
Abstract
Background
Midline catheters (MC) are 10-20 cm intravenous (IV) lines inserted in the peripheral veins of the upper arm and utilized for patients who require longer term IV access, making them advantageous in the intensive care unit (ICU). Guidelines on medication infusion through MC are limited and clinical practice varies. It is unclear how MC practice variation affects critical care fellowship experience.
Objectives
We sought to investigate the relationship between institutional practices surrounding MC and the role of trainees.
Methods
A survey was sent to all Critical Care Fellowship program directors investigating their use of MC. Program type, number of hospital beds and trainees were collected. The use of vasopressors (VP), hypertonic saline (HS), and parenteral nutrition (PN) through MC was assessed, as well as which providers were placing MC (interventional radiology (IR), fellows, residents, or advanced practice providers). Statistical analysis was performed using IBM SPSS statistics. Associations between clinical variables were assessed using Fisher's exact test.
Results
Seventy programs responded to the survey (30.4% response rate). Of these 70 programs, 53 (75.7%) reported MC use. IR placed MC at 79.2% of programs. Larger hospitals (≥500 beds) were significantly more likely to use IR (88.9% vs 58.8%, P = .025), while smaller hospitals more often utilized residents (17.6% vs 2.8%, P = .032). Among programs using MC, 66% administered vasopressors (VP), 62.3% used hypertonic saline (HS), and 20.8% gave parenteral nutrition (PN). Critically, programs with fellow-placed MC were significantly more likely to use VPs (93.3% vs 55.3%, P = .03) and PN (33.3% vs 15.8%, P = .030) compared to programs without fellow involvement. No differences in MC use were found across institution types, bed capacities, or trainee numbers.
Conclusions
Though MC use in critical care ICUs in the US is prevalent, hospital factors appear to influence who is placing the MC and how MC are utilized.
Keywords
Introduction
Venous access for the delivery of vasopressors, hypertonic saline (HS), and parenteral nutrition (PN) is essential for a majority of intensive care unit (ICU) treatment plans. Traditionally, a central venous catheter (CVC) has been the standard for the administration of certain medications, when multiple lumens are needed and when required access is anticipated for a prolonged duration. Although CVC is commonly utilized for critically ill patients, it is associated with increased morbidity due to pneumothorax, bloodstream infection, deep vein thrombosis, and arterial puncture.1–3
Recent literature suggests that midline catheters (MC) may serve as a viable alternative to CVC.4,5 MC are 10-20 cm intravenous lines inserted into deep peripheral veins of the arm - typically the basilic, cephalic, or brachial - with the tip terminating at or below the axillary vein. 6 They are currently indicated for patients with difficult intravenous access or those requiring venous access for more than six days. 7
In the clinical setting, MC represent a “middle ground” between central access (peripherally inserted catheters [PICC] and CVC) and peripheral intravenous access. MC offer similar dwell times as PICC and reduce the risks inherent to CVC placement. However, they offer more secure long term access than standard peripheral intravenous access.8,9 Compared to CVC, MC have been associated with a 69% reduction in the odds of mortality, bloodstream infection, mechanical complications, thrombosis, and line-related readmission. 4 Device-related bloodstream infection rates range from 0-0.9%, comparable to standard peripheral intravenous catheters (PIV), but substantially lower than those reported for PICC and CVC.8–10 MC placement may also provide notable cost savings, particularly in patients with difficult access or to circumvent prolonged CVC placement. 8 By reducing repeated venipuncture, minimizing complications, and supporting intermediate-term vascular access, MC offer a potentially safe, efficient, and cost-effective peripheral venous access device option.
Despite these advantages, MC use is not without risk. Potential complications include bloodstream infection, thrombosis, occlusion, leakage, dislodgement, and extravascular infiltration.7,11,12 A 2021 systematic review by Tripathi et al noted a midline catheter failure rate of 12.5% and calculated adjusted average rates of other significant complications, factoring in sample size, to be 4.1% for deep vein thrombosis, 5.0% for dislodgement, 3.8% for occlusion, 3.4% for phlebitis, and 1.9% for infiltration. 9 Furthermore, evidence regarding vasopressor administration through MC remains limited, though a recent study suggests they can be safely and effectively used for prolonged infusions. 13
Although gaining popularity, MC utilization varies considerably across hospitals. 11 MC placement requires ultrasound guidance, which may limit its use across institutions due to personnel training. 7 However, the extent to which variation in practice and training influences MC utilization has not been well explored in the literature. To our knowledge, no national survey of fellowship programs regarding MC current practices, training exposure, and perceived barriers to better characterize MC utilization has been conducted. The objective of this study was to characterize national MC practices in ICUs and determine how institutional characteristics and trainee involvement influence MC utilization patterns, with a focus on medications, duration limits, placement personnel, and training perspectives.
Methods
A multicenter, anonymous survey of all critical care fellowships in the United States was conducted. Survey questions were developed using a consensus panel of experts in critical care. An independent group of reviewers then validated the questions for relevance, clarity, and educational merit. The survey was distributed electronically to 230 fellowship program directors identified through the American Medical Association Residency and Fellowship Database. Responses were collected from February 2025 through May 2025. The study was deemed IRB exempt by the George Washington University Hospitals review board, NCR245646. Study data were collected and managed using REDCap electronic data capture tools hosted at George Washington University Hospital. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies. 14
The survey introduced midline catheters using its common descriptor: “a venous access device inserted into a peripheral vein of the upper arm (either the basilic, cephalic, or brachial vein) with the distal tip located at the level of the axilla in children and adults”.6,8 Respondents provided institutional demographic information, including hospital type, total bed capacity, and number of trainees. Questions assessed whether midline catheters were used in their intensive care units, the types of providers responsible for insertion (interventional radiology (IR), fellows, residents, or advanced practice providers (APPs)), and the training methods employed for placement. Program directors were asked to report their institutional practices regarding medication administration through midlines, specifically the use of vasopressors (VP), hypertonic saline (HS), and parenteral nutrition (PN), as well as any limits placed on the duration of such infusions. Additional items addressed perceived educational value of midline catheter training, adequacy of vascular access after adoption of midlines, and whether respondents believed midline use had reduced central line–associated bloodstream infections. Survey responses were collected anonymously and statistical analysis was performed using IBM SPSS Statistics [version 30.0] (IBM Corp., Armonk, N.Y., USA). Descriptive statistics were calculated for all variables, with categorical variables presented as frequencies and percentages, and continuous variables presented as means with standard deviations and medians with ranges. Associations between categorical variables were assessed using Pearson's chi-square test. When chi-square assumptions were violated (expected cell counts <5 in >20% of cells), Fisher's exact test was used instead. Statistical significance was set at P < .05 for all analyses.
Results
Response Rates and Demographics
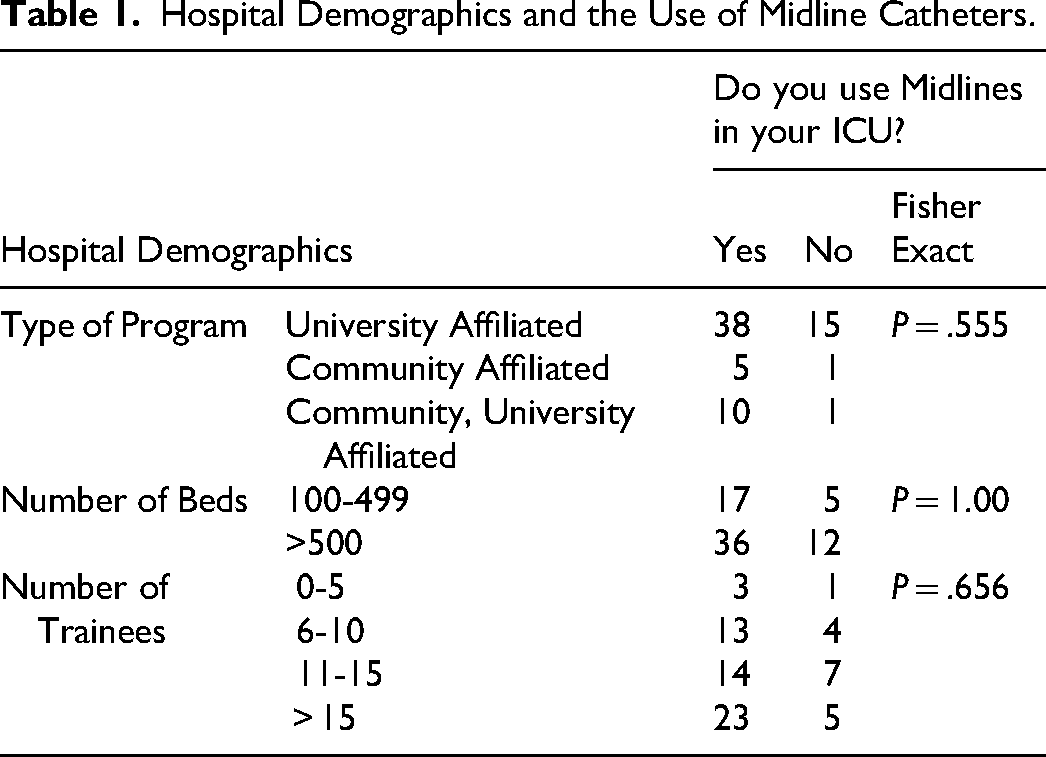
Of the 230 Critical Care Fellowship program directors contacted, 70 (30.4%) completed the survey. Responding institutions varied in type, bed capacity, and trainee volume, with the majority (75.7%) being university-affiliated. (Table 1). Of the 70 survey respondents, 53 (75.7%) reported MC use in the ICU. There was no significant association between institution type, number of beds, or number of trainees and midline catheter use. Midline utilization was high across all program types. There was no difference in the use of VP, HS, or PN across institution types, bed capacities, or the number of trainees.
Hospital Demographics and the Use of Midline Catheters.
Who Places Midlines
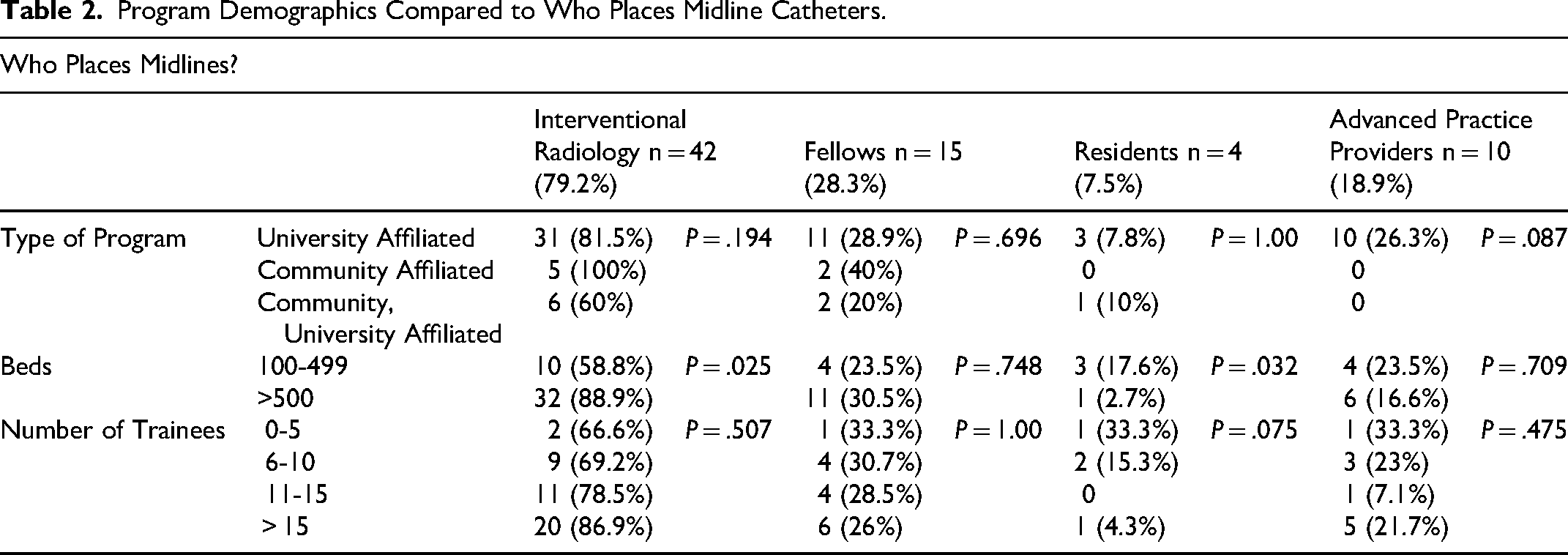
Forty two (79.2%) programs indicated IR as the provider inserting MC. (Table 2) Critical care fellows, rotating residents, and APPs insert MC at 15 (28.3%), 4 (7.5%), and 10 (18.9%) programs, respectively. IR teams were reported to be available for MC insertion during weekday day time hours at 41 (97.6%) of programs, weekday night time hours at 13 (31.0%) of programs, and on weekends at 24 (57.1%) of programs. Larger hospitals (≥500 beds) are significantly more likely to have IR place MC compared to smaller hospitals (88.9% vs 58.8%, P = .025). (Table 2) Smaller hospitals (100-499 beds) are significantly more likely to have residents place MC compared to larger hospitals (17.6% vs 2.8%, P = .032). There was no significance associated with the type of program nor the number of trainees in regards to which service places the MC.
Program Demographics Compared to Who Places Midline Catheters.
Medication Utilization Patterns
VP use was reported in 35 (66.0%) of those who used MC. Norepinephrine was the most frequently administered agent (85.7%), followed by phenylephrine (68.6%), epinephrine (57.1%), vasopressin (57.1%), and dopamine (51.4%), while angiotensin II (22.9%) was used less commonly (Figure 1). Twenty one (60%) respondents reported no duration limit to the infusion of VP. A smaller proportion of respondents, 9 (25.7%), indicated a 24-72 h duration limit and 5 (14.3%) indicated a < 24 h limit for vasopressor use in MC. Of the 53 programs using MC, fellows placed them at 15 (28.3%) programs. Programs utilizing fellows for MC placement were significantly more likely to use vasopressors compared to programs using alternative providers (93.3% vs 55.3%, P = .03). This association was not observed for IR, resident, or APP placement.
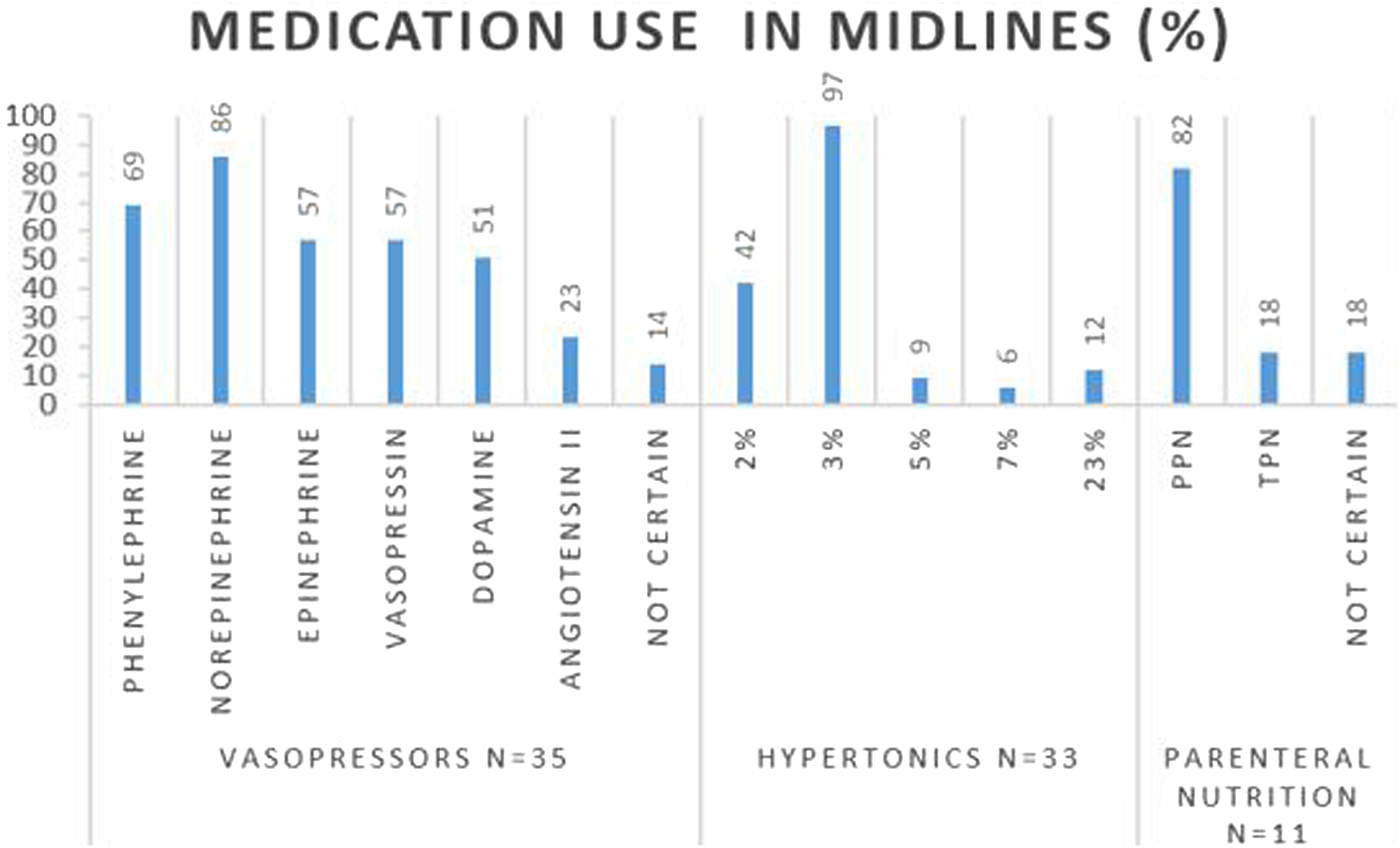
Medication use in midlines across all training hospitals.
Association Between Fellow Placement and Advanced Applications
Hypertonic saline (HS) administration through MC was reported in 33 (62.3%) of those who used MC, with 3% as the most frequently used concentration (97%). Fifteen (45%) respondents reported having no duration limit on infusion of hypertonic saline with 14 (42%) respondents indicating uncertainty on duration limits. There was no significant correlation between any providers placing MC and the use of hypertonics. (Table 3)
Clinical Utilization of Midline Catheters.
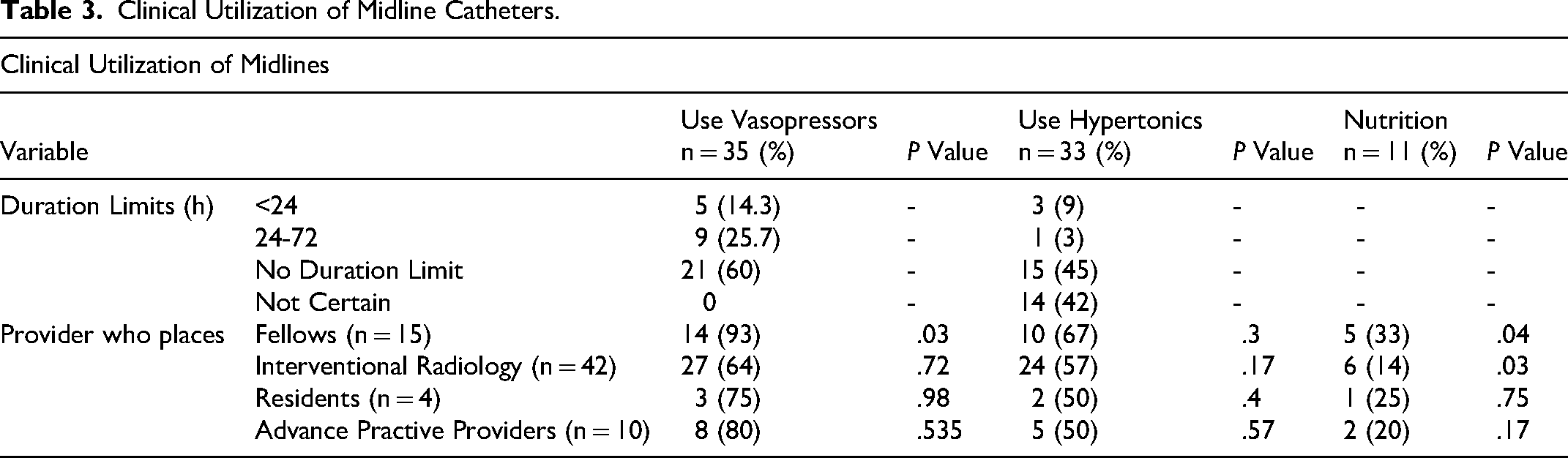
Parenteral nutrition administration through MC was reported in 11 (20.8%) programs using MC. Of these, 9 (81.8%) permitted partial PN, 2 (18.2%) permitted total PN, and 2 (18.2%) were uncertain. Two distinct practice patterns emerged: programs utilizing fellows for MC placement were significantly more likely to administer PN through midlines (33.3% vs 15.8%, P = .030), while programs relying on IR for placement were significantly less likely to use PN (54.5% vs 80.6%, P = .030). No significant associations were found with resident or APP placement.
To assess whether institutions adopted uniform versus medication-specific policies, we examined associations between high-risk medication uses and created a composite score (0-3) representing the number of high-risk medication classes used through midlines. Overall, 35 programs (50.0%) did not use midlines for any high-risk medications, 18 (25.7%) used them for one medication class, 12 (17.1%) for two classes, and 5 (7.1%) for all three classes.
Parenteral nutrition use was significantly associated with both vasopressor use (P = .023) and hypertonic saline use (P = .021). Among programs using vasopressors, 28.6% (10/35) also administered parenteral nutrition, compared to 6.3% (1/16) of programs not using vasopressors. Similarly, 30.3% (10/33) of programs using hypertonic saline also used parenteral nutrition, whereas none of the programs avoiding hypertonic saline permitted PN (0/10). Among the 11 programs permitting parenteral nutrition, 10 (90.9%) used it in combination with at least one other high-risk medication class, with 5 (45.5%) using all three classes. In contrast, vasopressor and hypertonic saline use were not significantly associated (P = .452).
The number of high-risk medication classes used was not significantly associated with fellow involvement in catheter placement (P = .927), suggesting the ‘all-in’ pattern reflects institutional culture rather than procedural training factors.”
Educational and Clinical Perspectives
Fellows and residents are trained to place MC most frequently by senior fellows (60.0%). Of the programs that utilize fellows for MC placement, 100% of program directors indicated that they felt it was apositive educational experience for the trainees.
MC dressings are changed via a nursing protocol similar to central line dressings at 39 (73.6%) of the institutions who report using MC; 12 (22.6%) were uncertain of the protocol utilized at their institution. Of those who utilize MC, 12 (28.3%) reported a reduction in CLABSIs with the utilization of MC. However, 28 (52.8%) programs were uncertain if rates of CLABSIs have reduced with MC utilization. A reduction in the incidence of inadequate vascular access with the introduction of MC was reported at 25 (47.2%) institutions. Of those who do not utilize MC, 8 (47.1%) reported an interest in adding MC as a vascular access option in their ICU; 7 (41.2%) were uncertain regarding interest, and 2 (11.8%) reported no.
Discussion
In this national survey of critical care fellowship programs, we found that MC are widely incorporated into ICU practice, with three-quarters of responding programs reporting their use. Vasopressors were the most frequently administered high-risk medications through MC, with norepinephrine cited most often. Hypertonic saline was also commonly infused, typically in 3% concentrations, whereas PN was rarely permitted, though a small proportion of programs allowed total PN administration via MC. Importantly, fellow involvement appeared to be associated with practice variation: Programs in which fellows placed midlines were significantly more likely to use them for vasopressors and PN. Institutional size influenced who placed midlines, with larger hospitals relying more on interventional radiology, while smaller hospitals involve residents. However, hospital size did not affect overall adoption of MC use.
A central finding of this study is the strong association between trainee involvement and expanded MC utilization. Programs in which fellows placed MC demonstrated significantly higher rates of vasopressor and parenteral nutrition administration compared to programs relying on other providers. This pattern suggests that hands-on procedural experience may foster greater institutional comfort with advanced MC applications. Conversely, the inverse relationship between IR placement and PN use raises the possibility that programs depending on IR for MC insertion may adopt more conservative medication protocols, potentially reflecting differing risk tolerance or communication barriers between services. Notably, the ‘all-in’ pattern was relatively uncommon (7.1% of all programs), and half of programs did not use midlines for any high-risk medications, suggesting considerable institutional heterogeneity in risk tolerance. The finding that fellow involvement did not predict the number of high-risk medication classes used (P = .927) indicates that while fellows’ procedural involvement correlates with use of specific medications (as demonstrated earlier), the broader institutional philosophy of aggressive versus conservative midline adoption operates independently of training structure.
These findings carry several clinical implications. The frequent use of vasopressors through MC aligns with emerging evidence supporting their safety in select patients. Prasanna et al demonstrated that vasopressor administration via MC was not associated with higher extravasation or failure rates than central lines, 13 and systematic reviews suggest vasoactive agents can be used safely under defined conditions.6,9 In contrast, PN administration through MC remains controversial. Infusion Nurses Society standards recommend against midlines for PN or for solutions exceeding 900 mOsm/L, citing risks of thrombosis and extravasation.15,16 Our finding that some institutions permit PN highlights a need for further research to define safety in this domain. Hypertonic saline infusion through MC appeared to be widely accepted, consistent with reports that 3% NaCl can be tolerated, though institutional policies regarding duration limits varied considerably.15,16
The educational implications merit emphasis. Program directors universally endorsed MC placement as valuable for trainees, and our data suggest that procedural competence among critical care housestaff translates into expanded clinical application. This finding has parallels in other procedural domains, where provider familiarity influences practice patterns. However, it also raises questions about whether trainee-driven expansion of MC use is evidence-based or represents institutional practice drift. Further research should examine whether fellow-placed midlines are associated with different complication rates or outcomes compared to IR-placed lines.
Our findings both confirm and extend prior work. Consistent with previous guidelines, we observed substantial variation in midline use across institutions. 10 Previous observational cohorts and systematic reviews have documented heterogeneity in dwell times, complications, and outcomes.9,11 Recent comparative studies underscore the trade-offs: Swaminathan et al reported that MC had lower infection and occlusion rates than PICCs for short-term indications 17 , whereas Thomsen et al, in a randomized trial, found no difference in catheter-related bloodstream infection but a higher overall complication rate with MC. 6 By adding a national perspective specific to fellowship programs, our study also identifies a novel association between fellow involvement and broader adoption of high-risk infusions through MC.
Several limitations warrant mention. Our survey response rate of 30% raises the possibility of nonresponse bias, and the anonymous design prevents exclusion of duplicate responses from the same institution. We did not capture catheter length or tip position, both of which may influence complication rates, and no patient-level outcome data were collected. Thus, our findings reflect reported practices rather than directly measured safety or efficacy. We did not assess the training level or competency requirements for fellows placing MC, which may influence both procedural success rates and institutional comfort with advanced applications. Additionally, we did not capture complication rates or patient outcomes, limiting our ability to determine whether practice variations impact safety.
Future work should address these gaps. Prospective multicenter studies are needed to evaluate the safety of vasopressors and PN through MC, ideally stratified by catheter characteristics. Randomized and observational studies to date have yielded mixed results, reinforcing the need for further evidence.6,17 Efforts to define appropriate duration limits for high-risk infusions are also warranted, as evidence-based training protocols could standardize safe practice across institutions.
Conclusions
MC are widely adopted in US ICUs. Vasopressors and hypertonic saline are frequently infused, often without explicit duration limits, whereas PN remains rare but present. Fellow involvement strongly predicts expanded utilization, while institutional size dictates who places midlines but not whether they are used. These findings highlight the variability of practice and the urgent need for evidence-based guidelines and prospective outcome studies to define the optimal role of MC in critical care.
Footnotes
Acknowledgments
The authors thank the critical care fellowship program directors who participated in this survey for their time and thoughtful responses. The authors also acknowledge George Washington University Hospital for institutional support.
ORCID iDs
Ethical Approval Statement
This study was reviewed by the George Washington University Hospital Institutional Review Board and was deemed exempt from review (IRB protocol NCR245646).
Patient Consent Statement
Not applicable. This study did not involve human subjects or identifiable patient data
Author Contributions
All authors contributed substantially to the conception and design of the study. Survey development was performed by the study authors. Data collection was conducted by the authors. Statistical analysis was performed by the authors. All authors contributed to data interpretation, drafting and critical revision of the manuscript for important intellectual content, approved the final version of the manuscript, and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Data are not publicly available due to institutional policies and to protect respondent confidentiality.
Permissions / Prior Publication Disclosure
This work has not been previously published and is not under consideration for publication elsewhere. No portion of this manuscript has been funded by tobacco industry sources. Portions of this work have not been presented as abstracts at scientific meetings. No data in this manuscript have been derived from previously published reports.