
Abstract
Objective
To compare the efficacy and safety of etomidate versus ketamine as induction agents for rapid sequence intubation in critically ill adults, focusing on 28-day mortality and post-intubation hypotension.
Data Sources
PubMed, Embase, and the Cochrane Library were systematically searched from inception to January 2026. Reference lists of included studies were also manually screened.
Study Selection
We included randomized controlled trials (RCTs) comparing single-dose intravenous ketamine versus etomidate for emergency rapid sequence intubation in critically ill adults (≥ 18 years) in non-operating room settings (eg, intensive care unit or emergency department).
Data Extraction
Two investigators independently screened records, extracted data using a standardized form and assessed the risk of bias using the RoB 2 tool. The certainty of evidence was evaluated using the GRADE framework.
Data Synthesis
Six RCTs comprising 4108 randomized patients (2046 assigned to ketamine and 2062 to etomidate) were included. For the primary outcome, the pooled analysis evaluated 4102 patients and showed no statistically significant difference in 28-day mortality between the ketamine and etomidate groups (28.7% vs 29.9%; relative risk [RR] 0.96; 95% CI, 0.87-1.05; I2 = 13.8%). In a prespecified subgroup analysis of patients with sepsis (n = 1546), mortality also did not differ significantly (RR 1.04; 95% CI, 0.91-1.19). However, ketamine was associated with a statistically significant increase in the incidence of post-intubation hypotension (14.2% vs 11.3%; RR 1.25; 95% CI, 1.01-1.53; I2 = 0%). Conversely, ketamine significantly reduced the risk of adrenal suppression compared to etomidate (5.3% vs 14.7%; RR 0.36; 95% CI, 0.17-0.75). No significant differences were observed regarding peri-intubation cardiac arrest or first-attempt intubation success.
Conclusions
For emergency intubation in critically ill adults, including those with sepsis, 28-day mortality is similar between etomidate and ketamine. However, ketamine may increase post-intubation hypotension, whereas etomidate may increase adrenal suppression.
Introduction
Rapid sequence intubation (RSI) is the standard of care for securing the airway in critically ill patients, a high-risk procedure associated with significant rates of life-threatening complications, including severe hypotension and cardiac arrest.1,2 Selecting the induction agent is critical to mitigating these risks. Etomidate and ketamine are the two most commonly used agents in this setting due to their favorable pharmacokinetic profiles and rapid onset of action.3,4
Etomidate has traditionally been favored for its hemodynamic stability. 5 However, it is well-established that even a single bolus dose inhibits the enzyme 11β-hydroxylase, causing reversible adrenal suppression. 6 This “pharmacologic adrenalectomy” has raised persistent concerns regarding its safety in patients with sepsis, potentially impairing the physiological stress response and increasing mortality. 7 Conversely, ketamine is a dissociative anesthetic with sympathomimetic properties that theoretically maintain blood pressure through catecholamine release. 8 Consequently, ketamine has been increasingly advocated for use in patients with shock. 9
Despite these theoretical advantages, the clinical superiority of one agent over the other remains controversial. While etomidate causes adrenal inhibition, it is unclear if this translates to increased mortality or vasopressor requirements.10–12 On the other hand, the hemodynamic safety of ketamine has been challenged; recent evidence suggests it may precipitate cardiovascular collapse in catecholamine-depleted patients, such as those with prolonged septic shock.13,14 Current clinical practice guidelines do not recommend one agent over the other due to conflicting evidence. 15
Prior systematic reviews and meta-analyses7,12,16 have attempted to resolve this debate but have faced significant methodological limitations. Many of these reviews incorporated observational data, which are inherently vulnerable to confounding by indication—specifically, the tendency of clinicians to preferentially administer etomidate to the most hemodynamically unstable patients due to its perceived immediate safety profile. 13 Other meta-analyses have pooled quasi-randomized trials or evaluated admixtures (such as ketamine combined with propofol or midazolam) rather than pure agents, artificially diluting the specific comparative effects of ketamine and etomidate.17,18 The persistent concern over etomidate-induced corticosteroid insufficiency and its potential link to mortality has escalated to the point where regulatory agencies in some countries have restricted or completely removed etomidate from the market, despite the lack of definitive randomized evidence.19,20
Recently, the landscape of available evidence has shifted dramatically. New large-scale randomized controlled trials (RCTs) have been published,21,22 contributing thousands of patients and substantial high-quality data regarding both mortality and peri-intubation hemodynamic complications. Given this influx of new evidence, an updated synthesis is imperative to guide clinical practice. We therefore conducted a systematic review and meta-analysis exclusively focused on RCTs—strictly excluding observational cohorts and quasi-randomized studies—to compare the efficacy and safety of single-dose etomidate versus ketamine in critically ill adults, with a specific focus on 28-day mortality.
Methods
This systematic review follows the Cochrane Handbook for Systematic Reviews of Interventions 23 and complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 24 ; the protocol was prospectively registered in PROSPERO (CRD420261279883).
Eligibility Criteria
Studies were deemed eligible for inclusion if they met the following criteria: (a) study design consisting of randomized controlled trials (RCTs) conducted in non-operating room settings, such as the emergency department (ED) or intensive care unit (ICU); (b) adult patients (aged ≥ 18 years) with critical illness requiring emergency RSI; (c) direct comparison of single-dose intravenous ketamine versus etomidate as the primary induction agent; and (d) reporting clinical outcomes of interest. To ensure the analysis focused on high-quality evidence and this specific physiologic profile, we applied the following exclusion criteria: (a) observational studies; (b) trials involving pregnant patients; (c) prisoners; and (d) patients in cardiac arrest prior to intubation.
Search Strategy and Data Extraction
We systematically searched PubMed, Embase, and the Cochrane Library from their inception through January 2026, using a combination of controlled vocabulary and keywords relevant to ‘etomidate’, ‘ketamine’, ‘rapid sequence intubation’, and ‘critical illness’. To ensure comprehensive coverage, we also manually screened the reference lists of all included studies and relevant systematic reviews to identify potential trials not captured by the electronic search. Following the search, two investigators independently screened titles and abstracts for eligibility and extracted data from the included studies using a standardized form, strictly adhering to the pre-established inclusion criteria; any discrepancies were resolved through discussion or adjudication by a third reviewer.
Endpoints and Sensitivity Analysis
The primary outcome was 28-day mortality. Secondary outcomes included periprocedural cardiac arrest, first-attempt intubation success, post-intubation hypotension, adrenal suppression, ICU-free days, and mechanical ventilator-free days. We acknowledge that endpoint definitions varied among the included trials; for instance, cardiac arrest definitions differed slightly regarding the peri-intubation time window, and hypotension was defined by some authors as a percentage decrease from baseline (eg, >20% drop), while others used absolute systolic blood pressure thresholds ranging from <90 mm Hg to <80 mm Hg (Supplemental Material, Post-intubation hypotension definitions). We performed a prespecified subgroup analysis restricted to patients with sepsis to evaluate safety in this high-risk population.
Due to the limited number of studies (N < 10), we assessed potential publication bias and small-study effects for the post-intubation hypotension outcome using a prespecified sensitivity analysis incorporating data from an unpublished quasi-randomized trial (Powers WF, ClinicalTrials.gov NCT03545503). For adrenal suppression, we conducted sensitivity analyses including high risk of bias data and poor proxy information.
Quality Assessment
Two investigators independently assessed the risk of bias for each included trial using the Revised Cochrane Risk of Bias tool for randomized trials (RoB 2). 25 Additionally, the certainty of the evidence for primary and secondary outcomes was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. 26 Any discrepancies in the quality assessment were resolved through consensus.
Statistical Analysis
For binary outcomes, we calculated risk ratios (RRs) with 95% confidence intervals (CIs), while mean differences (MDs) were used for continuous outcomes. Data pooling was performed using the Inverse Variance method for all outcomes, except for peri-intubation cardiac arrest, for which the Mantel-Haenszel method was applied. Continuous variables in the included trials were predominantly reported as medians with interquartile ranges (IQRs), we estimated the sample means and standard deviations using the method described by Wan et al 27 Statistical heterogeneity was evaluated using the Cochrane Q test and the I2 statistic 23 ; heterogeneity was considered significant if the Q test p-value was < .10 or I2 > 50%. All meta-analyses were conducted using a random-effects model. The between-study variance (Tau2) was estimated using the Restricted Maximum Likelihood (REML) method, and 95% CIs were calculated using the classic method. All statistical analyses were performed using R software, version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). 28
Data Availability
The template data collection forms, data extracted from included studies, data used for all analyses, and analytic code generated during this systematic review are not publicly available but can be obtained from the corresponding author upon request.
Results
Study Selection and Baseline Characteristics
The initial electronic search identified a total of 1680 records. After removing duplicates and clearly ineligible studies, the 26 remaining articles were fully reviewed for eligibility. Ultimately, 6 randomized controlled trials21,22,29–32 were included in the quantitative synthesis. The detailed screening process is illustrated in the PRISMA flow diagram (Figure 1).
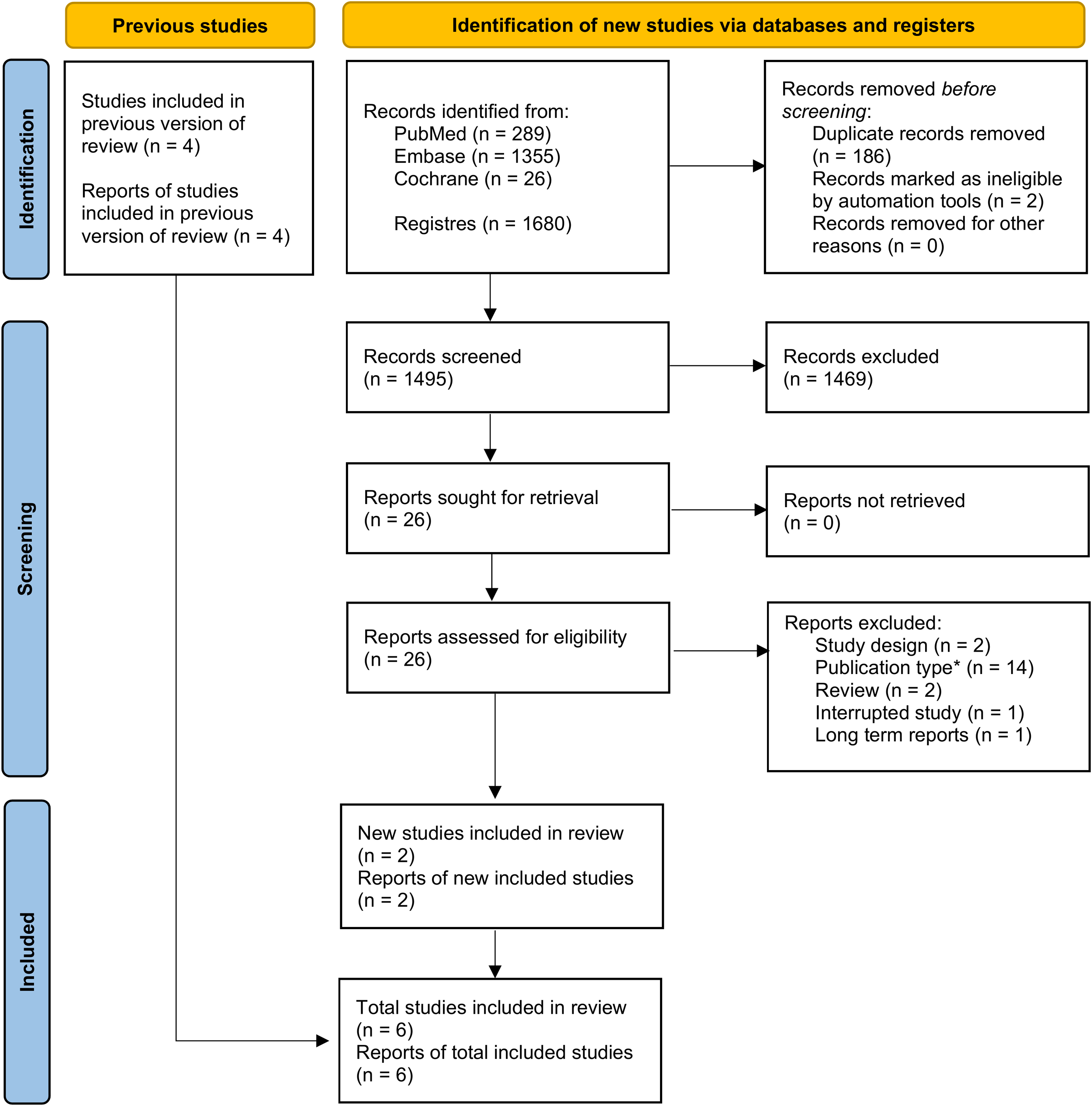
PRISMA flow diagram detailing the study selection process. *Including notes (1), editorials (1), protocols (2), letters (5), commentaries (2), interim analysis (1) and duplicated trial registries (2). Adapted from: Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021.
A total of 4108 randomized patients were included in the quantitative synthesis, with 2046 (49.8%) assigned to the ketamine group and 2062 (50.2%) to the etomidate group. The recent multicenter trial contributed most of the pooled population (n = 2365). 22 The included trials exhibited significant clinical heterogeneity regarding the prevalence of sepsis. Regarding the intervention, dosing protocols varied between fixed weight-based doses and weight-based ranges across trials. Despite these variations, baseline demographics were generally well-balanced between the study arms across all trials (Table 1).
Baseline Characteristics of Included Studies.
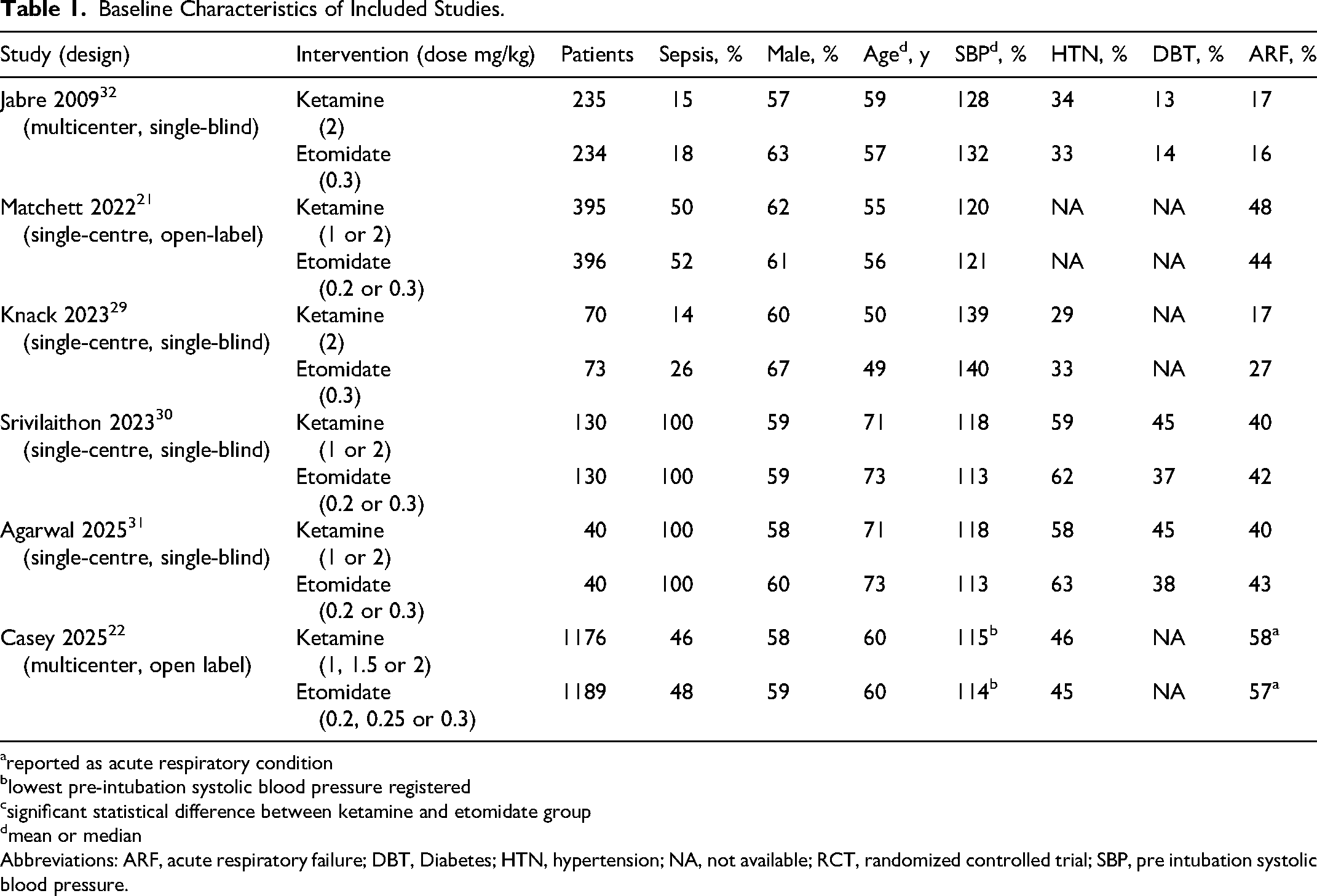
reported as acute respiratory condition
lowest pre-intubation systolic blood pressure registered
significant statistical difference between ketamine and etomidate group
mean or median
Abbreviations: ARF, acute respiratory failure; DBT, Diabetes; HTN, hypertension; NA, not available; RCT, randomized controlled trial; SBP, pre intubation systolic blood pressure.
Pooled Analysis of all Studies
Regarding the primary outcome (n = 4102) the pooled analysis of six trials showed no difference in 28-day mortality between the ketamine (n = 2043) and etomidate (n = 2059) groups (28.7% vs 29.9%; Risk Ratio [RR] 0.96; 95% Confidence Interval [CI], 0.87 to 1.05; P = 0.38). Heterogeneity for this outcome was low (I2 = 13.8%). (Figure 2)
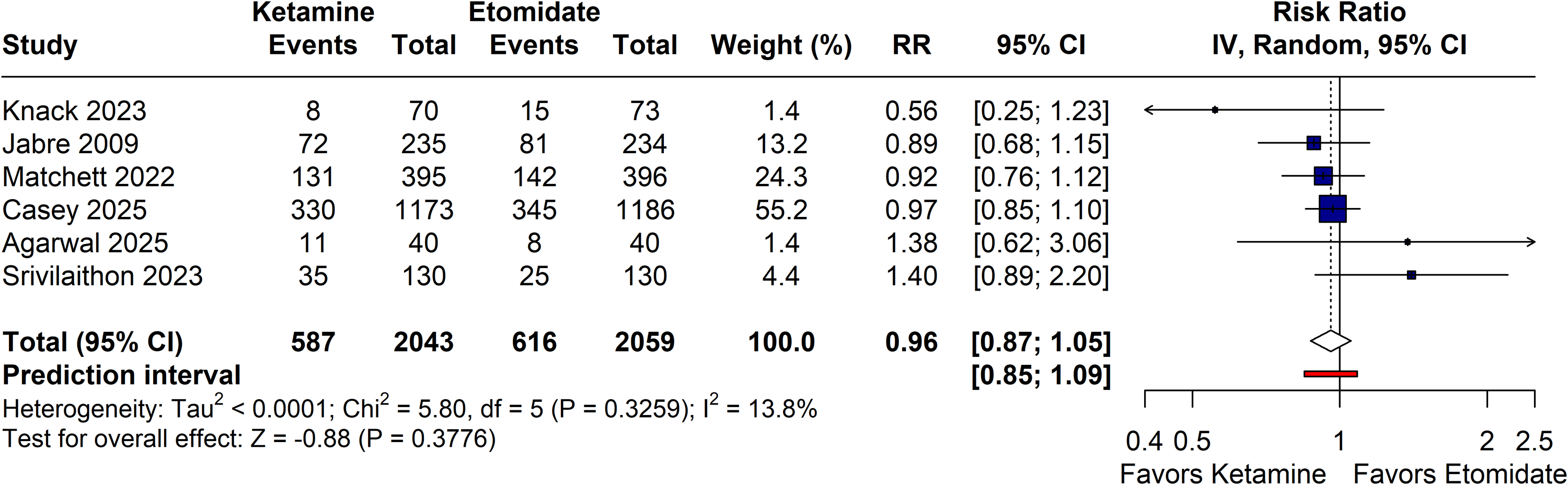
Forest plot comparing 28-day all-cause mortality of rapid sequence intubation using ketamine versus etomidate. Abbreviations: CI, confidence interval; IV, inverse variance; RR, risk ratio.
For secondary outcomes, ketamine was associated with a higher risk of post-intubation hypotension (RR 1.25; 95% CI, 1.01 to 1.53; I2 = 0%) and a lower risk of adrenal suppression (RR 0.36; 95% CI, 0.17 to 0.75; I2 = 0%) compared to etomidate. These hemodynamic and endocrine differences did not translate into a significant difference in the incidence of peri-intubation cardiac arrest (RR 1.13; 95% CI, 0.71 to 1.81; I2 = 0%). Procedural efficacy, measured by first-attempt intubation success, was also similar between groups (RR 0.99; 95% CI, 0.97 to 1.02; I2 = 0%) (Figure 3).
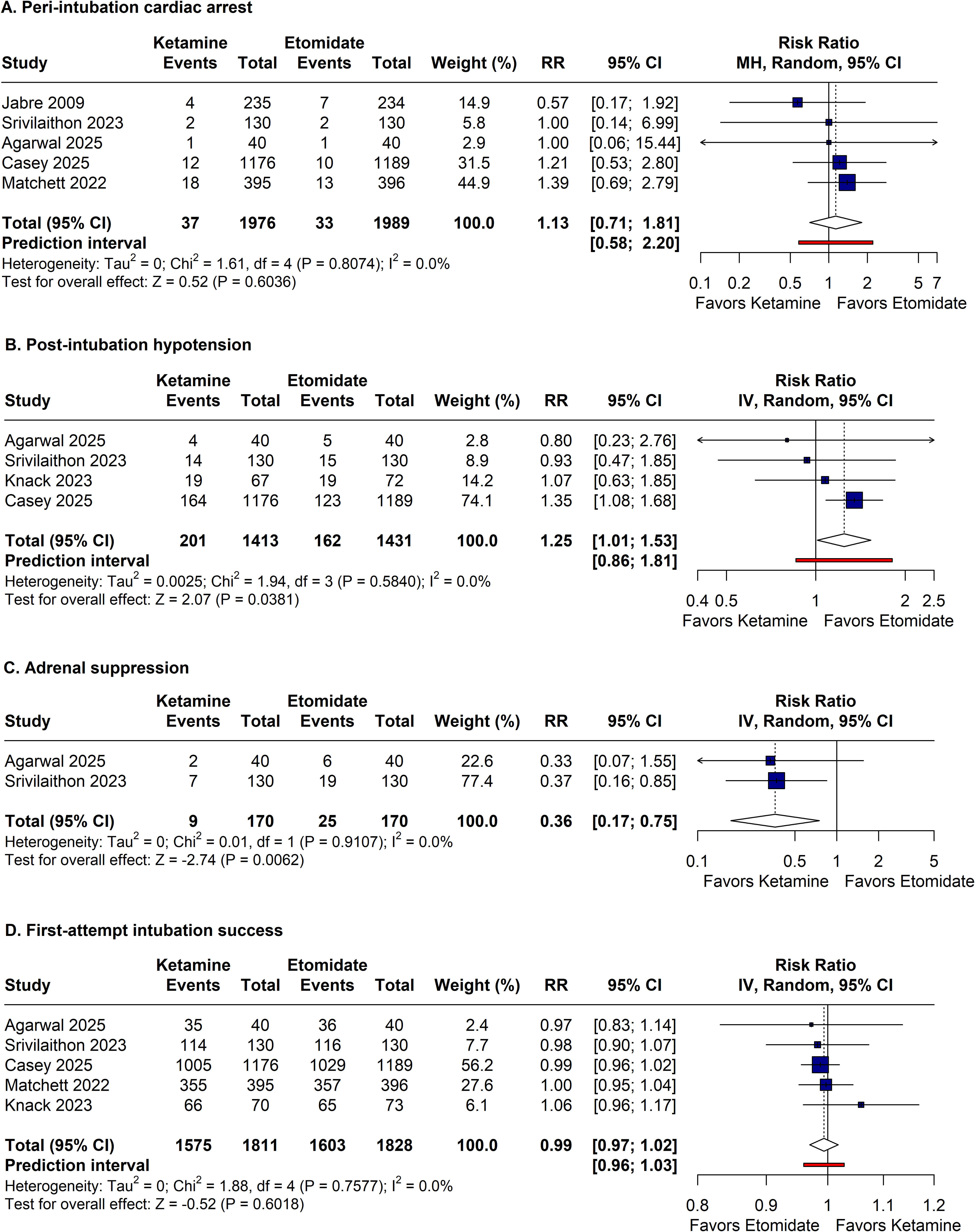
Forest plots comparing procedural efficacy and peri-intubation adverse events of rapid sequence intubation using ketamine versus etomidate. The panels illustrate the pooled effect estimates for (A) peri-intubation cardiac arrest, (B) post-intubation hypotension, (C) adrenal suppression, and (D) first-attempt intubation success. Abbreviations: CI, confidence interval; IV, inverse variance; MH, mantel-haenszel; RR, risk ratio.
Furthermore, no differences were observed in resource utilization outcomes, including ICU-free days (Mean Difference [MD] −0.3 days; 95% CI, −1.5 to 0.9) and mechanical ventilation-free days (MD −0.3 days; 95% CI, −0.9 to 0.3) (Supplemental Material, eFigure 8).
Subanalyses in Selected Populations
Subgroup analysis revealed no difference in 28-day mortality between ketamine and etomidate for septic (n = 1546; 35.6% vs 33.9%; RR 1.04; 95% CI, 0.91 to 1.19) or non-septic patients (n = 1765; 21% vs 23.6%; RR 0.89; 95% CI, 0.75 to 1.06), with no interaction between sepsis status and treatment effect (P = 0.17; I2 = 0%) (Figure 4).
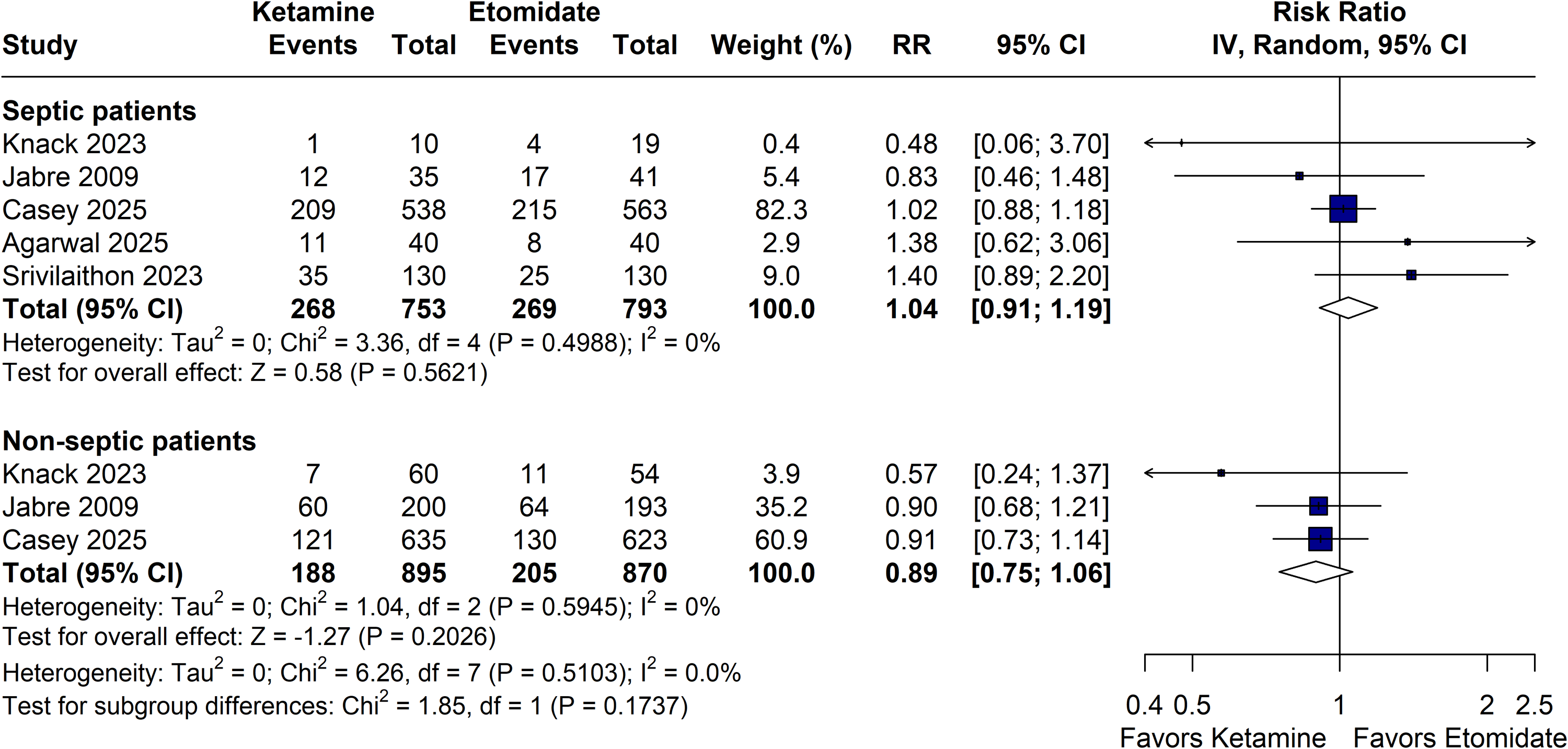
Subgroup analysis of 28-day mortality stratified by the presence of sepsis. Forest plots comparing the pooled effect estimates of rapid sequence intubation using ketamine versus etomidate in septic and non-septic patients. Abbreviations: CI, confidence interval; IV, inverse variance; RR, risk ratio.
Sensitivity analysis incorporating an unpublished trial (n = 398) did not alter post-intubation hypotension findings nor observed heterogeneity (n = 3242; 15.7% vs 12.2%; RR 1.29; 95% CI, 1.08 to 1.53; I2 = 0%) (Supplemental Material, eFigure 10). Conversely, including previously excluded trials with high risk of bias or indirectness for the adrenal suppression outcome substantially skewed the pooled estimate, although it yielded narrower confidence intervals (n = 1506; 10.5% vs 19.2%; RR 0.56; 95% CI, 0.46 to 0.67; I2 = 17.4%) (Supplemental Material, eFigure 9).
Quality Assessment
Assessment using the RoB-2 tool indicated that none of the included peer-reviewed trials were at high risk of bias for the primary outcomes (Supplemental Material, eFigures 1–7). The main sources of potential bias were the measurement of the outcome (Domain 4) due to the lack of blinding in open-label designs—mitigated by the objective nature of the endpoints—and the selection of the reported result (Domain 5) in Srivilaithon et al 30 and Agarwal et al 31 due to the absence of prospective protocol registration—concerns deemed mitigated by the high consistency in endpoint reporting observed across all included trials. The unpublished trial (Powers et al) was classified as high risk arising from its quasi-randomized allocation method (Domain 1).
Finally, the certainty of evidence was evaluated using the GRADE framework. Evidence was rated as ‘high’ certainty for first-attempt intubation success. The 28-day mortality, septic subgroup 28-day mortality and resource utilization outcomes were downgraded to ‘moderate’ certainty due to imprecision and the need for mathematical approximations, respectively. Evidence for adverse events—post-intubation hypotension, peri-intubation cardiac arrest, and adrenal suppression—was rated as ‘low’ certainty, primarily driven by imprecision (fragile estimates or wide confidence intervals) and indirectness (varying endpoint definitions and the use of proxies) (Table 2).
Summary of Findings and Certainty of Evidence.
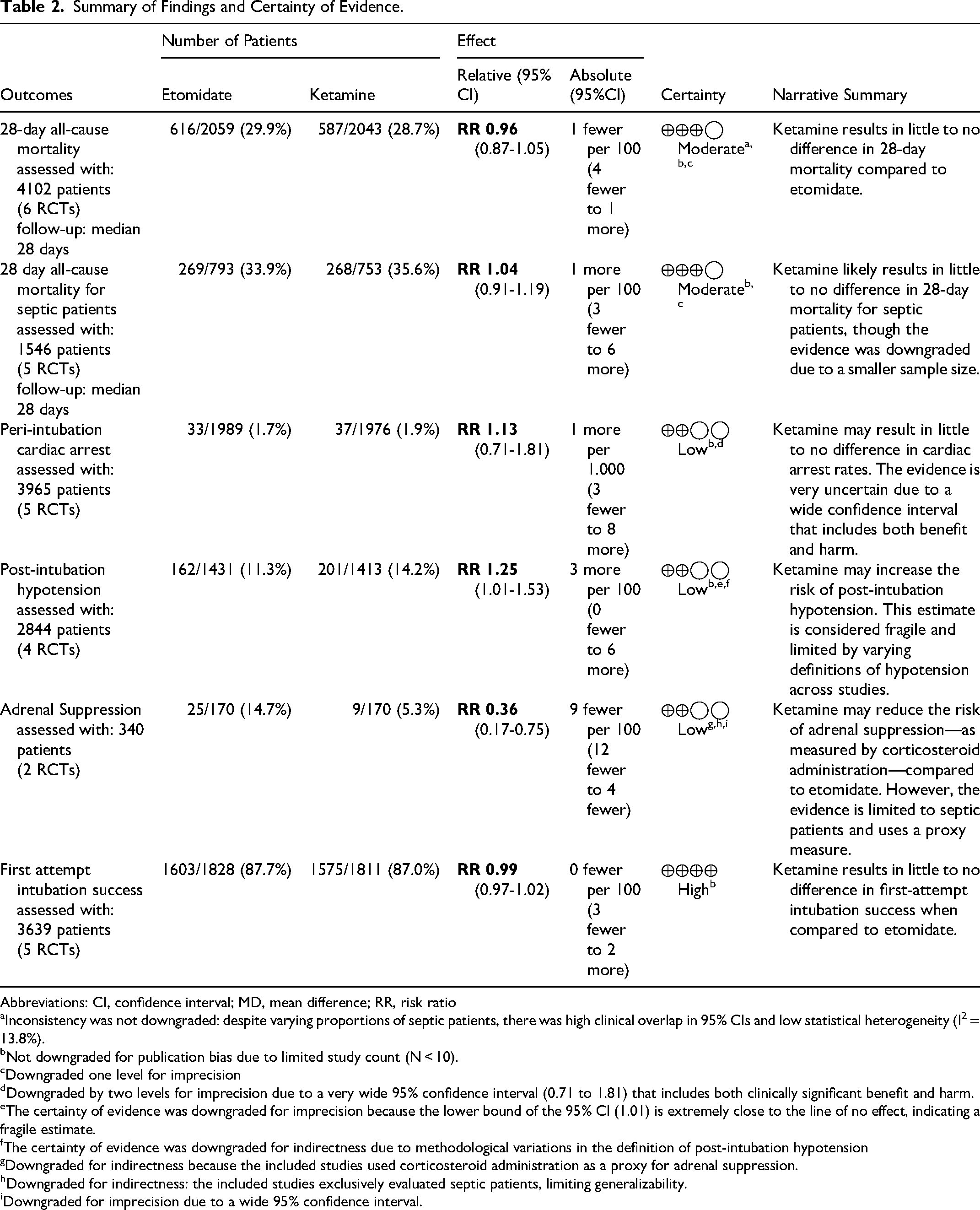
Abbreviations: CI, confidence interval; MD, mean difference; RR, risk ratio
Inconsistency was not downgraded: despite varying proportions of septic patients, there was high clinical overlap in 95% CIs and low statistical heterogeneity (I2 = 13.8%).
Not downgraded for publication bias due to limited study count (N < 10).
Downgraded one level for imprecision
Downgraded by two levels for imprecision due to a very wide 95% confidence interval (0.71 to 1.81) that includes both clinically significant benefit and harm.
The certainty of evidence was downgraded for imprecision because the lower bound of the 95% CI (1.01) is extremely close to the line of no effect, indicating a fragile estimate.
The certainty of evidence was downgraded for indirectness due to methodological variations in the definition of post-intubation hypotension
Downgraded for indirectness because the included studies used corticosteroid administration as a proxy for adrenal suppression.
Downgraded for indirectness: the included studies exclusively evaluated septic patients, limiting generalizability.
Downgraded for imprecision due to a wide 95% confidence interval.
Discussion
In this systematic review and meta-analysis of six randomized controlled trials involving 4108 critically ill adults undergoing RSI, we compared the efficacy and safety of etomidate versus ketamine. Our pooled analysis yielded several key findings: (a) no significant difference in 28-day all-cause mortality between patients induced with etomidate or ketamine, a finding that persisted in the subgroup analysis of patients with sepsis (moderate certainty); (b) ketamine induction was associated with a significant increase in the risk of post-intubation hypotension compared to etomidate (low certainty); (c) ketamine was associated with reduced incidence of adrenal suppression, as measured by corticosteroid administration (low certainty); and (d) no significant differences were observed regarding first-pass intubation success (high certainty), peri-intubation cardiac arrest (low certainty), or hospital resource utilization (moderate certainty).
Our mortality findings address a longstanding controversy regarding etomidate. By directly inhibiting adrenal mitochondrial 11β-hydroxylase, a single induction dose causes a transient ‘pharmacologic adrenalectomy’, impairing cortisol synthesis for up to 72 h. 33 This effect is particularly concerning in septic patients, who already face a high risk of relative adrenal insufficiency and rely heavily on endogenous cortisol to maintain vascular tone—explaining the frequent observation of increased delayed vasopressor requirements following etomidate administration. 34 However, previous meta-analyses evaluating this topic were limited by methodological confounders, including the pooling of observational data, 12 quasi-randomized trials (eg, Powers WF, ClinicalTrials.gov NCT03545503), and studies evaluating sedative combinations rather than pure agents, such as the co-administration of midazolam with ketamine (eg, Cinar et al 17 and Punt et al 18 ) in the main analysis. 16 Driven by high-quality data from recent large-scale RCTs, our analysis provides robust evidence that this transient endocrine suppression does not translate into higher 28-day mortality.
The discrepancy between our randomized findings and previous observational data regarding mortality is primarily driven by selection bias and confounding by indication. Because etomidate preserves immediate blood pressure, clinicians have preferentially administered it to the most hemodynamically unstable patients, falsely attributing the higher baseline mortality of this cohort to the drug itself.10,13 Additionally, non-randomized studies cannot adequately adjust for critical unmeasured confounders in sepsis management—such as the timeliness of antibiotic administration, adequacy of fluid resuscitation, and end-of-life care decisions—, inherently compromising prior meta-analyses that pooled such data. While individual trials demonstrate that etomidate-induced adrenal suppression increases delayed vasopressor requirements,30,31 our pooled results confirm this transient biochemical effect does not translate into higher short-term mortality.
Regarding hemodynamic stability, our findings reveal a critical temporal dichotomy between the two agents. Ketamine induction was associated with a higher risk of immediate post-intubation hypotension, challenging its perceived early safety profile. Although ketamine is increasingly favored for its indirect sympathomimetic effects—which theoretically increase blood pressure and heart rate—it also acts as a direct myocardial depressant and vasodilator. In critically ill patients with profound shock and depleted endogenous catecholamine reserves, this indirect support often fails, unmasking ketamine's direct negative inotropic effects.14,35 This “catecholamine depletion” mechanism explains the higher risk of immediate periprocedural cardiovascular collapse observed in our pooled results, aligning with recent large-scale RCTs 22 and observational registry data.13,36
Conversely, while etomidate effectively preserves hemodynamic stability during the immediate minutes following intubation, its endocrine penalty manifests as delayed cardiovascular instability. Recent sepsis-specific RCTs consistently demonstrate that patients receiving etomidate require significantly more continuous vasopressor support within the first 24 h post-intubation compared to those receiving ketamine.30,31 This is further corroborated by recent meta-analytic data indicating that ketamine use significantly reduces the need for the initiation of continuous infusion vasopressors in the ICU. 16 Therefore, the clinical trade-off is stark: clinicians must weigh the immediate risk of peri-intubation cardiovascular collapse with ketamine against the delayed, prolonged vasopressor dependence associated with etomidate's pharmacological adrenalectomy.
These nuanced hemodynamic profiles carry significant implications for personalized airway management. Since our analysis confirms no overall or sepsis-specific 28-day mortality difference, the selection of an induction agent should shift from a rigid protocol to an individualized approach based on the patient's immediate physiological phenotype. Ketamine may be the optimal choice for patients who are relatively hemodynamically stable at the time of intubation, minimizing downstream adrenal suppression. In contrast, etomidate remains highly valuable for patients presenting with profound, acute hemodynamic instability or refractory shock, where surviving the immediate peri-intubation period supersedes the delayed risk of prolonged vasopressor use.16,22
Considering the respective hemodynamic and endocrine limitations of ketamine and etomidate revealed by our findings, future research should explore alternative pharmacological strategies to mitigate these risks. For instance, the theoretical advantage of combining agents with opposing hemodynamic profiles, such as ketamine and propofol (ketofol), has gained traction. The KEEP PACE trial evaluated a reduced-dose ketamine/propofol admixture versus etomidate in critically ill adults and observed no significant differences in post-intubation blood pressure or vasopressor requirements. 37 Similarly, the use of adjuvants to offset specific adverse effects—such as co-administering low-dose midazolam with ketamine—represents another viable customized regimen. A prospective trial by Punt et al comparing etomidate to S-ketamine combined with midazolam for intensive care intubations reported no significant differences in 28-day mortality (38% vs 39%), duration of norepinephrine support, or length of stay, corroborating that ketamine-based combinations can yield comparable clinical outcomes. 18 Additionally, the individualization of induction agents must heavily weigh patient age and cardiovascular reserve; some evidence suggests that the negative inotropic properties and sympathomimetic failure of ketamine may precipitate myocardial ischemia and severe hypotension particularly in elderly patients.38,39 Therefore, future large-scale trials should not only focus on single-agent comparisons but also evaluate customized dosing regimens and admixtures in high-risk demographic subgroups.
Limitations
Despite the robustness of our findings, this study has limitations that should be contextualized in two domains: limitations inherent to the included primary literature and methodological limitations of our meta-analysis.
Regarding the included primary trials, four main limitations exist. First, definitions of post-intubation hypotension varied; however, the lack of statistical heterogeneity (I2 = 0%) indicates a highly consistent biological signal. Second, the open-label design of the largest trials introduces potential performance bias in periprocedural management, although our primary endpoint of 28-day mortality is highly resistant to such bias. Third, due to high risk of bias and indirectness in assessing adrenal suppression, we restricted our pooled estimate strictly to trials utilizing objective short-term proxies, with full rationale provided in the Supplemental Digital Content. Fourth, while variations in dosing protocols may increase clinical heterogeneity and subsequent imprecision, they accurately reflect daily clinical practice, thereby improving the external validity of our results.
Regarding methodological limitations, two points warrant discussion. First, the small number of trials (N < 10) prevented formal publication bias testing. 40 Mitigating this risk of missing evidence, our sensitivity analysis incorporating an unpublished trial (Powers WF, ClinicalTrials.gov NCT03545503) did not alter the post-intubation hypotension findings, reinforcing our conclusions’ robustness. Second, several secondary estimates were downgraded to ‘moderate’ or ‘low’ certainty within the GRADE framework due to imprecision and indirectness, highlighting the need for larger pooled cohorts to achieve definitive clinical certainty.
Conclusion
In this meta-analysis of randomized controlled trials involving critically ill adults, 28-day mortality did not differ between etomidate and ketamine for emergency intubation in critically ill adults, including septic patients. Conversely, ketamine was associated with a higher risk of post-intubation hypotension, while etomidate was associated with greater adrenal suppression, emphasizing that the choice of induction agent must be highly individualized.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261460825 - Supplemental material for Etomidate Versus Ketamine for Emergency Intubation in Critically Ill Patients: An Updated Meta-Analysis and Systematic Review
Supplemental material, sj-docx-1-jic-10.1177_08850666261460825 for Etomidate Versus Ketamine for Emergency Intubation in Critically Ill Patients: An Updated Meta-Analysis and Systematic Review by Vítor H. Andriazzi, Renato P. Curcio, Michael A. R. A. Novais, Bernardo L. G. Fernandes, Giovana C. Rosa, Juan G. S. Vasconcelos and Juliano N. Quineper in Journal of Intensive Care Medicine
Footnotes
ORCID iDs
Author Contributions
V. H. A.: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Project Administration, Writing – Original Draft, and Writing – Review & Editing (participated in all stages of the project as the first author).
R. P. C.: Investigation (responsible for screening and study selection) and Methodology (participated in the selection of outcomes of interest).
B. L. G. F.: Data Curation (data extraction of outcomes), Formal Analysis, Methodology (helped define methodological issues), and Writing – Review & Editing.
J. G. S. V.: Validation (reviewed extracted data for ![]() and reviewed the PRISMA checklist) and Investigation (full paper availability and retrieval).
and reviewed the PRISMA checklist) and Investigation (full paper availability and retrieval).
M. A. R. A. N.: Data Curation (data extraction for ![]() ) and Project Administration (contact and partnership establishment with the senior author).
) and Project Administration (contact and partnership establishment with the senior author).
G. C. R.: Writing – Review & Editing (final review of the manuscript) and Visualization (preparation of the 280-character summary for social media).
J. N. Q.: Supervision and Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Preprint Deposit
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.