
Abstract
The objective of the present study was to incorporate strontium into calcium phosphate cement combined with a lower single-dose local administration of bone morphogenetic protein-2 to enhance its in vivo biodegradation and bone tissue growth. After the creation of a rodent critical-sized femoral metaphyseal bone defect, strontium-modified calcium phosphate cement was prepared by mixing sieved granules of calcium phosphate cement and 5% SrCO3 for medical use, and then strontium-modified calcium phosphate cement with dripped bone morphogenetic protein-2 solution (5 µg) was implanted into the defect of OVX rats until death at eight weeks. The defected area in distal femurs of rats was harvested for evaluation by histology, micro-CT, and biomechanics. The results of our study show that a lower single-dose local administration of bone morphogenetic protein-2 combined local usage of strontium-modified calcium phosphate cement can increase the healing of defects in OVX rats. Furthermore, treatments with single-dose local administration of bone morphogenetic protein-2 and strontium-modified calcium phosphate cement showed a stronger effect on accelerating the local bone formation than calcium phosphate cement and strontium-modified calcium phosphate cement used alone. The results from our study demonstrate that combination of a lower single-dose local administration of bone morphogenetic protein-2 and strontium-modified calcium phosphate cement had an additive effect on local bone formation in osteoporosis rats.
Keywords
Introduction
Osteoporosis, the most common bone disease characterized by microarchitectural deterioration, low bone mass, and bone fragility leading to an increased risk of fractures, has become a major health problem worldwide.1–3 Once bone fracture or defect occurs, plastic surgery is needed for bone repair. One of the most common programs which has been widely accepted to treat bone fractures and regenerate bone loss is the autograft.4,5 Nowadays, the synthetic materials have received much attention since limited availability of donor sites and potential rejection syndromes for autologous bone grafts and allogenous bone grafts, respectively. 6 Calcium phosphate cement (CPC) is one of the most widely used bioactive ceramics for bone regeneration materials, owing to its high biocompatibility, biodegradability, and osteoconductivity. 7 Unfortunately, the currently available synthetic orthopaedic implants showed limited satisfaction of bioactivity and therapeutic efficacy, which motivated the design of new bone substitutes or modification of these old ones, such as by entrapping growth factors or metal ions.8,9
Strontium (Sr), a bone-seeking element, has been shown to be an effective anti-osteoporotic drug, owing to its anti-resorptive and bone-forming effects, through both in vitro and in vivo experiments. 10 Our previous studies demonstrated that the presence of Sr in calcium phosphate promotes biomaterials resorbability and subsequent bone formation.9,11 It has also been demonstrated that Sr at low dose enhances the replication of preosteoblastic cells, suppresses bone resorption and maintains bone formation. 12 The use of growth factors is a common means of enhancing effectiveness and accelerating the healing process: Bone morphogenetic protein-2 (BMP-2) is one that triggers increased bone formation. 13 BMP-2 has been widely studied as a treatment for bone healing due to its excellent osteoinductivity. BMP-2 can regenerate bone by gathering osteoprogenitor cells and inducing osteogenic differentiation. The combination of microporous calcium phosphate scaffolds and BMP-2 can accelerate healing up to 4-fold. 14 A number of studies support the use of BMP-2 in the complicated cases of open tibial shaft fractures and in tibial nonunions. 15
It has reported that Sr promotes osteoblast differentiation including upregulating expression of the endogenous BMP-2 probably via a calcium sensing receptor (CaR)-dependent mechanism. 16 Inspired by these above investigations, we want to further explore whether exogenous Sr can exert effects on improvement bioactivity of exogenous BMP-2, and the promotion bone defects healing. The objective of this study is to develop strontium-CPC combined with single-dose local administration of BMP-2 (BSCPC), and use the composite biomaterials to release Sr. We assumed that the composite biomaterials would combine the advantages of CPC, BMP-2 and Sr, and therefore exhibit excellent osteoconductivity and osteoinductivity. In this study, we investigated the BSCPC and its effects on osteoporotic bone defects in rats.
Materials and methods
Preparation of CPC and SCPC
The CPC precursor powders were prepared with equimolar TTCP (Ca4 (PO4) 2O) and DCPA (CaHPO4) as in the previous study. 7 For the SCPC, SrCO3 was introduced into the CPC precursor powders with different contents at a solid phase, considering that SrCO3 is a stable compound containing fixed Sr. The prepared cement powders were then mixed into a paste with ultrapure water in a liquid-to-solid ratio (L/S) of 250 μL/g. Then, the cement paste was packed in a stainless-steel mold (3 × 5 mm, diameter × height) at 1 MPa for 1 min, after which the resulted samples were placed at 37°C and 100% relative humidity for 72 h. The samples with 0 and 5 wt.% of SrCO3 were named as CPC and SCPC, respectively, and the 5% ratio of Sr content according to previous reports.9,11,17
Animals
Seventy female Sprague Dawley (SD) rats (three months old) with an average weight of 230 g were included in this study. Every four animals were kept in one cage with climate-controlled conditions (25°C; 55% humidity; 12 hours of light alternating with 12 h of darkness). Free access to standard laboratory diet and tap water was permitted. Principles of laboratory animal care were followed, and the study protocol was approved by the Animal Research Committee of the university.
Surgery and treatment
After bilateral ovariectomy (N = 45) or sham operation (N = 5) according to previous reports,9,18 12 weeks were allowed to pass before defect surgery for the establishment of standard osteoporotic animal models. Each five randomly selected ovariectomized (OVX) rats and the five sham-operated ones were euthanized. The distal femurs were harvested for bone mineral density (BMD) evaluation to confirm the establishment of osteoporosis. Then all animals were randomly divided into four groups (10 rats in each group), control group (CON), CPC group (CPC), SCPC group (SCPC) and BSCPC group (BSCPC); Afterwards, femoral cylindrical defects were created, which were standardized at 3 mm in diameter, penetrated internal and external about 5 mm in length, and lay above the distal epiphyseal growth plate as previously described,19,20 and the defects from group CPC were filled with CPC material, SCPC and BSCPC were filled with SCPC composite material; and the defects of group BSCPC were dripped 1 ml physiological saline solution with 5 μg BMP-2 (recombinant human BMP-2, Peprotech, Rocky Hill, NJ) at the same time. The subcutaneous and skin layers were closed, using resorbable polyglactin (Vicryl, 4–0; Ethicon, USA) and resorbable Monocryl (4–0; Ethicon, USA) sutures respectively; 800,000 IU penicillin sodium (North China Pharmaceutical Group Corporation, China) was injected intramuscularly before and after operation for three days to prevent infection. The retrieval procedure was performed at 8 weeks (10 rats at each time point), when the animals were sacrificed using an overdose of barbiturate (Mebumal, ACO L €akemedel AB, Solna, Sweden). For the subsequent analytical technique at eight weeks, the skin was carefully reopened and the bone defect site with the overlying membrane and soft tissue were harvested en bloc and preserved in formalin.
Animal sacrifice and specimen collection
At the end of the observation time (eight weeks after defect), animals were euthanized by cardiac puncture under general anesthesia in the early morning. At necropsy, the rats were exsanguinated by cardiac puncture. At the time of sacrifice, the right distal femurs were used for Micro-CT, histological evaluations, biomechanical tests.
Micro-CT evaluation
The samples were fixed in 4% formaldehyde for 24 h at room temperature. A Micro-CT imaging system (μCT 50, Scanco Medical AG, Bassersdorf, Switzerland) was used to evaluate new bone formation within the defect region. All samples were placed in a custom-made holder to ensure that the long axis of the drilled channel was oriented perpendicular to the axis of X-ray beam. Scanning was performed at 55 kV and 114 μA with a thickness of 0.048 mm per slice in medium resolution mode, 1024 reconstruction matrix, and 200 ms integration time. For analysis of the bone regeneration process within the defect, the central 2.5-mm diameter region of the 3-mm diameter defect was defined by drawing circular contour as area of measurement per slice, thus to obtain a consistent volume of interest (VOI) and to avoid including the native bone margins. The parameters computed from these data included bone volume/tissue volume (BV/TV), trabecular thickness (Tb.Th), trabecular number (Tb.N), and trabecular separation (Tb.Sp) as previously described.21,22
Biomechanical testing
Compression testing of the distal femoral metaphysis was conducted as previously described.23,24 The end of the dorsal distal femur (both condyles) was placed in a 5 mm wide and 2 mm-deep notch of an aluminum alloy base, which was fixed to the mechanical testing system (MTS Landmark Systems, USA). This position resulted in stable three-point contact with the base so that the femur could not slip during the breaking test. A 1 N preload was applied to the ventral aspect of the condyles and then compressed until failure at a rate of 2 mm/min. The ultimate load at failure was determined as the strength of the condyles.
Histological examination
The histological specimens were fixed in 4% paraformaldehyde for seven days, dehydrated with ethyl alcohol, embedded in methylmethacrylate (MMA), and sectioned transversely at a thickness of 50 μm with the Leica SP1600 saw microtome (Leica Biosystems, German) in the middle third in length of the distal femoral metaphysis. The slides were stained with Van Gieson for histological evaluations. The bone formations in the scaffolds were observed using a microscope and a digital camera (Leica Microsystems) as previously described.25,26
Statistical analysis
Data were expressed as mean ± standard deviation (SD). Statistical analyses were performed using the statistics package SPSS 19.0 (SPSS, Chicago, IL, USA). Multiple comparisons between groups were carried out using one-way ANOVA and Tukey's post hoc test. The significance level of 0.05 was applied for all analyses.
Results
Clinical observation
Five rats in total were excluded from analysis due to anesthetic accident, infection, and there were five animals left for evaluation in each group at each observation time. The BMD of the tibial metaphysic was measured in vivo by dual-energy X-ray absorptiometry (Lunar Prodigy Advance, GE Lunar, Madison, WI, USA). The BMD of the tibial metaphysis from the Sham and OVX groups was 230.23 ± 29.23 (mg/cm2) and 164.46 ± 26.89 (mg/cm2). In quantitative analysis, the BMD of the tibial metaphysis from sham-operated rats was 28.7% higher than those of OVX rats (t test, P < 0.05). These results confirmed the establishment of osteoporosis in OVX rats.
Microstructure parameters
The images of the three-dimensional reconstructions of the trabecular in the defects are clearly shown in Figure 1 and the quantitative results were expressed as BV/TV, Tb.Th, Tb.N and Tb.Sp (Figure 2). After treatment with CPC, BMP-2 and Sr for eight weeks, the microarchitecture parameters BV/TV, Tb.Th, Tb.N were significantly lower, and the microarchitecture parameters Tb.Sp were significantly higher than the CON group(P < 0.05), and notable difference in BV/TV, Tb.Th, Tb.N and Tb.Sp was observed among group CPC, SCPC and BSCPC (P < 0.05). Moreover, the rats in group BSCPC presented the strongest effect on BV/TV, Tb.Th, Tb.N and Tb.Sp regardless of treatment groups.
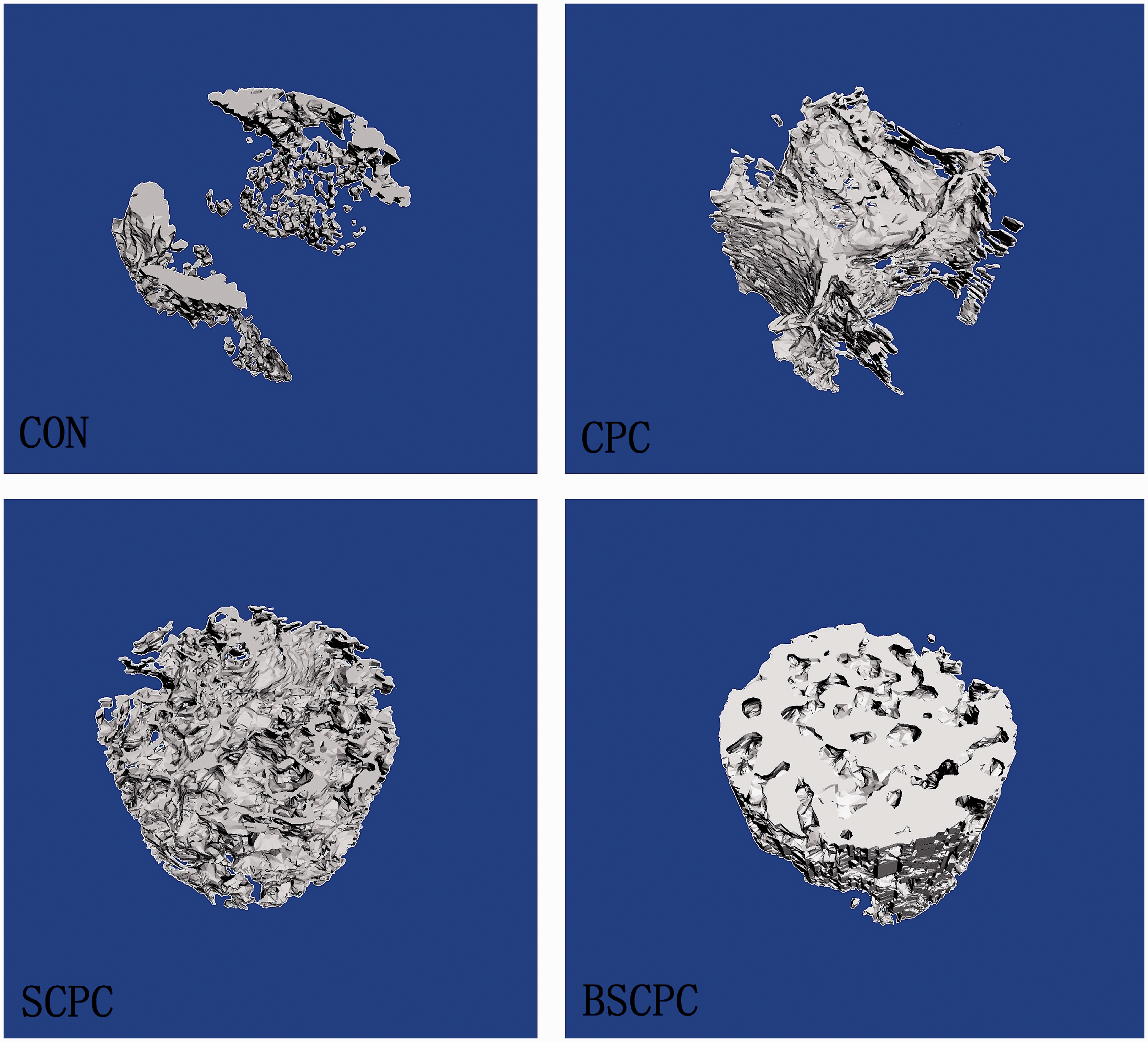
Conditions of repairing in defect was exhibited by 3D reconstruction after euthanasia of each rat in four groups for eight weeks.
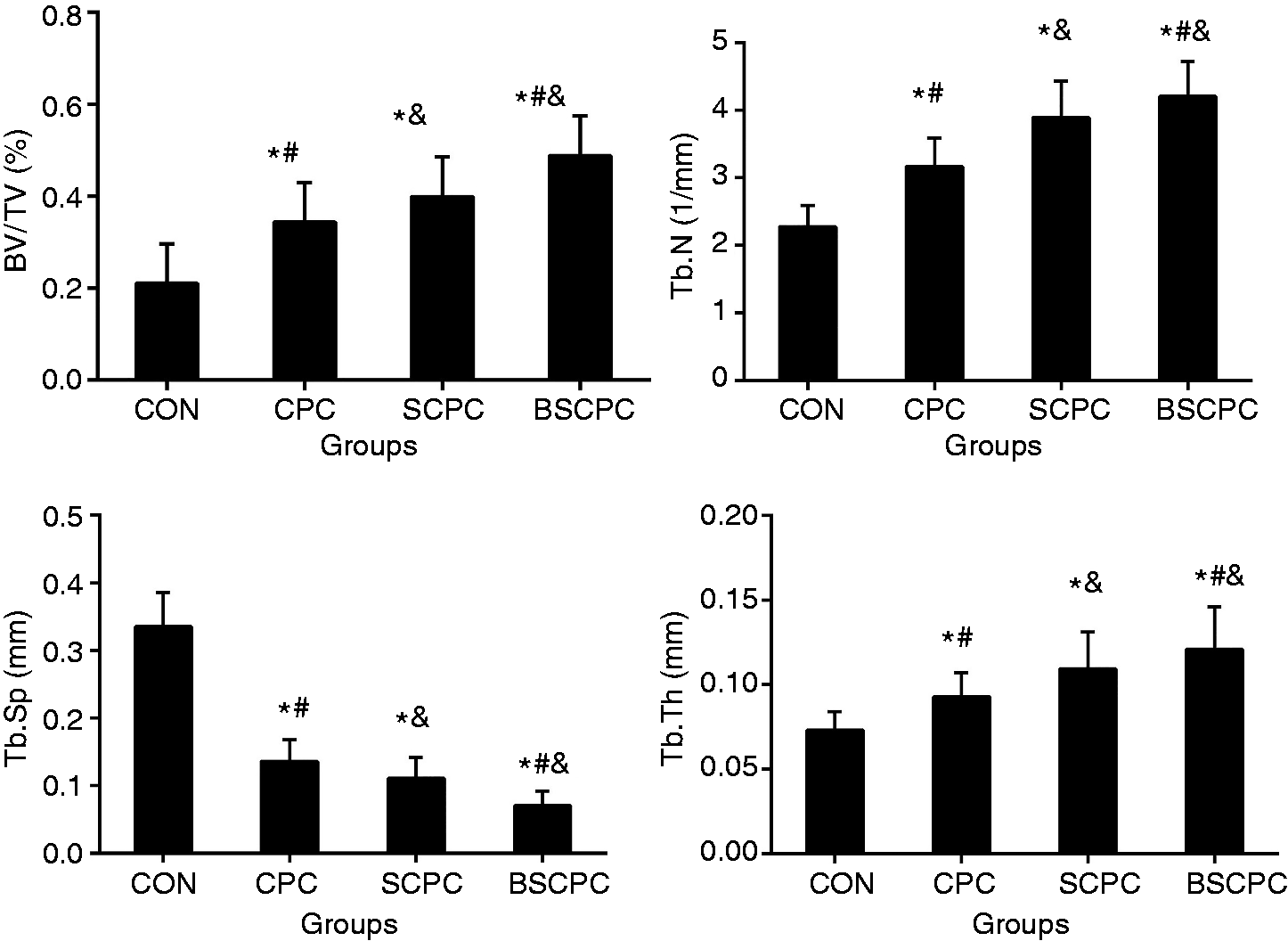
Quantitative results of Micro-CT analysis expressed as BV/TV, TB.N, Tb.Sp, and Tb.Th. Data were expressed as mean ± SD; error bars in the figure are presented as SD, N = 5 specimens/group. *P< 0.05 versus CON group, #P < 0.05 versus CPC group, &P < 0.05 versus SCPC group (by one-way ANOVA and Tukey’s post hoc test).
Histology analysis
At eight weeks post-surgery, defects were filled with a thin, loose connective tissue with minimal new bone formation from CON group, while the quantity of the newly formed bone was greater than that observed at the same time from group CPC, SCPC and BSCPC. Compared with CON group, the defect sites were filled with much new bone formation and a greater number of defected zone disappear from group CPC, and more new bone formation and less residual biomaterials in defected area from group BSCPC and SCPC. Compared with treatment by CPC or SCPC, defect sites exhibited more bone formation from the defect margin to the center and the specimens showed more advanced stages of remodeling and consolidation from group BSCPC (Figure 3).

Van Gieson staining revealed new bone matrix deposition within defects in the above mentioned groups (a: group CON, b: group CPC, c: group SCPC and d: group BSCPC. Red arrow: new bone, the collagen fibers of bone tissue were dyed bright red. Yellow arrow: biomaterials, bar = 200 mm).
The percentage of remaining biomaterials and bone fill in the defects
The quantitative results were shown as the percentage of remaining biomaterials and bone fill in the defects (Figure 4(a) and (b)). At eight weeks, compared with group CPC, BMP-2 and Sr decreased the percentage of remaining biomaterials from groups SCPC and BSCPC by 1.18- and 2.74-fold, respectively (P < 0.05); for analysis of the percentage of bone fill in the defects, the percentages of bone fill from groups CPC, SCPC and BSCPC were significantly increasing by 1.83-, 2.75- and 4.64-fold at eight weeks (P < 0.05), respectively, as compared with group CON.
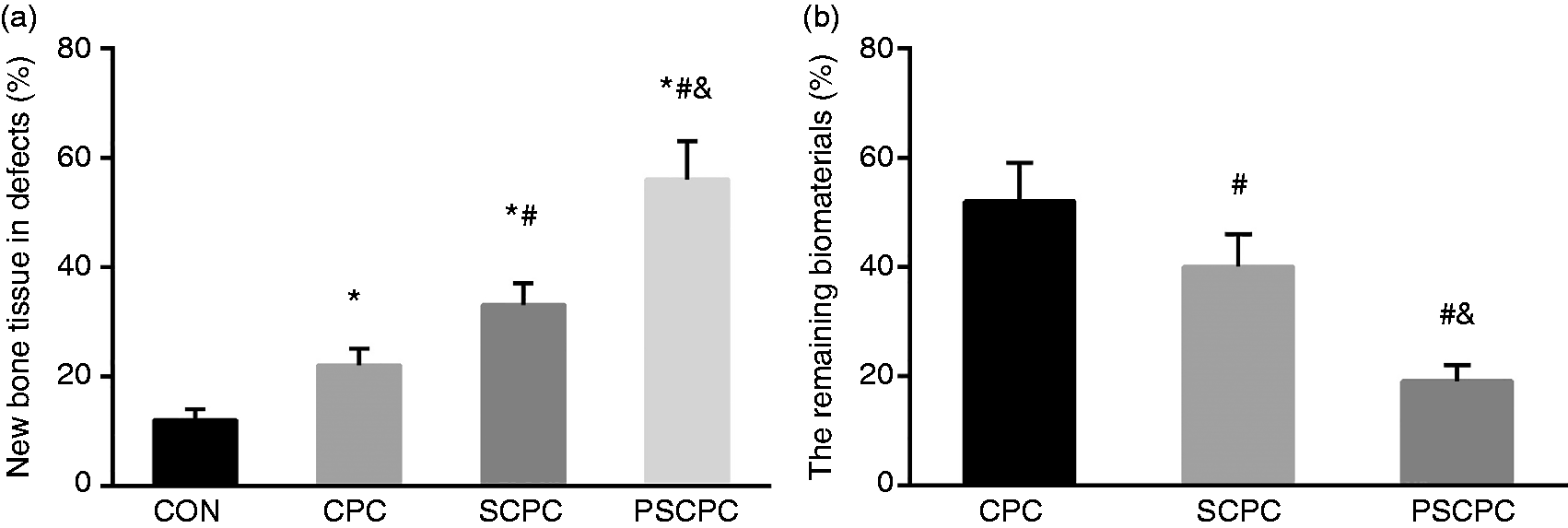
(a) Result of bone fill in the defects by Van Gieson examination. (b) Result of the remaining percentage of biomaterials by Van Gieson examination. Data were expressed as mean ± SD; error bars in the figure are presented as SD, N = 5 specimens/group. *P< 0.05 versus CON group, #P < 0.05 versus CPC group, &P < 0.05 versus SCPC group (by one-way ANOVA and Tukey’s post hoc test).
Biomechanical test
Results of biomechanical test of femoral condyles were expressed as ultimate load (Figure 5). After treatment for eight weeks, the strongest effects on strength of femoral condyles were observed in the BSCPC group. After treatment with BMP-2 and SCPC composite for eight weeks, the ultimate load of CPC, SCPC and BSCPC groups was significantly increased by 2.55-, 3.25- and 3.72-fold, respectively, as compared with group CON and significant was observed among four groups (P < 0.05).
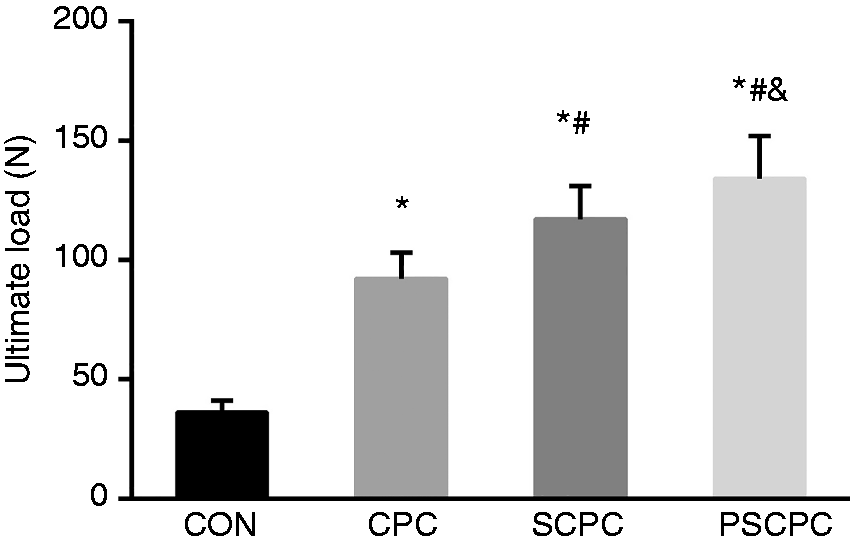
Biomechanical results expressed as ultimate load force. Data were expressed as mean ± SD; error bars in the figure are presented as SD, N = 5 specimens/group. *P < 0.05 versus CON group, #P <0.05 versus CPC group, &P <0.05 versus SCPC group (by one-way ANOVA and Tukey’s post hoc test).
Discussion
In general, during the bone repair, there should be enough quantity and good quality osteoinductive to complete the reconstruction of bone structure for long-term success. However, the number of patients with osteoporotic bone defects that are not suitable for autologous bone graft has increased due to the growing number of elderly people in the population and the need for re-surgery. Thus, the present study was conducted to improve bone formation at a site that has bone defect or insufficient bone quality, and to evaluate bone defect healing using single-dose local administration of BMP-2, and a mixture of Sr and CPC microsphere, which has well-established osteoconductivity and binds well with Sr.
The characteristics of skeletal physiology in the OVX rat are similar with those of early post-menopausal women, including increase rate of bone turnover and greater loss of cancellous than cortical bone. 27 Therefore, the OVX rat model was widely used for study postmenopausal osteoporosis. An excellent methodology uses already confirmed surgical creation of critical defects as the assessment tests on bone regeneration. A critical-sized bone defect is defined as an intraosseous wound that will not spontaneously heal completely without intervention, 28 the diameter of 3 mm considered as critical in animal model of OVX rat, 29 including already confirmed previous studies by our group.19,30
The operative management of critical-size bone defects in humans is an outstanding problem in contemporary orthopedics and trauma surgery. To date, autologous bone graft is the gold standard to treat such injuries but this method is greatly restricted by important morbidities related to the bone graft collection procedure 31 and there is a crucial need for developing new bone substitutes. Organic and synthetic acting as bone substitutes has been the focus of investigation of many research groups, considering CPC as a relevant material group. CPC stand out from other scaffold materials due to their compressive strength, excellent biocompatibility and osteoconductivity and, depending on their composition, resorbability. However, despite the above advantages, the lack of osteoinductivity is one of the critical drawbacks of CPC, which might result in bone nonunion, especially in the reconstruction of large defect in the state of osteoporosis. As the most representative bone growth factor, BMP-2 has been approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMEA) for the treatment of spinal fusion and tibial fractures combined with a matrix like collagen or decalcified bone. 32 Among the trace elements within bone mineral, strontium is of particular interest due to its reported osteogenic and antiresorptive effects. 33 To date, various Sr-doped CPCs have been developed for treating osteoporotic bone fractures. 34 Incorporation with bioactive growth factors and metal elements might be an efficient strategy endowing the osteoinductive activity.
In the present work, we endeavored to develop a sound CPC bone substitute system by incorporating Sr-ions and BMP-2 into CPC to enhance bone tissue growth. To develop a series of SCPC, strontium carbonate (SrCO3) particles were homogeneously mixed with CPC powders at different contents (0 and 5 wt.%). 35 At the same time, BMP-2 has a short half-life and always appears bolus release at a very early period which may impair the bone regeneration. 32 Higher doses of BMP-2 can achieve better results, but significantly increased the incidence of adverse reactions such as retrograde ejaculation, antibodies formation, postoperative radiculitis, postoperative nerve root injury, ectopic bone formation, hematoma formation, wound healing complications and risk of new onset of tumors. 36 In the present study, we observed significant improvements in osteoporotic femora defect following combination therapy with a lower single-dose local administration of BMP-2 and SCPC. In adjunctive therapy with SCPC, BMP-2 enhanced the effects of SCPC by increasing bone mass, bone strength and bone formation at the defect region. Compared with CPC and SCPC group, there was abundant formation of new trabecular bone as well as higher BV/TV, Tb-N, and Tb-Th and lower Tb-Sp in the treatment of bone defects after treatment by BSCPC. Large amounts of bone formation or bone fill were observed in animals receiving the BSCPC at eight weeks, significantly higher than that in sites exposed to CPC and SCPC, suggesting that BSCPC actually may enhance bone formation. Why did the single-dose local administration of BMP-2 treatment combination therapy with SCPC show a stronger effect on bone formation in defected area? Specific mechanism not yet known, it is mainly owing to the increase of local bone formation by BMP-2 local function and the sustained Sr release from SCPC, as well as rapid degradation of CPC.
In summary, our findings regarding the effect on new bone formation in the critical-sized osseous defects indicate that using a lower single-dose local administration of BMP-2 together with strontium-modified CPCs composite would be promising as a method of achieving rapid and bone regeneration of osseous defects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant from the natural science foundation for education department of Anhui Province (Grant no. KJ2017A266).