
Abstract
Objective
Although dexmedetomidine (DEX) is commonly used in sepsis management, its effect on prognosis in patients with concomitant heart failure (HF) remains controversial. This study aims to examine the association between DEX use and 30-day mortality in this population.
Methods
This retrospective cohort study identified patients meeting Sepsis-3.0 criteria with comorbid HF from the MIMIC-IV database. Subjects were stratified into DEX and non-DEX groups according to intensive care unit (ICU) medication records. Propensity score matching (PSM) was applied to balance baseline characteristics and reduce confounding. Primary and secondary outcomes were 30-day and 90-day mortality, respectively. Logistic regression and Kaplan-Meier analyses were used to assess the association of DEX use, dosage, and administration duration with patient prognosis.
Results
After PSM, 1331 patients were divided into a DEX group and a non-DEX group, with balanced baseline characteristics. Multivariable-adjusted logistic regression showed that no association was observed between DEX use and 30-day mortality (OR = 0.861, 95% CI: 0.702-1.056, P = .151). However, DEX administration within the first 24 h was associated with a lower 30-day mortality rate (OR = 0.742, 95% CI: 0.588-0.932, P = .011). A low dose of DEX (<399.983mcg) was associated with a lower 30-day mortality rate (OR = 0.697, 95% CI: 0.527-0.913, P = .010), whereas no association was noted for a medium dose (399.983-2472.306mcg) or a high dose (>2472.306mcg).
Conclusion
In this cohort, DEX use was not associated with a lowered 30-day or 90-day mortality rate among patients with sepsis and concomitant HF. Nevertheless, shorter exposure to DEX (in terms of dose and duration) may be associated with ameliorated outcomes.
Introduction
Sepsis is a critical disease resulting from a dysregulated host response to infection, leading to life-threatening organ dysfunction. 1 Globally, an estimated 48.9 million cases of sepsis occur annually, contributing to 11 million deaths, which account for nearly 20% of all mortalities worldwide. 2
In clinical practice, patients with sepsis complicated by heart failure (HF) are frequently encountered and are associated with an extremely high mortality rate. 3 A pathophysiological vicious cycle exists among patients with sepsis and concomitant HF, in which the inflammation storm 4 and vasoplegia 5 associated with sepsis exacerbate HF and further lead to hemodynamic instability. Consequently, these patients frequently require mechanical ventilation and sedation. However, traditional sedatives carry considerable risks due to their side effects on vasodilation and myocardial depression. 6 Therefore, it is of vital importance to identify a sedation strategy that minimizes hemodynamic compromise or even is protective for the heart.
Dexmedetomidine (DEX), a highly selective α-2 adrenergic receptor agonist, has garnered widespread attention for its unique property of providing mild sedation along with potential anti-inflammatory and organ-protective effects.7–9 A study has shown that DEX increases the survival rate of myocardial cells, reduces myocardial injury, promotes energy metabolism, and regulates autophagy, indicating potential cardioprotective effects. 10
Nevertheless, the administration of DEX in patients with sepsis and concomitant HF remains highly controversial. Although some research suggests that DEX use may improve prognosis through antisympathetic effects, 11 its known side effects, such as bradycardia and hypotension, may be critically detrimental to patients with compromised cardiac functional reserve. 12 Current evidence is mainly derived from studies on the general population with sepsis or perioperative patients, leaving a knowledge gap regarding the high-risk subgroup of ‘sepsis complicated by HF’. Furthermore, the impact of the dose, infusion rate, and timing of administration of DEX on long-term survival among such patients remains largely unexplored.
For the purpose of addressing this clinical uncertainty, this study is performed based on the Medical Information Mart for Intensive Care IV (MIMIC-IV) database to assess the association between DEX use and all-cause mortality rate within 30 days among critically ill patients with sepsis complicated by HF. Moreover, the aim is to explore whether a therapeutic window for survival benefit exists regarding the administration duration, cumulative dose, and infusion rate of DEX in association with a 30-day mortality rate. It is hypothesized that, among ICU patients with sepsis and concomitant HF, appropriate administration of DEX is independently associated with ameliorated survival outcomes compared with non-use of DEX.
Methods and Materials
Data Source
This retrospective cohort study covered a period from 2008 to 2022. This study was based on a publicly available, de-identified database; therefore, patient data complied with the Safe Harbor standards of the U.S. Health Insurance Portability and Accountability Act (HIPAA). Since patient identifiers were replaced with random codes and all timestamps were uniformly shifted, the requirement for ethical approval and individual informed consent was waived.
Details of the MIMIC-IV Database
The newly released MIMIC-IV (version 3.1) dataset was utilized in this study (accessible via PhysioNet at https://physionet.org/content/mimiciv/3.1/). This database originates from the emergency department and intensive care units (ICUs) of Beth Israel Deaconess Medical Center in Boston, Massachusetts, USA. The MIMIC-IV database adopts a modular structure (including the hosp and icu modules) to separately record hospital-level and ICU-level information. The database encompasses clinical data from 364 627 patients, involving 546 028 hospital admissions and 94 458 ICU stays in total. Prior to data extraction, the first author completed the Collaborative Institutional Training Initiative (CITI) program and passed the exams on ‘Conflict of Interest’ and ‘Research Involving Data or Specimens Only’ (ID: 68 611 044).
Study Population and Definitions
In this study, sepsis was defined according to the Sepsis-3.0 diagnostic criteria, which required the presence of suspected infection accompanied by organ dysfunction (defined as a Sequential Organ Failure Assessment [SOFA] score of ≥ 2). The diagnosis of HF was identified based on the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes, 13 encompassing all patients with these codes regardless of whether HF was a pre-existing condition at admission, a new diagnosis established during hospitalization, or documented at discharge. Ultimately, a total of 9556 patients diagnosed with sepsis complicated by HF were included.
The inclusion criteria were: (1) patients aged 18 years or above; (2) patients meeting the Sepsis-3.0 diagnostic criteria; (3) individuals diagnosed with HF.
The exclusion criteria were: (1) patients with abnormal data (such as negative survival time); (2) patients with a length of ICU stay ≤ 24 h. Ultimately, 8507 patients were included, and all laboratory indicators were derived from the first test within 24 h of admission to the ICU.
Data Extraction
In this study, pgAdmin4 PostgreSQL 17 (version 4.1) was utilized for data extraction from MIMIC-IV. The extracted variables comprised demographic characteristics (sex, age, and race), vital signs (respiratory rate, heart rate, oxygen saturation, diastolic blood pressure, systolic blood pressure, and temperature), comorbidities (diabetes mellitus, atrial fibrillation, cirrhosis, hypertension, chronic kidney disease, and chronic lung disease), laboratory tests (red blood cells, white blood cells, creatinine, lactate, sodium, platelets, potassium, blood urea nitrogen, and fasting blood glucose), scores (SAPSII, SOFA, and GCS), and treatment regimens (aspirin, angiotensin-converting enzyme inhibitors (ACEIs), fibrates, β-blockers, vasopressors, CRRT, and IMV).
Definition of Independent Variables
To assess the impact of the characteristics of DEX use on clinical outcomes, patients were categorized based on both administration duration and cumulative dose. For the analysis based on the duration of DEX administration, patients were divided into the following four groups: Group Q1 (non-exposed group), consisting of patients who did not receive DEX; Group Q2, comprising patients who received DEX for 0–24 h; Group Q3, consisting of patients who received DEX for 24–72 h; and Group Q4, comprising patients who received DEX for more than 72 h. The cutoff points of 24 h and 72 h for this categorization were selected based on specific rationales. Specifically, the former was chosen considering the potential risk of withdrawal effects associated with prolonged DEX administration, as highlighted in previous literature. 14 The latter was selected because it represents a critical time window for the clinical evolution and mortality risk among patients with septic shock. 15
For the analysis based on cumulative dose, to analyze the influence of DEX dose on clinical outcomes, all patients who were exposed to DEX were stratified into three dose levels (low, medium, and high) according to the tertiles of their cumulative dose of DEX. The specific groupings were defined as follows: Group G1 (non-exposed group), comprising patients who did not receive DEX; Group G2 (low-dose group), consisting of patients with a cumulative dose below 399.983mcg; Group G3 (medium-dose group), comprising patients with a cumulative dose ranging from 399.983mcg to 2472.306mcg; and Group G4 (high-dose group), consisting of patients with a cumulative dose exceeding 2472.306mcg.
For the analysis based on the average administration rate, all DEX-exposed patients were divided into three rate categories according to the tertiles of the weight-adjusted dose (μg/kg/h). The resulting groups were defined as follows: Group R1 (non-exposed): patients who did not receive DEX; Group R2 (low rate): average rate 0–0.488mcg/kg/h; Group R3 (medium rate): average rate 0.488–0.753mcg/kg/h; and Group R4 (high rate): average rate >0.753mcg/kg/h.
Several variables were derived or aggregated prior to analysis, with all data strictly extracted from the patient's first ICU admission. The weight-adjusted average infusion rate of DEX during this initial ICU stay was calculated by dividing the total cumulative dose by the patient's admission body weight and the duration of administration. For continuous physiological parameters (eg, hemodynamics) and laboratory tests with multiple measurements, the first recorded values within the initial 24 h following the first ICU admission were extracted. Clinical severity scores (SAPSII, SOFA, and GCS) were computed using the worst physiological parameters during this 24 h window. Baseline comorbidities were defined as binary variables (present or absent) based on medical records at the time of the first ICU admission. Length of ICU stay for the entire cohort was defined as the time from ICU admission to discharge or death.
Outcomes
The primary outcome indicator was 30-day mortality rate, and the secondary outcome was 90-day mortality rate.
Statistical Analysis
Participants were divided into two groups according to DEX exposure: those who received DEX treatment (DEX group) and those who did not (non-DEX group). All continuous variables were first tested for normality using the Kolmogorov-Smirnov test or the Shapiro-Wilk test. Given the non-normal distribution of the data, continuous variables were presented as medians with interquartile ranges (IQRs), and comparisons between groups were performed using the Wilcoxon rank-sum test. Categorical variables were expressed as counts and percentages, and comparisons between groups were conducted using Fisher's exact test or the Chi-squared test, as appropriate.
To adjust for marked baseline differences, propensity score matching (PSM) was performed using a 1:1 nearest neighbor matching algorithm with a caliper width of 0.2. For the primary outcome, Kaplan-Meier survival curves were generated, and comparisons between groups were performed using the log-rank test to assess the effect of DEX administration on survival time at 30 days and 90 days among patients with sepsis and concomitant HF.
Prior to logistic regression analysis, multicollinearity among the independent variables was assessed using the variance inflation factor to ensure model stability and reliability. Multivariable logistic regression was then performed to evaluate the associations of the use, administration duration, and dose of DEX with adverse outcomes among individuals with sepsis complicated by HF. Odds ratios (ORs) alongside 95% confidence intervals (CIs) were calculated. The non-DEX group was treated as the control, and unadjusted and progressively adjusted multivariable logistic regression models were constructed. To verify the robustness of the results, sensitivity analyses were performed based on a multivariable Cox regression to assess the association of DEX use with 30-day mortality rate and 90-day mortality rate. The results are detailed in Supplemental Materials 7 and 8.
Model I was unadjusted. Model II was adjusted for sex and age. Model III, constructed on Model II, was further adjusted for race, heart rate, non-invasive diastolic blood pressure, non-invasive systolic blood pressure, oxygen saturation, body temperature, respiratory rate, liver cirrhosis, diabetes mellitus, hypertension, chronic lung disease, atrial fibrillation, chronic kidney disease, red blood cells, serum creatinine, white blood cells, sodium, potassium, blood urea nitrogen, lactate, fasting blood glucose, platelets, SOFA, SAPSII, GCS, continuous renal replacement therapy, aspirin, vasopressin, fibrates, β-blockers, and ACEIs.
Subgroup analyses were performed to examine whether demographic characteristics, laboratory tests, comorbidities, or other relevant factors modified the association of DEX use, duration of use, and dose with mortality. All statistical analyses were conducted using R (version 4.5.0). A two-sided P < .05 was indicative of statistical significance.
Results
Characteristics of Participants
In total, 27 882 records of patients with sepsis were initially extracted from the MIMIC-IV database. According to the exclusion criteria, 8426 patients were ultimately included, comprising 1342 patients in the DEX group and 7084 patients in the non-DEX group (Figure 1).
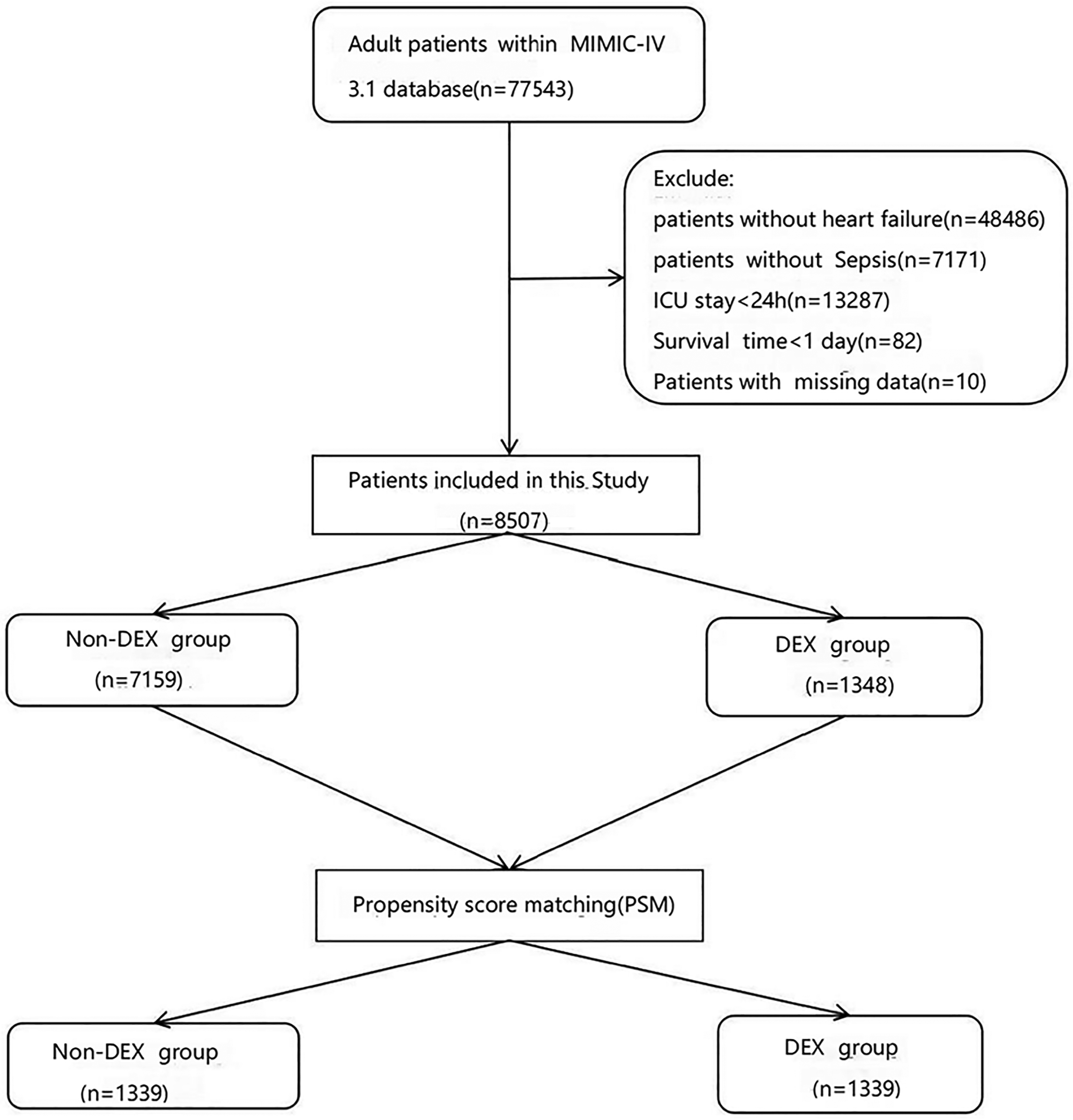
Flowchart for participant selection. ICU: intensive care unit; MIMIC: Medical Information Mart for Intensive Care.
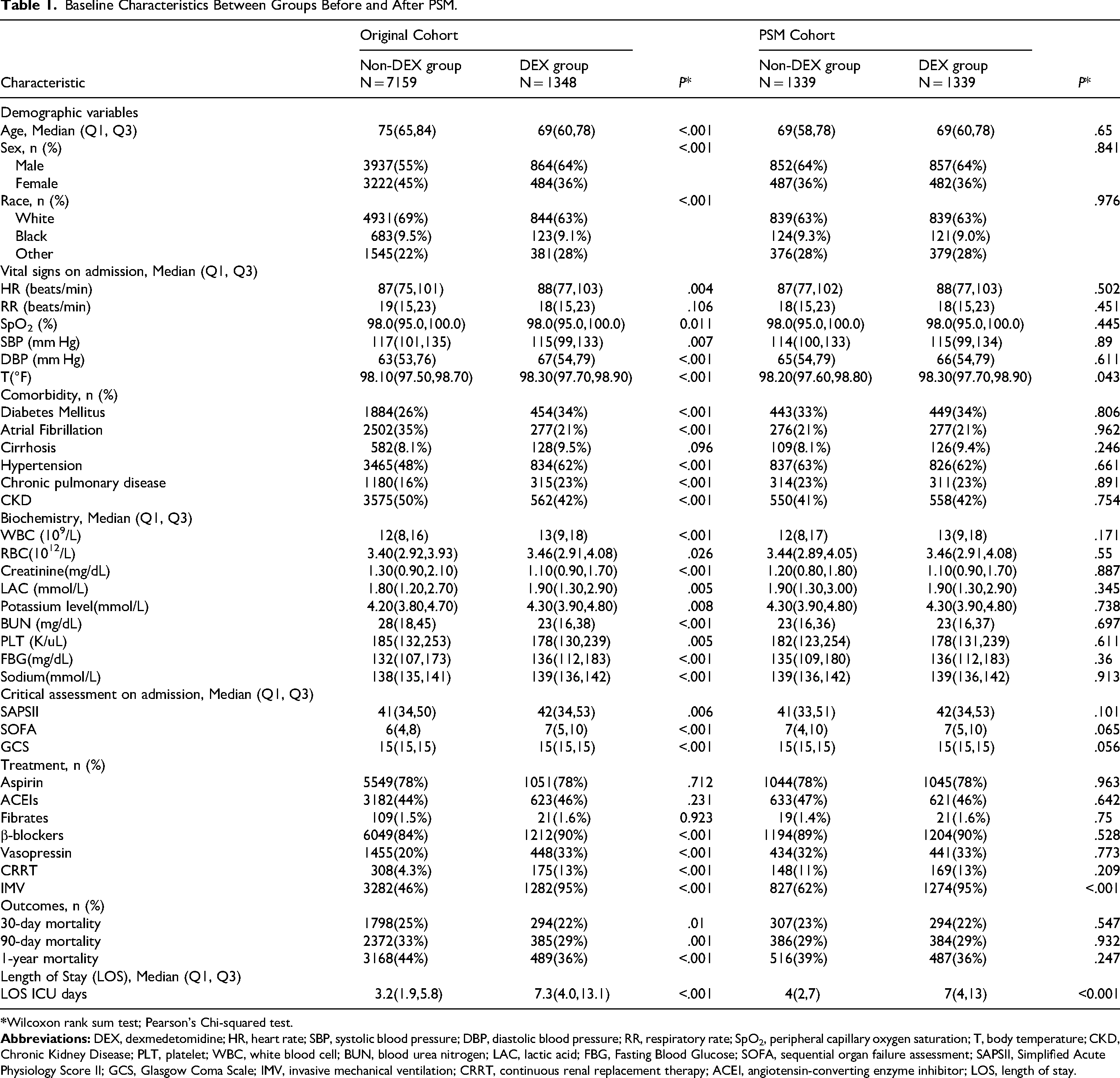
Regarding demographic characteristics, patients in the DEX group were found to be significantly younger than those in the non-DEX group, with median ages of 69 (60-78) years and 75 (65-84) years, respectively. Furthermore, a significantly higher proportion of male patients was observed in the DEX group (64%) compared with the non-DEX group (55%).
In the original cohort, marked differences were observed between the DEX group and the non-DEX group across numerous baseline characteristics and treatment measures (P < .05). These included age, sex, race, heart rate, SpO₂, systolic blood pressure, diastolic blood pressure, body temperature, diabetes mellitus, atrial fibrillation, hypertension, chronic lung disease, chronic kidney disease, white blood cell count, red blood cell count, creatinine, lactate, potassium, blood urea nitrogen, platelet count, fasting blood glucose, sodium, SAPSII score, GCS score, β-blocker use, vasopressin use, CRRT, and IMV. No statistically significant differences were found between the groups regarding respiratory rate, liver cirrhosis, or aspirin use, ACEIs, or fibrates (P > .05).
For outcome indicators, significantly lower short-term and long-term all-cause mortality rates were observed in the DEX group compared with the non-DEX group. Specifically, these included 30-day mortality rate (22% in the DEX group vs 25% in the non-DEX group, P = .01), 90-day mortality rate (29% vs 33%, P = .001), and 1-year mortality rate (36% vs 44%, P < .001). Nevertheless, the length of ICU stay was significantly longer for patients in the DEX group in comparison with those in the non-DEX group [median: 7.3 (4.0, 13.1) days versus 3.2 (1.9, 5.8) days, P < .001].
After PSM, 1331 patients from the DEX group were successfully matched with 1331 patients from the non-DEX group. Following matching, the distribution of covariates between the two groups was more balanced, indicating a substantial reduction in covariate imbalance. Only body temperature (T) and IMV showed marked differences between the two groups (P < .05) (Table 1). Regarding the outcome indicators after PSM, the 30-day mortality rate was 289 (21.71%) in the DEX group and 314 (23.59%) in the non-DEX group, and the risk ratio (RR) was 0.920 (95% CI: 0.801-1.058). The 90-day mortality rate was 378 (28.4%) in the DEX group and 401 (30.13%) in the non-DEX group, with an RR of 0.943 (95% CI: 0.833-1.066). This suggested that after adjusting for confounding factors at baseline, no marked association was observed between DEX use and prolonged long-term survival.
Baseline Characteristics Between Groups Before and After PSM.
Kaplan-Meier Analysis
Following PSM, Kaplan-Meier survival analysis was performed. The overall survival curve for 30-day follow-up (Figure 2A, Log-rank P = .28) was not significantly separated between the non-DEX group and the DEX group.
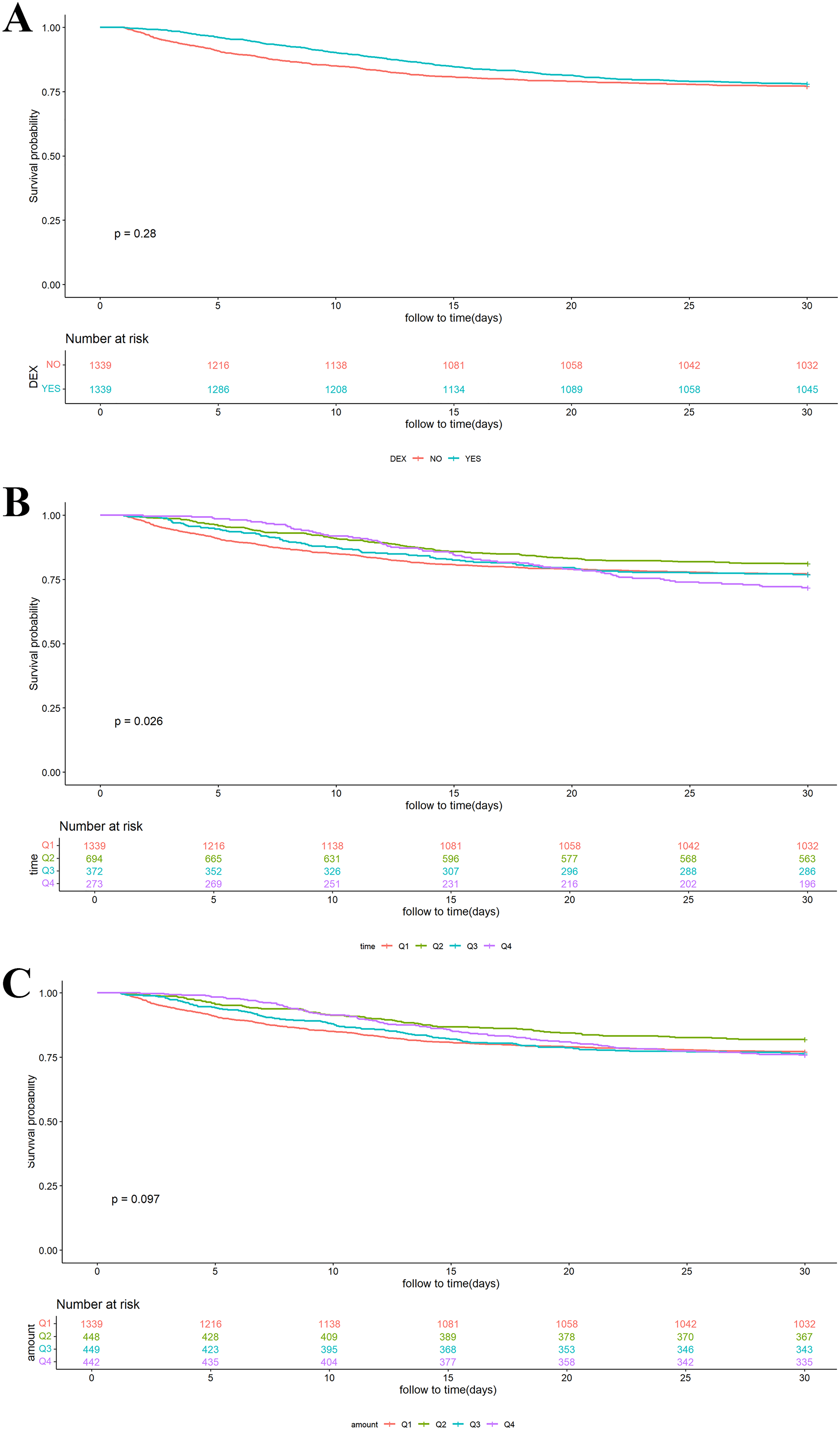
Kaplan-Meier curves for the DEX group and the non-DEX group (A) mortality rate within 30 days after PSM; (B) mortality rate within 30 days by duration of use after PSM; (C) mortality rate within 30 days by dose after PSM. Q1: Non-DEX group; Q2: 0-24 h group; Q3: 24-72 h group; Q4: >72 h group. G1: Non-DEX group; G2: <399.983mcg group; G3: 399.983-2472.306mcg group; G4: >2472.306mcg group.
However, a significant association was observed between the duration of DEX use and the survival rate of patients (Figure 2B, Log-rank P = .026). Specifically, the subgroup with a duration of 0-24 h (Q2) was the most effective regimen, with a cumulative 30-day mortality rate significantly lower compared with the other subgroups. In contrast, patients with a duration exceeding 72 h (Q4) were confronted with the highest cumulative 90-day mortality rate. The details are provided in Supplementary Figure 1.
Regarding the dose of DEX use, a trend toward separation was observed in the survival curve for 30-day follow-up; however, statistical significance was not reached (Figure 2C, Log-rank P = .097). In contrast, a marked difference was detected for the 90-day follow-up (Log-rank P < .05). In this analysis, a marked survival advantage was observed in the low-dose group (<399.983mcg) at 90 days, whereas no benefit was noted in the high-dose group (>2472.306mcg). The details are presented in Supplementary Figure 1
Relationship of DEX use with Mortality Rate
Following PSM, multivariable logistic regression models were performed to assess the association between DEX use and 30-day mortality rate (Table 2). The results indicated that in the unadjusted, partially adjusted, and fully adjusted models, no significant association was observed between DEX use and lowered 30-day mortality rate (unadjusted model: OR = 0.898, 95% CI: 0.749-1.077, P = .247; partially adjusted model: OR = 0.887, 95% CI: 0.735-1.070, P = .210; fully adjusted model: OR = 0.861, 95% CI: 0.702-1.056, P = .151).
Association Between DEX use and Mortality.
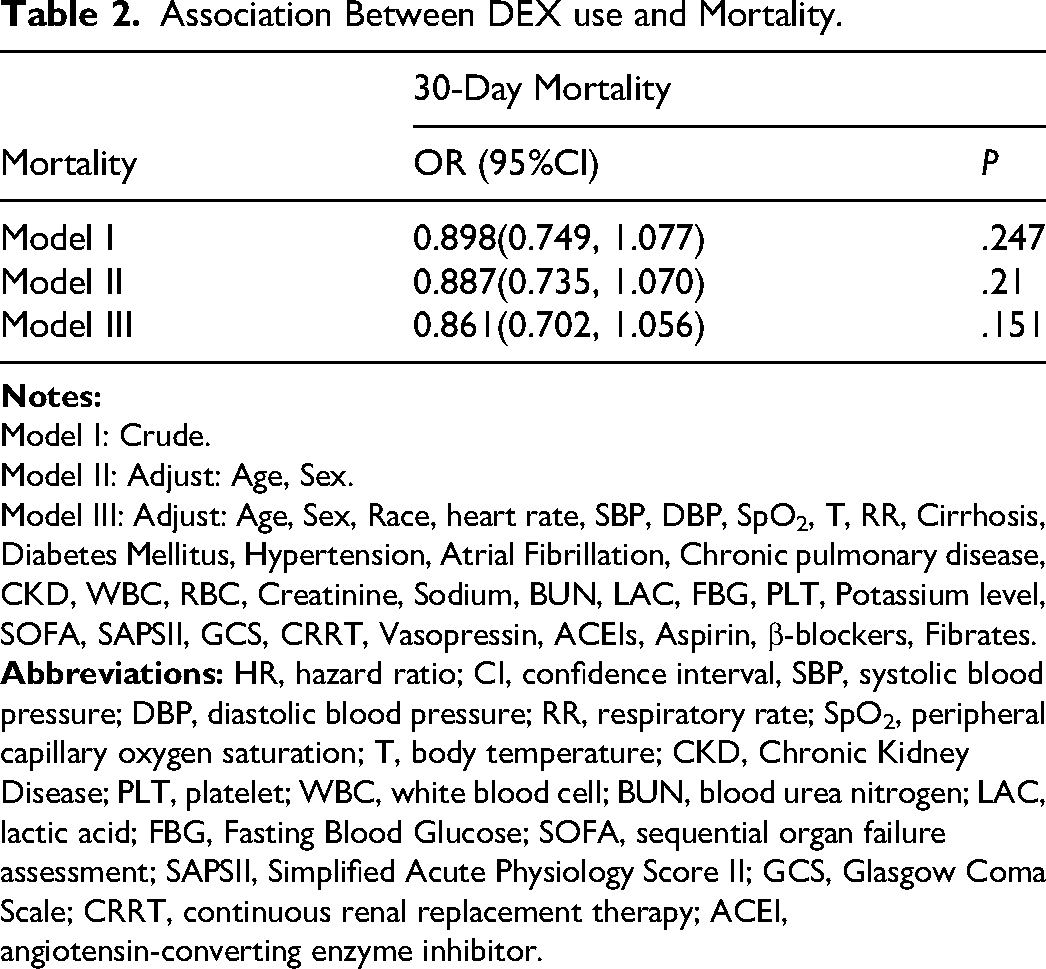
Model I: Crude.
Model II: Adjust: Age, Sex.
Model III: Adjust: Age, Sex, Race, heart rate, SBP, DBP, SpO2, T, RR, Cirrhosis, Diabetes Mellitus, Hypertension, Atrial Fibrillation, Chronic pulmonary disease, CKD, WBC, RBC, Creatinine, Sodium, BUN, LAC, FBG, PLT, Potassium level, SOFA, SAPSII, GCS, CRRT, Vasopressin, ACEIs, Aspirin, β-blockers, Fibrates.
Consistent findings were validated by the sensitivity analyses performed based on a multivariable Cox regression (Supplementary Table 1-2). The multivariable logistic regression prior to PSM is provided in Supplementary Table 3.
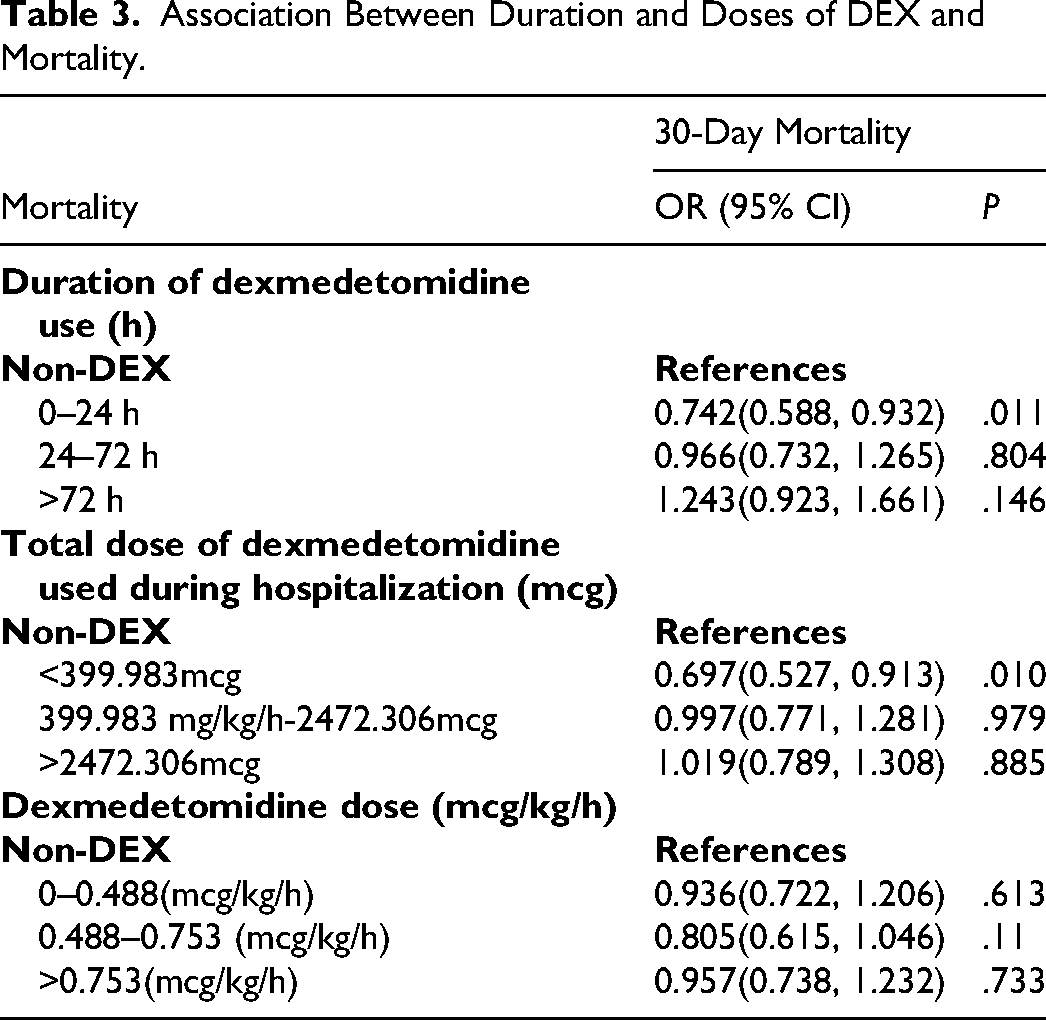
Association of Duration and Dosage of DEX use with All-Cause Mortality Rate
Regarding the duration of DEX use, short-term administration (0-24 h) was found to be associated with a survival benefit, with a 25.8% reduction in the risk of 30-day mortality rate compared with the non-DEX group (OR = 0.742, 95% CI: 0.588-0.932, P = .011). However, this protective effect was no longer observed when administration duration was extended to medium (24-72 h) or long-term (>72 h) use, with no statistically significant prolongation in survival noted.
Concerning the dose of DEX use, a marked reduction in 30-day mortality rate was observed exclusively in the low-dose group (<399.98mcg) (OR = 0.697, 95% CI: 0.527-0.913, P = .010). In contrast, no marked survival benefit was noted in either the medium-dose group (399.983-2472.306mcg) or the high-dose group (>2472.306mcg).
In the sensitivity analyses examining the effect of infusion rate, the infusion rate of DEX use was validated based on both multivariable logistic regression and Cox regression models. The results indicated that a moderate infusion rate (0.488-0.753mcg/kg/h) was significantly associated with a lowered 30-day mortality rate only in Model I before PSM (P < .05) (Supplementary Tables 4 and 5). However, in the analyses performed after PSM, the effect of infusion rate on 30-day mortality rate did not reach statistical significance (Table 3).
Association Between Duration and Doses of DEX and Mortality.
Subsequently, sensitivity analyses based on Cox regression models were performed to assess the associations of the duration, dose, and infusion rate of DEX use with 30-day and 90-day mortality rates. Similar trends were observed, as shown in Supplementary Tables 4–7.
Subgroup Analysis
To additionally investigate whether the association of DEX administration with all-cause mortality rates within 30 days and 90 days persisted across different subgroups, subgroup analyses were implemented. These analyses were stratified by sex, age, race, history of hypertension, diabetes mellitus, atrial fibrillation, cirrhosis, chronic kidney disease, chronic lung disease, use of β-blockers, use of vasopressors, and use of CRRT. Interaction results revealed differences in outcomes between subgroups with and without use of β-blockers (P for interaction <.05) (Figures 3-5). The results for all-cause mortality rate within 90 days are shown in Supplementary Figures 2-4.
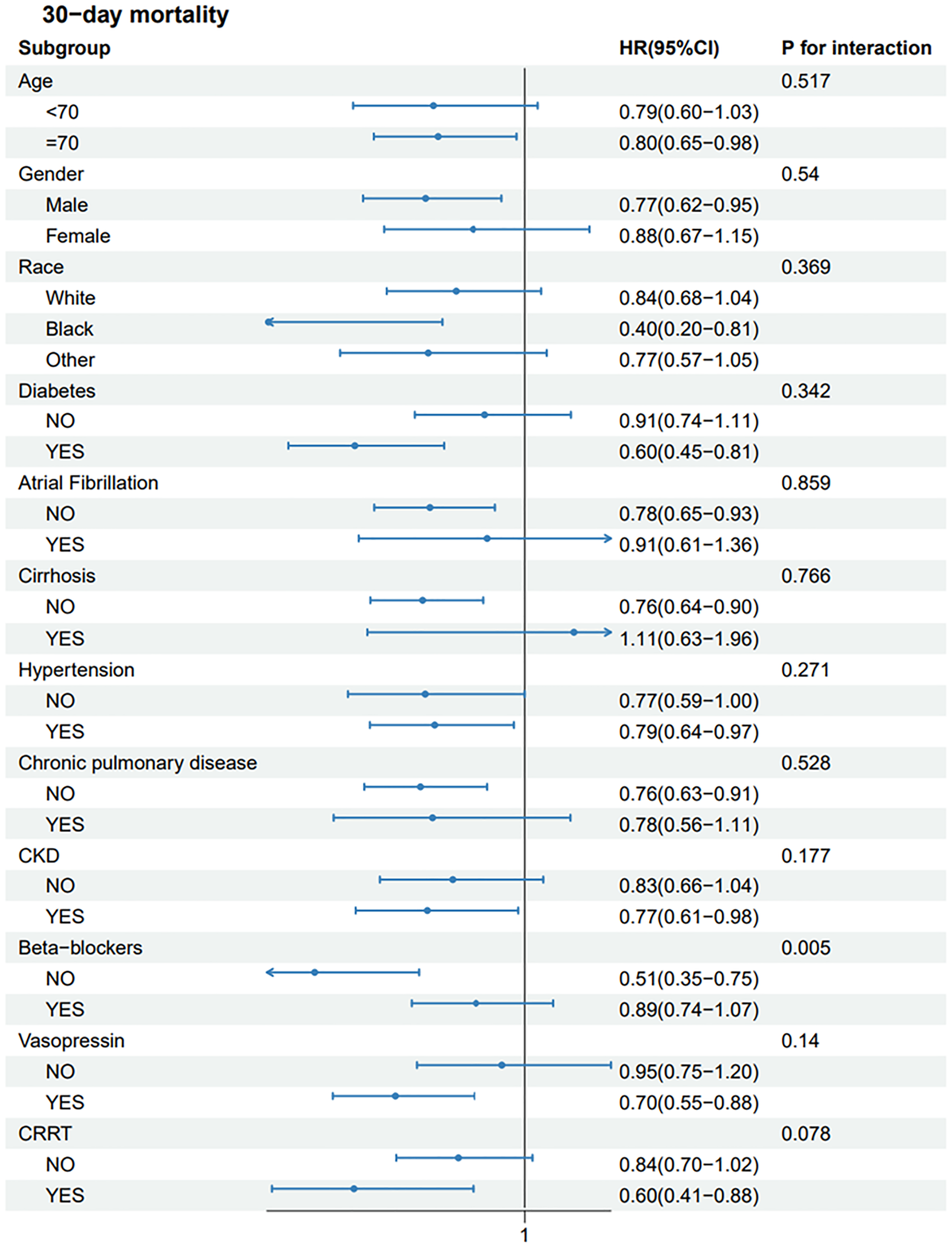
Association of DEX use with Mortality Rate within 30 days.
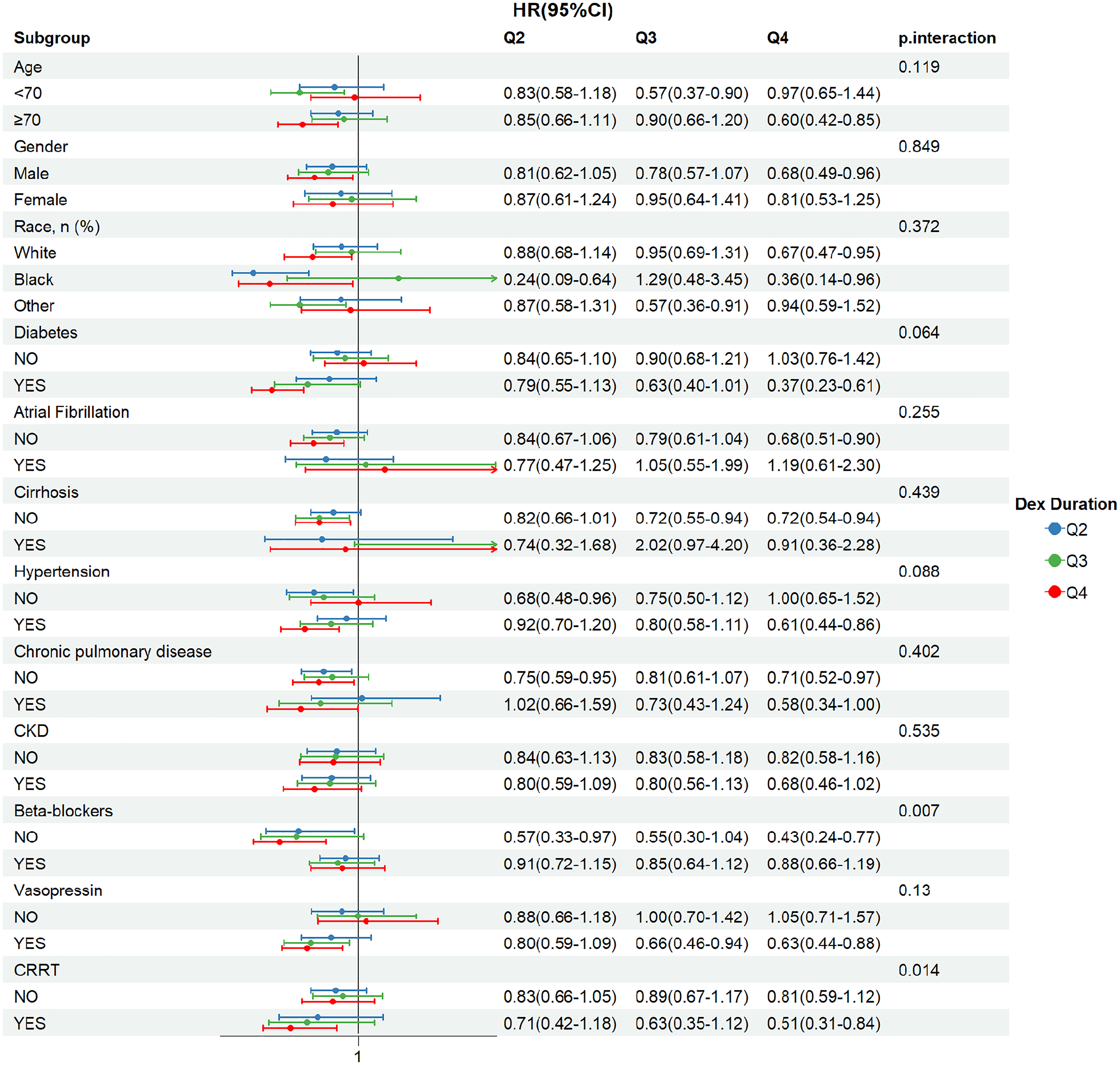
Association of DEX duration with Mortality Rate within 30 days.
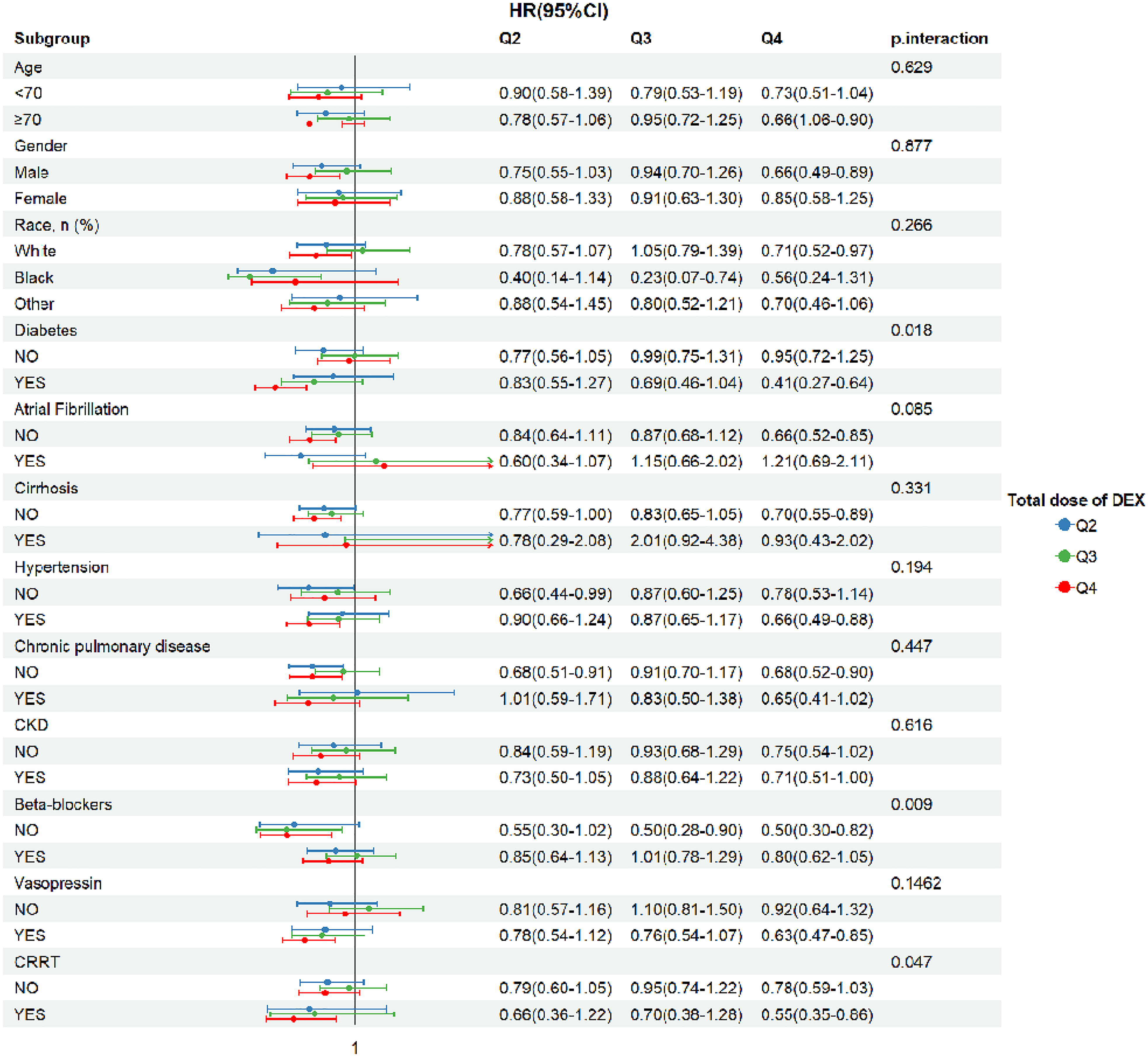
Association of DEX dose with Mortality Rate within 30 days.
Discussion
This study found that among ICU patients with sepsis complicated by HF, overall DEX administration was not associated with 30-day mortality. No survival benefit was observed across multivariable logistic regression and post-PSM survival analyses. However, the secondary analyses revealed a time- and dose-dependent efficacy of DEX. Specifically, a robust survival benefit was identified exclusively among patients receiving early intervention (0-24 h) or low-dose administration. In contrast, a moderate-to-high dose or a prolonged course of DEX failed to ameliorate prognosis. These findings suggest that the overall clinical value of DEX may be obscured by suboptimal timing of administration or doses, suggesting that precise, individualized administration of DEX may be of vital importance.
No association between DEX use and a reduced 30-day mortality rate was observed in this study. Such a conclusion has also been reached in some studies.16–18 This may be attributed to the inherently fragile hemodynamic status of patients with sepsis and concomitant HF. Although DEX features anti-sympathetic and anti-inflammatory properties, it is also associated with dose-dependent bradycardia and hypotension, and real-world data indicate that cardiovascular events are the adverse effects most frequently reported. 19 Unrestricted or high-dose DEX may offset its potential protection mechanisms through cardiovascular adverse effects,20–22 leading to an overall neutral result.
Second, the secondary analyses showed that the efficacy was time- and dose-dependent: early use (within 24 h) and low doses prolong survival, whereas moderate-to-high doses did not. When patients receiving different DEX regimens are pooled together, the true signal of benefit is masked, and the overall effect appears null.
Third, sepsis complicated by HF creates an extremely dangerous clinical situation. Patients are typically confronted with conflicting life-threatening mechanisms (eg, cardiogenic shock, refractory infection, and multi-organ failure), ultimately resulting in an extremely high mortality rate. 17 Under such extreme conditions, even the modest survival benefit provided by a pleiotropic sedative may be insufficient to alter the overall disease trajectory.
Overall, these factors may collectively account for the neutral primary outcome. Nevertheless, as shown by the exploratory analyses, this does not preclude the possibility that specific subgroups might still derive benefit. The findings in this study suggest that, in this vulnerable population, DEX should be used with individualization, optimal timing, and strict dose control.
Contrary to the findings in this study, several studies have reported that DEX use in individuals with sepsis reduces a 28-day mortality rate23,24 and the risk of death associated with acute kidney injury. 25 Some studies have even suggested a survival benefit of moderate-to-high doses of DEX among patients with sepsis-induced myocardial injury. 26 These discrepancies possibly stem from heterogeneity in study populations. Previous studies predominantly targeted the general population, with sepsis, potentially excluding individuals with severe cardiac dysfunction, and did not perform detailed stratification by timing and dose. Typically, a fixed-rate infusion method was adopted. 26
Although DEX was not superior to non-use in terms of overall mortality, the exploratory analyses in this study suggested that the timing and dose of DEX administration may be key factors influencing prognosis. Early use (0-24 h) and low-dose administration were both associated with a lowered 30-day mortality rate. Research has highlighted the critical role of α-2 adrenergic receptors in the protective effects of DEX. For instance, knockout of these receptors in late-stage sepsis reduces survival and exacerbates myocardial dysfunction in mice, 27 whereas early pretreatment provides cardioprotection. 28
Differing from some viewpoints, high-dose DEX is ineffective, and prolonged use may even be harmful. A possible explanation is receptor saturation: the protection peak is reached with short-term use, and a prolonged duration of use or a higher dose confers no additional benefit. 29 The disappearance of survival benefit with moderate-to-high doses may also be related to the dose-dependent biphasic pharmacodynamics of DEX. At low doses, it primarily activates central α2A receptors, conferring benefits. At higher doses, receptor selectivity is lost, and it begins to stimulate peripheral α2B and α1 receptors, triggering vasoconstriction, increased afterload, and worsened microcirculation. Consequently, the hemodynamic side effects at high doses counteract the anti-inflammation advantages.20,30
The protective effect of low-dose DEX is clinically plausible and aligns with current ICU sedation concepts. Studies recommend ‘light sedation’ rather than ‘deep sedation’ to facilitate early awakening and weaning. 6 As an α2 agonist, DEX provides cooperative sedation without suppressing breathing, fitting this strategy precisely. 31 We hypothesize that low-dose DEX offers adequate sedation and analgesia, prevents anxiety-related complications, and avoids the bradycardia and hypotension commonly observed with a moderate-to-high dose. This balance reduces adverse events, promotes early weaning, and thus confers a survival benefit.
Finally, we assessed whether different clinical characteristics influence the relationship between DEX dose or duration and 30-day mortality rate. First, the survival benefit of DEX was more significant among patients not receiving β-blockers. Mechanistically, β-blockers improve cardiac function by reducing heart rate and myocardial oxygen consumption. 32 The combination of DEX with β-blockers may lead to excessive heart rate slowing and decreased cardiac output, 33 potentially counteracting some of the protective effects of DEX. This suggests that in clinical practice, patients already on β-blocker therapy require more careful hemodynamic monitoring when DEX is co-administered.
Second, in patients with diabetes mellitus, the dose-dependent effect of DEX was more prominent. Only high-dose DEX (Group G4) reduced mortality risk in patients with diabetes mellitus, possibly because hyperglycemia suppresses cardioprotection pathways (eg, PI3 K/Akt and GSK-3β), causing the myocardium to be resistant to conventional therapies. 34
Third, patients receiving continuous renal replacement therapy (CRRT) might benefit from a specific duration of DEX use (24-72 h). However, given the small sample size, the extremely critical condition of patients on CRRT, and the fact that CRRT may alter DEX pharmacokinetics, this finding should be interpreted with caution.
This study was based on a large sample of 8426 cases. After PSM 1342 DEX users with 7084 non-DEX users, 1331 well-balanced pairs were obtained. The real clinical value of our findings lies in guiding more individualized, evidence-based sedation for patients with sepsis complicated by HF. It is recommended that DEX be initiated as the primary or adjunct sedative early after resuscitation and hemodynamic stabilization. During DEX use, the dose should be slowly titrated within routine ICU maintenance ranges to achieve a target sedation, and maintained for 1–2 days. Moreover, the dose should be adjusted according to individual conditions, and adverse reactions such as bradycardia and hypotension should be closely monitored. This strategy is beneficial for earlier and more stable blockade of upstream pathological circuits (eg, ferroptosis, inflammation, and microcirculatory collapse). Additionally, this strategy reduces oxygen demand and enhances DEX perfusion among patients with HF, thereby ameliorating the prognosis for patients with sepsis complicated by HF.
Several limitations in this study should be accounted for when interpreting the results. First, its retrospective design inevitably introduces selection bias and potential confounding factors. Second, the absence of certain critical clinical data, such as left ventricular ejection fraction (LVEF) and brain natriuretic peptide (BNP), precluded further stratification based on HF phenotype. Third, although the average infusion rate might offer greater clinical guidance than the cumulative total dose, accurately calculating the rate was extremely challenging due to weight fluctuations among critically ill patients, as documented in retrospective records. While the effect of infusion rate was explored in supplementary analyses, no statistical significance was observed. This may be attributed to the fact that potential effects are masked by inherent temporal recording biases in retrospective data, or it may suggest a non-linear dose-response relationship for DEX within a specific range. Fourth, the lack of data on specific doses and compliance with standardized anti-HF medications may also introduce bias. Finally, exploring mechanisms in this study was primarily based on previous literature and has not been experimentally validated, and the single-center data possibly limited the generalizability of the findings. In the future, prospective studies based on multicenter data are urgently warranted to further verify these conclusions by precisely recording infusion rates (mcg/kg/h), dynamic biomarkers, and hemodynamic parameters.
Conclusion
In this cohort, DEX did not reduce the mortality rate at 30 days or 90-days among patients with sepsis complicated by HF. However, reduced exposure to DEX (in terms of dose and duration) may be associated with ameliorated outcomes.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261461553 - Supplemental material for Dexmedetomidine for Reducing Mortality in Patients with Sepsis and Concomitant Heart Failure: A Retrospective Cohort Study
Supplemental material, sj-docx-1-jic-10.1177_08850666261461553 for Dexmedetomidine for Reducing Mortality in Patients with Sepsis and Concomitant Heart Failure: A Retrospective Cohort Study by Jinjing Mo, Hongyuan Zhang, Yusang Chen and Xingwang Li in Journal of Intensive Care Medicine
Supplemental Material
sj-doc-2-jic-10.1177_08850666261461553 - Supplemental material for Dexmedetomidine for Reducing Mortality in Patients with Sepsis and Concomitant Heart Failure: A Retrospective Cohort Study
Supplemental material, sj-doc-2-jic-10.1177_08850666261461553 for Dexmedetomidine for Reducing Mortality in Patients with Sepsis and Concomitant Heart Failure: A Retrospective Cohort Study by Jinjing Mo, Hongyuan Zhang, Yusang Chen and Xingwang Li in Journal of Intensive Care Medicine
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
The MlMIC-IV database was approved by the Massachusetts Institute of Technology (Cambridge, MA) and Beth Israel Deaconess Medical Center (Boston, MA), and consent was obtained for the collection of original data. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Therefore, ethical approval and the need for informed consent were waived for this study.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
All authors contributed to the study conception and design. Xingwang Li: Conceptualization, Methodology; Jinjing Mo: Data curation, Writing - Original draft preparation; Hongyuan Zhang: Writing - Reviewing and Editing; Yusang Chen: Supervision. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.