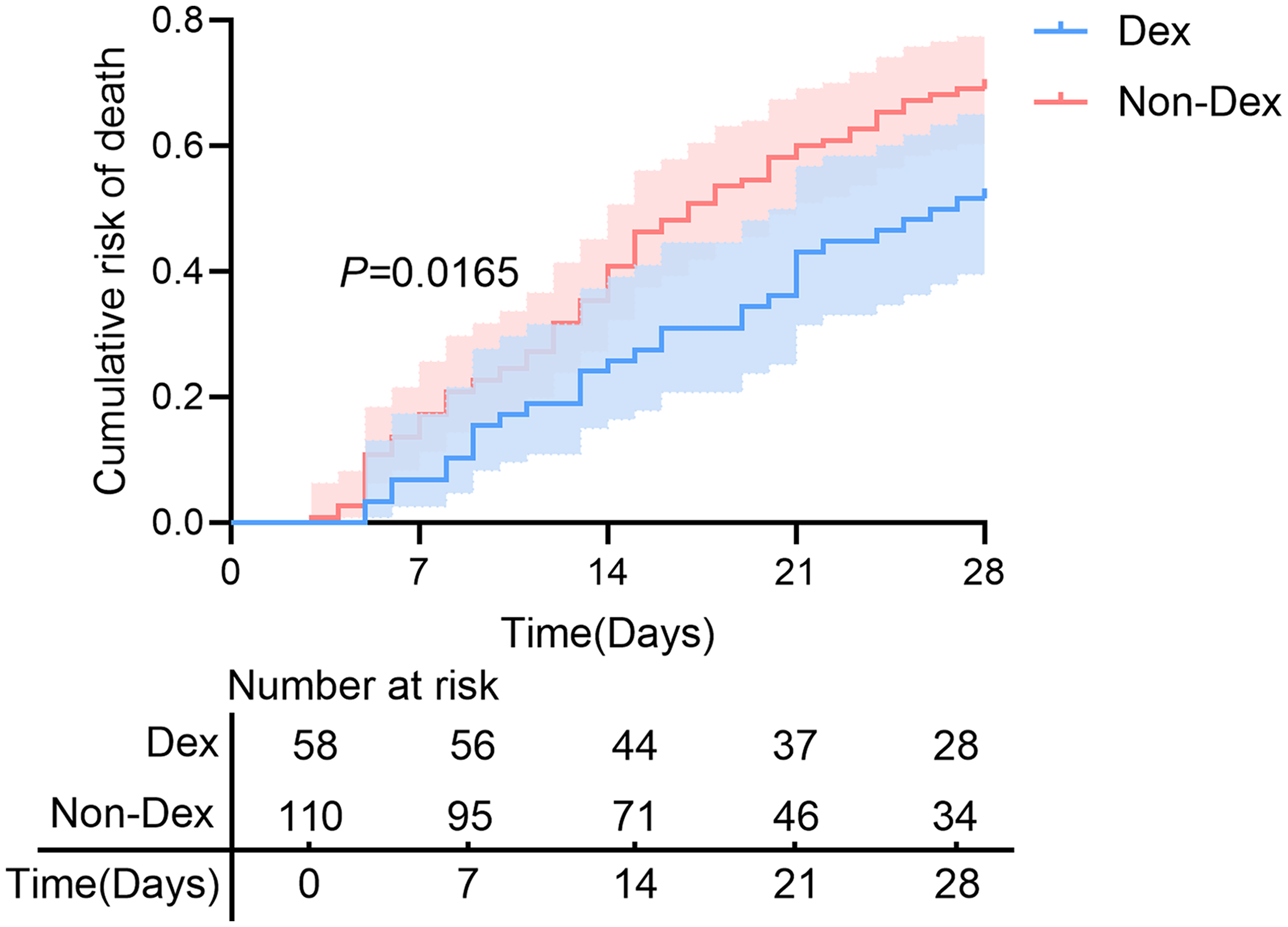
Comparison of Cumulative Mortality Risk Between Dexmedetomidine and Non-Dexmedetomidine Groups. Note: Dex = Dexmedetomidine group, Non-Dex = Non-Dexmedetomidine group.
Cox Regression Results
Based on the results of univariate analysis (P < 0.05), using backward stepwise regression combined with clinical significance, the following variables were included in the multivariable Cox model: group assignment, sex, shock status, vasopressor use, CRRT, white blood cell count, CRP, PCT, lactate level, multi-site infection, history of cerebrovascular disease, chronic liver/renal disease, diabetes, SOFA score, malignancy, and age. Multicollinearity diagnostics showed variance inflation factors for all included variables were less than 5.
The analysis results showed that after adjusting for confounding factors, the 28-day mortality risk remained significantly lower in the dexmedetomidine group compared to the non-dexmedetomidine group (HR = 0.65, 95% CI: 0.46-0.79, P = 0.00362) (Figure 3) . Male sex, age, multi-site infection, history of cerebrovascular disease, history of chronic liver/kidney disease, diabetes, and history of malignancy were independent risk factors for increased mortality, with hazard ratios (HR) of 1.71, 1.02, 1.72, 1.59, 1.47, 1.93, and 1.63, respectively, and corresponding P-values all less than 0.05. Shock status was associated with increased risk (HR = 1.51, 95% CI: 1.32-1.63, P = 0.0012). Conversely, receiving continuous renal replacement therapy and using vasopressors showed protective associations, with HR values of 0.64 and 0.49, respectively. Sensitivity analyses addressing potential time-dependent bias yielded consistent results. In the landmark analysis at 48 h (excluding 12 early deaths), the adjusted HR for 28-day mortality associated with dexmedetomidine exposure was 0.68 (95% CI: 0.49-0.83, P = 0.041). In the time-dependent Cox regression model, the HR was 0.62 (95% CI: 0.44-0.77, P = 0.029). These findings support the robustness of the primary analysis. In an exploratory analysis examining potential dose-response effects, patients in the DEX group were divided into low-dose (<38.4 μg/kg cumulative, n = 29) and high-dose (≥38.4 μg/kg, n = 29) subgroups. Compared with the non-DEX group, the adjusted HRs for 28-day mortality were 0.71 (95% CI: 0.49-0.89) for the low-dose subgroup and 0.58 (95% CI: 0.38-0.76) for the high-dose subgroup, suggesting a trend toward greater benefit with higher cumulative exposure, although the difference between the two DEX subgroups was not statistically significant (P for trend = 0.19). These findings should be considered hypothesis-generating due to limited sample size. In sensitivity analyses examining the impact of initiation timing, the protective association between dexmedetomidine and 28-day mortality persisted when the analysis was restricted to patients who received the drug within the first 24 h (HR = 0.63, 95% CI: 0.44-0.81, P = 0.038) and when late users (>48 h, n = 5) were excluded (HR = 0.64, 95% CI: 0.45-0.80, P = 0.035). These findings suggest that the observed survival benefit is not solely driven by late initiation in less severely ill patients.
Sensitivity Analyses Addressing Potential Overfitting
To assess the robustness of the primary Cox model against potential overfitting due to the EPV of 6.6, several sensitivity analyses were performed. In the LASSO-penalized Cox regression, 9 variables were selected (group, shock, CRRT, vasopressor use, malignancy, diabetes, cerebrovascular disease, SOFA score, and lactate), and the adjusted HR for dexmedetomidine was 0.67 (95% CI: 0.49-0.84, P = 0.031). In the reduced parsimonious model including only age, SOFA score, shock, malignancy, and group assignment (5 variables, EPV ≈ 21.2), the HR for dexmedetomidine was 0.61 (95% CI: 0.43-0.78, P = 0.028). Bootstrap internal validation (500 resamples) yielded an optimism-corrected C-index of 0.73 (original C-index 0.76), indicating acceptable model performance with limited overfitting.
Comparison of Secondary Outcome Measures Between Groups
Duration of mechanical ventilation (hours), hospital length of stay (days), and ICU length of stay (days) were not normally distributed and were compared using the Mann-Whitney U test. The results showed no statistically significant difference in the duration of mechanical ventilation (hours) between the dexmedetomidine and non-dexmedetomidine groups (P = 0.2217). Statistically significant differences were found in ICU length of stay (days) and total hospital length of stay (days) (P = 0.015, 0.0484, respectively) (Figure 4). This may be due to the higher survival rate in the dexmedetomidine group, leading to a longer required rehabilitation period.
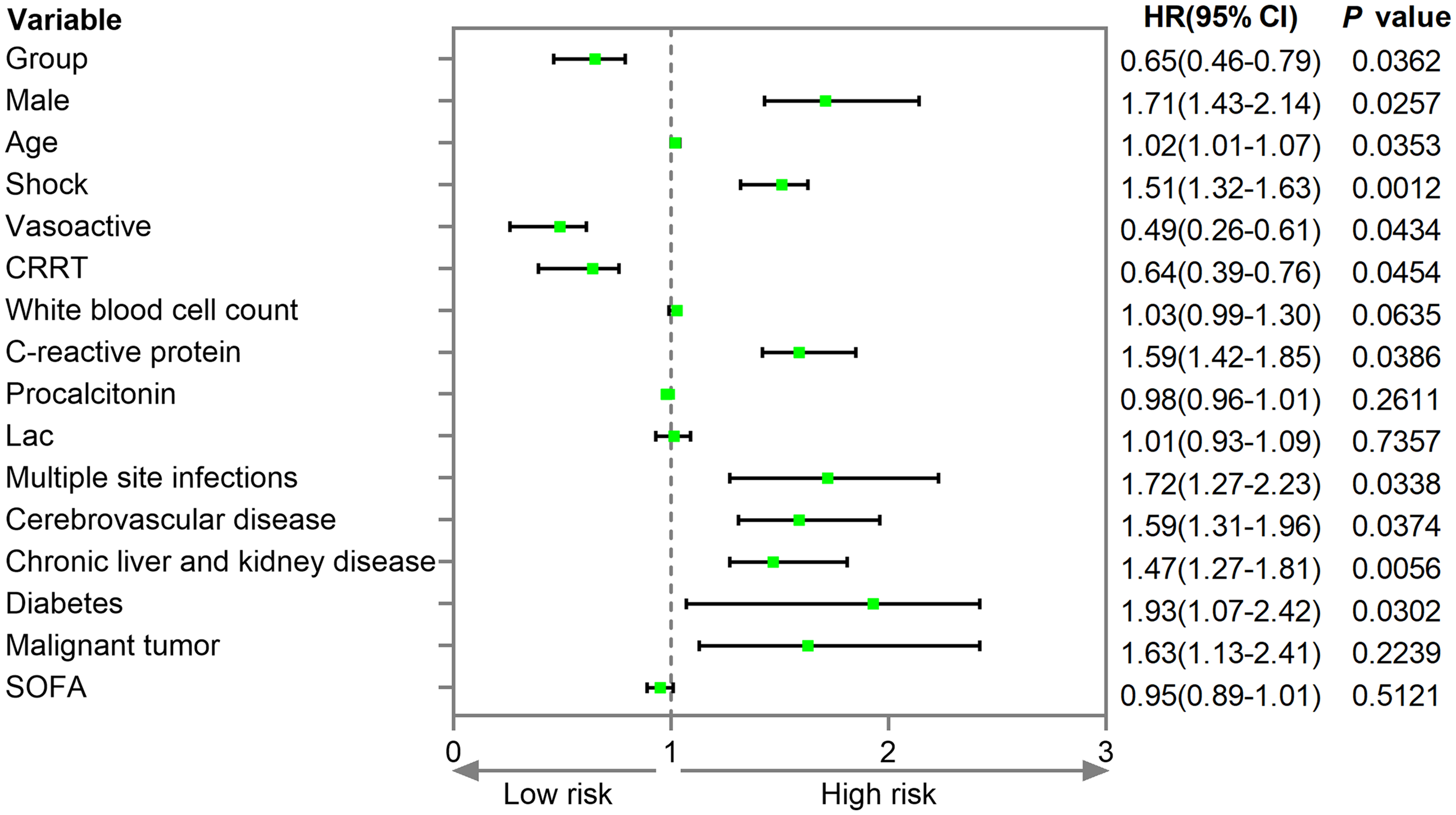
Forest Plot of the Cox Proportional Hazards Model for Enrolled Patients with Sepsis. Note: Group Comparisons Were Referenced Against the non-Dexmedetomidine Group, and all Other Categorical Variables Were Referenced Against the “No” Category. CRRT = Continuous Renal Replacement Therapy. SOFA = Sequential Organ Failure Assessment, Lac = Lactate.
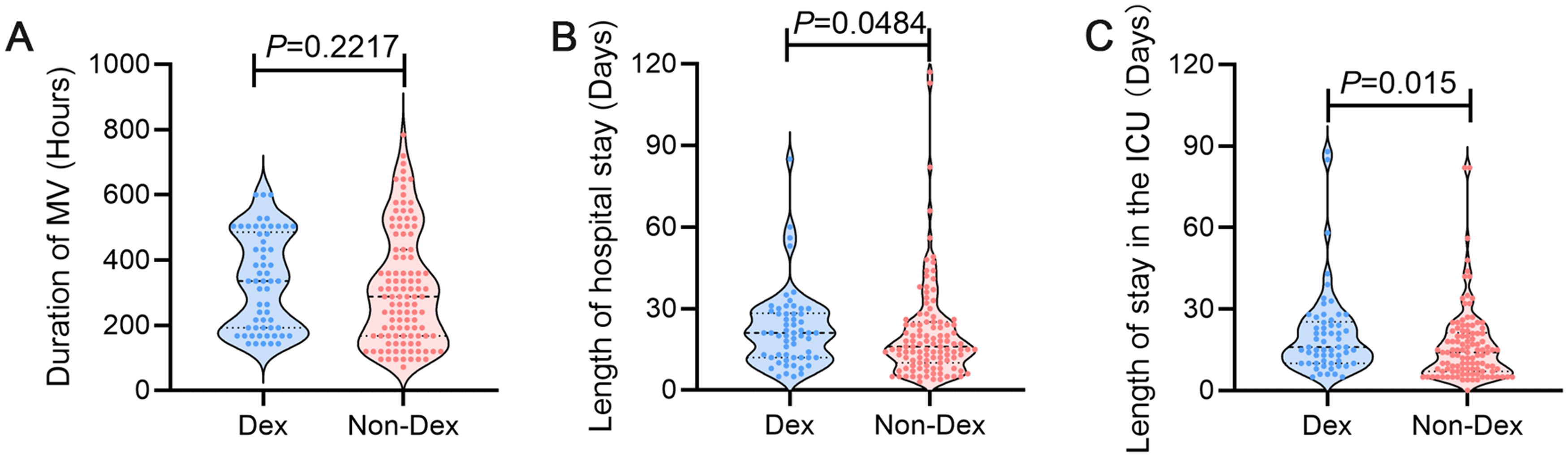
Comparison of Secondary Outcomes Between the Two Groups. Note: Dex = Dexmedetomidine group, Non-Dex = Non-Dexmedetomidine group.
Comparison of BALF Inflammatory Factors and Oxidative Stress Levels Between Groups
As shown in Figure 5, utilizing the hospital's sepsis patient data platform and acute lung injury biobank, we measured BALF inflammatory factors and oxidative stress indicators in both groups (if multiple bronchoscopies were performed, the specimen obtained 48 h to 1 week after sedative use was selected). There were 8 missing BALF specimens (4.8%). Multiple imputation was performed as detailed in the Methods section (2.2.4). After imputation, all data fell within normal ranges. Complete-case analysis (excluding the 8 patients) yielded nearly identical results, and a worst-case sensitivity analysis assuming MNAR also showed significant between-group differences (all P < 0.05), supporting the robustness of the findings. Data from both groups were not normally distributed and were analyzed using non-parametric tests. The results showed significantly lower levels of the inflammatory factors (TNF-α, IL-6), as well as significant improvement in oxidative stress markers (MDA, SOD) in the dexmedetomidine-exposed group BALF, with all differences being statistically significant (P < 0.05).
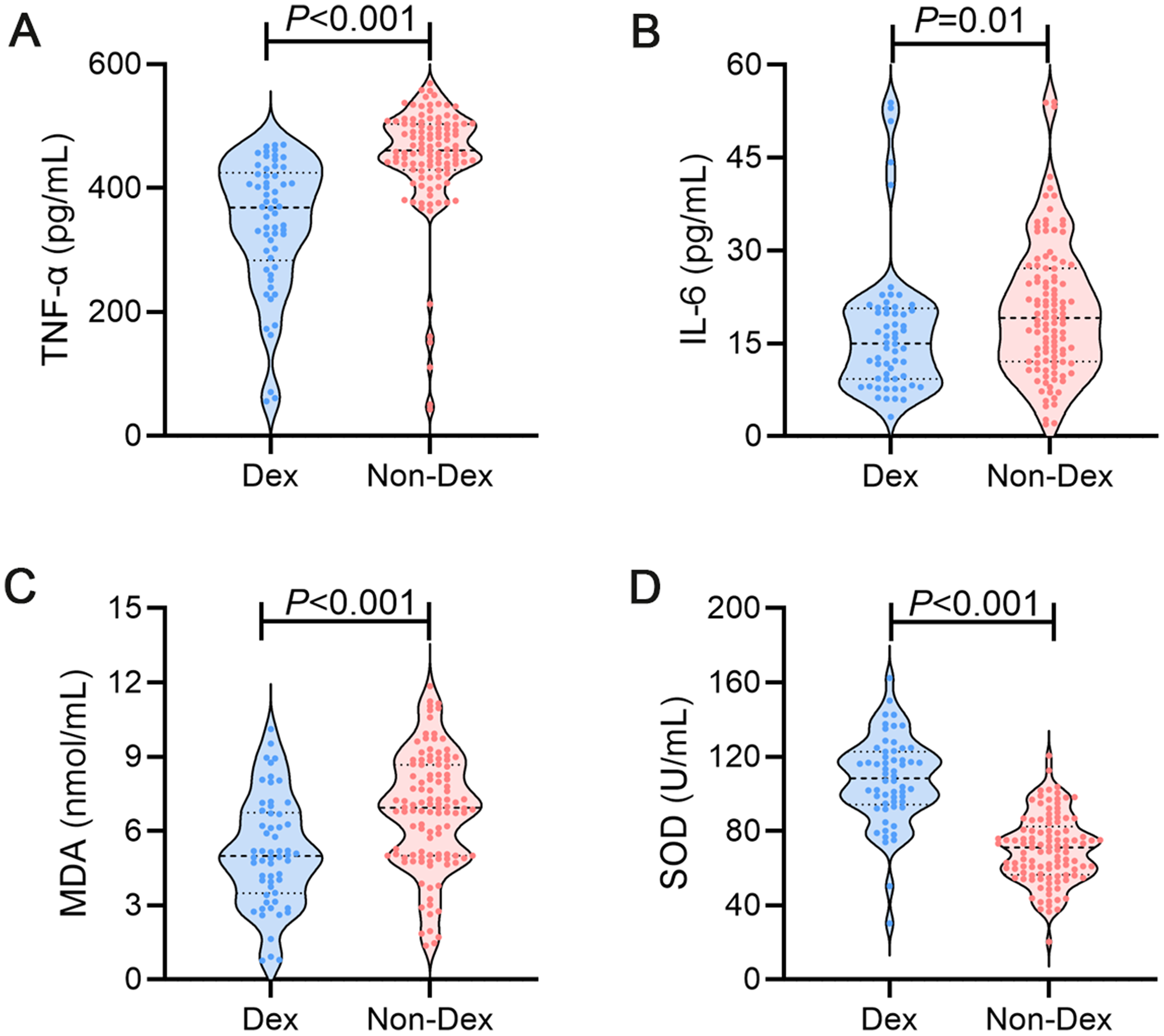
Comparison of Inflammatory and Oxidative Stress Markers in BALF Between the Two Groups. Note: Dex = Dexmedetomidine Group, Non-Dex = Non-Dexmedetomidine Group. TNF-α = Tumor Necrosis Factor-Alpha, IL-6 = Interleukin-6. MDA = Malondialdehyde, SOD = Superoxide Dismutase.
Among the 160 patients with available BALF samples (8 missing), the median time from sedative initiation to BALF collection was 96 h (IQR: 72-120 h). The distribution of collection timing was similar between the DEX and non-DEX groups (P = 0.42). To assess whether collection timing influenced these results, several sensitivity analyses were performed. First, adding the exact collection time as a covariate in the between-group comparison did not alter the significance of the differences (all P < 0.05). Second, stratified analysis by time window (48-72 h, 72-96 h, 96-120 h, 120-168 h) showed consistent directional effects across all strata. Third, when the analysis was restricted to the narrower window of 72–120 h (n = 96), all between-group differences remained statistically significant. These findings suggest that the observed differences in BALF biomarkers between the two groups are robust to variability in collection timing.
Several limitations of this study should be acknowledged. First, this was a single-center retrospective cohort study, and residual confounding cannot be completely excluded despite multivariable adjustment and IPTW sensitivity analysis. Second, dexmedetomidine exposure was heterogeneous in terms of timing, indication, dose, and duration, and was primarily analyzed as a binary variable. Although multiple sensitivity analyses yielded consistent results, the potential for time-dependent bias, confounding by indication, and uncertainty regarding the optimal dosing strategy remain. Third, the EPV of the primary Cox model was lower than ideal, raising the possibility of overfitting, although LASSO regression, a reduced parsimonious model, and bootstrap internal validation supported the robustness of the findings. Fourth, BALF samples were collected at variable time points within a relatively wide window because of the retrospective and clinically driven nature of bronchoscopy. Although additional sensitivity analyses suggested that this variability did not materially affect the results, prospective studies with standardized and serial sampling would be preferable. Finally, the generalizability of our findings to other populations and healthcare settings remains uncertain and requires validation in larger prospective multicenter studies. Despite these limitations, our study provides novel clinical evidence linking dexmedetomidine use with improved pulmonary inflammatory and oxidative stress profiles in mechanically ventilated sepsis patients.
Conclusion
This retrospective cohort study, conducted using the hospital's sepsis data platform and acute lung injury biobank targeting mechanically ventilated sepsis patients, aimed to explore the association between dexmedetomidine exposure and clinical prognosis, rather than to establish causality. It innovatively assessed the impact of dexmedetomidine on local pulmonary inflammation and oxidative stress status through BALF sample analysis. The primary outcome showed that after adjusting for multiple confounders such as disease severity, shock status, and organ support, dexmedetomidine exposure was independently associated with reduced 28-day mortality risk. Secondary outcomes showed no statistically significant difference in the duration of mechanical ventilation between the dexmedetomidine and non-dexmedetomidine groups, but statistically significant differences were found in ICU and hospital length of stay. Notably, the dexmedetomidine-exposed group showed lower levels of the inflammatory factors TNF-α and IL-6 in BALF, along with significant improvement in oxidative stress markers (lower MDA and higher SOD). This suggests that dexmedetomidine ameliorated the oxidative stress state accompanying the local pulmonary inflammatory storm, potentially contributing to a stronger trend toward survival benefit. The finding provides clinical clues for explaining the potential mechanism underlying its improvement of sepsis prognosis.
These findings are consistent with most existing clinical evidence. A post-hoc subgroup analysis of the MENDS randomized controlled trial indicated that compared to lorazepam, dexmedetomidine reduced the 28-day mortality risk in mechanically ventilated sepsis patients, with a more pronounced benefit in sepsis patients compared to non-sepsis patients. 20 A Japanese retrospective study also supports the protective effect of dexmedetomidine, finding that compared to midazolam or propofol, it significantly reduced 28-day all-cause mortality and shortened mechanical ventilation duration in mechanically ventilated sepsis patients. 23 The potential protective effect of dexmedetomidine in sepsis patients may stem from its multi-target pharmacological properties, including anti-inflammatory, antioxidant, organ-protective, and sympatholytic effects.24–27 Animal experiments confirmed that the drug can inhibit lipopolysaccharide-induced sympathetic overexcitation and superoxide generation, downregulate plasma TNF-α and IL-1β levels, thereby attenuating injury to vital organs such as the lungs and kidneys. 28 Beyond inhibiting the sympathetic pathway, dexmedetomidine might also modulate the stress response by activating the cholinergic anti-inflammatory pathway. The pathway primarily acts through the α7 nicotinic acetylcholine receptor on macrophages, playing a crucial role in suppressing systemic excessive inflammation and oxidative stress. 18 Consequently, unlike most previous clinical studies focusing on systemic indicators,20,21 our study, through direct measurement of inflammatory and oxidative stress markers in BALF, provided the first clinical evidence at the patient level that dexmedetomidine may significantly improve the pathological microenvironment of local lung injury in mechanically ventilated sepsis patients. Pro-inflammatory cytokines (TNF-α, IL-6) and the oxidative stress marker MDA in BALF were significantly lower in the dexmedetomidine group, while antioxidant enzyme SOD activity was significantly higher. These results not only confirm the key role of inflammation and oxidative stress in sepsis-induced lung injury but also suggest that dexmedetomidine may improve patient prognosis by reducing pulmonary oxidative damage and inflammatory response, which is highly consistent with its anti-inflammatory, antioxidant, and organ-protective mechanisms demonstrated in animal experiments.14,15,29
Although no significant difference was observed in the duration of mechanical ventilation between the two groups, the significantly longer ICU and hospital stays in the dexmedetomidine group, combined with its lower in-hospital mortality, suggested that dexmedetomidine may, by reducing inflammation and improving organ function, enable more critically ill patients to survive the acute critical phase and progress to the rehabilitation stage. In contrast, patients in the non-dexmedetomidine group may have experienced early death due to rapid disease progression, shortening their hospital stay. Therefore, the prolonged hospital stay was not accompanied by an increased mortality risk but was instead associated with improved patient survival. This reflects, to some extent, a shift in the paradigm of critical care: the success of treatment is not only measured by the shortening of short-term organ support duration but also by the survival of critically ill patients entering subsequent recovery. This result aligns with recent clinical observations regarding the “prolonged recovery period in surviving critically ill patients,” suggesting that extended hospital stay may be a concomitant phenomenon of improved outcomes in critical care. 30
In summary, the results of the study indicate that dexmedetomidine reduces the 28-day mortality risk in mechanically ventilated sepsis patients, and this protective effect may be related to its ability to ameliorate local pulmonary inflammation and oxidative stress. The study innovatively links the local pulmonary microenvironment with clinical outcomes in sepsis patients, providing potential clinical evidence for the organ-protective role of dexmedetomidine in sepsis-induced lung injury, extending its role from a traditional sedative to an adjunctive therapy with potential disease-modifying effects. Future prospective multicenter studies are needed to further validate the targeted therapeutic value of dexmedetomidine in patients with specific biomarker phenotypes (eg, high oxidative stress status) and to clarify its optimal timing, dosage, and synergistic effects with other sedatives, thereby advancing the development of personalized sedation and organ protection strategies in sepsis.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the Department of Education of Anhui Province, Anhui Medical University, (grant number 2025AHGXZK30415, 2023xkj131).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.