
Abstract
Injectable hydrogels that aim to mechanically stabilise the weakened left ventricle wall to restore cardiac function or to deliver stem cells in cardiac regenerative therapy have shown promising data. However, the clinical translation of hydrogel-based therapies has been limited due to difficulties injecting them through catheters. We have engineered a novel catheter,
Introduction
Cardiovascular disease (CVD) causes significant morbidity, mortality and economic burden worldwide. CVD causes >17 million deaths globally per year, which is expected to reach 23.6 million by 2030. 1 The greatest proportion of CVD is accredited to coronary heart disease including angina, myocardial infarction (MI) and coronary death. 1 Coronary artery revascularisation, following MI and ischemia, are effective at restoring blood flow; however, residual myocardial scarring remains permanently. Ischemic heart disease and MI result in progressive myocardial remodelling and left ventricular (LV) dysfunction. This reduces heart function and capacity over time and can lead to heart failure. Restoration of full cardiac function and elimination of myocardial scarring post-MI could eliminate the cascade of events leading to heart failure.2,3
Acellular injectable hydrogels that aim to mechanically stabilise the weakened LV wall in an attempt to restore cardiac function have been investigated. Algisyl (LoneStar Heart, Inc., USA) is one such hydrogel that is at an advanced stage of clinical development. Algisyl aims to mechanically stabilise the heart using an acellular alginate-based hydrogel (elastic modulus 3–5 kPa in vivo) and is delivered via an anterior thoracotomy and epicardial injections.4,5 This therapy relies on ventricular wall thickening and geometry restoration to provide its mechanism of action. Interestingly, the Lonestar Heart website reports that a minimally invasive version of Algisyl is in late pre-clinical trials, but no further details are available to date. VentriGel (Ventrix, Inc., USA) and IK-5001 (Bellerophon Therapeutics, USA) are two other hydrogels at advanced stages of development. Minimally invasive delivery via percutaneous injection offers many advantages over surgical intervention, including lower procedure risks, quicker recovery times, reduced damage to target and surrounding tissue and higher potential for clinical integration.6,7 However, minimally invasive delivery of hydrogels to the heart is inherently difficult. Over the past decade progress has been made in the development of both cellular, acellular, physical and covalently cross-linked hydrogels for cardiovascular applications.4,8–11 Despite advances in the development of these biomaterial therapies, there has been a lag in the development of minimally invasive endocardial catheters. To date, only physically cross-linked hydrogels have been delivered percutaneously via single lumen catheters as previously discussed.10,12 Maintaining the biomaterial properties and cell viability (if included) while utilising a minimally invasive approach is challenging.
Regenerative therapy, particularly stem cell technology has shown promising preliminary clinical data in the cardiac field. Despite its great potential, one major challenge has presented itself; studies have unanimously shown poor retention/survival of delivered cells.3,13,14 In order for stem cell therapy to achieve successful outcomes, it is necessary to enhance cell viability and retention during delivery and their ability to survive within the harsh post-MI heart. Such regenerative approaches could be optimised by utilising biomaterials, specifically hydrogels, as delivery vehicles to enhance cell survival. 15 The translation of these therapies has also been limited by a lack of development of minimally invasive endocardial catheters. The “holy grail” of cell delivery for cardiac regeneration is the development of a biomaterial delivery system that optimises cell delivery, survival and engraftment, and is compatible with catheter technology ensuring minimally invasive delivery.
Hyaluronic acid (HA) is a naturally occurring linear unbranched polysaccharide found in the connective, epithelial and neural tissues of vertebrates. HA has been used for tissue engineering, in particular in cardiac epicardial approaches,9,16 due to its inherent biocompatibility, biodegradability and viscoelastic characteristics. For cardiac endocardial approaches the solution must gel rapidly at the injection site to retain the therapy at the desired site when the needle is retracted. HA needs to be modified as it is rapidly metabolised by hyaluronidases in vivo. Covalently cross-linkable derivatives of HA are a potential solution, exhibiting an extended biological half-life in addition to being able to withstand high mechanical loads. One such material is a hydroxyphenyl derivative (HA-PH) which is capable of forming a covalently cross-linked hydrogel via an oxidative coupling reaction catalysed by horse radish peroxidase (HRP) and hydrogen peroxide (H2O2). 17 The solution is agitated with a static mixer to expose the HRP to the H2O2, which results in oxidation of the HRP and the phenol moiety of the HA-PH conjugate. Cross-linking of oxidised HA-PH molecules then occurs forming a robust hydrogel. The mechanical properties and degradation rate of the hydrogels can be modified by altering the cross-linking concentration. Cell attachment to HA is thermodynamically unfavorable because of its hydrophilic and polyanionic properties. 18 Fibronectin-derived RGD is an oligopeptide which stimulates integrin-mediated cell adhesion. 19 Contipro (Czech Republic) have synthesised an HA derivative (HA-PH-RGD) bearing both hydroxyphenyl moiety and RGD, and can undergo HRP-mediated cross-linking to form robust hydrogels favorable for cell attachment, as described in this study.
Achieving an injectable biomaterial for minimally invasive delivery is inherently difficult due to the viscous nature of biomaterials, the length of the delivery device, the small profile of the injection needle and the “blind” nature of endocardial delivery, as previously discussed.
20
Additionally, therapies of this nature require numerous injections (9–26 injections
21
) to distribute the therapy to various regions of the infarct. For these reasons, it is important to understand the design requirements of minimally invasive catheter delivery in relation to viscous materials/hydrogels. In this study, we developed a minimally invasive endocardial catheter AMCath (
Materials and methods
Design features of AMCath
AMCath, a minimally invasive endocardial catheter for the delivery of fast-gelling HA, was developed in this study as partially described in the patent application 15715054. 22 The full assembly is shown in Figure 1(a). The device consists of:

AMCath – The inner component (a), the outer sheath (b), the handle (c) and the adapter housing (d) of the catheter described in Section Design features of AMCath. AMCath: advanced materials catheter.
Inner component: 1.2 m of dual-lumen tubing (outer diameter 1.5 mm), each lumen having an inner diameter of 0.5 mm, which is connected to a 5 µL reservoir at the distal tip. A needle (diameter 0.24 mm ± 0.01) is connected to distal tip of the reservoir. The hydrogel precursor solutions pass through the individual lumens and mix in the reservoir (cross-linking reaction initiated) before being ejected through the needle.
Outer sheath: An Oscor deflectable sheath (Oscor Destino Twist® Deflectable Steerable Guiding Sheath, 6.5 French and 9 mm curve configuration), which can be actuated to 180°, is the main component of the outer sheath, allowing the device to be steerable and deflectable. This is connected to a tip (Figure 1(b)) comprising a PTFE insert attached to the distal end of the Oscor sheath to allow for the needle to be retracted.
Handle: The primary function of the handle is to extend/retract the needle a specified distance. It consists of several parts as in Figure 1(c). A torque lock at the top prevents the dual-lumen inner component from slipping and is fixed to the cap. The cap actuates up and down and locks to a threaded trigger mechanism that controls the extent of the caps actuation. This can be user-defined by manipulating the dial at the centre of the device. A spring near the base of the device allows the cap to return to its starting position when the trigger is released. A torque lock at the bottom of the catheter anchors the PTFE sheath that passes through the Oscor sheath.
Adapter housing in Figure 1(d) allows a simple assembly and activation of the syringes containing the precursor solutions.
HA-PH-RGD hydrogel preparation
HA-PH-RGD (60–90 kDa) as described in the Supplemental Material was rehydrated in phosphate-buffered saline (PBS) (pH 7.4) on a rocker (Stuart, SRT9D) overnight to form a 2% w/v solution. The polymer solution was cross-linked using HRP and H2O2. HRP powder was dissolved in 0.1% bovine serum albumin (BSA) in PBS at 8 U/mL and vortexed to form a stock solution which was stored at –20°C; 0.1% (w/w) H2O2 solution was prepared fresh for every use.
To prepare hydrogels, the 2% HA-PH-RGD solution was divided equally into two separate vials, which are referred to as hydrogel precursor solutions part A and part B. To part A, HRP stock solution was added dependent on the required cross-linking concentration of the final hydrogel, see Table 1. Similarly, 0.1% H2O2 solution as shown in Table 1 was added to part B. Parts A and B were agitated on a rocker for 2 min to ensure a homogenous solution. Each solution was drawn into a separate syringe and attached to AMCath (Figure 1) or the laboratory scale benchtop hydrogel mixer (BHM) (Contipro, Czech Republic), as shown in Figure 2. The syringes were depressed in parallel and parts A and B were forced into contact at the reservoir of either the BHM or AMCath. A key feature of the BHM is the presence of a static mixer in the reservoir which ensures mixing of precursor solutions and results in homogenous gelation. This static mixer is not present in the reservoir of AMCath due to the size constraints of minimally invasive catheters. Hydrogels were injected into custom-built polytetrafluoroethylene (PTFE) moulds (8 mm diameter, 4 mm height) and left for 1 min to ensure complete cross-linking. Hydrogels were left for 30 min before measuring the mechanical and viscoelastic properties.
Concentration and activity of cross-linking agents.
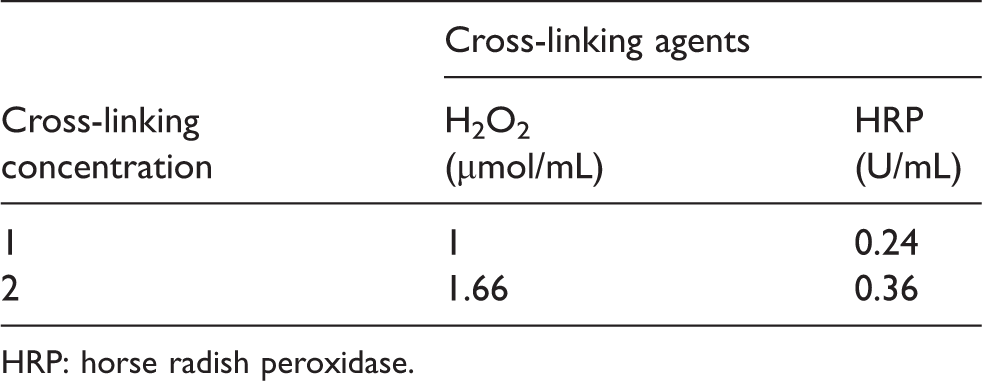
HRP: horse radish peroxidase.
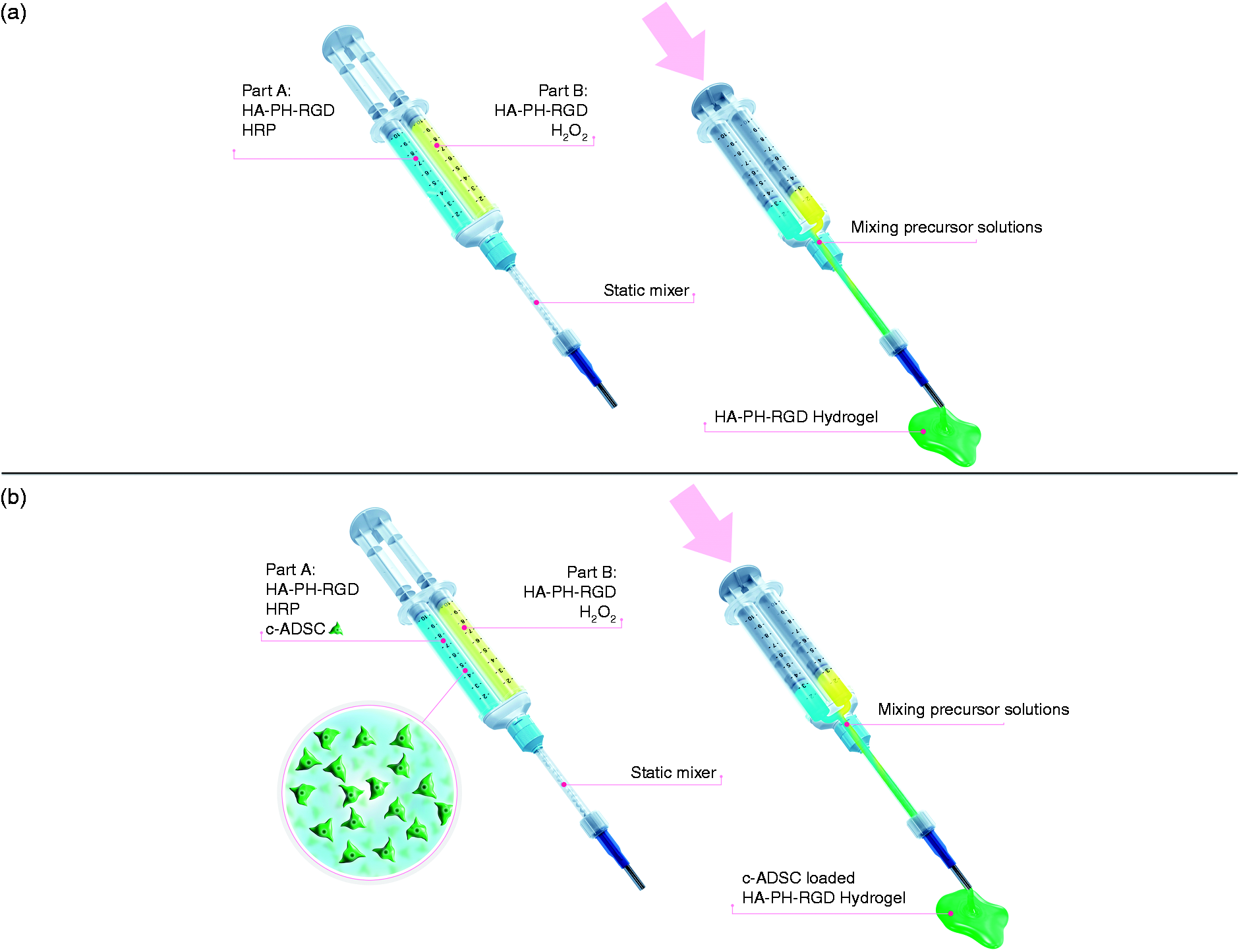
HA-PH-RGD hydrogel preparation using benchtop hydrogel mixer – The components and precursor solutions used to prepare (a) the HA-PH-RGD and (b) c-ADSC-loaded HA-PH-RGD hydrogels. HA: hyaluronic acid; c-ADSC: cardiopoietic adipose-derived stem cell.
Hydrogel gelation time, viscosity and mechanical properties are directly related to the degree of cross-linking. Two cross-linking concentrations were investigated for this study. Cross-linking concentration 1 from Table 1 was used when no cells were present, while cross-linking concentration 2 was used when 20 million cardiopoietic adipose-derived stem cell (c-ADSCs)/mL were encapsulated (Section Human c-ADSC encapsulation in HA-PH-RGD hydrogels). No cytotoxic effects were associated with the cross-linking concentrations used in this study as measured using CellTiter-Glo assay (Promega, USA) (data not shown).
Injectability
The force required to inject the hydrogel precursor solutions through AMCath (gelation is initiated in reservoir at distal tip of AMCath) was investigated as previously described. 23 Briefly, 200 µL of precursor solutions using cross-linking concentration 1 (Table 1) was injected through AMCath. A Zwick mechanical testing machine (Z050, Zwick/Roell) with a 5 kN load cell was used to apply a constant feed-rate, corresponding to 200 µL/12 s, to the plunger of the syringe. The plunger was attached to the load cell using a custom-built adapter. The maximum force per injection was recorded (n = 3).
Viscoelastic and mechanical characterisation of HA-PH-RGD hydrogels
Kinetics of gelation of HA-PH-RGD hydrogels
Gelation was measured on an AR-G2 Rheometer (TA Instruments) using a parallel plate (40 mm) geometry and 400 µm gap. 525 µL of precursor solution was added to the plate and pre-shear 2000 1/s for 1 s was used to homogenise the solutions. An oscillation time sweep at a frequency of 1 Hz and displacement 0.001 radian was performed at 37°C (n = 5). Information regarding the properties of the HA-PH-RGD hydrogel can be found in Supplemental Figures 8, 9 and 10, where we show the viscosity as a function of shear rate, zero rate viscosity of 0.4 Pa.S, gelation time of 19 s and the gelation curve of 2% HA-PH-RGD (60–90 kDa).
Hydrogel viscoelastic and mechanical properties
Rheological properties of the hydrogels were measured by an AR-G2 Rheometer (TA Instruments) using a cross-hatched surface geometry to avoid slippage of hydrogel. A strain sweep test with frequency of 1 Hz and a displacement range of 10−3 to 2 radians was performed (n = 5).
The mechanical properties of the hydrogels were measured using a Single Column Materials Testing System (INSTRON3342) in compression. The capacity of this device is 500 N and the capacity of compression platen is 100 N. The testing speed was set to 2 mm/min. 400 μL hydrogels were used for these experiments; the diameter of the hydrogels was 11.1 mm corresponding to the diameter of the moulds, the height of the hydrogels were measured to be 4 ± 0.5 mm. The compressive modulus was determined as the slope between 0 and 10% strain of the resulting stress–strain curve (n = 5). Toughness was determined as an area under the stress–strain curve per unit volume (n = 5).
Swelling ratio of hydrogels
200 μL hydrogels were weighed immediately after preparation, placed into 3 mL of PBS at 37°C for 24 h and weighed. Swelling ratio was calculated from ratio of weight after and before swelling (n = 5).
Preliminary assessment of in vivo feasibility of AMCath
A 90 kg pig (Landrace, female) was used to test the feasibility of AMCath. Ethical approval was obtained preceding in vivo assessment (Ethics approval No. 904/2015-PR). Prior to the procedure, the thickness of the LV wall was estimated and the extended needle length was adjusted to half the thickness, and the injection lumen of the catheter were primed with HA-PH-RGD without cross-linkers. The abdominal aortic access point was prepared by a 14 F introducer (Boston Scientific) and the device was inserted through the sheath. Under fluoroscopic guidance AMCath was slowly advanced through the abdominal aorta, the aortic arch and then placed into the LV. Once the desired site of injection was attained, the syringes containing the precursor solutions were attached to the proximal end of AMCath. The needle was extended and locked into position. Needle anchoring was confirmed via X-ray and a successful penetration of the myocardium was indicated in ECG by the occurrence of premature ventricular contractions. The precursor solutions were injected through AMCath at 200 µL/12 s. The needle was kept in position for 30 s to ensure gelation. Three 200 µL injections were made 20 min before the animal was euthanised by IV injection of Tanax (0.3 mL/kg BW). The heart was excised, cut open for visual confirmation of needle puncture, frozen and a post-mortem MRI (Philips Achieva 3T) was used to confirm hydrogel presence within the LV wall. Conditions and pulse sequences of MRI are detailed in the Supplemental Material. Mimics (Materialise), image-processing software, was employed to generate three-dimensional volumes of hydrogel injections. MRI dicom files were imported into Mimics and thresholded (350–555 in the unit of gray value (GV)) to segment the hydrogel bolus from the surrounding myocardium.
Human c-ADSC encapsulation in HA-PH-RGD hydrogels
To investigate the potential of using AMCath to deliver cell-loaded hydrogels, ADSCs were included HA-PH-RGD hydrogels. ADSCs were chosen for this study as human adipose tissue is distributed throughout the body and is routinely discarded during liposuction and other cosmetic surgery, making it an ideal inexpensive source of mesenchymal stem cells. It can be harvested in large quantities and has been shown to contain more stem cells than bone marrow,6 making it an ideal source of starting material for an allogeneic product. ADSC isolation and culture description is available in the Supplemental Material. Following ADSC expansion and priming towards the cardiovascular phenotype (c-ADSCs), the cells were stored in liquid nitrogen until use. Lineage specification was confirmed on cryopreserved samples by immunofluorescence to confirm the nuclear expression of MEF2C (Supplemental Figure 12). c-ADSCs were incorporated into part A (HA-PH-RGD + HRP) at 40 million cells/mL (Figure 2(b)) resulting in a final cell concentration of 20 million c-ADSCs/mL of HA-PH-RGD hydrogel. This density was chosen to maximise the number of cells delivered while minimising the number of injections required per patient.
c-ADSC viability after prolonged incubation in HA-PH-RGD + HRP precursor solution
The effect of prolonged incubation of cells in HA-PH-RGD + HRP precursor solution was investigated. This situation may arise in the clinical environment if a delay occurs during the procedure. c-ADSCs were maintained in 2 mL of part A (HA-PH-RGD+HRP) at 40 million cells/mL for up to 7 h at room temperature or 4°C. Samples were diluted in culture medium and seeded on 24-well plates at 1 × 104 cells/mL/well at each time-point. Cell viability was measured 24 and 48 h after seeding using Cell-titre Glo assay (Promega). Wells were rinsed before 125 µL PBS and 25 µL of CellTiter-Glo reagent was added. Plates were incubated for 15 min on orbital shaker at 250 r/min, protected from light. The plate was removed from shaker and incubated for 15 min. Luminescence was read on fluorescent reader TECAN Infinite 200.
c-ADSC viability after HA-PH-RGD hydrogel preparation
To appraise the effect of injecting the cells through AMCath, c-ADSCs were incorporated into HA-PH-RGD + HRP precursor solution and 200 µL hydrogels were prepared (as described in Section HA-PH-RGD hydrogel preparation) using AMCath (1.2 m in length), see Figure 1)) and the BHM (0.04 m in length), see Figure 2. Hydrogels were then placed in 2 mL of complete c-ADSC medium and incubated under normal growth conditions: 37°C, 5% CO2 and 90% humidity; 24 and 48 h post-preparation hydrogels were stained (n = 3) with LIVE/DEAD® Viability/Cytotoxicity Kit (BioScience Ltd.) and incubated for 30 min protected from light. Samples were imaged by confocal laser scanning microscopy (Carl Zeiss LSM710) using Zen®2008 software to generate image mosaics at ×100. Image analysis and quantification were performed using CellProfiler software. 24 Live or dead cells were identified using an automated global two-class Otsu thresholding and quantified. FIJI software was used for image preparation. 25
c-ADSC metabolic activity after HA-PH-RGD hydrogel preparation
Metabolic activity was measured with alamar blue reagent (Invitrogen) as described previously. 26 Briefly, 24 and 48 h post-preparation 10% (v/v) alamar blue was added to the culture medium of each hydrogel (n = 3) and incubated for 3 h protected from light. Absorbance of the cell-conditioned alamar blue was measured at 560 nm using 590 nm as excitation wavelength (Varioskan flash spectrophotometer).
Statistical analysis
For comparison of two samples a paired student’s t-test was performed (significant p < 0.05). Data are expressed as mean ± standard deviation.
Results
Injectability and gelation of HA-PH-RGD hydrogels
The force required to inject the hydrogel precursor solutions through AMCath remained below the maximum male and female pinch strength (70 N and 50 N, respectively).23,27 The force increased up to 3 min between each injection, and then became constant at ∼43 N, Figure 3(a). At this point, the polymerised hydrogel in the AMCath reservoir resulted in slightly higher injection forces to inject the material. If >3 min passed between each injection the polymerised hydrogel could still be ejected from AMCath with <50 N force (female pinch strength23,27) due to the small size profile of the reservoir. This result is in agreement with the gelation curve which shows that gelation occurs between 0 and 3 min, Figure 3(b). This result also informed our injection procedure described in Section Preliminary assessment of in vivo feasibility of AMCath whereby the needle was kept in position after each injection for 30 s to ensure gelation was initiated.
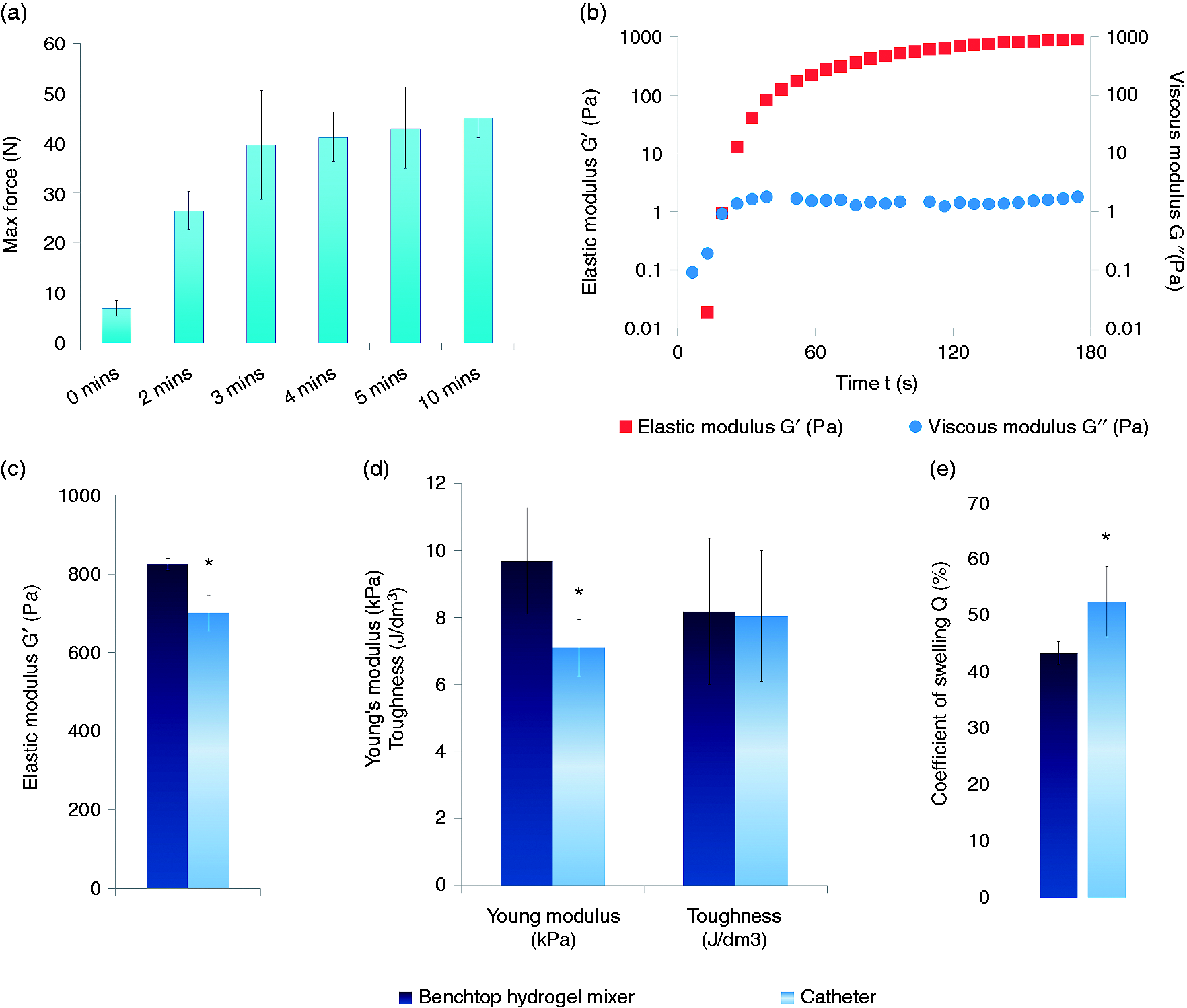
Characterisation of HA-PH-RGD hydrogels – (a) Injection force and (b) Gelation curve of HA-PH-RGD hydrogel at cross-linking concentration 1, (c) elastic modulus, (d) Young’s modulus and toughness and (e) swellability of HA-PH-RGD hydrogel at cross-linking concentration 1 prepared by BHM and AMCath. BHM: benchtop hydrogel mixer; AMCath: advanced materials catheter.
Injection through AMCath reduced the properties of HA-PH-RGD hydrogels
There were statistical differences between the elastic modulus (825 versus 701 Pa, p = 0.0002), Young’s modulus (9.7 versus 7.7 kPa, p = 0.0007) and swelling coefficient (43.3 versus 52.5% p = 0.0077) for the hydrogels prepared by the BHM compared to AMCath, no significant difference was observed in the toughness (8.2 versus 8.0 J/dm3), Figure 3(c to e).
Preliminary assessment of in vivo feasibility of AMCath
Under fluoroscopic guidance AMCath was advanced to the aortic arch and into the LV by abdominal aortic access, see Figure 4(a to f). This site was chosen due to a length restriction in the AMCath prototype, ordinarily femoral access would be preferred. Once in place in the LV, the hydrogel was successfully injected into the LV wall as demonstrated by MIMICs reconstruction of the hydrogel bolus’ from MRI dicom files, Figures 4(g) and (h).
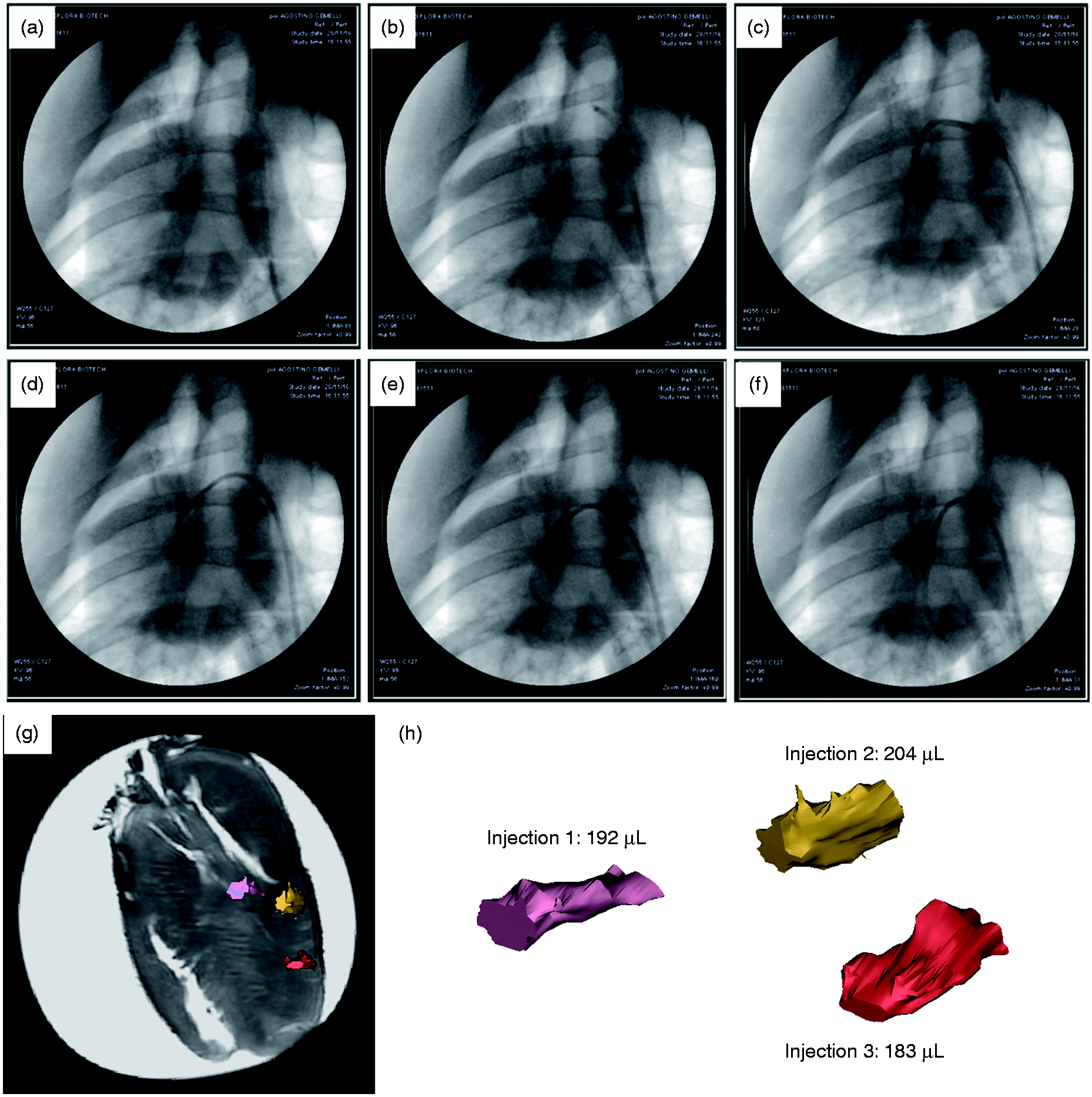
Preliminary In vivo Feasibility of AMCath – AMCath was advanced into the abdominal and the descending aorta (a and b), through the aortic arch (c) and mitral valve (d) into the LV (e). The device was positioned to the target site of injection (f). Mimics reconstruction and segmentation of three injections (200 μL delivered) from MRI dicom files measuring 192, 204 and 183 μL (g and h). AMCath: advanced materials catheter; LV: left ventricle.
AMCath can also deliver c-ADSC-loaded HA-PH-RGD hydrogels
Increasing the cross-linking concentration when 20 million c-ADSCs/mL is present maintains the mechanical properties
The inclusion of a high density of cells physically interfered with this cross-linking reaction reducing the mechanical properties of the hydrogel. There was a statistical reduction in the Young’s modulus in the hydrogels prepared at cross-linking concentration 1 (see Table 1) with the BHM without and with 20 million c-ADSCs/mL (9.7 versus 5.6 kPa, p < 0.05). There was a statistical reduction in the Young’s modulus in the hydrogels prepared at cross-linking concentration 2 (see Table 1) prepared with the BHM without and with 20 million c-ADSCs/mL (12.6 versus 8.6 kPa, p < 0.05). However, there was no statistical difference in the Young’s modulus of the hydrogels prepared at cross-linking concentration 1 without cells and at cross-linking concentration 2 with 20 million c-ADSCs/mL, see Figure 5(a). To maintain the hydrogel mechanical properties when 20 million cells/mL were incorporated cross-linking concentration 2 was used.
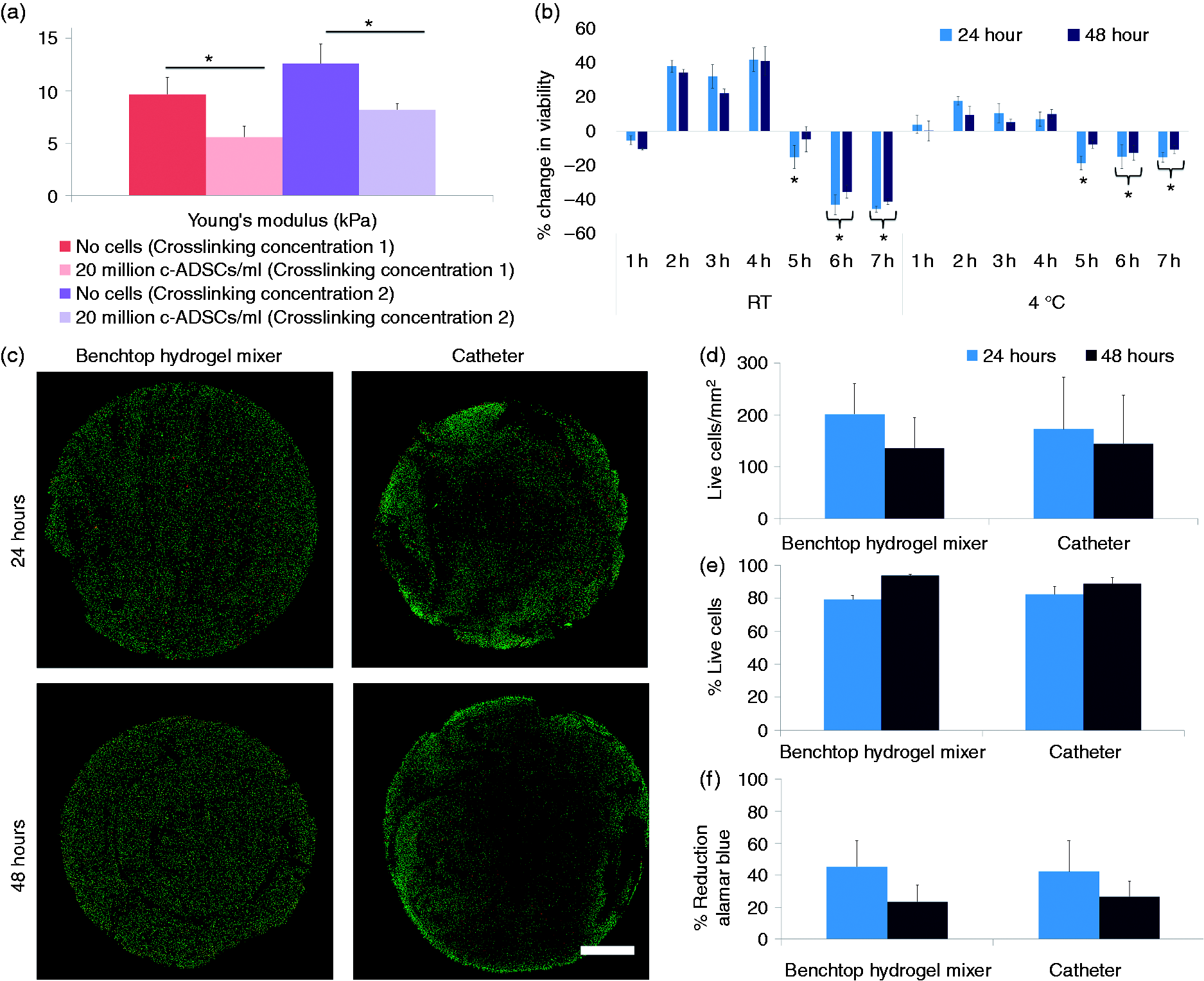
Viability of encapsulated c-ADSC – (a) Young’s modulus of HA-PH-RGD hydrogel prepared with BHM with/out 20 million cells/mL at cross-linking concentrations 1 and 2. (b) Prolonged incubation of c-ADSCs in HA-PH-RGD + HRP precursor solution, (c) confocal scans (scale bar = 1 mm), (d) number and (e) percentage of live cells and (f) metabolic activity of 20 million c-ADSCs/mL of HA-PH-RGD. BHM: benchtop hydrogel mixer.
c-ADSC viability was not affected by 4 h incubation in HA-PH-RGD+HRP precursor solution
There was no significant loss to cell viability when 40 million c-ADSCs cells/mL were stored in HA-PH-RGD + HRP precursor solution for 4 h, while a significant decrease was seen for storage longer than 4 h (p < 0.05), independent of the storage temperature, see Figure 5(b). Based on these results the authors advise that the c-ADSC loaded HA-PH-RGD + HRP precursor solution should be injected ≤4 h after preparation.
c-ADSC viability and metabolic activity was not affected by injection through AMCath
Representative confocal images of the cross-sectional area of the cell-loaded hydrogels can be seen clearly in Figure 5(c). No significant difference was seen in cell viability or metabolic activity in the hydrogels injected through AMCath compared to the BHM, Figure 5(d) to (f). Additionally, % c-ADSC viability remained above the acceptable viability specification, which is generally set at 70% as outlined by the FDA. 28
Discussion
We have successfully developed and tested an endocardial minimally invasive catheter (AMCath) which enables the delivery of a fast-gelling covalently cross-linked HA hydrogel to beating myocardial tissue and as such shown an advancement in the field. The preliminary in vivo feasibility of AMCath was demonstrated by accessing the LV of a pig by means of abdominal aortic access. We have shown that the hydrogel was retained in the myocardium, thus demonstrating efficacy of AMCath to deliver and retain the therapy to the target location; moreover, there were no adverse events observed. Furthermore, AMCath enables us to inject the fast-gelling hydrogel with a low force ∼43 N (<female pinch strength 27 ). The mechanical properties of the hydrogels were reduced by AMCath showing differences to the BHM (825 versus 701 Pa); however, the hydrogels are still robust and within a similar range of epicardially delivered alternatives such as modified HA hydrogel described by Rodell et al. 10 (800 Pa) and alginate-based Algysil (3–5 kPa).4,5 Therefore, we have demonstrated preliminary in vivo feasibility of AMCath for the delivery of fast-gelling covalently cross-linked HA hydrogels.
In addition to this, we have shown that AMCath can deliver c-ADSC-loaded hydrogels with 80% of the delivered cells remaining viable 48 h after injection through AMCath. Here, we provide an alternative to cell delivery in saline (current clinical standard), by delivering cells in the protective support structure of the hydrogel, with the overall aim of improving cell survival and retention. A study published by our lab showed that incorporation of cells in biomaterials improved the efficacy and retention of cell delivery compared to cells delivered in saline. 15 In the current study, we have incorporated 20 million cells/mL (4 million cells/200 µL injection). The recent C-Cure clinical trial for cell delivery in saline required 10–20 injections to deliver the desired cell dose of 600 million cells, whereby 2–25% retention has been reported.13,21 Therefore, if 10–20 injections of our hydrogel at 20 million cells/mL are made to the myocardium, the cell dose delivered will be 40–80 million cells. As hydrogels can help keep cells localised and viable, this delivered cell dose may result in a much higher number of healthy cells available to regenerate local tissue and thus overcome the problems associated with previously reported saline studies. A limitation of this study is that AMCath was advanced into the LV by abdominal aortic access. This site was chosen due to a length restriction in the AMCath prototype, ordinarily femoral access would be preferred. The outer sheath used to make the AMCath device steerable and deflectable had a usable length of 90 cm which caused the length restriction in this study. The length restriction can be overcome easily by using a longer custom sheath.
Hydrogel formation parameters inform the design of delivery devices and vice versa, therefore it is difficult to design a catheter that is compatible with a range of different hydrogels. This may indeed be the reason for the lag in developments in minimally invasive delivery for biomaterials. In the case of covalently cross-linked hydrogels, as presented here, gelation time is an important factor. The solution must gel rapidly at the site of injection in order to retain the therapy at the desired site, while premature gelation may block the catheter, rendering the therapeutic and catheter unusable, thus preventing covalent cross-linked hydrogels from being delivered percutaneously. Injectability of the material through the catheter is directly related to the gelation time and is an important feature to consider when designing a delivery device. To simultaneously address the need for rapid gelation, injectable delivery and cytocompatibility, we have engineered a catheter that allows covalent cross-linking at the proximal end of the catheter. This reduces embolisation risk and allows final gelation to occur in situ. We have shown that it is possible to inject our hydrogel with a low force. Furthermore, we have shown that injection through AMCath did not affect the viability of the c-ADSCs encapsulated within the hydrogel. This is the crux of the catheter described in this study – the reservoir located at the distal tip of AMCath has been minimised to reduce the force required to inject the hydrogel once gelled but also allows the precursor solutions to form a robust cell-loaded hydrogel as shown. We have shown that this design is effective to deliver a hydrogel with a Young’s modulus of ∼9 kPa and low-viscosity precursor solutions (zero rate viscosity 0.4 Pa.S). However, we predict that it may not be appropriate for hydrogels with a higher Young’s modulus and higher viscosity precursor solutions. We predict that the force required to inject more robust fully polymerised hydrogel will increase above 50 N force (female pinch strength), depending on the properties of the hydrogel. Additionally, the reservoir may not provide sufficient mixing for more viscous precursor solutions. In this case, a small profile static mixer may need to be included in the reservoir. This clearly demonstrates that it is difficult to design a catheter that is compatible with a range of different hydrogels as hydrogel formation parameters must inform the design of delivery devices and vice versa. The catheter solution we describe in this manuscript allows these scalable hydrogels to be used in a clinical context and within the current clinical treatment paradigm, and demonstrates a true inter-disciplinary approach to overcoming translational challenges.
Conclusion
In this study, we have demonstrated that a carefully chosen covalently cross-linkable cell-embedded biomaterial can be successfully delivered using a 1.2 m length, small lumen catheter technology. In these experiments, the biomaterial maintains appropriate physical properties, viable cells and does not possess any properties that inhibit successful material delivery – such as too high injection forces or blockages of the catheter lumen. Furthermore, the AMCath device was successfully used in a large animal experiment and we demonstrated that the hydrogel could be delivered and was retained in the myocardium of a beating heart. In summary, these experiments demonstrate that careful biomaterial choices and parallel catheter design activities can result in a potentially new clinical strategy to repair damaged myocardium.
Supplemental Material
Supplemental material for A dvanced M aterial Cath eter (AMCath), a minimally invasive endocardial catheter for the delivery of fast-gelling covalently cross-linked hyaluronic acid hydrogels
Supplemental material for
Footnotes
Declaration of Conflicting Interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LK, MP, IS and RS are employed by Contipro. VV is the owner of Contipro. DD and NB are employed by Celyad. GB and SS are employed by Explora Biotech. AF is employed by Boston Scientific. All companies are members of the AMCARE consortium.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AMCARE consortium (FP7/2007-2013) under Grant Agreement No.604531.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.