
Abstract
Background
Acute liver failure (ALF) is a life-threatening syndrome characterized by abrupt hepatic dysfunction accompanied by systemic inflammatory response and immune dysregulation, resulting in a high susceptibility to infectious complications. In the intensive care unit (ICU) setting, bacterial sepsis and invasive fungal infections represent critical determinants of multiorgan failure, liver transplant eligibility, and patient survival.
Main body
This narrative review synthesizes current evidence on infectious risk, diagnostic challenges, and antimicrobial management in ALF. The immune response to massive hepatocellular necrosis is initially driven by damage-associated and pathogen-associated molecular patterns, resulting in a sepsis-like hyperinflammatory state. This phase is followed by profound immunoparesis, characterized by impaired innate and adaptive immune responses, which facilitates fbacterial translocation, increases susceptibility to nosocomial infections, and promotes colonization and infection with multidrug-resistant (MDR) pathogens. Infections occur in most ALF patients, yet differentiation between sterile systemic inflammatory response and sepsis remains challenging as fever, leukocytosis, and hemodynamic instability are nonspecific and microbiological cultures frequently yield negative results. Conventional biomarkers primarily reflect hepatocellular injury rather than bacterial infection. Antimicrobial therapy should be individualized based on clinical severity, local epidemiology, and MDR colonization, while accounting for profound pharmacokinetic alterations associated with hepatic failure. In liver transplant candidates and recipients, short-course perioperative prophylaxis and judicious interpretation of MDR screening are pivotal to prevent early postoperative infections without promoting antimicrobial resistance.
Conclusions
Optimizing infection diagnosis, biomarker-guided decision-making, and individualized antimicrobial dosing in ALF, particularly in the peri-transplant ICU setting, is critical for improving patient outcomes and limiting the emergence of MDR pathogens.
Introduction
Acute liver failure (ALF) is a rare but life-threatening syndrome characterized by the rapid onset of severe hepatic dysfunction in patients without preexisting liver disease. It includes profound systemic derangements with circulatory instability, metabolic disturbances, and multiorgan failure, requiring advanced supportive care in the intensive care unit (ICU). The immune response in ALF is highly dynamic and dysregulated with biphasic immune dysfunction, from an initial hyperinflammatory phase followed by a state of functional immunoparesis that increase susceptibility to bacterial and fungal infections. At the same time, the clinical overlap between systemic inflammatory response and true infection, combined with the limited reliability of conventional microbiological and biomarker-based diagnostics, makes early and accurate identification of infection particularly challenging.
This review specifically addresses infections in ALF with a particular focus on immune dysregulation and the antimicrobial management of infectious complications in the critical care setting of patients with ALF and in the perioperative care of LT recipients.
Definitions of Acute Liver Failure
ALF is a rapidly progressive syndrome characterized by the abrupt loss of hepatic synthetic, metabolic, and detoxification functions, leading to profound systemic homeostatic derangements, multi-organ dysfunction, and high mortality rates.1,2
Based on the presence or absence of underlying chronic liver disease, two main clinical entities can be distinguished: ALF, which develops in patients without pre-existing liver disease, and acute-on-chronic liver failure (ACLF), which occurs in the setting of chronic liver disease, most commonly cirrhosis. Although ALF and ACLF differ in underlying hepatic substrate, precipitating factors, and diagnostic criteria, both are characterized by profound systemic inflammation, a high rate of organ dysfunction and infectious complications.1–5
ALF is defined by the rapid onset, following an acute hepatic insult, of liver injury associated with coagulopathy (typically an international normalized ratio ≥1.5) and hepatic encephalopathy of any grade in a patient without evidence of chronic liver disease.1,2,6–8 Historically, the interval between the onset of jaundice and the development of encephalopathy has been used to classify ALF into hyperacute (<7 days), acute (7-21 days), and subacute (>21 days and <26 weeks) forms. Although this classification currently has a predominantly descriptive rather than decision-making role, it retains prognostic relevance. Hyperacute forms, most associated with ischemic injury or acetaminophen toxicity, are characterized by a higher risk of neurological complications such as cerebral edema but a greater likelihood of transplant-free survival. In contrast, acute and subacute forms, often related to non-A viral hepatitis, non-acetaminophen drug-induced liver injury, or autoimmune disease, are associated with more pronounced jaundice, lower aminotransferase levels, and poorer outcomes in the absence of liver transplantation (LT).1,6–8
From an etiological perspective, ALF represents the final common pathway of multiple hepatic insults, the identification of which is essential to guide causal therapy, prognostication, and LT selection. The relative prevalence of specific etiologies varies according to geographic region, immunization coverage, and patient age. Major etiological categories include toxic and drug-induced causes (acetaminophen, prescription drugs, herbal and dietary supplements, mushroom toxins), hepatotropic and non-hepatotropic viral infections (HAV, HEV, HBV with or without HDV, HSV, VZV, EBV, adenovirus), autoimmune disorders, metabolic diseases (such as Wilson disease), pregnancy-related conditions (acute fatty liver of pregnancy, HELLP syndrome), ischemic injury, malignant infiltration, and indeterminate causes.1,2,6–8
Pathophysiology of Immune Dysfunction in ALF
The immune response in ALF exhibits a biphasic trajectory, beginning with hyperinflammatory phase that gradually progresses toward functional immunoparesis. This transition reflects a dynamic continuum rather than a discrete shift, with simultaneous features of immune hyperactivation and immunosuppression often coexisting.3–5,9–11
The main danger signals involved in this process are pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs). PAMPs, including lipopolysaccharide, peptidoglycan, and microbial nucleic acids, arise primarily from bacterial translocation along the gut–liver axis and activate innate immune responses in resident hepatic cells, such as Kupffer cells, as well as in circulating immune cells, including monocytes and neutrophils. DAMPs are released from necrotic or metabolically stressed hepatocytes and are particularly relevant in ALF.3–5,9–11
PAMPs and DAMPs interact with specific pattern-recognition receptors (PRRs), including toll-like receptors and nod-like receptors, thereby activating intracellular signaling pathways such as NF-κB and mitogen-activated protein kinases. This leads to the initiation of a systemic inflammatory response characterized by the production of pro-inflammatory cytokines and chemokines (TNF-α, IL-1β, IL-6, IL-8, CXCL10), leukocyte recruitment, and amplification of endothelial and microvascular injury.3–5,9,10,12–14
In the early phases of ALF, massive hepatocellular necrosis represents the primary source of DAMPs, resulting in a systemic inflammatory response of sufficient magnitude to induce distributive shock. This response mirrors the hemodynamic profile observed in sepsis, characterized by hyperdynamic circulation and reduced systemic vascular resistance. The hyperinflammatory phase is commonly succeeded by functional immunoparesis, defined by a reduced capacity of the immune system to recognize, and eliminate pathogens and cellular debris, thereby increasing susceptibility to infections.3–5,9,10,12–14
A hallmark of immunoparesis in acute liver failure (ALF) is the functional impairment of Kupffer cells, which under physiological conditions mediate the clearance of apoptotic cells, immune complexes, and microorganisms from the portal circulation. This hypofunction compromises antimicrobial defenses. Concurrently, specific hepatic macrophage subsets expressing the MerTK receptor facilitate resolution of inflammation and apoptotic cell clearance, promoting the transition toward a reparative phase of liver injury..3,4,9–11,14,15
ALF can be conceptualized as a complex systemic syndrome in which the liver is the primary site of injury but not the sole determinant of clinical outcome. The immune response, initially hyperactivated and subsequently impaired plays a pivotal role in the development of multi- organ failures, increased susceptibility to infection, and overall prognosis. A detailed understanding of the underlying immunological mechanisms, including PRR activation, the role of innate hepatic immune cells, and the transition toward immunoparesis, is therefore critical for elucidating disease pathophysiology and identifying potential therapeutic targets and prognostic biomarkers.1–5,7–11,13–15
Epidemiology of Infections in ALF
Infections complicate the clinical course in over 75% of patients with ALF, with reported rates of bacteremia ranging from 22% to 80%; however only about one-third of patients show positive microbiological cultures.6–8,16 A high index of clinical suspicion is therefore essential in ALF patients who exhibit clinical deterioration, as systemic inflammatory response syndrome (SIRS) and sepsis exhibit overlapping pathophysiological mechanisms, complicating the differentiation between sterile inflammation and true infection.13,14,17,18
In a U.S.-based study the most common sites of positive cultures were urine and blood, followed by tracheal aspirates, intravascular catheters, ascitic fluid, and wound sites. When rigorous microbiological surveillance is employed, clinical or bacteriological evidence of infection can be identified in up to 90% of ALF patients. Gram-positive bacteria (eg Staphylococcus aureus, Staphylococcus epidermidis, Enterococcus spp.) are the most frequently isolated pathogens, followed by Gram-negative organisms (eg Escherichia coli, Pseudomonas spp., Enterobacter spp., Haemophilus spp., Citrobacter spp., Klebsiella spp., Neisseria spp.) and fungi. In patients who progress to grade III–IV hepatic encephalopathy, Gram-negative organisms become more predominant.6–8,16 High rates of bacterial infection, with enteric Gram-negative organisms predominating, suggest clinically relevant bacterial translocation from the gut as a major source of pathogens. However, because direct culture of mesenteric lymph nodes or portal blood is not feasible in humans, the quantitative contribution of translocation to the overall infection burden in ALF remains incompletely defined.
Antimicrobial Agents and Hepatic Impairment.
Risk factors for infection and colonization by MDR organisms include prolonged ICU stay, the presence of invasive devices, mechanical ventilation, and renal replacement therapy.19–24 Overall, approximately two-thirds of infections in ALF patients are bacterial, while the remaining one-third are of fungal origin.6–8,16
In critically ill patients, distinguishing between community-acquired infections (CAIs) and hospital-acquired infections (HAIs) is essential for evaluating the risk of MDR pathogens and for guiding appropriate antimicrobial therapy. CAIs typically involve respiratory, intra-abdominal, or urinary tract infections, whereas HAIs are associated with medical interventions, such as surgical site infections, catheter-related bloodstream infections, and ventilator-associated pneumonia.19–24 The profound immune dysfunction observed in ALF patients further complicates identification of the source of infection, determination of the causative organism, and optimization of the timing and choice of antimicrobial therapy.3–5,9,10,13,14
Diagnosis of Infections in ALF
In ALF patients, differentiating SIRS from sepsis is challenging for several reasons.13,14,17,18 Conventional blood culture methods, although considered the gold standard for diagnosing infection, are time-consuming and have limited sensitivity for many unusual or fastidious pathogens. Rapid diagnostic tools for pathogen detection may support the earlier initiation of targeted therapy; however, their clinical utility in ALF remains insufficiently studied. Conversely, negative results from rapid tests may support a decision to withhold or delay antibiotic treatment in carefully selected cases. The MULTI-CAP study, for example, demonstrated more rapid de-escalation and reduced use of broad-spectrum antimicrobials in patients with hospital-acquired pneumonia when syndromic diagnostic tests were used. In the context of rapid microbiological diagnostics in clinical practice, it is nevertheless crucial to be fully aware of the technical and interpretative limitations of each assay to avoid misclassification of infection status. Multiplex PCR panels and cartridge-based systems are inherently restricted to a predefined list of targets; pathogens that are not represented on the panel, or that show significant genetic variability, may yield false-negative results despite being clinically relevant.
Moreover, distinguishing between colonization and true infection can be difficult when microbiological samples are positive. The utility of infections biomarkers becomes pivotal in ALF patients with suspected sepsis.
C-reactive protein (CRP) is an acute-phase protein synthesized by the liver following inflammatory stimuli. As ALF is characterized by massive hepatocellular necrosis, CRP production is impaired, and CRP levels are commonly low in ALF patients. Silvestre et al demonstrated decreased CRP levels in ALF patients with sepsis. 25
Procalcitonin (PCT), the precursor of calcitonin, is produced primarily by thyroid C cells in healthy individuals. In response to systemic infection, PCT levels begin to rise within 2–3 h and typically peak at around 24 h. PCT elevations are most pronounced in Gram-negative sepsis, whereas levels are only modestly increased in patients with fungal infections. In patients with sepsis, pneumonia, and other infectious conditions, PCT has been validated as a useful biomarker to distinguish sepsis from non-infectious inflammatory states. 17 PCT cut-offs measured on subsequent days after ICU admission are also helpful in shortening the duration of antibiotic therapy in clinically improving patients. In ALF patients, with or without concomitant bacterial infection, severe hepatocyte necrosis and associated inflammation result in elevated PCT levels, rendering this biomarker unreliable in this specific setting. In a retrospective study, Rule et al observed PCT values above the usual diagnostic cut-offs in ALF patients, roughly proportional to the degree of hepatic necrosis. 26
Presepsin is a soluble cleavage fragment of CD14, a glycoprotein expressed on monocytes, macrophages, and polymorphonuclear neutrophils. Lee et al found that presepsin levels were significantly higher in patients with sepsis than in those with non-infectious organ failure, and significantly higher in patients with septic shock than in those with sepsis without shock. 27 Following infection by Gram-negative or Gram-positive bacteria and fungal pathogens, presepsin levels rise as early as 2 h, with peak concentrations reached at approximately 3 h. Chen et al demonstrated that presepsin performs better than CRP and PCT for diagnosing infection in patients with liver failure. 28
Soluble mannose receptor (sMR/CD206) has also been proposed as a biomarker of hepatic macrophage activation and liver injury, although its role in ALF remains to be fully clarified. 29
(1→3)-β-D-glucan (BDG) is a broad-spectrum fungal biomarker, representing a structural polysaccharide component of the cell wall of most pathogenic fungi, including Candida, Aspergillus, Fusarium, Trichosporon, Saccharomyces, Acremonium, and Pneumocystis jirovecii, and is released into the circulation during invasive disease. BDG assays demonstrate high sensitivity (74-86%) but only moderate specificity (49-71%), while maintaining a strong negative predictive value, making them particularly valuable for ruling out invasive fungal infections. These diagnostic features support the use of BDG within antifungal stewardship strategies, especially to guide early discontinuation of empirical antifungal therapy in critically ill patients even if integrating BDG with clinical context may enhance diagnostic accuracy. Notably, evidence from a single-center study by Verma et al indicates that the diagnostic performance of BDG in patients with ALF is comparable to that observed in the general ICU population, supporting its potential applicability even in this highly complex clinical context.
Galactomannan (GM), detected in both serum and bronchoalveolar lavage (BAL) fluid, is a well-established biomarker for invasive aspergillosis, particularly in neutropenic hematologic populations.30–32 However, its diagnostic performance is considerably less robust in non-neutropenic patients. Emerging evidence suggests that GM testing in BAL fluid may offer superior diagnostic yield compared with serum in critically ill patients, although results remain heterogeneous and are influenced by sampling techniques and assay cutoffs. As a result, the overall diagnostic role of GM in the ICU setting remains uncertain, highlighting the need for further studies to better define its accuracy and optimal clinical application in high-risk, nonhematologic populations. In patients with ALF serum GM performs and studies focusing on liver failure and LT populations report a high rate of false-positive results, likely related to profound hepatic dysfunction, increased intestinal permeability, antibiotic exposure, and the use of blood products and extracorporeal therapies. 30 Conversely, GM detection in BAL fluid appears more informative in this setting, demonstrating improved diagnostic performance in critically ill and transplant populations. 33 Accordingly, current evidence supports a multimodal diagnostic approach in ALF and advanced liver disease, integrating GM, preferably from BAL samples, with clinical evaluation, high-resolution imaging, and complementary microbiological assays to enhance the accuracy and timeliness of invasive aspergillosis diagnosis.30–33
Biomarkers of infection in patients with ALF have major diagnostic limitations. CRP is often falsely low, whereas procalcitonin (PCT) is frequently elevated in proportion to hepatocellular necrosis even without infection. Emerging markers such as presepsin and soluble mannose receptor (sMR/CD206) are promising but require validation in larger ALF cohorts before routine use. Fungal biomarkers (β-D-glucan, galactomannan) are prone to false positives and negatives, particularly in ALF and the peri-transplant setting, and should only be interpreted within a multimodal framework. Consequently, antimicrobial decisions in ALF should not rely on any single biomarker result.
Treatment of Infections in ALF
Sepsis in ALF patients remains a leading cause of infection-related mortality, particularly when not promptly recognized and treated, and timely diagnosis and intervention are therefore critical.16,17 The 2021 Surviving Sepsis Campaign guidelines recommend immediate administration of antimicrobial therapy, ideally within one hour of recognition, for adult patients with suspected septic shock. In cases of suspected sepsis without shock, a rapid assessment to distinguish between infectious and non-infectious etiologies is advised, with appropriate antimicrobial therapy to be initiated within three hours of clinical recognition. 17 Although there is broad consensus that antimicrobial therapy should be initiated as early as possible, definitive evidence on the optimal timing is lacking.17,18 In ALF, diagnostic challenges are amplified by overlapping clinical features with sepsis.6–8,16 The prolonged disease course and the development of a compensatory anti-inflammatory response syndrome (CARS), a state of relative immunosuppression, may contribute to the elevated risk of bloodstream infection (BSI) in this population.3–5,9,10,13,14
Infections in ALF patients are frequently associated with worsening hepatic encephalopathy, additional organ failures, and progression to septic shock. Vaquero et al demonstrated a correlation between culture-positive infections and progression to advanced stages of hepatic coma, while Schmidt et al reported higher infection rates in patients with more advanced grades of hepatic encephalopathy and clinical manifestations of SIRS.6–8,16 The imperative for early antibiotic administration, driven by the intrinsic susceptibility to infection and the high mortality associated with ALF (with BSI linked to increased 21-day mortality), must be carefully balanced against the risks of antibiotic overuse and the emergence of antimicrobial resistance.19–21
Empirical treatment of infections in ALF should be individualized based on local epidemiology, known MDR colonization, and the severity of illness.19–24 In patients with CAIs, third-generation cephalosporins are generally recommended, whereas piperacillin–tazobactam should be preferred in cases where HAIs are suspected.6–8,16,19–21 In ALF with septic shock, carbapenems should be empirically considered, particularly where the local prevalence of extended-spectrum β-lactamase (ESBL)-producing organisms is high.19–22 Infections caused by MDR pathogens, including difficult-to-treat organisms encompassed by the acronym “ESKAPE” (Enterococcus faecium, Staphylococcus aureus, Acinetobacter baumannii, Klebsiella pneumoniae, Enterobacter spp., and Pseudomonas aeruginosa), are associated with high mortality rates, especially in septic shock.22,34,35 To achieve appropriate empirical antimicrobial coverage of likely pathogens, individual risk factors for MDR infection should be considered, including prolonged hospitalization, prior hospital admissions, the presence of invasive medical devices, and previous colonization or infection with MDR organisms.19–24 In critically ill patients, active surveillance for carriage of multidrug-resistant organisms (MDROs) is generally considered a key component of infection prevention and control. MDRO carrier status strongly influences antibiotic selection, particularly in ALF patients awaiting liver transplantation or in the early post-transplant period with severe, life-threatening infections.19–24 The most controversial clinical scenarios include patients with severe infections but negative MDRO screening, and patients with uncomplicated infections but positive MDRO screening.
Optimal management of infectious diseases relies on early identification of the infection source, accurate syndromic assessment, and, whenever feasible, microbiological documentation of the causative agent, integrated with the use of validated biomarkers of infection and treatment response. These elements rationally guide both the initiation of broad-spectrum empiric therapy and subsequent de-escalation to the narrowest effective targeted regimen, enabling optimization of treatment duration and selection of agents with an appropriate spectrum, PK/PD profile, and hepatic safety, while limiting toxicity, strengthening antimicrobial stewardship, and curbing the further spread of MDR organisms.
The role of antimicrobial prophylaxis in ALF remains controversial. Previous studies have demonstrated that prophylactic antimicrobials reduce the incidence of infections in ALF patients but do not improve survival. 10 Accordingly, the most recent guidelines from the American Association for the Study of Liver Diseases (AASLD) do not recommend routine antimicrobial prophylaxis in ALF.2,11
Liver–Antibiotic Interactions: A Pharmacological Perspective
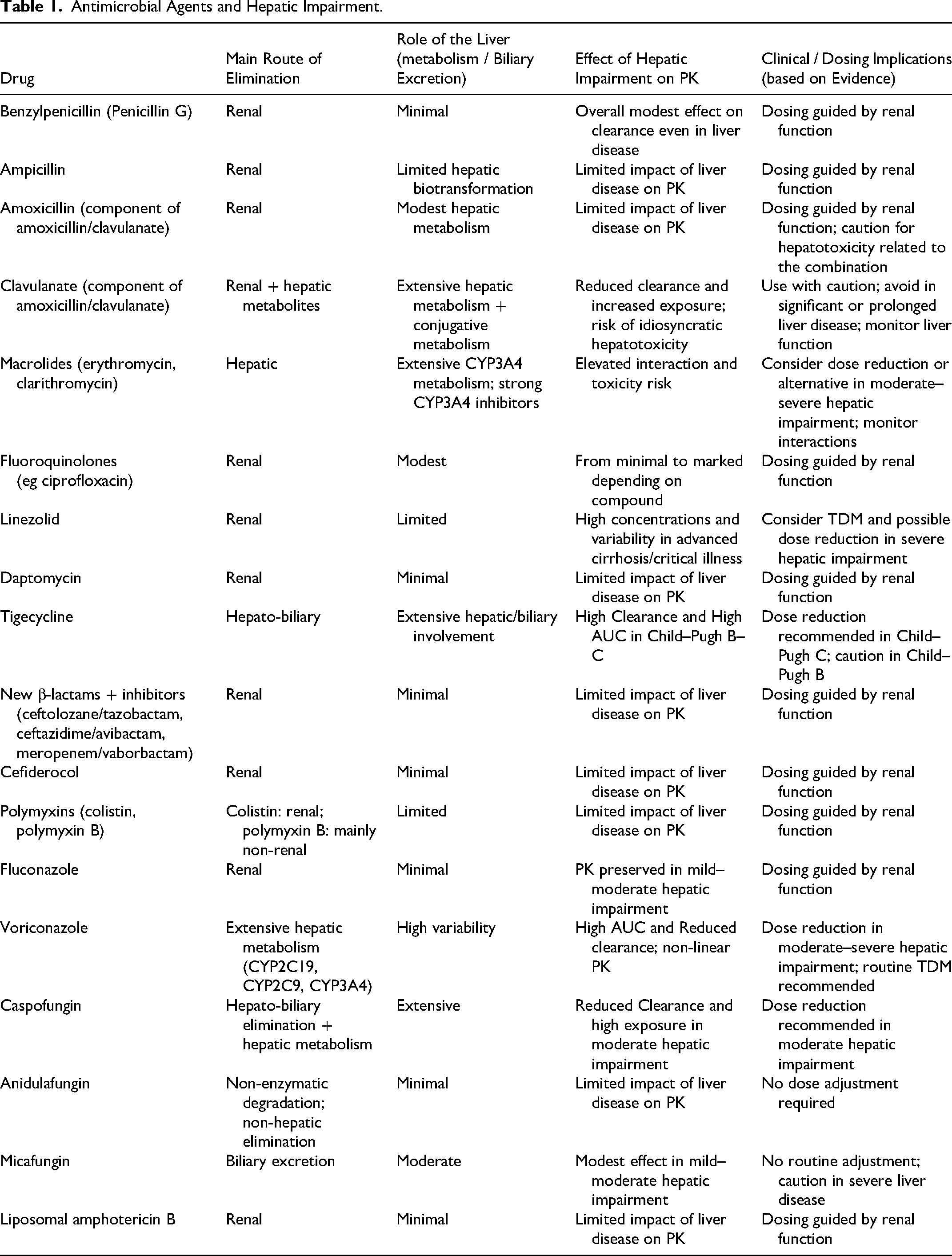
Antimicrobial therapy in patients with hepatic impairment is primarily determined by the extent of hepatic metabolism and biliary excretion of individual agents. The liver plays a central role in phase I and II biotransformation and in the synthesis of drug-binding proteins, thereby influencing systemic exposure and pharmacokinetic–pharmacodynamic (PK/PD) relationships. In acute liver failure, reduced functional hepatocyte mass, altered hepatic blood flow, intrahepatic shunting, and cholestasis can significantly modify the pharmacokinetics of drugs undergoing substantial hepatic metabolism (Table 1).36,37
Among β-lactam antibiotics, benzylpenicillin and ampicillin are mainly renally eliminated and are minimally affected by hepatic dysfunction, whereas clavulanate undergoes more extensive hepatic oxidative and conjugative metabolism.38,39 Macrolides are highly dependent on CYP3A4-mediated hepatic metabolism, with significant first-pass effects, potential drug–drug interactions, and additional anti-inflammatory and immunomodulatory properties that may be relevant in critically ill patients. 40 Fluoroquinolones exhibit heterogeneous pharmacokinetics, with the impact of hepatic impairment ranging from negligible to clinically significant depending on the compound.23,38
Linezolid, although primarily eliminated via non-CYP pathways, may show increased and more variable plasma concentrations in severe hepatic dysfunction, supporting the use of therapeutic drug monitoring (TDM).41–43 Daptomycin and newer β-lactam/β-lactamase inhibitor combinations are largely renally cleared and generally do not require dose adjustment based on liver function,44–47 like polymyxins, for which renal function remains the main determinant of dosing. 48 In contrast, tigecycline undergoes extensive hepatobiliary elimination and requires dose reduction in patients with severe hepatic impairment.49,50
New β-lactams + inhibitors (ceftolozane/tazobactam, ceftazidime/avibactam, meropenem/vaborbactam) and Cefiderocol has almost exclusively renal as unchanged drug with Minimal hepatic metabolism; negligible biliary excretion therefore no hepatic dose adjustment is needed.
In invasive fungal infections, fluconazole pharmacokinetics are relatively preserved in mild to moderate hepatic dysfunction, whereas voriconazole, which is extensively metabolized by hepatic CYP enzymes, shows increased exposure and reduced clearance, warranting dose reduction and routine TDM.24,51,52 Among echinocandins, caspofungin requires adjustment in moderate hepatic impairment, while anidulafungin and micafungin are less affected by liver dysfunction.53–56 Lipid formulations of amphotericin B are minimally influenced by hepatic function and do not require dose modification.57,58
Prophylaxis in Liver Transplant Recipients
Liver transplantation (LT) remains a life-saving therapy for acute and chronic liver failure in the absence of contraindications. An active infection at the time of transplantation is no longer considered an absolute contraindication provided that it is adequately treated; however, it is associated with a significantly increased risk of perioperative morbidity and mortality, underscoring the importance of optimal infection control before LT.59–61 After transplantation, bacterial infections remain common and are a major cause of graft dysfunction, graft loss, and death. The most frequent infectious complications include intra-abdominal, surgical site, and bloodstream infections. Both Gram-positive organisms (eg, Enterococcus spp., Staphylococcus aureus) and Gram-negative bacteria (eg, Enterobacterales) are commonly involved. In recent years, there has been a marked rise in infections caused by MDROs among patients with cirrhosis and LT recipients19–24,59–62,. Pre-transplant colonization with MDROs is a well-recognized risk factor for post-transplant MDR infections.62,
Because induction immunosuppression is most intense during the early perioperative period (days 0-4 after transplantation), perioperative antibiotic prophylaxis is recommended to prevent postoperative bacterial infections. According to the 2023 ESCMID/EUCIC guidelines, screening LT candidates for MDRO colonization represents good clinical practice, particularly in settings with high MDR prevalence.67 However, current evidence remains insufficient to support or discourage the routine use of targeted perioperative chemoprophylaxis based solely on colonization status. 62
In low-risk patients, standard prophylaxis with a third-generation cephalosporin plus ampicillin (to ensure adequate Enterococcus coverage) or piperacillin–tazobactam (covering Enterobacterales, Enterococcus spp., and Pseudomonas aeruginosa) is recommended.59–61 Prophylaxis should generally be initiated within 60 min before surgical incision and should not exceed 24–72 h in uncomplicated procedures.
Colonization with MDROs represents a major challenge in LT and is consistently associated with an increased risk of early post-transplant infections caused by resistant pathogens.19–24,59–62 In the setting of LT, the transition from colonization to invasive infection is facilitated by surgical stress, ischemia–reperfusion injury, disruption of anatomical barriers, and profound immunosuppression in the immediate perioperative period.
Despite the strong association between MDRO colonization and subsequent infection, the optimal strategy for perioperative antibiotic prophylaxis in colonized patients remains controversial. Current international guidelines recommend systematic screening for MDRO colonization as part of pre-transplant evaluation but do not endorse routine modification of standard prophylactic regimens solely based on colonization status. 62 This cautious approach reflects the limited and heterogeneous evidence supporting targeted prophylaxis, as well as concerns regarding antimicrobial overuse, ecological impact, and further selection of resistance.
Targeted prophylaxis, when considered, should be restricted to carefully selected high-risk patients. In critically ill patients, prophylactic regimens should be tailored to local epidemiology and individual susceptibility profiles, ideally in consultation with infectious disease specialists and antimicrobial stewardship teams. Importantly, the duration of prophylaxis should remain limited to the perioperative period, as prolonged administration has not demonstrated additional benefit and may increase the risk of secondary infections and resistance emergence.19–24,59–62
Key Messages and Future Directions
Critical care management of patients with ALF is intrinsically complex and becomes particularly challenging in case of possible or proven infection. Future technological and investigative efforts should prioritize the validation and clinical implementation of novel biomarkers and rapid diagnostic test capable of accurately confirming or keeping out infection and identifying its etiologic agents in a timely manner. In parallel, further research is warranted to refine antimicrobial stewardship strategies, including the optimization of targeted prophylactic regimens in liver transplantation and the development of therapeutic drug monitoring–guided approaches to enhance the efficacy and safety of empiric antimicrobial therapy in patients with highly variable and dynamic hepatic function.
Footnotes
Acknowledgements
LC: conceptualization, investigation, methodology, project administration, supervision, validation, visualization, writing—original draft, and writing—review & editing. MP, MS, AT: conceptualization, investigation, methodology, project administration, validation, writing—original draft, and writing—review & editing. PR; ZC, LY, VA, GA, SF conceptualization, investigation, methodology, project administration, validation, writing—original draft, and writing—review & editing.
Ethical Approval
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Cremascoli Luca, Puppo Mattia, Martini Silvia, Toscano Antonio, Girombelli Alessandro, Saglietti Francesco, Voza Antonio, Zanza Christian, Longhitano Yaroslava.