
Abstract
Traumatic injury is the leading cause of death in people aged 44 or less in the US. It is also estimated that 82% of deaths from battlefield hemorrhage may be survivable with better treatment options. In this study, two biomaterial hemostats having disparate mechanisms were evaluated in a large animal lethal hemorrhage model and compared to a commercial product and standard cotton gauze. We hypothesized that the biomaterial with a biologically active mechanism, as opposed to a mechanical mechanism, would be the most effective in this model. Using a published study protocol, the femoral artery in swine was punctured and treated. KeraStat™ (KeraNetics) and Nanosan®-Sorb (SNS Nano) hemostats were compared to a commercial chitosan dressing (second generation Hemcon®) and cotton gauze. Both KeraStat and Nanosan increased survival, significantly increased mean arterial pressure (MAP), and significantly decreased shock index compared to both controls. The Hemcon dressing was no different than gauze. Platelet adhesion assays suggested that the KeraStat mechanism of action involves β1 integrin mediated platelet adhesion while Nanosan-Sorb operates similar to one reported mechanism for Hemcon, absorbing fluid and concentrating clotting components. The Nanosan also swelled considerably and created pressure within the wound site even after direct pressure was removed.
Introduction
Traumatic injury is the leading cause of death among people aged 36 or less worldwide 1 and aged 44 or less in the US. 2 Motor vehicle accidents and gunshot wounds are the most common cause of mortality in the US, both of which often create deep penetrating traumatic injuries and account for at least 60,000 deaths each year. 2 Unfortunately there are no good options for first responders to stop massive blood loss in these victims. Traumatic injury with uncontrollable hemorrhage is also a significant issue on the battlefield, where transport times can often be over an hour. Though battle mortality rates have dropped from 30% in WWII, to 24% in Vietnam to less than 10% in Operations Iraqi and Enduring Freedom (OIF and OEF), there continues to be gaps in what the combat medic or corpsman on the ground can treat. 3 In Vietnam, 10,000 service member deaths were the direct result of penetrating trauma and it has been estimated that 20% of those causalities could have been avoided with better treatment technologies. 4 In the recent Middle Eastern conflicts, only 31% of US service personnel had injuries that could be treated in the field, and analysis of autopsy data has suggested that 82% of those killed in action were from injuries that were potentially survivable.3,5
Due to the recent conflicts in Iraq and Afghanistan, there has been a tremendous amount of research and development of hemostatic agents and devices. This work has led to advances such as the self-applied Combat Application Tourniquet (CAT), which has saved countless lives in the conflicts in the Middle East. Wound dressing technology has also improved and been targeted to the civilian first-responder market, though there continue to be limitations with some of these products. Dressings containing acelyated poly-N-acetyl-glucosamine (Rapid Deployment Hemostat (RDH), Marine Polymer Technologies) or deacelyated poly-N-acetyl-glucosamine (Chitosan, HemCon Medical Technologies) work well in exposed low flow bleeding conditions but not in deep intra-cavity bleeding or under conditions of coagulopathy. 6 The granular zeolite known as QuikClot® (Z-Medica) has shown some effectiveness in a variety of injury models but often causes tissue damage due to its exothermic mechanism of action. 7 The current dressing used by the US Army in both Iraq and Afghanistan is Combat Gauze® (Z-Medica), which has been reported to work well as long as there are not significant tissue or vascular injuries. 8 The challenge that these dressings cannot overcome is that rigid or even flexible dressings are difficult to use for small tract penetrating injuries, and are not effective on large surface area bleeding often associated with massive soft tissue injury.
The ideal hemostat has been described by leaders in military trauma medicine as: (1) capable of stopping large-vessel arterial and venous bleeding, (2) ready to use with no special preparation, (3) simple to apply, (4) lightweight and durable, (5) stable at extreme temperatures, (6) causes no injury to the tissue and (7) be inexpensive. 3
There are currently no hemostats on the market that can independently address each of these specifications. The major limitations of currently available hemostats are that rigid dressings such as the Hemcon bandage and RDH work well in open, low flow injuries, and flexible hemostats such as Combat Gauze work well for compressible high flow injuries. Unfortunately these dressings do not have the versatility to work well in both injury types and neither works well in non-compressible truncal hemorrhage. To address these limitations, we sought to test two new potential solutions to these problems, a flexible and highly absorbent nanofiber polyurethane matrix called Nanosan-Sorb (NS), and an injectable keratin biomaterial based hydrogel called KeraStat (KS). These two novel materials were compared to standard cotton gauze and the second generation Hemcon bandage (HC), a compressed, rigid film made from chitosan.
These materials were selected to address the following questions:
Does increasing fluid absorption result in improved hemostasis (NS vs. control gauze)? Is flexibility important for tissue contact in high flow injuries (HC vs control gauze and NS)? Can a flowable hydrogel be used to stop high flow bleeding (KS)? Is a mechanical mode of action (gauze, NS, HC) more effective at achieving hemostasis than a biological mode (KS)? Could an injectable hydrogel (KS) be used to stop bleeding in a penetrating trauma model?
Materials and methods
Materials tested
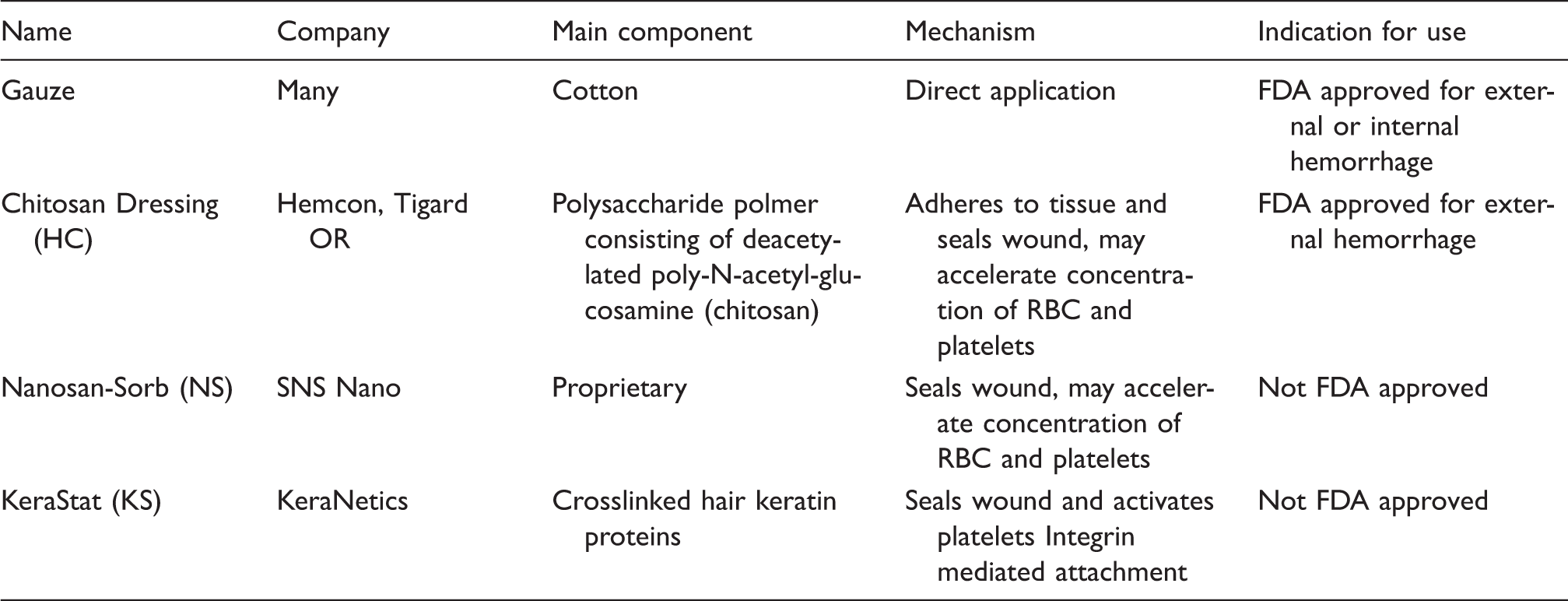
Four different material hemostats were selected for these experiments. These materials, their main composition and mechanism of action, if known, are summarized in Table 1. The configurations of each material as used in this experiment are shown in Figure 1(a) to (c).
(a) shows NS (left) and control 3 × 3 in gauze. (b) shows 20 cc of KS spread on 3 × 3 in gauze. (c) shows HC, cut in half from the 4 × 4 standard bandage in order to fit into the injury cavity. Description of dressings used.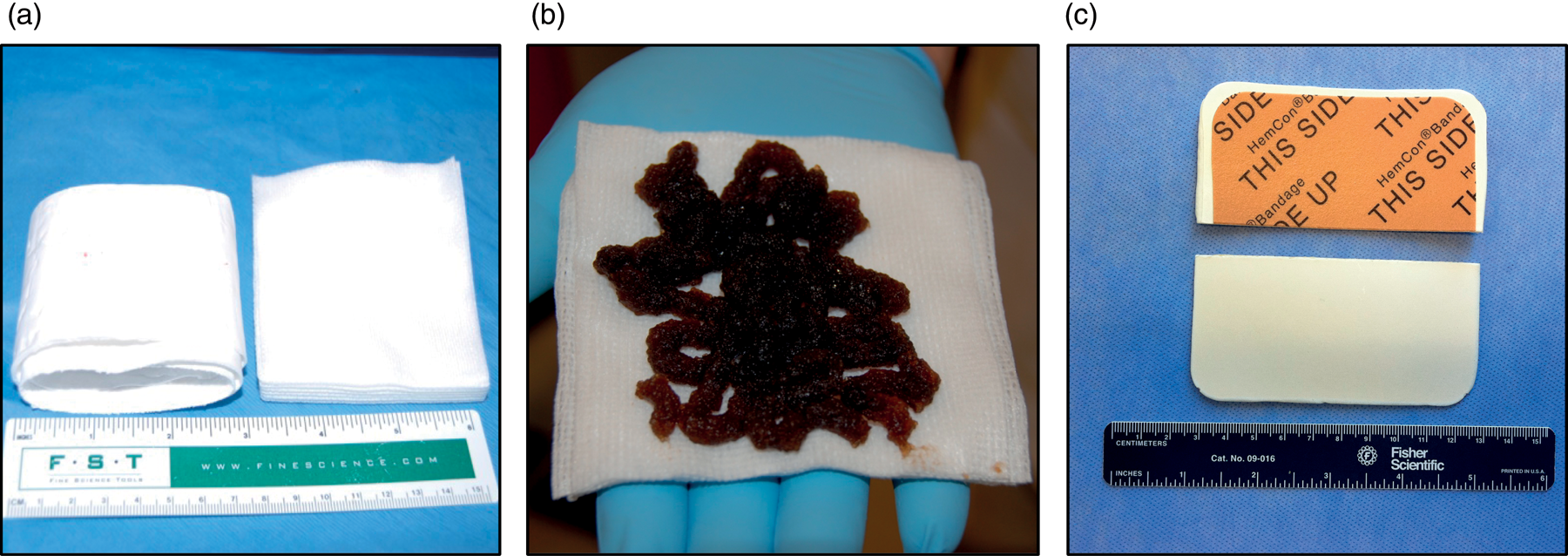
Femoral artery penetration model
Twenty-eight female Yorkshire pigs weighing 35.9 kg (±5.2 kg) were obtained from a licensed commercial vendor (any animal with a weight outside two times the standard deviation of the mean was removed from the study; this happened in two cases and these animals were not included in the total animal numbers). The animals were pair housed in an AAALAC accredited and USDA inspected facility maintained by Wake Forest University’s Animal Resource Program.
Surgical procedure
Baseline parameters pre- and post-injury.
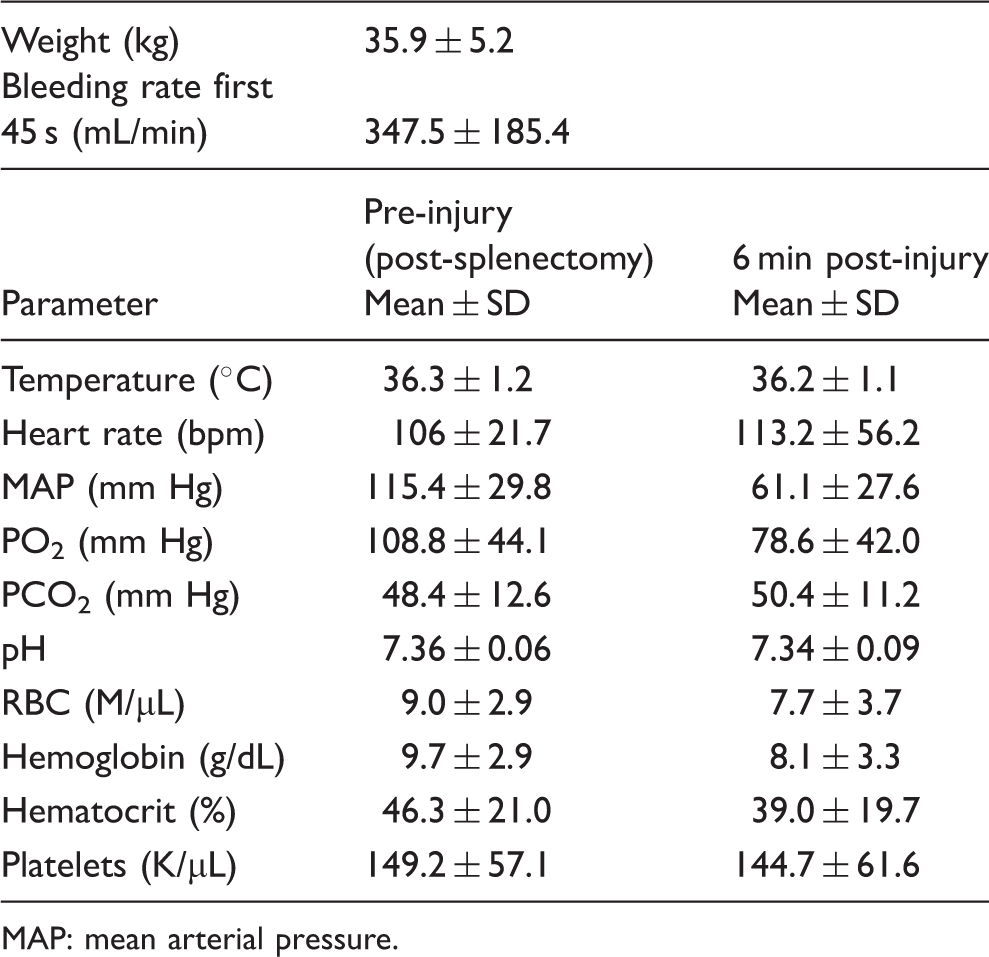
MAP: mean arterial pressure.
Injury
After puncture, the artery was allowed to free bleed for 45 s at which point one of the four treatments was applied through a pool of blood. Shed blood was collected by suction into a container placed on a pan balance and the accumulated weight recorded at each time point. The gauze-treated controls received six 3 × 3 in cotton gauze bandages stacked together, the HC-treated animals received one Hemcon dressing that was cut in half in order to fit on the wound, the NS-treated animals received a 3 × 18 inch strip of material that was folded to replicate the six gauze bandages. For the KS-treated animals, 20 cc of keratin gel was spread on six 3 × 3 inch gauze bandages (stacked together) and was placed over the arterial bleed. Images from the surgical procedure shown in Figure 2(a) and (b) show the punctured artery and the bleeding injury, respectively.
Shown are images of the injury. In (a) a 6 × 2 mm2 arterial punch is used to form a consistent injury (blue arrow shows the puncture wound on the clamped artery). In (b), blue arrow shows an example of the high flow bleeding injury before treatment.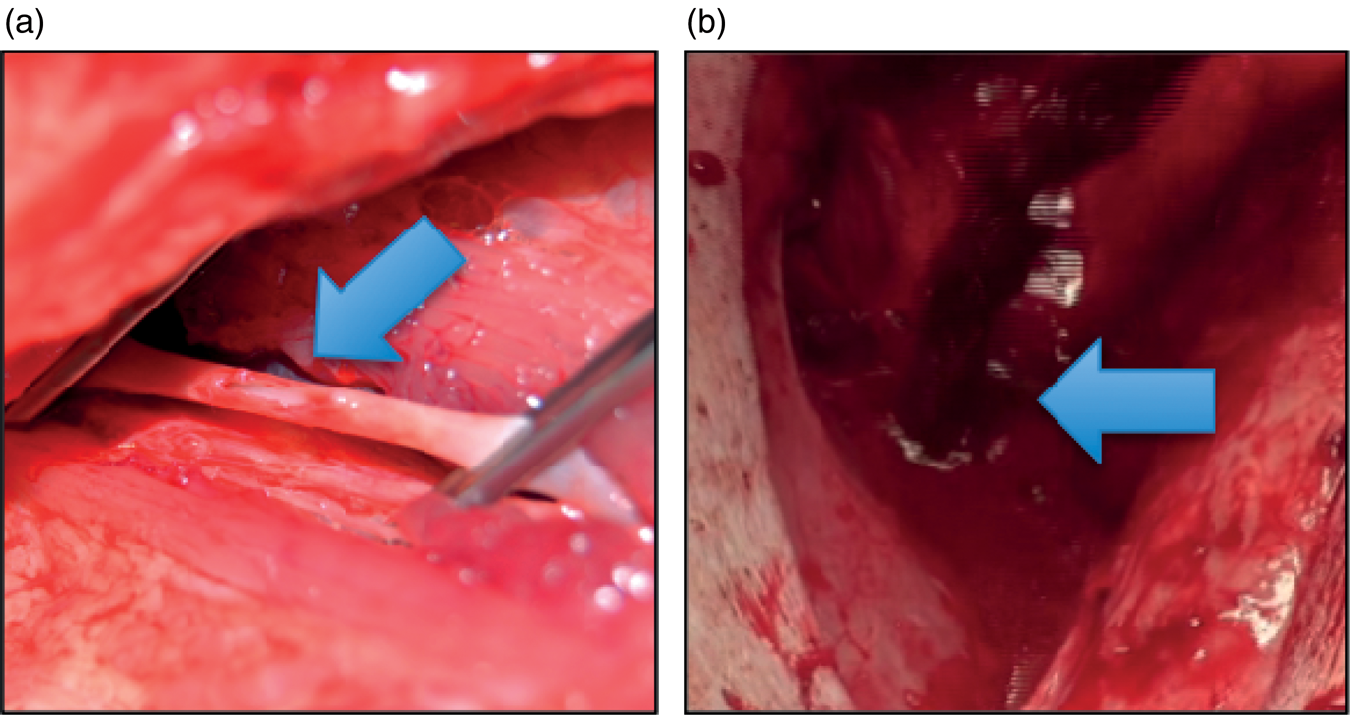
Once 45 s of bleeding was finished, one of the four treatments was applied with manual pressure for 3 min by one of two surgeons by directly contacting the bleeding vessel with the treatment material. Care was taken to ensure the treatment groups were divided evenly between the two surgeons so no pressure bias was introduced. Post-hoc analysis of the data did not reveal any differences between the surgeons. Following this first manual pressure application, 3 min of no compression began were the dressings were not manipulated in any way. At the end of the no compression period (6 min 45 s from hemorrhage), blood was drawn to assess blood chemistries and gasses. This was followed by a final 3 min of compression at which point the animals were allowed to survive for 180 min or until death. Death was defined as a MAP of ≤20 mmHg for 5 min. Vitals were monitored constantly during this period and arterial blood was drawn initially, after 45 s of hemorrhage at 6 min following hemorrhage and then every 30 min for complete blood count (CBC) with differentials, chemistry, and blood gas analysis.
If the animal survived the entire 3-hour operative period, limb manipulation was performed to assure adhesion of the material to the tissue pocket. Following limb manipulation, the animals were euthanized with an overdose of Euthasol given IV consistent with the recommendations of the American Veterinary Medical Association. In each animal, the surrounding tissue and vessel was excised for gross visual examination, microscopy and histological analysis. NS (n = 3) and control gauze (n = 2) materials from each group that survived the full experiment were recovered and assessed for the amount of expansion and fluid absorption.
Data analysis and interpretation
All data was analyzed using Prism v 5.0 (GraphPad Software Inc.). Animals were evaluated for weight and pre-injury parameters (e.g. heart rate, oxygenation, core body temperature, MAP, CBC, chemistry, and blood gases) by calculating the mean and standard deviation in each treatment group. Any variance greater than twice the standard deviation for that group resulted in elimination of that animal’s data from further analysis (this happened in 2 cases for animal weight). In one animal, PO2 was measured as 309.0 mmHg but all other parameters including PCO2 (42.1 mmHg) were within normal values so it was determined that this was a measuring error from the Medica Easy Blood Gas system and that data point was removed but the animal’s data was not.
For the calculation of shock index, experimental data from non-surviving animals was treated as previously described. 14 The challenge for studies such as the one described here is that animals that exsanguinate before reaching the 180 min point cannot contribute complete data points for analysis. To compensate for this, initial data to calculate shock index was weighted and extrapolated out to 180 min using a best-fit second-order polynomial. A conservative approach was taken wherein real data was used when available and longer-surviving animal’s data was weighted more heavily to avoid bias from animals that drop out early. Data was evaluated for distribution normalcy and reported as mean ± standard error of the mean (SEM).
Non-parametric data such as survival analyses were analyzed using a log rank test (Mantel–Cox). All other data was analyzed using a one or two-factor ANOVA followed by Tukey’s Multiple Comparison test or t tests depending on the number of comparisons made.
Femoral artery transection model
Five Yorkshire female pigs were used for this experiment under an approved Wake Forest Animal Care and Use Committee protocol (4 treated with KS, 1 with gauze). They were cared for and sedated exactly as described above. Animals were placed supine on a surgical table and the femoral artery was identified by palpation. A US Army M7 bayonet was used to make a stab penetration that transected the femoral artery and vein. The animals were allowed to bleed for 45 s at which point 50–110 mL of KS was injected into the penetration tract by either a 60 cc syringe or a custom designed applicator (Diversified Products and Research III Inc.). Gauze was held over the wound site for 2–5 min to prevent the KS gel from being washed back out of the wound. The gauze was then removed and the animal was allowed to survive for 180 min and vitals were monitored. Following the monitoring period, the animals were euthanized as described above and the injury site dissected for visual examination.
Colorimetric assay for platelet adhesion
A microwell plate colorimetric assay was used to assess platelet adhesion to the surface of a keratin hydrogel (the same base material in the KS hemostat) compared to a collagen gel and albumin coating. Adhesion was quantified by measuring acid phosphatase activity, an enzyme whose activity is not dependent on platelet activation. Whole blood was obtained from consenting donors with Wake Forest Institutional Review Board approval by venipuncture in citrated BD Vacutainer® tubes. The platelet-rich-plasma (PRP) was isolated through centrifugal force (800 r/min, 15 min, 22℃) and run through a Sepharose 2B column equilibrated with albumin containing HEPES-Tyrode buffer (pH 7.4, 2 mM CaCl2, 5 mM MgCl2). The isolated platelets, which have increased turbidity, were collected and layered (100 µL) over the various substrates. The plate was then incubated at 37℃ for 15 min to allow for platelet adhesion. After the incubation period, unbound platelets were washed with albumin-HEPES-Tyrode buffer for 5 min with mild shaking. The wells were then supplemented with 100 µL of 0.1 M citrate buffer (pH 5.4) containing 5 mM para-nitrophenylphosphate (pNPP) and 0.1% triton-X. A detergent is necessary to lyse the platelets and allow the acid phosphatase to react with pNPP and produce para-nitrophenol after a 60 min incubation period at 37℃. The reaction was then quenched using 100 µL of 2 N NaOH and the absorbance measured at 405 nm using a plate reader (Molecular Devices, SpectraMax Pro 5.4). Platelet adhesion to albumin coatings served as an external control for non-specific adhesion. As an internal control for non-specific adhesion on each substrate, a fraction of the PRP was fixed with 10% formaldehyde (15 min, room temperature) prior to platelet isolation. To determine receptor involvement in the adhesion mechanism of platelets to keratin, a monoclonal antibody against integrin β1 was utilized to inhibit receptor function (mouse anti-β1 clone 656, Millipore #MAB2253Z). The platelet receptors involved in platelet adhesion to collagen has been well established.15–17 Isolated platelets were pre-incubated with monoclonal antibodies with a final concentration of 20 µg/mL for 30 min at room temperature. The assay described above was repeated using the antibody-blocked platelets.
Results
Survival
The survival rates varied from 28% in the gauze group to 71% in the NS group. The Kaplan–Meier survival curve is shown in Figure 3(a) and survival times for each group are shown in Figure 3(b). There were no statistical differences in survival times or curves using a log-rank (Mantel–Cox) test between the groups. The NS and KS groups each had only one animal with a catastrophic treatment failure in the first 1.5 h compared to 4/7 of the HC-treated group and 3/7 in the gauze. Hazard analysis yielded survival ratios of 3.41 (95% CI 0.72-16.22) for NS vs. gauze and 2.16 (95% CI 0.53–8.91) for KS vs. gauze.
In (a), Kaplan–Meyer survival plot is shown for four groups (n = 7 per group). Log rank (Mantel–Cox) test yielded no significant differences in either NS vs. control (χ2 = 2.38, df = 1, p = 0.12), or KS vs. control (χ2 = 1.14, df = 1, p = 0.28). In (b), average survival times are shown for each group. The only significant difference in survival times occurred between NS vs. control (*p = 0.04, t-test, n = 7). NS: Nanosan-Sorb; KS: KeraStat.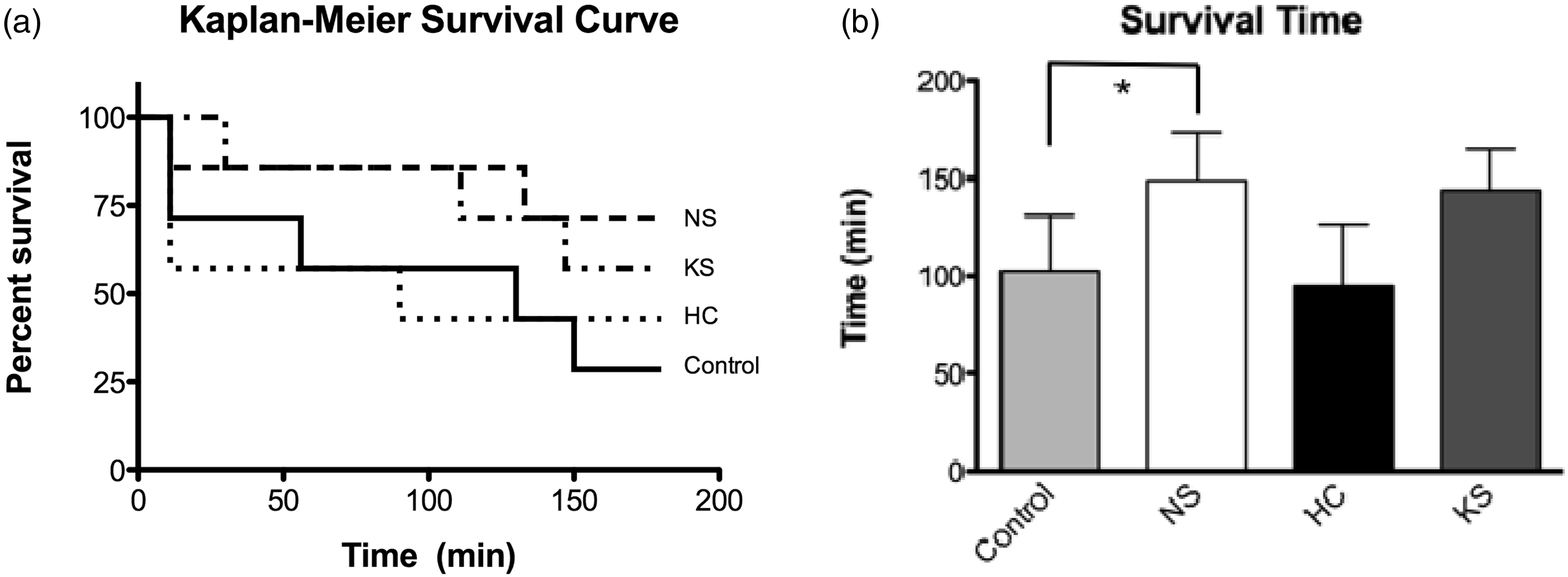
Blood loss
The initial bleeding and total blood/plasma loss is shown in Figure 4, adjusted for animal weight. Pre-treatment blood loss is shown in black and post-treatment in gray. There were no differences in pre-treatment blood loss, and losses for each group were within 1.4 mL/kg representing 10–13% of starting total fluid volume. There were also no significant differences in post-treatment blood losses.
Average shed blood in pre- and post-treatment in each of the four groups. There were no significant differences in any of the treatment groups.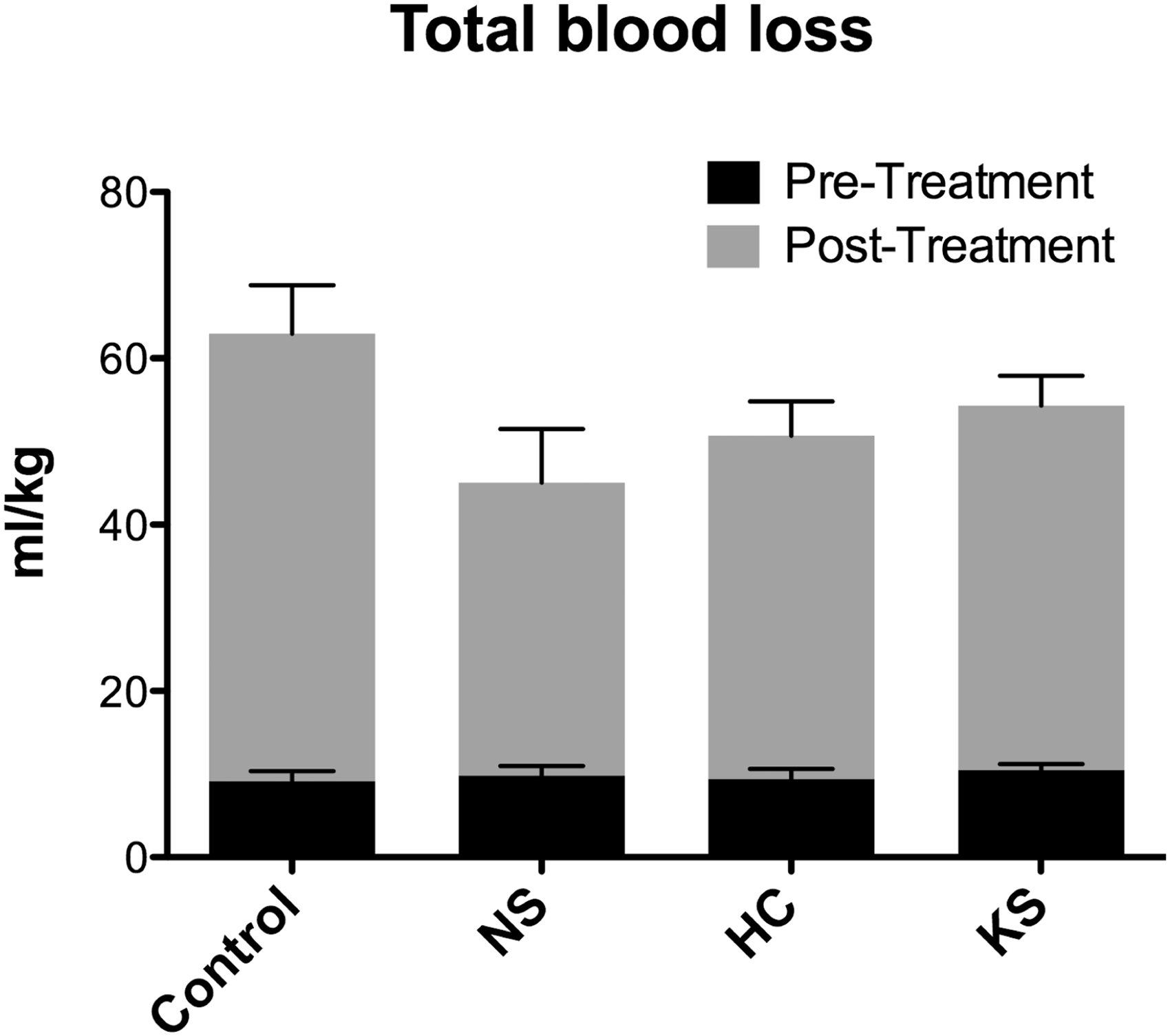
Shock index
Shock index was significantly different in the NS and KS groups compared to the HC- and gauze-treated animals as shown in Figure 5. Shock indexes for NS and KS remained close to 2 throughout the duration of the experiment. These data included extrapolated values for the animals that died prior to 180 min and show that dressing failures in this model were generally catastrophic in the HC and gauze groups, while the animals that did fail when treated with NS and KS, generally failed slower and after over an hour of hold time.
Shock index (heart rate/MAP) is shown for the four treatments tested. Both Nanosan-Sorb and KeraStat had significantly lower shock indexes than control (p < 0.05, Tukey’s multiple comparison test). MAP: mean arterial pressure.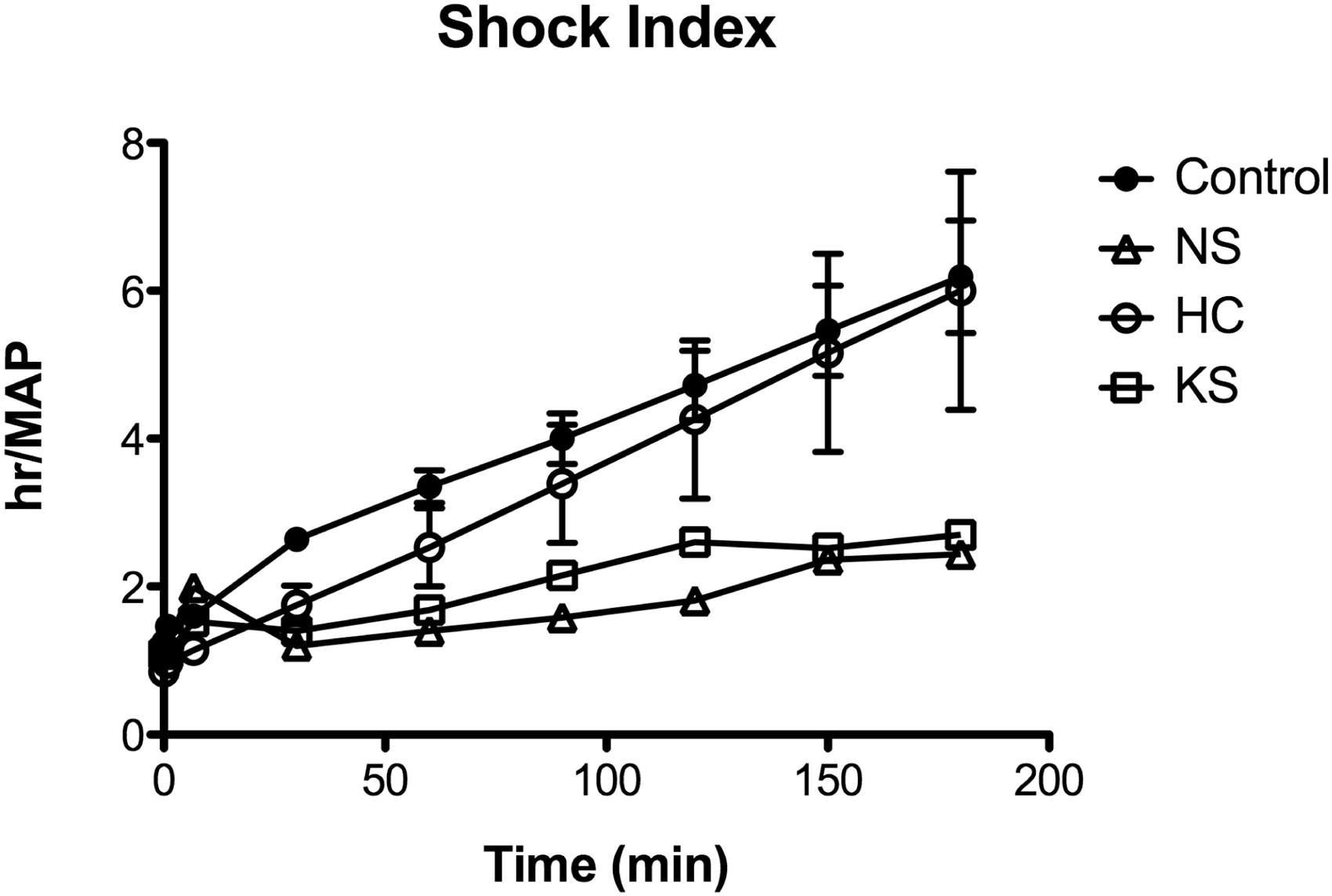
NS blood/plasma absorption and expansion
As shown in Figure 6(a), NS absorbed significantly more blood and plasma per gram of material compared to HC and gauze after 180 min, absorbing more than 15 × its original weight. Additionally the NS material expanded significantly more than standard cotton gauze controls as shown in Figure 6(b). NS doubled its original size while the control gauze only expanded 3.3%.
NS absorption and expansion compared to gauze. Shown in (a) is the absorbed blood/ plasma per gram of gauze and NS; *p = 0.04, t-test, n = 5. Shown in (b) is the percent in area expansion for NS compared to gauze; **p = 0.007, t-test, n = 6. NS: Nanosan-Sorb.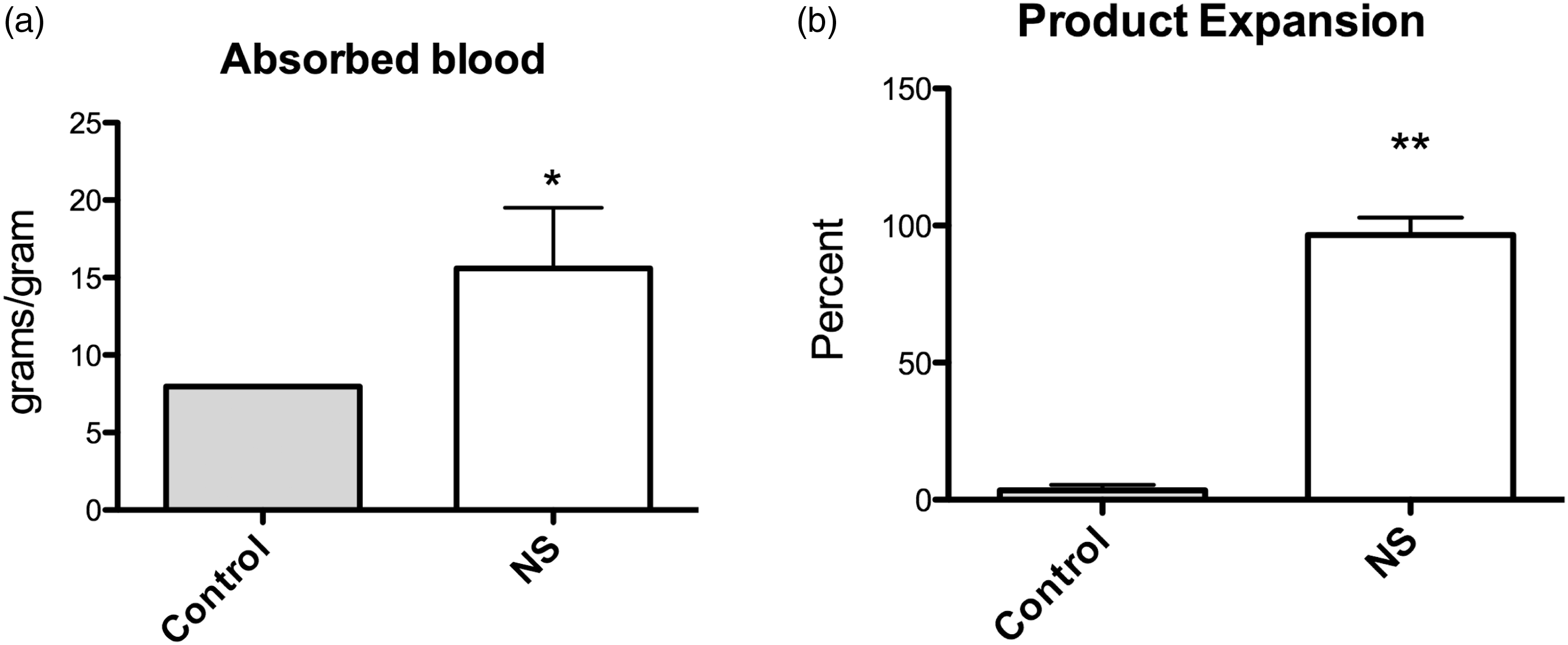
Femoral artery transection model
In order to test the feasibility of using the injectable KS hemostat for non-compressible hemorrhage, a single deep penetration injury was made in 5 animals (4 treated with KS, 1 gauze-treated control) with a US Army M7 bayonet that transected the femoral artery and vein. This injury is shown in the panels in Figure 7(a) and application of the hemostat in Figure 7(b). The four animals receiving KS in this pilot test survived the full 3 h of the test (representative animal shown at 3 h post-treatment in Figure 7(c)). The one animal that was used as a gauze control exsanguinated and was pronounced dead in 11 min. After euthanasia, each injury was examined by gross dissection to confirm that the vessels had been completely transected in all cases.
Shown is the femoral artery puncture model. The femoral artery was located anatomically and verified by palpation. A single stab wound was made with a bayonet shown in (a). KS was then injected in the wound track via a 60 cc syringe (b). 180 min after injury, vitals are stable and there is no additional blood loss even after leg is put through a full range of motion (c). KS: KeraStat.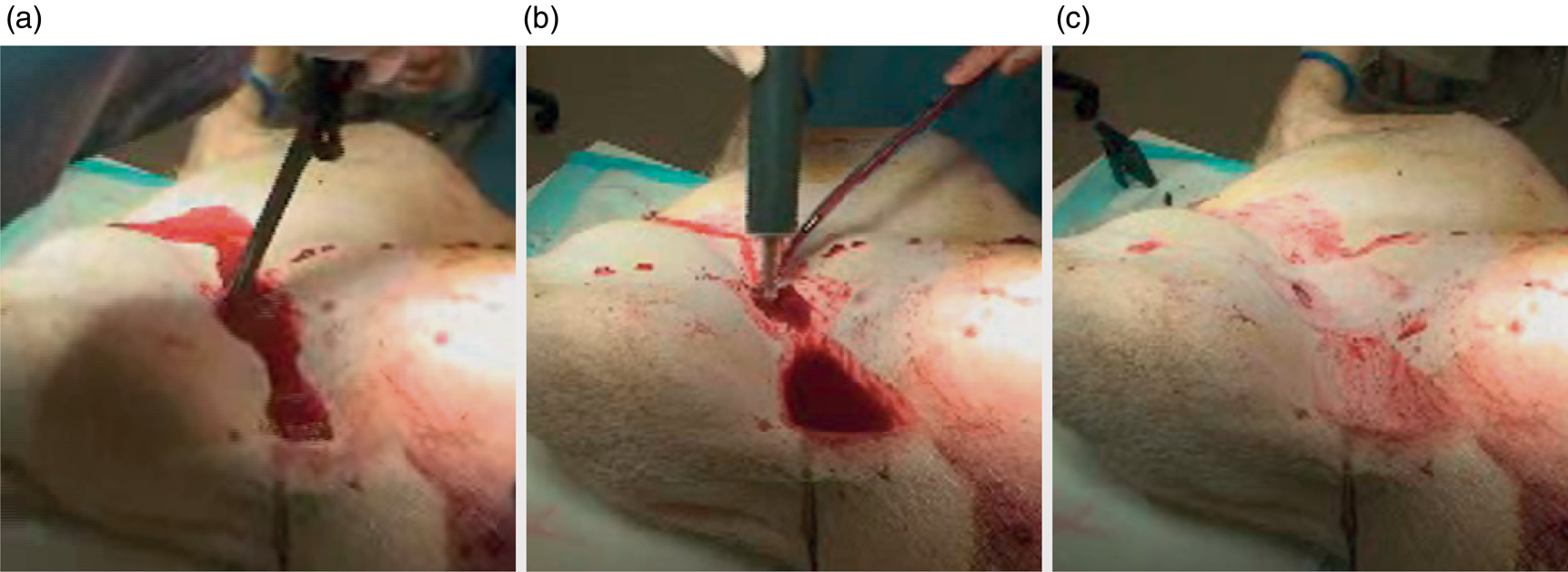
Platelet adhesion assay
To test the hypothesis that platelets bind to the KS surface and that this occurs through integrin binding, gel filtered platelets adhesion was investigated using a colorimetric assay. Prior to incubation with the keratin, platelets were pre-treated with a monoclonal antibody against the β1 integrin subunit. Results shown in Figure 8 demonstrate a 28% decrease in platelet adhesion in the presence of a β1 blocking antibody (p < 0.01, Tukey’s multiple comparison test). The β1 integrin subunit is known to contribute to platelet adhesion on the surface of collagen.15–17 Despite recent work that has shown α2β1 contributes in a supporting role to Glycoprotein VI,
18
β1 integrin mediated adhesion to collagen is the appropriate control to an extracellular matrix-like protein such as keratin. Therefore polymerized type I rat tail collagen hydrogels were utilized as controls, where a significant 22% decrease in adhesion was observed (p < 0.05, Tukey’s multiple comparison test). Platelet adhesion to the negative control, albumin, was not significantly different between active and formaldehyde fixed platelets.
Platelet adhesion to collagen, keratin and albumin substrates. Platelet adhesion was assessed using a colorimetric assay in the presence (β1 blocked) and absence (untreated, positive control) of antibodies against the β1 integrin subunit. Collagen and albumin represented positive and negative controls, respectively, and formaldehyde fixed platelets (Fix. Plt) were internal controls. Platelets pretreated with β1 mAB showed significantly less adhesion on both collagen and keratin substrates. As expected, there was little adhesion to the albumin coating when platelet receptors were fixed (*p < 0.05, **p < 0.01, Tukey’s multiple comparison test).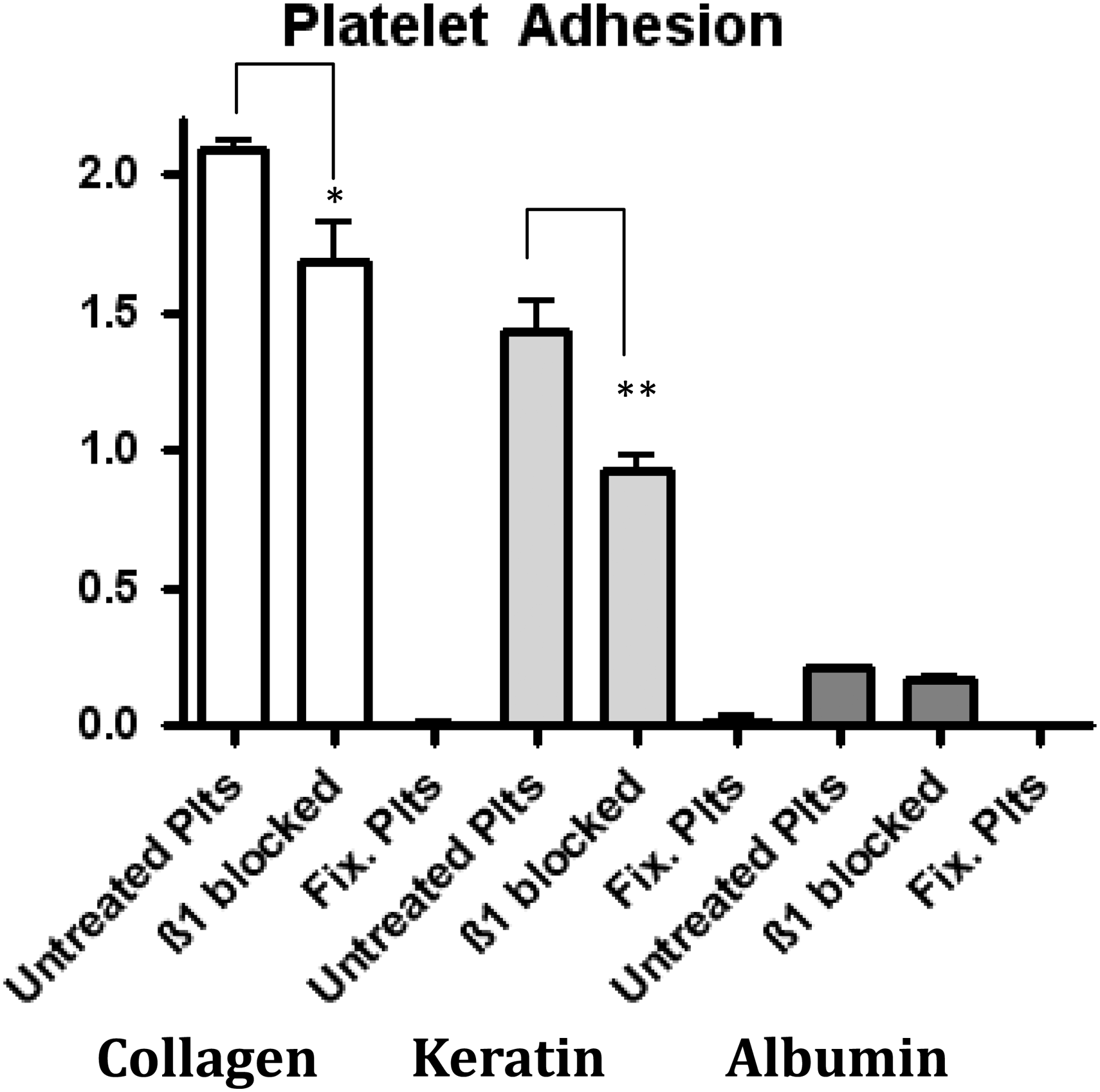
Discussion
In the past decade there have been several studies, many from the USAISR or the Naval Medical Center that have examined the effectiveness of hemostatic agents for treating hemorrhage. These studies have been conducted in models ranging from high flow truncal hemorrhage such as aortic puncture,
19
to low flow liver hemorrhage20,21 or using the model used in this study, high flow lethal extremity hemorrhage.9,10,22–25 In the lethal extremity trauma model in particular, it has been suggested that a highly flexible or injectable agent might provide better hemostasis in a non-compressible or difficult to compress penetrating injury.
20
To test this, we selected two novel hemostatic materials that were either highly flexible like standard gauze (Nanosan-Sorb), or injectable (KeraStat). NS was selected based on the hypothesis that removable, light-weight woven dressings are the main types of hemostatic materials currently used by first responders or combat medics and improvements in their design and function could yield significantly better point of injury care. NS did in fact provide better hemostatic characteristics in terms of survival than the other hemostats tested, presumably by increasing absorption and providing better contact with the wound via increased expansion (see image of expanded NS material in Figure 9(a)). Moreover, the expansion of NS as it absorbed fluid may have sustained some level of compression as the dressing was confined within the wound site. This finding provides a potential future direction for development of new hemostatic materials. Though polyurethane (the base material of NS) is not known to be biologically active, it has been formulated to contain chitosan, kaolin clay or other currently available active ingredients in hemostatic agents that could potentially increase its hemostatic ability.
Shown are three examples of NS (a), HC (b) and KS (c) in three animals that survived the full 180 min. In (a), NS has expanded dramatically and filled the injury cavity. In (b), HC is shown adhered to the injury and surrounding tissue. (c) shows KS after peeling back the gauze secondary dressing. Note the apparent adherence to tissue and fascia.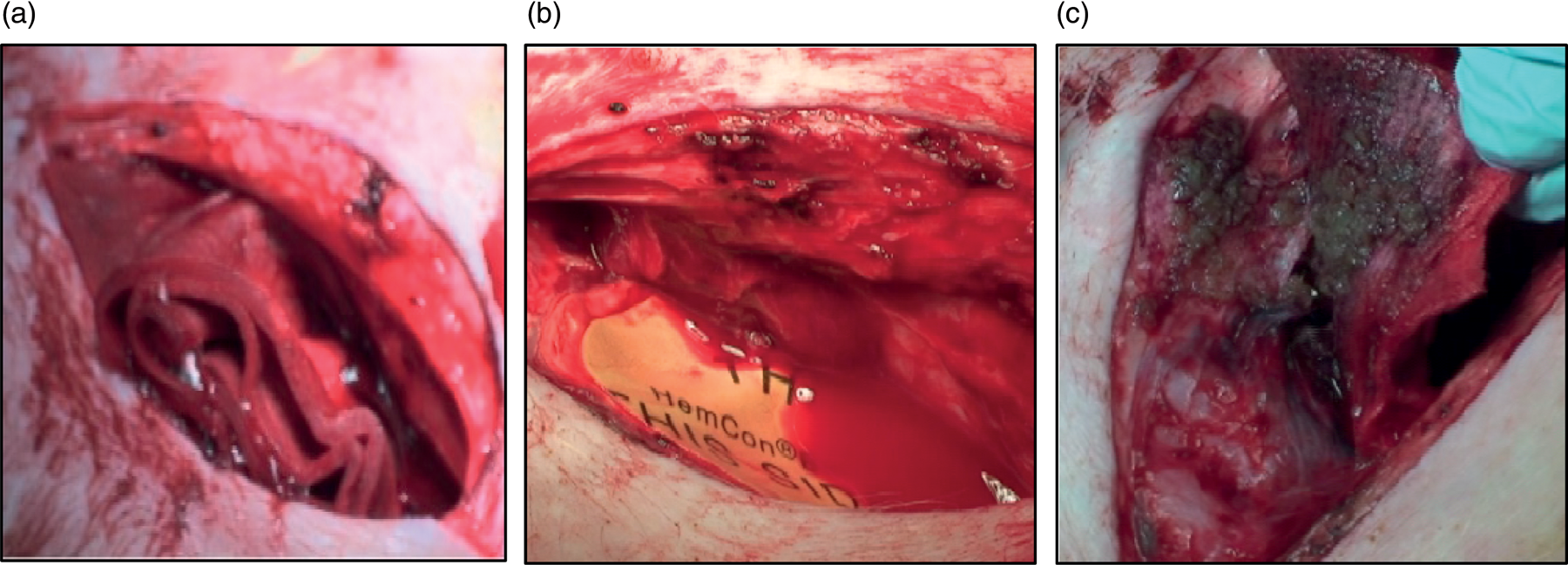
Rigid hemostats such as the second generation HC chitosan bandage did not work very well in this model. Though this bandage adhered well to the surrounding tissue (Figure 9(b)), it was not flexible enough to make consistent contact with the bleeding injury and resulted in high animal mortality. Hemcon Medical Technologies has released a potential solution to this problem known as the ChitoFlex™ bandage that has increased flexibility to conform to contoured wounds. ChitoFlex was not available when this study was conducted, though recent tests that included dressings such as ChitoFlex showed similar performance. 23 Although the HC bandage did not work well in this model, it is important to note that the first generation of this bandage has successfully treated hundreds of service personnel in Iraq and Afghanistan as well as civilian trauma victims and remains a premier solution to tissue injuries that can be visualized or in low flow tissue avulsion injuries.
Another possible avenue for improving hemostat material technology is to develop injectable, left-in-place viscous hemostatic gels such as KS. Injectable, biocompatible agents overcome the inherent limitations of non-degradable materials in that they can be used in non-compressible, difficult to reach single-track injuries such as is often found in gun shot wounds. Additionally, KS is biocompatible and could be left in place if surgical repair is unnecessary, 14 preventing the need for further damage to the injury site during surgery. Historically, the problem with this approach is that viscous injectable materials have not yet been able to overcome high flow arterial hemorrhage that disintegrates the material and prevents it from functioning. While KS is mildly adhesive to the tissue, which may have provided some hemostatic benefit in this study, it required a secondary dressing of cotton gauze to keep the material in place long enough to initiate the clotting cascade. Though this is not necessarily ideal, the type of injury produced in this model provided enough access that packing the wound with gauze would be standard practice for any combat medic or first responder.
The lack of significant differences in blood loss between KS versus control and HC (despite high mortality in the control and HC groups) was likely due to the fact that our definition of death in this model was a MAP <20 for 5 min, not total exsanguination. Animals whose treatments failed early reached this death threshold often with lower blood losses than animals whose treatments failed over the course of several hours, though this was not true in every case. Though it is reasonable to assume that longer surviving animals will increase fluid volume over time via fluid compensation from interstitial spaces, the data was not conclusive. The most conservative interpretation of these data is that total blood loss may not be the best indicator of hemostat performance but should be examined over time with respect to mechanism of failure.
As shown in Figure 9(c), KS integrated to the damaged tissue, forming a thick coating around the injury. Based on this observation, we conducted a pilot study using a femoral artery transection model to test if KS could be used in a single-track high flow hemorrhage. In the four animals that received KS in this model, the confined space of the wound track allowed the material to remain in place with simple manual coverage of the entry wound for approximately 2–3 min. This suggests that injectable agents such as KS could be effective in providing hemostasis in small tract penetrating wounds presumably due to the fact that the proximity of the surrounding tissue to the injury acts to physically stabilize the material and hold it in place. Histological examination of the proximal femoral artery and veins following euthanasia showed that no KS material entered the systemic circulation as has been shown with granulated hemostatic agents. 24 Although this finding was encouraging, it needs to be tested more thoroughly if KS were to be further developed for this type of injury.
To examine the potential mechanism of action for KS, we conducted experiments to test platelet adhesion and activation to KS materials. These data showed that blocking the β1 integrin sub-unit led to a decrease in platelet adhesion on KS and that KS induces platelet activation. Thus we have concluded that β1 integrin platelet adherence and activation is likely involved in the KS mechanism of action.
Testing hemostatic materials often yields inconclusive results based on model design and the fact that trauma is often complicated. The solution has been to engineer very carefully designed and elegant animal models so that they produce consistent injuries with which to test materials. This strategy has limitations and it is important to take the performance of a hemostat in the context of the animal model used to test it. This was recently highlighted in one recent study from the Naval Medical Center using a single-track injury model that showed no differences in four different hemostatic materials compared to gauze. 25 The study concluded that proper wound packing and pressure might be more important than the hemostat used. Though this may be the case in some wounds, it is clearly not the case in all wounds and the data presented here suggest that a strategy of using a highly absorbent expanding material or injectable biologically active material could be a potentially viable solution for certain traumatic injuries.
Footnotes
Acknowledgement
The authors thank Dr Roy Hantgan for his guidance to author Maria B Rahmany in the platelet adhesion assays.
Funding
Partial funding for this project was provided by KeraNetics LLC and SNS Nano.
Mark Van Dyke holds stock and is an officer in the company, KeraNetics LLC, who has provided partial funding for this research. Wake Forest School University of Medicine has a potential financial interest in KeraNetics through licensing agreements. Luke Burnett is currently an employee of KeraNetics LLC, who has provided partial funding for this research, but was formerly a postdoctoral fellow at the Wake Forest University School of Medicine when the swine experiments were conducted. Dr Burnett had no conflict of interest while an employee of WFUSM.
Conflict of interest
None declared.