
Abstract
Preterm premature rupture of fetal membranes is a leading cause of preterm delivery. Preterm labour can compromise fetal survival, and even if a pregnancy affected by preterm premature rupture of fetal membrane continues, major complications associated with leakage of amniotic fluid and risk of infection can affect the normal development and survival of the baby. There are limited management options for preterm premature rupture of fetal membrane other than delivery of the baby if ascending infection (chorioamnionitis) is suspected. We have previously reported the development and characterisation of an implantable membrane with the aim of using it to occlude the internal os of the cervix, in order to prevent amniotic fluid loss, allow fluid reaccumulation and reduce the risk of chorioamnionitis. For this, an electrospun biocompatible and distensible bilayer membrane was designed with mechanical properties similar to the human amniotic membrane. In this study, we consider the effects of sterilization on the membrane, how to insert the membrane and visualise it using routine clinical methods. To do this, we used e-beam sterilisation and examined the ability of the membrane to adhere to ex vivo human cervical tissues. We also studied its insertion into a custom-synthesised model of a 20-week pregnant uterus and imaged the membrane using ultrasound.
Sterilisation produced minor effects on physical and mechanical properties, but these did not affect the capacity of the membrane to be sutured or to provide a fluid barrier. We demonstrated that fibrin glue can successfully adhere the bilayer membrane to cervical tissues. Finally, we demonstrated that the membrane can be inserted through the cervix as well as visualized in place using ultrasound imaging and an endoscope.
In summary, we suggest this membrane is a candidate for further development in an appropriate animal model, supported by appropriate imaging, to precede possible future human studies if judged to demonstrate satisfactory safety and efficacy profiles.
Keywords
Introduction
Preterm premature rupture of fetal membranes (PPROM) is a leading cause of preterm delivery, contributing up to 30% of cases. 1 About 40% of cases of fetal membrane rupture proceed to spontaneous labour within a week. 1 Even when a pregnancy complicated by PPROM continues beyond 24 weeks, substantial fetal morbidity (including pulmonary hypoplasia, ascending fetal infection and prematurity) complicates up to 20% of cases. 2
Currently, there are no effective therapies for PPROM. The insertion of an ‘amniopatch’ (concentrated platelet infusion) to seal off amniotic membrane leaks especially following fetoscopic procedures, 3 and amniotic fluid instillation 4 has been investigated. However, this approach has been largely unsuccessful and has not been associated with improved pregnancy outcomes. Given the lack of effective technologies, we sought to develop new approaches to the treatment of PPROM by achieving a seal of the internal cervical os, which will facilitate the continuation of the pregnancy towards term. To achieve this, we developed a bilayer electrospun membrane that combines two polymers approved by the US Food and Drug Administration (FDA); Poly-L-lactic acid (PLA) microfibres to encourage cell ingrowth in vivo, and compact polyurethane nanofibres, which contribute elasticity and offer a partial barrier to fluid penetration. The combination of these two polymers creates a fluid-resisting distensible barrier. Our in vitro assessments of this membrane demonstrated that it has mechanical properties close to the native amniotic membrane, that it is a barrier to fluid entry, and that it can withstand distension. 5
This bilayer membrane was designed to be inserted through the cervix. The aim of this study was to examine some of the practicalities of how to insert the membrane, suture it or adhere it to patient's tissues and visualise it post insertion. We also addressed the issue of how to sterilise the membranes without significantly affecting their functional properties.
Sterilization is required before any devices can be clinically employed. Determination of sterilization approaches is crucial for the routine production of any device under good manufacturing practice (GMP) conditions. We therefore assessed the physical and mechanical properties of the membrane before and after e-beam sterilization. We tested the ability of the membrane to be sutured and we used fibrin glue to adhere the membrane to ex vivo human cervical tissues. To assess the feasibility of inserting this membrane, we commissioned a realistic model of a synthetic uterus of a 20-week pregnant woman working with the company SynDaver. Furthermore, we developed methods for the trans-cervical insertion of the membrane and were able to assess its correct location using conventional ultrasound imaging.
Material and methods
Polymers and electrospinning
PLA (Goodfellow, Cambridge, UK) was dissolved in dichloromethane (DCM) at 10% (wt/v). Polyurethane (Z3; Biomer technologies, Cheshire, UK) was dissolved in 70:30 dimethylformamide:tetrahydrofuran (DMF:THF) at 10% (wt/v).
The bilayer membranes were produced as previously described. 5 Briefly, the polymer solution was loaded into four syringes (5 mL each; 20 mL in total for each polymer), fitted with blunt tipped 21G needles and placed in a syringe pump (GenieTM_Plus, Kent Scientific, USA) on either side of a rotating mandrel. Z3 was delivered at 40 µl/min per syringe with an accelerating voltage of 20 kV DC from a high voltage supply (Genvolt, UK) and collected on an aluminium foil-covered earthed mandrel (80 mm diameter, 160 mm length) rotating at 300 rpm/min, with a needle to collector distance of 17 cm at 21°C and ∼30% humidity. After 17.6 mL of Z3 solution was electrospun (1 h and 50 min), electrospinning of the PLA solution from the opposite end of the mandrel was commenced using the same conditions as for Z3. Both solutions (2.4 mL each) were electrospun simultaneously for 15 min to create a region of interwoven Z3 and PLA fibres. Then 17.6 mL of PLA solution was electrospun in isolation (1 h and 50 min) to produce the bilayer membrane.
E-beam sterilization
E-beam sterilization was performed by Steris (Daventry Site, UK) using a dose range of 25–35 kGy.
Physical and mechanical properties
Physical and mechanical properties of the bilayer membrane were assessed before and after sterilization, as previously described. 5 Briefly, samples were cut and mounted on 12.5 mm stubs. The samples were gold sputter coated to a depth of 25 nm (Gold coater; Edwards sputter coater S150B, Crawley, England), and then examined using a scanning electron microscope (SEM) (Philips/FEI XL-20 SEM; Cambridge, UK) at an accelerating voltage of between 10 and 15 kV and a SPOT size between 2 and 3.A.
Mechanical properties were measured using a uniaxial tensile test. Samples were cut, areas measured (thickness × width), and were then clamped between two grips in a tensiometer (BOSE Electroforce test instruments, MN, USA) using a grip distance of 88 mm and a 45 N load cell (BOSE Electroforce test instruments, MN, USA). Preconditioning of the samples was performed as previously described by using a ramp test to elongate the material at a rate of 1 mm/s up to 25% of displacement of its original length for five cycles. 6 Then a ramp test was applied at a rate of 0.1 mm/s with a maximum displacement of 7 mm. Stress was normalized by the area and the strain by the length of the samples (distance between grips). The first failure point or plateau was recorded as the load at failure (or ultimate tensile strength (UTS)) and the slope of this plot was calculated as the Young’s modulus, both shown as N/mm2. These values were compared to those for human fetal membranes obtained from the literature using the same protocol. 6
A suture retention test was performed using the BOSE tensiometer. Materials were cut to a length of 10 mm and a width of 5 mm. A stainless steel wire of 0.22 mm diameter (50 g, Scientific Wire Company, Essex, UK) was passed through a point 0.25 cm away from the top edge of the centre of the sample. Samples were then clamped from the bottom 0.5 cm away from the edge, and the suture was clamped using the top grid with a gap between the two grids of 0.75 cm. A ramp test of 0.11 mm/s was run. Data were plotted as N/mm2, showing the maximum strength achieved before the suture pulled through the bilayer membrane and the Young’s modulus to indicate material stiffness.
Resistance to fluid penetration
A column of water was used to test resistance to fluid penetration. A U-shaped column of water was formed using Tygon® tubing. Both sterilized and non-sterilized samples of 20 mm × 20 mm were fixed in this tube using a P3D chamber with a 10 mm diameter hole (EBERS Medical Technology SL, Zaragoza, Spain). A 50-mL Plastipak syringe was placed at the other side of the tube to provide the water column. Distilled water was added to the system with this syringe and the P3D chamber initially held level. The syringe was then raised to 160 mm in height to apply a pressure (1569.06 Pa), which is equivalent to the intrauterine baseline pressure at full-term pregnancy obtained from the literature 7 and the time taken for water to pass through the bilayer membrane was measured.
Adhesion of the membrane to ex vivo cervical tissue
Fibrin glue was made by mixing fibrinogen (Sigma-Aldrich, Dorset, UK) with thrombin (Sigma-Aldrich, Dorset, UK). Three different concentrations were made and 1:1 mixtures were used to make fibrin glue: 25 mg/mL and 25 U/mL, 50 mg/mL and 50 U/mL, and 100 mg/mL and 100 U/mL for fibrinogen and thrombin, respectively. Initially, the optimum concentration of fibrin required to adhere the membrane to another piece of membrane was determined. This was accomplished using 40 µL of the fibrinogen/thrombin mixtures. Fibrin glue was placed between two pieces of the bilayer membrane between the PLA and a PU Z3 surface by applying manually pressure for 5 to 10 s. Then fibrin glue was allowed 5 min to form a clot. Then, employing the highest concentration of fibrin glue (100 mg/mL of fibrinogen and 100 U/mL of thrombin, 1:1), the same procedure was used to glue a PLA surface of a membrane to a sample of cervical tissue obtained under Ethical Approval from the South Yorkshire Research Ethics Committee 08/H1310/35. The membrane was clamped to the upper grid of the tensiometer, while the adhered membrane/cervix was clamped to the lower grid. A ramp test was then performed at a rate of 0.11 mm/s. Data were plotted as N/mm and standardised for width, which demonstrates the Young’s modulus and the maximum strength achieved before the two membranes were pulled apart.
Introduction of the membrane into a synthetic cervix
A SynDaver (8506 Benjamin Road, Suite C, Tampa, FL 33634) pregnant uterus was used to test the introduction of a sterilized 50 mm × 50 mm membrane. This custom-made model was made to represent the pelvis of a woman lying down, with a 20-week pregnancy including an external perineum, vaginal introitus, and the internal vaginal canal which connects through the cervical canal with a uterus. The pregnant uterus has a cavity with a phantom of a foetus inside the amniotic sac.
First, we explored introducing a 16Ch flexible cystoscope (Olympus, Southend-on-Sea, UK) to record the procedure from the inside of the uterus while introducing the catheter with the membrane into the vagina. A puncture was made in the synthetic model directly into the uterus which was used to introduce the cystoscope. A 16 G soft latex Foley catheter (Teleflex®, Morrisville, NC) was used to deliver the membrane into the cervix by wrapping the bilayer membrane around the catheter balloon. The catheter was then inserted into the cervix and inflated inside the uterus using 10 mL of water.
A 60 × 40 mm membrane was also inserted as an alternative insertion technique using a flexible polypropylene (Pipelle) cannula with an outer diameter of 3.11 mm (Pipelle®) that had lines to measure how far the membrane was introduced. The membrane was introduced to a distance of 30 mm and then the Pipelle cannula was removed, leaving the membrane in this position.
This procedure was visualised in real-time using an obstetric ultrasound device machine (Voluson™ E8) which is routinely used at the Feto-Maternal Unit at Jessop Wing, Sheffield NHS Teaching Hospital. Images were obtained and recorded using a 2–5 MHz wideband curved linear array transducer (C1–5-D).
Statistics
All experiments were performed in triplicate. Differences were tested statistically against a null hypothesis of no difference between samples using a two sample T test with equal variance not assumed. Significance was taken as p < 0.05.
Results
A well-established e-beam sterilisation technique was conducted at Steris UK (Daventry Site) to sterilize the bilayer membrane and then the effects of sterilisation on physical and mechanical properties were assessed. SEM images showed that sterilisation increased the presence of pores on the surface of the PLA fibres, while polyurethane (Z3) fibres were unaffected (Figure 1).
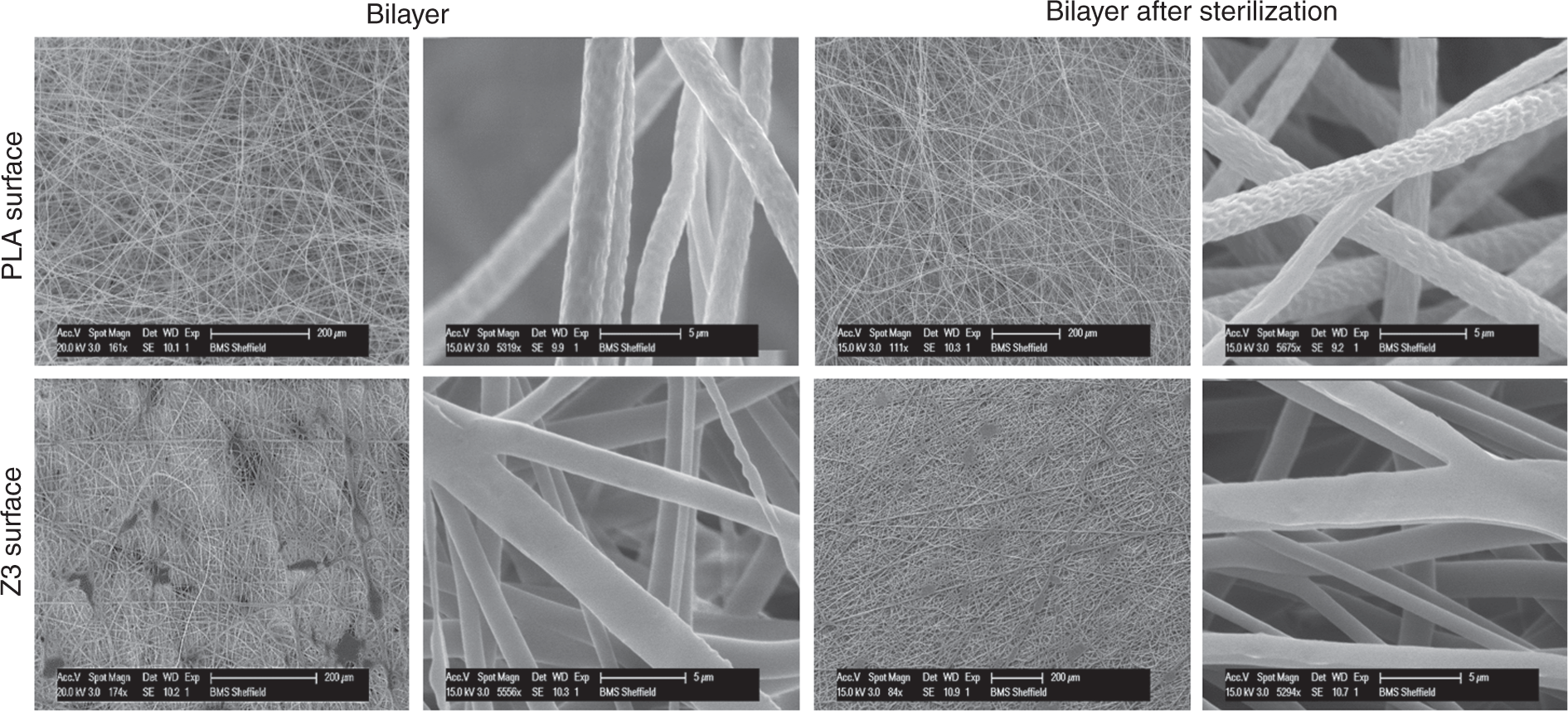
Physical characterization of the bilayer membrane before and after sterilization using SEM images. The SEM images are representing the both surfaces of the bilayer membrane before and after sterilization, and at low and high magnifications.
Samples had a similar Young’s modulus after sterilization with the same significant decrease of the Young’s modulus from the first to the second cycle (Figure 2). Also, a similar plastic deformation was found for both membranes (Figure 2). The tensile test showed a significant increase of the UTS of the sterilized material (Figure 3); however, both membranes had values for UTS and Young’s modulus above or within the range for human fetal membranes obtained from the literature. 6 The Young’s modulus was significantly reduced when using the suture retention test, while UTS was not affected by sterilisation (Figure 3).
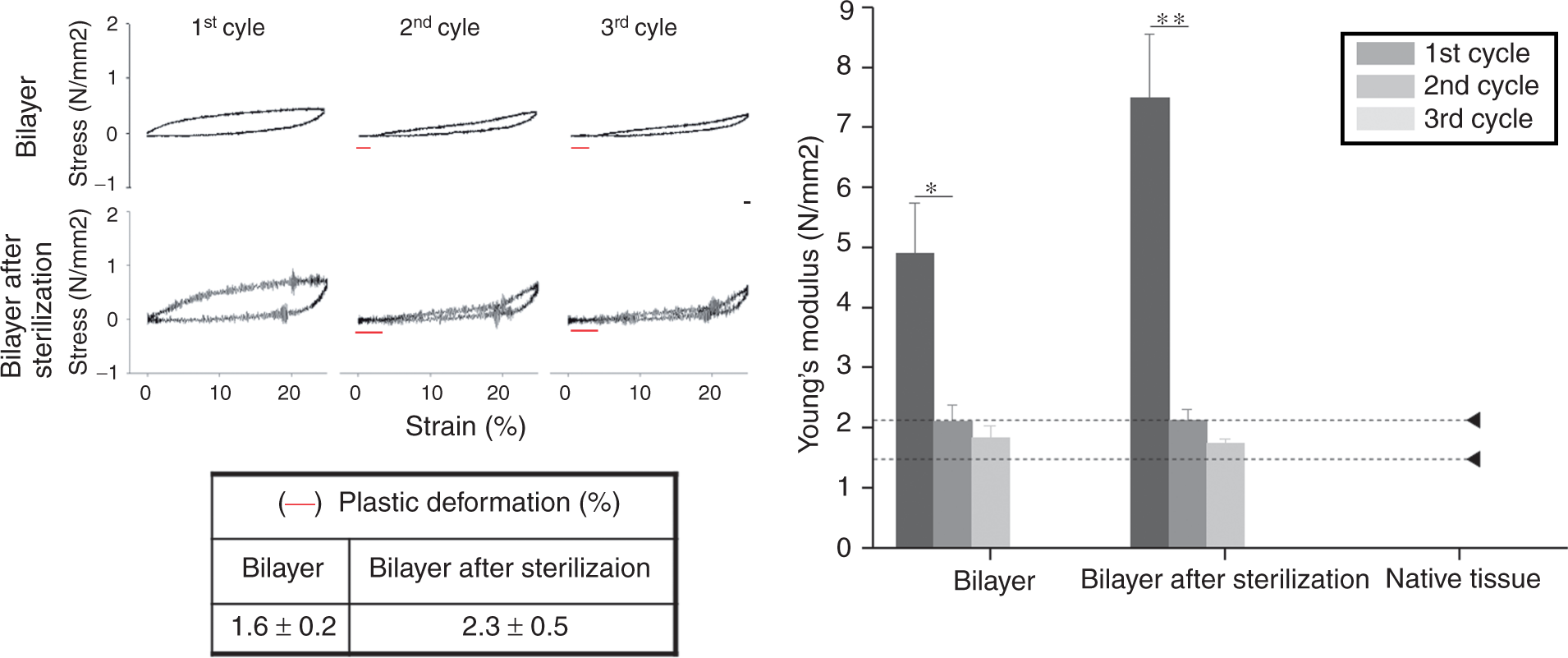
Ability of the membrane to withstand repetitive stress during a cyclic tensile test (n = 3, *p < 0.05, **p < 0.001).
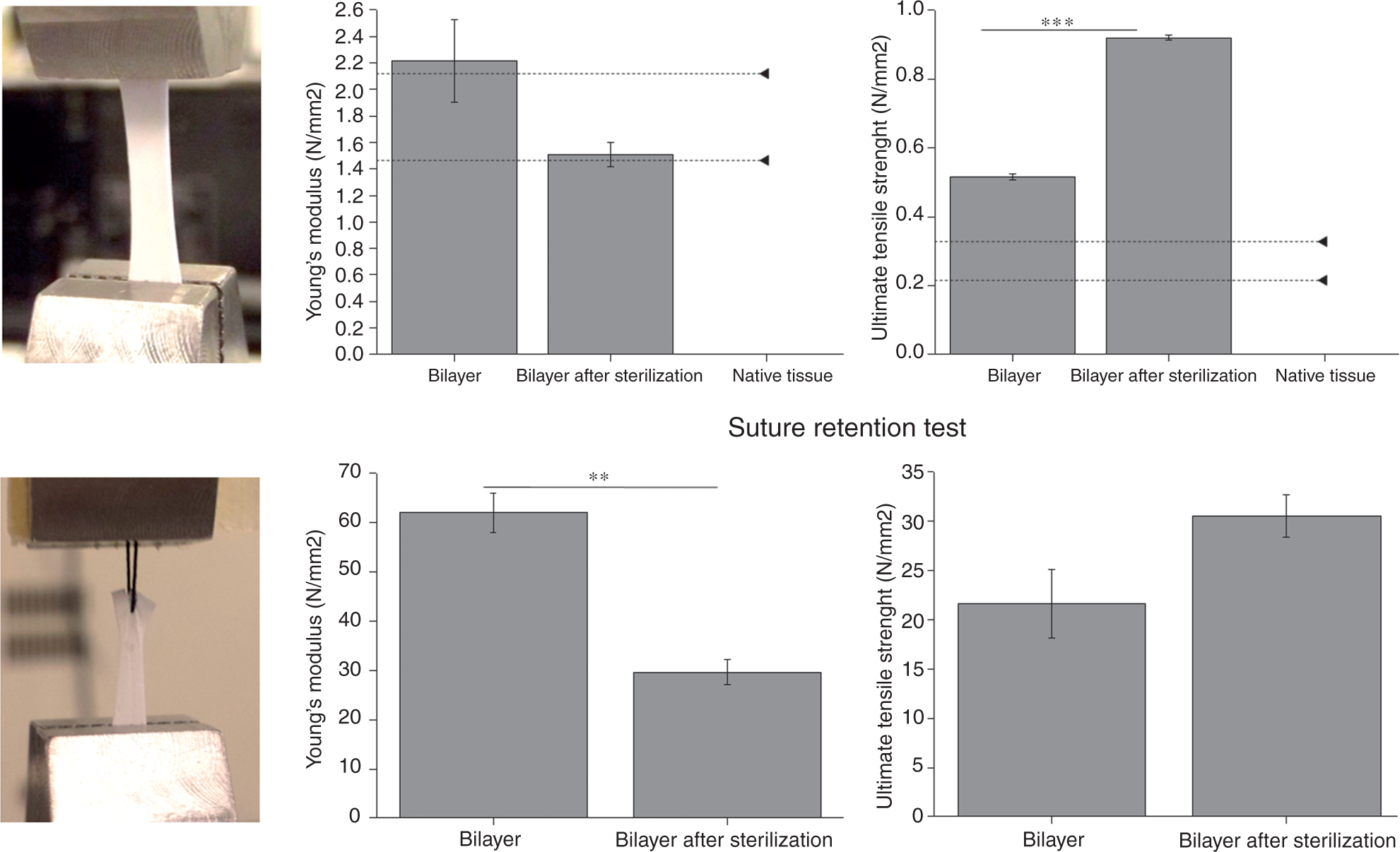
Tensile test and suture retention test of the bilayer before and after sterilization (n = 3, **p < 0.001, ***p < 0.0001).
The ability of the bilayer membrane to act as a fluid barrier when applying intrauterine pressures experienced at full-term pregnancy showed some reduction in properties post sterilisation, with some samples withstanding the column of water overnight and other samples for only up to 6 h (Figure 4). All non-sterilized samples withstood the column of water overnight.
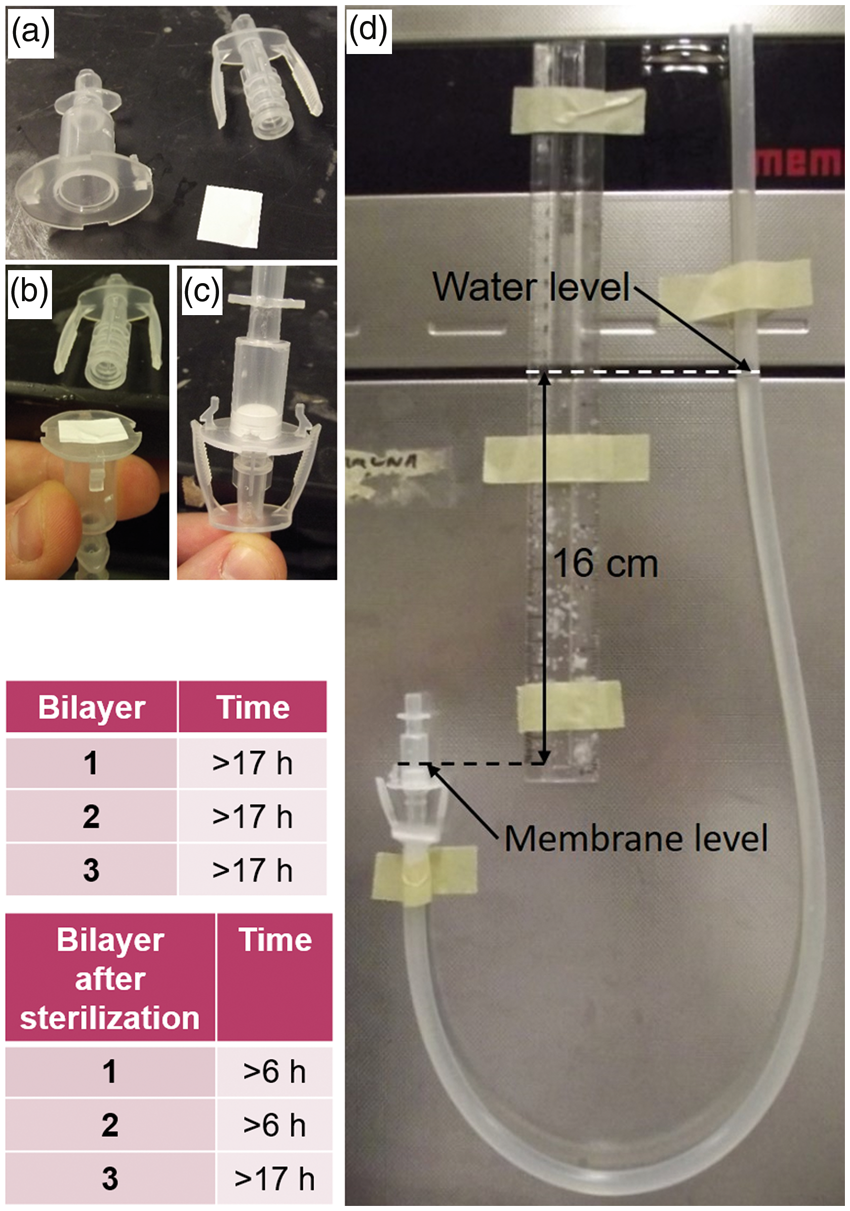
Fluid retention test. Bilayer samples were fixed using a P3D chamber (a, b and c). A U-shaped column of water was formed using Tygon® tubing (d). The table shows the time measured for water to go thought the sample.
Then the ability of the bilayer membrane to be glued to the cervix was assessed, firstly by determining the optimal fibrin glue concentration to glue the membrane to itself. The highest concentration of fibrin glue employed was significantly better for gluing the membranes together in terms of both UTS and Young’s modulus. We then used this concentration of fibrin glue to explore gluing the membrane to human cervical tissue. Lower concentrations were ineffective in gluing the membrane to the cervical tissue (Figure 5).
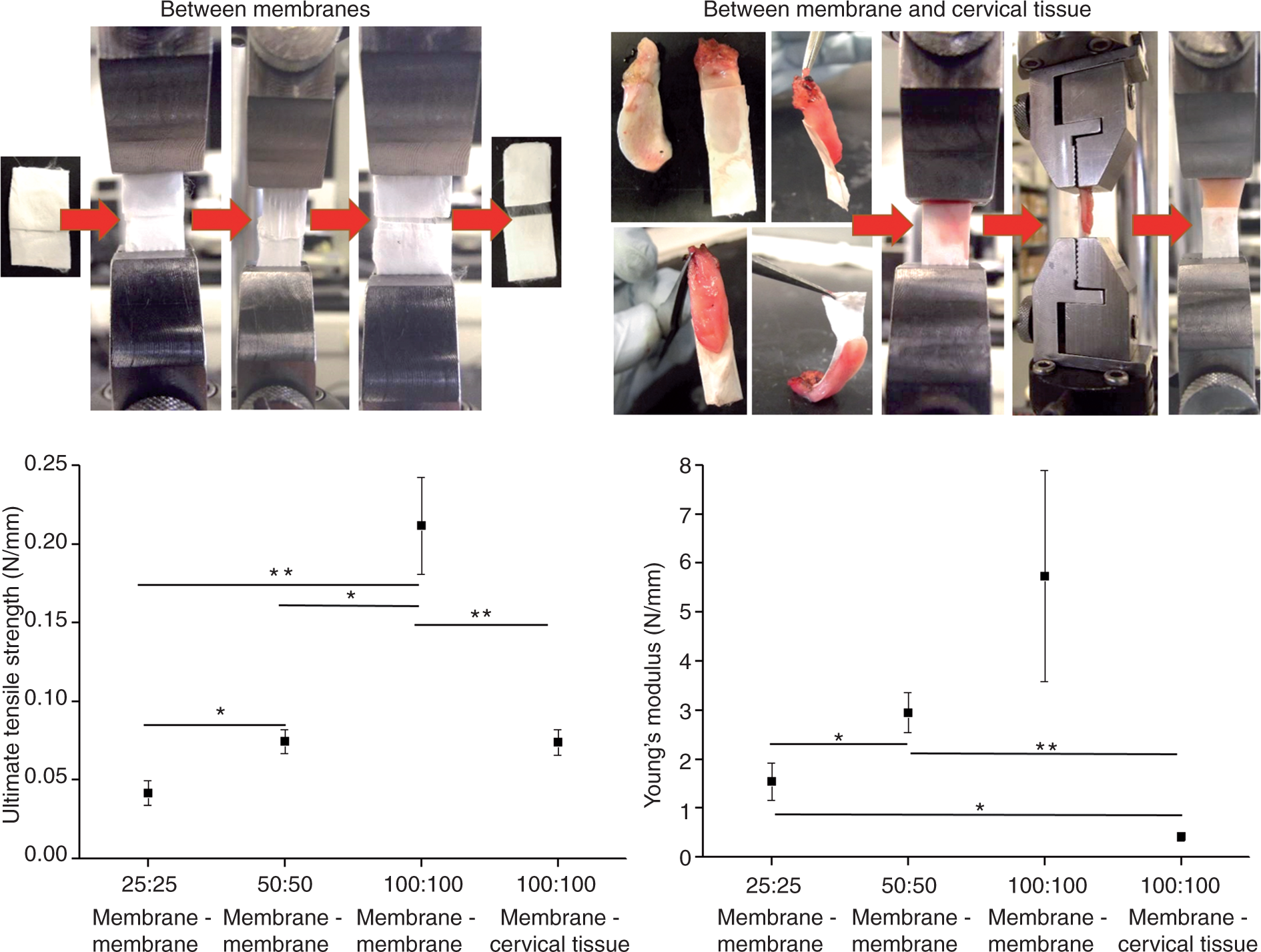
Tear strength test. Forces applied to pull apart membrane-membrane or membrane-cervical tissue glued with different concentrations of fibrin glue (25:25 is 25 mg/mL and 25 U/mL, 50:50 is 50 mg/mL and 50 U/mL, and 100:100 is 100 mg/mL and 100 U/mL of fibrinogen and thrombin, respectively).
Finally, using a SynDaver synthetic uterus (as shown in Figure 6), the membrane was inserted into the synthetic cervix. After exploring the synthetic model with the cystoscope (Figure 7, top row), the introduction of the catheter (Figure 7 middle row), or the catheter with the membrane (Figure 7 bottom row) was recorded from the inside of this model. The membrane was inserted through the cervical canal to the entrance to the cavity of the uterus and the balloon was inflated.
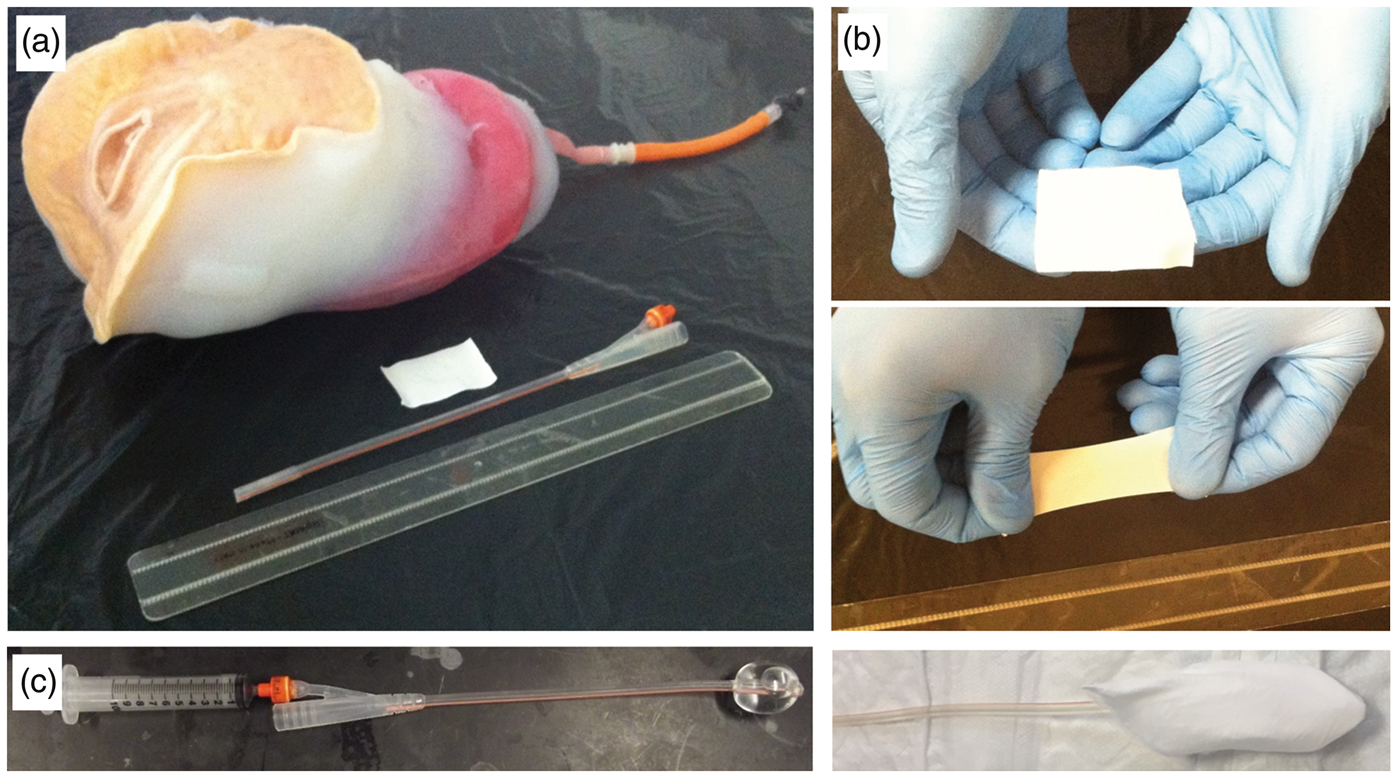
Illustration of the SynDaver pregnant uterus model representing the pelvis of a woman lying down, together with the bilayer membrane to be inserted and the catheter balloon (a). Ease of handling of the bilayer membrane stretched by hand before being inserted into the synthetic model (b). Soft latex Foley catheter balloon with and without the bilayer membrane wrapped around (c).
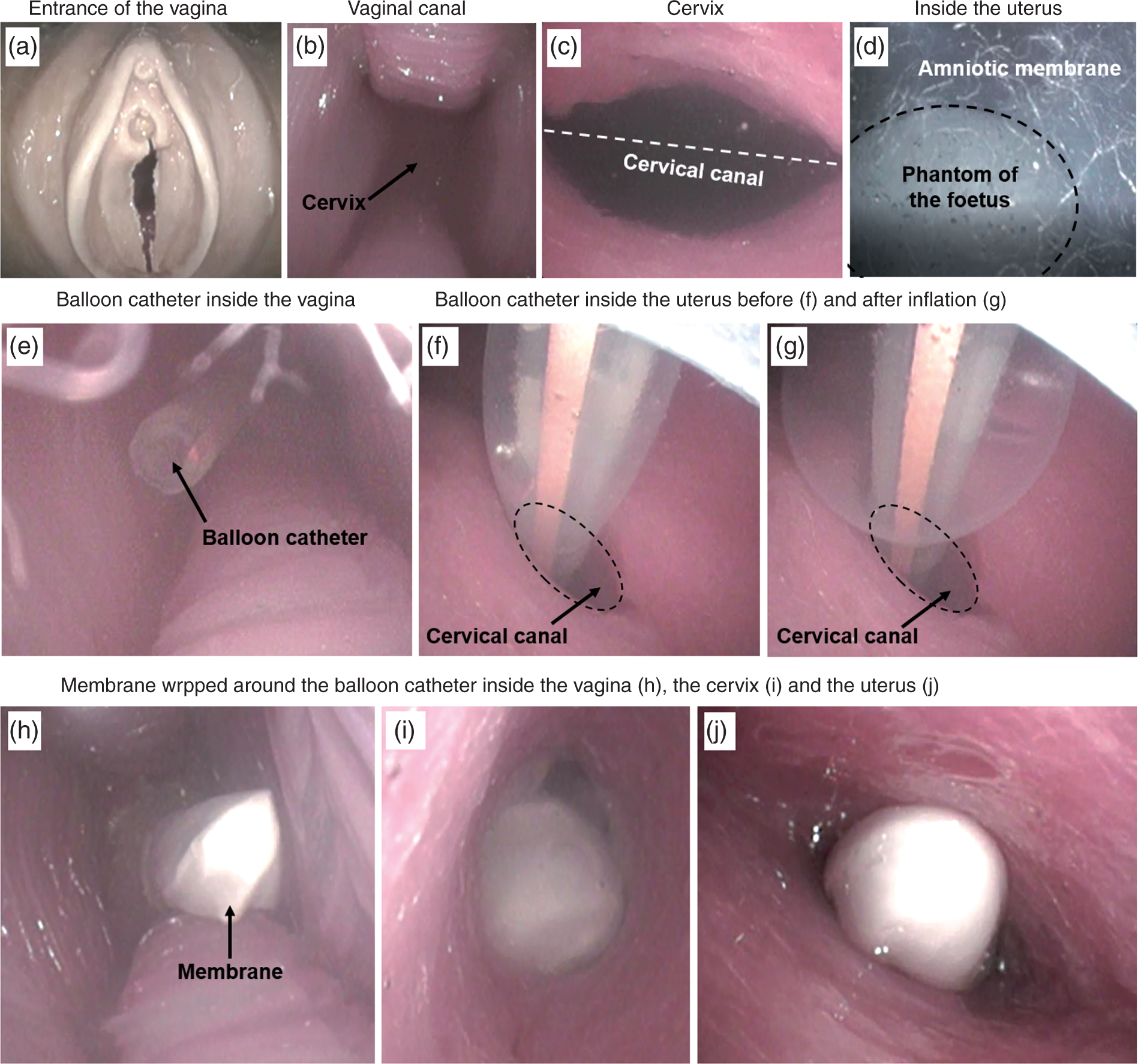
First row illustrates the exploration of the synthetic model using cystoscopy from the outside (a) through the vaginal canal (b) and cervix (c) and then inside the uterus viewing the phantom of the foetus inside the amniotic membrane (d). Second row illustrates the balloon catheter introduced through the vagina (e) and cervix inside the uterus (f) where it is inflated (g). Third row illustrates the membrane wrapped around the catheter and introduced through the vagina (h) and cervix (i) inside the uterus (j).
Similarly, using the Pipelle cannula and assisted by ultrasound imaging, the membrane was introduced for about 30 mm into the cervical canal, with the catheter tip just beyond the entrance to the cavity of the uterus. Then the Pipelle cannula was removed leaving the membrane in this position.
The correct location of the membrane was confirmed by ultrasonography employing an external ultrasound probe placed on the anterior surface of the synthetic uterus (Figure 8).
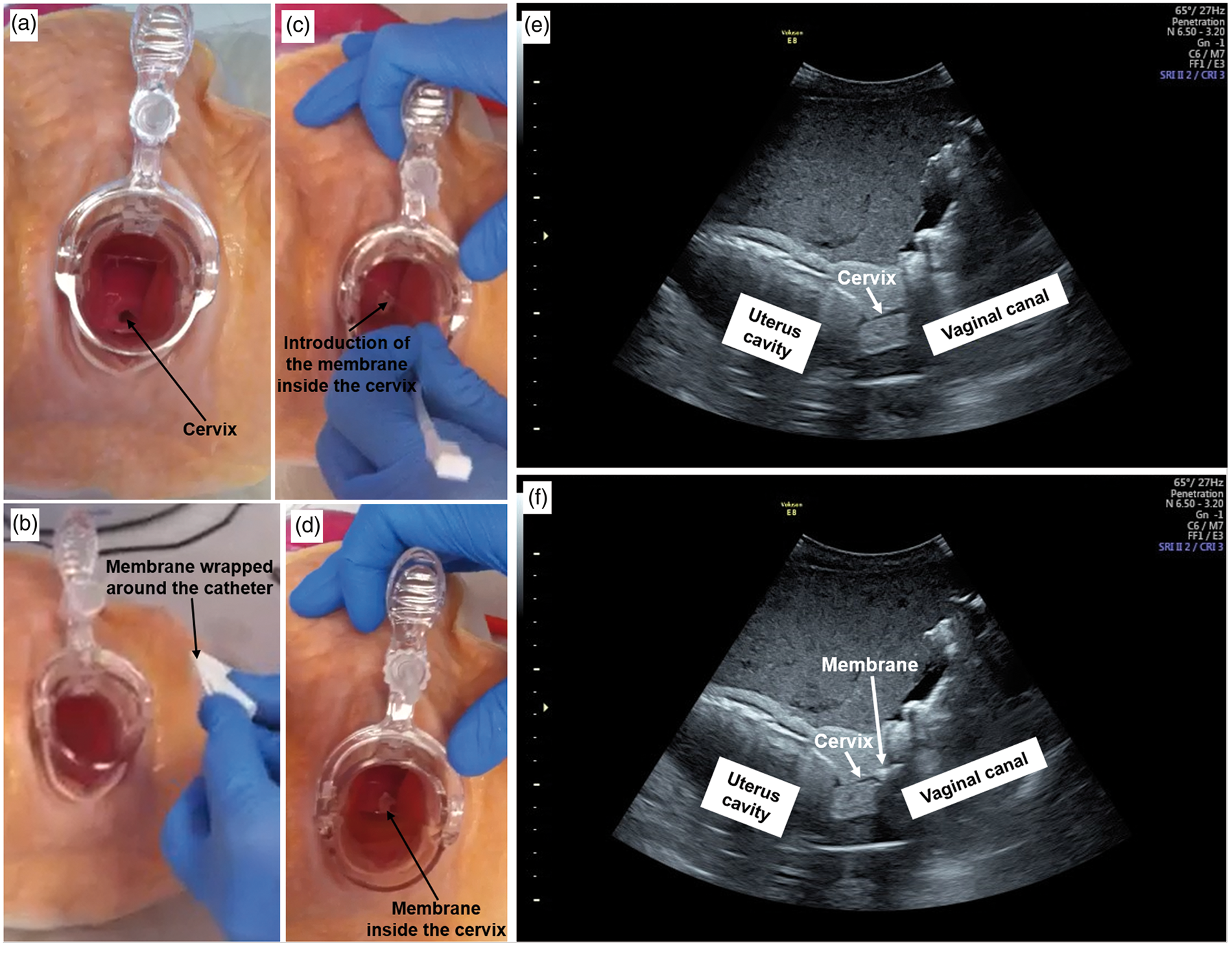
On the left hand side, image sequence illustrates the synthetic model with views of the cervix through the vaginal canal using a speculum (a), and then the membrane is wrapped around the Pipelle cannula (b) and introduced into the cervix (c). Finally, the membrane is left inside the cervix after removal of the cannula (d). On the right hand side, ultrasound images of the synthetic model are used to identify the different anatomical structures (e) and to show introduction of the membrane into the cervical canal using the Pipelle cannula (f).
Discussion
With more than 10 million premature births annually globally and PPROM occurring in up to 25% of them, 8 there is a need for new interventions to reduce spontaneous preterm birth caused by PPROM, especially between 14 and 22 weeks’ gestation when current therapeutic approaches are ineffective. 9
Our proposed approach involves using existing FDA-approved materials with good favourable safety profiles to make a barrier membrane to temporarily occlude the leak from the cervix, thereby assisting amniotic fluid to be retained in the uterus so that the pregnancy can continue towards term. If successfully deployed in vivo, using this distensible membrane barrier to seal the utero-cervical opening may minimise amniotic fluid loss as well as reduce the risk of ascending uterine infections. Spontaneous PPROM at these early gestations is associated with poor rates for pregnancy prolongation and fetal survival without treatment. Also, many babies born alive die soon after or suffer chronic lung dysfunction from pulmonary hypoplasia, mandating the development of solutions that improve the chance of pregnancy prolongation, amniotic fluid accumulation and perinatal survival.
The aim of this study was to progress the development of this membrane towards clinical use by first assessing the impact of sterilisation on it and secondly to explore the feasibility of introducing the membrane into the uterus using a practical custom-designed model of a 20-week pregnant uterus.
Sterilization is required for the routine production of any device under GMP conditions that is intended for clinical use, and we selected e-beam sterilisation as the most appropriate for these polymers. It is important to always quantify the effect of the sterilization on the performance of any device. Irradiation may enhance polymer degradation 10 ; however, the morphological appearance of the membranes did not change significantly as there was a similar fibre distribution and pore size (data not shown). There was evidence of some pitting of the surface of the PLA fibres post e-beam sterilisation. On the other hand, it has been shown previously that e-beam irradiation has a crosslinking effect on polyurethane materials, 11 and although that was not measured in this study, this may explain the slight increase in the UTS shown on tensile testing. However, the mechanical properties of the bilayer membrane were not significantly affected and remained above or within the range of values for human fetal membranes, 6 which can be interpreted as an indicator of a good mechanical performance when subjected to pressures experienced during pregnancy. The data suggest only a slight effect of sterilisation on the plastic deformation with fibres becoming slightly more brittle as observed with the Young’s modulus particularly in the suture retention test, although this did not affect the capacity of the membrane to retain sutures.
We designed this bilayer membrane to act as a fluid barrier to intrauterine pressures, ideally to cope with the effect of the pressure of placental growth and amniotic fluid on fetal membranes in vivo, and all membranes were able to support a column of fluid for at least 6 h and in some cases for 24 h. As sterilisation had some slight adverse effects on the ability of the membranes to withstand a column of fluid, this is an area where we can improve on the membranes possibly by adding a thicker layer of electrospun nanofibres of polyurethane. This further optimisation would be done during the GMP production of these materials prior to any animal testing as part of seeking approval for a first in woman safety study. To produce materials for clinical use, the membranes will need to be scaled up and manufactured under GMP conditions and their manufacture made reproducible. Similarly, although the sterilization was performed using a certified testing facility, the process was not validated with a bioburden test to determine the sterilization selection dose.
When it comes to introducing the membrane, we demonstrated that the membrane was capable of retaining sutures as one route for securing the membrane in place. We also showed that high concentrations of fibrin glue enabled the membrane to adhere to human cervical tissue. Given that the concentrations of fibrinogen and thrombin in commercial fibrin products used in the clinic are usually as high or higher than those we employed in this study, 12 this suggests that fibrin glue could be an alternative or additional means of securing the membrane in place. Prior work from the MacNeil laboratory has shown that fibrin can promote cell migration from human corneal explants. 13 Thus, we hypothesise that the use of fibrin glue may not only help to secure the membrane in place but may stimulate cell ingrowth from the uterine lining (the decidua). This warrants further study in an animal model. We have previously demonstrated the ability of cells to migrate and grow into PLA microfibrous electrospun fibres 5 and it is these fibres that would be in contact with human cervical tissues. In addition, while the mingling of the two different fibres (PLA and polyurethane) achieves the smallest porous size to prevent bacterial entry, uterine cells growing onto the PLA surface of the membrane could potentially achieve a better seal, thereby improving the resistance to fluid leakage as well as improving its barrier function against bacteria. Electrospun PLA fibres can withstand considerable distension and will only degrade very slowly to lactic acid and be eliminated by normal tissue metabolic processes of the human cells in contact with them. 5 These should therefore not affect the foetus. However, as with all devices intended for the clinic safety, studies will be required in animal experiments to look critically at issues of toxicity and where possible efficacy.
Finally, the feasibility of handling and introducing the bilayer membrane into the cervix was examined using a custom-made synthetic “pregnant” uterus manufactured by Syndaver Ltd. This company has developed a range of realistic synthetic organs and they are produced and validated against mechanical, physicochemical thermal and dielectric properties of living tissue and are compatible with imaging equipment such as MRI, CT, fluoroscopy and ultrasound.
For this project, we requested a customer synthesis of a 20 weeks’ pregnant uterus. We took into account that the average length of an adult cervix canal is about 30 mm 14 to conduct experiments inserting the membrane into the uterine cavity through the cervix. There are many benefits to using an in vitro synthetic human model at this stage – it allows one to investigate to what extent existing surgical catheters and probes and indeed imaging techniques – in this case ultrasound – can be used in the insertion and initial assessment of the location of the bilayer membrane into the uterus.
We compared the use of two catheters – a balloon catheter and a Pipelle cannula as alternative insertion methods since the latter was thinner and more rigid than the balloon catheter and it allowed us to introduce the membrane to an exact location more easily. It was also easier to remove leaving the membrane in place. We employed a membrane of sufficient size (60 × 40 mm) to ensure visualisation of the membrane in the cervical canal and also enable suturing to external cervical tissue, also facilitating removal before childbirth.
In summary, while the safety and efficacy of the membrane will need to be tested in an appropriate animal model, the work undertaken in this study has allowed us to identify practical approaches and challenges to handling and imaging this membrane. We could visualise the membrane in the desired anatomical position and confirm that the material can be scanned in simulated conditions; nevertheless, the final method for insertion will be determined during preclinical testing.
Sealing the rupture site of the amniotic membrane is technically very challenging; therefore, we suggest an approach where the membrane simply closes the neck of the womb by plugging it. Briefly, this will include applying fibrin glue to the synthetic membrane, catheter-facilitated introduction of the membrane via the transvaginal route through the cervical canal, deployment of the membrane by inflating the balloon at the tip of the catheter, as demonstrated in this study, and application of some pressure on the membrane against the inner uterine cavity lining to promote better adhesion/sealing. After deflating the balloon and its removal, we then envisage using a stitch to close the membrane-sealed cervix and minimise the leak. The suture will not be through the membrane but through the cervix, keeping the membrane in situ through the remainder of the pregnancy with a strip of it extruding through the cervical opening for ease of removal when the suture is removed.
The membrane has been designed to be distensible to cope with the pregnancy as it advances and we anticipate that the membrane would be removed before delivery which can be readily done by removal of non-absorbable sutures used to anchor the membrane to the ectocervix, deployed either as a number of interrupted sutures or as a purse-string suture around the cervix as used for cervical cerclage procedures. We anticipate substantial challenges to define the best approach to the insertion of the membrane into the human uterus through the cervix. Firstly, an aseptic approach that minimises the risk of introducing infection into the uterus has to be developed. Secondly, we will need to develop an insertion technique that minimises the risk of further trauma to the adjacent membrane following trans-cervical insertion. Thirdly, we will need to define optimum approaches to retaining the membrane within the uterus where it occludes the internal cervical os. A method of removal of the membrane at the end of pregnancy or following spontaneous labour onset will need to be developed. To define the optimum approaches to address these technical and clinical challenges, we anticipate undertaking experiments employing an appropriate animal model to demonstrate proof of clinical principle in the future.
In conclusion, this paper has advanced the development of a synthetic dispensable membrane for use in PPROM. To move towards the clinic, it will require evaluating in a suitable animal model. Challenges will be the safe introduction and suturing of the membrane in place together with the use of fibrin glue, but also assessing the risk of infection because of inserting a synthetic membrane or of indeed inducing premature labour by dilatation of the cervix which could cause local release of tissue hormones that promote labour.
Footnotes
Acknowledgements
We gratefully acknowledge the help of Dr Rob McKean of the Electrospinning Company for assisting with the e-beam sterilization of the material at Steris.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the Jessop Wing small Grant scheme from the Sheffield Teaching Hospitals.