
Abstract
Objectives
The Coronavirus Disease-2019 (COVID-19) pandemic had indirect impacts on healthcare provided to critically ill intensive care unit (ICU) non-COVID patients and their outcomes. Therefore, we examined the effect of the COVID-19 pandemic on patients with non-COVID critical illness during the pandemic and pre-pandemic epochs.
Design
Retrospective, population-based, observational cohort study.
Setting
All adult patients admitted to general ICUs in Alberta, Canada, from March 2017–2020 (pre-pandemic period) and March 2020–2023 (pandemic period).
Data sources
Data was captured from an integrated critical care clinical information system (eCritical Alberta) and Alberta Health Services (AHS) administrative databases were utilized.
Measurements and main results
A total of 80 540 non-COVID patients were admitted to ICUs in Alberta in the period between March 2017 and March 2023, equally distributed between the pandemic (40,196, 50.1%) and pre-pandemic (40,344, 49.9%) periods. For pandemic versus pre-pandemic cohorts, patient mean age was 57.7 ± 16.2 versus 58.5 ± 16.6 years and mean APACHE II score was 19.5 ± 8.8 versus 18.8 ± 8.5, respectively. ICU mortality was higher during the pandemic compared with pre-pandemic (14.2% vs 11.2%, mean difference [MD]: +3.1%, adjusted odds ratio [OR]:
Conclusion
During the pandemic period, non-COVID patients had worse outcomes, greater adjusted ICU and hospital mortality, with increased ICU lengths of stay, but shorter hospital lengths of stay, when compared with pre-pandemic periods.
Background
The coronavirus 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was a global health emergency as declared by the World Health Organization (WHO). 1 As of May 5, 2023 when the WHO declared the pandemic over, there were over 750 million confirmed cases and over 7 million deaths been reported globally. 2 Correspondingly, Canada experienced over 4.8 million cases (12% cases, 12 thousand cases per 100 000 population) and almost 56 thousand total deaths (0.14% deaths, 140 deaths per 100 000 population). In Alberta, over 644 thousand cases (12.8% cases, 12 800 cases per 100 000 population) and just over 6000 deaths (0.12% deaths, 120 deaths per 100 000 population).3,4 There is evidence to suggest that non-COVID-19 patients suffered indirect harm during the COVID-19 pandemic, with increased mortality, morbidity, disruptions in care, and changes to hospitalization patterns during the pandemic, when compared to pre-pandemic epochs.5,6 One hypothesis for these observations may relate to the “rule of rescue” where the most acute and sickest patients who require intensive care unit (ICU) and hospital resources (COVID-19 pandemic patients) are triaged ahead of non-COVID-19 patients (eg, scheduled surgeries, non-urgent medical illnesses).5–7 Patients may have also avoided healthcare settings from fear of COVID-19 contraction, potentially worsening outcomes from delayed presentations for care (eg, acute coronary syndromes).8–10
Overall, focusing solely on mortality and morbidity attributable to COVID-19 does not accurately estimate the full impact of the COVID-19 pandemic on the healthcare system. It is crucial to evaluate total excess (eg, avoidable or unanticipated) mortality (inclusive of both COVID-19 and non-COVID patients) during the pandemic as compared to non-pandemic times.5,6,11,12
Therefore, our study aims to describe and compare the demographic, clinical characteristics, and outcomes (ICU and hospital mortality) of the non-COVID adult population admitted to ICUs in Alberta during the pandemic (March 2020-2023) and pre-pandemic periods (March 2017-2020).
Methods
We followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) for reporting observational studies. 13 Ethics approval was obtained from the University of Alberta Health Research Ethics Board (File # PRO00130042, approved April 14, 2023).
Design, Setting, and Population
This was a retrospective, population-based, observational cohort study. We included all adult patients admitted to any of the general mixed medical/surgical and subspecialized adult ICUs or all adult patients in pediatric ICUs, who were cared for by adult intensivists in Alberta, Canada, from March 5, 2020 (date of first COVID-19 ICU admission in Alberta) to March 5, 2023 (3 years since start of pandemic in Alberta). Our control period (prior to the pandemic) includes all adult patients admitted to the same ICUs from March 5, 2017, to March 4, 2020.
Data Collection and Sources
Data collected included demographics (eg, age, sex), primary diagnosis, admission source, Clinical Frailty Score (CFS), 14 patient illness severity (eg, Acute Physiology and Chronic Health Evaluation (APACHE) II and III, 15 admission Sequential Organ Failure Assessment (SOFA) 16 for adults, organ support therapy (eg, vasopressors, invasive/non-invasive ventilation, prone positioning, renal replacement therapy, etc), and in-hospital complications (eg, nosocomial infections, bleeding, stroke), and patient outcomes (eg, death in the ICU and in hospital, hospital discharge destination).
Data sources include eCritical Alberta/TRACER and Connect Care/Enterprise/Alberta Health Services and Analytics data repositories,17,18 which provided demographics, admissions, discharges/transfers, vital statistics and mortality, Discharge abstract database (DAD), diagnostic/case-mix, illness severity: APACHE II and III scores; admission SOFA score, health care utilization in Alberta, including organ supports and lengths of stay. 18 COVID-19 was defined as a documented COVID-19 diagnosis within 14 days of hospital admission, while all other patients were classified as non-COVID. Comorbidities were taken from the patients’ electronic medical records.
Outcomes
The primary outcome was mortality (hospital and ICU). Secondary outcomes included 1) ICU and hospital lengths of stay, 2) hospital discharge destination, and 3) healthcare resource utilization.
Reporting and Analysis
Descriptive statistics were tabulated according to the relation to COVID-19 (pre-COVID and during COVID-19). Continuous data were reported as means with standard deviations (SD) and compared using t-tests, while categorical variables were presented as counts or proportions and compared using the Chi-square test. Median and interquartile ranges (IQR) were reported for non-normally distributed variables and compared using the Wilcoxon rank-sum test. Analysis was performed on complete cases only (those with data included). Significance was set to p < 0.05.
Variables were assessed using clinical rationale to be included in a multinomial regression analysis 19 to estimate the adjusted OR (aOR) for ICU and hospital mortality. Candidate covariables were age (categorized), sex, admission APACHE II, admission class, histories of respiratory insufficiency, diabetes mellitus, liver disease, and heart disease. Logistic regression analysis was performed to assess the association of time and period with ICU and hospital mortality.
Subgroup analysis was performed for age groups (10-year tranches, based on prior reporting of age subgroups in COVID-19, 20 and sex; SOFA score ≥5 or <5, 21 APACHE II ≥17 or <17 score, 22 and CFS ≥4 or <4, 23 based on the cut points used in previous studies.
We also performed propensity-score matching (PSM) 24 cohort comparisons using a logistic regression model that included the same set of covariables used in the multinomial regression analysis (sex, admission APACHE II, admission class, histories of respiratory insufficiency, diabetes mellitus, liver disease, and heart disease). Patients in the COVID period were matched 1:1 to those in pre-COVID, using narrow caliper widths to the nearest neighbor matching without replacement. 24 Following PSM, baseline demographics, clinical characteristics, and outcomes were re-evaluated using regression models for the matched cohort. For comparison, we also evaluated and described the remaining unmatched cohort as well.
Results
Baseline Demographics and Clinical Characteristics
Overall, there were 80 540 non-COVID patients admitted to ICUs in Alberta in the period between March 2017 and March 2023, relatively equally distributed between pre-COVID (n = 40,196, 50.1%) and during the COVID-19 pandemic period (n = 40,344, 49.9%), not including expanded capacity in the dedicated COVID-19 ICUs (as non-COVID patients were not admitted there). Table 1 shows the characteristics of patients admitted to ICU. Age and sex distribution were similar. There was no significant difference between pre-pandemic and pandemic periods in mean admission SOFA score [6.5 ± 3.9 versus 6.4 ± 3.9, p = 0.51]. However, there were significant differences in mean weight [84.5 ± 24.5 versus 86.2 ± 25.7 kg, p < 0.001], APACHE II score [84.5 ± 24.5 versus 86.2 ± 25.7, p < 0.001], and CFS score [3.64 ± 1.65 versus 3.57 ± 1.57, p < 0.001] in pre-pandemic versus pandemic periods (Table 1). To adjust for potential confounding, we also performed propensity-matching using a logistic multivariable regression model based on age and illness severity (APACHE II, SOFA, CFS). We present both the propensity-matched (Supplemental Table 1) and non-propensity-matched cohorts (Supplemental Table 2).
Patient Characteristics.
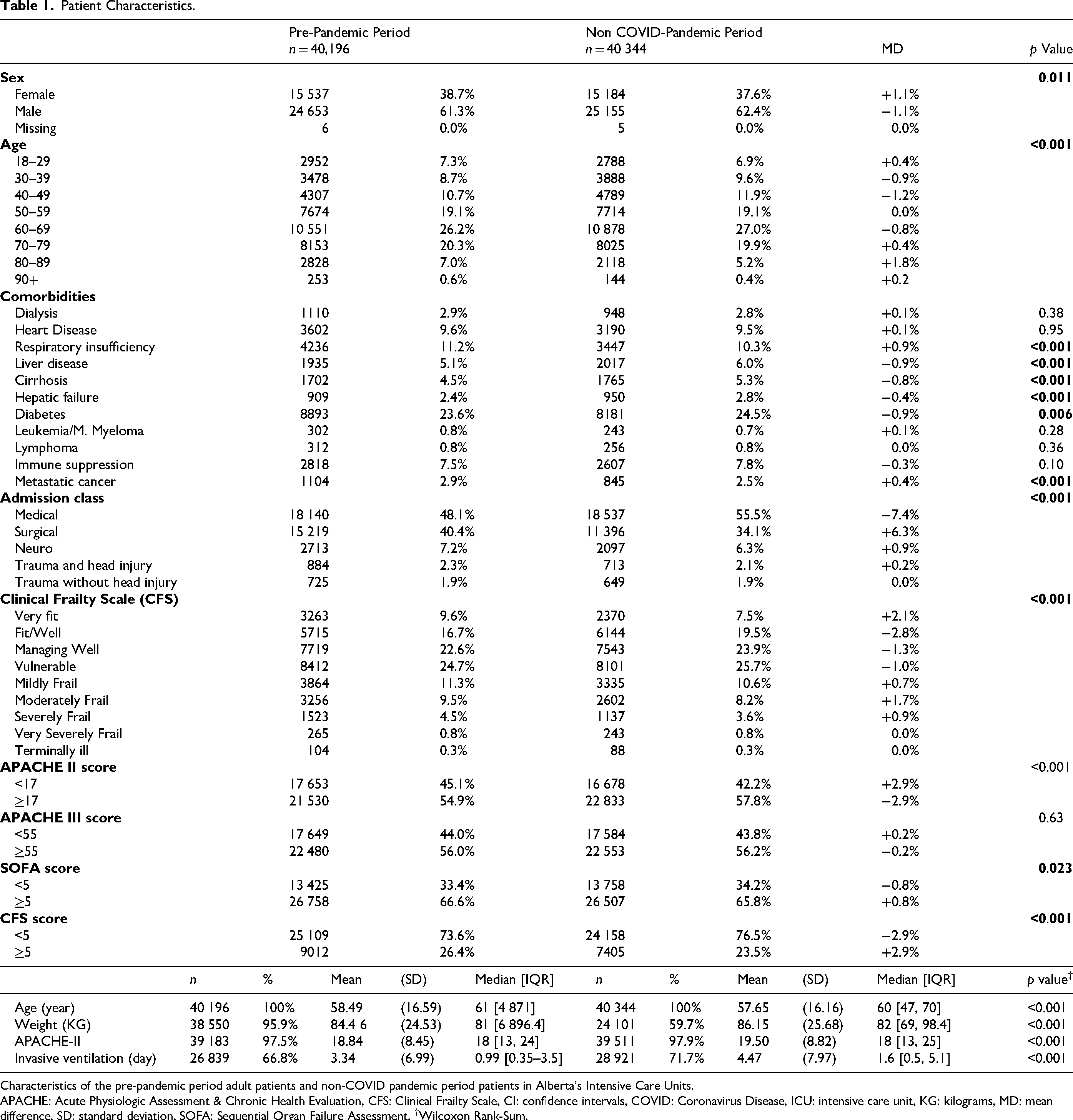
Characteristics of the pre-pandemic period adult patients and non-COVID pandemic period patients in Alberta's Intensive Care Units.
APACHE: Acute Physiologic Assessment & Chronic Health Evaluation, CFS: Clinical Frailty Scale, CI: confidence intervals, COVID: Coronavirus Disease, ICU: intensive care unit, KG: kilograms, MD: mean difference, SD: standard deviation, SOFA: Sequential Organ Failure Assessment, †Wilcoxon Rank-Sum.
Admission Geographic Location and Subtypes
Supplemental Table 3 shows the distribution of ICU admissions by geographic hospital location, specialty (eg, general, neurologic vs cardiovascular), and academic versus community subtypes. Subspecialized ICUs (eg, cardiovascular and neurological) experienced fewer admissions during the pandemic than in pre-pandemic periods. There was no distinct trend of increased or reduced utilization between academic and community hospitals.
Admission Diagnosis Subtypes
Supplemental Table 4 shows the types of ICU admissions during the pandemic versus the pre-pandemic periods. Of note, there were significantly fewer elective operations during the pandemic compared to pre-pandemic periods. There was a significant increase in medical and ICU admissions of various subtypes (eg, cardiovascular, gastrointestinal, hematology, genitourinary, metabolic, musculoskeletal, neurological, pulmonary, transplant, and trauma).
ICU Mortality
The ICU mortality for non-COVID ICU patients was significantly higher in the pandemic period 14.2% versus the pre-pandemic period 11.2% (mean difference [MD]: +3.0%) (Table 2, Figure 1). Crude ICU mortality odds ratio OR: 1.31 (95% CI: 1.26-1.37, p < 0.001), and adjusted mortality (aOR) was: 1.21 (95% CI: 1.14-1.28, p < 0.001) when adjusted for age, sex, weight, APACHE II score, admission class, respiratory insufficiency, diabetes, liver disease and heart disease.
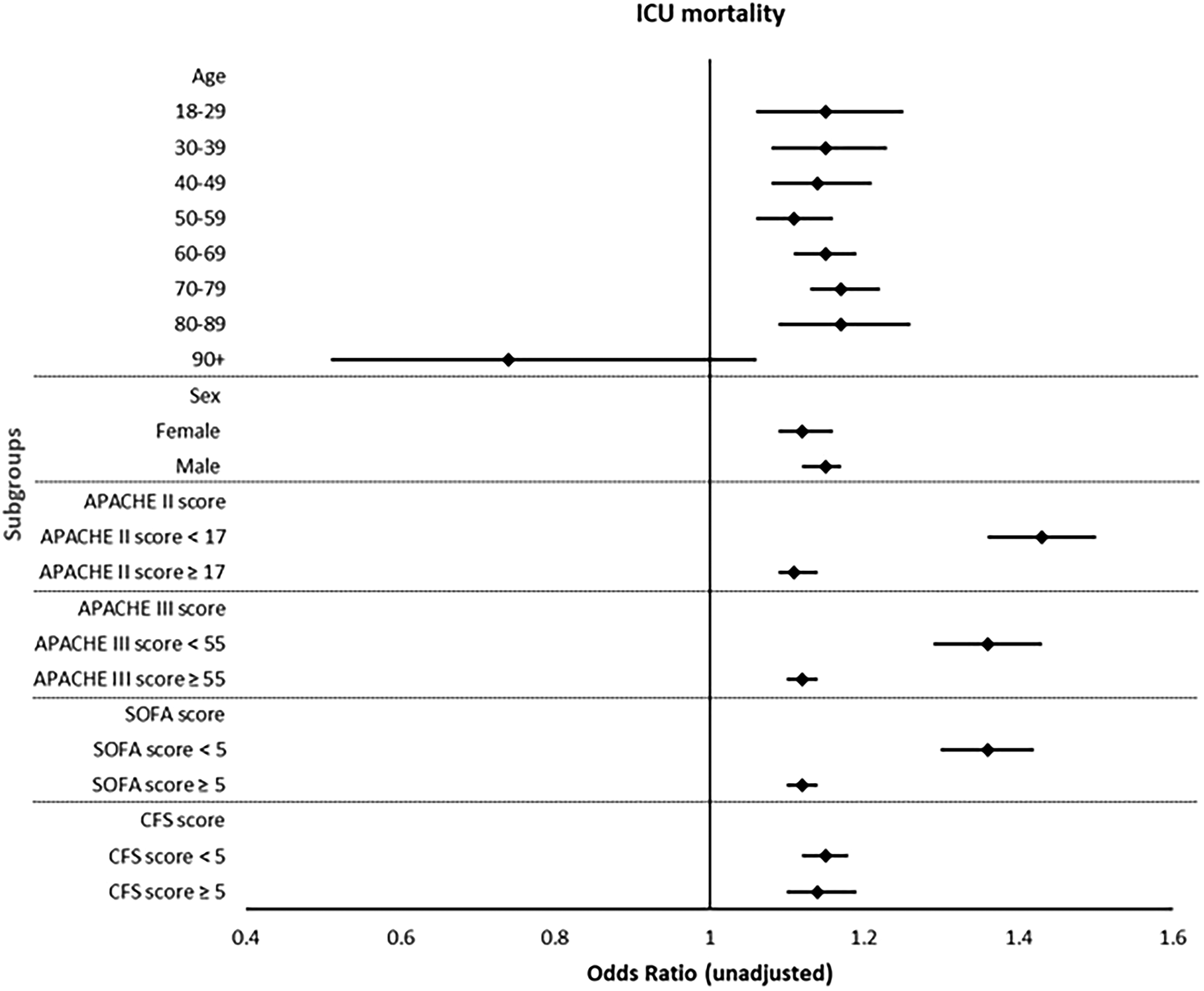
ICU Mortality (Subgroup Analysis).
Outcomes.
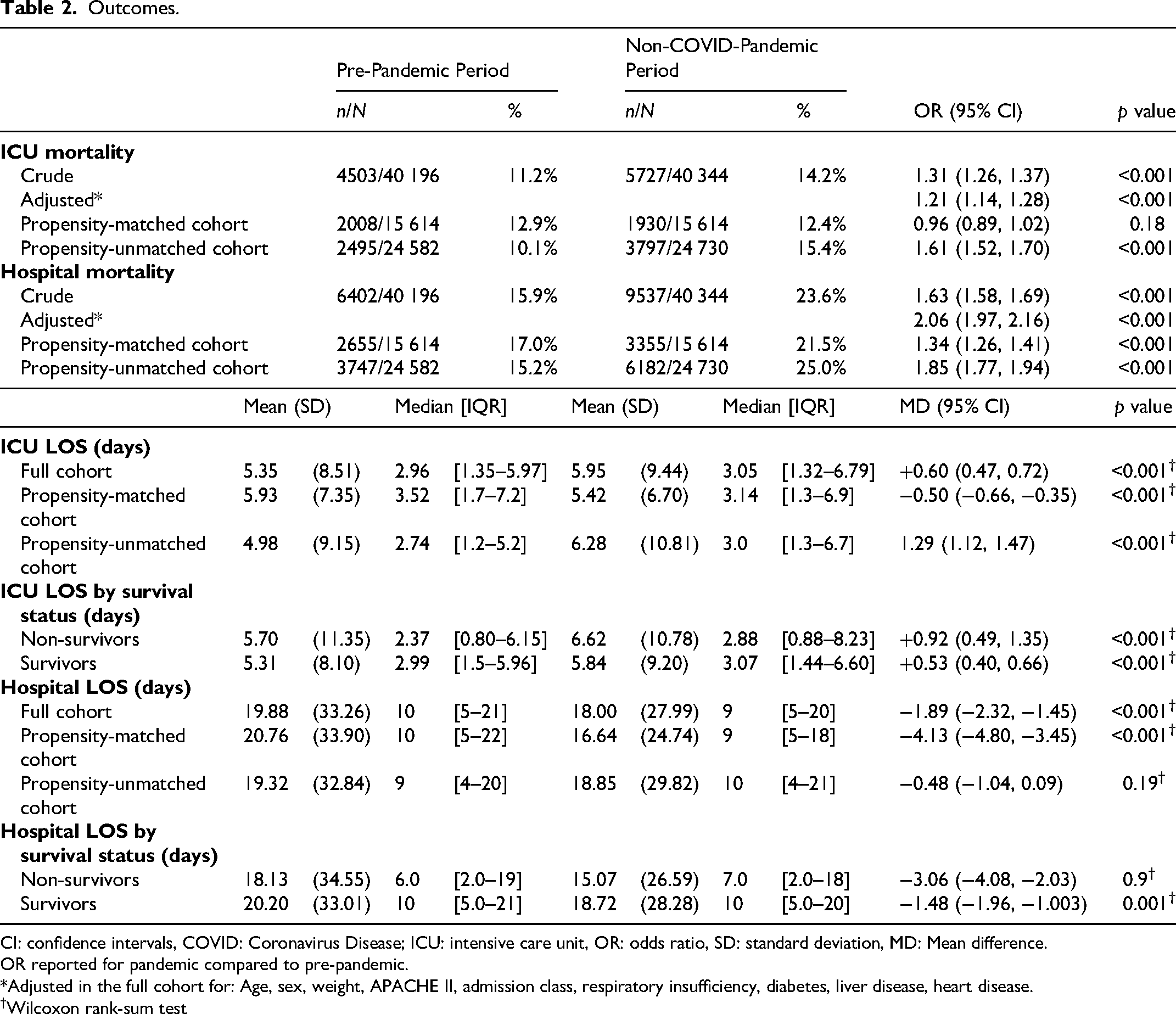
CI: confidence intervals, COVID: Coronavirus Disease; ICU: intensive care unit, OR: odds ratio, SD: standard deviation, MD: Mean difference.
OR reported for pandemic compared to pre-pandemic.
*Adjusted in the full cohort for: Age, sex, weight, APACHE II, admission class, respiratory insufficiency, diabetes, liver disease, heart disease.
Wilcoxon rank-sum test
In the propensity-matched cohort, ICU mortality was similar between the pre-pandemic and COVID-pandemic periods (12.9% vs 12.4%; MD: −0.5, OR 0.96, 95% CI 0.89-1.02; p = 0.18). (Table 2)
In the logistic regression model, patients in the pre-COVID period had higher odds of ICU survival compared with the COVID-19 period (OR 1.11, 95% CI 1.01-1.21; p = 0.023). Overall, the odds of ICU survival declined over time (OR per study month 0.99, 95% CI 0.99-0.99; p < 0.001). However, a significant interaction between period and study month was observed (interaction OR 1.01, 95% CI 1.01-1.01; p < 0.001), indicating a more favorable temporal trend in ICU survival during the pre-COVID period compared with the COVID period (Supplemental Table 5).
Hospital Mortality
The in-hospital mortality was significantly higher in pandemic period versus the pre-pandemic period (Figure 1), with 23.6% versus 15.9% (mean difference [MD]: +7.7%, OR: 1.63, 95% CI: 1.58-1.69, p < 0.001) for crude mortality rate, and adjusted mortality (aOR): 2.06, 95% CI: 1.97–2.16, p < 0.001) (Table 2).
In the propensity-matched cohort, hospital mortality was significantly higher during the COVID-19 pandemic period compared with the pre-pandemic period (21.5% vs 17.0%; MD: +4.5, OR 1.34, 95% CI 1.26-1.41; p < 0.001) (Table 2).
In the logistic regression model, patients in the pre-COVID period had higher odds of hospital survival compared with the COVID period (OR 1.08, 95% CI 1.00-1.17; p = 0.041). Overall, the odds of hospital survival declined significantly over time (OR per study month 0.98, 95% CI 0.98-0.98; p < 0.001). However, a significant interaction between intervention period and study month was observed (interaction OR 1.02, 95% CI 1.02-1.03; p < 0.001), indicating a more favorable temporal trend in hospital survival during the pre-COVID period compared with the COVID period (Supplemental Table 5).
ICU Length of Stay
The length of stay (LOS) in ICU was longer in the pandemic period compared to the pre-pandemic period for non-COVID patients (mean: 5.95 ± 9.44 days vs 5.35 ± 8.51 days, MD: +0.63 days [95% CI: 0.47-0.72], p < 0.001).
In the propensity-matched cohort, ICU length of stay was shorter during the COVID-pandemic period compared with the pre-pandemic period (mean: 5.42 ± 6.70 days vs 5.93 ± 7.35 days, MD: −0.50 days [95% CI: −0.66 to −0.35], p < 0.001) and the COVID-pandemic period (Table 2).
ICU LOS was shorter in the pre-pandemic period compared to the COVID-19 pandemic period for both ICU survivors (5.31 ± 8.10 days vs 5.84 ± 9.20 days, MD: +0.53 days [95% CI: +0.40 to 0.66], p < 0.001) and non-survivors (5.70 ± 11.35 days vs 6.62 ± 10.78 days, MD: +0.92 days [95% CI: 0.49 to 1.35], p < 0.001)
Hospital LOS
The hospital LOS was significantly shorter in the COVID-19 pandemic period compared to the pre-pandemic period (18.00 ± 27.99 days vs 5.35 ± 8.51 days, MD: −1.89 days [95% CI: −2.32 to −1.45], p < 0.001).
In the propensity-matched cohort, hospital LOS was shorter during the COVID-19 pandemic period (16.64 ± 24.74 days vs 20.76 ± 33.90 days, MD: −4.13 days [95% CI: −4.80 to −3.45], p < 0.001), reflecting a significant shift toward shorter hospitalizations (Table 2).
For hospital LOS among survivors, there was a statistically significant difference (15.07 ± 24.74 days vs 20.76 ± 33.90 days, MD: −1.48 days [95% CI: −1.96 to −1.003], p = 0.001) between the non-COVID pandemic period versus the pre-pandemic period. However, for non-survivors, there was no significant difference between the pre-COVID and COVID-19 periods (15.07 ± 24.74 days vs 18.13 ± 34.55 days, MD: −3.06 days [95% CI: −4.08 to −2.03], p = 0.9).
Subgroup Mortality Analysis
Table 3 demonstrates various subgroup differences in mortality between the pre-pandemic and pandemic non-COVID critically ill patient cohorts, alongside a subgroup forest plot in Figures 2a and 2b. ICU and hospital mortality were significantly higher during the pandemic compared to the pre-pandemic periods for the majority of subgroups: age 18–90, any sex, any SOFA, APACHE and CFS score.
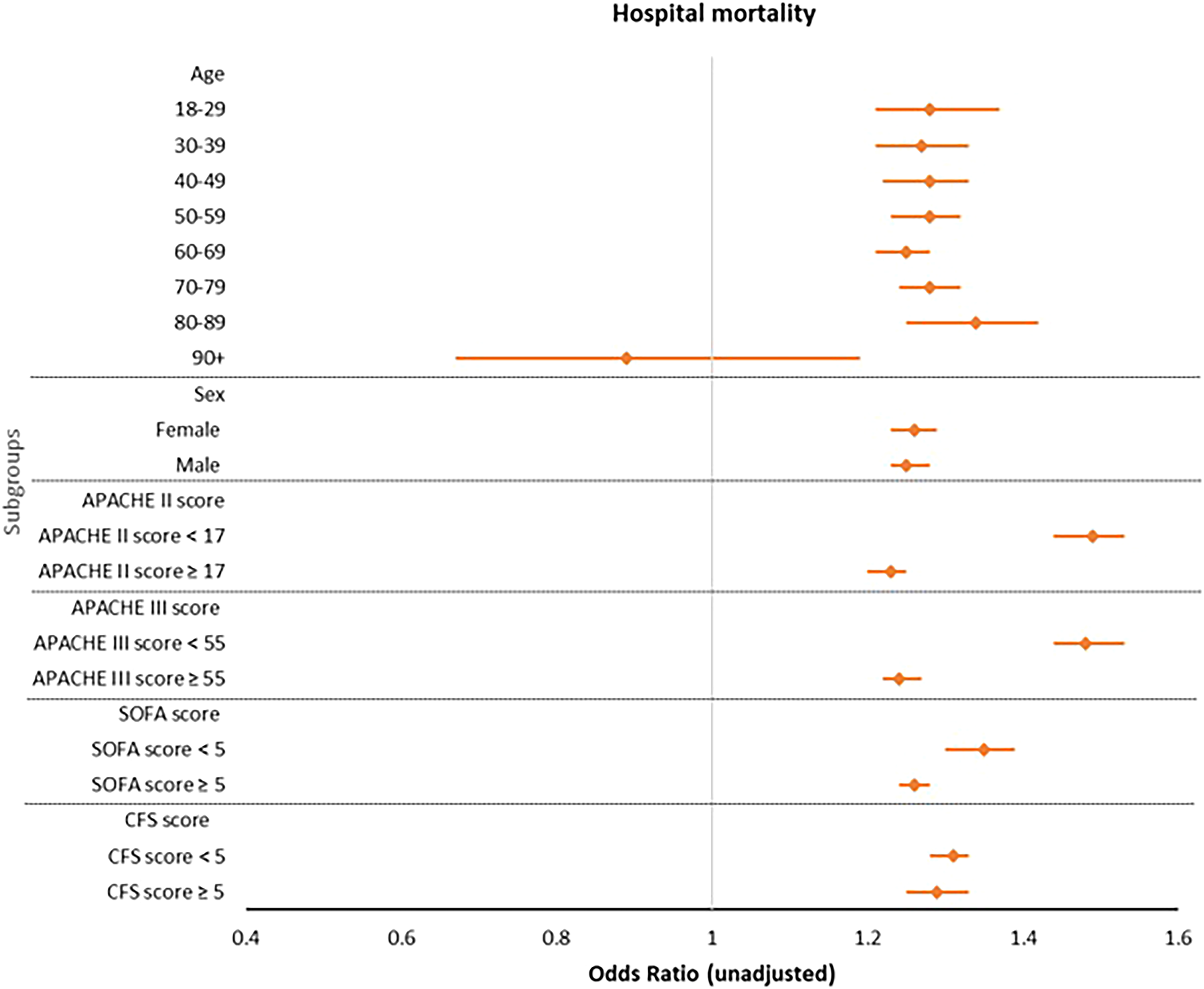
Hospital Mortality (Subgroup Analysis).
Subgroups Outcome.
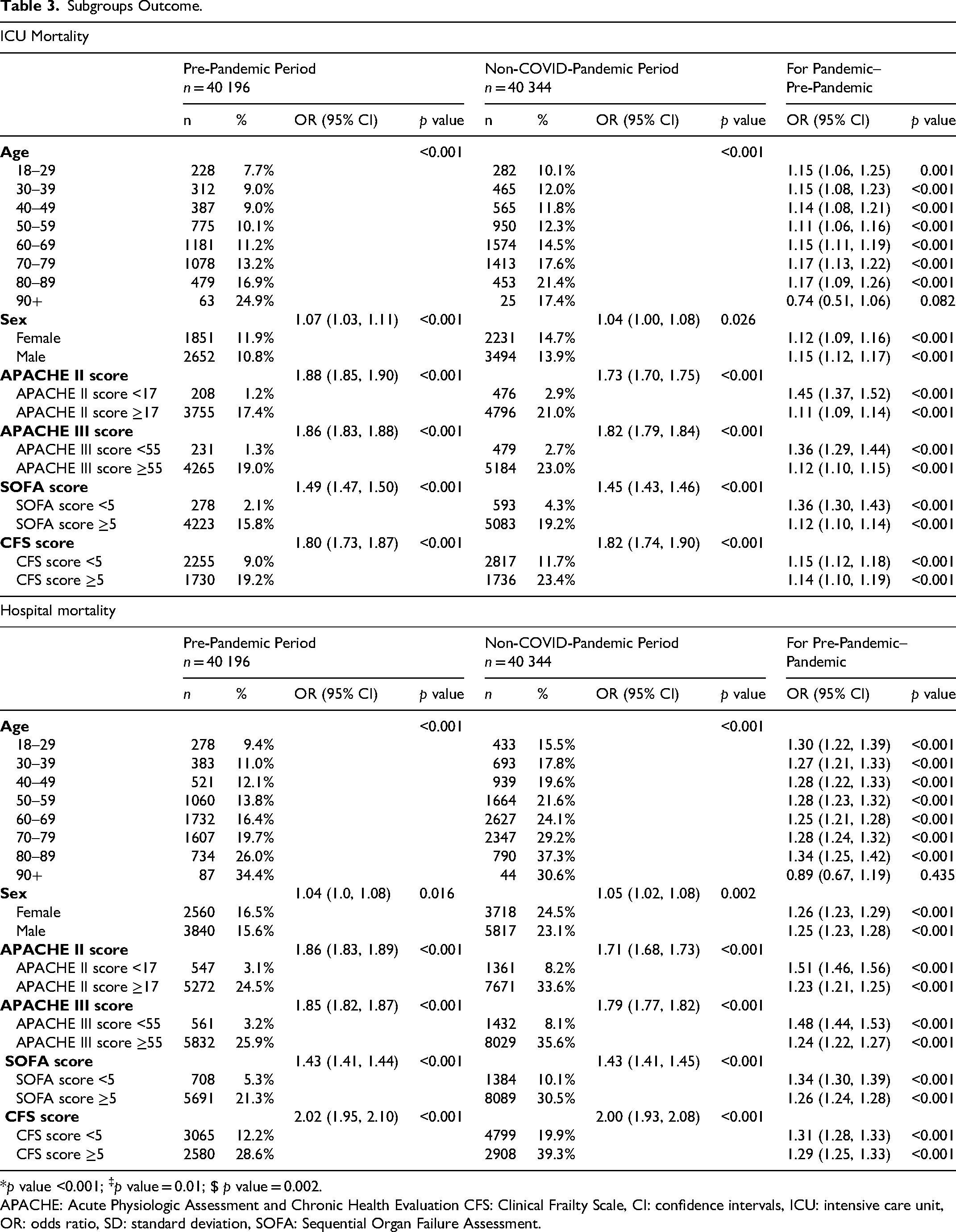
*p value <0.001; ‡p value = 0.01; $ p value = 0.002.
APACHE: Acute Physiologic Assessment and Chronic Health Evaluation CFS: Clinical Frailty Scale, CI: confidence intervals, ICU: intensive care unit, OR: odds ratio, SD: standard deviation, SOFA: Sequential Organ Failure Assessment.
Resource use and Organ Supports
Supplemental Table 6 shows the resource utilization, including ICU level organs supports (eg, ventilation, vasopressors, dialysis). There was a significant increase in the proportion of non-COVID ICU patients who needed invasive ventilation [71.7% versus 66.8%, p < 0.001] and median days of invasive ventilation in the pandemic period versus the pre-pandemic period (median: 1.6 days [IQR: 0.5-5.1] vs 1.0 days [0.3-3.5], p < 0.001. There was also a significant difference in days of utilization on an average per-patient basis for non-invasive ventilation and continuous renal replacement, but no difference in the hours of intermittent hemodialysis.
Discussion
In this retrospective, observational cohort study, we found an increase in crude and adjusted ICU and hospital mortality for patients with non-COVID during the COVID-19 pandemic compared to historical non-pandemic epochs. This observation was consistent across all subgroups, including age, sex, and illness severity scores. There was also longer ICU LOS but shorter hospital LOS during the pandemic vs the pre-pandemic period, likely secondary to increased mortality on the hospital wards, which was seen in both survivors and non-survivors.
This analysis provides insight into the potential trade-offs that have occurred for both patients with non-COVID illness and health systems’ capacity to meet standards of care. In multiple jurisdictions, excess all-cause mortality (USA: 72 deaths per 100 000 patient population, UK: 95 deaths/100,000, Spain: 102 deaths/100 000) has been reported over and above recorded COVID-19 deaths alone. 25 Multiple jurisdictions have reported increased ICU and hospital mortality for non-COVID critically ill patients as compared to historical norms.5,6,26–35 There is emerging literature that excess mortality is not only driven by COVID-19 deaths, 6 but there is also non-COVID excess mortality and morbidity, 5 including in intensive care units, 35 potentially secondary to disruptions of global healthcare services by the COVID-19 pandemic.5,6 The intensity of disruption (severity multiplied by duration) may have altered the apparent effects among non-COVID illnesses, leading to the variability observed for different jurisdictions and illnesses. This highlights that the pandemic itself has had unintended damage to the normal functioning of our health systems and negatively impacted outcomes for non-COVID patients.5,6,36
In Alberta ICUs, our non-COVID patient populations pre and during the pandemic are usually quite sick, as indicated by our higher illness severity scores (APACHE II) as compared to other jurisdictions (eg, Australia and New Zealand). Given that many ICUs in Alberta were overcapacity, with higher ICU thresholds for admission and considerations about enacting triage protocols, where only patients who had a higher chance of survival would be admitted. We believe that because the illness severity scores like APACHE II were worse during pandemic as compared to pre-pandemic levels, ICUs were still prioritizing very ill non-COVID ICU patients, despite having a large cohort of COVID-19 patients to deal with as well. As such, there may have been non-COVID patients who passed away on the wards while in hospital, as opposed to being admitted to ICU. And likely because of high capacity strain, both hospital survivors and non-survivors both had shorter lengths of stay.
Due to the “rule of rescue”, which states that we use available resources to save the life in front of us, even if those resources might be better used elsewhere.7,37 This can be at the expense of other patients. Because COVID-19 patients often had the highest acuity of illness, resources may have been preferentially directed to them, potentially at the expense of non-COVID critically ill patients. In healthcare, this tension arises between the injunction to do as much good as possible with scarce resources and the injunction to rescue identifiable individuals in immediate peril, regardless of cost. This tension can generate serious ethical and political difficulties for healthcare public policy makers faced with making explicit decisions about public funding. 38
Our findings demonstrated higher hospital mortality during the COVID-19 period despite a more favorable temporal trend in ICU survival. This may reflect improvements in ICU management over time, while persistent healthcare system strain, prolonged hospitalization, and post-ICU complications continued to adversely affect overall hospital outcomes. Previous studies have similarly shown that hospital strain and resource limitations were associated with worse in-hospital outcomes during the pandemic.37,38
Several studies have demonstrated that non-COVID patients experienced worse outcomes during the pandemic period, likely related to healthcare system strain, disrupted standards of care, delayed presentations, and resource reallocation. Hospital saturation, ICU occupancy, staffing shortages, and prioritization of COVID-19 patients may have contributed to these adverse outcomes despite improvements in critical care management over time. 6
There may be ongoing challenges. There has been evidence of increased ICU healthcare worker turnover,39–43 which can further compromise patient care going forward post-pandemic. There is evidence demonstrating an increased association with mortality when ICU staffing-to-patient ratio is compromised44–54 where patient-to-nurse ratios >2:1 are associated with increased adjusted relative risk (RR) of mortality of 2.3, and ratios >2.5:1 are associated with adjusted RR of 3.5. 55 Given this association, it will be important to monitor ICU healthcare worker turnover and to see if ICU mortality returns to historical norms or if they remain elevated post-pandemic.
The strengths of our study include adherence to STROBE guidelines, 13 presenting both crude and adjusted mortality for age, and using a multiple illness severity score to ensure proper interpretation of baseline cohort differences using logistic regression analysis. We also have extended the reference pre-pandemic cohort and pandemic cohorts to three years to observe both the pandemic and post-pandemic trends in mortality, as well as provide a more robust pre-pandemic control cohort to ensure proper adjustment of baseline prognostic risk factors. The data repositories covering all Alberta ICUs in the province (population-based study) are also a strength of this study. We are also one of the only studies to report on sedative, analgesic, and paralytic medication use during the pandemic period on non-COVID patients, which may explain the increased ventilator days for this cohort compared to pre-pandemic periods.
This study also has several limitations. First, we do not have data on morbidity or health-related quality of life in critically ill ICU patients from the registry population-level dataset, as mortality is not the only patient-important outcome to be studied. Second, we do not currently have capacity strain, bed census, and occupancy or healthcare provider (eg, registered nurses) to patient ratios data to supplement our analysis as a marker of potential reasons for increased mortality; however, this is an area of future research to determine if there are correlations between these capacity strain, ICU staffing, and increased mortality. Third, despite Alberta having a robust, single provincial repository for data, there was still a large proportion of patients who had missing data, potentially as a product of how busy clinicians were during the COVID-19 pandemic, that routine data capture and charting were foregone because of heightened patient care duties. Fourth, despite our adjustment when we looked at mortality, there are likely other confounders that were not accounted for during logistic regression modeling analysis, which may impact the results. Fifth, the difference between adjusted regression and propensity-matched estimates in the ICU mortality could be the result of the reduction in the sample size and the change in precision with matching for PSM. These methods target different populations; regression models estimate conditional associations in the full cohort, whereas PSM restricts analysis to patients with overlapping propensity scores, potentially excluding extreme-risk individuals and altering covariable weighting, especially when the PSM matching of the cohorts is a low percentage of the overall full cohort (PSM: 39%). Thus, discrepancies likely reflect methodological differences rather than conflicting results, and reporting both analyses provides complementary evidence. Furthermore, there is still consistent messaging that both the adjusted regression and the propensity-matched estimates show an increased mortality for hospital mortality. The unmatched non-COVID propensity cohort shows increased mortality, which is likely the explanation for the adjusted regression increased mortality, as this cohort is clinically different, potentially from the pre-pandemic cohort, including having higher illness severity scores and higher mortality. Additionally, given that the reason for admission is input by clinicians, missing data (eg, CFS, admission reason) is likely within the registry database, due to clinicians not routinely inputting admission diagnoses due to other clinical priorities at the time, which was a limitation of the registry databases used for this manuscript.
Finally, there was a potential limitation in the possibility of COVID-19 misclassification. COVID-19 status was defined based on a documented diagnosis within 14 days of hospital admission; therefore, some patients with presymptomatic infection or initially false-negative testing may have been misclassified as non-COVID, particularly during the early phases of the pandemic when testing availability and sensitivity were more limited. However, the extent of such misclassification is likely small and unlikely to have materially affected the overall study findings.
Conclusion
The COVID-19 pandemic had effects on non-COVID illness, including increased ICU and hospital mortality (both crude and adjusted), increased ICU length of stay, but decreased hospital length of stay (perhaps secondary to increased death) in Alberta ICUs and hospitals. Informing public healthcare policy and decision-makers of the potential pandemic effects is crucial to mitigate the impact of the COVID-19 pandemic on both COVID-19 and non-COVID patients, in particular, excess mortality, morbidity, and disruptions in care.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-1-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-2-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-3-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-3-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-4-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-4-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-5-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-5-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-6-jic-10.1177_08850666261465346 - Supplemental material for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study
Supplemental material, sj-docx-6-jic-10.1177_08850666261465346 for Intensive Care Unit and Hospital Mortality for non-COVID Critically ill Patients Before, and During the COVID-19 Pandemic in Alberta Hospitals: Retrospective, Observational Cohort Study by Vincent I. Lau, Fadi Hammal, Fernando G. Zampieri, Wendy I. Sligl, Constantine J. Karvellas, Michael Jacka, Demetrios J. Kutsogiannis, Dawn Opgenorth, M. Elizabeth Wilcox, Kirsten M. Fiest, Daniel J. Niven, Henry T. Stelfox, Danny J. Zuege, Ken Parhar, Sean M. Bagshaw and Oleksa Rewa in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
Not applicable.
Authors’ Contributions
All authors attest to the originality of the text, and the originality of any/all supporting tables, images, and supplementary electronic materials as related to this document, except where otherwise indicated that the material has been reproduced with the appropriate permissions. We also hereby affirm that ethical approval for this work was obtained as appropriate to this work.
All authors have made material contributions to this manuscript according to the rules of authorship as explained in the Instructions for Authors. We also accept the terms of reference for manuscript submission and editorial peer review as outlined in the Instructions for Authors.
Availability of Supporting Data
Not applicable.
Consent for Publication
We agree to the terms of any copyright transfer statements, which shall be deemed in effect if and when the manuscript is accepted for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Human Ethics and Consent to Participate Declarations
No individual patient consent was required; data were obtained without any patient identifiers. The study was conducted in accordance with applicable ethical standards, and institutional review board approval was obtained from the University of Alberta Health Research Ethics Board (File # PRO00130042, approved April 14, 2023).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.