
Abstract
Objective
This study aimed to compare the clinical efficacy of intravascular ultrasound (IVUS)-guided versus coronary angiography (CAG)-guided percutaneous coronary intervention (PCI) in patients with coronary heart disease (CHD).
Methods
One hundred CHD patients were randomized into two groups. The control group (n = 50) underwent CAG-guided PCI, while the study group (n = 50) underwent IVUS examination following CAG and received IVUS-guided PCI. Evaluated outcomes included lesion characteristics, stent parameters, postoperative complications, major adverse cardiovascular events (MACE), and coronary restenosis.
Results
Following stent implantation, the minimal lumen diameter in the study group was wider than that in the control group, while the diameter stenosis and plaque burden were lower than those in the control group (P < .05). The maximum stent diameter, maximum balloon diameter for post-dilation, maximum balloon pressure, immediate postoperative minimum stent diameter, and minimum stent cross-sectional area in the study group were greater than those in the control group. Additionally, the stent placement success rate in the study group was higher than that in the control group (P < .05). There was no difference in postoperative complications between the two groups (P > .05). During one-year follow-up, the study group had lower incidence of MACE compared with the control group (P < .05). The incidence of stent restenosis in the study group was lower than that in the control group, but the difference was not statistically significant (P > .05).
Conclusion
Compared with CAG guidance alone, IVUS-guided PCI for CHD can effectively improve coronary blood flow, enhance stent implantation efficacy, and reduce MACE incidence.
Keywords
Introduction
Coronary heart disease (CHD) is one of the most prevalent cardiovascular disorders worldwide. Its primary pathological basis is coronary atherosclerosis, which can result in myocardial ischemia, hypoxia, and even necrosis. 1 In recent years, remarkable advances in coronary intervention have enabled more effective percutaneous management of complex coronary lesions. 2 Percutaneous coronary intervention (PCI) has become a cornerstone in the treatment of coronary atherosclerotic disease, effectively reducing mortality and improving patient outcomes. 3 Evidence consistently supports PCI as the most widely applied invasive therapeutic strategy for patients with CHD.4,5 When PCI is indicated, the therapeutic goal should be complete revascularization achieved through physiology- and imaging-guided interventions with optimal lesion preparation. 6
For decades, coronary angiography (CAG) has served as the gold standard for diagnosing coronary artery disease and guiding PCI. 7 Although relatively safe, CAG remains an invasive examination with potential risks and complications. 8 Moreover, its role in guiding PCI is inherently limited. As a two-dimensional lumen imaging modality, CAG cannot provide detailed information about vascular wall structure, plaque composition, degree of stenosis, or lesion length. It also lacks the ability to evaluate stent apposition and expansion following deployment, factors that are critical in preventing adverse outcomes such as in-stent restenosis and stent thrombosis, which may compromise the long-term efficacy of PCI.9,10
Intravascular ultrasound (IVUS) has emerged as a valuable intravascular imaging modality capable of overcoming many of the limitations of CAG-guided PCI. 10 By providing high-resolution, cross-sectional images of the coronary arteries, IVUS allows for detailed visualization of both the lumen and vessel wall. This capability facilitates precise assessment of plaque morphology, accurate measurement of vessel dimensions, and more rational stent selection and deployment.10–12 PCI guided by IVUS is therefore expected to reduce peri-procedural complications and enhance long-term clinical outcomes. 10
Although multiple studies and meta-analyses in recent years have demonstrated that IVUS-guided PCI can significantly improve prognosis, particularly in complex lesions such as left main disease, bifurcations, and long lesions,10,13,14 its routine application remains debated, and adoption rates vary widely among centers. Thus, clarifying the clinical value of IVUS guidance has important implications for standardizing interventional practice and improving patient outcomes. The present study was designed to comprehensively evaluate the efficacy of IVUS-guided PCI compared with CAG-guided PCI in patients with CHD, focusing on lesion characterization, stent optimization, and long-term prognosis, with the aim of providing high-quality evidence to support the standardized integration of IVUS into clinical practice.
Materials and Methods
Ethics Statement
This study was approved by the Ethic Committee of Liyang People's Hospital. Written informed consent was obtained from all patients and their families prior to enrollment.
Patients
The CHD patients who underwent PCI at Liyang People's Hospital between January 2022 and August 2022 were enrolled.
Inclusion Criteria
Eligible patients met the diagnostic criteria for CHD, 15 fulfilled the indications for CAG or IVUS16,17 and had at least one coronary lesion with ≥70% diameter stenosis in a single or multiple vessels requiring PCI. Patients were required to have provided informed consent and to be free from psychiatric or cognitive disorders that could impair cooperation.
Exclusion Criteria
Exclusion criteria included: contraindications to CAG or IVUS (eg, iodine allergy, uncontrolled arrhythmias, psychiatric disorders, severe hepatic or renal dysfunction; allergy to thrombolytic agents; pre-excitation syndrome, sinus block, sick sinus syndrome, severe valvular disease, or cardiomyopathy; acute or chronic infections, malignancy, peripheral vascular or thyroid disease; immune-releted diseases (eg, arteritis, systemic lupus erythematosus); bleeding disorders (eg, leukemia, disseminated intravascular coagulation); complete coronary occlusion; emergency PCI procedures; more than two PCI procedures during a single hospitalization; or prior history of myocardial infarction, PCI, or coronary artery bypass grafting.
Randomization and Blinding
All eligible participants were randomly assigned to two groups in a 1:1 ratio using a simple randomization table in Microsoft Excel, without any stratification. They were divided into a control group (undergoing CAG-guided PCI) and a study group (undergoing IVUS-guided PCI). To ensure allocation concealment and reduce selection bias, sealed, nontransparent envelopes containing the randomization codes were prepared. Each participant was allocated to a group based on the code in their envelope. This task was performed by an independent third party not involved in patient recruitment, evaluation, or data analysis.
In this study, both the outcome evaluator and data analyst remained unaware of the treatment assignments throughout the study. The evaluator input data into a Microsoft Excel spreadsheet after completing data collection, without any knowledge of which participants belonged to which treatment groups. All recorded data were encoded and stripped of any non-essential details. The blinding was only lifted after the data analysis had been finalized. However, due to the nature of the interventions, the participants and the lead researcher overseeing the treatments were not blinded.
Methods
Drug preparation and routine interventions: Three days before the operation, patients received a loading dose of aspirin enteric-coated tablets (Bayer Healthcare Co., Ltd, approval no. J20130078) 300 mg once daily, clopidogrel tablets (Shenzhen Salubris Pharmaceuticals Co., Ltd, approval no. H20000542) 300 mg once daily, and an intraoperative loading dose of heparin (calculated based on body weight, 100 μg/kg) was administered. Preoperative routine examinations included an iodine allergy test and penicillin skin test. Patients fasted and abstained from alcohol prior to surgery, and bilateral inguinal skin preparation was performed.
Operation interventions: (1) Control Group (CAG-guided PCI): Patients underwent PCI under the guidance of CAG. Equipment included a Philips 128-row 256-slice Brilliance iCT system and a Philips FD20 large flat-panel digital subtraction angiography system. Iopromide (Ultravist 300, 100 mL: 30 gI) was used as the contrast agent. Patients were placed in the supine position, intravenous access was established, and local anesthesia administered. Before imaging, 200 μg nitroglycerin (Shanxi Kangbao Biological Product Co., Ltd, approval no. H14022197) was injected into the coronary artery to prevent spasm. CAG was performed via the femoral artery using the Judkins technique. For each lesion, at least two orthogonal projections were obtained, and the degree of stenosis was quantified from the view with the most severe narrowing. Vessel and plaque characteristics were analyzed using the angiographic system's quantitative analysis function. A guiding catheter was introduced into the coronary ostium, and a PTCA guidewire was advanced across the stenosis to its distal end. Pre-dilatation was performed with an appropriate balloon, followed by stent implantation selected according to vessel diameter. After stent placement, 0.4 mL of low molecular weight heparin calcium was administered subcutaneously. Angiographic images were recorded post-procedure.
(2) Study group (IVUS-guided PCI): Patients underwent PCI guided by IVUS. Instruments included the Boston Coronary IVUS system (model H749iLab220CART0) and the Atlantis SR Pro Coronary Ultrasound Imaging Catheter (model H749389420). Following CAG, IVUS was performed in the target lesion vessels. The ultrasound catheter was advanced distally across the stenosis and retracted automatically at 1 mm/s to the proximal lesion edge. IVUS imaging was used to quantitatively assess vessel dimensions and plaque morphology. A pressure guidewire was then introduced via a 6F guiding catheter to the coronary ostium, calibrated, and advanced distally across the stenosis. Adenosine triphosphate was infused intravenously to induce maximal hyperemia. Stents were selected based on a diameter-to-vessel ratio of 1.0–1.1, deployed to fully cover the lesion, and checked for proximal and distal edge apposition. Post-dilatation was performed as required. After stent implantation, repeat IVUS was used to evaluate stent expansion and apposition. If malapposition was observed, high-pressure balloon dilation was repeated. All procedures were performed by the same experienced interventional team.
Both groups were given dual antiplatelet therapy (aspirin 100 mg + clopidogrel 75 mg) the day after the operation, which was maintained until one year postoperatively. Regular follow-up visits were conducted for electrocardiogram and echocardiogram examinations. Medication adherence was assessed through pill counts.
Measures
Lesion vessel characteristics: The minimal lumen diameter (MLD), diameter stenosis (DS), and plaque burden (PB) were measured in both groups before and after stent implantation. DS = (reference vessel diameter − MLD)/reference vessel diameter × 100%. PB = plaque area/extravascular elastic membrane area × 100%.
Stent placement parameters: The number of stents, maximum stent diameter, stent length, number of post-dilatations, maximum balloon diameter, maximum balloon pressure, and stent placement success rate were recorded. Criteria for determining stent placement success: residual stenosis of the infarction-related coronary artery lumen ≤20%; minimum to maximum stent lumen diameter ratio >0.7; and no gaps between stent struts and the vessel wall.
Time indicators: Operation duration and length of hospital stay were recorded for both groups.
Complications: The incidence of early postoperative complications was recorded, including vasospasm, pseudoaneurysm, local hematoma, etc.
Stent restenosis rate and major adverse cardiovascular events (MACE): Follow-up was conducted via outpatient visits or telephone calls to record the stent restenosis rate during the follow-up period and MACE one year postoperatively, including cardiac death, myocardial infarction, and target vessel revascularization.
Sample Size Estimation
Based on the results of a preliminary experiment, the MACE incidence rate was approximately 3% for patients undergoing PCI under CAG guidance and approximately 23% for those under IVUS guidance. Using PASS2021 software, with a power (1-β) of 80% and a significance level (α) of 0.05, a sample size of 41 cases per group was calculated. Considering a 20% sample attrition rate, at least 50 cases per group were required.
Statistical Analysis
Data were processed by SPSS 28.0 software. The Kolmogorov-Smirnov test was used to assess the normality of continuous variables. Continuous variables conformed to normal distribution were described by mean ± standard deviation (SD), the independent samples t-test was used to detect intergroup differences, and the paired samples t-test was used to detect intragroup differences. Non-normally distributed variables were expressed as median (quartile range) (Q1, Q3) and analyzed using Mann-Whitney U test. Categorical variables were presented as counts and percentages [n (%)] and analyzed by the Chi-square test or continuity-corrected chi-square test (when the theoretical frequency in a cell is 1 ≤ T < 5) or Fisher's exact test (when the expected frequency T < 1). A two-sided P-value <.05 was considered statistically significant.
Results
Baseline Data
Patients were assigned to the control group (n = 50) and the study group (n = 50). Baseline characteristics (age, body mass index, heart rate, left ventricular ejection fraction, gender, number of diseased vessels, underlying diseases, smoking history, and drinking history) were collected and analyzed. No differences in baseline data were observed between the two groups (P > .05), indicating comparability (Table 1).
Baseline Data Between the Two Groups.
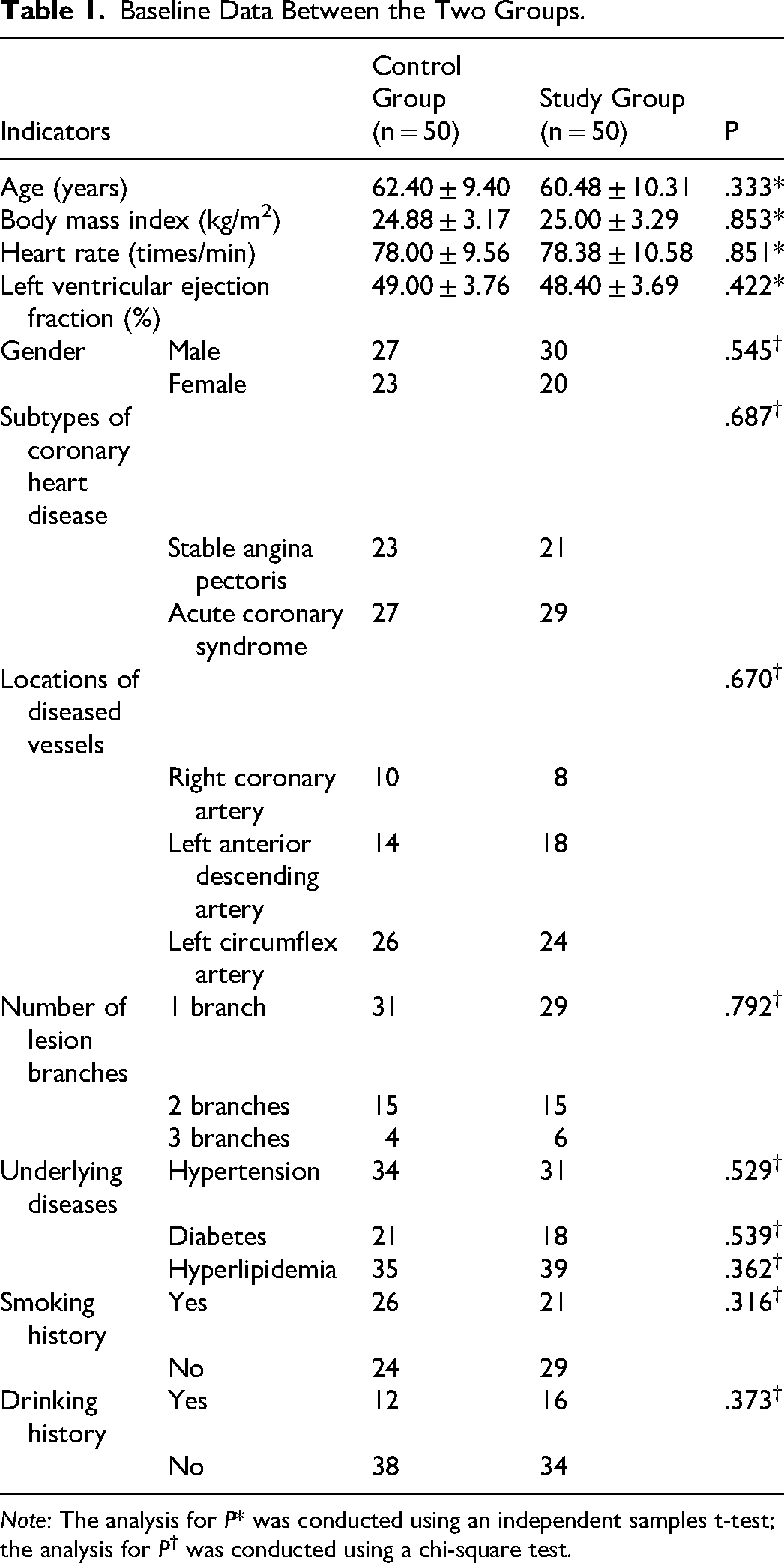
Note: The analysis for P* was conducted using an independent samples t-test; the analysis for P† was conducted using a chi-square test.
Lesion Vessel Characteristics
Prior to stent implantation, the differences in MLD, DS, or PB between the two groups were not significant (P > .05). After stent implantation, MLD increased and both DS and PB decreased in both groups, with the study group exhibiting wider MLD and lower DS and PB than the control group (P < .05); meanwhile, the ΔMLD in the study group was greater than that in the control group, while the ΔDS and ΔPB were smaller than those in the control group (P < .05) (Table 2).
Lesion Vessel Characteristics of s Between the Two Groups.
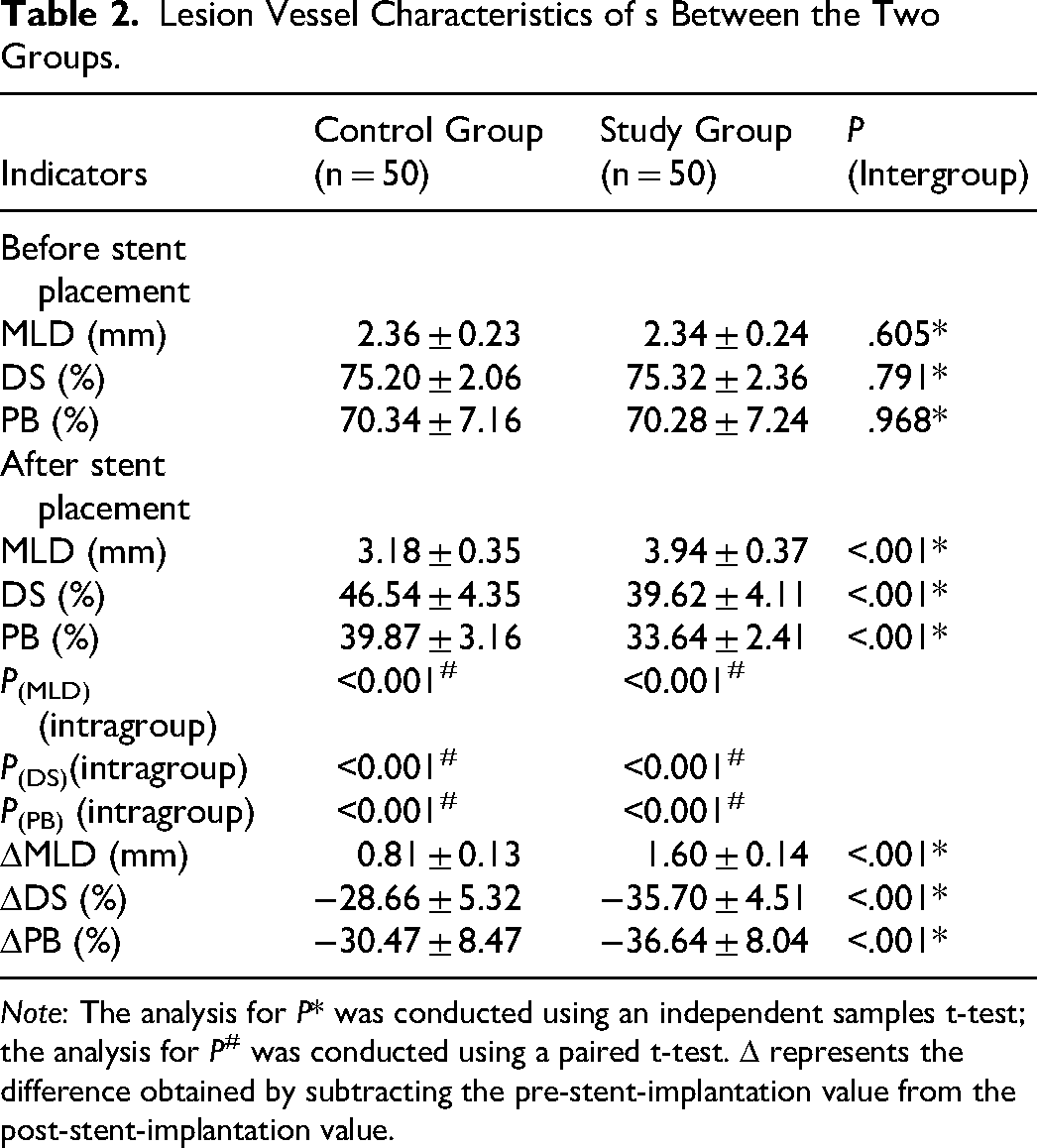
Note: The analysis for P* was conducted using an independent samples t-test; the analysis for P# was conducted using a paired t-test. Δ represents the difference obtained by subtracting the pre-stent-implantation value from the post-stent-implantation value.
Stent Placement Parameters
There were no significant differences between the two groups in the number of stents implanted, stent length, or number of post-dilatations (P > .05). However, the study group achieved a larger maximum stent diameter, maximum balloon diameter for post-dilation, maximum balloon pressure, immediate postoperative minimum stent diameter, and minimum stent cross-sectional area in contrast with the control group (P < .05). Meanwhile, the stent placement success rate in the study group was higher than that in the control group (Table 3).
Stent Placement Parameters Between the Two Groups.
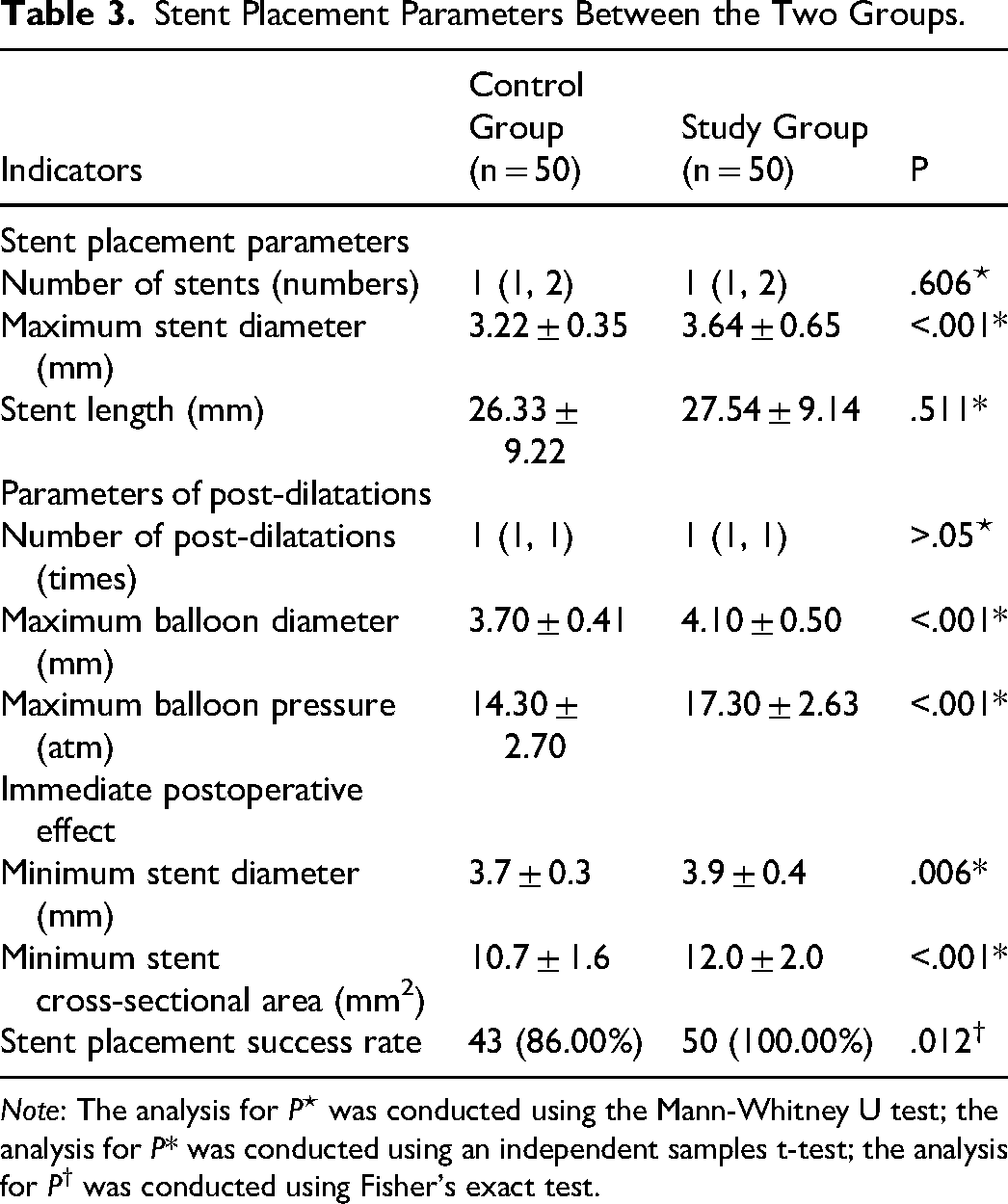
Note: The analysis for P⋆ was conducted using the Mann-Whitney U test; the analysis for P* was conducted using an independent samples t-test; the analysis for P† was conducted using Fisher's exact test.
Time Indicators
No significant differences were observed between groups in operation time or length of hospital stay (P > .05) (Table 4).
Time Indicators Between the Two Groups.
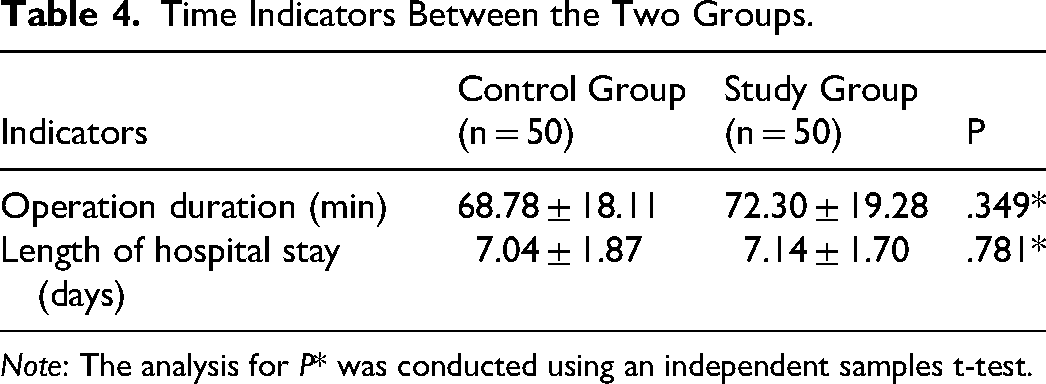
Note: The analysis for P* was conducted using an independent samples t-test.
Complications During Follow-up
No statistically significant difference in the incidence of complications (vasospasm, pseudoaneurysm, local hematoma) was observed between the study and control groups (P > .05) (Table 5).
Complications Between the Two Groups During the Follow-Up.
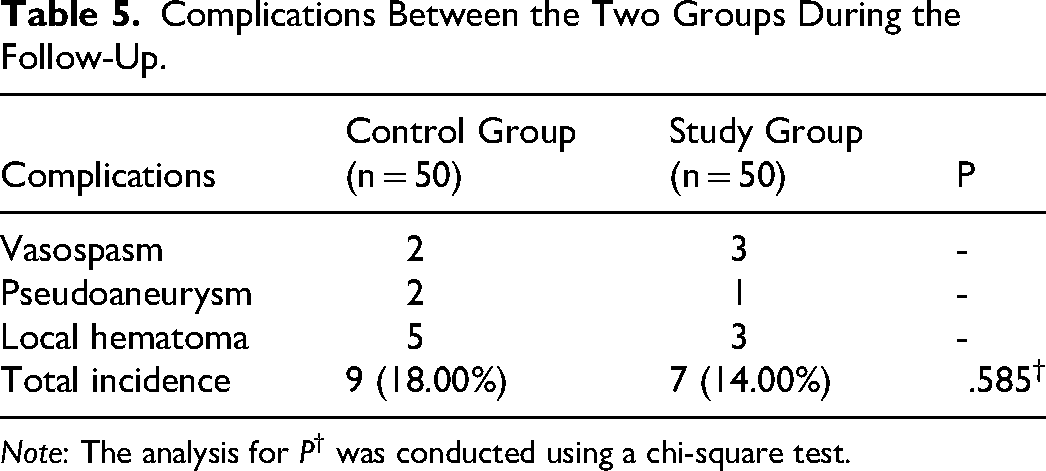
Note: The analysis for P† was conducted using a chi-square test.
MACE and Coronary Restenosis
Within one-year follow-up, the incidences of MACE were lower in the study group compared with in the control group (P < .05). The stent restenosis rate in the study group was lower than that in the control group, but the difference was not statistically significant (P > .05) (Table 6).
MACE and Coronary Artery Restenosis Between the Two Groups During Follow-Up.
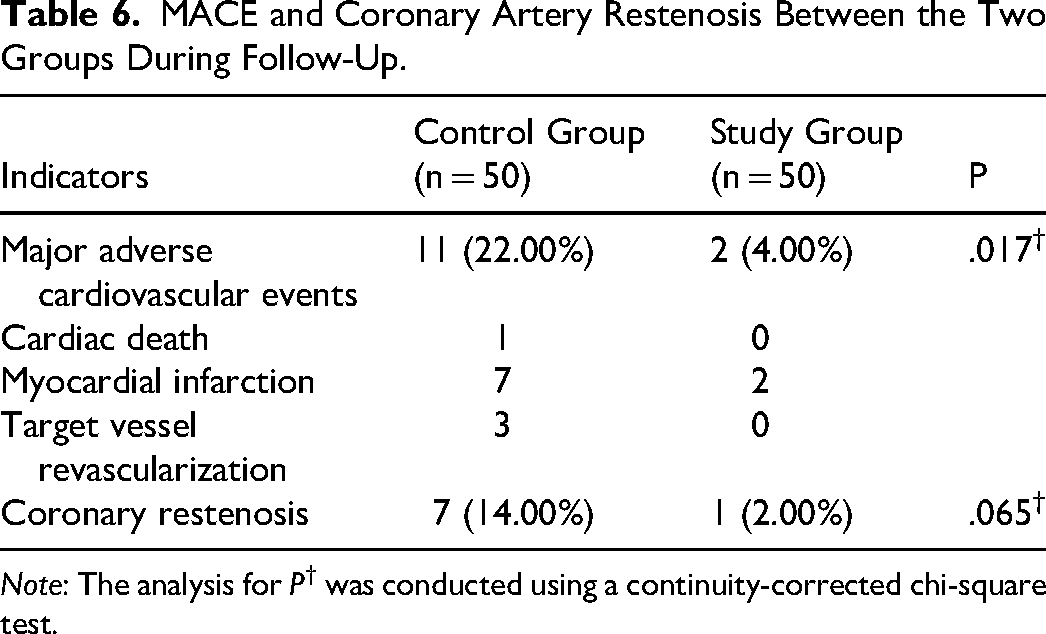
Note: The analysis for P† was conducted using a continuity-corrected chi-square test.
Discussion
CHD is a condition with high global morbidity and mortality, characterized by chronic immunoinflammatory and fibroproliferative processes driven by lipid accumulation. 18 Therefore, evaluating the clinical efficacy of IVUS-guided PCI in CHD is of significant clinical relevance. In this study, we compared the outcomes of CAG-guided and IVUS-guided PCI, with particular emphasis on the clinical value of IVUS in lesion assessment, stent optimization, and long-term prognosis.
Lee et al reported that IVUS-guided PCI improves post-procedural and long-term outcomes in patients with both complex and non-complex lesions. 19 The clinical advantages of IVUS-guided PCI can be attributed to three key aspects: (1) providing a better understanding of the revascularization mechanism; (2) allowing early anticipation and management of potential complications; and (3) optimizing PCI outcomes through real-time guidance and feedback. 20 This study found that while both groups improved after stent implantation, the study group had significantly greater changes from baseline (ΔMLD, ΔDS, ΔPB) than the control group, indicating that the intervention provided additional benefit beyond the stent effect alone. Additionally, the study group achieved larger maximum stent diameter, maximum balloon diameter after dilation, maximum balloon pressure, immediate postoperative minimum stent diameter, and minimum stent cross-sectional area. The optimization of these immediate parameters highlights the advantages of IVUS-guided PCI. Gao et al similarly reported that IVUS-guided PCI was associated with larger MLD and smaller residual stenosis at follow-up compared with angiography-guided PCI. 21 Lee et al confirmed that the stent-to-reference vessel diameter ratio is higher in IVUS-guided PCI than in CAG-guided PCI, and the utilization rate of high-pressure post-dilation is also higher. 22 Regarding the identification of angiographically invisible issues such as stent malapposition and stent edge dissection, a case study reported by Zhang et al demonstrated that IVUS can accurately identify characteristics of tissue prolapse (thickness: 0.9 mm, area: approximately 2.01 mm2), which appears as a vague shadow on angiography, suggesting the irreplaceable value of IVUS in identifying complications in angiographic blind spots. 23 Furthermore, in a study by Jia et al focusing on stenotic lesions near the proximal end of myocardial bridges, IVUS guidance is found to enable shorter stent lengths, lower diameter stenosis rates, and more precise stent positioning. 24 This study further confirmed that IVUS offers particularly prominent positioning advantages in lesions with complex anatomical structures.
Moreover, this study showed that the stent implantation success rate was higher in the study group than in the control group. This result aligns with the core value of image-guided PCI—by providing real-time information on the vessel wall, IVUS assists operators in immediately identifying and correcting issues such as stent underexpansion, malapposition, and edge dissection during the procedure.25,26 This study also confirmed that there were no significant differences in operative time and hospital stay between the two groups. This finding holds significant clinical practical implications: IVUS guidance does not compromise surgical quality at the expense of prolonged operative time, suggesting its feasibility and efficiency in routine clinical practice.
Simultaneously, no statistically significant differences were observed in the incidence of complications such as vasospasm, pseudoaneurysm, and local hematoma between the two groups, further confirming the safety of IVUS guidance. It has been reported that IVUS guidance and CAG guidance show no significant differences in safety endpoints, but IVUS reduces the risk of long-term events such as cardiac death, stent thrombosis, and target vessel revascularization. 27 The results of this study echo this evidence: during the one-year follow-up, the incidence of MACE was lower in the study group than in the control group, and the stent restenosis rate was also lower in the study group, although the difference was not statistically significant. This result supports the value of IVUS guidance in improving long-term clinical outcomes. Data from a study by Jin et al showed that CAG guidance is associated with a higher risk of target lesion failure and stent thrombosis compared to IVUS. 28 Additionally, it has been reported that IVUS-guided PCI is associated with lower risks of all-cause mortality, MACE, and target vessel revascularization29,30; intravascular lithotripsy performed under IVUS guidance for severely calcified lesions achieved high procedural success, no peri-procedural complications, and a low one-year MACE rate. 31
In summary, compared to CAG guidance alone, IVUS-guided PCI offers advantages in optimizing surgical parameters, improving stent implantation success rates, and reducing long-term MACE without increasing operative time, hospital stay, or complication risks. The results of this study to some extent support the application of IVUS-guided PCI in clinical practice, particularly in patients with complex lesions.
Nevertheless, this study has several limitations. It was a single-center study with a relatively small sample size and short follow-up, which may affect the generalizability and robustness of the findings. Future studies should involve multicenter, large-scale randomized controlled trials with extended follow-up and a wider range of lesion types to better define the clinical benefits of IVUS-guided PCI. Furthermore, the integration of other intravascular imaging and physiological techniques, such as optical coherence tomography and fractional flow reserve, may support the development of more individualized and precise interventional strategies.
Footnotes
Funding
This work was supported by the Science and Technology Project of Changzhou Health Commission (WZ202028) and the Clinical Medical Science and Technology Development Fund of Jiangsu University (JLY 2021143).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.