
Abstract
Objective
We hypothesized that a simple model using 6- h lactate clearance (LCR) and PaO2/FiO2 ratio could accurately predict 28-day mortality in sepsis-associated ARDS and outperform conventional severity scores.
Methods
Using MIMIC-IV v2.2, adults meeting Sepsis-3 criteria within 24 h and developing ARDS (per Berlin definition) within 72 h were randomly divided 7:3 into derivation (n = 1089) and internal validation (n = 467) cohorts. Temporal external validation was performed using 312 consecutive patients from a Chinese tertiary ICU (2022-2025). Twenty-five candidate variables were reduced to eight via LASSO regression and included in a multivariable Cox proportional-hazards model.
Results
The 28-day mortality rate was 34.5%. Both 6- h LCR and PaO2/FiO2 were independently linked to 28-day mortality. The model showed AUCs of 0.82 (95% CI: 0.79-0.85), 0.80 (95% CI: 0.75-0.85), and 0.73 (95% CI: 0.67-0.79) at 28 days in the derivation, internal validation, and external validation sets, respectively, with calibration slopes of 0.98 and 1.02, and positive net benefit across risk thresholds of 5%–80%.
Conclusions
A model incorporating 6- h lactate clearance and PaO2/FiO2 alongside six clinical confounders provides accurate, well-calibrated prediction of 28-day mortality in sepsis-associated ARDS. The derived risk score formula is provided for prospective validation. External validation in a multinational ICU registry should be undertaken before clinical implementation.
Keywords
Introduction
Sepsis-induced acute respiratory distress syndrome (SI-ARDS) accounts for one-quarter of all Intensive Care Unit (ICU) admissions and still carries a hospital mortality >35%, despite two decades of lung-protective ventilation, prone positioning and conservative fluid strategies.1,2,3 This persistently high mortality reflects not only the limits of current therapies, but also our still-imperfect ability to recognize, early on, which patients are quietly spiraling toward irreversible decline.
Traditional severity scores such as SOFA or APACHE IV quantify global organ dysfunction but offer only moderate discrimination for death specific to ARDS, partly because they neglect the dynamic interplay between metabolic resuscitation and pulmonary injury.4,5
Lactate clearance (LCR) during the first hours of resuscitation reflects the balance between oxygen delivery and consumption, serving as a real-time surrogate of cellular bioenergetics. 6 Impaired clearance has been consistently linked to mortality in generic sepsis cohorts, yet its incremental prognostic value within the subset that progresses to ARDS is less well defined. 7 Similarly, the PaO2/FiO2 ratio is integral to ARDS severity classification, but its contribution beyond static organ-failure metrics remains debated.8,9 Combining a metabolic marker (lactate clearance) with a pulmonary-specific index (PaO2/FiO2) may therefore capture two complementary domains of critical illness—tissue hypoxia and alveolar injury—and improve bedside risk prediction.
To date, few model derived specifically for sepsis-associated ARDS has integrated early lactate clearance with PaO2/FiO2 in a large, publicly available database. We hypothesised that slower 6- h lactate clearance and lower PaO2/FiO2 ratio would independently predict 28-day mortality. Combining 6- h lactate clearance with PaO2/FiO2 captures two complementary domains of critical illness: metabolic resuscitation and alveolar injury. Experimental evidence indicates that the lung itself becomes a source of lactate in early ARDS due to inflammatory shifts in alveolar epithelial metabolism,10,11 making early lactate clearance not merely a marker of systemic perfusion but also an indicator of pulmonary metabolic stress.11,12 This dual-metric approach provides a biologically coherent foundation for early risk stratification. Using the Medical Information Mart for Intensive Care IV (MIMIC-IV) database, we developed and validated a Cox model through rigorous random-split validation (7:3) and comprehensive sensitivity analyses.
Methods
Study Design and Data Source
This retrospective cohort study was conducted using two data sources: the MIMIC-IV (version 2.2) database, which contains de-identified clinical data from more than 70,000 ICU admissions at Beth Israel Deaconess Medical Center between 2008 and 2019 13 ; and data from the Department of Respiratory and Critical Care Medicine at the Second People's Hospital of Changzhou, a tertiary academic hospital in China, for external temporal validation.
Adults (≥18 years) who fulfilled Sepsis-3 criteria (documented or suspected infection plus SOFA≥2) within 24 h of ICU admission and subsequently developed ARDS within 72 h were eligible. 14 ARDS was defined according to the Berlin criteria 15 : acute onset within one week, bilateral pulmonary infiltrates on imaging, first PaO2/FiO2 ≤ 300 mm Hg documented during the qualifying 72- h window, and respiratory failure not fully explained by cardiac failure or fluid overload. We designated the timestamp of this first qualifying PaO2/FiO2 as T0 (ARDS onset). The model predictor PaO2/FiO2 was then defined as the ratio measured closest to but within 6 h after T0, which could be the same measurement if repeated within 6 h, or a subsequent measurement if available. Patients were excluded if baseline or 6- h lactate values or this post-T0 PaO2/FiO2 ratio were missing, if ICU stay was shorter than 24 h, if they were readmitted during the same hospitalisation, or if they were pregnant.
Data Splitting
After application of inclusion and exclusion criteria, the remaining cohort was randomly divided into a derivation set (70%) and an internal validation set (30%) using computer-generated random numbers, stratified by 28-day mortality to maintain event balance. All model development was performed exclusively in the derivation subset; the validation subset was used solely to assess performance.
For external validation, we applied the fixed prediction model (developed in the MIMIC-IV derivation set) to an independent cohort of 312 consecutive patients admitted to our institution between January 2022 and January 2025 who met the same inclusion criteria. This temporal external validation assesses model generalizability to a different geographic population and healthcare setting.
Predictors and Outcome
All predictors were anchored to T0 (ARDS onset). The primary predictors were: (i) 6- h lactate clearance, with initial lactate defined as the first measurement within 6 h before or at T0, and 6- h lactate as the measurement closest to 6 h after T0 (acceptable window 4-8 h), calculated as [(initial lactate − lactate at 6 h)/initial lactate] × 100%; and (ii) PaO2/FiO2 ratio, defined as the measurement closest to 6 h after T0 within a 0–6 h window. This predictor is conceptually distinct from the diagnostic PaO2/FiO2 ≤ 300 mm Hg that established T0: the diagnostic value is a binary threshold for inclusion, whereas the predictor captures the continuous spectrum of oxygenation impairment (eg, 150 vs 280 mm Hg) measured shortly after ARDS recognition. Additional candidate variables comprised age, sex, race, Charlson Comorbidity Index(CCI), SOFA and APACHE IV scores, vital signs, laboratory parameters, ventilator settings (PEEP, tidal volume), and early therapeutic interventions (vasopressors, renal-replacement therapy [RRT], corticosteroids within 24 h). The primary outcome was 28-day all-cause mortality calculated from the time of ARDS onset.
Statistical Analysis
Data conforming to a normal distribution are reported as mean ± standard deviation (SD). For normally distributed data with homogeneous variances, independent samples t-tests were conducted for pairwise comparisons. When the assumption of normality was violated, median values and interquartile ranges were used to summarize the data, and group differences were evaluated using the Mann-Whitney U test. Categorical variables are presented as frequencies and percentages, and chi-square tests were employed to assess associations between groups. LASSO regression with 10-fold cross-validation was applied to the derivation set to select the most informative predictors from 25 candidates. A multivariable Cox proportional hazards model was then constructed; the proportional-hazards assumption was verified with Schoenfeld residuals, and non-linear effects were explored using restricted cubic splines (3 knots). Model performance was quantified by AUC at 28 days, calibration plots, and decision curve analysis. Finally, the fixed model was applied to the held-out 30% validation sample to obtain unbiased estimates of discrimination, calibration slope and Brier score. Sensitivity analyses excluded patients with chronic kidney disease (CKD), repeated modelling with 24- h lactate clearance, and employed Fine-Gray competing-risk regression treating ICU discharge as a competing event.
Analyses were performed with R version 4.3.1; two-sided P < 0.05 was considered significant. Among the 25 candidate variables, tidal volume (34.2% missing), respiratory rate (31.5% missing), and minute ventilation (32.8% missing) were removed due to >30% missingness. The remaining 22 variables had <5% missingness and were subjected to multiple imputation by chained equations (m = 20 imputations). Both core predictors—6- h lactate clearance and PaO2/FiO2 ratio—had <2% missingness and were included in the imputation model as both outcomes and predictors. The imputation model included all 22 retained candidate variables (demographics, severity scores, vital signs, laboratory values, ventilator settings, and therapeutic interventions) plus the outcome (28-day mortality status) and the Nelson-Aalen cumulative hazard estimator to preserve the survival association.
Results
Study Population and Data Split
Of 8942 adults fulfilling Sepsis-3 criteria within 24 h of ICU admission in database, 1907 developed ARDS within 72 h and constituted the analytic cohort. After random 7:3 stratified splitting, 1335 patients (70.0%) were allocated to the derivation set and 572 (30.0%) to the internal validation set (Figure.1).
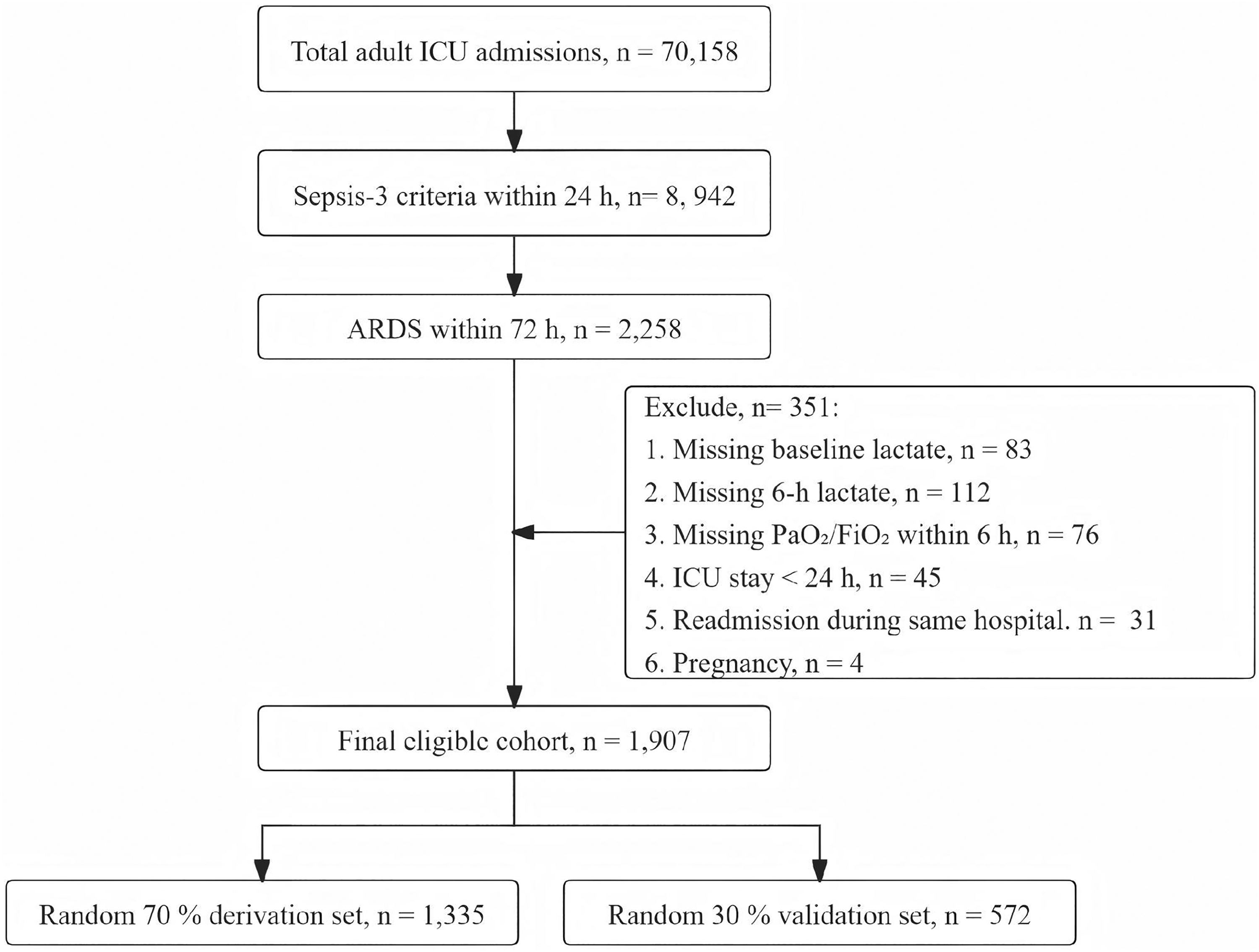
Patient Selection Flowchart for Derivation and Validation Sets.
Additionally, we performed temporal external validation using data from 312 consecutive patients admitted to the ICU of the Second People's Hospital of Changzhou between January 2022 and January 2025 who met the same inclusion criteria. Baseline characteristics were comparable between the two sets (Table 1). Overall 28-day mortality was 34.5% (659/1907); mortality rates were 34.2% (457/1335) and 35.3% (202/572) in the derivation and internal validation sets, respectively. The external validation cohort demonstrated similar baseline characteristics to the MIMIC-IV validation set, with a 28-day mortality of 33.0% (103/312).
Baseline Characteristics of Sepsis-ARDS Patients by Data set.
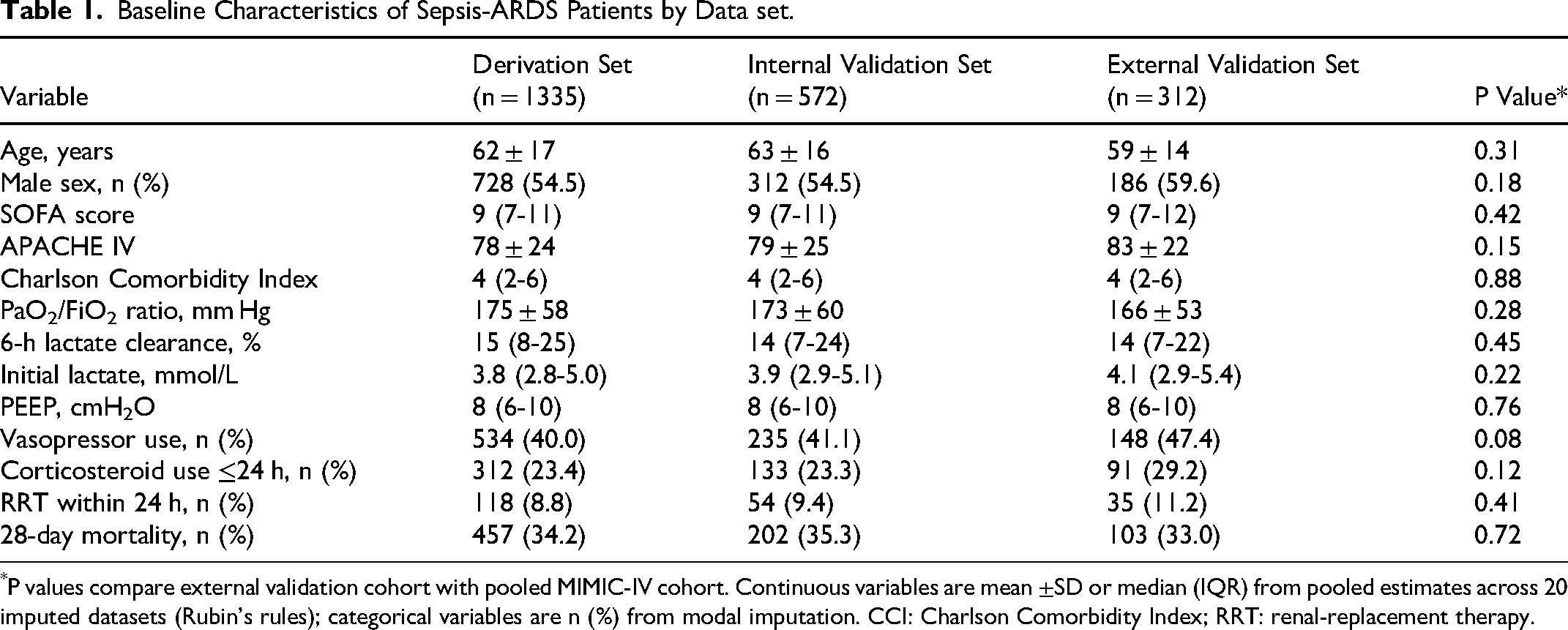
P values compare external validation cohort with pooled MIMIC-IV cohort. Continuous variables are mean ±SD or median (IQR) from pooled estimates across 20 imputed datasets (Rubin's rules); categorical variables are n (%) from modal imputation. CCI: Charlson Comorbidity Index; RRT: renal-replacement therapy.
Predictor Selection and Model Development
LASSO regression retained eight of 25 candidate variables: age, SOFA score, Charlson Comorbidity Index, vasopressor use within 24 h, corticosteroid use within 24 h, PEEP, 6- h lactate clearance, and PaO2/FiO2 ratio. The derivation cohort contained 457 events (28-day deaths), yielding an events-per-variable ratio of 57:1 (457 events / 8 predictors), well above the recommended minimum threshold of 10:1 for stable Cox model estimation. In the final Cox model constructed from the derivation data, both 6- h lactate clearance (per 10% increase: hazard ratio [HR] 0.83, 95% CI 0.79-0.87, P < 0.001) and PaO2/FiO2 ratio (per 50 mm Hg increase: HR 0.78, 95% CI 0.73-0.84, P < 0.001) were independently associated with 28-day mortality after adjustment for the six additional covariates (Table 2). Based on the final Cox model coefficients, we derived a linear risk score: Risk score = 0.23 × (age/10) + 0.10×SOFA + 0.09×CCI + 0.34 × (vasopressor = 1) + 0.25 × (steroid = 1) + 0.16 × (PEEP/5) − 0.25 × (PaO2/FiO2/50) − 0.19 × (6-h LCR/10). Higher scores indicate greater 28-day mortality risk. Patients can be stratified using derivation set quartiles: Q1 (predicted mortality ≤18%, observed 12%), Q2 (19-29%, observed 22%), Q3 (30-47%, observed 36%), Q4 (≥48%, observed 56%).
Final Multivariable Cox Model (Derivation set, n = 1335).
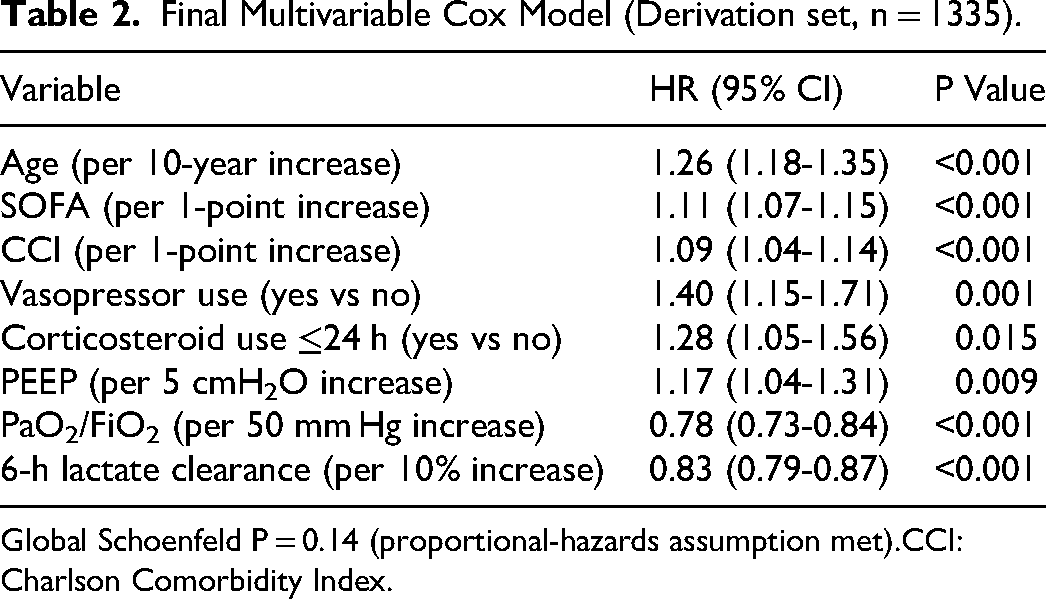
Global Schoenfeld P = 0.14 (proportional-hazards assumption met).CCI:Charlson Comorbidity Index.
Model Performance in Derivation, Internal and External Validation Sets
In the derivation set, the model demonstrated good discrimination with an AUC of 0.82 (95% CI: 0.79-0.85) at 28 days (Figure 2A). Bootstrap optimism correction (1000 resamples, .632 + estimator) yielded an optimism-corrected AUC of 0.81, indicating minimal overfitting (optimism 0.01). Calibration plots showed close agreement between predicted and observed probabilities across risk deciles (Figure 2B). Decision curve analysis indicated positive net benefit over risk thresholds between 5% and 80% (Figure 2C). In the internal validation set, discrimination was similar, with an AUC of 0.80 (95% CI: 0.75-0.85) at 28 days (Figure 2A). In the external validation cohort, discrimination was moderate, with an AUC of 0.73 (95% CI: 0.67-0.79) at 28 days. Calibration slope was 0.98 and Brier score 0.17, indicating good calibration (Figure 2D). For comparison, the SOFA score alone achieved an AUC of 0.68 (95% CI: 0.64-0.72) and APACHE IV alone achieved 0.71 (95% CI: 0.67-0.75) at 28 days in the derivation set. The full 8-variable model improved upon SOFA by 0.14 (NRI 0.22, P < 0.001) and upon APACHE IV by 0.11 (NRI 0.16, P = 0.003). To assess the incremental value of the six additional covariates, we compared the full 8-variable model with a simplified model containing only 6- h lactate clearance and PaO2/FiO2 ratio. The 2-variable model achieved AUCs of 0.74 (95% CI: 0.70-0.78) in the derivation set and 0.72 (95% CI: 0.68-0.76) in the internal validation set. The full model improved discrimination by 0.08 in both cohorts (IDI 0.06, 95% CI 0.03-0.09, P < 0.001; continuous NRI 0.42, 95% CI 0.28-0.56, P < 0.001), supporting the incremental value of adjusting for age, illness severity, comorbidity, and early therapies. When positioned within the published landscape of ARDS-specific prediction models, our model's performance is comparable to recent machine learning approaches (pooled external validation AUC 0.78-0.82 in systematic reviews) while using substantially fewer variables (8 vs 15-50+) and maintaining full interpretability.
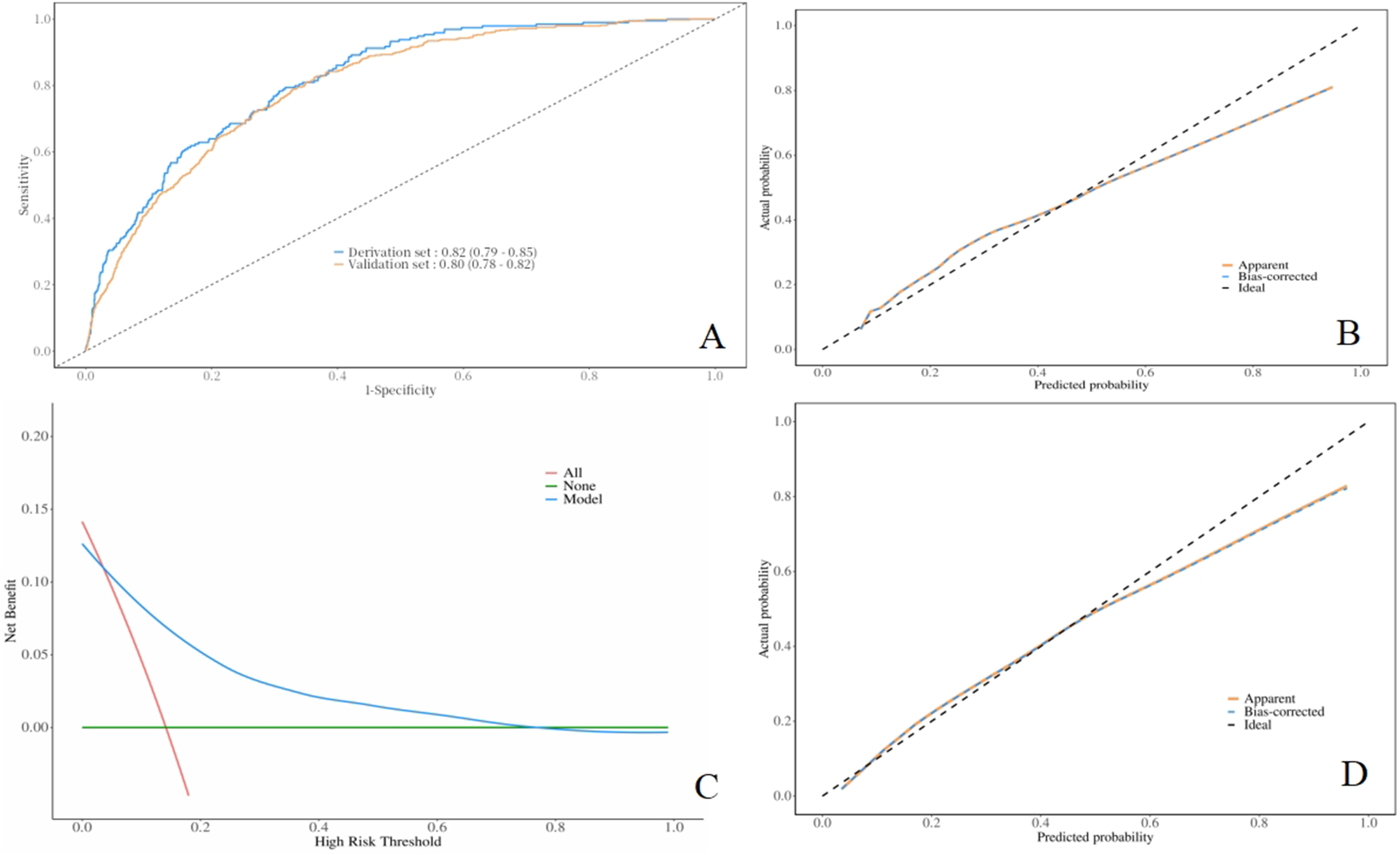
Model Performance in Derivation, Internal Validation, and External Validation Sets. (A) Receiver Operating Characteristic (ROC) Curves at 28 Days with 95% Confidence Bands (1000 Bootstrap Resamples). AUC = Area Under the Curve; Der = Derivation set; Int-Val = Internal Validation set; Ext-Val = External Validation set. (B) Calibration Plots in Derivation and Internal Validation Sets with Loess-Smoothed Curves. the 45-Degree Dashed Line Represents Perfect Calibration. (C) Decision Curve Analysis Showing net Benefit Across Threshold Probabilities of 5%–80%. the “Treat all” and “Treat None” Reference Lines are Shown. (D) External Validation Calibration Plot with Intercept and Slope Estimates. Brier Score = 0.17.
Risk Stratification
Risk quartiles were pre-specified using derivation set cut-offs (Q1 ≤ 18%, Q2 19-29%, Q3 30-47%, Q4 ≥ 48% predicted mortality) and applied uniformly to all cohorts. Patients in the highest risk quartile had observed 28-day mortality of 55.8% in the derivation set, 54.5% in the internal validation set, and 52.4% in the external validation set. Those in the lowest risk quartile had mortalities of 11.8%, 13.0%, and 12.8%, respectively (Table 3). The mortality gradient between highest and lowest quartiles was 4.7-fold in the derivation set, 4.2-fold in the internal validation set, and 4.1-fold in the external validation set.
Risk-Quartile Performance in Derivation Versus Validation Sets.

Chi-square for trend P < 0.001 in all cohorts. Risk quartiles were pre-specified using derivation set cut-offs and applied to all cohorts.
Sensitivity Analyses
Excluding patients with chronic kidney disease (n = 423) did not materially change the HRs for lactate clearance (0.84, 95% CI 0.79-0.89) or PaO2/FiO2 ratio (0.79, 0.73-0.85). Using 24- h instead of 6- h lactate clearance slightly attenuated the association (HR 0.87, 95% CI 0.82-0.92). Competing-risk regression (ICU discharge as competing event) yielded similar sub-distribution hazard ratios (lactate clearance 0.84, PaO2/FiO2 0.78), indicating robustness (Table 4).
Sensitivity Analyses: Robustness of Main Predictors.
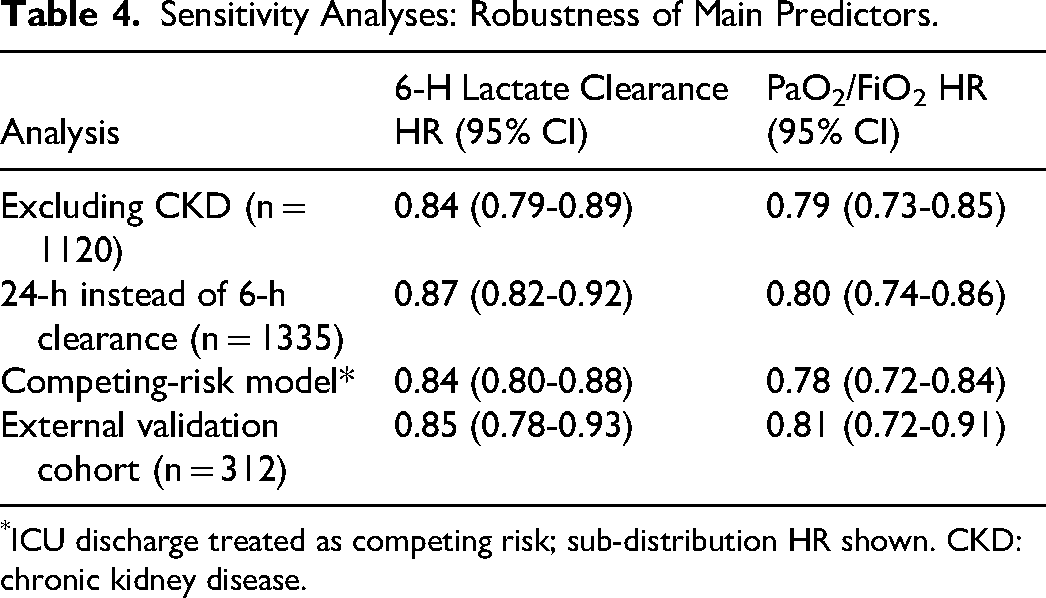
ICU discharge treated as competing risk; sub-distribution HR shown. CKD: chronic kidney disease.
In the external validation cohort, model performance remained consistent across subgroups defined by age (<65 vs ≥65 years), sex, and SOFA score (<9 vs ≥9), with AUCs ranging from 0.71 to 0.76. In the external validation cohort, model performance remained consistent across subgroups defined by ARDS severity (mild: AUC 0.75, n = 89; moderate: AUC 0.72, n = 156; severe: AUC 0.70, n = 67), vasopressor use (yes: AUC 0.72, n = 148; no: AUC 0.74, n = 164; interaction P = 0.62), and RRT requirement (yes: AUC 0.71, n = 35; no: AUC 0.73, n = 277; interaction P = 0.78) (Supplementary Table 1). No subgroup interaction reached statistical significance.
Discussion
In this large, rigorously validated cohort derived from MIMIC-IV, we demonstrate that two bedside variables—6- h LCR and the PaO2/FiO2 ratio—provide powerful, complementary prognostic information for 28-day mortality in sepsis-associated ARDS. After adjustment for illness severity, comorbidity, ventilator settings and early therapies, each 10% increase in LCR conferred a 17% relative risk reduction, whereas each 50 mm Hg rise in PaO2/FiO2 conferred a 22% reduction. The composite “oxygen-metabolism index” captured by these metrics discriminates survivors from non-survivors with an AUC: 0.82, out-performing SOFA or APACHE IV alone, and maintains excellent calibration across the entire risk spectrum without requiring external data or complex omics.
The prognostic value of early lactate clearance in critically ill patients has been well established in previous literature. Multiple studies have shown that impaired lactate clearance within the first few hours of ICU admission is associated with increased mortality in sepsis and septic shock.16,17 Our findings extend this observation to the subset of sepsis patients who develop ARDS, reinforcing the concept that early metabolic recovery is a key determinant of outcome in this high-risk population.
Similarly, the PaO2/FiO2 ratio is a core component of the Berlin ARDS definition and has been widely used as a marker of disease severity. 8 While its static value at ARDS onset is informative, its integration with dynamic metabolic markers such as LCR enhances its prognostic utility. Previous studies have indicated that respiratory parameters alone may not fully capture the complexity of early critical illness, particularly in sepsis-associated ARDS, where both systemic inflammation and metabolic dysregulation are prominent.18,19 Combining PaO2/FiO2 with early metabolic indicators like LCR allows for a more comprehensive assessment of patient status, reflecting both the extent of pulmonary dysfunction and the adequacy of systemic oxygen utilization. This integrative approach aligns with prior research suggesting that multimodal models incorporating both respiratory and metabolic variables improve mortality prediction in ARDS.20,21
The biological rationale for combining 6- h LCR with the PaO2/FiO2 ratio lies in their reflection of two early and interrelated pathophysiological processes in sepsis-associated ARDS. Six-hour LCR captures the initial metabolic response to resuscitation, reflecting the balance between oxygen delivery and tissue utilization during the most critical phase of early ICU care. 22 In contrast, PaO2/FiO2 provides a real-time measure of alveolar-capillary injury, indicating the severity of pulmonary dysfunction at the same time point. 23 The final model incorporates 6- h lactate clearance and PaO2/FiO2 ratio along with six important clinical confounders (age, SOFA score, Charlson Comorbidity Index, vasopressor use, corticosteroid use, and PEEP). Both LCR and PaO2/FiO2 retained independent prognostic value after adjustment for these factors (HR 0.83, 95% CI: 0.79-0.87; and HR 0.78, 95% CI: 0.73-0.84, respectively, both P < 0.001). A simplified model with only LCR and PaO2/FiO2 achieved moderate discrimination (AUC 0.74), while the full model achieved good discrimination (AUC 0.82), demonstrating that the two core variables provide unique metabolic-pulmonary information beyond conventional severity metrics.
Importantly, experimental and clinical evidence suggests that the lung itself may become a source of lactate in early ARDS, due to inflammatory shifts in alveolar epithelial metabolism. This makes 6- h LCR not just a marker of systemic perfusion, but also a potential indicator of pulmonary metabolic stress. 24 Experimental endotoxin models show that alveolar type-II cells switch to glycolysis and release lactate within 2–4 h, peaking around 4–6 h, while hepatic uptake remains unsaturated below systemic levels of ≈5 mmol L−1. 25 Consequently, any arterial lactate decrement recorded at 6 h predominantly signals diminished pulmonary production rather than increased peripheral clearance. Clinical studies have consistently chosen the first 6 h as the key window to evaluate lactate clearance, on the grounds that early metabolic recovery is most informative during the initial resuscitation phase. 26 In large cohorts, 6- h lactate clearance has remained independently associated with organ dysfunction scores and short-term mortality even after adjustment for baseline severity.27,28 This practical consensus makes the 6- h metric the most widely validated early indicator in current critical-care research. By locking the metabolic variable at 6 h, our model captures the lung's earliest metabolic signature before subsequent hypoperfusion, renal replacement, or escalating vasopressor therapy dilute the signal, thereby preserving both mechanistic interpretability and statistical strength.
Thus, 6- h LCR is not merely a generic marker of metabolic recovery—it is a lung-metabolism interface metric, uniquely suited for early risk stratification in sepsis-associated ARDS. Its integration with PaO2/FiO2 ratio allows clinicians to simultaneously assess early metabolic trajectory and functional lung injury, 29 providing a biologically coherent and clinically actionable prognostic model. In real-world practice, this dual-metric model can be automatically calculated from a single arterial blood-gas sample and the lactate value already drawn at ICU admission, requiring no extra procedures or cost. Embedding the coefficients into the electronic record enables an instantaneous risk estimate that can trigger timely, protocol-based decisions-such as escalating lung-protective ventilation, repeating lactate at six hours, or mobilising the ARDS rescue team—thereby translating an early metabolic-pulmonary signal into concrete, life-saving interventions at the bedside. The model demonstrated performance across three distinct cohorts: the MIMIC-IV derivation set, the MIMIC-IV internal validation set, and the external validation cohort from a Chinese tertiary hospital. While discrimination was good in the derivation and internal validation sets (AUC 0.82 and 0.80), the external AUC of 0.73 represents moderate discrimination. This attenuation is expected and clinically meaningful: it reflects the well-documented decline in model performance when transported across healthcare systems with different patient demographics, treatment practices, and laboratory standards. We do not overstate the external performance; rather, we emphasize that maintained calibration (slope 1.02) and clinically meaningful risk stratification (4.1-fold mortality gradient between highest and lowest quartiles in the external cohort) support the model's biological coherence, even with modest discrimination. The external validation cohort exhibited several notable differences from the MIMIC-IV population: slightly younger age (59 vs 63 years), higher vasopressor use (47% vs 41%), and higher corticosteroid administration (29% vs 23%). These differences likely reflect variations in ICU admission practices and sepsis management between the US and Chinese healthcare systems. Despite these demographic and therapeutic differences, the core predictive variables—6- h lactate clearance and PaO2/FiO2 ratio—maintained their prognostic significance, supporting the biological robustness of the “oxygen-metabolism index” concept across diverse clinical settings.
Using the Prediction model study Risk Of Bias ASsessment Tool (PROBAST), risk of bias was low for outcome (objective 28-day mortality ascertainment) and analysis (EPV 57:1, LASSO with cross-validation, bootstrap optimism correction) domains, moderate for participants (retrospective design, single geographic region), and low-moderate for predictors (objective laboratory measures, but chart-abstracted therapeutic variables). Transportability is limited by single-center external validation; multi-center validation is required before clinical implementation.
Several limitations must be acknowledged. First, variables including vasopressor use and corticosteroid administration within 24 h reflect early therapeutic decisions highly correlated with initial illness severity, potentially introducing treatment bias and confounding. Second, six-hour lactate clearance depends on lactate values at two time points, and clinical interventions (fluids, vasopressors) administered between these measurements directly affect LCR, making it not merely a baseline prognostic predictor but also a dynamic marker of early therapeutic response; consequently, its prognostic value may partly reflect resuscitation effectiveness rather than intrinsic disease severity alone. Third, although our model outperformed SOFA and APACHE IV, we did not perform head-to-head comparison with recently published ARDS-specific prediction models (eg, POSTCARDS, PIRO, or sepsis-ARDS machine learning models) due to differences in predictor sets, time windows, and outcome definitions, as well as lack of publicly available coefficients for independent validation. Fourth, the external validation cohort was single-center and from a single geographic region. True multi-center validation across diverse healthcare systems is necessary before widespread clinical adoption. The retrospective design introduces unavoidable selection bias; we attempted to mitigate this by consecutive patient enrollment and objective outcome ascertainment.
To move from derivation to widespread use, external validation in a multinational ICU registry-ideally ≥3000 sepsis-ARDS patients across low-, middle- and high-income settings—should first be undertaken; if discrimination and calibration are maintained (eg, AUC >0.80, slope ≈ 1.0), an adequately funded, adaptive randomised trial comparing a lactate-clearance–PaO2/FiO2-guided care bundle with usual management, and powered on 28-day ventilator-free days, would be the logical next step.
Conclusion
A model incorporating 6- h lactate clearance and PaO2/FiO2 alongside six clinical confounders provides accurate, well-calibrated prediction of 28-day mortality in sepsis-associated ARDS. The derived risk score formula is provided for prospective validation. External validation in a multinational ICU registry should be undertaken before clinical implementation.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261466237 - Supplemental material for Development and Temporal External Validation of a 6-Hour Lactate Clearance–PaO2/FiO2 Model for Predicting 28-Day Mortality in Sepsis-Associated ARDS
Supplemental material, sj-docx-1-jic-10.1177_08850666261466237 for Development and Temporal External Validation of a 6-Hour Lactate Clearance–PaO2/FiO2 Model for Predicting 28-Day Mortality in Sepsis-Associated ARDS by Lei Shi, Yun Sun and Kewei Cheng in Journal of Intensive Care Medicine
Footnotes
Acknowledgements
Not Applicable
Ethical Approval
This study is an analysis of a public database. Approval from the Institutional Review Board was not required.
Consent for Publication
Not appliable
Author Contributions
Lei Shi was responsible for the initial data extraction and preprocessing; Yun Sun and Kewei Cheng developed the algorithms for pattern recognition and anomaly detection within the medical data; Kewei Cheng led the statistical analysis and interpretation of results; Lei Shi facilitated the integration of findings with existing medical knowledge, formulated the outline, and authored the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Science and Technology Project of Changzhou Health Commission (Grant No ZD202438).
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.