
Abstract
Background
The incidence of incisional hernia is with up to 30% one of the frequent long-term complication after laparotomy. After establishing minimal invasive operations, the laparoscopic intraperitoneal onlay mesh technique (lap. IPOM) was first described in 1993. Little is known about the foreign body reaction of IPOM-meshes, which covered a defect of the parietal peritoneum. This is becoming more important, since IPOM procedure with peritoneal-sac resection and hernia port closing (IPOM plus) is more frequently used.
Methods
In 18 female minipigs, two out of three Polyvinylidene-fluoride (PVDF) -meshes (I: standard IPOM; II: IPOM with modified structure [bigger pores]; III: IPOM with the same structure as IPOM II + degradable hydrogel-coating) were placed in a laparoscopic IPOM procedure. Before mesh placement, a 2x2cm peritoneal defect was created. After 30 days, animals were euthanized, adhesions were evaluated by re-laparoscopy and mesh samples were explanted for histological and immunohistochemichal investigations.
Results
All animals recovered after implantation and had no complications during the follow-up period. Analysing foreign body reaction, the IPOM II mesh had a significant smaller inner granuloma, compared to the other meshes (IPOM II: 8.4 µm ± 1.3 vs. IPOM I 9.1 µm ± 1.3, p < 0.001). The degradable hydrogel coating does not prevent adhesions measured by Diamond score (p = 0.46). A peritoneal defect covered by a standard or modified IPOM mesh was a significant factor for increasing foreign body granuloma, the amount of CD3+ lymphocytes, CD68+ macrophages and decrease of pore size.
Conclusion
A peritoneal defect covered by IPOM prostheses leads to an increased foreign body reaction compared to intact peritoneum. Whenever feasible, a peritoneal defect should be closed accurately before placing an IPOM-mesh to avoid an excessive foreign body reaction and therefore inferior biomaterial properties of the prosthesis.
Introduction
The incidence of incisional hernia is with up to 30% one of the frequent long-term complication after laparotomy and may cause pain, discomfort including cosmetic result and a potential danger of incarceration with ileus.1–4 After establishing minimal invasive operations in the early 1990s, the laparoscopic intraperitoneal onlay mesh technique (lap. IPOM) was first described in 1993 by LeBlanc. 5 The advantages and disadvantages of laparoscopic IPOM technique compared to open repair have been discussed in many studies over the years.1,6–9
Every surgical trauma, in particular the implantation of an alloplastic mesh prosthesis in IPOM position holds a high potential of adhesions due to close contact between mesh and intestine.10–12 In vivo, textile meshes are recognized from the (human)organism as a foreign body and covered with scar tissue in a chronic inflammatory, i.e., foreign body, reaction to a greater or lesser extent up to their biocompatibility.13,14 Knowing these facts, it is essential in the evaluation of IPOM meshes to spend differentiated consideration on the parietal site (abdominal wall) and visceral site (intestine) of the mesh. Furthermore, this two-layer approach provides more options of mesh modification e.g. (hydrogel) coating of the visceral-site. 15 In former animal studies, meshes were placed on untouched peritoneum.10,15,16 Therefore, little is yet known about the foreign body reaction of IPOM-meshes, which covered a defect of the parietal peritoneum. Peritoneal defect areas occur regularly during (laparoscopic) adhesiolysis. This is becoming more important, as IPOM procedure with peritoneal-sac resection and hernia port closing (IPOM plus) is more frequently used due to better cosmetic and functional results as lower seroma formation, less mesh bulging and lower long-time recurrence rate.17,18
The aim of our current study was to evaluate the influence of a peritoneal defect area in comparison with intact peritoneum on biocompatibility and adhesion formation of three different IPOM mesh prostheses regarding textile structure and coating
Materials and methods
All experiments were in accordance with the German legislation governing animal studies and the Guide for the Care and Use of Laboratory Animals (National Institutes of Health (NIH), Publication No 85–23, revised 2011). The experiments were approved by the Governmental Animal Care and Use Committee (LANUV, Landesamt für Natur Umwelt und Verbraucherschutz Nordrhein-Westfalen, Recklinghausen, Germany, reference number: 84–02.04.2015.A519. The report of this research was created considering the ARRIVE guidelines. 19
Animals
18 female minipigs (40–50 kg bodyweight) were used in this study. Animals were kept under standardized and hygienic optimized conditions: temperature between 22 °C and 24 °C; relative humidity 50%–60%; and 12 h/12h of light/dark cycle. They had free access to water and were fed 3% of bodyweight/day. Food was withdrawn for 12 h before surgery.
Prosthetic material
Three different IPOM mesh-modifications (10 × 15 cm, each in their original state) with different textile structure and coating were used in this study (Figure1).
A standard, commercially available Dynamesh® IPOM-mesh (10 × 15 cm) made out of PVDF/PP (IPOM I) A newly, experimental PVDF/PP-mesh IPOM II (10 × 15 cm) with modified structure (bigger pores and increased textile porosity with smaller yarn diameter). An experimental mesh with the same structure as IPOM II but in addition with a degradable hydrogel-coating on the visceral-site (IPOM III).
The large-pore IPOM II mesh was coated with a sprayed hydrogel based on porcine gelatin (10% porcine gelatin (Sigma-Aldrich), 7.5% glycerin (J.T. Baker) and aqua valde purrificata). After preparation, the solution was applied with a compressed-air spray coating system in a closed chamber with evacuation of the overspray. Afterwards, the coated mesh was placed in a drying chamber until residual moisture content reached 14–16%. The sprayed-on gelatine does not form a closed film, but envelops each individual fibre with an average thickness of the coating of 7 µm. The degradability of the coating is approximately 72 h. This means that an initial, but slightly reduced porosity, is retained also in the early postoperative period.
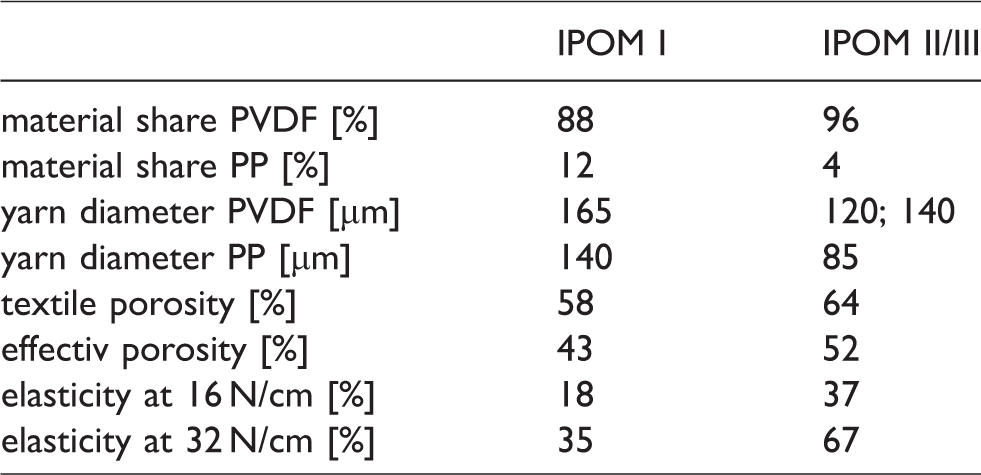
Table 1 describes the textile characteristic of the used meshes:
Textile characteristic of the used mesh prosthesis (IPOM III without hydrogel-coating).
Surgical procedures
Operations were carried out under general anesthesia, aseptic and sterile surgical conditions, and were performed by two independent surgeons.
Anesthesia was induced by a combination of 1% Atropine sulfate (10 mg/ml Atropin® Dr. Franz Köhler Chemie, Bensheim, Germany) and Azaperon (Stresnil® Elanco, Bad Homburg, Germany) i.m. After 15 minutes Ketamine 10% (Ketamin® Medistar, Ascheberg, Germany) was injected i.m. and before intubation additionally Propofol® 1% (Propofol Claris®, Phamore, Ibbenbüren, Germany). Further anesthesia and analgesia was ensured by inhalation of an isofluran (Baxter, Unterschleißheim, Germany) - (1.5 vol. %) - oxygen (30%) – air - mixture and fentanyl (Rotexmedica, Trittau, Germany).
Minipigs were fixed in a supine position and skin was shaved and disinfected with polyvidone-iodine solution (Braunosan Vet®, Braun Vet Care, Tuttlingen, Germany). No antibiotics were given.
After aseptic covering, we performed a laparoscopic implantation of two different and randomized IPOM-meshes with 6 transfascial sutures in each minipig. First, the mesh-outline including the fixation points was drawn on the skin. After implementation of pneumoperitoneum, two peritoneal defects of 2 × 2 cm were cut out (Figure 2).
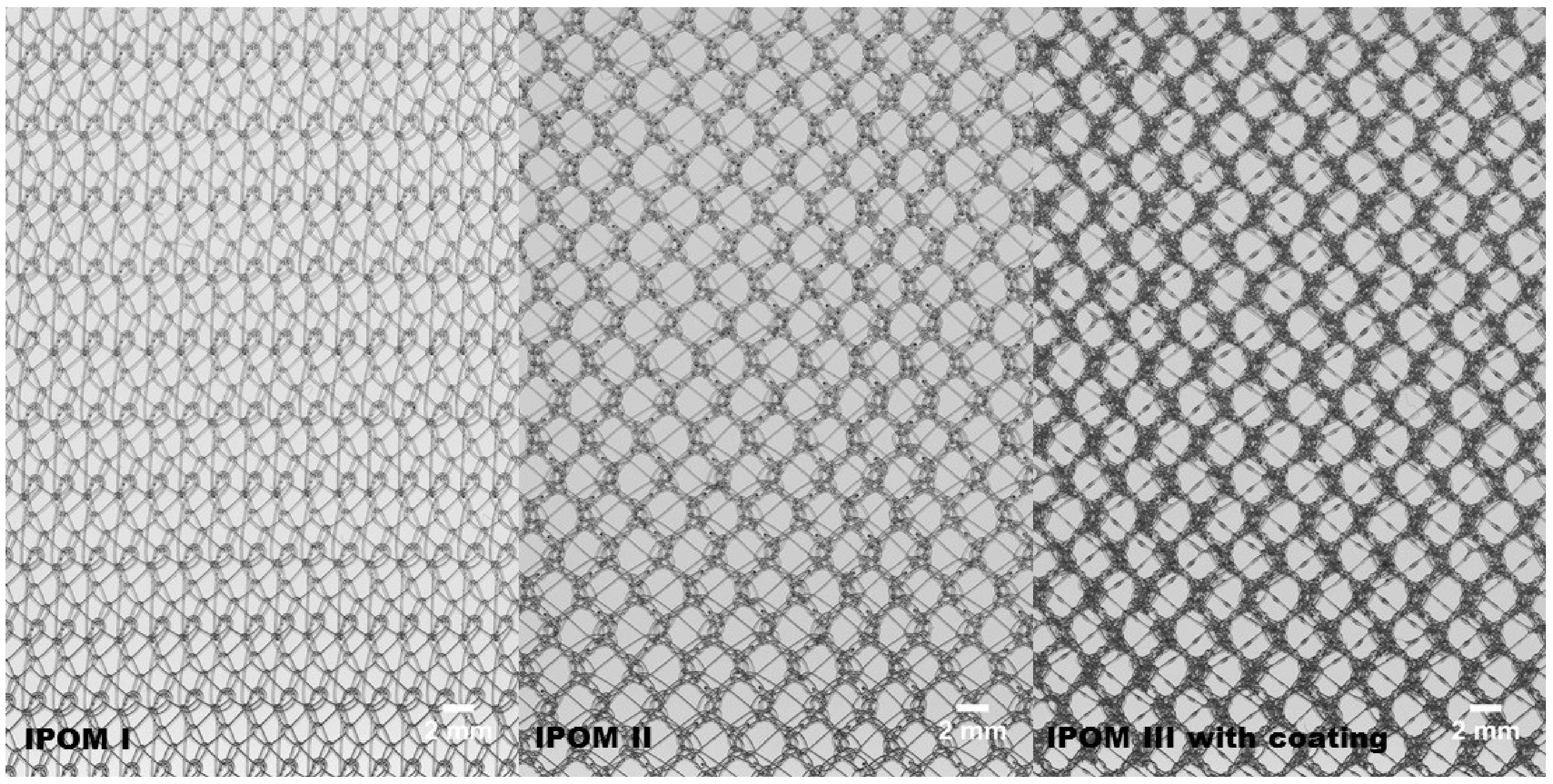
Textile composition of standard Dynamesh IPOM and modified meshes (Camera: AM-1600 GE, JAI Ltd., Denmark).
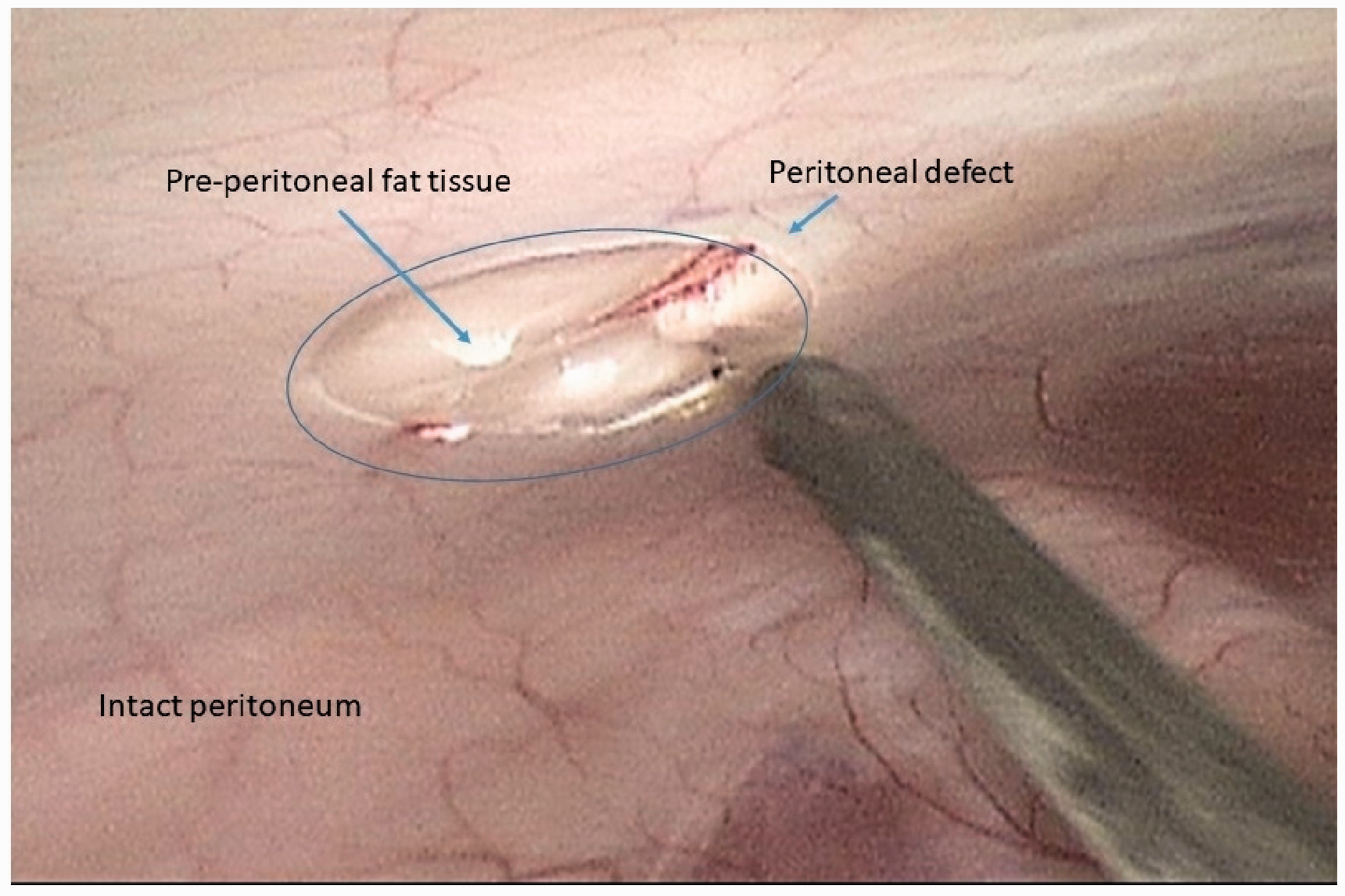
Peritoneal defect in situ. Laparoscopic view 30° to the top on the left lower quadrant.
Then one mesh on the left and one on the right site were placed and the defect was covered in each case by the central underpart of the mesh. Fixation of the meshes was ensured by 6 transfascial sutures (PVDF, multifilamental, USP 2–0) after deflation of pneumoperitoneum (Figure 3).
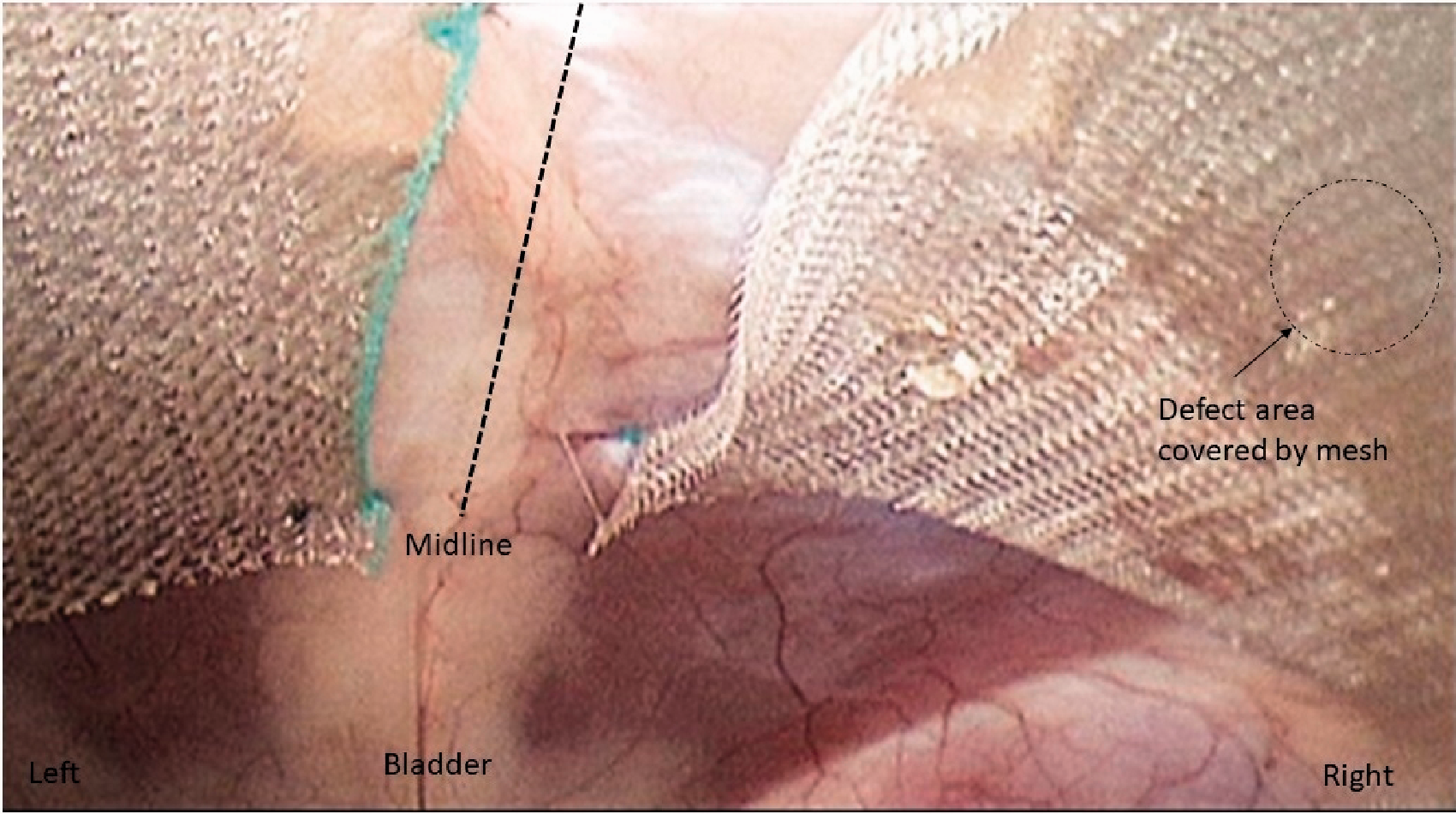
Fixed meshes in situ. Laparoscopic view 30° to the top on the lower abdomen.
Postoperative analgesia was ensured by 2 mg/kg BW flunixin meglumine (Finadyne®, MSD) i.m. injection directly after the operative procedure and repeated every 24 h for 72 h.
Welfare of the animals were assessed on daily basis by a structured score sheet (covering tachypnoe, dyspnoe, hypophagia, fasting, hypoactivity, surgical site infection, peritonitis, ileus).
After 30 days, animals were euthanized by an overdose Pentobarbital (Narcoren®) after establishing general anesthesia and complete exploring of the abdominal cavity by re-laparoscopy. Adhesion formations were scored differentiated for defect area and intact peritoneum in consensus by two observers by using an established score from Diamond et al. 20 Shrinkage of the meshes in comparison to the original state were determined by calculating the surface area after euthanasia and explantation of the meshes. Tissue samples of the defect area and the intact peritoneum-mesh interface were taken for histological and immunohistochemical investigations.
Histology and immunohistochemistry
Histological and immunohistochemical investigations were performed on paraffin embedded 3 µm sections after fixation of the samples for 48 h in 4% formalin. Sections were obtained from the mesh-peritoneal defect area and from intact peritoneum- mesh area out of each tissue-sample.
All sections were routinely stained with haematoxylin and eosin. The amount of inflammatory and connective tissue formation was analyzed by measuring the diameter of the inner and outer foreign body granuloma (FBG) representing the inflammatory infiltrate and the fibrotic tissue reaction. After capturing 8 granuloma per sample with a digital camera (Olympus C-3030, Hamburg, Germany), 2 separate measurements from the outer margin of a yarn junction granuloma were performed with the help of a digital image analyzing software (Image-Pro Plus, Media Cybernetics, Silver Spring, MD, USA) according to Klink et al. 21 (Figure 4). Pore-sizes were measured as distance from filament to filament 3 times in each sample. Furthermore, fibrotic bridging was assessed whether the inflammatory infiltrate (granuloma) was confluent between the pores or not.
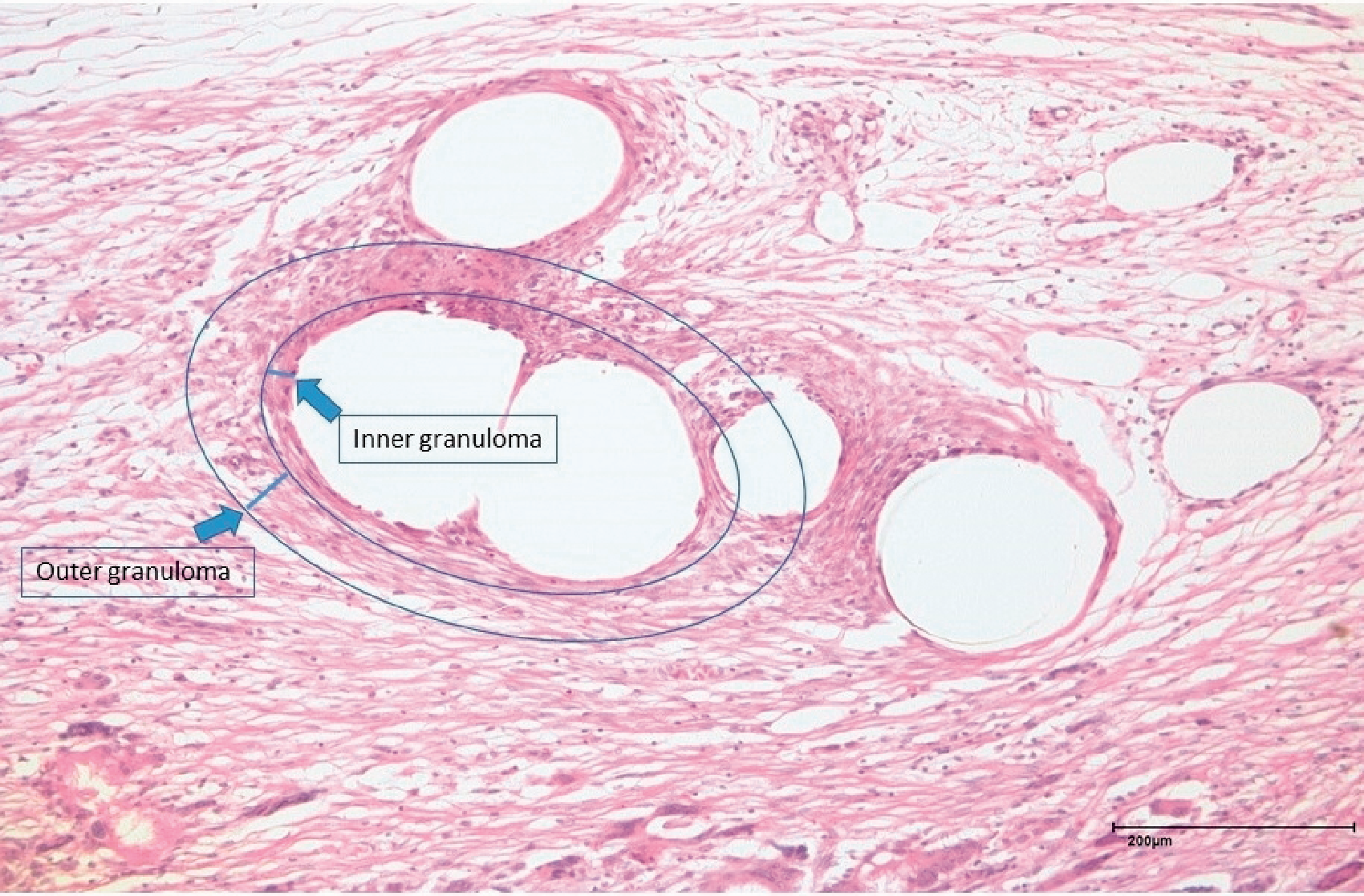
Schematic illustration of the inner and outer foreign body granuloma of a yarn junction. Mesurements were performed at the outer margin (100× magnification).
Immunohistochemistry was used to analyze the host response with the same differentiated investigation as described before. After pretreatment of the fixed specimen with microwave and citrate-buffer pH6 for three times, cells were identified by different monoclonal antibodies from Dako (Glostrup, Denmark). The inflammation was assessed by counting the number of macrophages (CD68 expression) and T-lymphocytes (CD3 expression) in the foreign body granuloma. As a marker for mesenchymal cells, Vimentin expression was measured. All sections were examined by standard light microscopy (Olympus BX51, Olympus, Hamburg, Germany).
The expression of immunohistochemical parameters was classified by two independent, blinded observers using a semi-quantitative immunoreactivity score (IRS) modified after Remmele et al. . 22 Intensity of staining was scored as 0 (0–5%), 1 (5–30%), 2 (30–80%) and 3 (80–100%), indicating the percentage of positive stained cells in a visual field.11,23
Statistical analysis
To test, whether the factor “IPOM type” has an effect on the outcome variables (“shrinkage”, “Diamond-score”), we first performed, separately for each outcome, a 1-way Analysis of Variance (ANOVA). Differences between the individual levels, i.e., IPOM types were then assessed by pairwise comparisons of means. Differences were deemed statistically significant at p < 0.05, corrected for multiple comparisons using Tukey's honest significant difference criterion.
For all other outcome variables, we performed a 2-way ANOVA including the factors “IPOM type” and “location (Mesh with intact peritoneum/defect)”, modelling both main effects and their interaction. The main effect describes the specific effect of a factor (type of mesh; intact peritoneum or peritoneal defect) regardless of other factors in the study. Differences between the individual factor levels were assessed by pairwise comparisons of marginal means. Differences were again considered to be statistically significant at p < 0.05, corrected for multiple comparisons using Tukey's honest significant difference criterion.
Results
All animals survived the operation procedure and recovered without any complications or particularities after the operation. In the follow-up period of 30 days, we observed no surgical site infection or problems due to the implanted meshes.
Foreign body reaction
We observed no fibrotic bridging between the pores in all groups and the granuloma surrounded only single mesh-filaments. Furthermore, the peritoneal defect area leads to a distinctive and increased inflammatory reaction and cellular response (Figure 5).
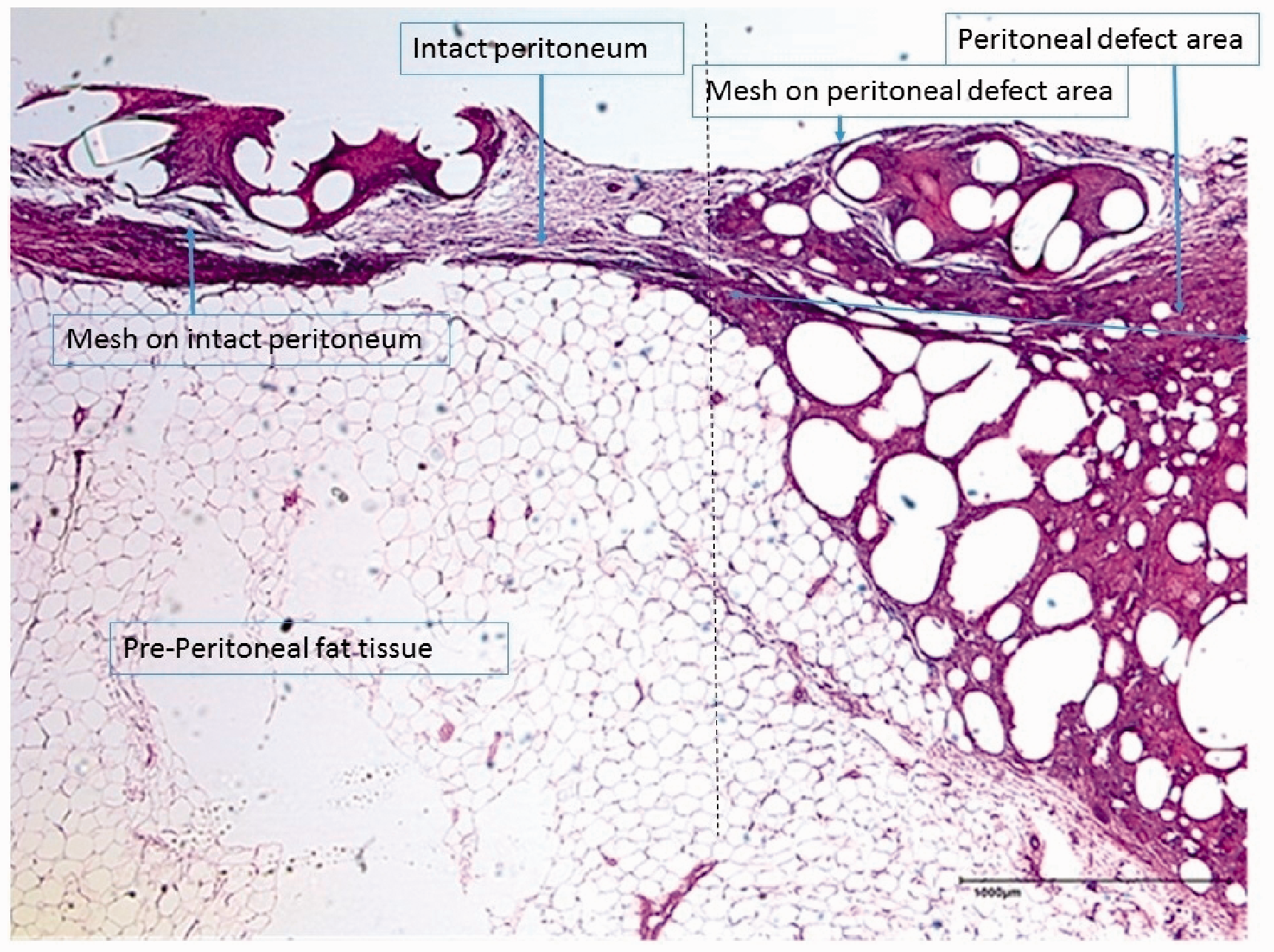
Cellular reaction intact peritoneum/peritoneal defect area (25× magnification).
Inner and outer granuloma
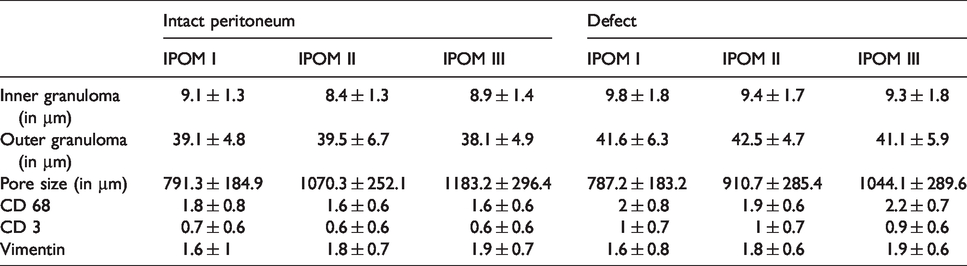
Analyzing the size of inner granuloma, which comprises most of the inflammatory cells, shows that regarding the main effect “mesh” IPOM II had a significant smaller inner granuloma compared to the other meshes (IPOM II: 8.4 µm ± 1.3 vs. IPOM I 9.1 µm ± 1.3, p < 0.001; vs. IPOM III 8.9 µm ± 1.4, p = 0.04). Furthermore, the peritoneal defect was a significant factor for increase of inner granuloma regardless type of mesh (p < 0.001, IPOM I: 9.8 µm ± 1.8; IPOM II: 9.4 µm ± 1.7; IPOM III: 9.3 µm ± 1.8). There was no interaction between the main effects (p = 0.25). Concerning the outer granuloma, we found no significant difference between the main effect “mesh” (p = 0.06, IPOM I: 39.1 µm ± 4.8; IPOM II: 39.5 µm ± 6.7; IPOM III: 38.1 µm ± 4.9). As before, a peritoneal defect (main effect) was a significant factor for increase of outer granuloma regardless the type of mesh (p < 0.001, IPOM I: 41.6 µm ± 6.3; IPOM II: 42.5 µm ± 4.7: IPOM III: 41.1 µm ± 5.9). There was no interaction between the main effects (p = 0.87), (Table 2).
Foreign body granuloma and immunhistochemistry analysis.
Pore size
Analyzing the distance between the filaments (pore size) IPOM III had significant bigger pores compared to all other meshes (IPOM III: 1183.2 µm ± 296.6 vs. IPOM II 910.7 µm ± 285.4, p = 0.02; IPOM I 791.5 µm ± 184.9 vs. IPOM II p < 0.001). A peritoneal defect is a significant factor for decreasing pore size and independent of mesh type (p = 0.01, IPOM I 787.2 µm ± 183.2; IPOM II 910.7 µm ± 285.4; IPOM III 1044.13 µm ± 289.6). There was no interaction between the main effect “mesh” and “intact/defect peritoneum” (p = 0.18) (Table 2).
Adhesions/mesh-shrinkage
Diamond-Score
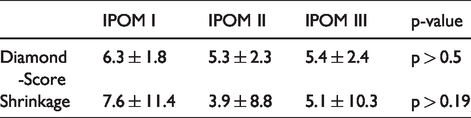
By scoring intraperitoneal adhesions between intestine and meshes using the Diamond-Score, we found no significant difference between the groups (p = 0.46, IPOM I: 6.3 ± 1.8; IPOM II: 5.3 ± 2.3; IPOM III: 5.4 ± 2.4) (Table 3) and no difference between peritoneal defect area and intact peritoneum.
Shrinkage in % and adhesions measured by diamond-score.
Shrinkage
There was no significant difference regarding shrinkage of meshes after explantation between the groups (p = 0.20, IPOM I: 7.6% ± 11.4; IPOM II: 3.9% ± 8.8; IPOM III: 5.1% ± 10.3) (Table 3).
Immunohistochemistry
CD 3
There was no significant difference between the amount of CD3 positive cells between the three mesh groups (p = 0.82, IPOM I: 0.7 ± 0.6; IPOM II: 0.6 ± 0.6; IPOM III: 0.6 ± 0.6). A peritoneal defect is a significant factor of increasing the amount of CD3 positive cells regardless the type of mesh (p < 0.001) without significant difference between the mesh groups and interactions between the main effects (p = 0.81) (Table 2).
CD 68
There was no significant difference between the amount of CD68 positive macrophages between the three mesh groups (p = 0.2, IPOM I: 1.8 ± 0.8; IPOM II: 1.6 ± 0.6; IPOM III: 1.6 ± 0.6). The peritoneal defect was as well a significant factor of increasing the amount of macrophages regardless the type of mesh (p < 0.001) without significant difference between the mesh groups and interactions between the main effects (p = 0.13) (Table 2).
Vimentin
The expression of vimentin as a marker of mesenchymal cells and cell integrity is physiologically increased after (peritoneal) trauma. IPOM I group had a significant lower amount of vimentin positive cells compared to IPOM III (p = 0.02, IPOM I: 1.6 ± 1; IPOM III: 1.9 ± 0.7). The peritoneal defect was no significant factor of increasing the amount of vimentin (p = 0.87) and there was either no significant difference between groups or interaction between the main effects (p = 0.98) (Table 2).
Discussion
Since the first description of laparoscopic IPOM-technique without hernia-sac resection or fascial closure in 1993 by Leblanc et al., abdominal wall hernia are repaired worldwide every day by using this technique. 5 This original technique of only covering the hernial orifice by a mesh prosthesis may cause seroma, mesh bulging and cosmetically distracting results of the abdominal wall.17,18 Therefore, in the last decade more IPOM procedures with resection of the hernia-sac and fascial closure (IPOM plus) were performed and became increasingly the norm. Christoffersen et al. showed a significant reduction of seroma and hernia recurrence in an RCT by using a fascial closing covered by a mesh prosthesis in umbilical hernias. 18 So far and referring to our aim of this study, there is no clear evidence of biocompatibility respectively cellular reaction of mesh prosthesis, which covered a peritoneal defect area.
The key finding of our study was that a peritoneal defect is in comparison to intact peritoneum a significant factor for increasing the inner and outer granuloma and for decreasing the meshes pore size independent of the type of mesh used. Furthermore, also on immune-response level a peritoneal defect covered by a mesh prosthesis is a significant factor for increasing the amount of CD 68 positive macrophages and CD 3 positive T-lymphocytes.
Biocompatibility of textile mesh prosthesis is a multi-factorial event and it is mostly defined by polymer, surface, geometry and composition, respectively pore-size.24–26 The biocompatibility of the reference PVDF-IPOM mesh is already evaluated and well described in previous studies. 27 Our current findings regarding foreign body reaction of meshes on intact peritoneum goes in line with these results. 28 In line with the results of Jerabek et al. who evaluated the influence of pore size of polypropylene meshes on the inflammatory reaction, our PVDF-IPOM II mesh with modified structure (bigger pores) had a significant smaller inner granuloma -which compromised most of the inflammatory cells- compared to the standard PVDF-IPOM I mesh (p < 0.001) . 29 Interestingly the IPOM III mesh with the same modified structure as IPOM II but in addition equipped with a degradable-hydrogel coating had a significantly larger inner granuloma compared to IPOM II (p = 0.04) which is attributable to the coating. To our knowledge, it was the first time that a biodegradable-hydrogel coating was used on a PVDF mesh. Therefore, there are no reference-values regarding biocompatibility and tissue response of this combination. In contrast to our results Poppas et al. examined in a rat model a non-degradable hydrogel coating in combination with a polypropylene mesh and found a significant decrease in foreign body reaction in comparison to an uncoated polypropylene mesh. 15 On the one hand, uncoated polypropylene shows an increase in inflammation especially in IPOM position in comparison to PVDF and it is therefore not recommended for direct contact with the viscera. 14 On the other hand, they used indeed a hydrogel coating but with a polyurethane and not a collagen background. In generally, coatings could be a potential method to modify biocompatibility of a mesh prosthesis according to the original performance of the raw material. 30
To come back to the initial question of resection of the hernia sac and fascial closing. Our results indicate an increased inflammatory- and foreign body reaction regardless the mesh type used in the area of the peritoneal defect. Therefore, our study suggests that accurate closing the parietal peritoneum in addition to fascial, respectively hernia port closing before placing an IPOM is recommended, as it enhances biocompatibility.
As a limitation of our study, results generated by animal experiments cannot be transferred directly to human application. On the other hand, the abdominal wall of minipigs are well comparable to humans and we used a standard Dynamesh IPOM prostheses which is approved for human application. Thus, we are committed that we got evidence how foreign body reaction can potentially be reduced in case of IPOM (plus) procedure.
Conclusion
A peritoneal defect covered by IPOM prostheses leads to a distinctive and increased foreign body reaction compared to intact peritoneum. Whenever feasible, a peritoneal defect in addition to the fascia should thus be accurately closed before placing an IPOM-mesh to avoid overspill immune reaction.
Footnotes
Availability of data
The datasets analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RE, AK, SE, MH, TR, UP, CK, AL: nothing to declare; UK: grants from Research projects in collaboration with Ethicon and FEG, personal fees from Ethicon and FEG, personal fees from expert testimony.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was granted by the BMBF (Federal Ministry of Education and Research) (Funding number: 13N12599.