
Abstract
It is not clear whether surface bioactive chemistry plays an important role in the early osseointegration of micro-structured titanium implants that have the same surface topography at the micrometer and submicrometer scales. In this study, magnetron sputtering methodology was employed for the preparation of Sr coating on sandblasted and acid-etched (SLA) titanium implant without changing the surface characteristics. The study of the surface morphology of the coating was carried out with the use of scanning electron microscopy, and the chemical composition of the surface was examined by X-ray energy-dispersive spectrometry. Twenty SLA implants together with 20 Sr-SLA implants were randomly inserted into the proximal tibia of 20 rats. The early osseointegration of the Sr-SLA implant was compared with SLA implant by removal torque test and histological analysis following two and eight weeks of implantation, correspondingly. As revealed by the surface characteristics, both Sr-SLA and SLA surfaces exhibited similar typical isotropic irregular indentations. The strontium ions were effectively incorporated into the SLA surface (the atomic ratio is 2%). Following two and eight weeks of healing, significant increases in removal torque values (p < 0.05) were taken into observation in respect of Sr-SLA implant. Histologically, the Sr-SLA implants displayed significantly higher bone-to-implant contact percentages and bone area ratio in comparison with the SLA implant at eight weeks (p < 0.05). At two weeks, the bone-implant contact percentages, together with bone area ratio of Sr-SLA surface appeared to be a little bit slightly greater than that of SLA surface. But the statistical difference was not significant. These results indicated that the chemical modification with Sr incorporated by magnetron sputtering treatment in moderately rough surfaced implants remarkably increases early bone apposition.
Introduction
Dental implant has been an efficient and predictable treatment for the replacement of missing teeth in edentulous patients. Wide use of titanium (Ti) is made for load-bearing application, which has exhibited extensive success owing to its exceptional mechanical properties and good machinability in the past decades. 1 For a successful titanium-based dental implant treatment, a direct bone-to-implant contact (BIC), also known as osseointegration, is expected. Nevertheless, in accordance with the guidelines of classical titanium-based implant dentistry, at least 12 weeks are required for the acquirement of appropriate osseointegrated fixation for the implant installation coming to the prosthetic procedure and loading. 2 Recently, various modifications of titanium implant surface have been applied to enhance rapid osseointegration and to shorten the healing period. These modifications are related to surface roughness, surface wettability and chemistry, which are considered as the major factors for successful osseointegration.3–6 Today it is well known that a moderate rough surface together with super wettability lead to an increased bone apposition and bone-implant contact in comparison with smooth surfaces.7–9 However, it is still not clear whether bioactive chemistry plays important role in the early osseointegration of implants or not.
Numbers of research works have demonstrated that Sr is capable of exhibiting pronounced impacts for the reduction of the bone fracture risk in osteoporotic patients. In addition to that, this element has also been reported to promote collagen protein synthesis, improve the osteoblast replication, and lower osteoclast differentiation.10–13 Moreover, recent researches have also reported that Sr is not only capable of promoting mesenchymal stem cell (MSC) commitment to bone lineage, but also it suppress the MSC commitment to adipocytes and chondrocytes.14,15 Owing to the multiple biological function of Sr, it has been introduced in practice for the improvement of the osseointegration of implants. Some studies have investigated the effects of Sr ion implantation on the osseointegration of titanium implants, and demonstrated the positive effects.16–19 But there are few studies that have thrown focus on the early osseointegration of implant.
Owing to the fact that interactions between the biomaterials and biological tissues are likely to undermine the potential of these materials to carry out their designed biological functions, it is considered significant to perform surface functionalization for the purpose of endowing currently available biomaterials with specific and desirable functions. Currently, surface modification can be put to use for the modulation of the surface attributes of substrates, for instance adhesion, wettability, biocompatibility, as well as antifouling. 20 In the recent years, various metal coating techniques have been used in Sr deposition, such as plasma spraying, laser deposition, the electrochemical deposition, poly (vinyl alcohol) (PVA)/poly (lactide-glycolideacid) (PLGA) nanoparticles (NPs), and the sol–gel method.21–24 As one way to employ bioactive ions in the surface modification of Ti implants, magnetron sputtering treatment is not only capable of making the deposition of Sr ions on titanium surface with predictable release values but it is also able to maintain a high mechanical stability. Thus, this study investigated the bioactivity of the Sr-loaded surface through this treatment.
In the present study, we have produced strontium-oxide layer by magnetron sputtering treatment with the use SrTiO3 on the sandblasted and acid-etched (SLA) treated titanium surface and investigated the early osseointegration behavior of Sr-SLA implants in comparison with SLA implants at two and eight weeks of implantation in rat models.
Materials and methods
Sample preparation
The threaded pure titanium implants roughed by sand blasting and acid etching (WEGO Jericom Biomaterials Co., Ltd, Weihai, Shandong, China) are 1.0 mm in outer diameter and 2 mm in length. These were manufactured with a self-tapping threaded area at the outer 1 mm implant end and an internal hex for insertion. This surface modification has been previously described in other studies. 25 To obtain strontium ions incorporated on the SLA implant surface, the magnetron sputtering treatment was used. Magnetron sputtering was performed with an industrial physical vapor deposition system (School of Mechanical Engineering, Shandong University), with material deposited from a sputtering target consisting of SrTiO3 powder with a purity of 99.99% (ZhongNuo Advanced Material Technology Co., Ltd, Beijing, People’s Republic of China). The films were deposited under the following conditions: argon with 0.5 Pa gas composition, 80 W power density, 2700 s deposition time, and 5.5 cm target–substrate distance. So in our study, SLA implant surface was employed as control group and Sr-SLA implant surface fabricated by SLA combined with magnetron sputtering were treated as experimental group. After preparation, all the implants were ultrasonically cleaned using acetone, ethanol, and deionized water, in an order, followed by sterilization with the cobalt-60 irradiation.
Surface morphology of SLA and Sr-SLA implant surfaces was examined by scanning electron microscopy (SEM) (JSM-6500F, JEOL, Tokyo, Japan), The chemical composition of the two kinds of surfaces was examined by X-ray energy dispersive spectrometry (EDS) (SU70, Hitachi, Tokyo, Japan).
Animals and surgical procedure
The rats used in this study were obtained from the Shandong Lvye Pharmaceutical Co., Ltd (Yantai, Shandong, China). Protocols were approved by the Institutional Animal Use Review Board. For this study, 20 female Sprague Dawley rats, aged three months with the body weight of 210 ± 33 g were utilized. Rats were housed with a 12-h light/dark cycle and allowed a standard pellet diet and tap water ad libitum throughout the observation period. Surgical procedures were performed as follows: rats were anesthetized with a peritoneal injection of 4% sodium pentobarbital (0.3 mL/100 g body weight). Forty implants with 20 for each group were randomly inserted into the proximal tibia of 20 rats with one implant for each tibia. Prior to implantation, a full-thickness incision was performed and the implant site was prepared with the use of a 0.9-mm-diameter drill under constant irrigation with sterilized physiological saline solution. Implants were directly inserted due to the self-tapping threaded area at the implant end and confirmed its stability by passive mechanical retention. The wound was closed with conventional sutures. After the surgical procedure, the rats received a single dose of 0.06 mL/kg of penicillin via intramuscular injection for three days.
Rats were sacrificed at two and eight weeks after implant surgery, respectively. The tibias with implants were retrieved for removal torque test and histological analysis.
Removal torque tests
Removal torque test was conducted to assess implant stability in the bone. The removal torque value in Newton centimeters (N cm) reflects the interfacial shear strength. The tibia with implant was fixed with a metal device specifically designed for this purpose, with one connecting shaft in connection with the torque wrench, which is inserted in the internal hex of implant. The pull-out strength was determined as the peak force applied to fully loosen the implant from the bone as measured with a digital torque meter (MGT20Z, Mark-10 Corp., New York, NY).
Histological evaluation
Immediately after sacrifice, the specimens used for undecalcified histological sections were maintained in a 4% neutral formalin buffered solution for three days, then washed, dehydrated in graded ethanol (40–100%), and embedded in methylmethacrylate without decalcification. The calcified bone with the implant in situ was cut into approximately 40–50 µm thick sections parallel to the long axes of the tibia and the implant (Exakt®, Germany). Then the sections above were stained with toluidine blue. All slides were observed and captured in the microscope (Olympus I×71, Japan). The percentage of BIC was measured as the percentage of the length of bone directly contacted with the implant surface. The percentage of bone area (BA) was evaluated by measuring the new mineralized bone tissue area inside all the implant threads.
Statistical analysis
Statistical analyses were conducted by using SPSS (version 14.0 for Windows). The means and standard deviations of data were calculated. Differences between groups were analyzed by Student’s t-test or the non-parametric Mann–Whitney test. Values of p < 0.05 were considered statistically significant.
Results
Surface characterization
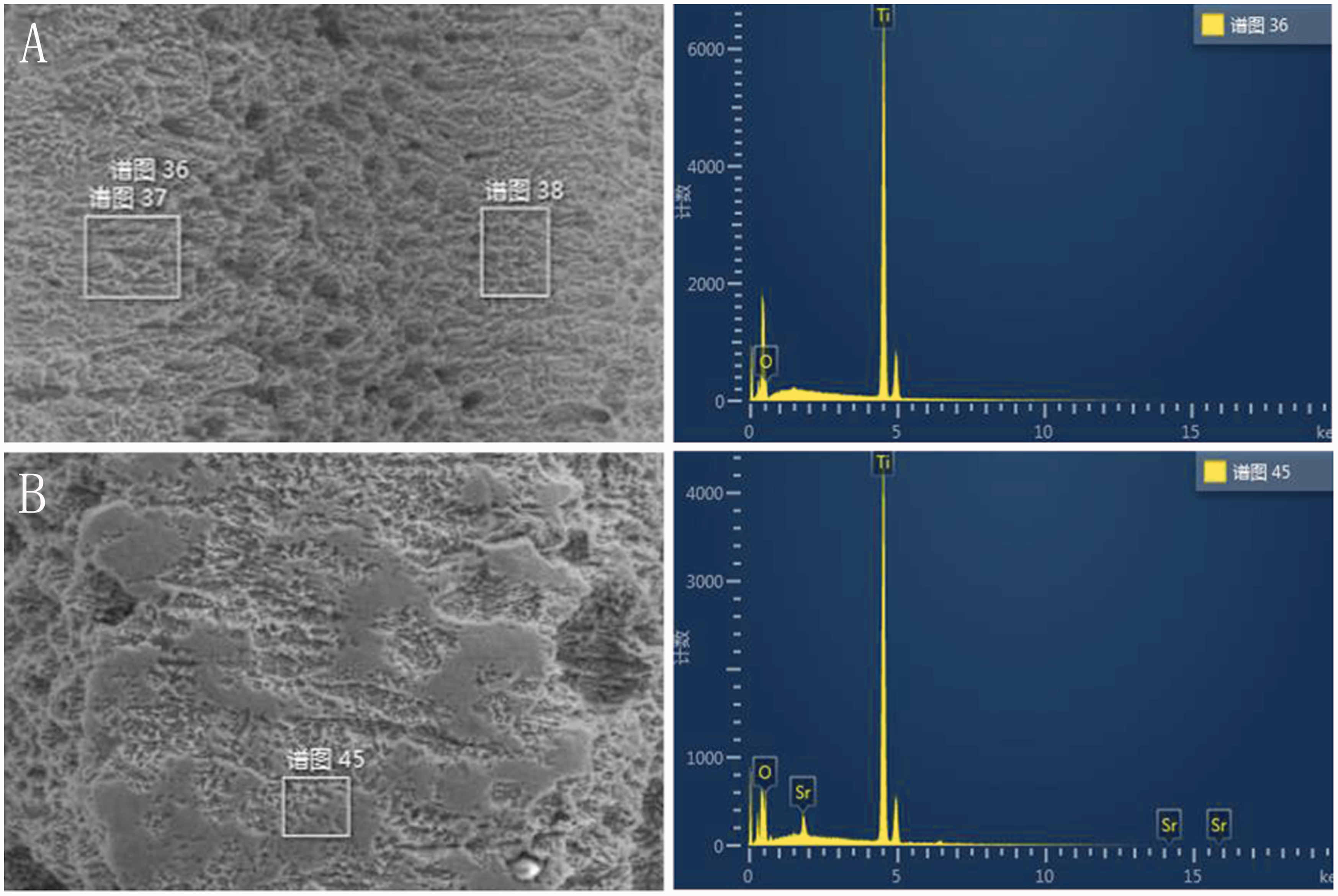
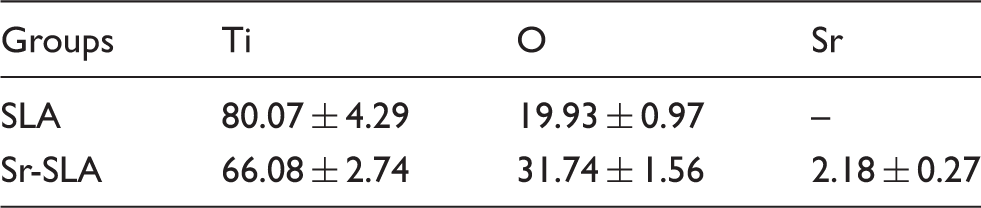
Figure 1 apparently depicted the surface topographies of SLA and Sr-SLA surfaces at macron, micron, and submicron scales. As revealed by the SEM examinations, there were no optical differences between the two surfaces. The chemical composition of the surfaces examined by EDS showed that the Sr-SLA surface primarily contained Ti, O, and Sr elements, while the SLA surface only contained Ti and O elements (Figure 2). The specific element concentration figured out by EDS was summarized in Table 1. These results indicated that the magnetron sputtering treatment can effectively incorporate Sr ions into the SLA surface without substantially altering the original surface topography at the micron and submicron scales.
SEM micrographs showing the surface roughness of SLA (A, B, C and D) and Sr-SLA (E, F, G and H) surfaces at magnifications of 100x (A and E), 2000x (B and F), 10,000x (C and G) and 20,000x (D and H). SEM: scanning electron microscopy; SLA: sandblasted and acid-etched. X-ray energy-dispersive spectrometry (EDS) of SLA (A) and Sr-SLA (B). SLA: sandblasted and acid-etched. Result of the Ti, O, and Sr element concentration determined by X-ray energy dispersive spectrometry which was expressed as atomic percentage (%) (n = 8). SLA: sandblasted and acid-etched.
Removal torque tests
The removal torques of the titanium implants in the Sr-SLA groups were significantly higher than that of SLA implants at two weeks (9.96 ± 1.87 vs. 7.43 ± 2.16 N cm, p < 0.05) and eight weeks (18.84 ± 3.38 vs. 15.04 ± 1.82 N cm, p < 0.05). The scatter diagram and of removal torque values for the two groups have been illustrated in Figure 3.
The removal torque value (N cm) for the two groups at two and eight weeks. Data are expressed as mean ± SD (n = 9). *Refers to p < 0.05 versus 2w SLA. #Refers to p < 0.05 versus 8w SLA. SLA: sandblasted and acid-etched.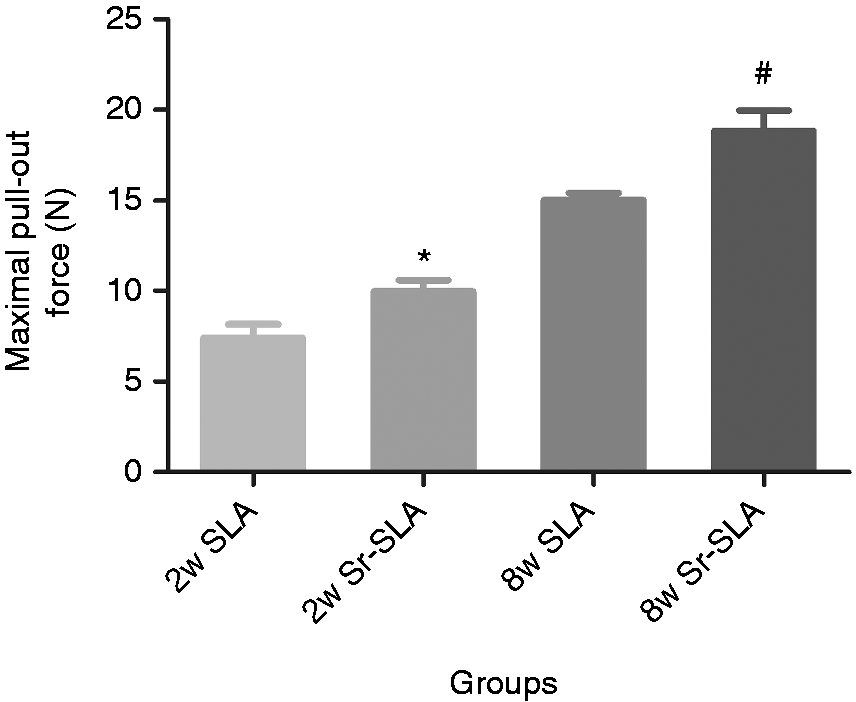
Histological evaluation
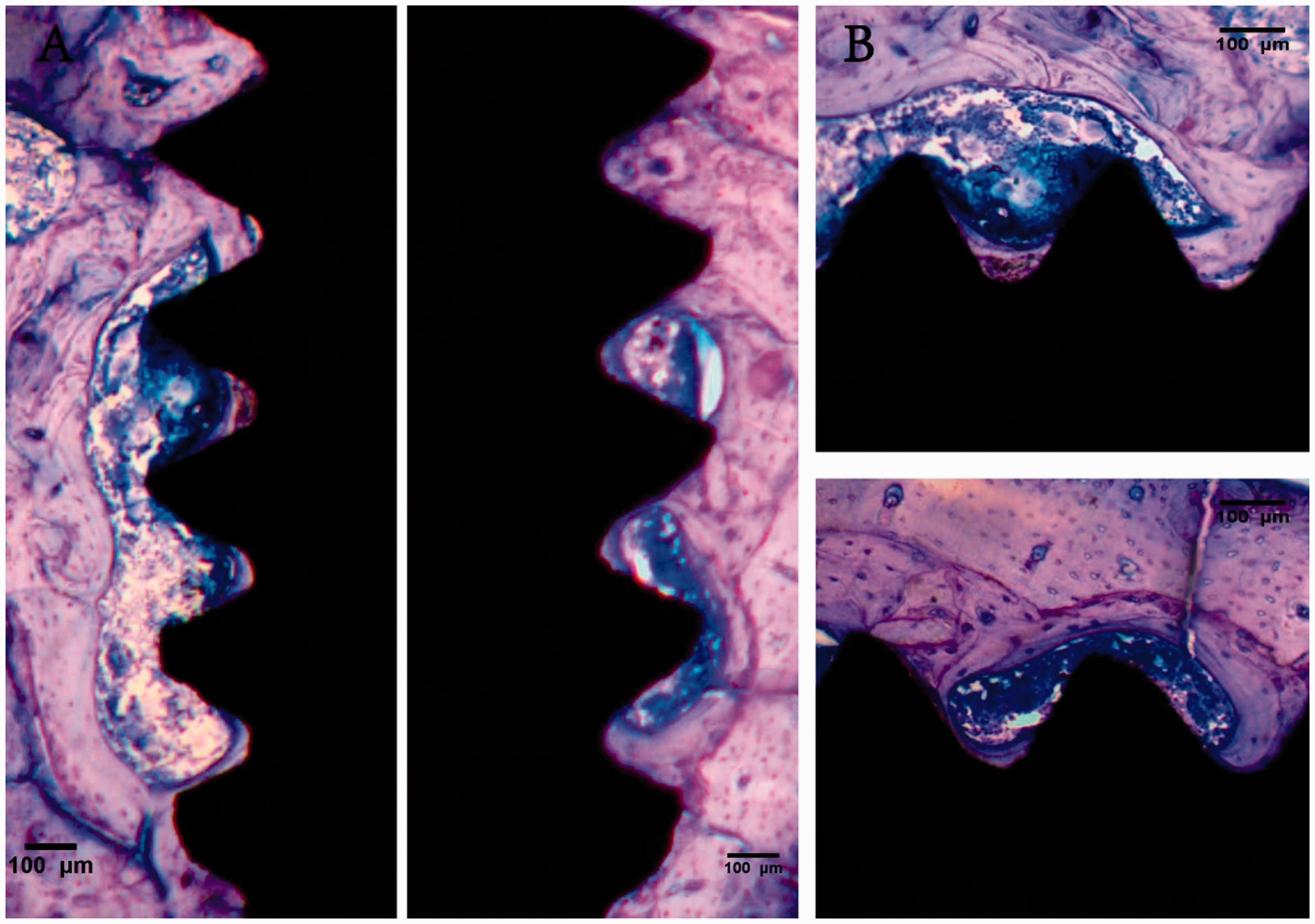
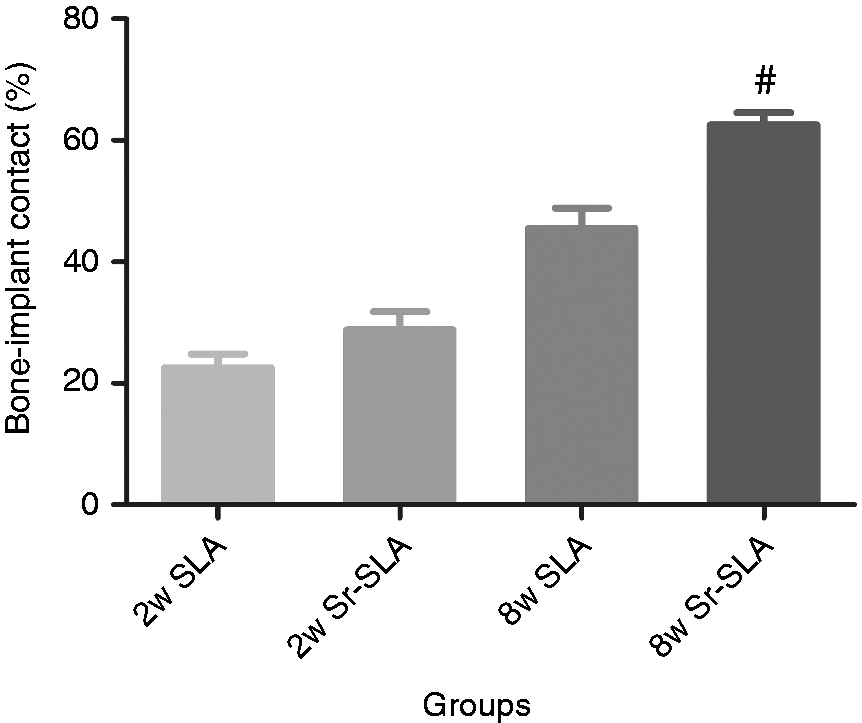
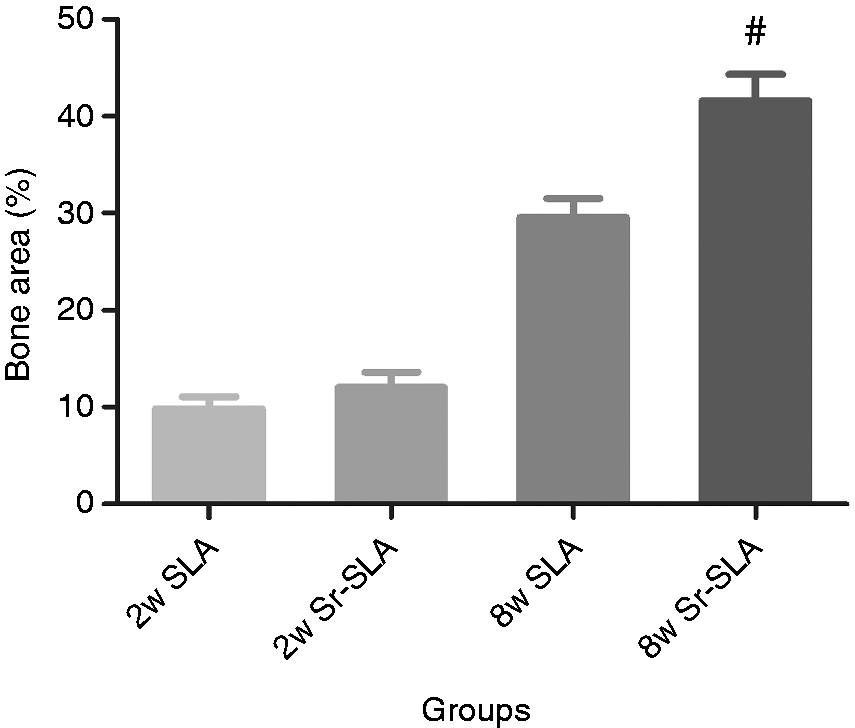
Two and eight weeks after implantation of all implants in the control and experimental groups had direct histological contact with the surrounding bone, showing no signs of inflammation at the bone-to-implant interface (Figures 4 and 5). Implant ossteointegration was evaluated by measurement of BIC and BA. The results of histological analysis and comparisons between the two groups have been shown in Figures 6 and 7. The BIC and BA values in each group increase notably with healing time. At two weeks BIC% (28.76 ± 8.44% vs. 22.57 ± 6.29%) and BA% (12.02 ± 4.45% vs. 9.82 ± 3.49%) were higher in the Sr-SLA group as compared with that in the SLA group, but not significantly higher. At eight weeks, the Sr-SLA implants showed significantly greater BIC% (62.53 ± 5.78% vs. 45.54 ± 9.59%, p < 0.05) and BA%(41.62 ± 7.75% vs. 29.55 ± 5.53%, p < 0.05) in comparison with the SLA implants.
Histological sections at (A) 40- magnification of the SLA (left) and Sr-SLA (right) implants showing entire threads and (B) 100-magnification of the SLA (upper) and Sr-SLA (lower) implants two weeks after implantation in proximal tibia of rats. The Sr-SLA implant shows more continuous bone apposition compared with the SLA implant (stained with toluidine blue). SLA: sandblasted and acid-etched. Histological sections at (A) 40- magnification of the SLA (left) and Sr-SLA (right) implants showing entire threads and (B)100-magnification of the SLA (upper) and Sr-SLA (lower) implants eight weeks after implantation in proximal tibia of rats. The Sr-SLA implant shows more continuous bone apposition compared with the SLA implant (stained with toluidine blue). SLA: sandblasted and acid-etched. BIC of implants after two and eight weeks of insertion. Data are expressed as mean ± SD (n = 8). #Refers to p < 0.05 versus 8w SLA. BIC: bone-to-implant contact; SLA: sandblasted and acid-etched. BA of implants after two and eight weeks of insertion. Data are expressed as mean ± SD (n = 8). #Refers to p < 0.05 versus 8w SLA. BA: bone area; SLA: sandblasted and acid-etched.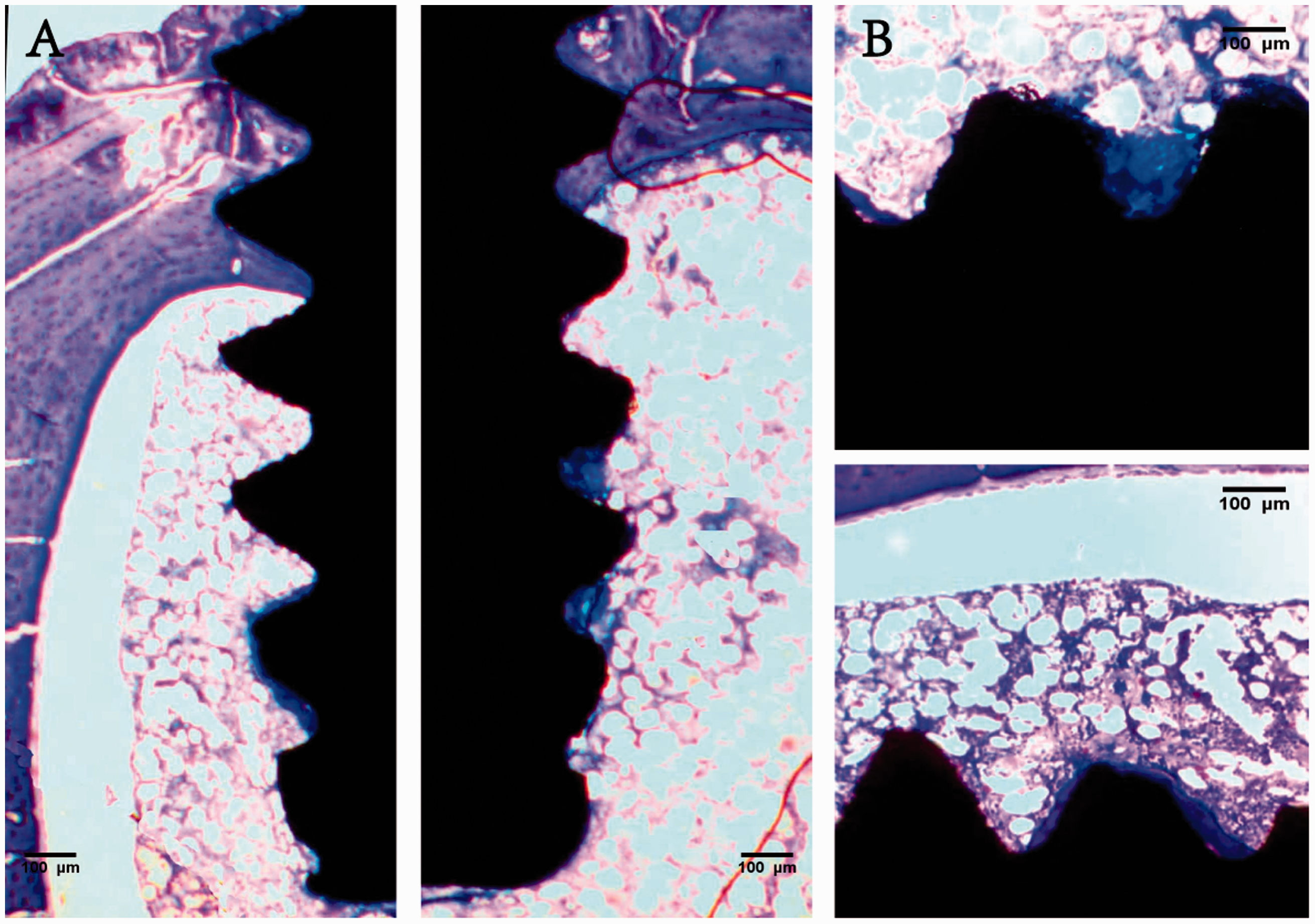
Discussion
In this study, Sr coatings on SLA Ti implants were prepared by magnetron sputtering methodology. The surface of Sr-SLA and SLA showed similar morphology from SEM micrographs. EDS analysis revealed that Sr ions were incorporated into Sr-SLA surfaces and the ratio of Sr-coatings determined was 2%. These experimental results demonstrate that Sr-SLA implants possess better bone formation and osseointegration properties in comparison with SLA implants from the removal torque test and histological analysis obtained at two and eight weeks.
Sr is termed a natural component of food and beverages. Currently, a considerable amount of research has indicated the dual effects of stable Sr ions to promote bone formation and reduce bone resorption.26–28 In addition to the systemic application of strontium, the local application of strontium is considered as an alternative methodology. Local application can avoid the potential adverse reactions, such as toxic epidermal necrolysis, drug rash with eosinophilia and systemic symptoms syndrome. 29 Accordingly, Sr surface coating was put to use in our study. For the modification of the chemistry, although strontium’s mechanisms of action on osteoblasts are not fully understood, the promotion and the acceleration of new-bone formation on normal as well as osteoporotic individuals were confirmed by a series of cellular and animal experiments. But the ratio of Sr is proven to be high in most of the studies.30–32 Nonetheless, a series studied demonstrated that the effects of Sr were dose-dependent: low dose of Sr was favorable for bone formation, and a high dose of Sr may have produced a destructive effect on the bone mineralization.33,34 Therefore, the atomic ratio of Sr-coatings on SLA surface was controlled with 2% in this study. In general, the impact of adding Sr into a bioactive layer for the enhancement of osseointegration can be analyzed by the preliminary amount of Sr in weight, in atomic or in molar concentration.31,35,36 In this work, the amount is detailed in atomic percentage.
Magnetron sputtering is widely used in various industrial applications with great success. The coating was prepared with the use of this treatment that had high bonding strength at the interface 37 and various inorganic components could be deposited on the materials by changing the targets. 38 Via these techniques, we developed a novel surface that was different from classical SLA surface in chemistry component. But in micron and submicron scales, it exhibited similar typical isotropic irregular indentations with SLA surface. These results indicated that the magnetron sputtering treatment effectively incorporates Sr ions into the SLA surface without substantially altering the original surface topography. Being different from this study, Li et al. 32 developed a Sr-loaded Ti surface fabricated through hydrofluoric acid etching followed by magnetron sputtering, which not only changed the chemistry component of the material surface but also obtained a nano-structured deposition. Another study investigated the biological effects of Sr-SLA implants in comparison with SLA implants by hydrothermal treatment also found that the Sr-SLA surfaces exhibited more thickly dotted nanostructures made of heterogeneous granules with a size of nearly 50 nm in diameter. 39 This may be interpreted by the specific preparation parameters or the magnification of SEM images of the surface is not sufficiently large. In addition, it is worth mentioning that the control group in our experiment was the SLA surface implant that was the most widely-used commercially available implants surface. Magnetron sputtering deposition has been reported to be producing Sr coatings on various material surface. The 2% Sr coatings were prepared on SLA surface implants by this methodology in this study for the first time. Therefore, the developed coating platform may have more clinical implications in implantology.
Overall, it can be suggested that Sr-SLA implants possess better bone formation property attributes as compared with SLA implants due to the Sr biological effects obtained by the biomechanical and histological results at early periods although there was a little tendency towards greater BIC and BA values for the Sr-SLA surface after two weeks in comparison with the SLA control surface. In regard to the early osseointegration of implant modification by Sr ions, Fan et al. 39 demonstrated that the Sr-SLA implants presented significantly higher removal torque value and presented higher BIC than SLA implants in cortical bone at three weeks. Park et al. 40 also observed the beneficial effects of Sr in vivo as bone formation. They found that chemically modified surfaces with Sr ions revealed higher torque removal values for Sr-enriched surfaces when compared to a SLA bioactive surface following a two-week implantation period. But the two studies above made use of hydrothermal treatment for the purpose of incorporating strontium ions into the titanium implants. On the other hand, we adopted the magnetron sputtering methodology. Li et al. 32 also developed a hierarchical hybrid micro/nanorough strontium-loaded Ti (MNT-Sr) surface fabricated through hydrofluoric acid etching followed by magnetron sputtering and discovered the fact that the novel MNT-Sr surface ultimately exerted a highly beneficial effect on osseointegration in comparison with other surfaces in cellular and animal experiments. But this paper investigated the long term effect of strontium-oxide layer on Ti surface at 12 weeks instead of the early period. Coincide with our result, there were still many studies that indicate that strontium increases bone formation and reduces bone resorption, leading to a gain in bone mass as well as improved bone mechanical properties in normal animals.41–44 However, due to the differing regions of interest, implant geometry and animal models, a direct comparison of those data with this study is not possible. Collectively, all the studies, including ours, point toward a benefit of Sr coating surface for early osseointegration with dental implants.
This study has three limitations. First of all, there was no group following four weeks of implantation in terms of the relative short healing period. On the second place, there were no groups containing different doses of metal ions, which can affect the results of our experiment. On the third place, extensive investigations of strontium have been carried out both in vitro and in vivo for its dual action of promotion of new bone formation and inhibiting bone resorption. The impact of Sr on osteoclast and bone resorption was inexistent in this study. Prospective detailed study designs are required for confirming the superior bone healing-promoting impact of Sr chemistry.
In summary, the chemical modification with Sr incorporated in moderately rough surfaced implants notably increases early bone apposition in comparison with the rough surface alone. As revealed by these results, the bone apposition promoting effect of micro-structured SLA implants may be further strengthened through the use of Sr chemistry.
Conclusions
The integration of 2% Sr ions into SLA surface by magnetron sputtering maintained the original surface topography. Moreover, EDS analysis confirmed that the Sr element existed in the coating. Sr-SLA surface showed increased removal torques, BIC, and new bone apposition around implants. The result indicated the Sr-SLA surface has a synergistic effect for enhanced early osseointegration, and it is likely to be a promising option for patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Taishan Oversea Expert Foundation (Grant No: tshw20120233) and Shandong Medical science and Technology Development Program (Grant No: 2016WS0694).