
Abstract

We thank Drs. Ayten and Yildirim for their thoughtful comments and interest in our study evaluating the association between long-acting insulin (LAI) use and hypoglycemia in critically ill surgical patients with type 2 diabetes mellitus. 1
We appreciate their observations regarding the potential for residual confounding and baseline differences between treatment groups. In response to these concerns, we performed an inverse probability of treatment weighting (IPTW) analysis to assess if choices with our analytic approach led to different results. We selected IPTW rather than propensity score matching to preserve the entire study population and maintain adequate power to detect a difference between cohorts. Propensity score matching could have excluded a meaningful proportion of patients from the analysis, potentially limiting the ability to identify differences.
Propensity scores were estimated using logistic regression to model the probability of receiving LAI in addition to sliding scale insulin (LAI + SSI) based on variables that were associated with hypoglycemia. These included age, sex, race, body mass index, baseline glucose, hemoglobin A1c (HbA1c), serum creatinine, bilirubin, acute kidney injury (AKI), sequential organ failure assessment (SOFA), surgery type, severity of diabetes, home anti-hyperglycemic medications, presence of corticosteroids and vasopressors. Multiple imputation was performed for missing variables. Once propensity scores were generated, inverse probability weights were calculated. Covariate balance was assessed using standardized mean differences (SMDs), with an absolute SMD < 0.10 considered adequate balance between treatment groups. Weighted logistic regression was performed to evaluate the association between LAI use and hypoglycemia. Statistical analyses were conducted using SAS version 9.4, and a two-sided p-value < 0.05 was considered statistically significant.
Baseline characteristics and standardized mean differences before and after weighting are presented in Table 1, demonstrating substantial improvement in covariate balance following weighting. Following IPTW adjustment, the association between LAI use and hypoglycemia remained consistent with our original findings. Hypoglycemia occurred in 17.8% of patients receiving LAI + SSI and 14.6% of patients receiving SSI alone (OR 1.27, 95% CI 0.63-2.57) (Table 2). These results suggest that the observed lack of association between LAI use and hypoglycemia was not influenced by measured baseline imbalances between cohorts.
Baseline Characteristics Before and After Inverse Probability of Treatment Weighting (IPTW).
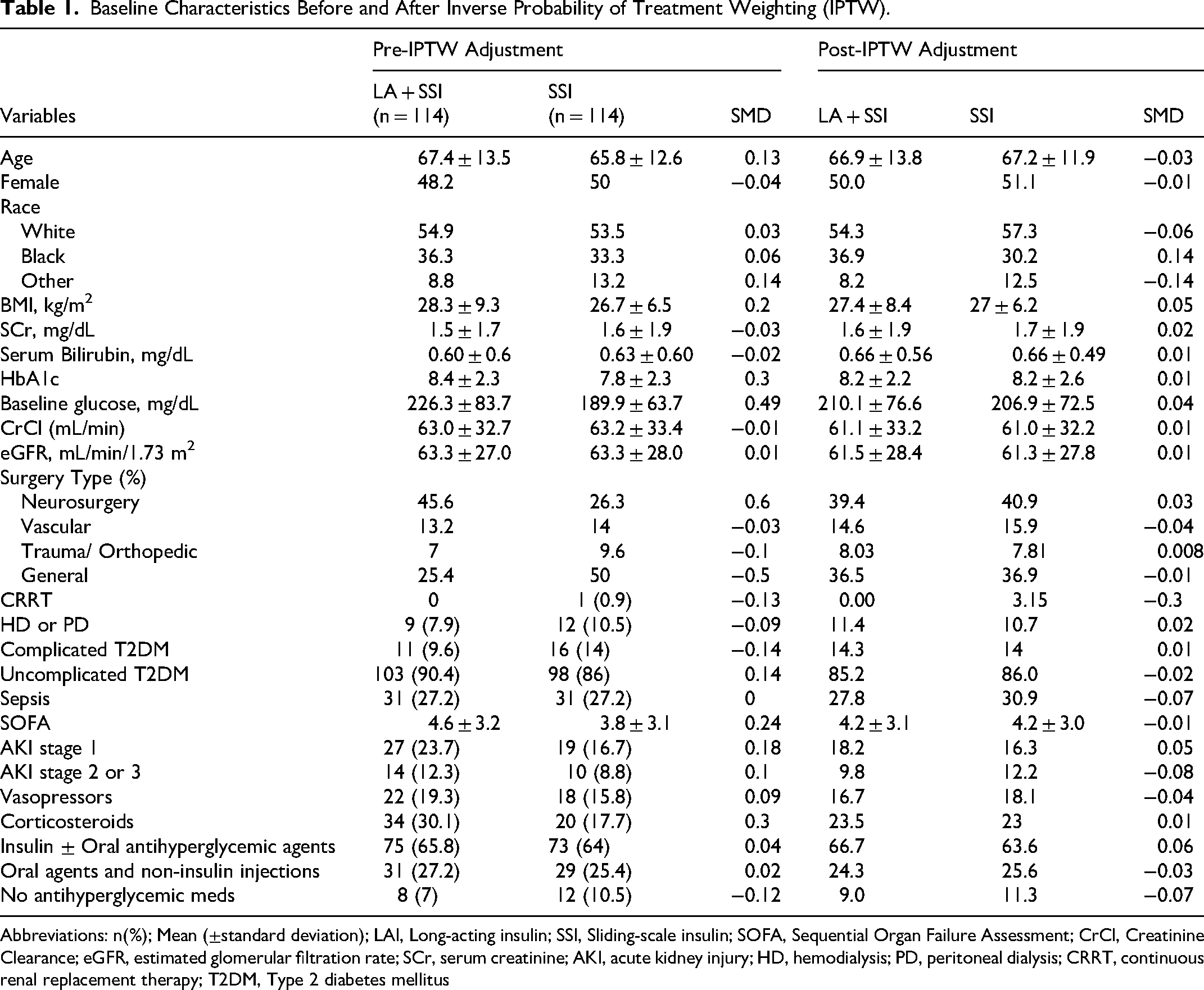
Abbreviations: n(%); Mean (±standard deviation); LAI, Long-acting insulin; SSI, Sliding-scale insulin; SOFA, Sequential Organ Failure Assessment; CrCl, Creatinine Clearance; eGFR, estimated glomerular filtration rate; SCr, serum creatinine; AKI, acute kidney injury; HD, hemodialysis; PD, peritoneal dialysis; CRRT, continuous renal replacement therapy; T2DM, Type 2 diabetes mellitus
IPTW-Adjusted Association Between Long-Acting Insulin use and Hypoglycemia.
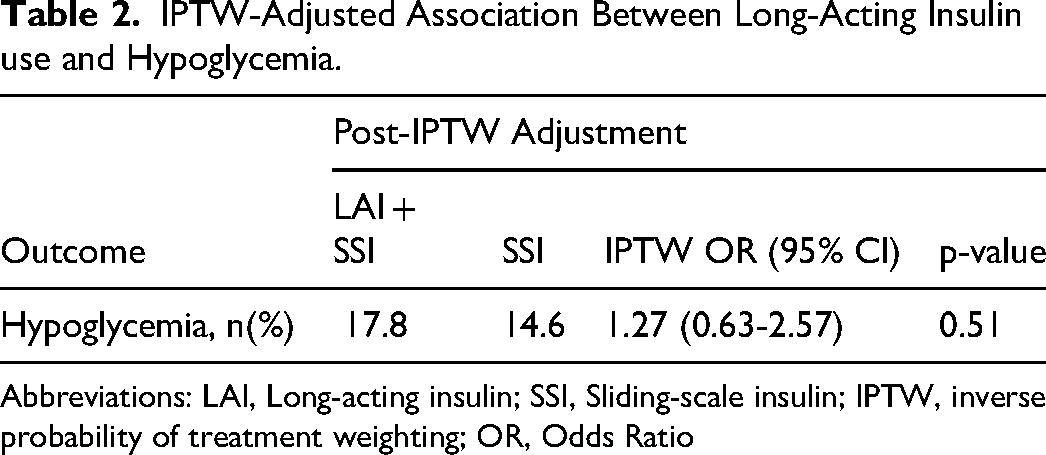
Abbreviations: LAI, Long-acting insulin; SSI, Sliding-scale insulin; IPTW, inverse probability of treatment weighting; OR, Odds Ratio
We agree that addressing potential cofounding is an important consideration in observational research. While our original analysis utilized matching based on duration of inpatient insulin use and anti-hyperglycemic therapy prior to admission, the IPTW analysis provides an additional sensitivity analysis incorporating a broader range of variables. Our group has previously utilized propensity score matching and weighting methodologies in multicenter observational studies, and these approaches have generally yielded findings consistent with multivariable analyses.2,3 Similarly, in the present study, the IPTW analysis produced results that were consistent with our original findings.
We sincerely appreciate the authors’ engagement with our work and agree that prospective studies are warranted to further evaluate the safety and effectiveness of LAI in critically ill patients with diabetes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.