
Abstract
Amniotic membrane (AM) has been shown to enhance corneal wound healing due to the abundance of growth factors, cytokines, and extracellular matrix (ECM) proteins inherent to the tissue. As such, AM has garnered widespread clinical utility as a biological dressing for a number of ophthalmic and soft tissue applications. The preparation, sterilization, and storage procedures used to manufacture AM grafts are extremely important for the conservation of inherent biological components within the membrane. Current processing techniques use harsh chemicals and sterilization agents that can compromise the fundamental wound healing properties of AM. Furthermore, commercially available cryopreserved AM products require specific storage conditions (e.g., ultra-low freezers) thereby limiting their clinical availability in austere environments. Supercritical carbon dioxide (SCCO2) technology allows for the sterilization of biological tissues without the resulting degradation of integral ECM proteins and other factors often seen with current tissue sterilization processes. With this study we demonstrate that lyophilized AM, sterilized using SCCO2, maintains similar biochemical properties and biocompatibility as that of commercially available AM products requiring specialized cold storage conditions.
Introduction
Amniotic membrane (AM) has been widely used in the clinic to treat corneal wounds. Numerous studies have shown enhanced regeneration of injured tissues due to the AM’s lack of immunogenicity and ability to reduce inflammation and scarring.1–3 The favorable therapeutic properties of AM are attributed to the growth factors, cytokines, chemokines and other non-protein mediators present in AM tissue that work in concert with neighboring epithelial cells and limbal stem cells to promote the re-epithelialization of injured corneal surfaces. 4 AM also acts as a physical barrier, protecting the injured corneal surface from eyelid friction and by preventing water loss through desiccation. Furthermore, when used as a graft to treat chronic corneal pathologies such as persistent corneal epithelial defects and limbal stem cell deficiencies, amniotic membrane serves as a substrate for the migration, adhesion, and proliferation of corneal epithelial cells and limbal stem cells. 5
While the many wound healing attributes of AM are well documented, processing and storage obstacles persist with commercially available products. Current sterilization techniques including gamma irradiation, ethylene oxide gas, steam, hydrogen peroxide plasma and chemical detergents have been shown to alter the morphological, structural and biochemical properties of AM and reduce its innate bioactivity and consequently, efficacy.6–8 Additionally, many of these techniques yield products requiring temperature sensitive transportation and storage conditions (e.g., ultra-low freezers), limiting their shelf-life and making them unsuitable for use as a deployable therapy by the military or for use in developing countries due to cold chain logistical constraints. 8
Supercritical carbon dioxide (SCCO2) sterilization is an emerging technology currently used in biomedical applications for the sterilization of medical devices, implants and human tissues for transplantation. 9 At temperature and pressure conditions above the critical point, CO2 exhibits gaseous viscosity and diffusion properties while at the same time, dissolution properties like that of a liquid.6,10 SCCO2 technology facilitates the diffusion of a sterilizing agent into sensitive biomaterials, providing a method for the inactivation of microorganisms at temperatures amenable to maintaining the structural integrity, biochemical and biomechanical properties of the tissue.6,10,11 Furthermore, the process of SCCO2 sterilization has the added benefit in that it is non-toxic and easily removed via depressurization and out-gassing. 6 Previous studies by our lab have determined AM sterilized via SCCO2 did not alter the structural, biochemical or biophysical properties of the tissue. In addition, SCCO2-sterilized AM supported stem cell attachment and expansion in vitro making it a viable alternative for treating corneal surface injuries and other injuries including dermal burns and ulcers. 10
Combining the gentle sterilization of SCCO2 with a lyophilization step may provide an attractive alternative to currently available AM products by rendering a sterile, shelf-stable product with preserved biological activity. We hypothesized that the incorporation of a lyophilization step following SCCO2 sterilization would result in a shelf-stable AM tissue graft with conserved extracellular matrix proteins and growth factors comparable to those found in native AM. Here we present a two-part study first examining the biocompatibility of SCCO2-sterilized AM in a rabbit corneal model as proof-of-concept for future studies. We further compared the structural and functional properties of SCCO2-processed and lyophilized AM with native amniotic membrane using an array of cell and molecular biology techniques to evaluate variations in important biological features as a result of our novel processing method.
Materials and methods
Amniotic membrane procurement and processing
Placentas from consenting donors undergoing cesarean deliveries were procured through the Cooperative Human Tissue Network, Southern Division (CHTN). Tissues were de-identified and screened for routine blood-borne pathogens by CHTN and shipped to the United States Army Institute of Surgical Research (USAISR) in a cooled primary container. The AM was separated from the chorion using blunt dissection and aseptic technique, thoroughly cleaned, rinsed in sterile saline and placed, epithelial side up, on nitrocellulose membrane (0.45 µm; GE Healthcare Life Sciences, Pittsburgh, PA) prior to sterilization (Figure 1(a) to (c)). Amniotic membrane samples were placed in two Tyvek® (DuPont™) packages and heat sealed before processing, as previously described. 10
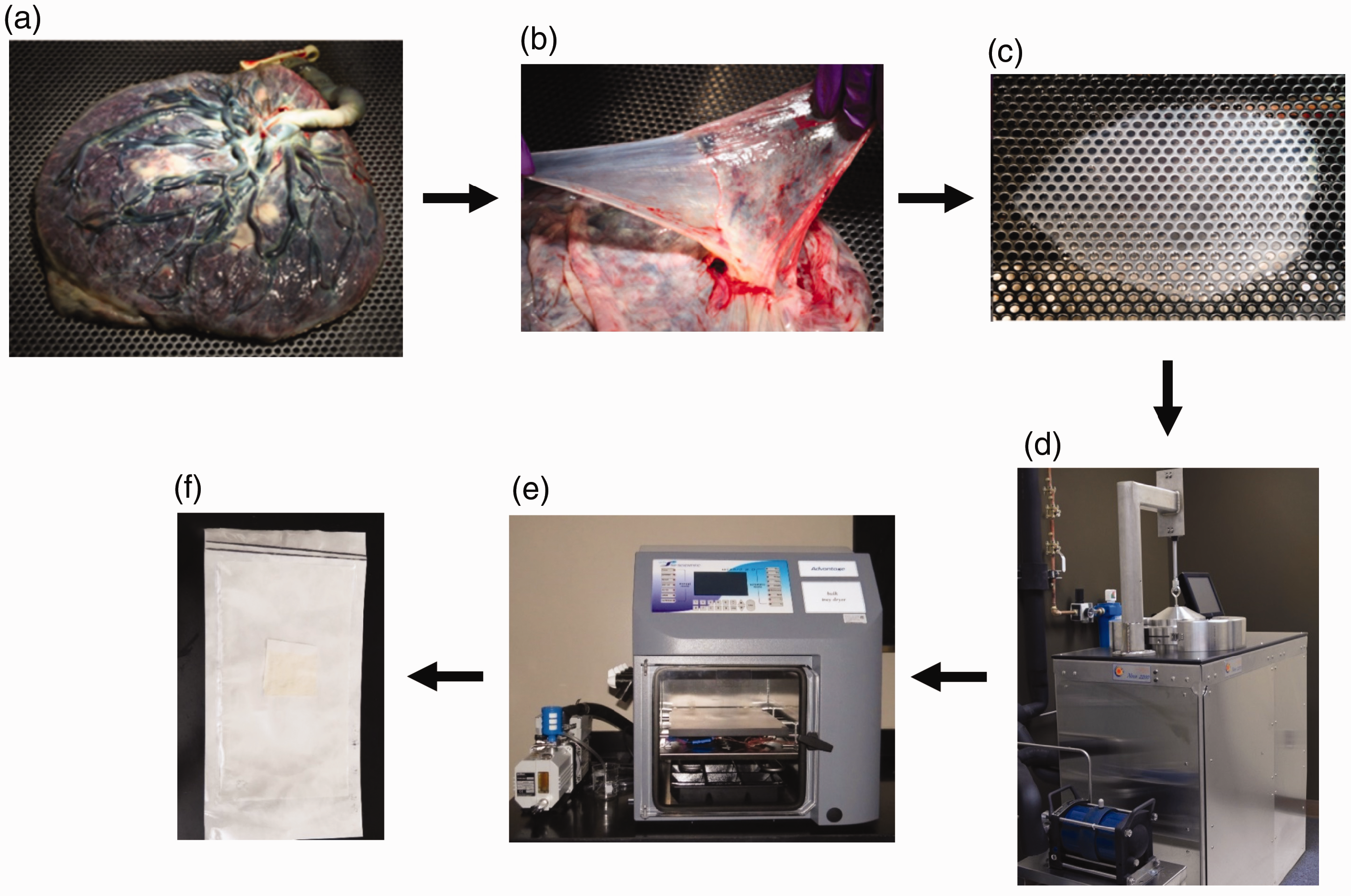
Amniotic membrane processing flow. Placentas from consenting donors were procured through the Cooperative Human Tissue Network (a) and the amnion separated from chorion using blunt dissection (b). AM was thoroughly cleaned (c), placed epithelial side up on nitrocellulose paper prior to sterilization and sealed in two Tyvek® packages. The amnion in Tyvek® packaging was sterilized in the Nova 2000 SCOO2 sterilizer (d) followed by water removal via lyophilization (e). The final product (f) was then stored at various temperatures and time points to evaluate shelf life.
Amniotic membrane sterilization and storage
Sterilization of AM tissue was carried out in a Nova 2200 SCCO2 sterilizing unit (Figure 1(d)) (NovaSterilis, Lansing, NY) which houses wire baskets for holding the Tyvek®-packaged samples as well as an additive pad to which 2 mL of peracetic acid (Sigma-Aldrich, St. Louis, MO) was added as previously described. 10 After sterilization, AM was either immediately stored at −80°C (S-AM), or lyophilized (L-AM), undergoing a 16 hour freeze-drying process (Figure 1(e)) (Advantage XL-70; VirTis SP Scientific, Warminster, PA) before being stored in a closed container at a room temperature (∼24°C) (Figure 1(f)). Unprocessed AM (native; N-AM) was also collected and stored at -80°C until ready for analyses.
In vivo ocular biocompatibility
For in vivo studies, male New Zealand white rabbits (Charles River Laboratories, Wilmington, MA) weighing 2.5–4.0 kg from Charles River Laboratories (Wilmington, MA) were used. Rabbits were allowed to acclimate for at least one week prior to start of procedures. Research was conducted in compliance with the Animal Welfare Act, the implementing Animal Welfare Regulations, and the principles of the Guide for the Care and Use of Laboratory Animals, National Research Council. The facility's Institutional Animal Care and Use Committee approved all research conducted in this study. The facility where this research was conducted is fully accredited by AAALAC.
To prevent dislocation of the amniotic membrane, the nictitating membrane was removed from the eyes of rabbits following established methods. 12 Briefly, the animals were placed under anesthesia with a mixture of ketamine (35–45 mg/kg) and xylazine (5 mg/kg) administered via intramuscular injection then placed on isoflurane (1–3.5%). The left eye of each rabbit was topically anesthetized with 0.5% tetracaine hydrochloride and disinfected with 5% betadine (Alcon, Fort Worth, TX) prior to the surgical removal of the nictitating membrane, as previously described (Figure 2(a) and (b)). 13 Post-nictitating membrane removal surgery, the eyes were treated with Bacitracin ophthalmic ointment (Figure 2(c)) and allowed to heal for two weeks prior to the placement of the amniotic membrane.
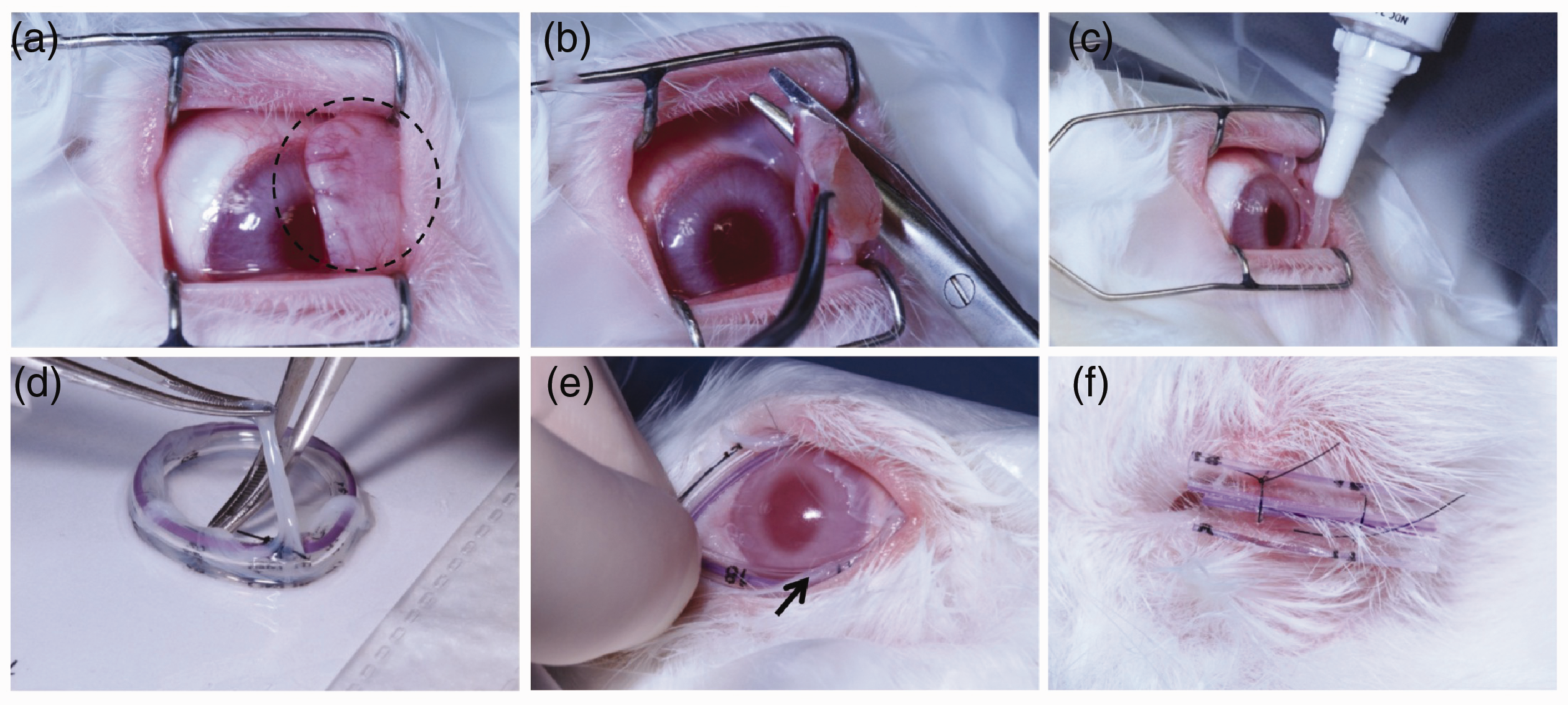
Amniotic membrane and ring placement procedure. To prevent the dislodging of any devices placed on the eye, the nictitating membrane (a; black circle) of the rabbit was removed (b) followed by treatment with Bacitracin ointment (c). After a two week recovery period, SCCO2-processed (S-AM) AM or AmnioGraft® was secured to a ring (d) so the entire inner portion of the ring contained a layer of amniotic membrane. The AM ring (arrow) was placed over the cornea and under the eyelids (e), and the eye closed using a partial tarsorrhaphy method (F).
For the amniotic membrane placement surgery, rabbits were anesthetized and prepared for surgery as described above. A total of 18 rabbits were randomly divided into three test groups (n = 3/group) to be terminally evaluated at 3 and 7 days for AM biocompatibility: SCCO2-sterilized amniotic membrane (with ring), BioTissue AmnioGraft® (TissueTech, Doral, FL) amniotic membrane (with ring), and ring only. AmnioGraft® is a commercially available, cryopreserved human amniotic membrane product commonly that is stored in glycerol at -80°C. AM tissue grafts were placed over the cornea and held in position using flexible polyurethane pediatric nasogastric feeding tubing secured by sutures to form a ring (Figure 2(d) and (e)). The rabbits received a partial tarsorrhaphy to suture the eyelids closed and maintain the position of the AM ring (Figure 2(f)). Animals were monitored daily for the duration of the study for signs of pain or irritation and graft and/or ring retention.
Histology of whole globes
For in vivo analysis, rabbit eyes were collected for histopathological processing and examination on days three and seven post amniotic membrane and/or ring placement. Whole globes were fixed in Modified Davidson’s solution for 24 hr before being transferred to 10% neutral buffered formalin (thermos Fisher Scientific, Middletown, VA). Eyes were bisected, placed cut side down in tissue cassette. Following histological processing, eyes were paraffin embedded, sectioned at 7 µm, and stained with H&E and MTS. Bright-field images were captured using a Leica DM2500 LED optical microscope (Buffalo Grove, IL).
Histology of amniotic membrane
Hematoxylin & Eosin (H&E) and Masson’s Trichrome (MTS) staining was performed on cryosectioned N-, S-, and L-AM samples to assess any potential changes in structural morphology due to processing and storage. The AM samples were placed in optimal cutting temperature (OCT; Tissue-Tek®, Sakura Fintek, Torrance, CA) compound, frozen and sectioned at 7 µm. Following routine H&E and MTS staining, images were captured with a Leica DM2500 LED optical microscope (Buffalo Grove, IL).
Immunohistochemistry
Frozen sections (7 µm) of N-, S-, and L-AM samples were embedded as described above then fixed with 4% paraformaldehyde for 15 min at room temperature, followed by three phosphate buffered saline (PBS, pH 7.4; Thermo Fisher Scientific) washes. After blocking (5% normal serum (antibody-species dependent) + 0.05% Tween-20 + 0.1% bovine serum albumin (BSA; Sigma-Aldrich) in PBS) for 1 hr at room temperature, slides were incubated with either anti-Collagen I (1:200; ab34710, Abcam, Cambridge, MA) , anti-Collagen III (1:1000; ab6310, Abcam), anti-Collagen IV (1:200; ab6586 Abcam), anti-Fibronectin (1:200; ab2413, Abcam) or anti-PTX3 (1:100; ab94649, Abcam) overnight at 4 °C in a humid chamber. Slides were washed with 0.05% Tween-20 + 0.1% BSA in PBS then incubated with appropriate Alexa Fluor 488-conjugated secondary antibodies (1:500; Ex-Max 495 nm/Em-Max 519 nm; ab11034 or ab11029, Abcam) for 1 hr at room temperature. Finally, slides were washed three times in 0.05% Tween-20 + 0.1% BSA in PBS, once with 1x PBS then coverslipped using ProLong™ Gold Mountant (Thermo Fisher Scientific) with DAPI (to visualize nuclei). Images were collected using a Leica DM2500 LED optical microscope (Buffalo Grove, IL) equipped with appropriate filters for fluorescent microscopy.
Protein isolation and quantification
At predetermined storage time points (1 week, 1, 3, and 6 months), AM tissue (2.54 cm2) from the described stored conditions was placed in 250 µL CelLytic MT Lysis Reagent (Sigma-Aldrich) with added protease inhibitor cocktail (10 µL PIC/mL lysis reagent; P-8340, Sigma-Aldrich) and homogenized on ice for 10 seconds. Lysate was centrifuged (20,000 × g) for 10 min at 4 °C and the supernatant stored at −80°C until ready for use. Total protein concentration was determined using the Pierce™ BCA Protein Assay Kit (Thermo Fisher Scientific, Waltham, MA) following manufacturer's recommendations.
Western blot analyses
Western blot analysis of AM samples was performed to determine the presence and maintenance of Pentraxin3 (PTX3) over the varying storage times and processing techniques. AM protein lysate samples were denatured and loaded (10 µg/lane) into 4%-12% Bis-Tris gradient gels (Thermo Fisher Scientific), electrophoresed then transferred to PVDF membranes (Thermo Fisher Scientific). Total protein (10 ug/lane) from two different lots of AmnioGraft® (stored at -80°C prior to protein isolation per manufacturer’s instructions; TissueTech) was used as a positive control. 14 Expression of PTX3 proteins was detected using anti-PTX3 antibody (1:400; ab125007, Abcam) and goat anti-rabbit IgG HRP-conjugated secondary antibody (1:1000; ab6721, Abcam) followed by detection of immunoreactive bands with Novex ECL Chemiluminescent substrate (Thermo Fisher Scientific).
Growth factor antibody array
To monitor variations in growth factor levels as a result of AM processing and storage, the expression profile of 41 growth factors was determined using the Human Growth Factor Antibody Array C1 (RayBiotech, Inc., Norcross, GA). Total protein (100 µg) from N-, S-, and L-AM samples stored for six months were analyzed following manufacturer’s instructions. Immunoreactive dots were visualized via chemiluminescent detection (Novex ECL Chemiluminescent substrate; Thermo Fisher Scientific).
Results
In vivo biocompatibility
To evaluate the biocompatibility of SCCO2-sterilized amniotic membrane on ocular structures, S-AM was evaluated in vivo in an uninjured rabbit model (Figure 3). To reduce the number of experimental animals used in this pilot study, we focused on the use of S-AM as it is most comparable morphologically and biochemically to native AM and AmnioGraft®. Insets of rings in Figure 3 show that the AM, although partially degraded, was maintained up to day 7. The corneas were translucent with no gross signs of inflammation or neovascularization. Eyes were evaluated histologically on days 3 and 7 post-operatively via H&E and MTS staining, and a normal, stratified corneal epithelium was observed in all treatment groups (Figure 4). Additionally, no evidence of edema, inflammation or neovascularization was noted.
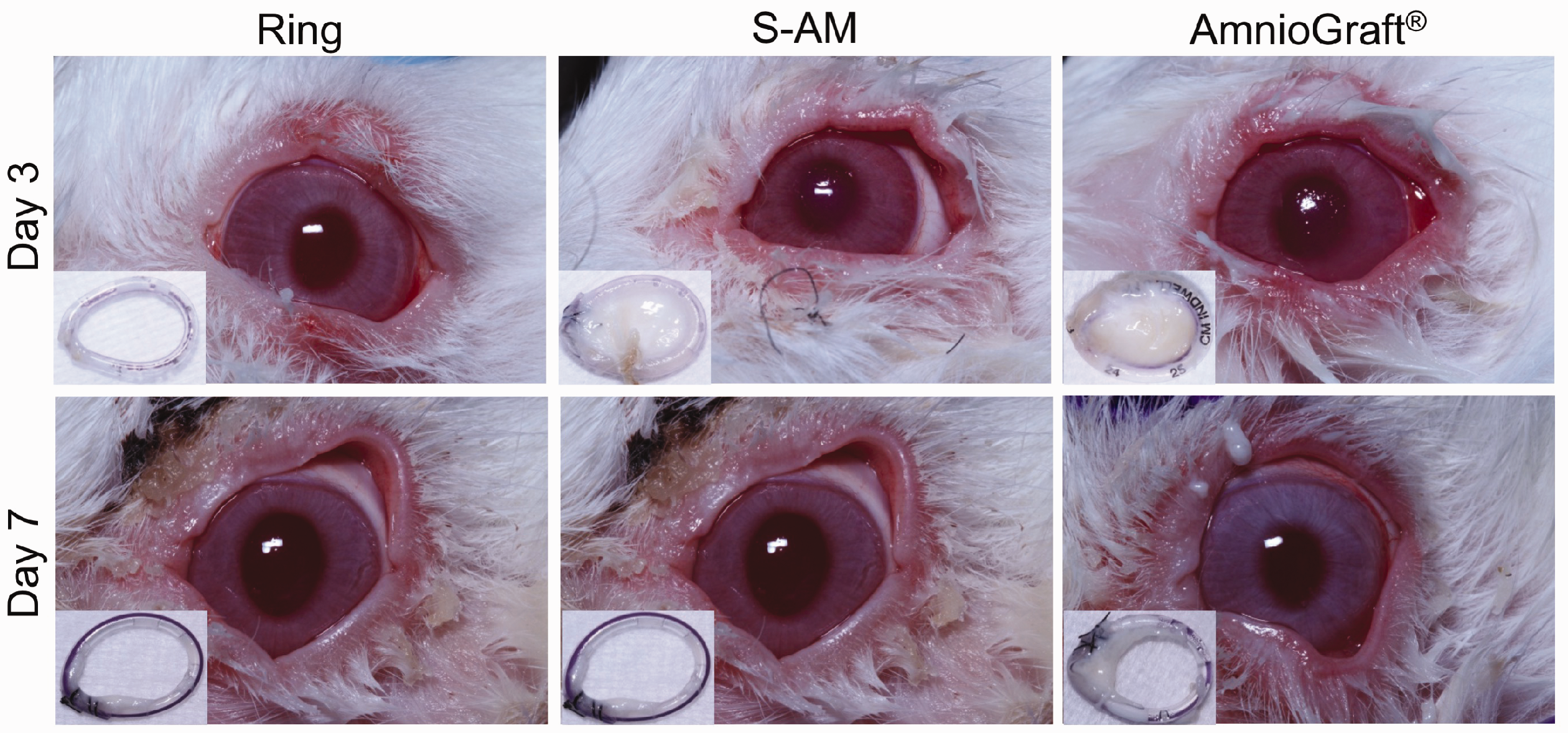
Amniotic membrane in vivo biocompatibility. Representative images demonstrating the gross appearance of the cornea, sclera and surrounding ocular regions of the S-AM or AmnioGraft®-treated eyes. Control eyes were treated with ring only. Insets show condition of the ring or AM + ring at the termination of study.
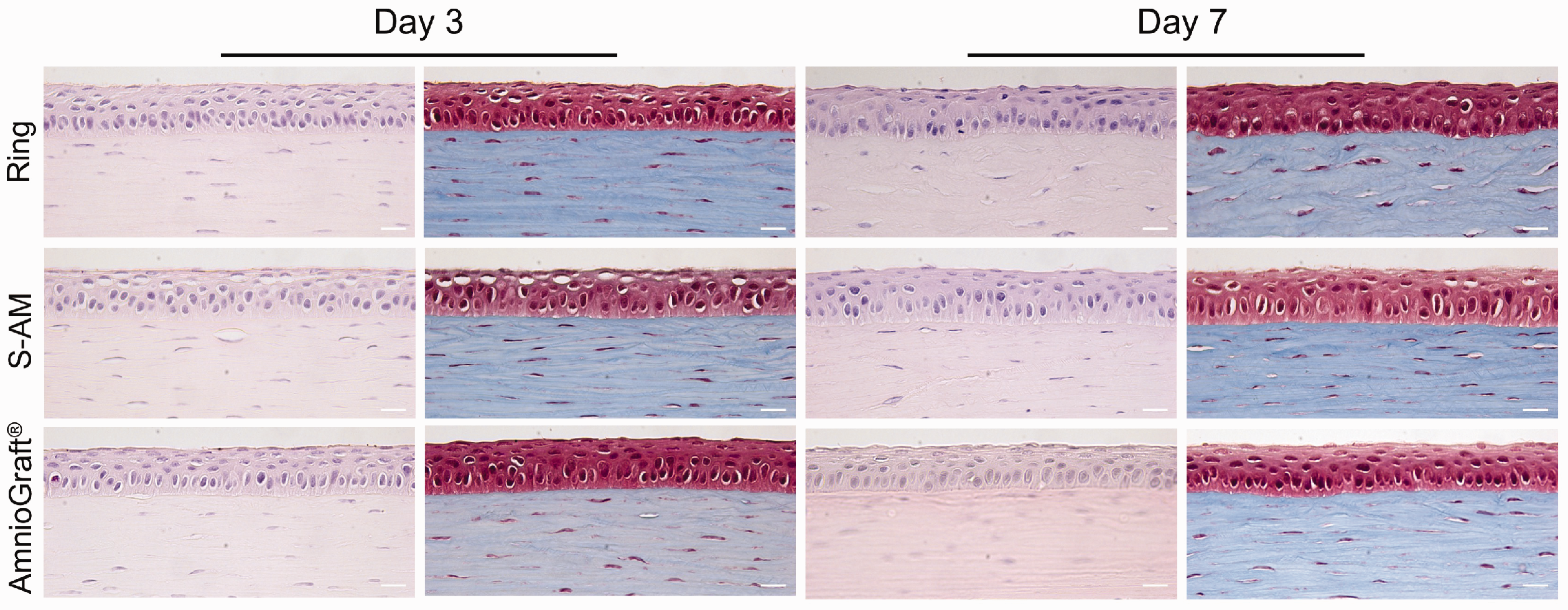
Amniotic membrane biocompatibility whole globe histology. Representative histological images of eyes. Images demonstrate normal structure of the cornea and a lack of inflammatory cells, indicating that the ring and membranes are well tolerated in the rabbit eye at days 3 and 7. (400x; scale bar = 20 µm).
Histological evaluation of native, SCCO2 and lyophilized amniotic membrane
Hematoxylin and eosin (H&E) and Masson’s Trichrome staining (MTS) was conducted to visualize any changes in the structure and morphology of the amniotic membrane as a result of SCCO2 sterilization and lyophilization (Figure 5). The various processing conditions did not appear to alter the staining of the AM tissues. Expectedly, the lyophilization process condensed the amniotic membrane layers as a result of water removal compared to N-AM and S-AM; however, the collagenous stroma remains intact.
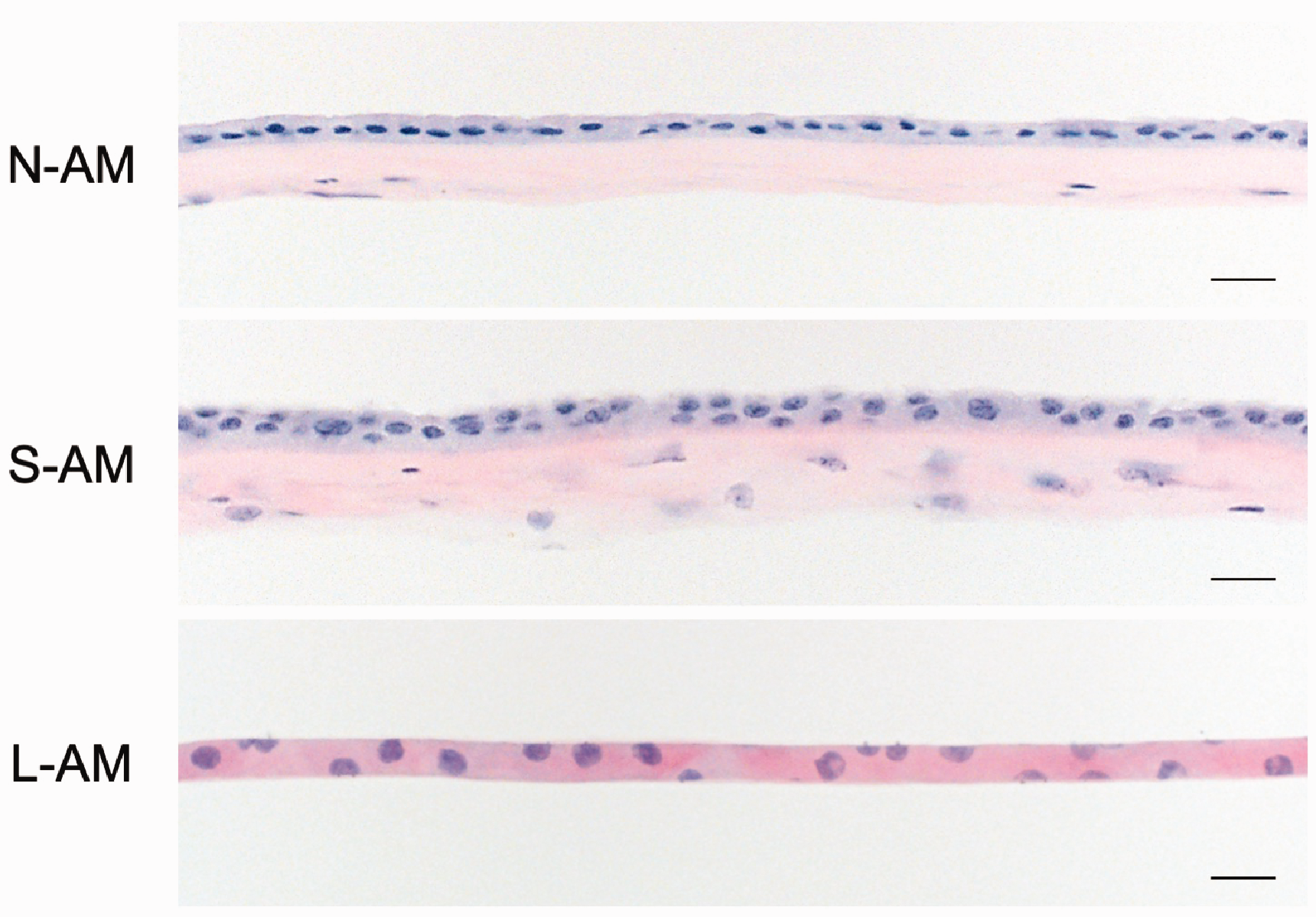
Amniotic membrane histology. Native (N-AM), SCCO2 (S-AM) and lyophilized (L-AM) amnion were sectioned and stained with H&E. The gross thickness and morphology is condensed after lyophilization compared to N-AM and S-AM due to water removal. However, the overall structures remain intact. (400x; scale bar = 20 µm).
Immunohistochemical examination of extracellular matrix molecules
To determine if SCCO2 sterilization and lyophilization processing cause degradation of proteins characteristic of native AM, the expression patterns of several extracellular matrix molecules were investigated in N-AM, S-AM, and L-AM samples (Figure 6). Immunohistochemical examination of collagen I, collagen III, collagen IV, and fibronectin revealed localization of proteins throughout the basement membrane and stromal regions in both N-AM and S-AM sections (Figure 6). Expression of these proteins was also observed in L-AM sections however due to gross morphological changes that occur post-lyophilization, specific regions could not be discerned on a microscopic level.
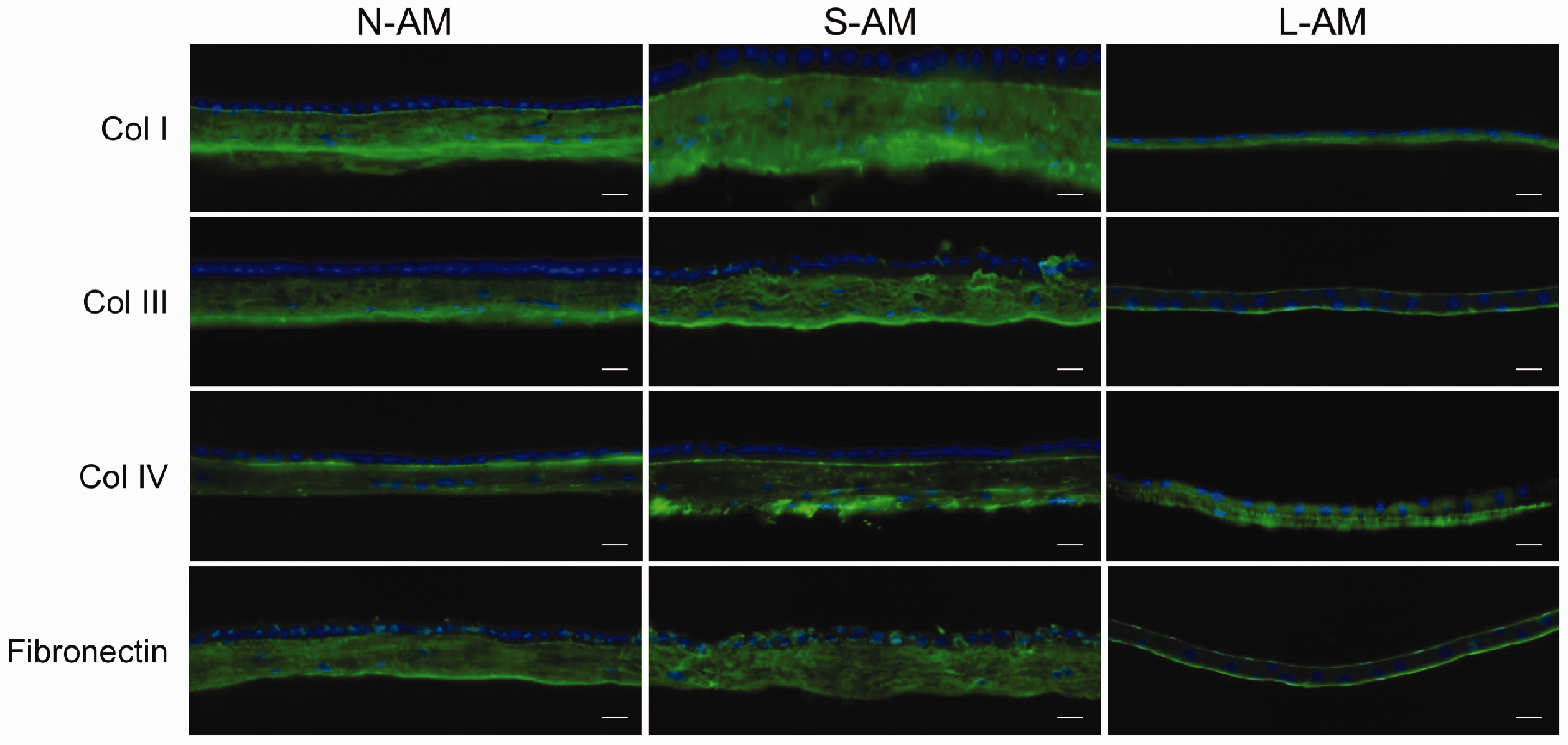
Amniotic membrane extracellular matrix immunostaining. Routine indirect immunohistochemistry was used to detect and evaluate the presence of extracellular matrix proteins inherent to AM. As is demonstrated by the green immunolabeling, each of the proteins evaluated persisted after SCCO2 processing alone or in combination with lyophilization. Nuclei are localized by DAPI staining (blue). (400x; scale bar = 20 µm).
PTX3 analyses
Pentraxin 3 (PTX3) is expressed throughout the amnion and believed to be an important mediator of inflammation. 15 Immunohistochemical staining was performed on N-AM, S-AM, and L-AM tissue sections to evaluate the preservation of PTX3 during processing (Figure 7). Staining revealed the presence of PTX3 in N-AM, S-AM, and L-AM sections demonstrating that the PTX3 protein is retained throughout SCCO2 processing and lyophilization of the amniotic membrane. Interestingly, expression was observed intermittently throughout the stromal layer of both native and processed AM alike.
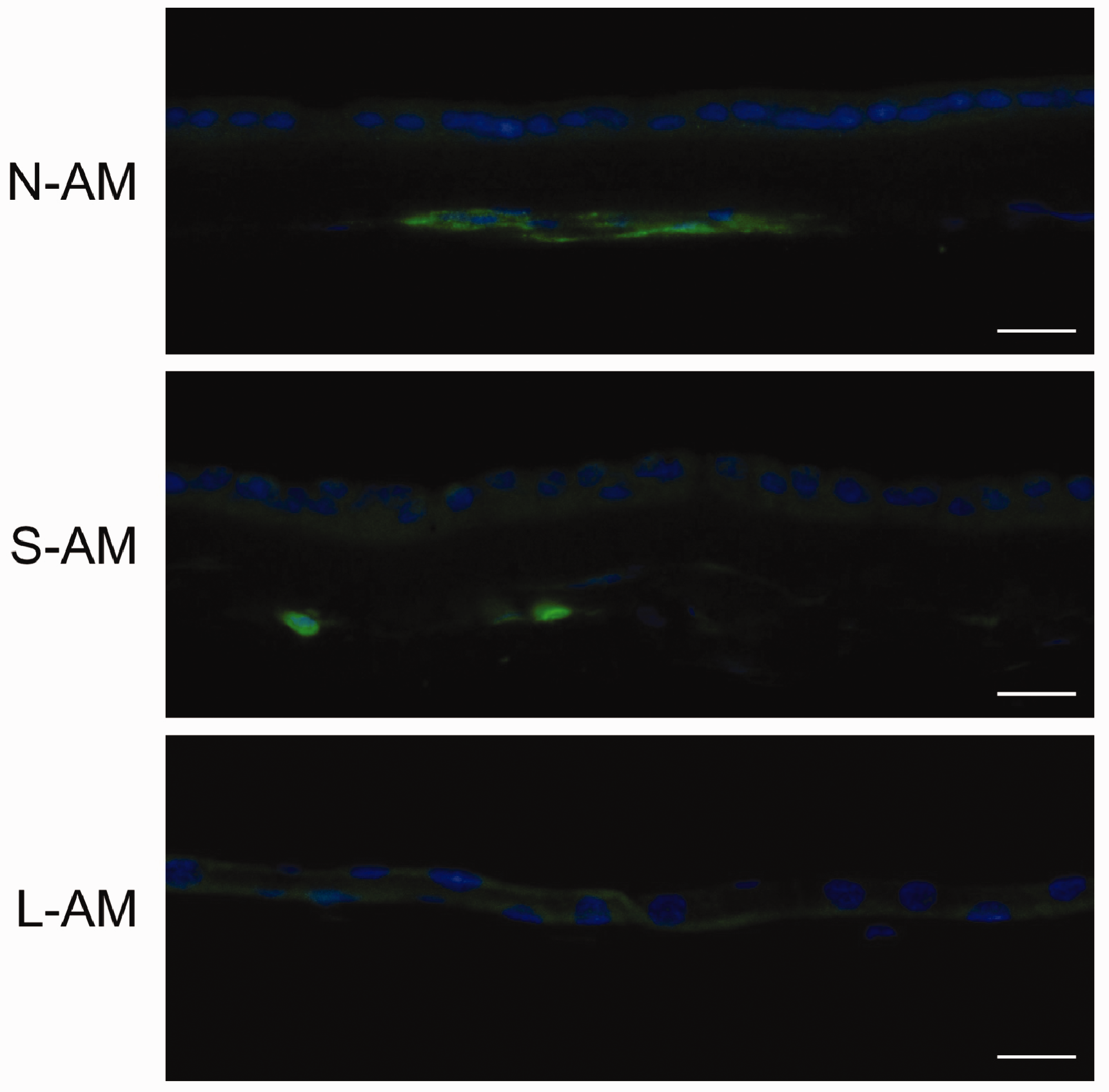
PTX3 immunostaining of amniotic membrane. To evaluate whether SCCO2-treatment allowed for the preservation of the unique biomolecule PTX3, samples of AM were evaluated for the presence of PTX3. Samples of N-AM, S-AM, and L-AM were processed for immunohistology and detection of PTX3. The green fluorescence depicts the localization of PTX3 in AM pre- and post-processed samples. Nuclei are visualized with DAPI (blue staining). (400x; scale bar = 20 µm).
Western blot analysis was performed to assess the presence and maintenance of PTX3 in N-AM, S-AM, and L-AM samples immediately after collection and processing (baseline) and stored at various time points (Figure 8). PTX3 was detected in each group and was maintained over the six month time period tested. Variations in PTX3 protein levels were observed among samples from the same donors regardless of processing treatment and despite loading equal total protein concentrations. We observed this in all donor amniotic membranes collected and commercially available AMs.
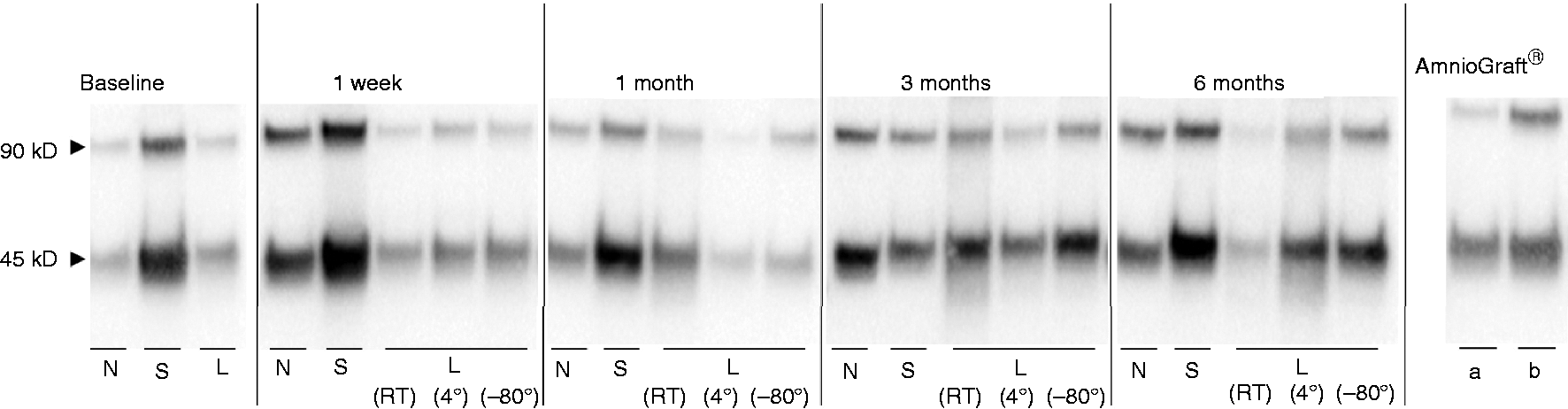
PTX3 western blot analysis of representative stored, processed, SCCO2- sterilized (S) and lyophilized (L) amniotic membrane sample. Total protein was isolated at designated time points and PTX3 expression assessed. Baseline represents protein isolated from samples immediately after collection (native, N-AM), post-SCCO2 (S-AM) and lyophilization processing (L-AM). S-AM and L-AM (RT, 4°, −80°) samples demonstrate the presence and maintenance of PTX3 protein over time comparable to native AM (N) and the commercially available AmnioGraft® (two lots stored at −80°C prior to protein extraction; a and b).
Growth factor antibody array
Growth factor antibody arrays were used to analyze the presence of 41 different proteins and identify potential changes in protein levels in AM samples that may result from the processing and storage methods tested. A six month period of storage was chosen as this is double the shelf life indicated for AmnioGraft® stored at 4 °C. Similar patterns of protein signal intensities were observed between the N-AM, S-AM, and L-AM samples. Relative intensities for each antibody tested in SCCO2-sterilized and lyophilized samples were compared to native amniotic membrane (Figure 9). Two of the highest signal intensities were seen with epidermal growth factor (EGF; red boxes, Figure 9) and insulin-like growth factor 2 (IGF-2; blue boxes, Figure 9) in each of the conditions tested.
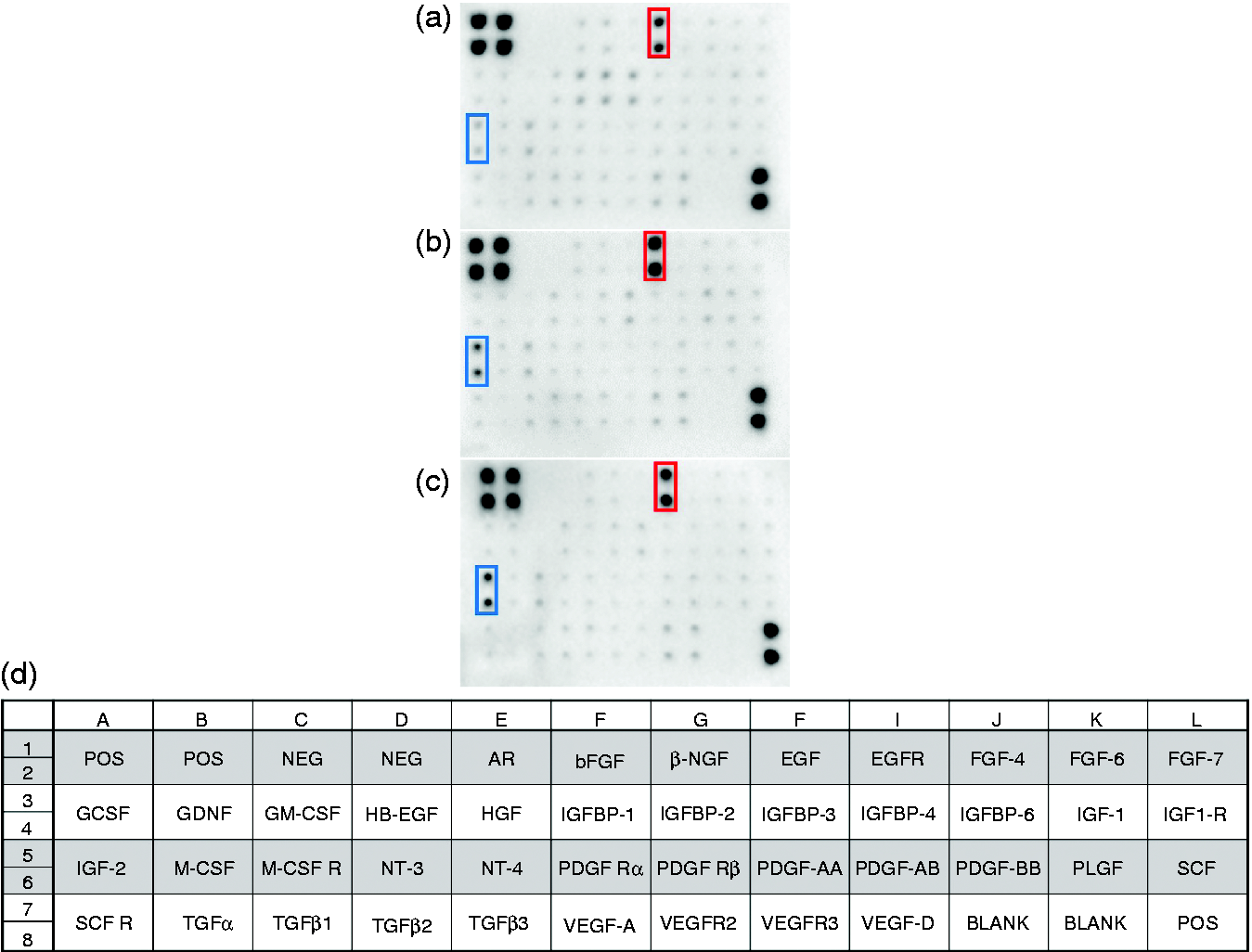
Amniotic membrane growth factor array. Dot blot analysis of the innate expression of 41 growth factors in AM was evaluated using the Human Growth Factor Antibody Array C1 (RayBiotech, Inc.). Total protein (100 µg) from six month AM samples was used following manufacturer’s instruction. Immunoreactive dots were visualized in N-AM (a), S-AM (B) and L-AM (c) samples via chemiluminescent detection. Expression patterns of growth factors are similar between N-AM and S-AM and L-AM. Red boxes highlight EGF expression and blue boxes, IGF-2 expression. Array map showing positions of growth factors tested (d).
Discussion
A tremendous clinical need exists for an ocular bandage capable of mitigating scarring and preserving vision by facilitating wound healing and tissue regeneration via long-term biocompatibility, infection control, bioactive molecule delivery, and therapeutic cell delivery. Human amniotic membrane satisfies many of these criteria, but current commercially available products are costly and processed such that their inherent biological properties are altered to an extent that minimizes AM’s therapeutic efficacy. Furthermore, products on the market must be maintained at ultra-cold temperatures, which make them difficult to deploy to austere environments or developing countries. The data presented in this study demonstrates that SCCO2 sterilization, when combined with a lyophilization step, may prepare AM in a fashion that allows for optimal preservation of growth factors and extracellular matrix proteins while at the same time yielding a shelf-stable product suitable for room temperature storage or deployment in a variety of conditions.
Amniotic membrane has been successfully used as a surgical and biological bandage to treat ophthalmic, soft tissue, orthopedic, and oral and maxillofacial injuries for more than a century. 16 The many benefits of AM include its ability to enhance wound healing, reduce inflammation and scarring, and serve as a substrate for cell attachment, proliferation and differentiation.17–19 In the ophthalmology clinic, AM has been used since 1946 20 to treat corneal and conjunctival defects and injuries as a permanent graft or temporary biological bandage. 4 Clinical ophthalmic indications for the use of AM include corneal surface reconstruction due to persistent corneal defects, infectious keratitis or keratopathy, limbal stem cell deficiencies as well conjunctival surface reconstruction and as a treatment for acute chemical/thermal burns and injuries. 4 Despite the well documented usage of amniotic membrane for the treatment of ocular surface defects, little is known about the mechanism by which AM imparts its wound healing properties. Mechanistically, amniotic membrane provides a basement membrane-type substrate (i.e., collagens, laminins and fibronectins) to the injured corneal epithelium as well as protection and hydration to the existing corneal epithelial cells. 21 Biochemically, amnion delivers growth factors and anti-inflammatory mediators to the anterior ocular structures to promote tissue regeneration and wound healing as well as inhibiting scar formation and corneal neovascularization. 22 Importantly, we show here the preservation of several growth factors and proteins believed to be essential for imparting the beneficial wound healing properties observed with clinically applied amniotic membrane products. When our S-AM and L-AM processed samples were evaluated for the presence of known AM proteins, many were detected, specifically ECM proteins including Col I, III, IV and fibronectin (Figure 6) and insulin and epidermal growth factors (Figure 9).
Recent studies have suggested that in addition to the therapeutic growth factors present in AM, heavy chain-hyaluronan/pentraxin3 (HC-HA/PTX3) might be a key biomolecule responsible for the favorable therapeutic properties intrinsic to AM. He et al. 15 and Zhang et al. 23 have shown that the HC-HA/PTX3 complex may be involved in many of the anti-inflammatory and pro-regenerative properties seen with the clinical application of amniotic membrane products. In our studies, we found that PTX3 was detectable before and after our processing techniques, and varying storage temperatures did not appear to alter its presence. It is noteworthy to mention that PTX3 detection was highly variable from donor to donor and from region to region within the structure of the AM. We hypothesize this may be due to differential spatial or regional distribution of the protein throughout the membrane. This could be a result of the biological heterogeneity of the membrane and the locations samples were collected from as seen with other studies demonstrating differences in metabolic activity and gene expression profiles throughout amniotic regions.24–27
Numerous techniques and methods have been reported for preparing AM for use in clinical applications. However, most techniques require the use of harsh chemicals and sterilizing agents that are damaging to delicate AM tissue matrix, compromise beneficial wound healing properties of the AM graft, and can potentially affect the patients’ clinical outcome.7,8 Supercritical carbon dioxide sterilization a novel method for AM graft preparation and sterilization while preserving the native biochemical and structural properties of the tissue. When combined with a lyophilization step, L-AM retains crucial bioactive molecules believed to be significant for wound healing including PTX3 and other GFs also found in N-AM.28,29 Our novel method of AM sterilization combined with lyophilization produces a tissue graft which can be used as a bandage or cell scaffold for ocular therapeutic applications without the need for costly and limiting storage requirements.
In addition to the advantages of increased shelf life and minimal storage requirements, numerous studies have shown therapeutic benefits for using lyophilized amniotic membrane products over cryopreserved for the treatment of ocular surface defects. Ahn et al. demonstrated improved corneal epithelium reconstruction using lyophilized amniotic membrane as compared to cryopreserved in an in vitro model for corneal transplantation. 30 In a rabbit model of ocular surface injury, lyophilized amniotic membrane performed comparably to cryopreserved amniotic membrane with similar handleability and graft integrity over time. 31 Similarly, Nakamura et al. showed that freeze-dried amniotic membrane graft retained most of the biological and morphological properties of cryopreserved amnion while also proving biocompatible when transplanted for the treatment of pterygium in patients.32,33
Biocompatibility is a hallmark characteristic required in a successful allograft product. The implanted biomaterial or allograft tissue must be biologically compatible in that it will not illicit an immunological response from the host tissue. 17 Although the cornea is an immune privileged tissue, rejection of transplanted tissue can occur. Kubo et al. 34 showed skin grafts were rejected three weeks post intracorneal transplantation in a rat model, with neovascularization and corneal edema being the mechanism underlying graft failure. By comparison, eyes transplanted with amniotic membrane showed no signs of inflammatory cell infiltrate or neovascularization. 34 In our study, we showed SCCO2-sterilized amniotic membrane transplantation was not associated with corneal edema, neovascularization or inflammatory cell infiltrate, making it a viable option for corneal grafting as well as for treating corneal wounds and chronic diseases.
In sum, the results of this study show that our unique amniotic membrane SCCO2-sterilization method exhibits in vivo biocompatibility as shown by the absence of inflammation or neovascularization when placed on the eyes of rabbits for up to seven days. Furthermore, we demonstrate that SCCO2-sterilization of amniotic membrane followed by lyophilization maintains the desirable properties of an AM ocular bandage as shown by the maintenance of essential extracellular matrix proteins, growth factors, cytokines and PTX3, the protein believed to the impart wound healing properties seen with the clinical application of amniotic membrane post processing. Taken together, these data suggest this product may be a viable treatment option for corneal surface injuries and provides the foundation for future in vivo studies utilizing lyophilized, SCCO2-sterilized amniotic membrane.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by U.S. Army Medical Research and Development Command (MRDC) Clinical and Rehabilitative Medicine Research Program. The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the U.S. Army Medical Department, Department of the Army, DoD, or the U.S. Government.