
Abstract
Background
The association between aspirin and mortality in patients with sepsis remains unclear. This study aimed to systematically evaluate the effects of aspirin on mortality and major bleeding in adults with sepsis.
Methods
This review was registered in Open Science Framework (DOI: 10.17605/OSF.IO/E5K87). We searched MEDLINE, Embase, CENTRAL, ICTRP, and ClinicalTrials.gov through May 9, 2025. We included one randomized controlled trial (RCT) and four non-randomized studies of interventions (NRSIs). Risk of bias was assessed using RoB 2 for RCTs and ROBINS-I for NRSIs. Random-effects meta-analysis was performed.
Results
Five studies involving 25 138 patients were included. Aspirin showed a possible reduction in mortality (RR 0.77, 95% CI 0.66-0.89; I2 = 61.9%), but the certainty of evidence was very low. No clear effect was observed on major bleeding (OR 1.20, 95% CI 0.46-3.11; I2 = 77.3%), also with very low certainty. Data for secondary outcomes (SOFA score, ICU length of stay) was sparse and very uncertain. Subgroup analyses showed no evidence of effect modification by aspirin timing or treatment setting, and sensitivity analyses limited to Sepsis-3 studies and exclusion of Wang et al produced similar results. Evidence was limited by the predominance of NRSIs, heterogeneity in sepsis definitions, and variability in dosing and timing of aspirin.
Conclusions
The evidence is very uncertain regarding the effect of aspirin on mortality or bleeding in sepsis. Routine aspirin use for patients with sepsis cannot be recommended. For patients already receiving aspirin before hospitalization, continuation should be guided by clinical judgment. Further high-quality RCTs are warranted.
Introduction
Sepsis represents one of the leading causes of hospital mortality, responsible for over 11 million deaths annually worldwide. 1 The health burden due to sepsis continues to increase globally despite advances in supportive care, with mortality rates often exceeding 25% and imposing substantial economic costs on healthcare systems. 2 The pathophysiology of sepsis involves a dysregulated host response to infection, characterized by systemic inflammation and activation of the coagulation cascade. Platelet activation and their interaction with endothelial cells and neutrophils contribute to microvascular thrombosis and subsequent organ dysfunction. 3 These mechanisms have prompted interest in therapeutic interventions targeting platelet function. Acetylsalicylic acid (ASA, aspirin) irreversibly inhibits cyclooxygenase and suppresses thromboxane A₂ synthesis, thereby preventing platelet aggregation and exerting potential anti-inflammatory effects.3,4
Despite its well-established antiplatelet properties, the application of aspirin in patients with sepsis remains inadequately explored. 5 Current evidence presents conflicting conclusions. Two meta-analyses6,7 concluded that antiplatelet drugs, particularly aspirin, could reduce mortality in patients with sepsis. However, these meta-analyses included only non-randomized studies of interventions (NRSIs), many of which were conducted before the Sepsis-3 definition 8 was introduced in 2016, potentially mixing heterogeneous patient populations. In contrast, a more recent randomized controlled trial (RCT) 9 failed to demonstrate mortality benefits with aspirin administration in this population. These discrepancies may, in part, be attributable to evolving sepsis definitions over time. The transition from Sepsis-1/210,11 to Sepsis-3 in 2016 marked a substantial shift in diagnostic criteria, leading to differences in the populations studied across earlier NRSIs and more recent RCT.
Given these inconsistencies, a comprehensive evaluation of the current evidence is warranted. To address the limitations of prior studies, we will conduct a systematic review and meta-analysis that includes both NRSIs and an RCT, with particular attention to the sepsis definitions employed. Sensitivity analyses will be performed to isolate studies using the Sepsis-3 definition and specific studies with potential methodological concerns, while subgroup analyses will explore the influence of aspirin administration timing (chronic use vs new initiation) and treatment setting (ICU vs non-ICU). By integrating data across study types and accounting for key sources of variability, this review aims to assess the effects of aspirin on mortality, organ dysfunction, and major bleeding in adult patients with sepsis or septic shock, thereby clarifying aspirin's potential role in contemporary sepsis management and informing future clinical practice guidelines.
Methods
Protocol
This systematic review and meta-analysis was preregistered on the Open Science Framework (OSF; DOI: 10.17605/OSF.IO/E5K87). 12 The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 13 We ensured PRISMA compliance by referring to the PRISMA 2020 checklist, 13 as summarized in Table S1.
Inclusion and Exclusion Criteria
We included RCTs, prospective cohort studies and retrospective observational studies that assessed aspirin in adult patients with sepsis or septic shock. We did not apply language or country restrictions. We included all papers including published, unpublished articles, abstract of conference and letter. We did not exclude studies based on the observation period or publication year. We included studies enrolling adult inpatients (≥18 years) diagnosed with sepsis or septic shock, defined according to Sepsis-3 criteria 8 or an equivalent clinical definition as judged by the study authors. We also included studies of patients with severe infections associated with documented or presumed bloodstream infection that were highly likely to meet Sepsis-3 criteria, 8 even if not explicitly stated. Eligible studies evaluated aspirin administered by any enteral route (oral, nasogastric, or orogastric tube), at any daily dose or frequency, whether used chronically prior to hospital admission or newly initiated during hospitalization. Early discontinuation of aspirin during admission was permitted when based on bleeding risk or clinical judgment. We excluded studies or participants with conditions that could confound or preclude the evaluation of aspirin therapy. Specifically, we excluded patients with a nonfunctional gastrointestinal tract that prevented oral or enteral administration of aspirin, pregnant patients, and those with an extreme risk of bleeding, such as active gastrointestinal bleeding. In addition, we excluded studies that investigated other antiplatelet agents (eg, clopidogrel, ticagrelor, or dipyridamole) without providing separate analyses for aspirin, to ensure that the effects assessed were attributable solely to aspirin. We deliberately restricted inclusion to aspirin monotherapy to minimize heterogeneity and to focus on its unique anti-inflammatory and antithrombotic mechanisms, which differ from those of other antiplatelet agents. This approach allows for a more precise assessment of aspirin's specific effects in sepsis. Comparators were placebo and/or standard sepsis management without aspirin.
Primary Outcomes
The primary outcomes of this review were all-cause mortality and major bleeding. All-cause mortality was assessed as reported in each study, including ICU, in-hospital, 28-day, 30-day, 60-day, or 90-day mortality. When multiple mortality time points were available, the longest follow-up period closest to 90 days was selected for the primary analysis, consistent with previous evidence showing strong correlations among different mortality time points. 14 Major bleeding was defined, when available, according to the International Society on Thrombosis and Haemostasis (ISTH) criteria—any fatal bleeding, symptomatic bleeding in a critical area or organ, a hemoglobin decrease of ≥20 g/L, or transfusion of ≥2 units of whole blood or red cells within 24 h. 15 In studies without an explicit ISTH-based definition, comparable definitions (eg, life-threatening, gastrointestinal, or intracranial bleeding) were accepted, and the exact criteria were extracted. Bleeding events were included if they occurred after hospital admission, with the observation period extending from admission to discharge or day 90, whichever was longer. Shorter observation periods (eg, 14 or 28 days) were accepted if clearly defined, and when not specified, the period was assumed to match the study's overall follow-up. 16
Secondary Outcomes
Secondary outcomes included the change in organ dysfunction severity, ICU length of stay, and hospital length of stay. Change in organ dysfunction was defined as the difference in the Sequential Organ Failure Assessment (SOFA) score between baseline (admission) and follow-up, measured from admission to day 7 or ICU discharge, whichever occurred first. ICU length of stay was defined as the total number of days from ICU admission to ICU discharge, and hospital length of stay as the total number of days from hospital admission to hospital discharge.
Literature Search
We conducted a comprehensive literature search from database inception to May 9, 2025, with the last search for each source performed on that date. The following electronic databases were searched: MEDLINE (via PubMed), the Cochrane Central Register of Controlled Trials (CENTRAL), and EMBASE (Dialog). To identify ongoing or unpublished studies, we also searched the World Health Organization International Clinical Trials Registry Platform (ICTRP) and ClinicalTrials.gov.
In addition, we manually screened the reference lists of eligible studies, relevant reviews, and key international guidelines such as the Surviving Sepsis Campaign 2021. 17 We also reviewed citations to eligible studies and contacted corresponding authors to obtain unpublished or additional data when necessary. The search strategies combined controlled vocabulary (eg, MeSH/Emtree terms) and free-text keywords related to sepsis (eg, “sepsis,” “septic shock,” “bloodstream infection,” “bacteremia,” “septicemia”) and aspirin (eg, “aspirin,” “acetylsalicylic acid,” “ASA”), joined using Boolean operators. No restrictions were placed on language, publication date, or study status. The complete, line-by-line search strategies for each database and registry are provided in Table S2.
Screening, Data Extraction, and Appraisal
Two reviewers (Y.H. and S.K.) independently screened all titles and abstracts for eligibility, followed by full-text assessment of potentially relevant reports. Disagreements were resolved through discussion, and if consensus could not be reached, a third reviewer (E.I. or Y.K.) acted as an adjudicator. We contacted study authors for clarification or to obtain missing data when necessary. The full selection process, including de-duplication and reasons for exclusion, is illustrated in the PRISMA flow diagram (Figure 1). Data from eligible studies were independently extracted by the same two reviewers (Y.H. and S.K.) using a standardized and piloted data extraction form, which was tested on a random sample of 10 studies before implementation. The extraction form captured study characteristics (author, year, country, design, sample size), patient demographics (age, sex, comorbidities, baseline SOFA score, sepsis definition), intervention details (aspirin dose, timing, duration, route), comparators, and outcomes (mortality, major bleeding, SOFA change, ICU and hospital length of stay). Funding sources and conflicts of interest were also recorded. Discrepancies in data extraction were resolved by consensus or, when necessary, arbitration by a third reviewer (E.I. or Y.K.). For Wang et al, 18 outcome data were extracted from the subgroup analysis reported in the study, while baseline characteristics (eg, age, sex, and SOFA score) were obtained from the overall cohort due to limited availability of subgroup-specific data. Risk of bias was assessed independently by two reviewers (Y.H. and S.K.) using the Risk of Bias 2 (RoB 2) 19 tool for RCTs and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool20,21 for NRSIs. Domain-level and overall judgments followed the corresponding published guidance. Disagreements were discussed and resolved by consensus, with third-party adjudication (E.I. or Y.K.) when required. Authors were contacted for clarification when critical information was missing or unclear.
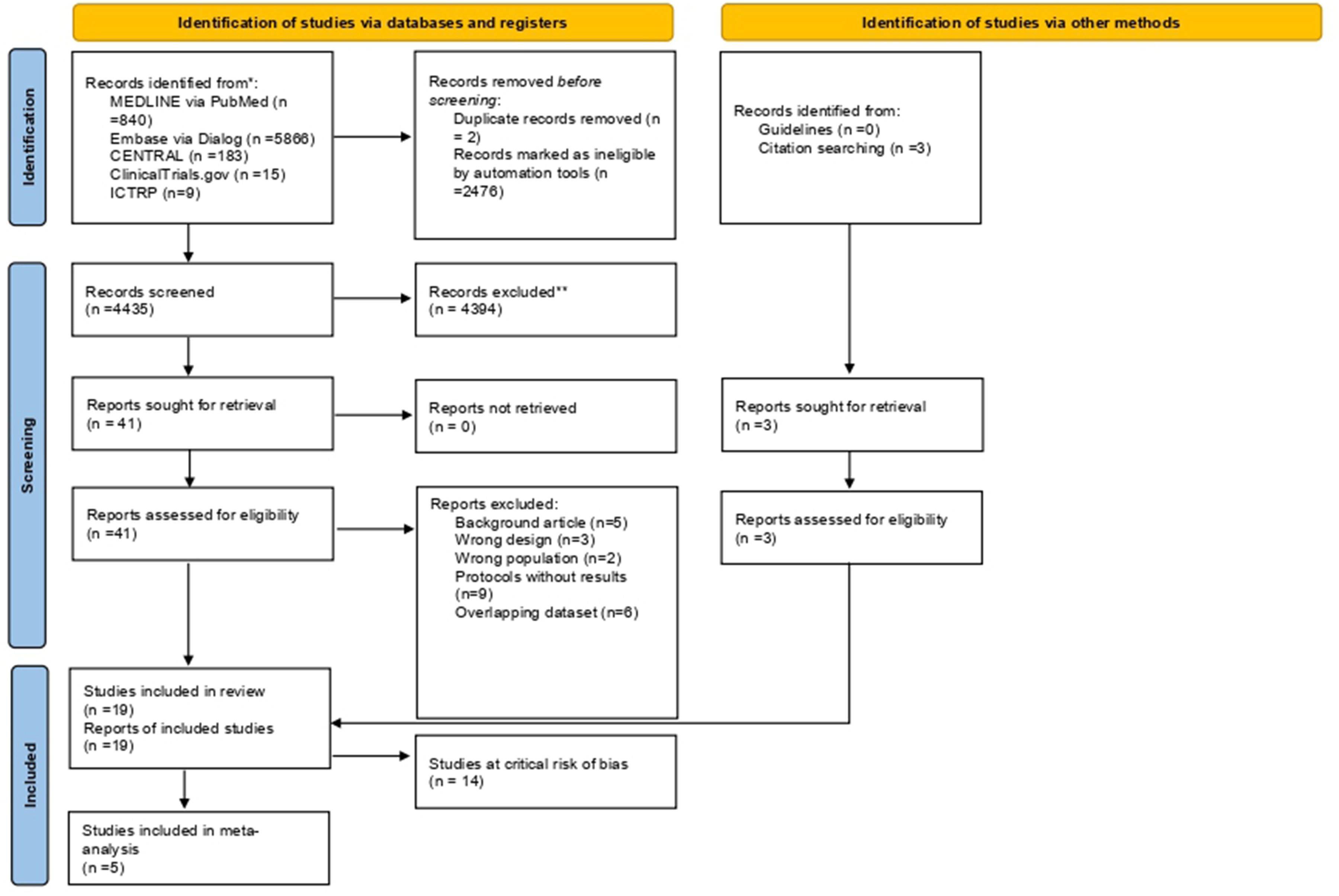
PRISMA 2019 flow diagram. CENTRAL, Cochrane Central Register of Controlled Trials; ICTRP, International Clinical Trials Registry Platform; RCTs, randomized controlled trials.
Data Analysis
For dichotomous outcomes (all-cause mortality and major bleeding), we calculated risk ratios (RRs) or odds ratios (ORs) with 95% confidence intervals (CIs) using a random-effects model with the restricted maximum likelihood estimator. Meta-analyses were conducted using the metafor package in R (version 4.3.3). Studies assessed as having a critical risk of bias based on the ROBINS-I tool 21 were excluded from quantitative synthesis to minimize methodological bias. Statistical heterogeneity was assessed using the I2 statistic, τ2, and Cochran's Q test, with I2 values of 0%-40%, 30%-60%, 50%-90%, and 75%-100% interpreted as indicating low, moderate, substantial, and considerable heterogeneity, respectively.
We performed prespecified subgroup analyses for the primary outcome (all-cause mortality) to explore potential effect modifiers. Subgroups were defined according to (1) the timing of aspirin administration—chronic use prior to hospital admission versus new initiation during hospitalization—and (2) the treatment setting—ICU versus non-ICU patients. These analyses were intended to examine whether pre-existing aspirin use conferred a protective effect compared with aspirin initiated after sepsis diagnosis, and whether the treatment effect differed according to care setting and disease severity. When studies reported only mean and SD values for continuous outcomes, we calculated mean differences and corresponding 95% CIs following the Cochrane Handbookd. 22 When studies reported medians and interquartile ranges (IQRs), we approximated means and SDs assuming an approximately normal distribution, using the method described by Wan et al 23 For outcomes synthesized using odds ratios, we converted pooled odds ratios to relative risks using the formula: RR = OR / [(1 − P₀) + (P₀ × OR)], where P₀ represents the baseline risk in the control group. Absolute risks were then calculated by multiplying the converted relative risk by the baseline control risk (Risk_with_intervention = P₀ × RR). 16 These converted absolute risks and their 95% confidence intervals were used in the Summary of Findings table. Baseline risks (P₀) were derived from the pooled mean control rate of all RCTs contributing data to each outcome.
Sensitivity analyses were conducted to assess the robustness of the primary findings with respect to key methodological decisions. For all-cause mortality, we repeated the analyses restricted to studies that explicitly applied the Sepsis-3 criteria for patient inclusion. Given the limited availability of subgroup-specific data and potential inconsistency between subgroup-derived outcomes and overall baseline characteristics, we performed an additional sensitivity analysis excluding Wang et al 18 to evaluate the impact of this study on the pooled estimates.
Publication bias was evaluated using funnel plots and Egger's test when sufficient studies were available.
Certainty of evidence for each outcome was assessed using the GRADE approach and summarized in Summary of Findings tables. 24
Although the protocol prespecified additional analyses—including meta-analyses of continuous outcomes (SOFA score change, ICU and hospital length of stay), sensitivity analyses for major bleeding, and exploration of missing data impact—these were not performed due to insufficient available data across studies.
Results
Study Selection
A total of 6913 records were identified through database searching and other sources. After removing 2478 duplicates, 4435 records were screened by title and abstract, of which 4394 were excluded. The full texts of 44 reports were assessed for eligibility, and 25 were excluded for reasons such as protocols without results (n = 9), overlapping dataset (n = 6), and background article (n = 5). Details of excluded studies are presented in Table S3. Finally, 19 studies met the inclusion criteria, consisting of one RCT and 18 NRSIs. Of these, 14 studies in Table S4 were excluded from quantitative synthesis due to a critical risk of bias or insufficient data, leaving five studies for the meta-analysis (Figure 1).
Study Characteristics
The characteristics of the included studies are summarized in Table 1. Among the five studies,9,18,25–27 one was an RCT conducted in South America, 9 and the remaining four were NRSIs from North America,18,25 Europe, 27 and the Middle East. 26 Sample sizes varied widely, ranging from 166 participants in the smallest study 9 to 15 397 in the largest. 18 Median ages were highest in studies of chronic aspirin users and lowest in those investigating newly initiated aspirin during hospitalization. The proportion of male patients was generally balanced across studies, ranging from 42.3% to 57.2%. Baseline severity was most reported using SOFA scores, although one study reported APACHE II scores instead. The timing of aspirin administration differed across studies: three9,25,27 evaluated newly initiated aspirin during hospitalization, while two18,26 focused on chronic pre-hospital use. Sepsis-3 criteria were explicitly used in three studies,9,25,26 whereas the remaining two18,27 applied alternative definitions. Mortality endpoints were most assessed at 90 days, although some studies9,18 used 28-day mortality. For one large database study, 18 demographic variables such as age, sex, and severity were reported from the original dataset, while subgroup data were used for other variables.
Study Characteristics.
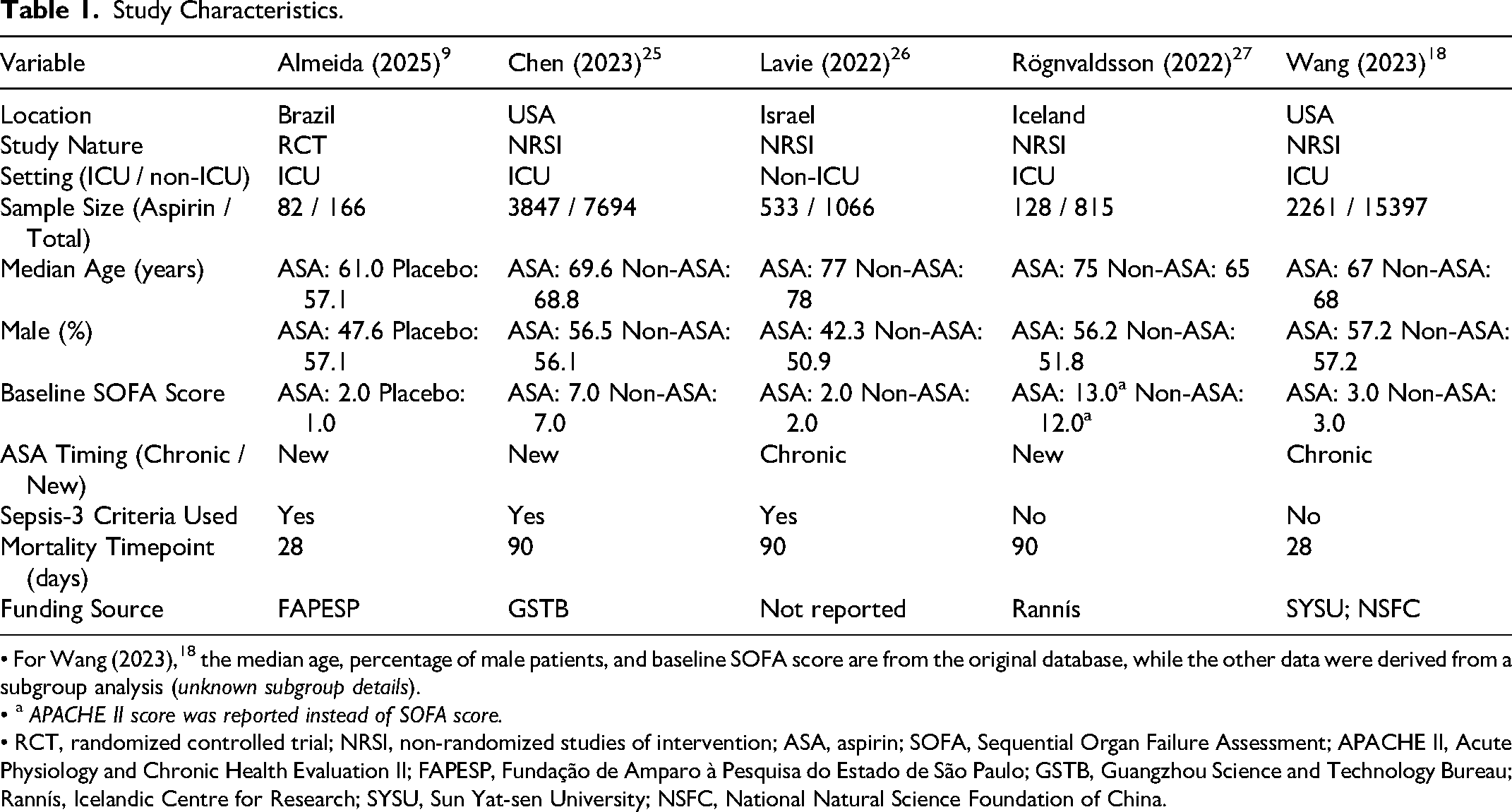
• For Wang (2023), 18 the median age, percentage of male patients, and baseline SOFA score are from the original database, while the other data were derived from a subgroup analysis (unknown subgroup details).
• a APACHE II score was reported instead of SOFA score.
• RCT, randomized controlled trial; NRSI, non-randomized studies of intervention; ASA, aspirin; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; FAPESP, Fundação de Amparo à Pesquisa do Estado de São Paulo; GSTB, Guangzhou Science and Technology Bureau; Rannís, Icelandic Centre for Research; SYSU, Sun Yat-sen University; NSFC, National Natural Science Foundation of China.
Risk of Bias
Risk-of-bias assessments using ROB 2 (for RCT) and ROBINS-I (for NRSIs) are shown in Figures 2 and 3, respectively. The RCT was judged to have a low overall risk of bias. Among the NRSIs, most demonstrated low risk in outcome measurement and intervention classification domains, but serious to critical risk for confounding and incomplete data. Fourteen NRSIs rated as critical were excluded from quantitative synthesis.
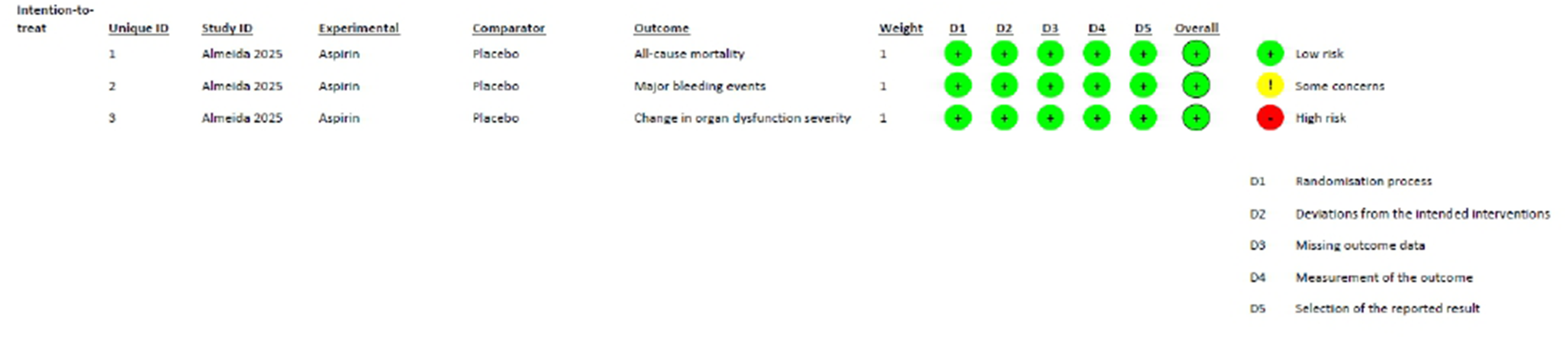
Risk of bias assessment for the RCT(9) using the RoB 2 tool.

Risk of bias assessment for mortality outcome using the ROBINS-I tool.
Primary Outcome
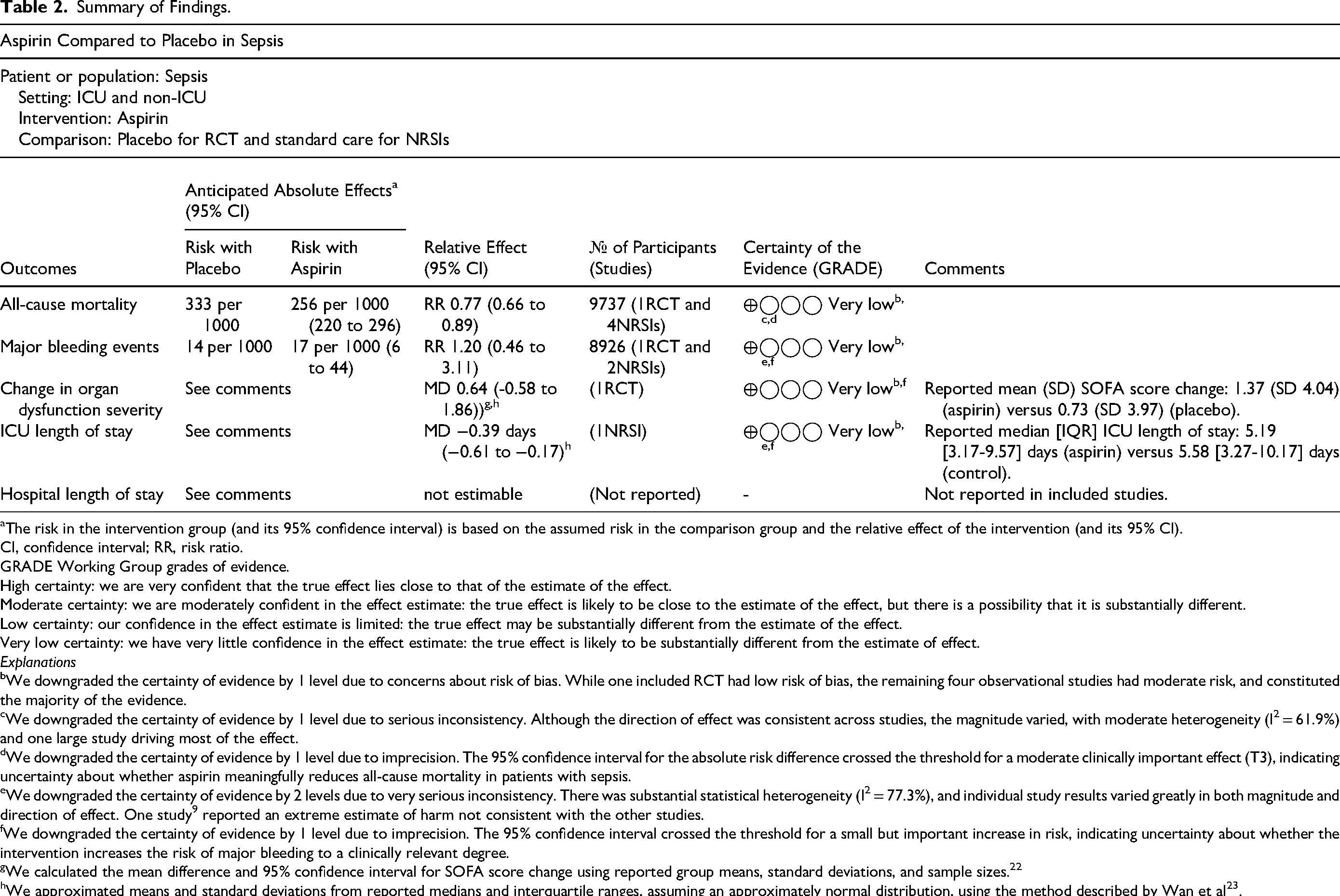
All-cause mortality and major bleeding outcomes are summarized in Table 2 and illustrated in Figure 4. In the pooled random-effects meta-analysis, aspirin use was associated with a reduction in all-cause mortality compared with no aspirin use (RR 0.77, 95% CI 0.66-0.89; I2 = 61.9%; very low certainty of evidence). There was substantial heterogeneity among the included studies.
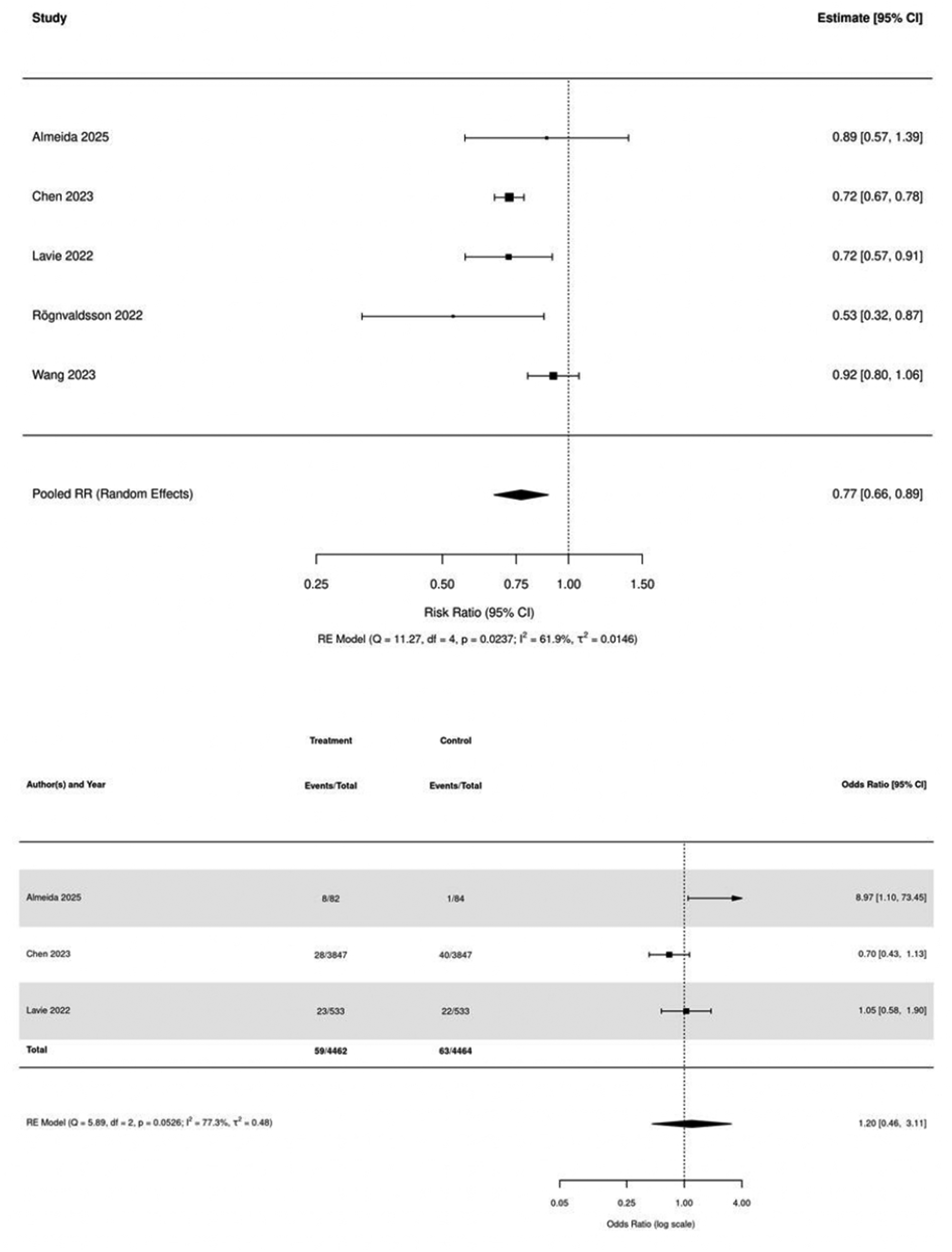
Forest plot of the effect of aspirin on all-cause mortality and the risk of major bleeding in patients with sepsis.
Summary of Findings.
The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI, confidence interval; RR, risk ratio.
GRADE Working Group grades of evidence.
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Explanations
We downgraded the certainty of evidence by 1 level due to concerns about risk of bias. While one included RCT had low risk of bias, the remaining four observational studies had moderate risk, and constituted the majority of the evidence.
We downgraded the certainty of evidence by 1 level due to serious inconsistency. Although the direction of effect was consistent across studies, the magnitude varied, with moderate heterogeneity (I2 = 61.9%) and one large study driving most of the effect.
We downgraded the certainty of evidence by 1 level due to imprecision. The 95% confidence interval for the absolute risk difference crossed the threshold for a moderate clinically important effect (T3), indicating uncertainty about whether aspirin meaningfully reduces all-cause mortality in patients with sepsis.
We downgraded the certainty of evidence by 2 levels due to very serious inconsistency. There was substantial statistical heterogeneity (I2 = 77.3%), and individual study results varied greatly in both magnitude and direction of effect. One study 9 reported an extreme estimate of harm not consistent with the other studies.
We downgraded the certainty of evidence by 1 level due to imprecision. The 95% confidence interval crossed the threshold for a small but important increase in risk, indicating uncertainty about whether the intervention increases the risk of major bleeding to a clinically relevant degree.
We calculated the mean difference and 95% confidence interval for SOFA score change using reported group means, standard deviations, and sample sizes. 22
We approximated means and standard deviations from reported medians and interquartile ranges, assuming an approximately normal distribution, using the method described by Wan et al 23 .
Three studies reported data on major bleeding events, and pooled analysis showed no evidence of a difference in bleeding risk between the aspirin and control groups (OR 1.20, 95% CI 0.46-3.11; I2 = 77.3%; very low certainty of evidence).
According to the GRADE assessment, the certainty of evidence for both outcomes was rated as very low, downgraded for risk of bias, inconsistency, and imprecision.
Secondary Outcomes
Only one RCT 9 reported changes in SOFA scores, showing mean (SD) values of 1.37 (4.04) in the aspirin group and 0.73 (3.97) in the placebo group, corresponding to a mean difference of 0.64 (95% CI −0.58 to 1.86).
Similarly, only one NRSI 25 reported ICU length of stay, with a median of 5.19 days [IQR 3.17-9.57] in the aspirin group and 5.58 days [IQR 3.27-10.17] in the control group, corresponding to an estimated mean difference of −0.39 days (95% CI −0.61 to −0.17). 23 No included studies reported hospital length of stay.
Subgroup and Sensitivity Analyses
The pooled effect on all-cause mortality was consistent across subgroups (Figures S1-S2). No significant differences were observed by aspirin timing (chronic vs new initiation; P = .268) or treatment setting (ICU vs non-ICU; P = .705), with pooled RRs ranging from 0.72 to 0.83 across subgroups. In sensitivity analysis restricted to studies that explicitly applied the Sepsis-3 criteria (Figure S3), the pooled estimate was similar to the primary analysis. In addition, exclusion of Wang et al 18 yielded similar results (RR 0.85, 95% CI 0.73-0.99), indicating that the overall findings were robust and not driven by this study.
Reporting Bias
Funnel plots (Figure S4) did not suggest clear asymmetry, and Egger's test was not statistically significant (P = .943). Because the number of included studies was small, formal evaluation of reporting bias was of limited value. Accordingly, funnel plot findings (Figure S4) were interpreted cautiously, and the possibility of publication bias or other small-study effects cannot be ruled out, particularly for observational studies.
Discussion
This systematic review and meta-analysis included five studies—one RCT 9 and four NRSIs18,25–27—encompassing a total of 25 138 patients with sepsis. The pooled estimates suggest that aspirin use might reduce all-cause mortality (RR 0.77, 95% CI 0.66-0.89), but the certainty of this evidence is very low due to methodological limitations and heterogeneity. Aspirin may have little to no effect on major bleeding, but the evidence is very uncertain. Substantial heterogeneity was observed in the pooled mortality analysis (I2 = 61.9%), which may reflect differences in study design, populations, timing of aspirin administration, and sepsis definitions across included studies. For major bleeding, heterogeneity was considerable (I2 = 77.3%), likely due to variations in bleeding definitions, reporting methods, and differences in how preexisting versus newly initiated aspirin exposure was handled. These variations underscore the methodological and clinical diversity among the included studies and contribute to the overall uncertainty of the pooled estimates. Secondary outcomes, including changes in SOFA score and ICU length of stay, were reported in only a few studies. The only RCT 9 showed no clear improvement in organ dysfunction (mean difference 0.64, 95% CI −0.58 to 1.86), whereas one NRSI 25 suggested a modest reduction in ICU stay (mean difference −0.39 days, 95% CI −0.61 to −0.17). Although both findings were based on very low-certainty evidence, they suggest possible but uncertain benefits that warrant further investigation. The pooled estimates for all-cause mortality were consistent across prespecified subgroups, with no evidence of effect modification by aspirin timing or treatment setting. These subgroup analyses were based on a limited number of studies and were likely underpowered; therefore, the absence of significant differences does not exclude meaningful differences between subgroups. A conceptual consideration is that the potential benefit of aspirin may depend on early administration in sepsis, as it targets platelet activation and thromboinflammatory pathways that evolve over the course of illness. 28 However, we were unable to examine time-to-initiation within individual studies because granular timing data were not consistently reported. Future trials should therefore prespecify stratification by time from sepsis onset to aspirin initiation. Sensitivity analyses restricted to studies using Sepsis-3 criteria and exclusion of Wang et al 18 yielded similar results. The pooled estimates suggest a possible reduction in mortality, and the direction of effect is consistent with prior observational studies, which may support a potential benefit of aspirin in sepsis. Although the certainty of evidence remains very low, the consistency of findings across observational studies and the overall direction of effect observed in the available prospective evidence may further increase interest in aspirin as a potential therapeutic strategy in sepsis. However, the balance between potential benefit and harm remains uncertain. Therefore, these findings should be interpreted cautiously, further clinical studies are needed before routine initiation of aspirin can be recommended.
Previous systematic reviews6,7 reported statistically significant reductions in mortality with antiplatelet therapy in sepsis. In Wang et al, 7 the certainty of evidence was rated as low using GRADE, 24 yet the authors highlighted a significant mortality reduction and underscored the potential benefit of antiplatelet therapy. Moreover, this study included several NRSIs derived from overlapping databases and assessed study quality using the Newcastle–Ottawa Scale, 29 which does not adequately capture confounding domains relevant to intervention research. In contrast, our review—while observing a similar direction of effect—judged the overall certainty of evidence to be very low and therefore does not support the routine initiation of aspirin in patients with sepsis. Several factors explain this divergence. Earlier reviews pooled various antiplatelet agents, mixed pre-sepsis and post-sepsis exposure windows, and relied on risk-of-bias tools that provide limited insight into confounding relevant to intervention research. As a result, the true effect of aspirin alone in sepsis—distinct from mixed antiplatelet regimens—remains unclear. Our analysis focused specifically on aspirin, distinguished between chronic pre-hospital use and new initiation during acute sepsis, incorporated Sepsis-3 severity definitions, and applied ROBINS-I 21 to exclude studies at critical risk of bias. These refinements clarified that apparent mortality reductions observed in previous reviews are highly uncertain and likely influenced by residual confounding and clinical heterogeneity. Thus, although the statistical association observed in conventional cohorts is broadly consistent across analyses, the triangulation of evidence from timing-specific subgroups, severity-based strata, and rigorous bias assessment suggests that the true effect of aspirin in sepsis remains very uncertain. Accordingly, our findings imply that clinicians should not initiate aspirin as a treatment for sepsis.
From the perspective of bleeding risk, routine initiation of aspirin therapy remains unsupported by the current evidence. The safety of aspirin in sepsis remains uncertain due to the very low certainty of evidence regarding bleeding complications. Although aspirin may have little to no effect on major bleeding based on available data, the evidence is too uncertain to exclude potential harm. A clinical trial 30 of aspirin was prematurely terminated due to an increased incidence of bleeding in the aspirin group, underscoring the importance of safety monitoring in future trials. Moreover, sepsis and septic shock frequently cause coagulopathy, including disseminated intravascular coagulation, which can manifest as both microvascular thrombosis and bleeding due to platelet and coagulation factor consumption. 31 Thrombocytopenia is also common and is associated with a higher risk of major bleeding and poor outcomes. 32 These pathophysiologic conditions may further amplify bleeding risk with antiplatelet therapy, supporting a conservative approach to aspirin initiation during acute sepsis. In cardiovascular disease, bleeding risk associated with antiplatelet therapy is generally accepted as a trade-off for preventing thrombotic events. 33 However, in sepsis, the balance between potential mortality benefit and bleeding risk remains uncertain. In addition, the increased risk of myocardial infarction after sepsis discharge should be considered when evaluating the timing and appropriateness of aspirin therapy. 34 Thus, decisions regarding aspirin use in patients with sepsis should be individualized by balancing bleeding risk, cardiovascular indications, and the potential timing of benefit.
The included studies were generally aligned with our research question in terms of population, intervention, comparator, and outcomes, supporting our judgment that indirectness was not serious overall. Although some studies included patients not explicitly defined using Sepsis-3 criteria, 8 these populations were highly likely to meet the criteria. Rögnvaldsson et al 27 enrolled patients with bacteremic pneumococcal pneumonia, with APACHE II scores (median 13 vs 12) indicating a severity consistent with sepsis. While there is no direct equivalence between APACHE II and SOFA scores, the observed severity and associated mortality risk appear broadly consistent with populations meeting Sepsis-3 criteria.8,35 Similarly, Wang et al reported SOFA scores (median 3 [IQR 1-5]) in the original cohort, suggesting that most patients met Sepsis-3 criteria. Although some concerns remain due to variations in study populations and clinical settings, these factors are unlikely to substantially affect the generalizability of our findings.
For patients who were already receiving aspirin prior to hospitalization, discontinuation should be carefully considered in light of cardiovascular indications and bleeding risk. NRSIs18,26 have suggested that chronic aspirin use is associated with reduced mortality in sepsis, whereas an RCT 36 has not confirmed a mortality benefit. Although the pooled estimates suggested a possible reduction in mortality, the certainty of evidence is very low, and there is no direct evidence comparing continuation versus discontinuation. Future adequately powered multicenter RCTs should clarify not only whether aspirin reduces all-cause mortality, but also in whom and when its potential benefit outweighs bleeding risk. Such trials should prespecify the timing of aspirin initiation, stratify patients by preexisting aspirin use and baseline bleeding risk, and assess major bleeding as well as thrombotic outcomes such as myocardial infarction and stroke. Consideration of racial, ethnic, and regional differences in bleeding and thrombotic risk would also be important for evaluating the generalizability of the risk-benefit profile.
Several limitations should be acknowledged. Only one RCT was available, and the remaining evidence was derived from NRSIs that are inherently prone to residual confounding. Considerable heterogeneity existed across studies in sepsis definitions, aspirin dosing regimens, and timing of administration, which may have influenced pooled estimates. Additionally, some included studies relied on administrative databases lacking detailed clinical data, such as infection source or organ dysfunction scores. Furthermore, in one large study, outcome data were derived from a subgroup analysis without fully reported subgroup definitions, while baseline characteristics were obtained from the overall cohort, which may introduce potential selection bias and limit comparability with other studies.
Conclusion
This systematic review and meta-analysis suggest that the evidence is very uncertain about the effect of aspirin on mortality and major bleeding in patients with sepsis. Routine initiation of aspirin therapy cannot be recommended. For patients already receiving aspirin prior to hospitalization, continuation should be guided by individual clinical judgement considering cardiovascular indications. Further high-quality RCTs are needed to clarify both the efficacy and safety of aspirin in this population.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261464950 - Supplemental material for Effect of Acetylsalicylic Acid on Mortality in Sepsis: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jic-10.1177_08850666261464950 for Effect of Acetylsalicylic Acid on Mortality in Sepsis: A Systematic Review and Meta-Analysis by Yusuke Hirao, Shunsuke Kondo, Brent Matsuda, Eriya Imai, Satoshi Miyashita and Yuki Kataoka in Journal of Intensive Care Medicine
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this work, the authors used ChatGPT to assist in improving the English grammar, clarity, and overall structure of the manuscript. After using this tool, the authors carefully reviewed and edited the text to ensure that it accurately reflects their own ideas and interpretations. The authors take full responsibility for the content of the published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.