
Abstract
Objective
Although opioids are used frequently in pediatric intensive care units (PICUs) for analgesia and safety, the long-term consequences of opioid exposure in PICU are unknown. We performed this exploratory study to examine the relationship between PICU-related opioid exposure and chronic prescription opioid use in adult survivors. Our primary outcome was the prevalence of chronic prescription opioid use, defined as filled opioid prescriptions covering >70% of days within a 3-month period during the adult observation period.
Design and setting
Patients
We included children (birth to 16 years) who required PICU admission for critical illness that included opioid exposure and ≥48 h of mechanical ventilation after January 1, 1995 and reached adulthood (18 years) by January 1, 2015. We examined adult opioid prescription data for the 5 years from 2015 to 2019.
Interventions
None
Measurements and main results
Of 313 eligible participants, we excluded 194 for death, migration, or loss to follow-up; 119 were included. Six (5%) met criteria for chronic prescription opioid use as an adult. Compared with participants who had chronic opioid use, those without chronic opioid use had significantly fewer PICU admissions in childhood (median [IQR] = 3[1–6] vs 1[1–2] respectively, p = 0.040) and a higher mean Therapeutic Intervention Scoring System score (surrogate for severity of illness, mean [SD] = 29.3[6.6] vs 35.9[7.4], p = 0.036), but no difference in cumulative opioid exposure (median [IQR] mg/kg morphine equivalents = 8.4 [3.2-11.4] vs 7.3 [2.8-17.0], p = 0.49).
Conclusion
Adult survivors of pediatric ICU admissions demonstrated a prevalence of chronic prescription opioid use of 5%. Pediatric critical illness necessitating PICU admission and opioid prescription were not associated with chronic opioid prescription use in our cohort.
Keywords
Introduction
Opioids are a mainstay of sedation and analgesia management for children in pediatric intensive care units (PICUs). 1 While necessary for comfort and safety, opioids may cause adverse outcomes such as withdrawal, delirium, tolerance, and dependence. 2 Preliminary evidence in both pediatric and adult populations indicates that exposure to opioids is a risk for future use and abuse3,4; high school students demonstrated a 33% increased risk of opioid abuse after prescription. 5 The relationship between opioid administration for sedation and analgesia in PICU and later opioid prescribing and abuse in adult survivors has not been explored.
Chronic opioid use was demonstrated up to 2 years after adult ICU admission in one population-based study 6 though this was not reproduced in another, smaller study. 7 However, early exposure of the developing brain to neuroactive agents may impact long-term outcomes and children may have a different response to opioids at critical periods of neurodevelopment. Therefore, we performed this exploratory, hypothesis-generating study to examine the relationship between PICU-related opioid exposure and chronic prescription opioid use in adult survivors of PICU admissions. We hypothesized that the prevalence of chronic opioid use in our study population in adulthood is similar to other adults in our region (6.2%, N = 2595). 7
Materials and Methods
Design and Setting
We performed a single-center, retrospective cohort study that used linkage of databases from the PICU at IWK Health (IWK) to that of the Nova Scotia Prescription Monitoring Program (NSPMP). The PICU at IWK is a tertiary level, 8-bed mixed medical-surgical/cardiac PICU that provides care for patients from birth to 16 years from 3 Canadian provinces. The NSPMP is a provincial program overseen by the Nova Scotia (NS) Department of Health and Wellness. Data collected by the NSPMP includes opioids (and other monitored & controlled substances) dispensed at community pharmacies in NS. In 1995, NS health card numbers (HCNs) became digitized to allow patient tracking between programs and were consistently collected and recorded in the IWK databases thereafter. The study was approved by the IWK Research Ethics Board and the NSPMP. Study conduct and reporting were guided by the reporting of studies conducted using observational routinely collected health data statement for pharmacoepidemiology (RECORD-PE) checklist (Supplemental File 1). 8
Participants
We included Nova Scotian children (ages 37 weeks post-conceptual age to 16 years) admitted to IWK's PICU after January 1, 1995. Potential participants were born before January 1, 1997 to ensure they reached adulthood (18 years) by January 1, 2015. This was designed to allow 5 years of adult prescription drug monitoring data (January 1, 2015 - December 31, 2019) at the time of study planning. Though the study was interrupted for two years during COVID-19, study period were not shifted. We defined exposure as receipt of opioids and ≥48 h of mechanical ventilation to ensure a sufficiently ill population. Participants were excluded if they did not have an active Nova Scotia HCN at any point from January 1, 2015 to December 31, 2019 due to either death or migration.
Participant Identification and Data Collection
We identified potential participants through IWK's internally-maintained, electronic PICU database, which identifies patients by both health care and hospital chart numbers to allow linkage between admissions, and includes dates of admission, basic demographic data, presence of invasive ventilation, reason for admission, and mortality. We then examined the paper medical records of potential participants to confirm eligibility and, once confirmed, to collect PICU admission-related data including: demographics; major surgical procedure(s); reason for each admission; presence of chronic underlying medical conditions (eg congenital heart disease, asthma, cerebral palsy); number and length of PICU admission(s); total ventilated days in childhood; mean and maximum Therapeutic Intervention Scoring System (TISS) score (a validated measure of illness severity based on the intensity of ICU interventions)9,10 for each admission; and opioids received for each PICU admission. Data that retained the provincial HCN but was otherwise de-identified was sent to NSPMP. The NSPMP representative removed the data file for potential participants who did not have an active NS HCN at any point from 2015–2019, inserted opioid prescriptions that had been filled for the study cohort, removed the HCN, and returned the anonymized data. See Figure 1 for description of data collection and linking flow. Potential participants for whom medical record or NSPMP records were not available were removed from the study.
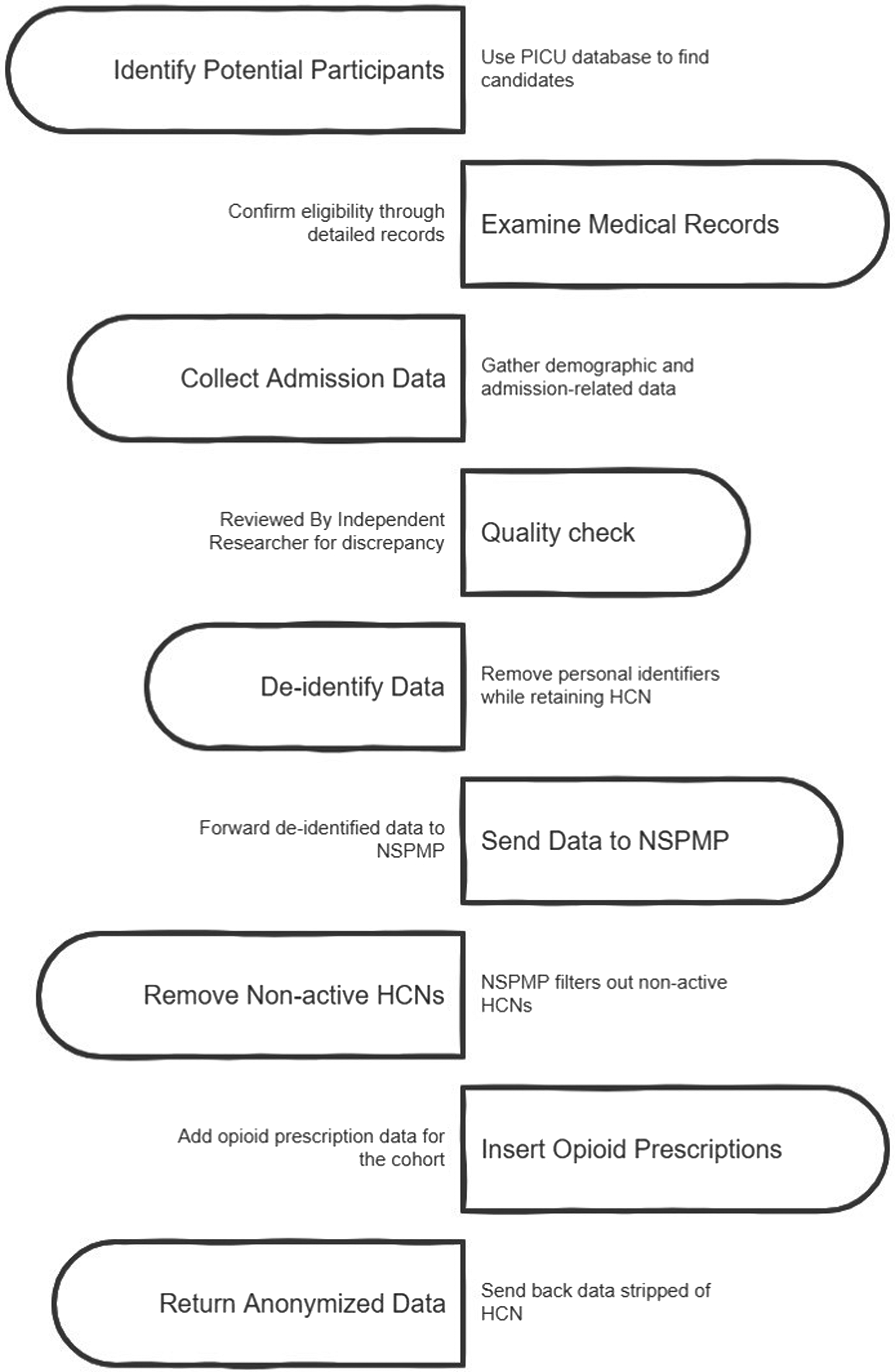
Data linking process.
Quality Assurance
Data abstraction followed a standard operating procedure based on a data dictionary. A second researcher performed independent data collection for 10% of charts; fewer than 5% of data points were noted to be discrepant.
Outcomes
We defined chronic opioid use as any filled opioid prescriptions covering ≥70% of days in a 3-month period in the period of adulthood observation (5-years). 7 This definition was based on previous study done by Yaffe et. al. in survivors of adult ICU in Nova Scotia. A fixed time point was chosen, rather than a fixed participant age, to optimize study and data extraction feasibility and assuming patients who had chronic opioid use would fill prescription during this 5-year period regardless of age and time from exposure if they had significant/persistent issues with chronic opioid use.
Analysis
We converted opioids to morphine equivalents (Supplemental File 2) to enable comparison and cumulative opioid dose calculation (sum of morphine equivalents in mg/kg over all admissions). We summarized data descriptively using means (standard deviation), medians (interquartile range) and frequency (percent). Secondary analyses were exploratory and hypothesis-generating, intended to identify potential associations between PICU exposure variables and adult opioid outcomes rather than to test confirmatory hypotheses. Baseline demographics were compared between those with and without adult chronic opioid use using the Student's t-test or the Mann-Whitney U test for continuous and Fisher's exact test for categorical variables. We used the Student's t-test or Spearman's rank correlation coefficient to assess relationships between total morphine equivalent dose per kg as a child and opioid use as an adult. A two-sided p-value of < 0.05 was the threshold for statistical significance. All analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, N.C, USA).
Results
We identified 313 eligible participants through the PICU database based on inclusion and exclusion criteria, excluded 155 through further chart review, and lost 11 to follow-up (Figure 2). The NSPMP excluded 28 for no active Nova Scotia HCN from 2015–2019. We included 119 patients in the final cohort. Demographic and baseline data are presented in Table 1.
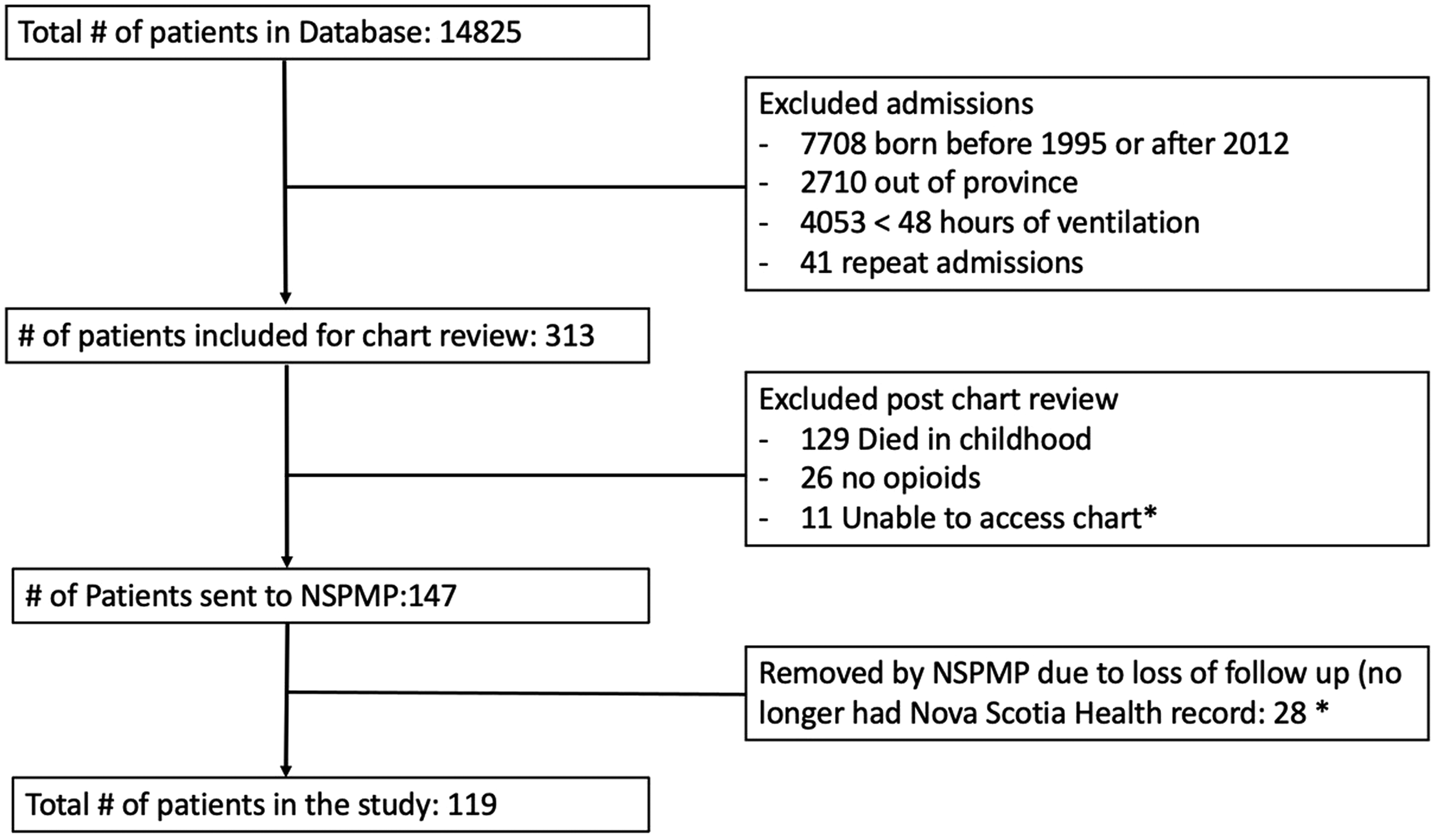
Patient inclusion and flow.
Admission and Demographic Data for Cohort and by Chronic Prescription Opioid Status. (Note, cell reporting has been censored where the number of participants is <5).
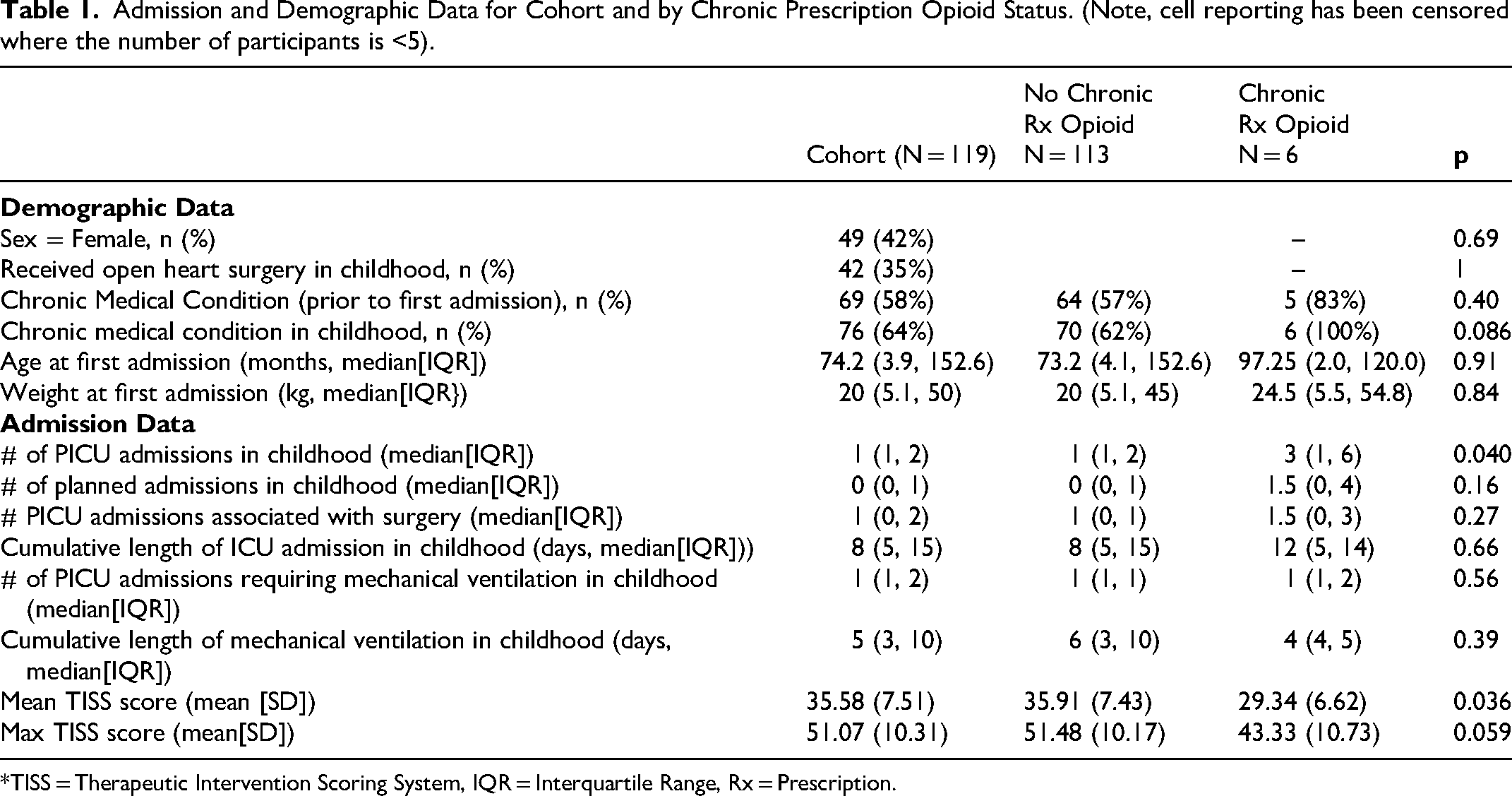
*TISS = Therapeutic Intervention Scoring System, IQR = Interquartile Range, Rx = Prescription.
Six participants (5%) met criteria for chronic opioid use as an adult. This was similar (Fisher's Exact probability 0.84) to the prevalence of chronic opioid use previously reported in a local population of adults prior to ICU admission. 7 Five participants (83%) who developed chronic opioid use in adulthood had chronic medical conditions in childhood (eg, cancer, congenital heart disease). Participants with chronic prescription opioid use had a median (IQR) of 3(1-6) PICU admissions in childhood, significantly more than those who did not have chronic prescription opioid use (1[1-2], [p = 0.04]), though they had a lower mean (SD) TISS than those without chronic use (29.3[6.6] vs 35.9[7.4] respectively, p = 0.036).
The range of PICU-based opioid exposures during childhood in the entire cohort was 0.04–100.6 mg/kg morphine equivalents. There was no difference in median (IQR) cumulative PICU opioid exposure between those with (8.4 [3.2-11.4] mg/kg morphine equivalents) and without (7.3 [2.8-17.0] mg/kg morphine equivalents) chronic prescription opioid use (p = 0.49) (Table 1). We did not identify a correlation between total PICU morphine equivalents (mg/kg) and either percent of adult days receiving opioids (Spearman's rho 0.003, p = 1.0) or morphine milligram equivalents prescribed per day as an adult (Spearman's rho 0.01, p = 0.9).
Discussion
In this exploratory study, the prevalence of chronic opioid use in adults who survived childhood PICU admission was 5% and similar to that in Nova Scotians prior to their adult ICU admission (6.2%). 7 There was no demonstrable relationship between the amount of opioid received during PICU admissions and opioid prescription requirement as an adult. This suggests that opioid exposure during a PICU admission may not be a risk factor for chronic opioid use in adults.
While extensive literature addresses neurodevelopmental, psychological, and chronic disease burden of neonatal and pediatric critical care-related opioid exposure, we are not aware of longitudinal data linking childhood ICU exposure to either adult or chronic opioid use. Prescription in children and youth during healthcare encounters, including during cancer therapy 11 and surgery, 12 has been associated with subsequent opioid use and, in some cohorts, longer term use into adulhood.4,13 However, these relationships are likely confounded by underlying illness and chronic pain.
We noted that participants with multiple PICU admissions, lower nursing care requirements, and those with chronic medical conditions were statistically more likely to have chronic opioid use as an adult. One might hypothesize that multiple admissions to PICU with recurrent childhood exposure to opioids places these children at higher risk for opioid use in adulthood than would be seen with higher doses of opioids associated with a single, high severity of illness admission. We also noted non-significant trends to increased opioid use in adult survivors who had more frequent planned PICU admissions, underwent more surgeries, and had pre-existing chronic medical conditions in childhood. Chronic disease starting in childhood and requiring PICU admission or co-morbidities acquired because of PICU admission may continue into adulthood, increasing risk for mental illness and pain. This, rather than the PICU admissions themselves, may account for chronic opioid use in adulthood, particularly given clear associations between pain, mental illness, and chronic disease.4,13,14
For similar reasons, it should be noted that the comparison group – adult patients prior to ICU admission – likely over-represents chronic opioid use compared with the general population. Adult ICU admission rates are higher for individuals who receive opioids; a Dutch study reported 1-year adult ICU admission rates of 5.9 per 1000 person-years in individuals who received any opioid prescription in the preceding 3 months, versus 2.2 per 1000 person-years for those who had not, though individuals who had chronic opioid use had lower admission rates than those who received a single prescription. 15 The population-based prevalence in our region has not been reported so, while our results are comparable to adult studies in Nova Scotia that used similar methodology, 7 it remains possible that the prevalence in our sample is higher than for the general population. Additionally, it may be important that a significant portion of the PICU population have severe neurologic impairment that limit communication and mobility 16 and may preclude manifestation of opioid dependence.
While this study represents the novel use of data linkage between two robust databases that have been maintained for several decades, there are several limitations that restrict generalizability. Our historic cohort size was small with significant loss to follow-up, primarily from migration or health record loss. Repeating the study in 10–15 years would provide a significantly larger number of adult participants, though studies using this methodology will not allow attribution of adult prescription opioid use to pediatric exposure. As a single-centered study, practice variations related to opioid management may have impacted opioid sensitization. Change in PICU populations and practice over eras may limit generalizability to current practice, as pre-PICU liberation opioid prescribing practices were likely more liberal. 17 It is also likely that our findings under-estimate the true prevalence of chronic opioid use in adults as we could only examine prescription, rather than non-prescribed, opioid use.
Conclusions
In this hypothesis generating, exploratory study, pediatric critical illness necessitating PICU admission and opioid prescription showed no correlation with chronic opioid prescription use in adulthood in our cohort. Future exploration, particularly multicentered, of the relationship between chronic opioid use and repeated PICU admission, planned PICU admissions, and chronic medical conditions may be warranted.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261459326 - Supplemental material for Chronic Opioid use in Adult Survivors of Pediatric ICU Admissions in Nova Scotia: A Retrospective Cohort Study
Supplemental material, sj-docx-1-jic-10.1177_08850666261459326 for Chronic Opioid use in Adult Survivors of Pediatric ICU Admissions in Nova Scotia: A Retrospective Cohort Study by Ayush Lacoul, Tobias Witter, Kristina Krmpotic, Kirstin Crabtree, Lilian Cristina Gomez and Jennifer R. Foster in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666261459326 - Supplemental material for Chronic Opioid use in Adult Survivors of Pediatric ICU Admissions in Nova Scotia: A Retrospective Cohort Study
Supplemental material, sj-docx-2-jic-10.1177_08850666261459326 for Chronic Opioid use in Adult Survivors of Pediatric ICU Admissions in Nova Scotia: A Retrospective Cohort Study by Ayush Lacoul, Tobias Witter, Kristina Krmpotic, Kirstin Crabtree, Lilian Cristina Gomez and Jennifer R. Foster in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge the support of Dr Chris Soder for assistance with database searching, and the Nova Scotia Prescription Monitoring Program for support with data linkage and adult prescription abstraction. The authors also thank Navjot Sandila and the Dalhousie Research Methods Unit for support with statistical analysis.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the IWK Research Ethics Board (#1025274) and the Nova Scotia Prescription Monitoring Program.
Funding
This work was funded by a peer-reviewed, mentored project grant from IWK Health, PI: Dr Ayush Lacoul, Supervisor: Dr Jennifer Foster.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.