
Abstract
Chronic wounds complicated by diabetes are a significant clinical issue, and their occurrence is expected to continue to rise due to an increased prevalence of diabetes mellitus, especially type 2 diabetes. Diabetic wounds frequently lead to nonhealing ulcers, and often eventually result in limb amputation due to the high risk of infection of the chronic wound. Here, we present a tissue-engineered treatment that combines a novel electrochemically deposited collagen wound matrix and human adipose-derived stem cells. The matrix fabrication process is optimized for voltage and time, and the final collagen biomaterial is thoroughly characterized. This collagen material possesses high tensile strength, high porosity, and excellent biocompatibility and cellular proliferation capabilities. Human adipose-derived stem cells were seeded onto the collagen wound matrix and this construct is investigated in a full thickness excisional wound in a mouse model of type 2 diabetes. This novel treatment is shown to stimulate excellent healing and tissue regeneration, resulting in increased granulation tissue formation, epidermal thickness, and overall higher quality tissue reformation. Both the collagen wound matrix alone and collagen wound matrix in combination with adipose derived stem cells appeared to be excellent treatments for diabetic skin wounds, and in the future can also be optimized to treat other injuries such as burns, blast injuries, surgical incisions, and other traumatic injuries.
Keywords
Introduction
Chronic wounds complicated by diabetes are a significant clinical issue, and their occurrence is expected to continue to rise due to an increased prevalence of diabetes mellitus. Diabetes affects approximately 10% of the US adult population, translating to over 30 million people, with 90–95% of these cases being type 2 diabetes. 1 By 2050, diabetes is forecasted to afflict 25% of the US adult population. 2 In addition to chronic kidney disease, cardiovascular disease, and increased risk of ischemic strokes, impaired wound healing is a significant cause of morbidity in diabetic patients, and it has been estimated that 25% of diabetic patients will develop a chronic wound (ulcer) during their lifetime. 3 These nonhealing wounds result from a combination of inadequate or inappropriate immune responses, peripheral neuropathy, poor arterial circulation, poor oxygenation to the wounds, and poor general systemic health due to the diabetic state. 4
Despite advances in modern medicine, nonhealing diabetic wounds still often result in amputation of the lower limb. These wounds account for up to 80% of nontraumatic lower limb amputations, and result in over 108,000 lower limb amputations in the United States annually.1,5 Current treatment options, such as topical delivery of growth factors and autologous or allogeneic skin grafts, are often not effective due to short enzymatic half-life in the wound, and poor integration of the treatment into the wound bed, respectively.
Cell-based regenerative medicine therapy is an attractive approach, especially using adipose-derived stem cells (ADSCs). Compared to other cell types, such as bone-marrow-derived stem cells, ADSCs are abundant, easy to harvest, and well-suited for tissue culture.6–9 ADSCs have also been shown to accelerate wound healing in chronic wounds by contributing to new vessel formation, re-epithelialization, and secretion of soluble factors crucial to the wound healing process.6,7,10–13 ADSCs delivered to wounds as sheets of cells, in solutions, and as cell aggregates resulted in increased tissue regeneration and healing in the diabetic wound.11,12,14,15
Tissue engineered treatments that combine cells with a biomaterial scaffold are a more advanced method for cellular wound treatments. The biomaterial scaffold provides a temporary extracellular matrix substitute than supports cell infiltration and proliferation as well as provides mechanical support while the natural ECM regenerates. The biomaterial gradually degrades as the natural tissue replaces it. Collagen, the main component of the skin ECM, has shown excellent capabilities for use as a material for skin tissue engineering. 16 It has been widely used as a cell carrier because of its excellent biocompatibility and biodegrability, and its low/no antigenicity. 16 In fact, collagen and ADSC combined constructs have been shown to result in superior healing over the delivery of ADSCs alone.17,18 However, many currently available collagen based scaffolds have poor mechanical properties and degrade too quickly in vitro for long-term cell culture. Instead of traditional gelated collagen as the scaffold, we use an electrochemical deposition method that produces skin-like, densely packed, robust collagen sheets.
Here, we present a novel electrochemically aligned collagen scaffold, termed “collagen wound matrix” (CWM) designed specifically for treatment of diabetic skin wounds that is formed via electrochemical deposition of collagen. The material is robust, porous, and an excellent substrate for cell seeding and culture. The CWM is combined with ADSCs to form a tissue engineered treatment that stimulates excellent natural tissue healing and regeneration in a full thickness excisional skin wound in a mouse model of type 2 diabetes.
Materials and methods
Materials
6 mg/mL highly purified bovine corium pepsin-soluble collagen, in 0.01M HCl (predominantly type I collagen, with approximately 5% Type III; Collagen Solutions, LLC, San Jose, CA) was dialyzed versus e-pure water at 5°C to facilitate removal of chloride ions until the chloride concentration was less than 1.37 mM. All chemicals were purchased from Millipore Sigma (St. Louis, MO). Human adipose derived stem cells (hADSCs) and RoosterNourish™ stem cell media were obtained from RoosterBio Inc. (Frederick, MD). Antibodies for immunohistochemical analysis were obtained from Abcam® (Cambridge, MA, USA).
Fabrication process optimization of collagen wound matrix
Figure 1 shows the electrochemical chamber and example of the CWM. Electrochemically aligned collagen constructs are formed through isoelectric focusing of the collagen molecules within an electrochemical chamber composed of two plate electrodes as shown in Figure 1(a). In this process, the bottom electrode was stainless steel and served as the cathode. The top electrode was an alloy of 90% Pt, 10% Ir, and served as the anode. Dialyzed collagen is placed between two plate electrodes, and a direct current voltage is applied. Due to the electrolysis of water, a pH gradient is formed within the chamber, and the collagen molecules electrophoretically migrate to its isoelectric point (pH∼9), forming a densely packed sheet of pure collagen, called the collagen wound matrix (CWM), on the cathode plate.19–22 Following deposition, the collagen matrix formed is collected, incubated in phosphate buffered saline (PBS) at 37°C to induce fibrillogenesis, cross-linked in 0.1% N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide hydrochloride (EDC)., washed with water, and lyophilized.
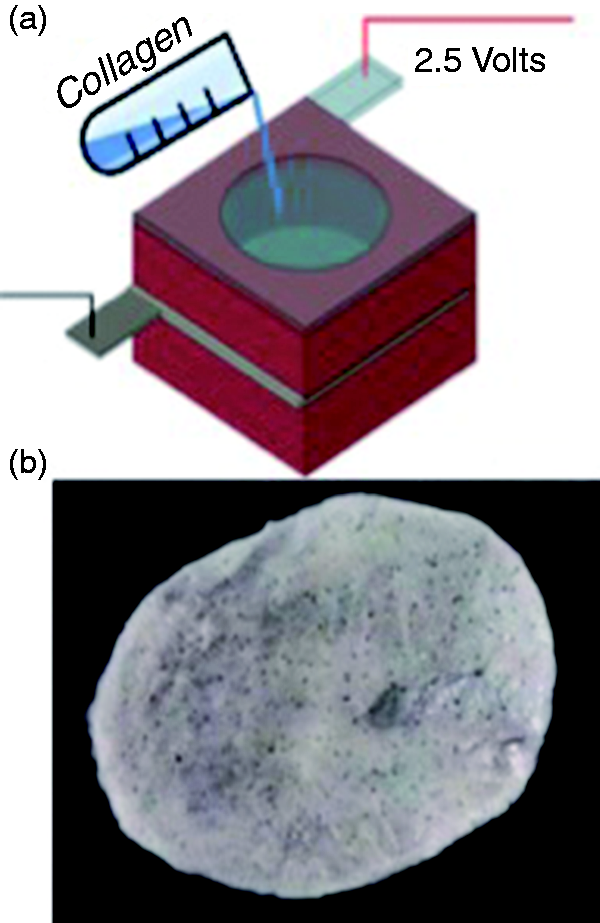
(a) Schematic of electrochemical chamber used for CWM fabrication. Collagen was added between two plate electrode, a direct current is applied, and a pH gradient forms due to the electrolysis of water. The collagen molecules migrate to the isoelectric point of collagen, and a densely packed, robust collagen wound matrix (CWM) is formed, which is collected, cross-linked, and lyophilized. (b) Lyophilized CWM composed of pure, electrochemically aligned medical grade collagen.
Time and voltage required for optimal electrochemical deposition
First, the time required for optimal deposition was investigated. 1 mL (6 mg/mL) collagen was placed in the chamber, 2.5V was applied for 40, 80, and 120 min. The matrix that formed was collected, incubated in PBS for 1 h, frozen at – 20°C, and lyophilized. The mass, thickness, and porosity of the resulting matrix was investigated. Percent porosity was calculated using the following equation, following the method used by Davidenko et al.
23
The relative density (ρ*/ρs) of the CWM was calculated from the measured density of the CWM post lyophilization and compared to the known density of solid collagen (gelatin) was assumed to be 1.3 mg/mm3.23–26 Porosity is defined as the percentage of void space in the 3D matrix, thus, a solid CWM would have a porosity of 0% using this method.
27

The voltage for optimal deposition was also determined. 1 mL (6 mg/mL) collagen was placed in the chamber and 2.5 V or 5.0 V of direct current was applied for 80 min. The matrix that formed was collected, incubated in PBS for 1 h, frozen at – 20°C, and lyophilized. The mass, thickness, and porosity of the resulting matrix was investigated.
Time and voltage investigation statistical analysis
For the investigation of the optimal time required for deposition, a one-way ANOVA was used to analyze significance for each parameter analyzed. The mean of each group was compared to the mean of every other group, and Tukey’s test was used to account for multiple comparisons. Significance was set at p < 0.05; n = 4 per group. For the investigation of the optimal voltage, an unpaired t-test was used to compare the mean of each group for each parameter analyzed. Significance was set at p < 0.05; n = 4 per group.
Characterization of CWM
Free amine group content and degree of cross-linking
The degree of cross-linking of the CWMs was determined by evaluating the content of free primary amine groups present in cross-linked and non-cross-linked samples. A 2,4,6-trinitro-benzene-sulfonic acid (TNBS) assay was conducted to determine the degree of cross-linking, based on available amino groups.28–30 To each sample (approximately 1 mg), 1 mL of a 4% (w/v) NaHCO3 solution and 1 mL of freshly prepared 0.5% (w/v) TNBS were added. The samples were reacted at 40°C for 5 h. 3 mL of 6 M HCl was added and the samples were hydrolyzed at 60°C for 90 min. The final solution was cooled to room temperature, diluted with 5 mL of e-pure water, and absorbance at 420 nm was measured using a Synergy H1 Hybrid Multi-Mode Reader (BioTek®, Winooski, VT). Control (blank) samples were prepared in the same way, except the HCl was added prior to the TNBS in order to eliminate any reaction of TNBS with amine groups. The absorbance of the control sample was subtracted from each sample’s value. The absorbance of the samples was correlated to a glycine concentration curve obtained using the same methods, with increasing concentrations of glycine in the NaHCO3 solution. Three replicates were used for each sample. The concentration of glycine was used to determine the number of amino groups present. Non-cross-linked CWM was assumed to have 100% of the available free amine groups. The degree of cross-linking is presented as the percentage of primary amino groups that were bound during cross-linking, with respect to the number of free amino groups in uncross-linked samples. Therefore, uncross-linked samples represent 0% cross-linking. In determining the degree of cross-linking, it was assumed that each lost amine group participates in one crosslink. 31
In vitro degradation
Two experiments to determine the CWM degradation were performed. First, CWMs were incubated in cell culture to investigate stability in cell culture. Secondly, CWMs were exposed to collagenase and the enzymatic degradation was monitored to mimic in vivo conditions.
To investigate degradation in cell culture, CWMs with mass of ∼5 mg were placed in a vial with 2 mL of RoosterNourish™ stem cell media and incubated at 37°C with 5% CO2 for two days. Following this incubation, the media was removed and replaced with keratinocyte serum-free media (KSFM) (Gibco, Grand Island, NY), which matches the culture media and procedure followed to prepare treatments for animal studies. After 24 h in KSFM, the scaffolds were collected, thoroughly rinsed with e-pure water, lyophilized, and dry sample mass was determined. Gravimetrical analysis was carried out to determine the percent degradation of the CWMs, according to the following equation

In the second degradation analysis, enzymatic degradation by collagenase was investigated. CWMs of approximately 5 mg were submerged in 2 mL 0.1M Tris-HCl with 50 mM CaCl2, pH = 7.4 at 37°C. 100 units of collagenase Type I (Worthington Biochemical Corporation, Lakewood, NJ) was added in 3.3 μL Hanks buffered salt solution. CWMs were incubated at 37°C for 1, 2, and 24 h (n = 3 per time point). At the specified time point, samples were placed on ice to stop enzymatic processes and the remaining sample was removed from the buffer. Samples were thoroughly rinsed in e-pure water, lyophilized, and dry sample mass was determined. Gravimetrical analysis was used to determine the percent degradation of the CWM. The amount of collagenase and buffer were selected in the mid-range of analyses of other collagen scaffolds for wound healing to provide some basis for comparison.32–34
Porosity and microstructure
Porosity and microstructure of the CWM was investigated using a Carl Zeiss Environmental Scanning Electron Microscope EQ 1209. Percent porosity was also calculated following the method used by Davidenko et al. 23 as described previously.
Tensile strength
The uniaxial tensile strength of the CWMs in both dry and wet conditions was tested on a Mark-10 Tensile Tester (Mark 10 Corporation, Copiague, NY) at room temperature. For the tensile test, specimens were fabricated in a dog-bone shape, adapted from ASTM standard D638-14. 35 The narrow section was approximately 6 mm wide. The same volume of collagen per surface area of matrix was used to fabricate the samples for tensile testing as used for in vivo investigation. Specimens were lyophilized and rolled with a micro-needle roller using the same methods as matrices used for in vivo investigations. Wet specimens were thoroughly soaked with PBS prior to testing and maintained wet throughout testing. Tensile strength of a dry scaffold fabricated with of an equal mass of traditionally gelated collagen that was cross-linked and lyophilized in the same manner as the CWM was included for comparison. The speed of the crosshead was set at 2 mm/min. Samples were tested until failure.
Tensile testing statistical analysis
Three samples were tested at each condition. An ordinary one-way ANOVA with Tukey’s test was performed to determine significant differences, with the significance level set at p < 0.05. The mean of every group was compared to the mean of every other group.
Cell culture and seeding on collagen wound matrix
hADSCs were obtained from RoosterBio, Inc. Cells were >70% positive for CD166, CD105, CD90, and CD73 and <20% positive for CD14, CD34, and CD45 surface marker expression. Passage 2 cells were cultured in RoosterNourish™ stem cell media, supplemented with 100 units/mL penicillin, 100 μg/mL streptomycin, and 0.25 μg/mL Amphotericin B (Antibiotic-Antimycotic, Gibco, Grand Island, NY) according to supplier’s guidelines. Three days prior to surgery and treatment hADSCs were trypsinized and diluted to 2 × 105 cells per mL in media. A sterile CWM was placed in a well of 6-well plate and seeded with 105 hADSCs in 0.5 mL media. Scaffolds and cells were incubated for 20 min at 37°C with 5% CO2 to allow for initial cell attachment. Following attachment, 1.5 mL media was added to each well. The day before surgery and treatment, CWMs with cells were rinsed with Dulbecco’s phosphate-buffered saline without Ca2+ and Mg2+ (Gibco, Grand Island, NY) and media was changed to serum free media (KSFM) with supplied supplements and 100 units/mL penicillin, 100 μg/mL streptomycin, and 0.25 μg/mL amphotericin B. Cell-seeded CWMs were incubated at 37°C with 5% CO2 until time of treatment. The 5 mm circular treatment delivered to each wound was determined to have approximately 105 cells. Cell counts were determined by degrading a seeded scaffold with collagenase, collecting the released cells, and quantifying with Trypan Blue assay. Three samples were used to determine the number of cells delivered.
Murine diabetic wound healing model
The efficacy of the CWM with and without stem cells was evaluated in vivo in the db/db mouse, a genetically diabetic and obese mouse model with a defect in the leptin receptor gene lepr that models human type 2 diabetes well. The db/db mouse has been well established for chronic ulcerative wound healing.36–38 Three groups were analyzed: nontreated animals, CWM alone, and CWM seeded with hADSCs. All mice were confirmed to be diabetic, as measured by blood glucose levels above 250 mg/dL. To mimic a chronic wound, hair was removed and two full thickness wounds with diameter of 5 mm, were created bilaterally on the dorsal surface of the mouse with a biopsy punch. The CWM was cut to exactly fit the wound size placed into the wound. Cell-seeded scaffolds were placed with the cell-seeded side of the scaffold directly into the wound bed. Secondary protective dressings consisting of a bandage containing antibiotic (0.8% Benzalkonium Chloride) and 1” wide surgical tape were applied. Animals were sacrificed after 7, 14, and 21 days of healing. Secondary dressing was changed every 7 days. The animals were cared for in accordance with the guidelines set forth by the Committee on Laboratory Resources, National Institutes of Health, and the surgical and care protocols were approved by Institutional Animal Care and Use Committee (IACUC) at the University of Texas Health Science Center at San Antonio.
Determination of open wound area
At days 0, 7, 14, and 21 post-wounding, photographs with a ruler were taken for each wound with a digital camera. The wound area was defined as the open area that had not yet been filled with tissue. The diameter of the wound at each time point was measured twice and an average was used. Wounds were considered to be circular. The wound areas are expressed as a percentage of their original area, which was measured immediately after wounding. The following formula was used
Wound size statistical analysis
Wound sizes were analyzed for statistically significant differences using an ordinary one-way ANOVA with Dunnett’s test. All groups were compared to the CWM alone as the control. Differences were considered significant at p < 0.05. All statistical analyses were performed with GraphPad Prism 7.0b (GraphPad Software, La Jolla, CA). In this analysis, the CWM alone was chosen as the control mainly due to its tensile strength. We hypothesized that the tensile strength of the matrices may inhibit the natural contraction of the rodent skin, making comparisons to untreated wounds inappropriate. However, it is critical to compare treated wounds with the untreated to investigate efficacy and quality of tissue formation, thus, an untreated group was included in the wound size comparisons as well.
Granulation tissue formation
At 7, 14, and 21 days post wounding, wounds were collected using an 8 mm biopsy punch, so the wound and some healthy surrounding skin was collected for comparison. The wound was bisected and fixed in formalin. 5 μm sections were processed for routine hematoxylin and eosin (H&E) analysis. ImageJ Software (NIH, Bethesda, MD) was used for quantitative analyses of the histological sections. Granulation tissue area was determined as the area of granulation tissue beneath the wound, excluding the eschar, and extending to the paniculus carnosus at the edge of the wounded area. Granulation tissue area was measured in mm2.
Granulation tissue formation statistical analysis
All values are expressed as mean ± SEM. For each group, n ≥ 3, except for animals treated with CWM + hADSCs sacrificed at 21 days, for which n = 2, due to animal sacrifice for non-study related reasons. Statistical analysis was performed using an ordinary one-way ANOVA with Dunnett’s test. Groups treated with CWM and CWM with hADSCs were compared with untreated wounds. Significance level was set at p < 0.05.
Epidermal thickness
The epidermal thickness of the reformed tissue of each wound was analyzed at 21 days after wounding. The epidermal thickness was measured as the distance from the basement membrane to the superficial aspect of the epidermis at nine random places within the wounded area. ImageJ software was used to quantify the thickness.
Epidermal thickness statistical analysis
The thickness at each time point was analyzed statistically with an ordinary one-way ANOVA followed by Tukey’s test to compare the mean of every group to the mean of every other group. Significance was set at p < 0.05.
Results
Fabrication process optimization of collagen wound matrix
Time and voltage required for optimal deposition
Based on deposition efficiency (analyzed by mass; 6 mg is 100% efficiency because 6 mg collagen was initially used in the deposition process), thickness, and porosity, the optimal voltage and deposition period for the CWM was determined, as shown in Figure 1.
Voltage higher than 5 V tends to result in violent electrolysis of water and bubbles being entrapped within collagen, which leads to nonuniform structure. On the other hand, voltage lower than 1.23 V (the threshold of water electrolysis) will not result in collagen electrochemical deposition. Thus, we choose 2.5 and 5.0 V as investigational conditions. The optimal voltage was determined to be 2.5 V. Although an increase in deposition efficiency was seen using 5.0 V, the CWMs formed with 5.0 V were significantly thinner and less porous than those formed using 2.5V (41.1 ± 12.6% and 84.6 ± 4.24%, porosity, respectively), as shown in Figure 2(a) to (c). 5.0 V formed matrices with very densely packed collagen molecules that were thinner and more solid after lyophilization than those formed at 2.5 V. Therefore, 2.5 V was determined to be the optimal deposition voltage due the higher porosity formed, which is an important physical characteristic in skin tissue engineering and wound healing treatments.
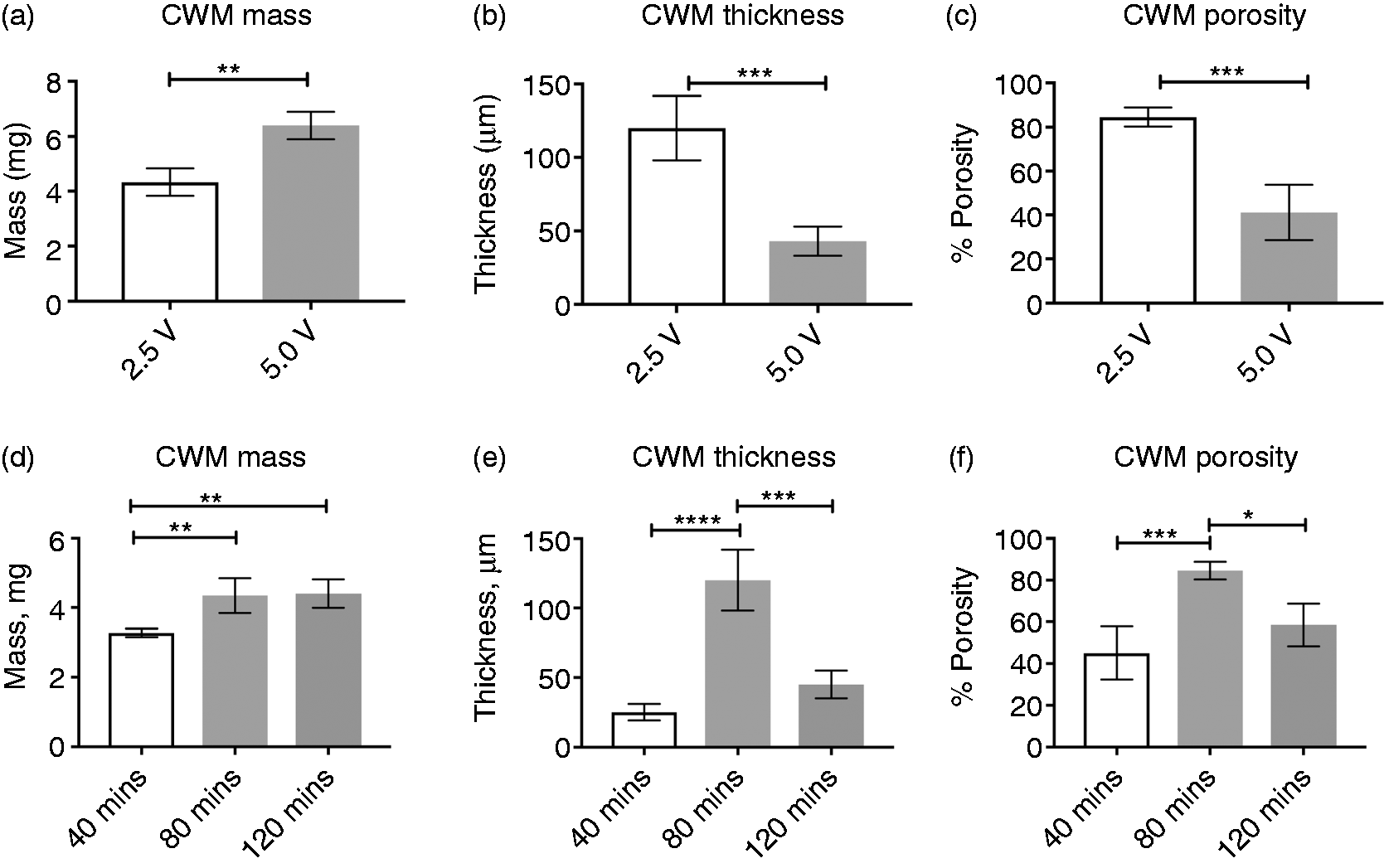
(a–c) CWM mass, thickness, and porosity of lyophilized CWM after deposition at 2.5 V or 5.0 V for 80 min. An unpaired t-test was used to compare the mean of each group. Significance was set at p < 0.05. Shown is the mean ± standard deviation, n = 4. **p < 0.002; ***p < 0.0007. (d–f) CWM mass, thickness, and porosity of lyophilized CWM after deposition at 2.5 V for 40, 80, or 120 min. One-way ANOVA with Tukey’s test was used to compare the mean of every group. Significance was set at p < 0.05. Shown is mean ± standard deviation, n = 4. *p < 0.0332; **p < 0.021; ***p < 0.002; ****p < 0.0001.
Figure 2(d) to (f) compares the mass, thickness, and porosity of CWMs formed by collagen deposition for 40, 80, and 120 min. Of the three deposition times investigated at 2.5 V, the desired deposition time is 80 min. At 40 min, the CWM formed was formed with low deposition efficiency, indicated by a significantly lower final mass than 80 or 120 min, and the matrix was thin with a mean porosity of 45 ± 13%, indicating 40 min was not long enough for sufficient collagen matrix formation. After 80 min, collagen deposition is increased, and a thicker scaffold was formed with significantly higher porosity (84.6 ± 4.24%) than both 40 and 120 min. At 120 min, the collagen also deposited with high efficiency, which was approximately equal to that at 80 min. However, the matrix formed was significantly thinner and less porous (58.5 ± 10.2%) than those formed for 80 min. A longer deposition time forms a matrix with very densely packed collagen molecules, resulting in a thinner and more solid matrix after lyophilization. For skin tissue engineering, high porosity is crucial. Thus, a deposition time of 80 min was used throughout this study to form CWMs with high efficiency and high porosity.
Final fabrication method of collagen wound matrix
About 2 mL of dialyzed collagen was placed between two electrodes in a circular-shaped electrochemical chamber with a 3 cm diameter. Any empty space in the chamber was filled with e-pure water and 2.5 V of direct current was applied for 80 min. The CWM that formed was collected and incubated in 1x PBS for at least 1 h to facilitate collagen fibril formation. Next, the CWM was rinsed with e-pure water, and submerged in 1.67 mL of 0.1% EDC in e-pure water at room temperature overnight to crosslink the collagen fibers. Following cross-linking, matrices were thoroughly rinsed with copious amounts of e-pure water, frozen at -20°C, and lyophilized. Next, CWMs were rolled with a micro-needle roller, in order to add porosity by the creation of larger pores than those formed inherently through ice crystal sublimation during lyophilization. The needle length is 1 mm, diameter of 0.3 mm, and 1 mm spacing between needles. Dried CWMs were sterilized with ethylene oxide. Final CWMs had a thickness of approximately 100 μm.
Characterization of collagen wound matrix
Free amine group content and degree of cross-linking
As expected, the number of free amine groups fell significantly after crosslinking. After cross-linking in 0.1% EDC, the degree of cross-linking of the CWM was found to be 67%, indicating that 67 ± 19% (mean ± SD) of the available amino groups were bound during cross-linking. Non-cross-linked samples were set as 0% cross-linked, as shown in Figure 3(a).
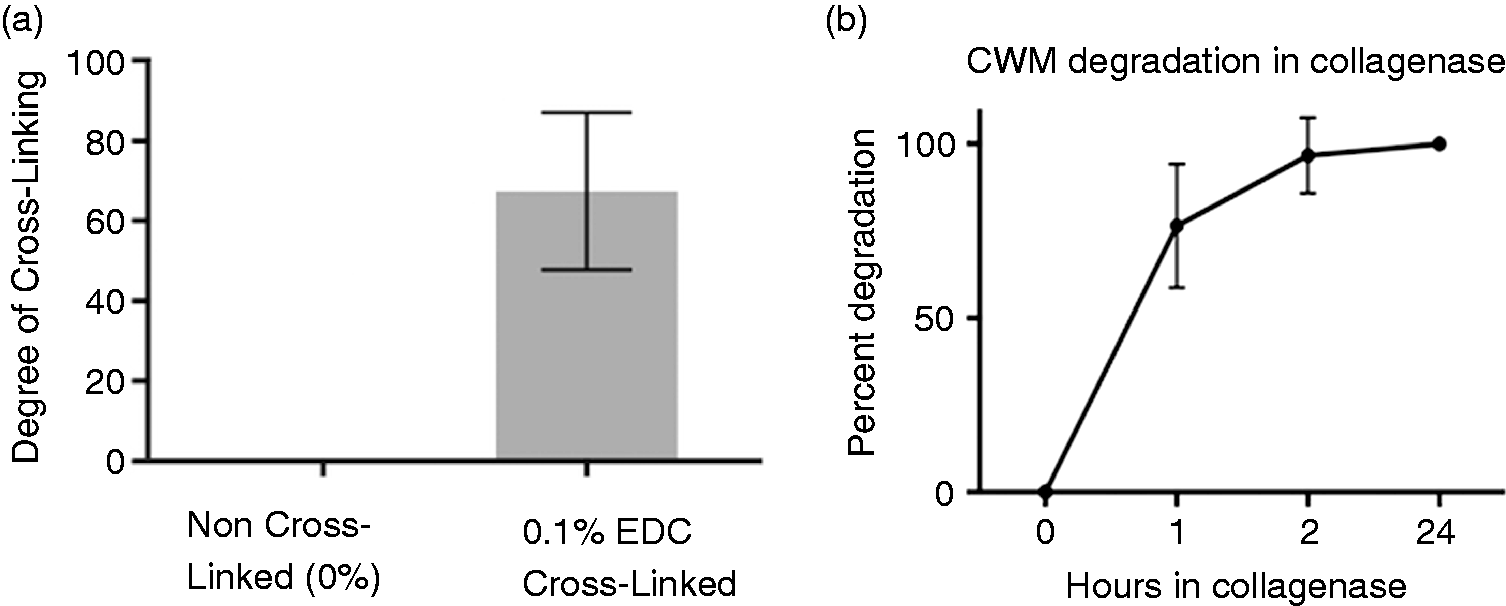
(a) Degree of cross-linking of CWM. Non-cross-linked matrices were set as a 0% degree of cross-linking, because 0% of available amino groups were bound. CWMs cross-linked in 0.1% EDC were found to have a 67% ± 19% (mean ± SD) degree of cross-linking, indicating approximately 67% of the available amino groups were bound. Presented is mean ± SD, ≥ 3 per group. (b) CWM degradation in the presence of 100 U collagenase at 37°C. Presented is mean ± SD, n = 3 per time point.
In vitro degradation
The matrices were shown to stay nearly completely intact in cell culture media during a four-day incubation, showing only 12 ± 2% degradation (mean ± SD). This matches the period required for stem cell culturing on the matrix before treatment, indicating that the matrices are well suited to culture prior to implantation. The CWMs were easily manipulated, flexible, and retained their shape well, making them a practical material for use in the clinical setting, even after submersion in media for several days.
In the presence of collagenase, the matrices were quickly degraded. After one hour in collagenase, the matrices were at 76% degradation, and after 2 h, matrices were 94% degraded. Matrices were completely degraded by the 24 h, as shown in Figure 3(b).
Porosity and microstructure
The CWM was found to be highly porous, showing large, interconnected pores. The SEM images of the porosity of the CWM are included in the supplementary data. Using gravimetrical analysis, the CWMs were found to have an average percent porosity of 84.6 ± 4.2% (mean ± SD).
Tensile strength
A crucial feature of this material is it is very high tensile strength when compared to a gelated collagen scaffold. Here, tensile strength of the CWM was analyzed in both dry and wet conditions in order to more closely mimic physiological states. The ultimate tensile strength (UTS) of the dry CWM was found to be 7.3 ± 0.5 MPa (mean ± SD), showing substantial strength despite being only ∼100 μm in thickness and including defects introduced by the micro-needle rolling. In the wet state, the CWM retained substantial strength. The UTS of wet CWM was found to be 2.5 ± 0.5 MPa (mean ± SD). Traditionally gelated collagen did not retain sufficient material properties to withstand tensile testing in the wet state, further highlighting the superiority of the electrochemically aligned collagen constructs. As shown in Figure 4, the ultimate tensile strength of the collagen was significantly reduced in a wet state. However, the CWM retained sufficient tensile strength to maintain adequate structural integrity and mechanical properties necessary for wound healing treatments.
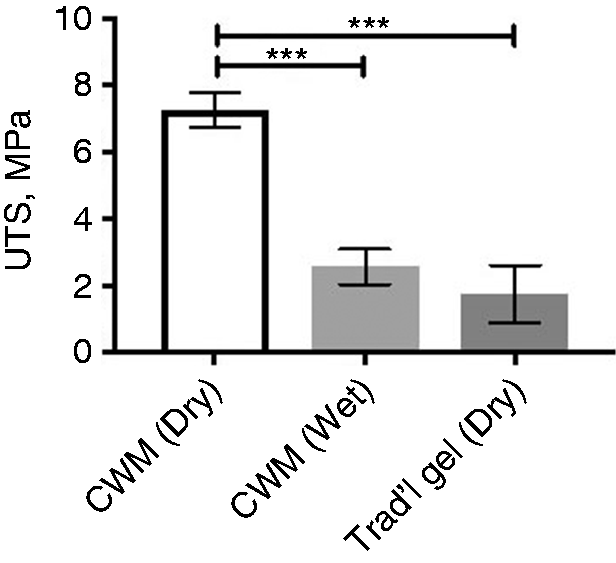
Ultimate tensile strength (UTS) of collagen wound matrix in wet and dry states. Shown is mean ± SD. Although the collagen wound matrix (CWM) tensile strength reduced significantly after wetting, adequate structural properties are maintained for wound healing applications. ***p < 0.0003. Analyzed with ordinary one-way ANOVA with Tukey’s test to compare the mean of every group to the mean of every other group, significance level set at p < 0.05.
Biocompatibility and cell proliferation on the CWM
Prior to in vivo studies, the biocompatibility and cell proliferation capability of the CWM was investigated. A direct contact test was run following the guidelines of ASTM F813-07 (2012) to assess the biocompatibility of the CWM. This test showed that the CWM material has high biocompatibility; no signs of cytotoxicity were observed, and the viability of cells that were in contact with the CWM were nearly equal to (99% of) the healthy control. Once the CWM was shown to be biocompatible, the growth and proliferation of hADSCs seeded on the CWM was investigated. This analysis determined that hADSCs are capable of growth and proliferation on the CWMs, and that the CWM is an adequate scaffold for delivery of CWMs to a wound. Detailed experimental methods, results, and figures of the biocompatibility and cell proliferation studies on the CWM are included with the supplemental material.
Murine diabetic wound healing model
The CWM with and without hADSCs was tested in full thickness excisional skin wounds in diabetic mice, and showed excellent tissue regeneration properties. Mice showed no adverse reactions during the study duration. No signs of immune rejection from either the collagen or the hADSCs were observed in any group. Mice did not lose a substantial amount of weight, and appeared to be in normal health. No signs of infection or inflammation were observed in any animal.
Determination of open wound area
Figure 5(a) shows representative wound images of wound healing at days 0, 7, 14, and 21. All wounds showed complete closure by day 21. Although time to wound closure was similar, notable differences were seen in the wounded sites after 21 days. The untreated wounds were a much darker color after closure, and the tissue formed was hard and rigid, indicative of scar tissue. The newly formed tissue was inflexible and would likely impair movement if the animal had been injured over a joint. The groups treated with CWM and CWM + hADSCs formed lighter colored, healthy appearing tissue where the skin had been injured. The tissue was flexible and appeared much more similar to healthy skin than to scar tissue. The quality of the tissue formed was further analyzed with histology. Figure 5(b) compares the percent of original wound size between untreated and treated groups. Wound size at each time point was analyzed for significant differences compared to the CWM alone using an ordinary one-way ANOVA with Dunnett’s correction, with the significance level set at p < 0.05. At both days 7 and 14 after injury, no significant differences were found between the wound area of mice treated with CWM alone, mice treated with CWM seeded with hADSCs (labeled in figures as CWM+hADSCs), or untreated wounds.
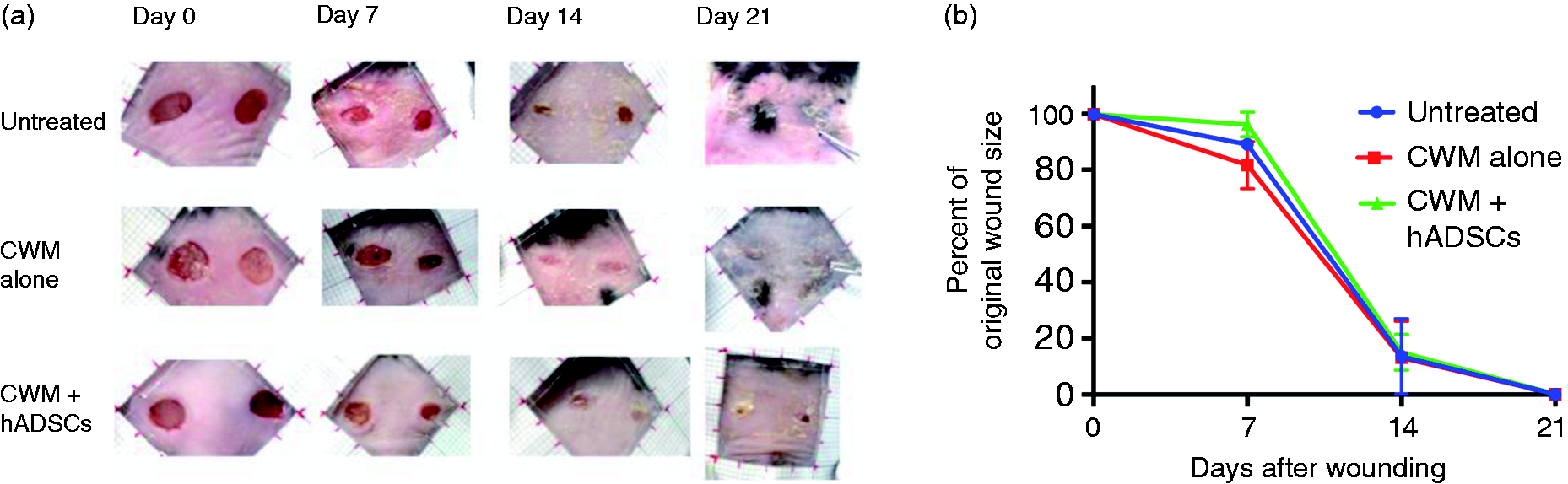
(a) Representative images of wound closure at days 0, 7, 14, and 21 after full thickness excisional wounds in db/db mouse. Complete closure was seen in every group by day 21. All pictures at same magnification; dark lines in ruler surrounding wound indicate 5 mm. Notable differences were seen in the quality of tissue formed between the treated and untreated wounds, which was further analyzed histologically. (b) Analysis of wound size at days 0, 7, 14, and 21 after wounding. Wound size at each time point was analyzed for significant differences compared to the untreated group using an ordinary one-way ANOVA with Dunnett’s correction. No groups showed statistically significant differences in wound size at any time point. Shown is mean ± SEM, n = 4 for each time point, except for animals treated with CWM + hADSCs sacrificed at 21 days, for which n = 2.
Granulation tissue formation
The histological analysis of the wounds showed that both the novel CWM alone and the hADSC seeded CWM stimulated excellent tissue regeneration, showing significant differences to the untreated wounds at 7, 14, and 21 days, as analyzed by formation of granulation tissue area (Figure 6(a)) and histological analyses of H&E stained specimens (Figure 7). After 7 days of healing, both wounds treated with the CWM alone and the CWM + hADSCs had increased granulation tissue formation. The same trend was seen at 14 days post wounding; treated groups had regenerated an increased amount of granulation tissue over untreated groups. By 14 days, the wounds treated with CWM + hADSCs showed significantly increased volumes of granulation tissue than untreated wounds. While granulation tissue increased between days 7 and 14 in both treated groups, very little granulation tissue accumulation was seen between days 7 and 14 in the untreated diabetic wound. By day 21, the untreated diabetic wound had significantly less granulation tissue formation than wounds treated with both the CWM alone and CWM + hADSCs, indicating the importance of effective intervention in the chronic wound. At all time points, wounds treated with the CWM alone or combined with hADSCs showed substantially increased healing, both in terms of granulation tissue formation and histological analysis.
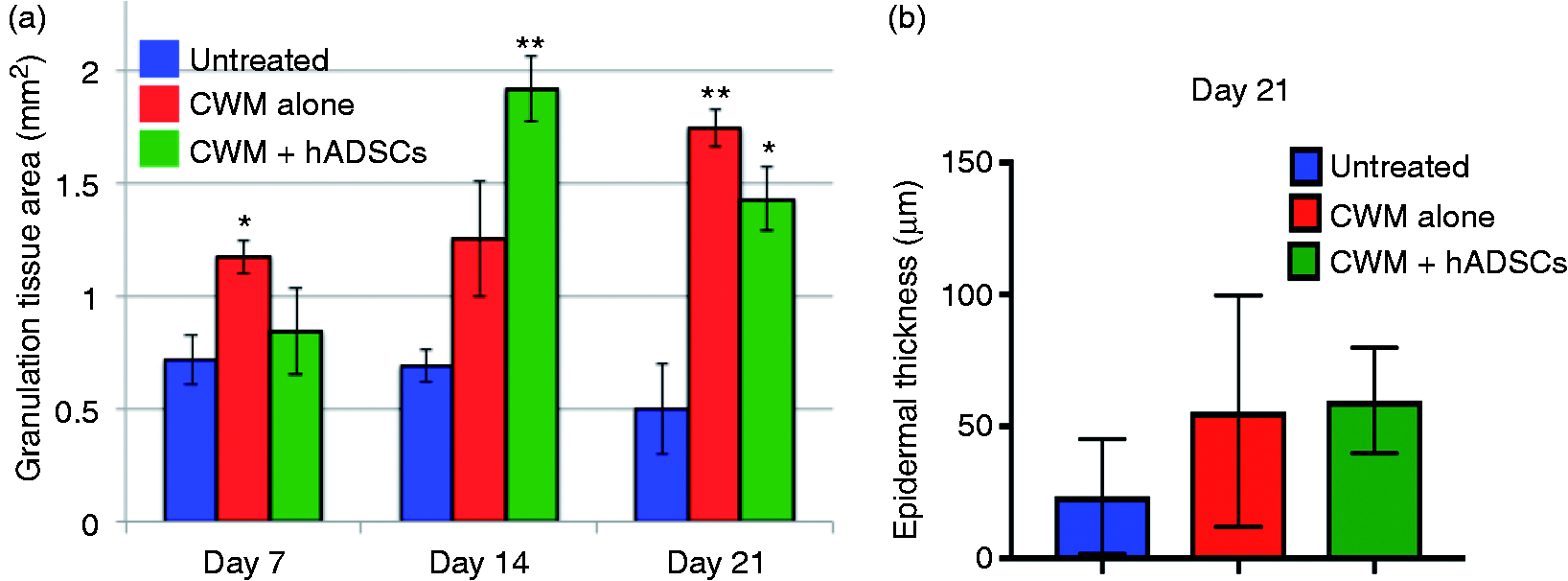
(a) Granulation tissue area of untreated wounds, wounds treated with the CWM alone, and wounds treated with CWM + hADSCs. Shown is mean ± SEM, n = 4 for each time point, except for animals treated with CWM + hADSCs sacrificed at 21 days, for which n = 2. Shown is mean ± SEM. Significant differences were assessed using an ordinary one-way ANOVA with Dunnett’s test. Groups treated with CWM and CWM + hADSCs were compared to untreated wounds. Significance level was set at p < 0.05. *p < 0.02; **p < 0.002. (b) Epidermal thickness at 21 days post wounding. No groups showed statistically significant differences. The thickness at each time point was analyzed statistically with an ordinary one-way ANOVA followed by Tukey’s test to compare the mean of every group to the mean of every other group. Significance was set at p < 0.05. Shown in mean ± standard deviation.
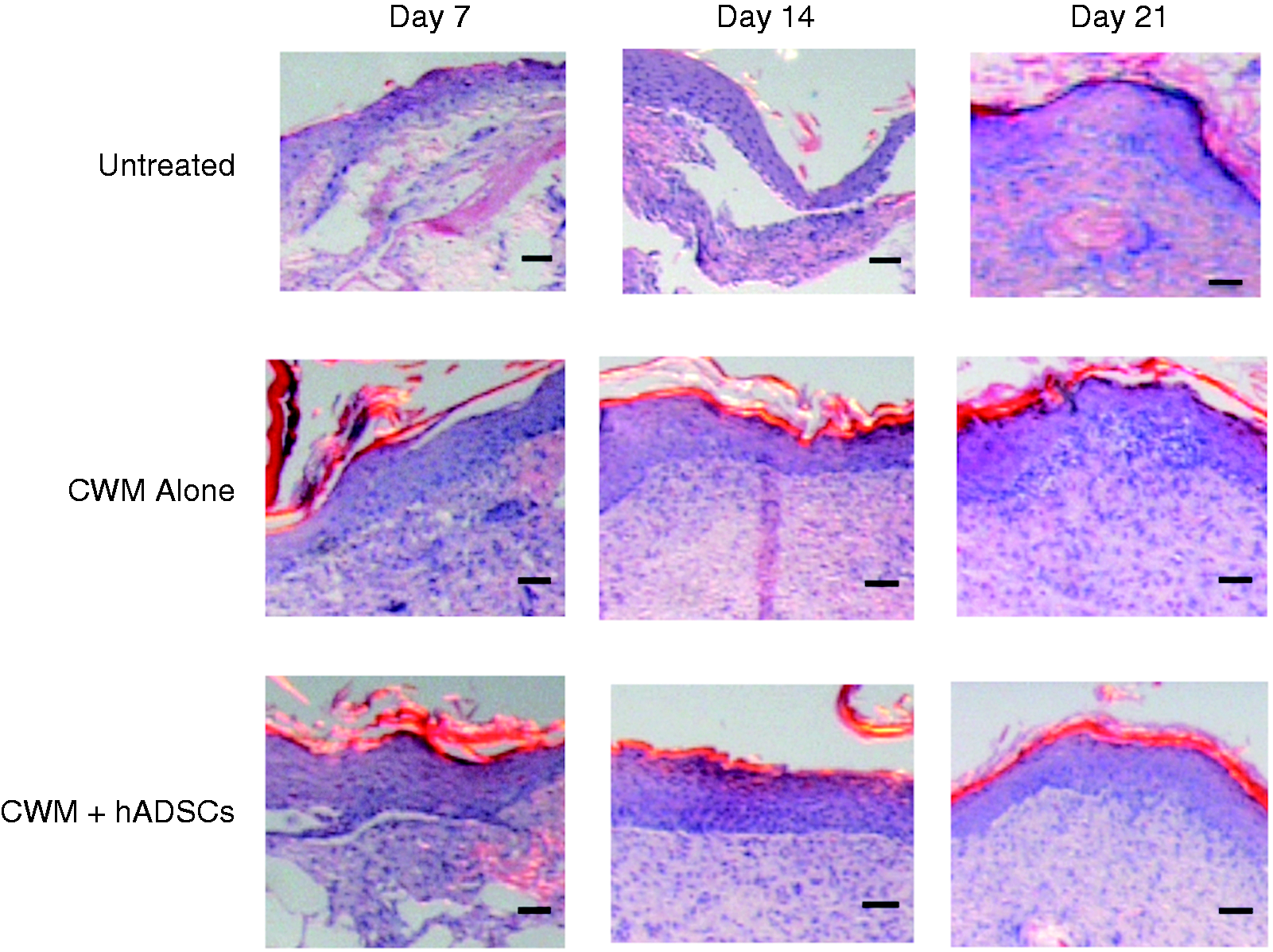
H&E stained sections of healing wounds at 7, 14, and 21 days post wounding. All examples are representative images of biopsies from wounds in each treatment group, taken near the center of the injured area. Scale bar indicates 50 μm.
Epidermal thickness
At every time point, wounds treated with the CWM alone and the CWM + hASDCs showed a more organized epidermal layer than the untreated wounds. By 21 days, wounds treated with the CWM alone and CWM + hADSCs had regenerated a thicker epidermal layer than untreated wounds. While the difference was not statistically significant, it does show a clear trend of increased healing in the treated groups compared to untreated. Groups treated with the CWM alone and the CWM + hADSCs resulted in approximately equal epidermal thickness at 21 days. Figure 6(b) shows epidermal thickness as 21 days post wounding.
Discussion
The electrochemical fabrication method developed here produces a pure collagen material that possesses much higher tensile strength than typical collagen materials fabricated by the heat gelation process. The CWM has high porosity, slow degradation in cell culture media, and excellent cell and tissue biocompatibility. The optimized process uses a low voltage for a moderate amount of time to form CWMs that are thick and robust, yet not overly densely packed that the porosity is decreased. This CWM material was shown to be an excellent treatment for chronic diabetic skin wounds, both with and without the addition of hADSCs.
An principal aspect of the pathology of chronic diabetic skin wounds is the failure to regenerate granulation tissue within the wound bed.
4
In the full thickness excisional model with db/db mice, this trait was mimicked. In untreated wounds, after initial granulation tissue formation within the first 7 days, very little additional granulation tissue was regenerated during the remainder of the 21-day study. A treatment that can stimulate healing and tissue reformation is needed in order to achieve healing in such wounds. When treated with the CWM and CWM + hADSCs, an increase in granulation tissue formation was seen after 7, 14, and 21 days. After 7 days, a significant increase in granulation tissue compared to untreated wounds was seen only in the group treated with the CWM alone, but by 14 days, a significant increase was present in the wounds treated with CWM + hADSCs. This trend may correspond to the transition between the inflammatory and proliferative phases of wound healing. Chronic wounds are in a persisting state of inflammation and often lack the biological cues necessary to progress to the proliferative phase of wound healing, in which granulation tissue is typically formed.
6
Perhaps the addition of the hADSCs is most effective during this transitional period, both by secreting factors that encourage granulation tissue formation in the wound and contributing to tissue formation by remaining in the wound. This hypothesis may explain why the largest increase in granulation tissue formation observed in the groups treated with hADSCs was between 7–14 days. By 21 days, both groups treated with CWM alone and CWM + hADSCs had formed significantly more granulation tissue than untreated wounds, indicating that both with and without hADSCs, the CWM is an effective treatment to stimulate healthy tissue regeneration in the diabetic wound.
A striking difference between the treated diabetic skin wound and normal diabetic skin can be seen in Figure 7. In diabetic skin, the epidermal and dermal layer was very thin and fragile, and did not show progressive regeneration through 21 days. However, in the CWM ± hADSC treated group, a thick epidermis layer, thick stem cell-rich layer, and very thick, cell-rich dermal layer were seen (Figure 7), and almost no fatty tissue was seen in the regenerated tissue in treatment groups.
Interestingly, there was little difference in wound size between the treated and untreated groups. It is well documented that rodent skin heals largely by contraction, as opposed to tissue regeneration mechanism seen in human skin.39–41 This healing mechanism often results in significant scarring and poorly formed dermal and epidermal structures, which was observed in the untreated animals in this study. Thus, it is logical to infer that the quick decrease in wound size in the untreated groups is largely due to this contraction mechanism. Here, it was hypothesized that the mechanical properties of the CWM, including its tensile strength, may act to prevent the skin from immediate contraction. On the contrary, little difference in wound size in the treated and untreated wounds was observed, indicating nearly identical contraction. To prevent contraction, the mechanical properties of the CWM, likely including increased tensile strength, should be investigated and manipulated further. Alternatively, a ring-shaped splint can be placed on the wound to mechanically prevent contraction, allowing for better investigation of tissue regeneration. Both methods will be considered in future CWM studies. Regardless of the similar wound size, the treated wounds presented here resulted in much higher tissue quality formation (e.g. granulation tissue, more organized layer, thicker epidermis) as well as increased volumes of tissue formation with much less fatty tissues. Notably, groups treated with both CWM and CWM + hADSCs had thicker, more organized epidermal layers than the untreated diabetic wound. Both with and without hADSCs, the CWM accelerated healing and regeneration and led to higher quality tissue reformation in the diabetic skin wound than an untreated wound.
Importantly, the survival and healing mechanisms of the hADSCs delivered with the CWM remains to be investigated. Future studies will analyze more in-depth the role of the hADSCs delivered with the CWM.
Conclusions
We have optimized an electrochemical deposition method to form a novel CWM and investigated for the first time, the combination of this CWM with hADSCs for diabetic skin wound healing. The CWM shows favorable biomechanical properties, high biocompatibility, porosity, and very high tensile strength. In vivo, excellent tissue regeneration is seen when used both alone and when combined with hADSCs, and results in a significant increase in granulation tissue formation at 7, 14, and 21 days compared to untreated wounds. Wounds treated with the CWM formed a well-defined dermal and epidermal layer, and had increased epidermal thickness and tissue organization compared to untreated wounds. The CWM material is an excellent treatment for diabetic skin ulcers and non-healing skin wounds, and in the future may also be used for other injuries such as burns, blast injuries, and surgical incisions. The CWM is light and portable, making it ideal for use in a field setting, such as a military battlefield. In the future, the CWM will be further optimized for treatment of chronic wounds as well as other medical challenges such as soft tissue facial reconstruction, burns, and other traumatic injuries.
Statement of significance
Chronic diabetic skin wounds are a significant clinical issue, often necessitating amputation of the limb due to the nonhealing wound. Previously, electrochemical alignment of type I collagen via an isoelectric focusing mechanism has been shown to produce robust collagen biomaterials. Here, we have optimized this method to form a collagen wound matrix and investigated, for the first time, the combination of this collagen matrix with adipose derived stem cells for diabetic skin wound healing. We have shown that treatment with the collagen matrix alone and in combination with stem cells improves cutaneous wound healing in a full thickness excisional wound in a mouse model of type 2 diabetes.
Supplemental Material
Supplemental material for An electrochemically deposited collagen wound matrix combined with adipose-derived stem cells improves cutaneous wound healing in a mouse model of type 2 diabetes
Supplemental Material for An electrochemically deposited collagen wound matrix combined with adipose-derived stem cells improves cutaneous wound healing in a mouse model of type 2 diabetes by Nicole Edwards, Denis Feliers, Qingwei Zhao, Randolph Stone, Robert Christy and Xingguo Cheng in Journal of Biomaterials Applications
Footnotes
Authors’ Note
The raw/processed data required to reproduce these findings are available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge funding from the San Antonio Medical Foundation (San Antonio, TX) and the Southwest Research Institute Advisory Committee for Research (San Antonio, TX). The funding sources had no involvement in the conduct of the research and/or preparation of the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.