
Abstract
This review outlines the current understanding of the interactions of titanium and its alloys with blood components, and the ways in which surface modification techniques can be used to alter the surface physicochemical and topographical features that determine blood–material interactions. Surface modification of the spontaneously formed titanium oxide surface layer is a highly attractive means of improving haemocompatibility without forgoing the advantageous mechanical and physical properties of titanium and its alloys. A number of surface modification techniques and treatment processes are discussed in the context of enhancing the haemocompatibility of titanium and its alloys, with a view to optimising the clinical efficacy of blood-contacting devices and materials.
Introduction
Blood-contacting medical implants and devices are revolutionising cardiovascular medicine, with applications ranging from catheters and haemodialysers, to stents, vascular grafts, heart assist devices, prosthetic heart valves and artificial hearts. The escalating usage of cardiovascular implants and devices has heightened research efforts in the search for biomaterials with superior haemocompatibility. Whilst the development of these implants and devices has led to major therapeutic advances, their usage nonetheless involves inherent risks of complications that arise from the thrombogenicity of many of these blood-contacting medical implants.
Thrombus formation continues to contribute to patient morbidity and mortality by means of local vessel occlusion, thrombus embolisation, chronic destruction and depletion of elements in the blood, and the production of inflammatory mediators that can have damaging systemic and haemodynamic effects. As a consequence, many of these devices can only be deemed safe when used alongside long-term anticoagulant drugs. Efforts have therefore been directed towards reducing the thrombogenicity of materials used in blood-contacting implants, to in turn reduce complication rates and lighten the financial burden associated with replacing failed implants and administering concomitant long-term anticoagulation therapy.
The thrombogenicity of a biomaterial surface is directly related to its surface physicochemical and topographical characteristics, which largely dictate the composition of the layer of ions and plasma proteins that is invariably adsorbed when a biomaterial first comes into contact with blood plasma. The acquisition of this layer of adsorbed protein transforms an inert biomaterial into a biologically active surface, and plays a crucial role in mediating interactions with haemostatic and inflammatory blood components, 1 – 3 namely platelets, the coagulation cascade, the complement system and leucocytes.
The adsorption of structurally and thermodynamically less stable proteins onto a surface is fundamentally because of electrostatic and hydrophobic/hydrophilic interactions. 4 The electron transfer that results from these interactions is thought to be primarily responsible for inducing conformational changes in the proteins, which can consequently lead to the activation of platelets, the clotting cascade and inflammation. 5 Hence, a biomaterial’s surface charge (as predetermined by its functional groups) and conductivity are important contributory factors to its haemocompatibility.
Aside from surface charge, surface topography is thought to be a major factor affecting surface thrombogenicity. 6 Not only does increased roughness lead to increased surface area onto which proteins can be adsorbed and thereby facilitate platelet and cell adhesion, but also it alters physical properties such as hydrophilicity and surface wettability, and also affects the orientation of adhered cells. Whilst an increase in roughness is expected to lead to an increase in platelet adhesion and hence thrombogenesis, studies have observed that macromolecular inhomogeneous surface domains, resulting from microstructural phase variations, improve haemocompatibility by interrupting interactions between plasma proteins and the surface, hence reducing protein adsorption. 7
Directly related to surface roughness, a surface’s interface energy and wettability has been demonstrated to be a key contributory factor in haemocompatibility, 8 – 10 since these surface characteristics govern the degree to which a surface makes contact with plasma. Greater surface–plasma contact increases the level of protein adsorption and hence activation of haemostatic and inflammatory pathways. However, whilst surface interface energy and roughness have been shown to play some part in influencing blood–surface interactions, they have not been proven to predict the surface’s haemocompatibility in the absence of flow conditions – reflecting the complexity of the phenomenon, 11 and some of the limitations of in vitro studies, animal studies and surface characterisation studies. 12
Surface modifications
Modifying an implant surface to alter its interaction with blood is an ideal means of improving the biomaterial’s haemocompatibility whilst retaining its advantageous mechanical and physical properties. Some examples of biomaterial surface modifications include: attempts to increase the hydrophilicity of surfaces to reduce protein adsorption and cell adhesion; 13 chemical modification by functional group substitution to reduce complement activation, although inhibiting one haematological process can often augment another; 14 the attachment of anticoagulants (such as heparin), platelet aggregation inhibitors and plasminogen activators as an effective means of suppressing haematological processes, although this approach has reduced application for long-term cardiovascular implants; 15 – 17 preadsorbing biomaterials with albumin, which has proven to be effective for certain clinical applications; 18 and the incorporation of phosphorylcholine and phosphate groups on biomaterial surfaces to mimic biological cell membranes, which have shown some success at reducing protein adsorption, platelet activation and complement activation in a number of materials.19,20
Titanium and its alloys
Amongst the biomaterials investigated for use in cardiovascular implants requiring long-term haemocompatibility are silicon carbide, alumina, diamond-like carbon and titanium. However, of all these biomaterials, it appears that only titanium implant surfaces have good haemocompatibility in comparison to that of low temperature isotropic carbon (LTIC), which is commonly used in artificial heart valves. Furthermore, titanium and its alloys have been widely used as implants for their low modulus, enhanced corrosion and fatigue resistance, machinability and superior biocompatibility. 21 These attractive properties have led to the early and widespread use of titanium for dental, orthopaedic and cardiovascular implants.
The physical properties of titanium are heavily dependent on its metallurgical composition, with various grades existing for commercially pure titanium according to the degree of oxygen incorporation. The Ti-6Al-4V alloy has received particular attention for its higher strength and fatigue resistance in comparison to commercially pure titanium, owing to the presence of aluminium and vanadium which act to stabilise the β-phase microstructure alongside the α-phase at lower temperatures. 21 The well-established biocompatibility of titanium is ascribed to the titanium oxide layer that forms spontaneously at room temperature on the metal’s surface. 22 This oxide layer plays a central role in preventing the release of titanium metal ions, which are known to be primarily responsible for inducing adverse local tissue reactions.23,24
Surface titanium oxide layer
The naturally occurring oxide layer is usually only 1.5–10 nm thick and contains many defects, but various studies have shown that by improving its quality and increasing its thickness, it is possible to significantly improve surface haemocompatibility, regardless of alloy composition. Both thickness and structure of the oxide layer play an important role in determining the degree of ion release, which is one of the principal mechanisms underlying surface biocompatibility and haemocompatibility.
Highlighting the importance of surface oxide thickness, Sunny et al. 25 reported that the ratio of albumin to fibrinogen adsorbed onto titanium increased by seven times as the oxide layer was thickened from several nanometres to 200 nm by anodic oxidation, demonstrating the potential of thicker titanium oxide layers to promote albumin adsorption in favour of fibrinogen, thereby reducing platelet adhesion and activation. In parallel, Huang et al. 26 observed that clotting time increased by a factor of 1.5 when oxide layer thickness was increased from 10 to 250 nm by means of a thermal oxidation process, indicating that greater oxide thickness may also reduce coagulation.
As previously mentioned, the microstructure of the titanium oxide layer is also an important contributory factor to ion release and surface interaction with biological components. Titanium oxide exists in a number of oxidation states, including TiO, Ti2O3, Ti3O5 and TiO2. TiO2 is the most abundant naturally occurring form, and constitutes the bulk of surface titanium oxide alongside suboxide layers of TiO and Ti2O3. 27 TiO2 exists in a number of phases, including the amorphous phase and various crystalline phases. The lattice structure of crystalline TiO2 varies depending on its phase: in both the rutile and anatase phases, the crystal structure is tetragonal, whilst in the brookite phase, the crystal structure is orthorhombic. 28 Rutile is the most thermodynamically stable phase and has been demonstrated to be more haemocompatible than both anatase and amorphous TiO2. This could possibly be explained by the effect of the oxide crystal structure on the physical and topographical features of the surface, in light of the fact that rutile crystal structure is denser and more closely packed than anatase, hence providing fewer paths for ion diffusion and release. 29 Furthermore, the crystal structure also has an impact on the degree of protein adsorption when the titanium oxide comes into contact with human plasma. McAlarney et al. 30 observed that an increase in both thickness and crystallinity of the oxide layer was associated with increased complement C3 adsorption, but also noted that oxide crystallinity was a more significant contributory factor.
A number of theories have been proposed to underlie the mechanism by which changes in the thickness, structure, chemical composition and topography of surface titanium oxide impact upon its haemocompatibility. Surface charge of the titanium oxide layer is believed to be a significant contributory factor towards determining the composition of the adsorbed protein layer, and hence also any subsequent cellular interactions. Upon contact with water, titanium oxide forms hydroxide groups on its surface and, owing to the amphoteric nature of titanium oxide, these groups can either become positively or negatively charged depending on the pH of the surrounding fluid. In the relatively acidic conditions associated with new wounds formed by the implantation process, the surface hydroxide groups accept protons and hence establish a positive charge on the titanium oxide surface. This positive charge is, in turn, deemed responsible for inhibiting the adsorption of positively charged plasma proteins like fibrinogen that facilitating platelet adhesion and thrombogenesis, whilst simultaneously promoting the adsorption of negatively charged plasma proteins like albumin that are widely thought to have antithrombogenic activity.
In addition to the positive surface charge, the low interfacial energy that titanium oxide films exhibits upon interaction with water, blood and plasma proteins is also thought to underlie the lower levels of fibrinogen adsorption. Surfaces like LTIC that have high surface energies and hence low wettability, cause plasma fibrinogen to anchor and adhere strongly onto the solid surface in an attempt to lower the solid–liquid interfacial tension. On the other hand, titanium oxide possesses low surface energy, which is further reduced by the increased atomic density of the crystal plane that is characteristic of the rutile phase. The lower surface energy has the effect of reducing the interaction of fibrinogen with titanium oxide films, thereby reducing its adsorption. In turn, the weaker protein–surface interactions are thought to considerably reduce distortion and conformational changes to the structure of fibrinogen, and hence lead to less fibrinogen-mediated activation of platelets, thereby reducing their aggregation and contribution to thrombogenesis. 31
In parallel with low surface tension, the semiconducting nature of titanium oxide is believed to be an important contributory factor to its haemocompatibility. The theory is based upon the mechanism of fibrinogen polymerisation into fibrin, which involves the cleavage of four negatively charged fibrinopeptides from the fibrinogen molecule, reducing the electrostatic repulsion of the chains that make up fibrinogen, and hence permitting their spontaneous association into fibrin polymers.
Although this conversion is usually mediated by thrombin generated by the clotting cascade, the cleavage of fibrinogen can also occur at a foreign surface that is capable of accepting electrons from the occupied valence bands of fibrinogen, thus inducing a conformational change in fibrinogen molecules that can lead to thrombus formation
32
and an increase in platelet activation via interactions of incomplete heterosaccharides on distorted fibrinogen molecules with glycosyl transferase groups on platelet membrane receptors.33–35 This oxidative transfer of charge depends on the electronic structural states of both fibrinogen and the material surface, in particular the band gaps between their respective valence bands and conduction bands. Fibrinogen has an electronic structure similar to that of semiconductors and a band gap of 1.8 eV,
36
whilst TiO2 is a semiconductor by nature with a band gap of 3.2 eV.
37
Since both the valence and conduction bands of fibrinogen lie within the band gap of TiO2, transfer of electrons from the fibrinogen to the oxide layer is inhibited, and hence distortion of fibrinogen molecules is reduced. Figure 1 outlines the relationship between the energy band structures within a system of titanium oxide and fibrinogen.
Schematic of the energy band structure of the TiO2/fibrinogen system.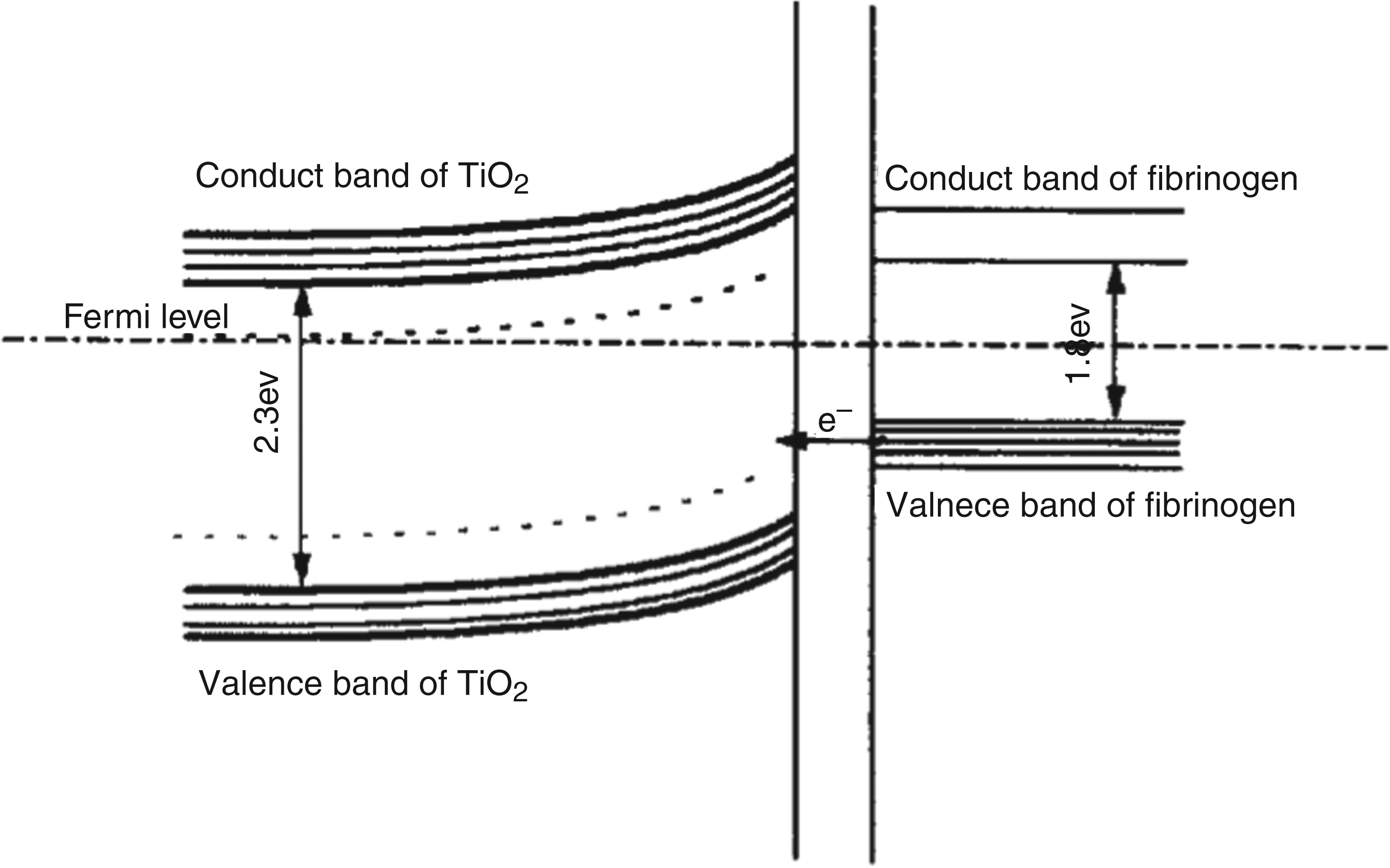
However, the inhibitory effect of TiO2 on electron transfer from fibrinogen molecules depends on the oxide layer having n-type semiconducting properties, which is determined by its microstructure. Using unbalanced magnetron sputtering to deposit titanium oxide films, Leng et al. 38 observed that the band gap of TiO2 varies with crystallinity, and that the only oxide layers with a band gap of 3.2 eV encompassing that of fibrinogen were those with a crystalline TiO2 structure (rutile and anatase) and no suboxide layers. On the other hand, less crystalline oxide layers with incorporated suboxides were found to have more local electronic states in their band gaps, which would enable them to accept electrons from fibrinogen and hence induce increased fibrinogen adsorption and conformational change. This goes towards explaining the lower levels of fibrinogen adsorption and platelet activation associated with the high crystallinity of rutile titanium oxide surfaces as well as that of anatase, in comparison to amorphous titanium oxide.
It is proposed that the n-type semiconducting properties underlying the inhibitory effect of titanium oxide on the acceptance of electrons from fibrinogen can be enhanced by element doping. Using magnetron sputtering and thermal oxidation to produce titanium oxide films containing tantalum, Chen et al. 31 observed that these Ti(Ta+5)O2 surfaces induce lower levels of fibrinogen adsorption and conformational change, and consequently reduced platelet adhesion. The authors propose that incorporating tantalum into titanium oxide films lowers the blood–surface interfacial energy, and hence only weak interactions are induced between the surface and fibrinogen. The authors also propose that the tantalum doping has the effect of raising the Fermi level of the oxide film, thereby reducing the work function of the film and facilitating the movement of electrons from the inner regions of the oxide layer to the surface, 39 which is believed to inhibit the transfer of electrons from fibrinogen to the surface and hence prevent fibrinogen structural distortion.
To explore the effects of element doping on titanium oxide films, Maitz et al. 4 prepared titanium oxide films implanted with either chromium or phosphorus ions, both of which are electron donors capable of preventing electron uptake by the surface. High doses of chromium ions were implanted onto amorphous TiO2 with the aim of inducing a chemical surface change that could prevent the oxidation of fibrinogen at the surface. In parallel, low doses of phosphorus ions were implanted onto the surface of semiconducting rutile TiO2, with some phosphorus-implanted oxides being subjected to a tempering process in order to incorporate the ions into the TiO2 crystal lattice, thereby enabling their n-doping electron donor properties to manifest and raising the Fermi level in order to inhibit electron transfer from fibrinogen to the oxide surface. The authors found that surface implantation with either ion had the effect of reducing clotting cascade activation by TiO2 surfaces; however this was only true for samples that had not undergone tempering, which seems to indicate that the theory that n-type semiconductors prevent electron transfer from fibrinogen may not extend to proteins involved in the clotting cascade, and that clotting activation on ion-implanted oxide surfaces may be reduced through other mechanisms such as lower interfacial energy or surface chemistry. The authors also observed that phosphorus ion-implantation led to lower platelet adherence and activation in association with lower clotting cascade activation, whilst chromium ion-implanted surfaces induced significantly higher levels of platelet adherence and activation. In actual fact, the opposing trend between the responses of platelets and the clotting cascade associated with chromium ion-implantation is consistent with a number of other studies;40,41 so, it is noteworthy that phosphorus ion-implantation leads to the concurrent reduction in both systems.
It has been proposed that the mechanism underlying the enhanced haemocompatibility of phosphorus ion-implanted titanium oxide surfaces is through simulating cell membranes that have high levels of phosphorus-based biomolecules. This would explain why tempering reduces the positive effect of phosphorus doping on haemocompatibility, since the phosphorus ions become incorporated into the crystal lattice of the oxide layer rather than being exposed on the oxide surface and exercising their biomimetic effect. This theory is supported by a number of other studies that have demonstrated the enhanced haemocompatibility of surfaces coated with various phosphorus-containing compounds such as phospholipids, 42 phosphorylcholine 43 and phosphazenes. 44
A number of other surface modifications are thought to exert their effects on haemocompatibility through associated changes in surface conductivity. In a study by Petersson et al., 45 the authors concluded that blasting titanium surfaces introduce defects into the oxide surface that lead to a significant increase in the number of charge carriers and hence conductivity, which would be expected to lead to higher levels of protein adsorption and conformational change. The increased roughness and defect density associated with blasting and etching would also influence surface–blood interactions by increasing the surface area upon which proteins can be adsorbed, thereby increasing levels of total protein adsorption. However, increased surface roughness of titanium oxide is associated with increased hydrophilicity, 46 which in turn leads to reduced adsorption of hydrophilic proteins such as albumin, 47 whilst promoting hydrophobic proteins such as fibrinogen and fibronectin. 46 A roughened TiO2 surface exposed to plasma would therefore be expected to promote platelet adhesion and thrombogenesis through the effects of adsorbed fibrinogen, and also promote cell adhesion as a consequence of fibronectin adsorption. 48 Hence, roughening of surfaces could have a detrimental impact on TiO2 surface haemocompatibility by reducing the ratio of albumin to fibrinogen; however, the increase in fibronectin adsorption and its effect on cell adhesion may provide opportunities for adopting endothelialisation as an alternative means of improving surface haemocompatibility.
Aside from increasing the roughness of the TiO2 surface, Petersson et al. 45 also observed that chemical etching with hydrofluoric acid led to the incorporation of fluoride ions into the TiO2 structure, thereby lowering the surface stoichiometry and increasing the number of charge carriers in the oxide film. The effect was to significantly increase the conductivity of the acid-etched oxide layer, which would be expected to increase levels of fibrinogen adsorption and electron transfer. The incorporation of fluoride ions into the oxide layer is also responsible for reducing the positive charge on TiO2 surfaces that is known to develop as a result of the low pH conditions associated with new wounds formed during the implantation process. 49 The authors use the fluoride-induced reduction in surface positive charge to explain the increased adsorption of positively charged plasma proteins such as fibrinogen, which would mediate an increase in platelet adhesion and thrombogenesis. On the other hand, surface titanium-fluoride groups are known to function as electron-trapping sites, 50 and could hence have beneficial effects by facilitating the healing process and reducing atherosclerosis.
Surface treatments
The treatment process that the titanium oxide surface layer undergoes has a significant impact on the structural, chemical, physical and topographical features of the surface. A wide range of titanium surface modifications exist, ranging from the deliberate thickening of the surface oxide layer, to the transformation of its phase and crystal structure and the incorporating elements into the layer, amongst others.
One of the principal areas of titanium surface modification envisaged to improve surface haemocompatibility is the thickening of the surface oxide layer. A number of methods are used to increase the thickness of this layer, each with their own unique modifying effects on the titanium oxide surface that may potentially alter surface haemocompatibility. Heat treatment to temperatures of greater than 200°C is a simple technique used for inducing substantial thickening of the oxide layer, and has been shown to have an impact on the adsorption of particular plasma proteins. 51 Pre-treatment of titanium implants with hydrogen peroxide (H2O2) is also used to produce a thicker and more porous titanium oxide layer, which has been found to have a slightly lower oxygen–titanium ratio 52 that promotes the adsorption of both fibrinogen and high molecular weight kininogen, 53 both of which contribute to the activation of platelets and the clotting cascade, respectively. Indeed, Takemotoa et al. 54 found that H2O2 treatment of titanium oxide led to significantly higher levels of platelet adsorption compared to titanium oxide layers that had undergone heat treatment at 300°C. Furthermore, the authors observed that titanium oxide films that had undergone H2O2 treatment and subsequent heat treatment were most inhibitory to platelet adhesion, thought to be due to the effects of high temperatures in creating thick oxide layers and decomposing radical species on the surface.
The deposition of a titanium oxide layer on surfaces can also be achieved by metal plasma deposition and metal plasma immersion ion-implantation and deposition, which involves the use of a metal plasma produced by cathodic arc evaporation from which ions are accelerated towards the negatively charged implant surface. By altering the deposition parameters, Maitz et al. 4 used this method to produce titanium oxide films with different phases and crystalline structures, observing only a slight and statistically precarious difference in platelet and clotting cascade activation by the various oxide films investigated. Oxide surfaces with greater crystallinity were found to induce less platelet adherence and activation in comparison to amorphous oxide surfaces; however, the opposite effect was observed on the clotting cascade, with crystalline rutile inducing the highest clotting activation. Corresponding to the trend of clotting cascade activation in relation to crystallinity, McAlarney et al. 30 reported an increase in complement factor C3 adsorption onto more crystalline titanium oxide surfaces, potentially leading to the spontaneous autoactivation of the C3 molecule and consequent activation of the complement system’s alternative pathway. These studies indicate an opposing trend in the effects of titanium oxide crystallinity on the response of platelets and that of the clotting and complement cascades.
Anodic oxidation
Anodic oxidation is an electrochemical process that is often used to deposit a porous oxide layer of controlled thickness onto titanium orthopaedic and maxillofacial implant surfaces, thereby improving the quality of the oxide layer and hence improving biocompatibility and bone interaction. In light of previously cited studies by Sunny et al. 25 and Huang et al. 26 demonstrating the role of thicker surface oxide layers in improving haemocompatibility, anodic oxidation of titanium cardiovascular implants may potentially offer an effective method of enhancing haemocompatibility and reducing thrombogenicity. However, the effect of anodic oxidation on the oxide layer is not merely that of increased thickness; it also has a number of chemical, physical and topographical effects on the surface layer that will invariably influence blood–material interactions.
The characteristics and thickness of the oxide layer formed by anodic oxidation are influenced by a variety of parameters, including electrolyte composition and concentration, in addition to applied voltage, current density and temperature. In particular, at voltages higher than the breakdown voltage, anodic oxidation can facilitate the adsorption of anions from the electrolyte onto the oxide layer. 55 This in turn alters the surface layer’s chemical and physical characteristics depending on the electrolyte used, with particular ions and associated functional groups affecting surface hydrophobicity, wettability and charge, which would in turn have an impact on surface interaction with biological components, such as plasma proteins and platelets in the context of blood-contacting implants. The incorporation of ions into the oxide layer and the application of a voltage exceeding breakdown voltage are the two principal factors responsible for changing the crystal structure of titanium oxide, forming one or a mixture of the rutile, anatase and even rare brookite phases. 56
Furthermore, the actual thickness of the anodic oxide layer also dictates its microstructure, with amorphous oxide transforming into a crystalline phase once an anodic oxide layer has reached a critical thickness.57,58 This crystallographic transformation is closely linked to the breakdown of anodic oxide films that results from the high compressive stresses associated with higher electric fields. These stresses are countered by the surface tension of the oxide layer, but this stabilising effect decreases with increasing anodic oxide film thickness, hence leading to mechanical deformation and breakdown beyond a critical thickness. 57 Since anion adsorption lowers the oxide surface tension, breakdown is heavily influenced by electrochemical parameters such as electrolyte concentration and activity, 59 and by current density.60,61 Not only does oxide thickness-related breakdown lead to crystallographic transformation from amorphous to crystalline phases, but it also results in pitting, crack formation and high defect densities. 57 These defects would in turn significantly impact the topographical features and hence blood interaction of the surface oxide layer, with associated increases in surface roughness and area potentially facilitating cell and platelet adhesion and protein adsorption.
Anodic oxide growth involves the migration of ions through the oxide film and the thickening of the oxide layer according to Faraday’s law. Despite this, growth constant values for anodic oxide films vary from study to study, 62 – 64 possibly as a result of varying surface preparations and electrochemical conditions. However, it is clear from these studies that the growth constant has a considerable impact on the characteristics of the anodic oxide surface layer, particularly on surface pore configuration, surface defect concentration profile 65 and the formation of an intermediate suboxide TiO2 − x layer between the deep TiO layer that forms on the titanium substrate, and the superficial TiO2 layer, 66 which would all influence surface–blood interactions. Hence, if anodic oxidation was to make its way into the clinical setting for cardiovascular implant treatment, efforts would need to be directed towards standardising these parameters to ensure consistent and evidence-based implant surfaces.
The effect of anodic oxidation on the surface oxide layer is of course influenced by the underlying phase, which differs between commercially pure titanium and the Ti-6Al-4V alloy. On Ti-6Al-4V, for example, there is variation in surface oxide pore size between the α-phase and the vanadium-rich β-phase. Furthermore, both the untreated and anodic oxide surface layers on Ti-6Al-4V are composed of TiO2 + Al2O3, with a Ti/Al ratio of 5 but no trace of vanadium. 67 In light of the subtle but potentially biologically significant differences between commercially pure titanium and the Ti-6Al-4V alloy, it is important to take care when comparing studies into these two commonly used and investigated biomaterials.
Superplastic forming
Having discussed important surface-modifying processes that can be used to enhance the haemocompatibility of cardiovascular titanium implants, it is important to appreciate the ways in which titanium can be shaped for the use in blood-contacting medical implants and devices. Since an implant’s short- and long-term performance is heavily dependent on its structural congruence with surrounding host anatomical features, the accurate shaping and formation of implants is crucial to avoid implant failure and clinical complications. This is particularly paramount in the context of the flow conditions that cardiovascular implants are continuously exposed to, where even the slightest irregularity can lead to mechanical destruction of erythrocytes, platelet activation and thrombus formation.
Cold forming, which is carried out below a material’s recrystallisation temperature, is the conventional processing technique used to shape titanium sheets into implants; however, owing to associated springback and incomplete adaptation, the process lacks the high precision and accuracy necessary for shaping complex implants. An immerging manufacturing technique for titanium implants that aims to address these problems has integrated superplastic forming (SPF) technology with scanning and computational simulation technology to produce patient-specific, complex and topographically accurate implants. Adopted from the aerospace industry, SPF technology has mainly been developed and applied in the context of dental and maxillofacial prostheses, but the potential for its use in cardiovascular medicine offers highly attractive prospects.
SPF is an inelastic large-deformation constant-volume process involving the use of a ceramic die upon which to mould the titanium sheet at temperatures reaching approximately 900°C. 68 It is necessary to maintain an optimal strain rate or flow stress for the duration of the process by varying the pressure in a deformation-dependent manner, and hence requires accurate numerical modelling to generate suitable and individualised pressure-time cycles. 69 Since SPF material behaviour is viscoplastic, large deformations are possible and it is possible to create lightweight and intricate implants of uniform thickness with little or no springback. 70 By creating computer-generated die geometrical models based on CT/MRI scans of the area to receive the implant, and by subsequently generating a die mesh for finite element SPF simulation, it is possible to produce highly patient-specific and intricate superplastically formed titanium implants. 69 In the context of cardiovascular devices, these are very attractive implant characteristics, providing the opportunity to accurately match implants to each patient’s anatomy. This individualised and accurate creation of implants could potentially reduce failure rates and complications arising from structural mismatches and irregularities in cardiovascular implants that require a high degree of specificity, such as heart valves and vascular stents. Aside from the superior quality of implants produced, an additional advantage that makes SPF a practical and implementable processing technique is its cost effectiveness, owing to the relatively low manufacturing and customisation costs and the use of low-cost castable ceramic dies made from dental investment materials. 69
Ti-6Al-4V has long been used in the aerospace industry for its strength, lightweight and low modulus. Aside from the fine-grain microstructure necessary for SPF processing, Ti-6Al-4V also has the added advantage of being able to diffusion bond with material it makes contact with during the SPF process, thereby forming bonds with the strength of the parent alloy. 70 Both its suitability for SPF and its biocompatibility have meant that the Ti-6Al-4V alloy has received substantial attention for its potential use in the production of medical implants. However, there is a high probability that during the SPF process, the surface of the Ti-6Al-4V alloy undergoes changes and modifications that may potentially have an impact on both surface biocompatibility and haemocompatibility. For one, heat treatment to temperatures above 200°C is known to induce thickening of the surface oxide layer and hence affect surface interactions with biological components, although the surrounding investment material may shield the surface from exposure to oxygen and hence limit oxide deposition. Furthermore, interactions between the titanium alloy and the die investment material during the extended periods of high temperature and pressure conditions would be expected to yield alterations in the chemical and physical properties of the alloy surface and hence impact on its interaction with biological components. This is particularly the case since titanium is, in actual fact, a very reactive metal, but is protected and rendered inert by the oxide layer that invariably forms on its surface at ambient temperatures; however, at the high temperatures involved in SPF, the oxide layer becomes soluble, thus exposing the unprotected titanium substrate to inevitable reactions with the investment material. Whilst the haemocompatibility of SPF titanium alloy does not appear to have been investigated, studies into its biocompatibility indicate that the surface modifications and presence of reaction products on the surface, have a cytotoxic effect on human osteoblast cells. 71
Endothelialisation
Although surface modifications may go a long way in reducing the thrombogenic potential of blood-contacting implants, it is highly improbable that a surface could be developed that posed no risks of activating the haematological processes underlying thrombus formation and inflammation. The cardiovascular endothelium remains the optimal blood-contacting surface, with none of the inherent risks associated with blood–biomaterial interactions. In light of this, an altogether different approach to reducing implant surface thrombogenicity is being explored by a parallel line of research into the potential of implant surface endothelialisation. This approach is in stark contrast to the growing use of drug eluting devices which, in addition to their intended inhibition of hyperplasia, also inhibit the re-establishment of a healthy endothelium and produce unwanted side effects. 72
Bearing in mind that a foreign surface can never be as haemocompatible as the native vascular endothelium, the inhibition of endothelialisation will inevitably increase the long-term potential for thrombogenic stimuli to induce cardiovascular complications. On the other hand, by devising surface modifications that promote the endothelialisation of blood-contacting implant surfaces, it may be possible to significantly reduce the risk of long-term thrombogenesis and its associated morbidity. The resulting composite structure would comprise the biomaterial base with desirable mechanical properties, in combination with the restored endothelium that would not only provide a fully haemocompatible interface with which blood can interact, but it would also isolate the biomaterial surface so as to limit its potential activation of haematological processes conducive to thrombosis and inflammation. Furthermore, the endothelium would also be able to carry out its central and unique physiological role of regulating and maintaining vascular function, including the active prostaglandin-mediated inhibition of thrombosis, and the production of factors such as nitric oxide, heparin sulphate, tissue plasminogen activator and thrombomodulin that all contribute to the inhibition of smooth muscle cell migration and proliferation and hence reduce intimal hyperplasia.73,74
Spontaneous endothelialisation of surfaces does not seem to occur in humans, as observed in the case of synthetic vascular grafts 75 and prosthetic heart valves. 76 Hence, most research has been directed towards pre-seeding endothelial cells onto biomaterial implants, concentrating on modifying the implant surface so as to promote endothelial cell long-term adhesion and proliferation, which are prerequisites for endothelial vascular function. Crucial to the long-term success of endothelialised implants in the high flow and shear stress conditions of the cardiovascular system is the resilience of the endothelial cell layer, which is significantly improved with longer in vitro incubation times that result in a confluent and well-established cell layer. A number of clinical trials 77 – 83 have demonstrated that endothelialised vascular grafts produced in this way have resulted in intimal tissue with long-term stability and functionality, and have significantly improved the performance and patency of prosthetic small-diameter vascular grafts.
The seeding of endothelial cells necessitates the availability of autologous host endothelial cells in numbers sufficient to cover relatively large implant surface areas, which can be invasively sourced from venous endothelia, microvascular endothelia or, according to recent studies, endothelial progenitor cells that can be obtained non-invasively from the circulation and have recently been used in animal implantation. 84 The process of harvesting, seeding and incubating cells on synthetic materials is time consuming, costly and not practical for emergency procedures; hence, there have been a number of investigations into implant surface modifications that stimulate in vivo self-endothelialisation. In the case of vascular grafts in animal models, spontaneous endothelialisation of implant surfaces occurs either by capillary infiltration through pores incorporated into the implant wall, or by ingrowth from the adjacent arteries as a continuous sheet across the synthetic graft.85,86 Whilst this process does not occur spontaneously in humans, a number of surface modifications have been proposed to promote in vivo endothelialisation, including coating luminal implant surfaces with fibrin glue containing angiogenic growth factors. 87
In light of the significant improvements in clinical outcome that could be achieved by the use of endothelialised cardiovascular implants, an attractive area of research is exploring the potential of various biomaterials and surface modifications in promoting the formation of a confluent endothelial cell layer, either by seeding in vitro or spontaneously in vivo. Along with its mechanical properties, the superior biocompatibility of the titanium oxide layer on titanium implants holds attractive prospects for creating endothelialised titanium cardiovascular implants. A study by Bruni et al. 88 has shown that Ti-6Al-4V alloy surfaces, whether untreated or subjected to furnace or glow-discharge treatments in air, demonstrate good biocompatibility towards Human Umbilical Vein Endothelial Cells (HUVECs) seeded onto the material; however, the increase in leucocyte-binding adhesion molecule expression seems to suggest a role for titanium in inducing an inflammatory response in HUVEC cultures. Another study by Pareta et al. used ionic plasma deposition of both commercially pure titanium and the Ti-6Al-4V alloy to create thicker oxide layers with nanostructured surface features. Such nanostructuring of surfaces has been shown to mimic the natural nanostructured surfaces of blood vessels, and this particular study found that endothelial cell adhesion increased with nanoroughness, and exhibited a weaker correlation with surface energy. The mechanism by which nanostructured surfaces promote cell adhesion is thought to be mediated by increased adsorption of select proteins. 89 Furthermore, Chai et al. 90 compared the endothelialisation of sol–gel derived titanium oxide coatings to that of stainless steel, SiO2 and Nb2O5, and found that titanium oxide surfaces promoted significantly faster endothelial cell adhesion upon initial seeding, and significantly improved cell proliferation in early culture periods. Taken together, these studies suggest the potential for titanium oxide surfaces to be used as implant bases for endothelialisation to improve cardiovascular clinical outcome; however, there is clearly a need for further extensive investigation into this groundbreaking area.
Inflammatory response and monocyte adhesion
The biocompatibility of titanium implants encompasses the material’s low capacity to induce an inflammatory response, characterised by only a transient influx of inflammatory cells in association with a transient secretion of proinflammatory cytokines. 91 A study comparing the response of monocytes to titanium, poly(urethane urea) and polystyrene, reported that fewer monocytes adhered to titanium surfaces, and that titanium surfaces induced higher levels of monocyte apoptosis, possibly linked with the higher release of tumour necrosis factor-alpha (TNF-α) observed upon contact with titanium. The study also reported that titanium surfaces induced a significantly higher release of interleukin-10 (IL-10), which acts to downregulate the production of various proinflammatory cytokines. 92 These findings seem to suggest that titanium surfaces provoke a diminished inflammatory response in comparison with other materials, and may even be mildly anti-inflammatory through the effects of the enhanced IL-10 release that is observed upon contact of monocytes with titanium surfaces.
Martinesi et al. 93 have shown that Ti-6Al-4V alloy surfaces, composed of a mixture of both rutile and anatase TiO2 phases, appear to discourage monocyte adhesion – particularly on surfaces that had undergone a glow-discharge treatment and thereby had thicker oxide layers. The same study reported that, compared to untreated titanium alloy surfaces, contact with the glow-discharge treated titanium alloy surfaces with thicker oxide layers was associated with significantly reduced TNF-α release by monocytes. This finding is particularly significant since TNF-α is a cytokine known to play a primary stimulatory role in the inflammatory cascade, 94 exerting a wide range of effects including the activation of a variety of leucocytes in addition to endothelial cells. 95 Furthermore, the samples with thicker oxide layers were also found to induce more monocyte apoptosis at a quicker rate than the untreated samples. Taken together, these observations suggest that thickening the titanium oxide layer could lead to a reduced monocyte-mediated inflammatory response, in addition to a reduction in the potential thrombogenic activity characteristic of granulocytes.
Göransson et al. 96 conducted studies into the adherence of monocytes to a variety of modified titanium surfaces, and found that adhesion was significantly higher on anodised surfaces, regardless of the electrolyte composition. Along with the effects of physicochemical changes resulting from anodic oxidation, it is likely that the increased surface roughness and porosity resulting from anodic oxidation is a principal contributory factor to enhanced monocyte adhesion, in light of the well-reported affinity of monocytes for rough surfaces. 97 – 100 In support of this theory, a study by Soskolne et al. 99 investigated the effect of increasing titanium surface roughness on the adhesion of monocytes, and found that rougher surfaces demonstrated significantly higher numbers of adhered monocytes compared to machined surfaces, together with increased monocyte release of TNF-α. It is suggested that the increased levels of adhesion are at least partly due to the substantially higher surface areas for protein adsorption and subsequent monocyte adhesion on rougher surfaces.
Conclusion
The physicochemical, mechanical and biological properties of titanium and its alloys render it a promising biomaterial for use in blood-contacting medical devices; however, the broad range of studies into the interactions of the titanium oxide surface layer with various blood components have highlighted the scope that exists for further investigation and optimisation of the surface oxide film haemocompatibility. In order for the complexity of the relationship between surface features and haematological responses to be taken into account, there is undoubtedly a need for investigations using more comprehensively representative models of the in vivo cardiovascular environment. Whether by means of in vivo implantation experiments on animals, or by the use of devices that simulate the in vivo environment such as parallel plate flow chambers to study the effects of flow and shear stress on the haematological responses to biomaterial surfaces, it is necessary to take steps towards developing optimal surface modification techniques if titanium and its alloys are to make their way to clinical trials and be used as cardiovascular devices and implants in the future.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.