
Abstract
The aim of the in vitro study was a comparison of an allogenic (ABSM) and a xenogenic bone substitute material (XBSM) with and without injectable platelet-rich fibrin (ABSM-i-PRF & XBSM-i-PRF) on cell characteristics of human osteoblasts (HOB). Here, ABSM and XBSM (+ i-PRF = test; - i-PRF = control) were incubated with HOB for 3, 7 and 10 days. HOB viability, migration, proliferation and differentiation (RT-PCR on alkaline phosphatase (AP), bone morphogenetic protein 2 (BMP-2) and osteonectin (OCN)) were measured and compared between groups. At day 3, an increased viability, migration and proliferation was seen for ABSM-i-PRF. For viability and proliferation (days 7 and 10) and for migration (day 10), ABSM-i-PRF/XBSM-i-PRF showed higher values compared to ABSM/XBSM with maximum values for ABSM-i-PRF and minimum values for XBSM. At days 3 and 7, the highest expression of AP was detected in ABSM-i-PRF/XBSM-i-PRF when compared to ABSM/XBSM, whereas at day 10, AP expression levels were elevated in ABSM-i-PRF/ABSM. The highest BMP-2 expression was seen in ABSM-i-PRF whereas OCN expression showed higher levels in ABSM-i-PRF/XBSM-i-PRF at days 3 and 7 with lowest expression for ABSM. Later on, elevated OC levels were detected for ABSM-i-PRF only. In conclusion, i-PRF in combination with ABSM enhances HOB activity when compared to XBSM-i-PRF or untreated BSM in vitro. Therefore, addition of i-PRF to ABSM and – to a lower extent – to XBSM may influence osteoblast activity in vivo.
Keywords
Introduction
For osseous regeneration, autologous bone is considered to be the biological gold standard in regard of its osteogenic, osteoconductive and osteoinductive properties. Whether or not autologous bone can be considered as the clinical gold standard in all cases can be discussed controversially as it entails a number of limitations, i.e. the need for an additional operative donor site with a higher morbidity and sometimes rapid resorption of the grafts. A clinical alternative to autologous bone may represent bone substitute materials (BSM) that are widely used in regenerative medicine as a valid approach for osseous reconstruction and each BSM has its advantages as well as limitations and disadvantages. Most frequently used BSM are of allogenic (ABSM), xenogenic (XBSM), or synthetic origin.1,2 For XBSM, mostly of bovine origin, the main effects – osteoconduction and a low absorbability rate – were described in detail. 3 It was also reported that a biomimetic modified xenograft could enhance angiogenesis and osteogenesis. 4 Mardinger et al. stated that xenografts have almost no changes or no changes in bone height in comparison to autogenous bone or a combination of both. 5 For ABSM, in addition to its unlimited availability, the possibility of patient-specific customization and its biocompatibility as well as decent osteoinductive properties are reported. 6
To enhance tissue regeneration, autologous platelet concentrates have been developed and successfully used in the clinical setting.7,8 Besides, platelets were found to enhance bone healing in healing-impaired cases by promoting early cellular proliferation leading to better qualitatively and quantitatively bone formation.9,10 Here, platelet-rich plasma (PRP) has been produced using a specific centrifugation protocol together with anti-coagulants. A number of studies reported a positive effect of PRP in combination with BSM on human osteoblasts (HOB) in vitro;11,12 however, others contradict it.13–15 Additionally, regenerative capacity of PRP was reported to be short and anti-coagulants needed for preparation of PRP seemed to inhibit wound healing processes.14,16,17
Platelet-rich fibrin (PRF) is a leucocyte- and platelet-rich fibrin matrix, a further development of PRP and therefore second generation of platelet concentrates as proposed by Choukroun et al. 18 Specific centrifugation pattern after blood harvest from a 10 ml blood sample enables PRF to build up a three-dimensional matrix of platelets and leukocytes. 19 Due to the fibrin component, PRF acts as a scaffold that triggers cell–cell contacts and proliferation. 20 Besides, PRF does not dissolve quickly after application that favors a gradual release of growth factors 21 for at least seven days. 22
Subsequently, the suitability of PRF as a biologically active scaffold has been illustrated proving a higher proliferation and differentiation rate of HOB and gingival fibroblasts.23–25 There is also emerging evidence that PRF may increase HOB migration and proliferation in vitro.18,23,26 Additionally, it has been demonstrated that PRF promotes angiogenesis. 27 Furthermore, among its advantages are also simple preparation without blood modification, ease of handling, and minimal expense. 28 Patients’ blood is collected through venipuncture and immediately centrifuged without addition of an anticoagulant, carrier, or activator, 29 leading to activation of the physiological coagulation cascade.30,31
Recently, a lower centrifugation protocol of PRF production, so called injectable-PRF (i-PRF) was developed. 32 I-PRF remains liquid for approximately 15 min. After application, it immediately coagulates into a PRF clot rich with blood-derived growth factors, which constantly release over 10–14 days. 33 I-PRF has advantage in higher number of leukocyte as far as it favors more growth factor release and thus tissue wound healing. 34 Although i-PRF is widely used alone and as a carrier for variety of biomolecules in medicine, its potential in combination with variety biomaterials still lacks scientific evidence. 35
Angiogenesis and osteogenesis are coupled in the process of osteogenesis. 36 BSM are routinely used in maxillofacial surgery as a valid alternative to the autologous bone as the gold standard when bone is lost due to trauma, cancer, or other pathologies. 37 Therefore, the combination of BSM with platelet concentrates such as i-PRF may represent a clinical pathway to enhance angiogenesis and therefore bone repair.
Therefore, the aim of this preclinical in vitro study was to compare the effect of allogenic and xenogenic BSM with and without additional i-PRF on HOB viability, attachment, proliferation, and differentiation. The null hypothesis was that allogenic and xenogenic BSM in combination with i-PRF may improve proliferation, cell attachment and differentiation of osteoblasts when compared to both BSM without i-PRF.
Materials and methods
In the current study, allogenic (ABSM; maxgrаft
A commercially available human osteoblast cell line (HOB, PromoCell, Heidelberg, Germany) was applied. For cultivation, a standard HOB medium was administered, which contained fetal calf serum (FCS, Gibco Invitrogen, Karlsruhe, Germany), Dulbecco’s modified Eagle’s medium (DMEM, Gibco Invitrogen), dexamethasone (100 nmol/l, Serva Bioproducts, Heidelberg, Germany), L-glutamine (Gibco Invitrogen), and streptomycin (100 mg/ml, Gibco Invitrogen). Cultivation of HOB was conducted at 37°C in a constant, humidified atmosphere with 95% room air and 5% CO2. The passaging of HOB was conducted on demand of their growth state (70% confluence), using 0.25% trypsin (Seromed Biochrom KG, Berlin, Germany).
Peripheral blood was collected from healthy laboratory members involved in this study (free of infectious diseases, without recent alcohol or nicotine consume; informed consent was signed following the consultation of the local ethics committee) into 10 ml i-PRF plain vacuum tubes (i‐PRF tubes, Process for PRF, Nice, France) and immediately centrifuged at 700 r/min for 3 min at room temperature using the Duo centrifuge (Duo Zentrifuge; Mectron, Cologne, Germany). The upper liquid layer was collected being i-PRF. 33
HOB at passage five were seeded in a density of 5 × 104 cells per well. Immediately after the seeding, 100 mg of ABSM and 100 mg of XBSM were incubated with 150 µl of i-PRF to each sample and added to the HOB. HOB with each of the two BSM without i-PRF served as the control groups. Compositions were incubated 3, 7 and 10 days at 37°C in a constant, humidified atmosphere with 95% room air and 5% CO2. A minimum of three replications of each test was carried out.
Cell viability
To visualize cell viability, cells were stained after 3, 7 and 10 days with CellTracker (Life Technologies, Thermo Fisher Scientific, Darmstadt, Germany; catalog number: C34552). Red dye was prepared according to the manufacturer’s instructions. Culture media was removed, warmed Red dye was added and plates were incubated for 30 min (37°C). After removal of the dye, serum-free medium was added and incubated for 30 min (37°C). Red fluorescence was detected with a fluorescence BZ-9000 microscope (Keyence, Osaka, Japan). Quantification of cells was conducted by ImageJ software (ACTREC, Navi Mumbai, India) as previously described. 38 In brief, images (magnification 10×) were converted to grayscale. The correction of background was conducted through image subtraction. Cell structures were extracted from the background by automatic thresholding and the area fraction (%) was calculated. Measures were made in triplication per sample (n = 3 for each group and each time point, three time points).
Cell migration
Cell attachment was studied by scratch test (ST). In brief, a scratch was manually applied to the bottom surface of the wells with a p200 pipet tip (Gilson, Middleton, USA) at days 3, 7, and 10 of incubation as described in the literature. 39 One day after ST, red staining with CellTracker was applied as described above. Quantification of cells migrated in the gap was conducted using ImageJ software in 10× fold magnification on digitalized images by means of percent area (%). 38 Selected area fraction of each image was customized according to the gap of their equivalent image on the first day of scratch. To compare results, all numbers were adjusted to an area of 100 square pixels. The measurements were carried out in triplication per group (n = 3 for each group and each time point, three time points).
Cell proliferation
Assessment of cell proliferation was provided using 3–(4, 5-Dimethylthiazol-2 - yl)-2, 5- diphenyltetrazolium bromide (MTT) assay on days 3, 7, and 10. MTT (200 µL, 2 mg/mL) was added to the wells and incubated for 4 h at 37°C. Then, culture medium was discarded, and 10 ml lysis buffer was added per well. The plates were read at 570 nm by a fluorescence microplate reader (Versamax, Molecular Devices, San Jose, CA, USA). Measures were made in triplication for each group (n = 3 for each group and each time point, three time points).
Real-time quantitative PCR
Evaluation of the real-time quantitative PCR (qRT-PCR) activity of alkaline phosphatase (AP), bone morphogenic protein 2 (BMP-2), and osteocalcin (OCN) was implemented. Total RNA was extracted after days 3, 7, and 10 using a commercial kit (Qiagen, Hilden, Germany). RNA was converted to cDNA by iScript cDNA synthesis kit (BioRad, Hercules, USA) according to manufacturers’ instructions. Actin and GAPDH genes were used as an internal control for normalization. Primers in following sequence were applied:
Statistical analyses
The numeric results of the study were interpreted in mean values with the estimate of its standard error of the mean (SEM) and rounded to second decimal place. Data was checked on normal distribution applying Shapiro-Wilk test (SWT). In case of normally distributed values, two groups were compared via two-sided Student’s t-test for paired samples (t-test). In case of non-normal distributions, Mann–Whitney test (MWT) was used to compare two groups. In order to compare all groups, Kruskal–Wallis rank sum test (KWT) was applied. A p ≤ 0.05 was considered to be statistically descriptive significant. Bar charts with error bars were used for data illustration.
Results
Cell viability
At day 3, ABSM-i-PRF and ABSM showed the highest cell number (48.79 ± 1.56 and 15.96 ± 9.21, respectively) and the cell number on ABSM-i-PRF was distinctively higher when compared to both XBSM groups (p ≤ 0.001; Figure 1). In ABSM, significantly more viable cells were counted when compared to XBSM (p ≤ 0.05) and XBSM-i-PRF had significantly higher numbers when compared to XBSM (p ≤ 0.05). On days 7 and 10, a distinctively increased HOB growth could be observed in BSM-i-PRF- versus non-i-PRF BSM-groups (p ≤ 0.05). However, ABSM-i-PRF remained higher than XBSM-i-PRF at both time points (p > 0.05) as well as ABSM remained higher than XBSM (p ≤ 0.05). The values of ABSM-i-PRF were higher than those of XBSM during the whole period (p ≤ 0.001). In total, there was a significant difference among ABSM-i-PRF and XBSM groups on days 7 and 10 (p ≤ 0.05) (Figures 1 and 2; Table 1).
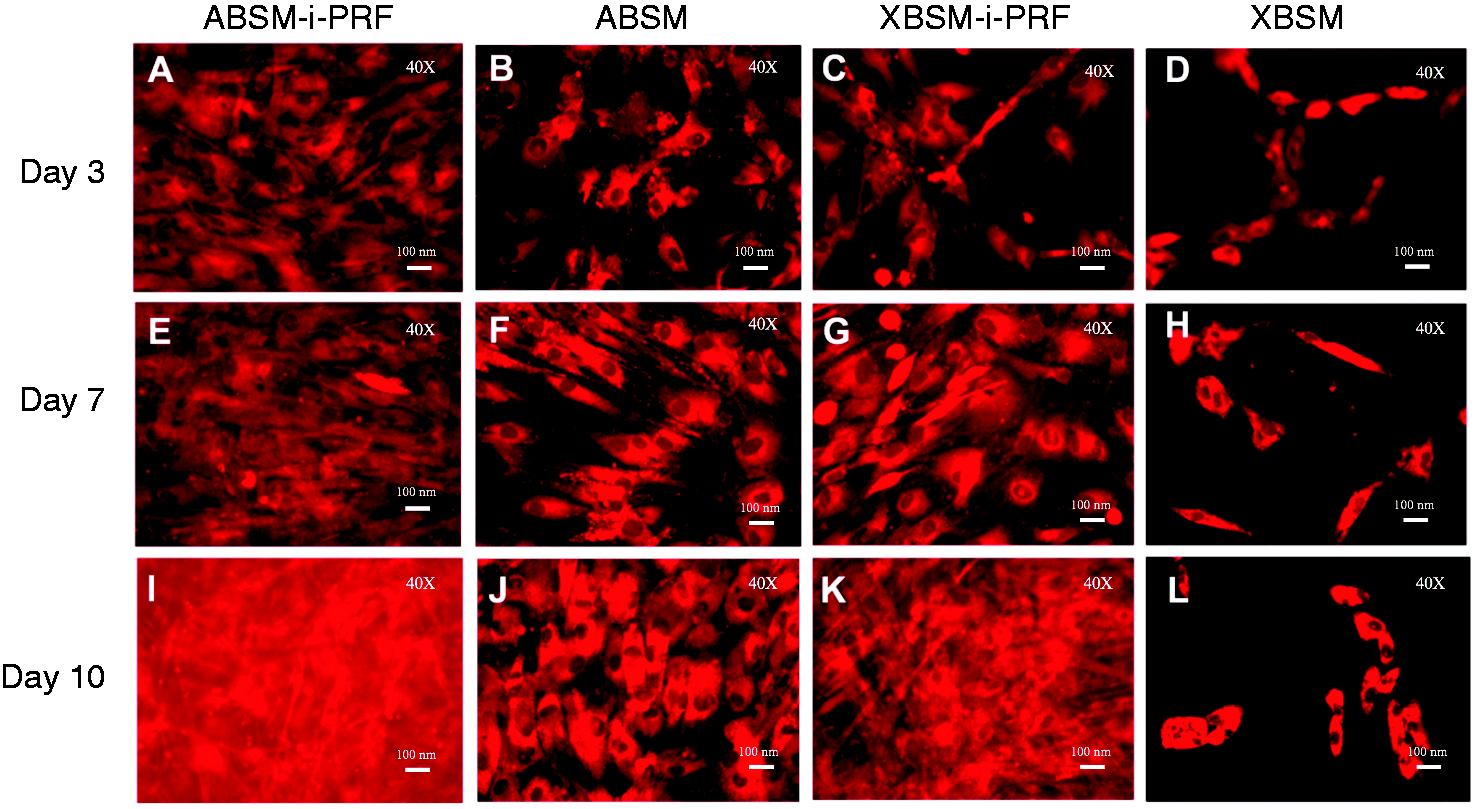
Exemplary figures of HOB viability (40×): ABSM-i-PRF (a, e, i), ABSM (b, f, j) as well as XBSM-i-PRF (c, g, k) and XBSM (d, h, l) on days 3, 7, and 10.
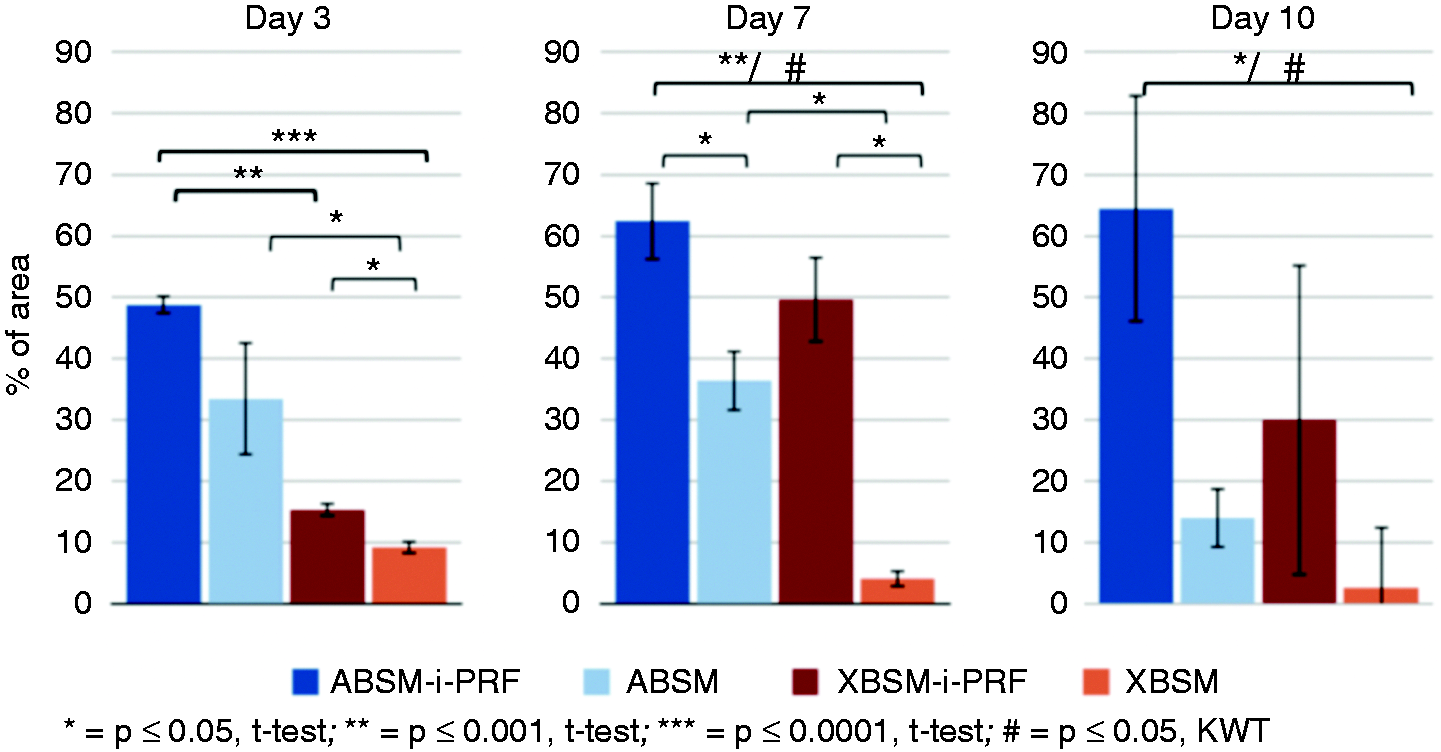
Bar charts: percent of viable HOB in comparison to the total area (software ImageJ (ACTREC, Navi Mumbai, India)); normal distributed variables of groups (ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM); mean values; error bars show SEM. n = 3 for each group and each time point, three time points.
Percentage of viable HOB in relation to the whole area; statistical significance by t-test when comparing the groups (ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM (normal distribution)) on days 3, 7, and 10; n = 3 for each group and each time point, three time points.
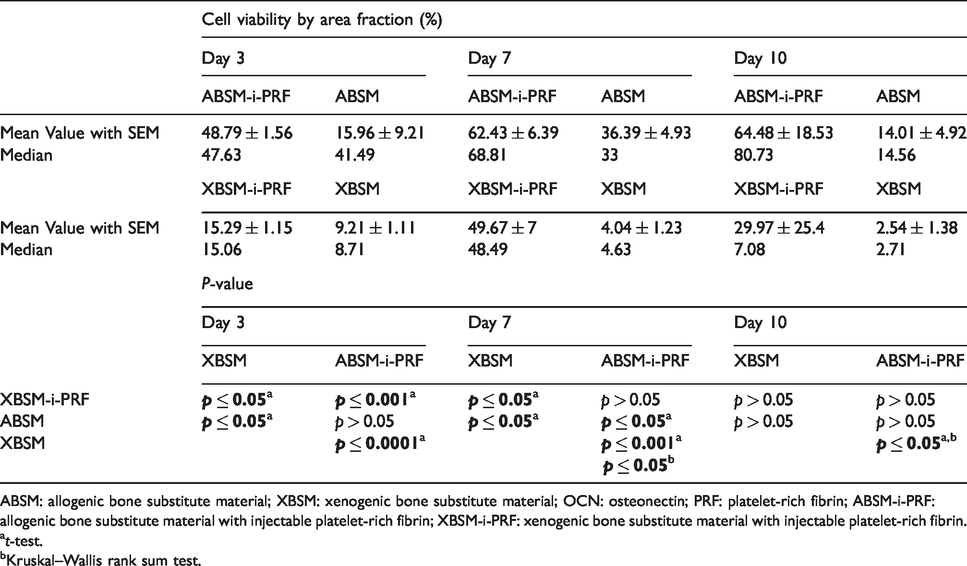
ABSM: allogenic bone substitute material; XBSM: xenogenic bone substitute material; OCN: osteonectin; PRF: platelet-rich fibrin; ABSM-i-PRF: allogenic bone substitute material with injectable platelet-rich fibrin; XBSM-i-PRF: xenogenic bone substitute material with injectable platelet-rich fibrin.
t-test.
Kruskal–Wallis rank sum test.
Cell migration
Concerning ST, extensive differences between the groups were detected. At day 3, closure of the gap was observed in all ABSM-i-PRF samples whereas no closure could be observed in the other groups (Figure 3). In accordance, the percentage of HOB in the gap of ABSM-i-PRF was almost doubled when compared to ABSM, XBSM-i-PRF and even more when compared to XBSM during the whole period (p > 0.05). At day 10, XBSM-i-PRF showed significantly higher values than XBSM (p ≤ 0.05). When compared to XBSM, ABSM also showed improved closure of the gap at all time points (p > 0.05). At days 1, 7 and 10, in ABSM-i-PRF were significantly more HOB within the gap when compared to XBSM (p > 0.05) (Figures 3 and 4; Table 2).
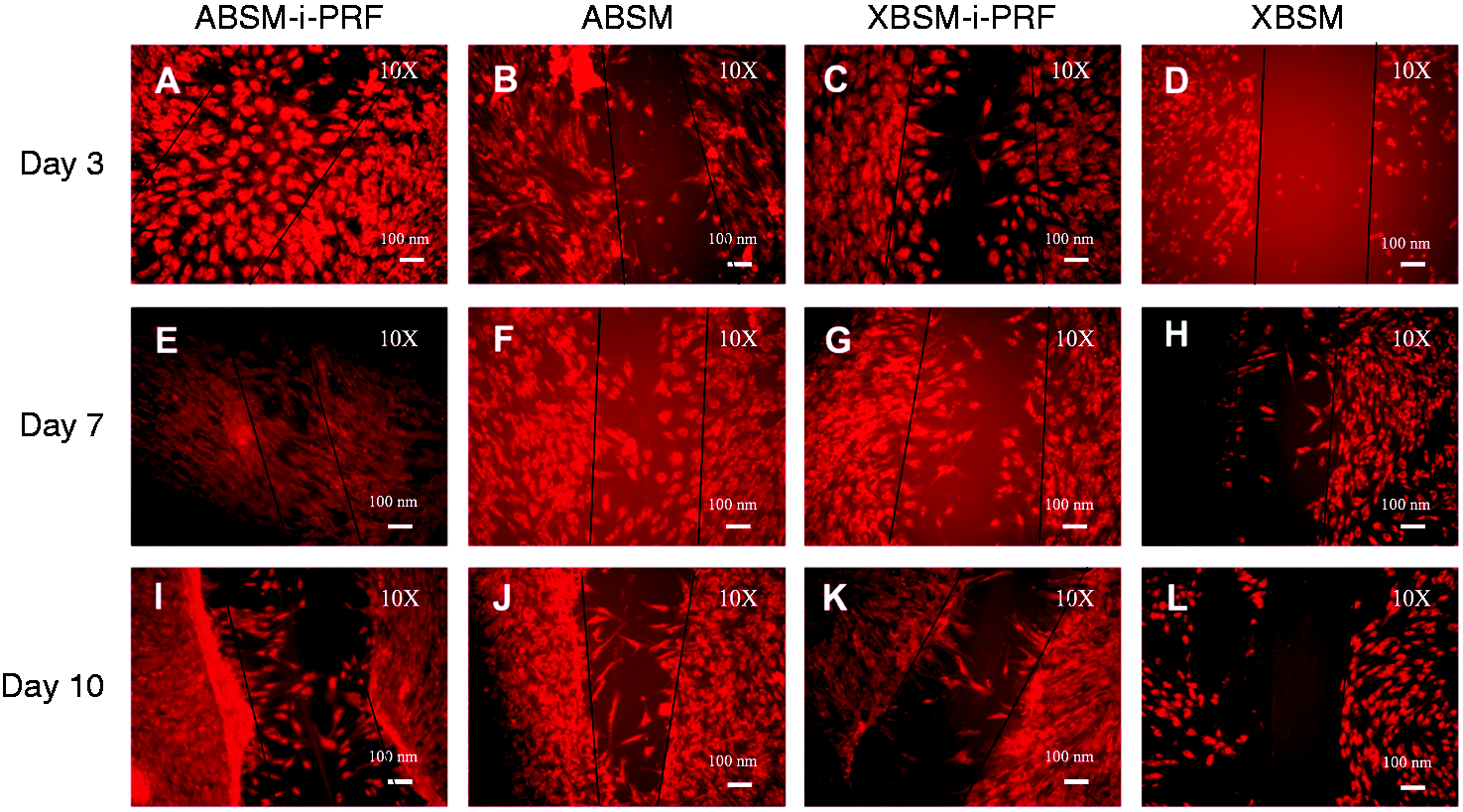
Exemplary figure of HOB attachment (fluorescence BZ-9000 microscope (Keyence, Osaka, Japan), enlargement 10×): groups with ABSM-i-PRF (a, e, i); ABSM (b, f, j); XBSM-i-PRF (c, g, k), and XBSM (d, h, l) at days 3, 7, and 10 after scratch test.
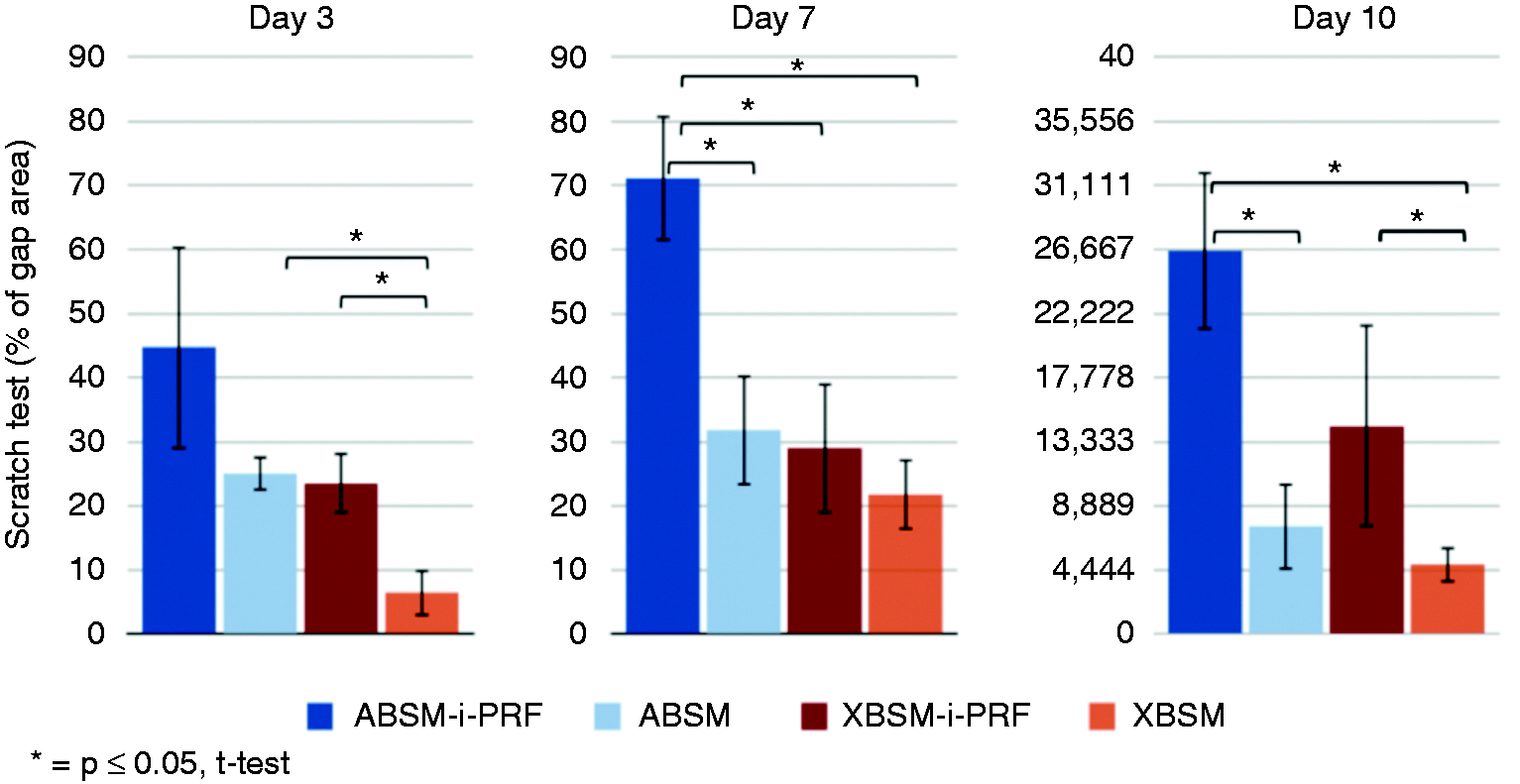
Bar charts: percent of HOB within the gap in comparison to the total scratch area (software ImageJ (ACTREC, Navi Mumbai, India)): ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM) on days 3, 7, and 10; normal distribution. Mean values; error bars show SEM. n = 3 for each group and each time point, three time points.
Percentage of newly attached HOB in relation to the scratch area; statistical significance by t-test: ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM (normal distribution) on the day 3, 7, and 10.
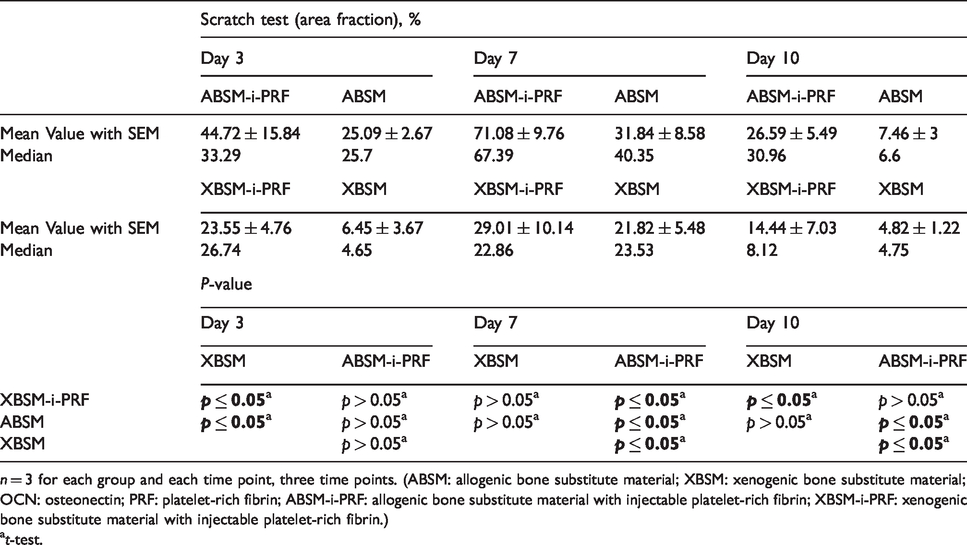
n = 3 for each group and each time point, three time points. (ABSM: allogenic bone substitute material; XBSM: xenogenic bone substitute material; OCN: osteonectin; PRF: platelet-rich fibrin; ABSM-i-PRF: allogenic bone substitute material with injectable platelet-rich fibrin; XBSM-i-PRF: xenogenic bone substitute material with injectable platelet-rich fibrin.)
t-test.
Cell proliferation
The significant highest proliferation rate could be observed in samples with ABSM-i-PRF when compared to the other groups during the whole period (p ≤ 0.05). Also, at all time points, XBSM-i-PRF as well as ABSM showed higher proliferation values when compared to XBSM (p ≤ 0.05) (Figure 5; Table 3).
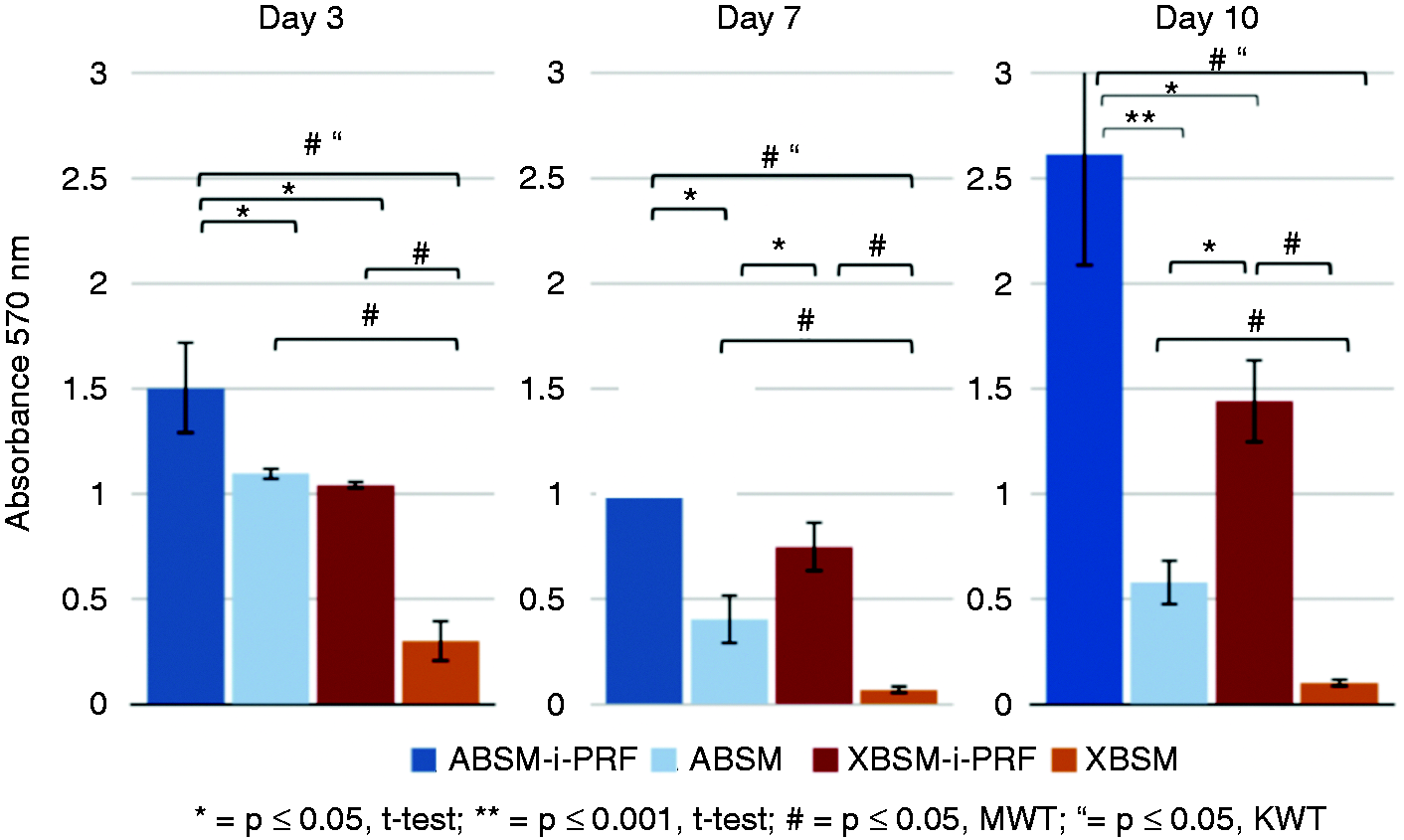
Bar charts showing the comparison in HOB proliferation rate (MTT) in ABSM-i-PRF, ABSM, XBSM-i-PRF with normal distribution) on days 3, 7, and 10; data of XBSM is not normally distributed; error bars show SEM. n = 3 for each group and each time point, three time points.
Proliferation rate of HOB (MTT assay); statistical significance by t-test (ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM) on the days 3, 7, and 10.
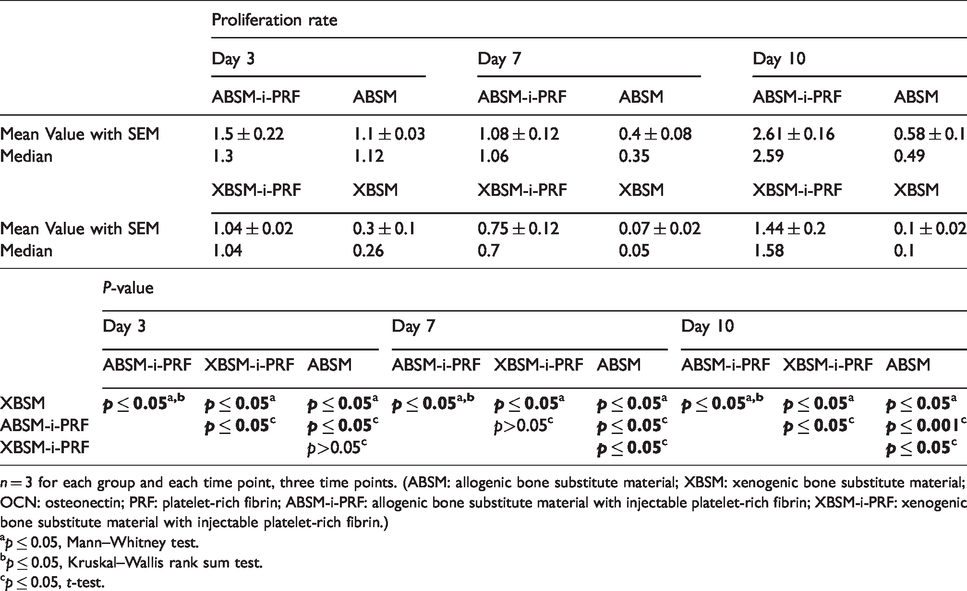
n = 3 for each group and each time point, three time points. (ABSM: allogenic bone substitute material; XBSM: xenogenic bone substitute material; OCN: osteonectin; PRF: platelet-rich fibrin; ABSM-i-PRF: allogenic bone substitute material with injectable platelet-rich fibrin; XBSM-i-PRF: xenogenic bone substitute material with injectable platelet-rich fibrin.)
p ≤ 0.05, Mann–Whitney test.
p ≤ 0.05, Kruskal–Wallis rank sum test.
p ≤ 0.05, t-test.
Real-time quantitative PCR
Alkaline phosphatase (AP) expression
A statistically significant difference was observed at day 7 between ABSM-i-PRF and ABSM as well as between ABSM-i-PRF/ABSM and X-BSM-i-PRF with the highest values for XBSM-i-PRF (p ≤ 0.05) (Figure 6(a); Table 4).
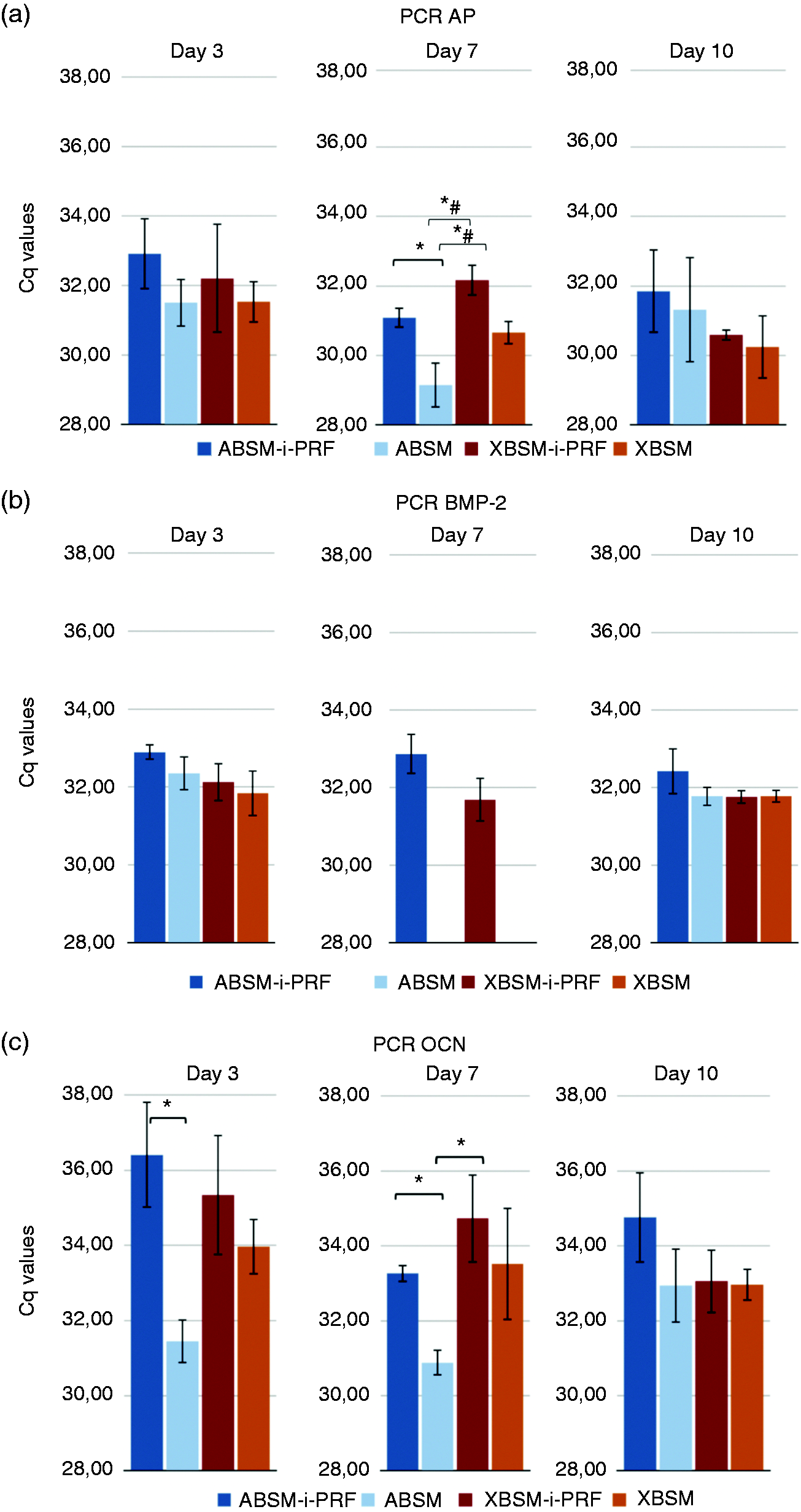
Bar charts showing AP (a), BMP-2 (b), and OCN expression (c) in the groups ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM on days 3, 7, and 10, measured by real-time quantitative PCR. Values of all groups were normally distributed except ABSM/XBSM in BMP expression groups; error bars show SEM. n=3 for each group and each time point, three time points. *p ≤ 0.05, t-test; #p ≤ 0.05, Kruskal–Wallis rank sum test.
Expression of AP, BMP-2, and OCN for ABSM-i-PRF, ABSM, XBSM-i-PRF, XBSM on days 3, 7, and 10.
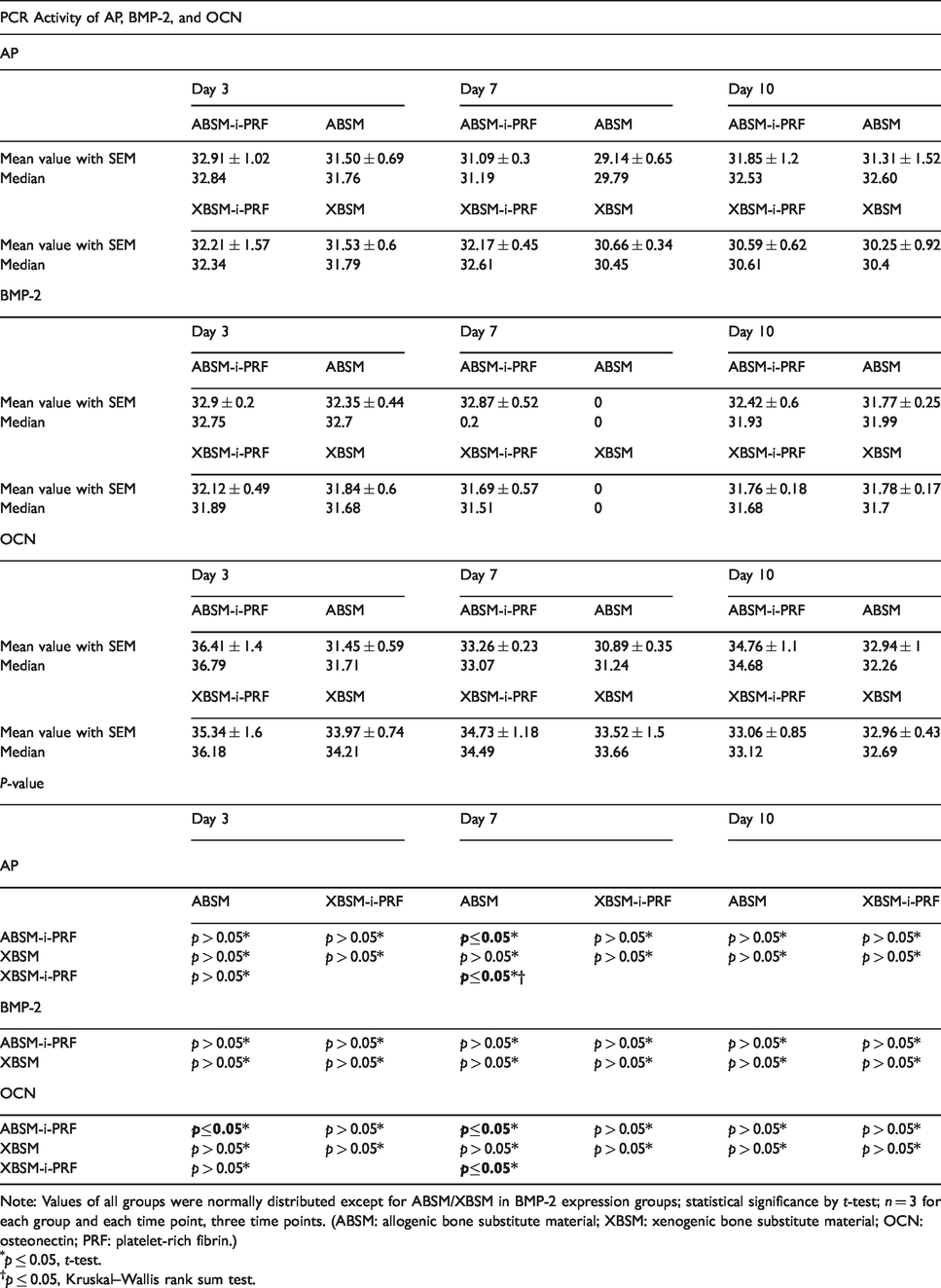
Note: Values of all groups were normally distributed except for ABSM/XBSM in BMP-2 expression groups; statistical significance by t-test; n = 3 for each group and each time point, three time points. (ABSM: allogenic bone substitute material; XBSM: xenogenic bone substitute material; OCN: osteonectin; PRF: platelet-rich fibrin.)
p ≤ 0.05, t-test.
p ≤ 0.05, Kruskal–Wallis rank sum test.
Bone morphogenetic protein 2 (BMP-2) expression
The non-significantly highest expression of BMP-2 (p > 0.05) was detected in groups with ABSM-i-PRF at days 3, 7, and 10 (32.9 ± 0.2, 32.87 ± 0.52, 32.42 ± 0.6, respectively). At day 7, in groups with non-i-PRF-BSM, there was no BMP-2 expression observed at all. With the exception of day 10, BMP-2 expression remained non-significantly higher (p > 0.05) in BSM-i-PRF groups when compared to their equivalent non-i-PRF-BSM groups (Figure 6(b), Table 4).
Osteonectin (OCN) expression
At days 3 and 7, the highest OCN expression of all groups could be observed in the ABSM-i-PRF group (36.41 ± 1.4 and 34.76 ± 1.1, respectively). At day 7, the highest OCN expression was shown in XBSM-i-PRF groups (34.73 ± 1.18). Significant differences were measured between the ABSM-i-PRF and ABSM groups at days 3 and 7 as well as between XBSM-i-PRF and ABSM at day 7 (all p ≤ 0.05) (Figure 6(c), Table 4).
Discussion
In this study, a beneficial in vitro effect of i-PRF in combination with an allogenic (ABSM) and a xenogenic bone substitute material (XBSM) on HOB characteristics was evaluated. BSM in combination with i-PRF showed a significantly elevated HOB viability, attachment and proliferation as well as expression of proliferation and differentiation markers when compared to non-i-PRF-BSM. However, XBSM-i-PRF as well as XBSM showed inferiority when compared to the allogenic bone substitute (ABSM) and, to a greater extent, to ABSM-i-PRF in most of the parameters. In conclusion, the obtained data clearly demonstrate the healing-enhancement effect of the PRF when combined with BSM. Another possible approach analyzed by others may represent the use of single growth factors such as VEGF or PDGF to enhance healing.40,41 However, due to high costs and strict regulations, the use of single growth factors in addition to BSM is not implemented up-to-date in the clinical pathway.
The main prerequisites for ideal BSM are both ease of its handling and application as well as biological characteristics close to autologous bone. 42 Considering that, allograft may be the BSM of choice, due to its unlimited availability, possibility of patient specific customization and its biocompatibility. Generally, ABSM has the potential to induce endochondral bone formation, that is feasible by incorporated BMPs and collagen type I,43–45 although limited in comparison to autologous bone. 46 First, this might be due to storage, processing, and sterilization procedures; 47 second, because of immunologic responses of the recipient. 48 However, on the final stage of incorporation, there are no histologic differences between allogenic and autologous graft.43,49 Thus, Soardi et al. have reported allograft to have best outcomes compared to other types of BSM in augmentation of severely atrophied alveolar ridges. 50 Tilaveridis et al. gave evidence for effectiveness of ABSM in sinus augmentation procedures in a retrospective study of critical cases. 1 It was also demonstrated that ABSM is equivalent to autogenous bone in augmentation of single tooth defects. 2 Tong et al. stated an increased effectiveness of demineralized freeze-dried bone in comparison to autologous bone considering implant survival. 51 Besides, Solakoglu et al. gave evidence for a low risk of residual alloimmunization of processed allografts. 52
Recently, it was shown that low speed centrifugation has a direct effect on matrix contents of PRF.32,53,54 Thus, reducing the relative centrifugation force, a new protocol of PRF processing was proposed that can produce a stable (advanced-PRF, A-PRF) or liquid (injectable, i-PRF) membrane. 32 In accordance, the main difference of i-PRF from conventional PRF is the lower speed of preparation and decreased time of centrifugation, that enables to keep some important cellular components in it.16,32,33 Due to these changes in centrifugation time, a significantly increase in leukocyte number in the PRF matrix and an increased expression of growth factors was seen.32,33,53,54 It was reported that i-PRF shows a significantly higher long-term release of growth factors and a higher fibroblast migration when compared to other platelet concentrates. 33 Considering that, i-PRF was chosen in the present study to test its synergic effect with different BSM.
Although i-PRF has shown success in various clinical implementation,34,55 there is a lack of reliable data considering preclinical and clinical issues of combination of i-PRF with ABSM and XBSM.56–58 Previous studies reported that PRF releases autologous growth factors gradually and expresses stronger and more durable effect on proliferation and differentiation of HOB in vitro more than any other platelet concentrates.21,22 In the present study, significant differences in between the groups in terms of HOB viability, attachment and proliferation were seen. Here, ABSM-i-PRF showed the most favorable in vitro results in comparison to XBSM-i-PRF, ABSM, and XBSM. This is in accordance with an animal study by Karayürek et al. that found an increased bone healing in the group with PRF and autografts. Even if the combination of β-tricalcium-phosphate with PRF could not provide superiority in terms of bone regeneration, the immunohistochemical results showed a high expression of proliferation marker such as osteopontin and osteonectin. 59 Some studies investigated the effect of PRF on XBSM. 60 However, there is only low-level evidence of benefits of the combination of PRF with XBSM in terms of graft maturation when transferred in the clinical setting.60–62
To the best of our knowledge, no other study analyzed the in vitro effect of i-PRF on HOB when combined with ABSM. However, the beneficial effect on ABSM was evaluated clinically as Choukron et al. demonstrated a reduction of healing time prior to implant placement after sinus augmentation with freeze-dried ABSM in combination with i-PRF.21,22 Addition of PRF to ABSM has shown to enhance bone maturation and to shorten the time span before implant placement. 63 This could be explained by the (minimal) osteoinductive potential of ABSM which may be further enhanced by platelet concentrates’ cellular components and could approximate induction properties of ABSM to autologous bone transplants, providing new approaches in bone regeneration. Interestingly, BMP-2 expression, despite the late HOB passage, showed relatively high expression rate in all groups except for the non-i-PRF groups on day 7 where it failed to show any expression at all.
This study suffers from some limitations. First, this is an in vitro pilot study. Therefore, results should be re-evaluated in an animal model and further prospective trials before implementation in the clinical workflow. Second, future studies should also include HOB alone with and without PRF to evaluate the effects of the biomaterials and PRF alone. Third, growth factor expression of PRF varies intra- and interindividual. Therefore, a cohort study may help to further characterize “optimal” expression levels for future clinical use.
Choukroun et al. revealed that the donor-related values of the platelet distribution and the leukocytes number by different protocols of PRF preparation were approximately similar. 33 On the other hand, there is emerging evidence of interindividual differences (age, sex, underlying conditions) concerning mainly the platelet counts of the different donors that seems to correlate with the fibrin network density and released growth factor levels. 64 Here further studies are also needed.
Conclusion
i-PRF in combination with ABSM and – to a lesser extent – to XBSM enhances proliferation, cell migration and differentiation of HOB when compared to non-i-PRF-BSM in vitro. This could ultimately result in a clinical advantage in terms of faster bony healing.
Footnotes
Authors’ contribution
The methodology followed in this study was taken care of by PWK, SK, and SB; SK, SB, AP, PWK were involved in Formal analysis and investigation; SK, PWK were involved in writing and original draft preparation; SK, SB, AP, DT, BAl-N, PWK took part in writing, review and editing; PWK and BAl-N were involved in supervision. SK und SB contributed equally to this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SK received a research grant from the Osteology Foundation. AP, BAl-N and PWK received honoraria for speaking at symposia by Straumann. BAl-N received honoraria for speaking at symposia by Straumann and Geistlich.
Ethical approval
All procedures participants were in accordance with the ethical standards of the local research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For venepuncture and collection of peripheral blood of healthy volunteers, informed consent was obtained from all individual participants included in the study. In accordance to the local Ethical Committee, further formal approval of this kind of study was not necessary.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Department of Oral and Maxillofacial Surgery, University Medical Center Mainz, Germany. SK received a Research Grant for Doctoral Candidates and Young Academics and Scientists from DAAD (German Academic Exchange Service; Deutscher Akademischer Austauschdienst).