
Abstract
Introduction
Transitions of care among ICU physicians have been shown to negatively affect care processes and could impact clinical outcomes. Liberation from mechanical ventilation is a judgment-based decision and may be delayed when continuity is disrupted by physician handoffs.
Objective
To assess the association between attending physician transitions of care and liberation of patients from mechanical ventilation.
Methods
Retrospective cohort study. Patients were included if they were admitted to one of three medical ICUs and received mechanical ventilation between January 2022 and May 2025. Transition days were defined as any day where the daytime attending intensivist was different than the day prior. Transition days were identified by review of schedules recorded on the online scheduling system.
Results
Of 3657 ICU days were analyzed, 2732 (74.7%) occurred on non-switch days and 925 (25.3%) on transition days. There were no ventilator liberations on 497 (53.7%) transition days, 1 liberation on 292 (31.56%) transition days, 2 liberations on 105 (11.4%) transition days, and >2 liberations on 31 (3.4%) days. Among non-transition days, there were 0 (1356 [49.6%]), 1 (920 [33.7%], 2 (357 [13.1%]), and >2 (99 [3.6%]) ventilator liberations per day. Transition days were associated with a 10% lower rate of liberations per ICU-day (aIRR 0.90, 95%CI 0.88-0.91, p < 0.01). There was no association between transition day and reintubation (aIRR 0.91, 95% CI 0.73-1.13).
Conclusions
Attending physician transition days were associated with a reduction in rates of ventilator liberation. Physician transition is a potentially modifiable contributor to delayed liberation from mechanical ventilation.
Background
Whether to liberate a patient from mechanical ventilation is a multifactorial decision driven by patient, disease, and provider factors. 1 Prior studies have demonstrated that delays in ventilator liberation for eligible patients are common,2,3 representing a potentially modifiable target for improvement. These delays have important implications for intensive care unit (ICU) outcomes, including increased duration of mechanical ventilation, higher complication rates, and greater resource use.
Clinician discontinuity of care has been identified as a potential patient-independent factor that could result in inappropriately delayed ventilator liberation. 4 A clinician starting a service block may be more cautious about liberating a patient whose history and physiology they have not yet fully assessed. In other areas of care, clinician discontinuity of care has been associated with adverse patient outcomes.5–10
Previous studies investigating the association between clinician discontinuity and the impact on ventilator liberation have yielded mixed results.4,11 Older evidence suggested that measures subject to individual preferences, such as liberating from mechanical ventilation, are impacted by discontinuity. 11 However, a recent study has suggested that ventilator liberation practices are consistent throughout a physician's days of service. 4
Given that the decision to liberate a patient from mechanical ventilation is very complex and influenced by many factors, it is likely to be particularly susceptible to inertia. In this study, we build upon prior evidence by leveraging electronically captured daily physician schedules and a more contemporary patient cohort, to examine the relationship between physician discontinuity and ventilator liberation.
Materials and Methods
Setting and Study Population
This was a retrospective cohort study conducted at three hospitals that are part of a single urban health system. Patients were included if they were admitted to the Medical Intensive Care Unit (ICU) and received mechanical ventilation between January 2022 and May 2025. This period was chosen to avoid any impact of the COVID-19 pandemic. Each of the three ICUs (one at each hospital) is overseen by a single attending intensivist; remaining provider staffing includes a combination of fellows, residents, and advanced practice providers. Overnight there is also coverage by a separate attending intensivist. The day time attending schedule roughly approximates to a week of coverage at a time. The night time attending schedule is less regular and generally coverage is for shorter periods of time, often with a different attending each night.
The Albert Einstein College of Medicine Institutional Review Board provided ethical approval for this study (IRB #2024-15783).
Primary Exposure
A transition day was defined as any day where the daytime staff intensivist for an ICU was different than the one the day prior.
Transition days were identified by review of past schedules recorded on the online scheduling platform used at the study site.
Primary Outcome
The primary outcome was the number of ventilator liberations per ICU-day. The number of patients liberated on an ICU-day who subsequently required re-intubation during their hospital course was included as a balancing measure.
Data Abstraction
Patient demographics, comorbidities, illness severity, and other factors were abstracted from the electronic health record. Three investigators were involved in the adjudicating the data abstracted, and a single investigator confirmed all adjudicated data. ICU-level information including ICU census, ICU severity of illness, and number of ventilated patients were also abstracted from the electronic health record using a temporal anchor of 7:00am.
Ventilator liberation was identified in the medical record by identifying patients that were documented as receiving invasive mechanical ventilation for at least 30 min who were then receiving a non-invasive mode of oxygen support or no oxygen support for at least 30 min on the same day.
Reintubation was defined as receipt of invasive mechanical ventilation for at least 30 min at any time following an initial ventilator liberation.
Following each data abstraction phase, 10 patient charts selected at random were reviewed by physician investigators in detail to ensure the accuracy of the data abstraction process. This continued until no errors in the 10 reviewed patients were identified.
Statistical Analysis
The unit of analysis was the ICU-day. An ICU day was defined as the 24-h time interval from 7:00AM until 7:00AM the following day.
As an initial descriptive analysis, we summarized the number and proportion of ventilator liberations occurring on attending switch and non-switch days.
For inferential analyses, daily ventilator liberation counts were modeled using negative binomial regression to account for overdispersion in count data.
The model adjusted for mean patient age, proportion of female patients, proportion of Black patients, total modified SOFA score (not including neurologic component) for ICU patients, year of ICU-day, month of ICU-day, and hospital site. To account for differences in the number of patients at risk for ventilator liberation across ICU days, models additionally adjusted for total ICU census. Robust standard errors were used for inference. Results are reported as incidence rate ratios (IRRs) with 95% confidence intervals. Standard errors were clustered at the ICU level to account for correlation of daily liberation counts within ICUs. As a sensitivity analysis, ventilator liberation rates were modeled using Poisson regression with an offset for the log of the daily mechanically ventilated census, restricting analyses to ICU-days with at least one mechanically ventilated patient. Reintubations prior to ICU discharge among patients extubated on a given ICU-day were analyzed using Poisson regression with a log link, with the number of liberations on that day included as an exposure term. Analyses were restricted to ICU-days with at least one liberation, and robust standard errors were used. For all comparative analyses, a two-sided p-value of 0.05 was used as the a priori threshold for statistical significance.
All analyses were performed using Stata (v18.5, College Station, Texas, USA).
Results
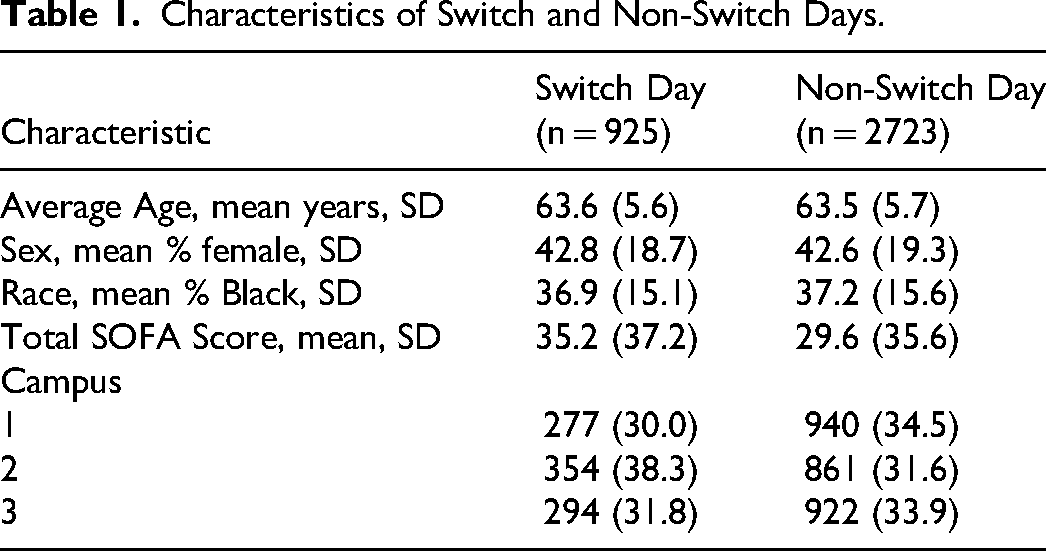
A total of 3657 ICU days were analyzed, of which 2732 (74.7%) occurred on non-switch days and 925 (25.3%) on switch days. Characteristics of switch days and non-switch days can be found in Table 1. Patient characteristics at the individual patient level can be found in Supplemental Table S1. At each hospital, the proportion of transition days was similar (Hospital A 277 (22.7%) days; Hospital B 354 (29.0%) days; Hospital C 294 (24.1%)). The median ICU-census was 10 (IQR 9-12) patients on both transition and non-transition days. On transition days, there were a median of 6 (IQR 5-7) patients receiving mechanical ventilation and a median of 6 (IQR 4-7) on non-transition days.
Characteristics of Switch and Non-Switch Days.
The distribution of ventilator liberations can be found in Figure 1, categorized by transition-day status. There were no ventilator liberations on 497 (53.7%) transition days, 1 liberation on 292 (31.56%) transition days, 2 liberations on 105 (11.4%) transition days, and >2 liberations on 31 (3.4%) transition days. Among non-transition days, there were 0 (1356 [49.6%]), 1 (920 [33.7%], 2 (357 [13.1%]), and >2 (99 [3.6%]) ventilator liberations per day (Figure 1).
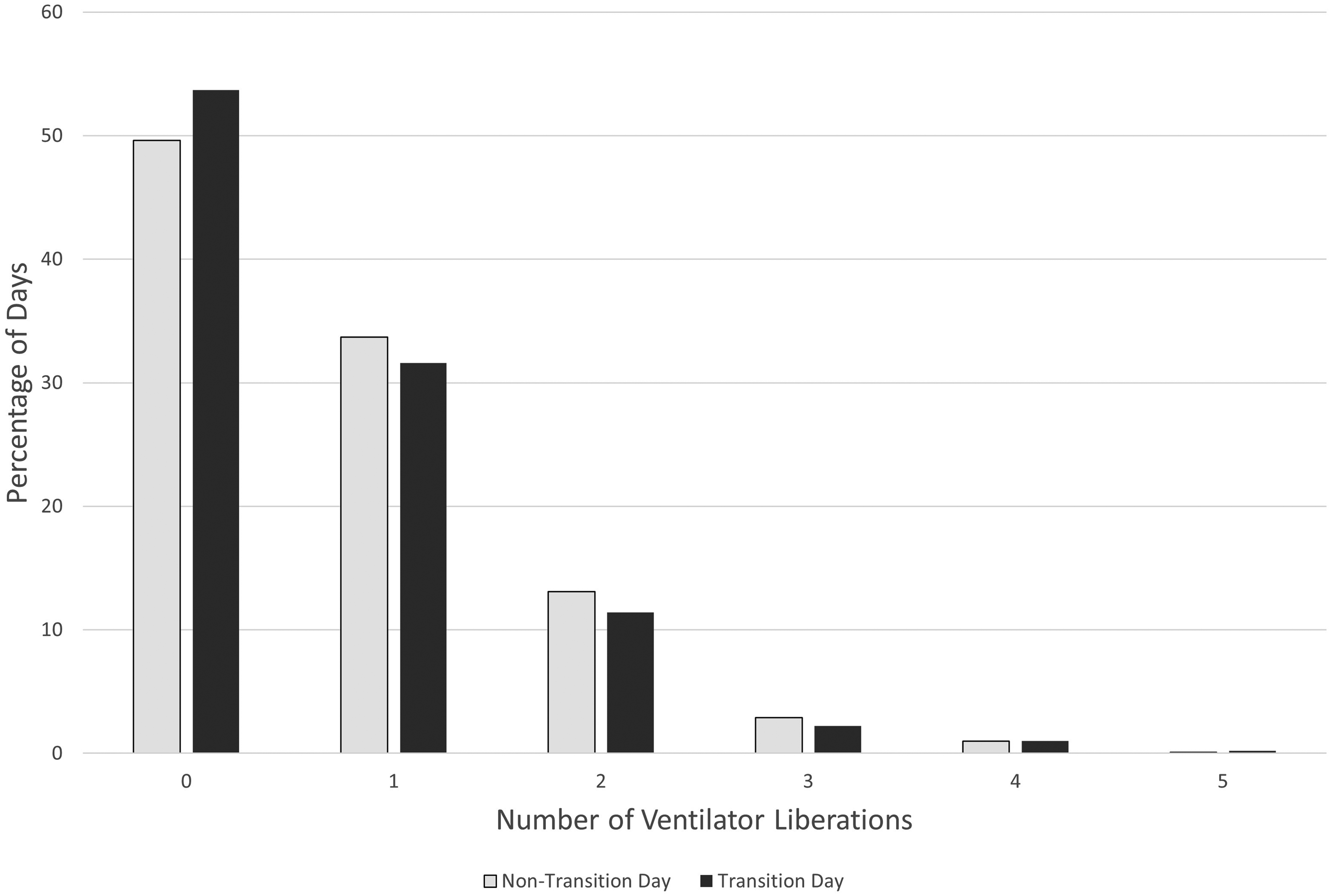
Graphical representation.
In the regression model, transition days were associated with an approximately 10% lower rate of liberations per ICU-day (aIRR 0.90, 95%CI 0.89-0.92, p < 0.01). Results were similar in sensitivity analyses modeling liberation rates per mechanically ventilated patient-day using an offset for ventilated census, with switch days associated with a lower liberation rate compared with non-switch days (aIRR 0.91, 95% CI 0.83-1.00; p = 0.05). There was a mean of 0.7 ventilator liberations a day. Over 100 days, there would be a mean of approximately 70 ventilator liberations.
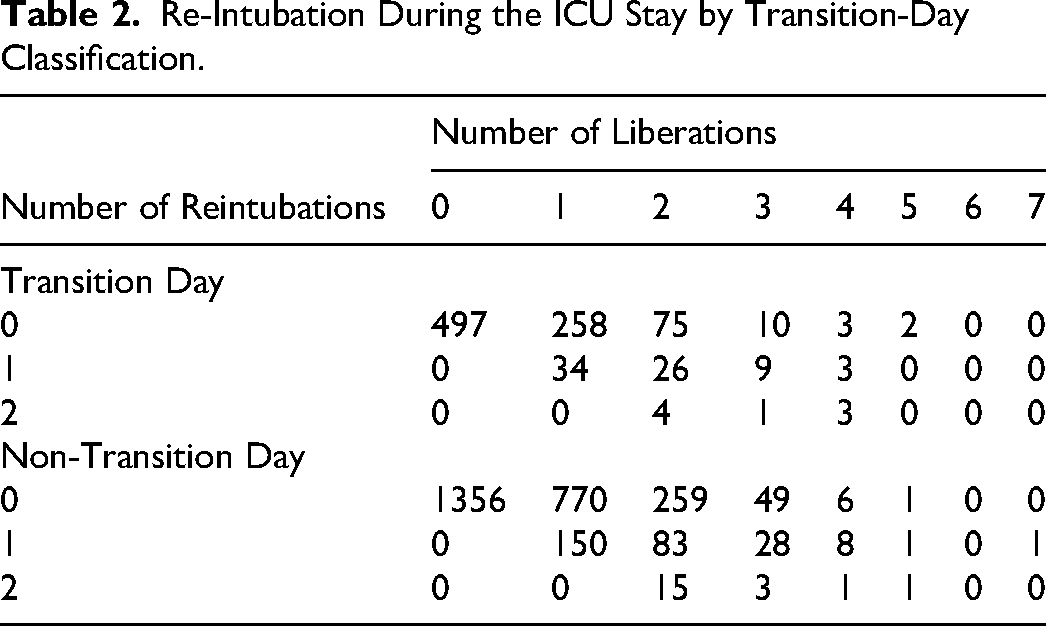
The distribution of re-intubations according to the number of ventilator liberations each ICU-day can be found in Table 2. There was no association between transition day and risk for reintubation (aIRR 0.91, 95% CI 0.73-1.13).
Re-Intubation During the ICU Stay by Transition-Day Classification.
Discussion
In the present study, we observed a modest association between attending transition days and the rate of liberation from mechanical ventilation. Despite the difference in liberation rates there was no significant difference in rates of reintubation between transition and non-transition days. Our findings build upon the growing body of literature on the impact of discontinuity in ICU care.4,11
Prior data on the impact of physician discontinuity on liberation from mechanical from Angriman et al, found that days with a change in attending physician were associated with a lower likelihood of liberation from mechanical ventilation after a successful spontaneous breathing trial with an odds ratio of 0.77. 11 Notably, there was less impact on other studied measures that were protocolized and less dependent on individual physician decision making. 11 A recent study by Barker et al, however, found that the day when an attending physician was on service (first, intermediate, or last) had no association with timely liberation from mechanical ventilation after a successful spontaneous breathing trial. 4 In the study, odds ratio for timely liberation on an intermediate day (neither first or last) compared to first service day was 1.12 (0.88 to 1.43) and on a last day odds ratio compared to first was 1.01 (0.72 to 1.42). 4
The study by Angriman et al leveraged a proxy (day of the week) for physician care discontinuity, and did not directly examine granular physician schedules which are often impacted by factors such as holidays, sick days, and other factors. 11 The study by Barker et al, examined timeliness of liberation from mechanical ventilation, which they defined as within 6 h of first passing SBT rather than examining whether liberation from mechanical ventilation occurred at all. 4 Our study, in contrast, directly examined the impact of transition of care without using any surrogate for either physician transition day or ventilator liberation. Given the contradiction between the prior two results, our study provides valuable additional evidence to help understand the impact of discontinuity on patient care and guide best practice standards.
While our study does not directly explain why the differential in liberation mechanical ventilation exists, it is possible to explain the difference with the framework of clinical inertia. This concept in medicine has been defined as the failure to initiate, alter, or intensify treatment when indicated, and is most considered when treatments are not escalated appropriately. 12 However our study implies that clinical inertia applies to some extent with regards to deescalation of therapy, which is analogous to an object in motion remaining in motion. 13 This inertia manifests as a hesitation on the part of providers to liberate patients from mechanical ventilation on transition days.
Our findings also suggest that the decision to liberate a patient from mechanical ventilation belongs to a category of decisions that may be impacted by the provider's particular experience caring for that individual patient. This effect can also be seen in other clinical decisions. Patients are less likely to be liberated from mechanical ventilation immediately post-operatively if there is a change in attending anesthesiologist during the case. 14 Length of stay has also been shown to be increased by change in general internal medicine provider. 15 Our study adds to this evidence that for a certain category of clinical decision making for which clinical inertia is primarily mitigated by first-hand experience of a patients clinical trajectory.
Our study has several limitations. We cannot definitively say which patients that were not extubated met appropriate criteria for liberation from mechanical ventilation. However, due to the large number of patients and the large effect size, it seems highly unlikely that there would be a sufficient difference between transition-days and non-transition days in clinical appropriateness for mechanical ventilation. Our data were acquired retrospectively, so it was dependent on accurate charting to avoid errors or missing information. We mitigated this weakness by utilizing a well-defined method of chart abstraction and manually reviewing a subset of cases to ensure accuracy. The decision to liberate a patient from mechanical ventilation is made with input from a multidisciplinary team such as medical trainees and respiratory therapists, our study does not consider the roll of staffing practices of these other members of the care team. We felt however, that it was attending transition that would have the greatest effect on the decision to extubate and decided to focus on measuring the impact of this parameter. Our study also does not consider the impact of changes in night time attending coverage. Because the analysis was performed at the ICU-day level, we were unable to evaluate patient-level time to ventilator liberation, formally account for competing risks such as death, or assess lagged effects following attending transition. In addition, because transition days were concentrated on Mondays and Saturdays, transition-day status was closely linked to the weekly staffing schedule, making it difficult to disentangle the effect of physician transition from broader day-of-week workflow patterns, although measured day-level characteristics were otherwise similar across days of the week. Table S2 shows the distribution of switch days across the week together with measured day-level characteristics by day of week. Although we adjusted for ICU-day level patient-mix and operational characteristics, we did not fully adjust for individual patient-level factors such as comorbidity burden, indication for mechanical ventilation, and duration of ventilation because the unit of analysis was the ICU-day rather than the individual patient; accordingly, residual confounding from patient-level differences remains possible. While we controlled for confounding factors based on prior literature, we cannot be sure that unmeasured confounding factors did not affect the results. Finally, the study was done at several hospitals that are part of a single hospital system. Replication of the results in other settings is warranted.
Our study also has several strengths. First, we manually searched the attending schedule to accurately define switch days rather than making assumptions based on days of the week. Second, the number of patients included in this study is large compared to the previous studies on this issue.4,11 Third, the population was diverse with a large percentage of women, non-white, and Hispanic patients represented. Finally, the results of sensitivity analyses were consistent with the main results.
In conclusion, liberation from mechanical ventilation is significantly less likely to happen on a day that the attending physician in the ICU changes. Further studies may expand our understanding of the ways in which clinical inertia may have other impacts in the ICU setting. Ideally, this will also elucidate exactly which decisions are affected disproportionately and which interventions will mitigate it. We hope that cognizance of the effect of clinical inertia may be the first step in mitigating its potential harmful effects and lead to improved patient outcomes.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261459323 - Supplemental material for Association Between Attending Physician Transition Days and Liberation from Mechanical Ventilation in the Intensive Care Unit
Supplemental material, sj-docx-1-jic-10.1177_08850666261459323 for Association Between Attending Physician Transition Days and Liberation from Mechanical Ventilation in the Intensive Care Unit by Suraj Nagaraj, Ari Moskowitz, Talya Lisker, Thomas Butler and Lewis A. Eisen in Journal of Intensive Care Medicine
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.