
Abstract
To investigate the biocompatibility of polylactic acid-glycolic acid copolymer (PLGA) and PLGA/gelatin scaffolds and their suitability for tubular urethral replacement in a canine model. PLGA and PLGA/gelatin scaffolds was constructed by electrospinning. Microstructural differences between the scaffolds was examined by Scanning electron microscopy (SEM) followed by mechanical properties testing. Biocompatibility of the material was evaluated using SEM 4, 8, 12 and 72 h after PLGA and PLGA/gelatin scaffolds co-culture with urothelial cells. And confocal analysis was also used to showed the cell adhesive and growth at 12 h. Approximately 2 cm of the anterior urethra of twelve dogs were removed and replaced with a scaffold. After the surgery for 1 month performed urethrography and for 3 month perform hematoxylin–eosin (H&E) and Masson. The results indicated that PLGA and PLGA/gelatin scaffolds had a void microfilament structure, similar to that of normal acellular matrix tissue. And the tensile strength was decreased whereas the tensile deformation and suture retention strength was increased in PLGA/gelatin scaffolds compared to that in PLGA scaffolds Urothelial cells grew well on both scaffolds. Postoperatively, animals recovered well and urinated spontaneously. However, urethrography showed varying degrees of urethral strictures in the reconstructed urethras. H&E and Masson showed that multilayer urothelial cells were formed in both the proximal and distal segments of the reconstructed urethras but without continuity. There was a small amount of smooth muscle and blood vessels under the epithelium, but regenerative urothelial cells at the midpoint of the reconstructed segment did not continue. Lots of lymphocyte infiltration was observed under the epithelium, some collagen tissue was deposited under the neo-urethral epithelium were observed. In conclusion, PLGA and PLGA/gelatin scaffolds are not suitable for tubularized urethral replacement in the canine model.
Keywords
Introduction
Reconstruction of the urethra is important for the treatment of common urological diseases such as hypospadias and urethral strictures. However, the reconstruction of long urethral segments is a challenge for urological surgeons.1,2 The main problem is limitations in the source of autologous non-urinary system grafts, such as the foreskin, oral mucosa, and bladder mucosa; there is not enough autologous tissue available to construct long urethral replacements, especially for patients who undergo repeated operations. 3 In the field of tissue engineering technology, the provision of non-autologous materials for urethral reconstruction to avoid shortages of source materials has become the subject of considerable interest in recent years. Two types of tissue engineering scaffold materials are used for urethral reconstruction: decellularized tissues, such as small intestine submucosa (SIS) and bladder acellular mucosa (BAM), and synthetic scaffolds, such as polylactic acid (PLA), PLA-glycolic acid copolymer (PLGA), poly(trimethylene carbonate) (PTMC) and collagen. It is also possible to use a conjugation of the materials and cells. 4
Synthetic scaffolding is most commonly used in clinical surgeries, because its degradation rate and mechanical properties can be adjusted, and it is less likely to carry antibodies and viruses than natural tissue. 5 Because of the different molecular structures and diverse manufacturing process of synthetic scaffolds, however, most of the studies using synthetic scaffolds for urethral reconstruction have used animal models, and few studies have been conducted to compare different synthetic scaffolds. 6 Few studies or randomized controlled clinical trials have been conducted into the application of synthetic scaffolds. 7 The scaffolds used to reconstruct the urethra in animal models are shaped into membranes, and the defects in these experiments are patchy, rather than tubularized, a phenomenon that greatly limits the application of synthetic materials in clinical surgeries. Although several studies have been conducted into the reconstruction of tubular urethral defects, the method used has been to simply sew the membrane into a tube. However, collapse of the membrane scaffolds due to defects in the material, or to gradual degradation of the material after implantation, may lead to strictures in the reconstructed urethra. Therefore, in this study, we used electrospinning to construct tubular PLGA and PLGA/gelatin scaffolds. To investigate the feasibility of using tubularized scaffolds in urethral reconstruction, the scaffolds were used to reconstruct a 2 cm urethral defect in a canine model. Cell experiments in vitro were applied to examine the biocompatibility of the scaffolds.
Materials and methods
Materials
Polylactic-glycolic acid (molar ratio 50:50), gelatin, and hexafluoroisopropanol were purchased from Aladdin (Aladdin Reagent Co. Ltd. China). The animal experiments were approved by the Institutional Animal Care and Use Committee of Guangzhou Medical University, Guangzhou, PR China. The study was performed following the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85–23, revised 1996).
Preparation of polylactic acid-glycolic acid copolymer, polylactic acid-glycolic acid copolymer/gelatin (mass ratio 3:1) scaffolds using electrospinning
PLGA and PLGA/gelatin (mass ratio 3:1) were dissolved in hexafluoroisopropanol to obtain the spinning solution. In an electrostatic spinning machine, a rotating roller with a diameter of 3 mm and a length of 15 cm was used as a collector. The distance from the spinneret to the cylinder was 10 cm, the speed was 2000 r/min, and the voltage was 15 kV. The nanofiber stent was removed after spinning for 1 h, and the cylinder was dried in an oven at 50 °C for 2 h to remove residual solvents. PLGA and PLGA/gelatin tubular scaffolds with a thickness of 0.3 mm were obtained. The scaffolds were vacuum sealed and gamma irradiated using a 60Co source.
Mechanical properties testing
The PLGA and PLGA/gelatin tubular scaffolds were cut into a specific size (1 cm × 6 cm). Then tensile strength and tensile deformation was measured using universal mechanical testing machine (EXCEED Model E43, MTS, USA) with a velocity of 200 mm per min. The average values of ten samples (five repeats for each samples) were calculated and compared.
The suture retention strength was detected as follows: a 4–0 suture to thread through the scaffolds at 2–3 mm from the edge, then suture to a semi-ring, and pull out the suture at a speed of 200 mm per min. After that, record the force pulling out from the scaffolds or damaging the scaffolds.
Culture of urothelial cells on PLGA and PLGA/gelatin scaffolds
Human urothelial cells were obtained from Shanghai Zhong Qiao Xin Zhou Biotechnology Co., Ltd (Shanghai, China). Cells were cultured to 70%–80% confluence in a 25 cm2 culture flask and then transferred to a 24-well plate. The two materials (PLGA and PLGA/gelatin) were cut into pieces of 1.5 cm × 1.5 cm and placed on the bottom of each plate under sterile conditions. The membranes were seeded with cells (5 × 104) and incubated with 1 ml Dulbecco’s Modified Eagle’s Medium with 10% fetal bovine serum.
Scanning electron microscopy (SEM) and confocal analysis
SEM (S-3400N, Hitachi Limited, Japan) was performed to evaluate the microstructure and morphology of the scaffolds and the cell membranes. Differences in the spinning diameters of the PLGA and PLGA/gelatin scaffolds were observed. After fixing with paraformaldehyde, urothelial cell-seeded membranes were incubated in different ethanol solutions (0%, 10%, 20%, 30%, 40%, 50%, 70%, 85%, 95%, and 100% ethanol) for 5–10 min until all water was removed and then dried under vacuum. A coater was used to coat the membranes with gold/palladium for 2 min, and SEM photographs were taken. The situation of cell adhesive and growth were also observed using confocal microscope (LSCM; LSM510, Carl Zeiss, Germany) after the 12 h urothelial cell-seeded membranes were stained with rhodamine-conjugated phalloidin and DAPI. The regent of actin-tracker red-rhodamine and DAPI solution was purchased from Beyotime Biotechnology (Shanghai, China).
Animal model and surgical procedure
Twelve adult male dogs were randomly divided into two groups, the PLGA group (n = 6) and the PLGA/gelatin group (n = 6). Dogs were prepared in a supine position, and general anesthetic was administered intravenously using pentobarbital sodium. The dogs were catheterized using a 6 F single-lumen catheter. A tourniquet was placed at the root of the penis. A longitudinal incision approximately 2.5 cm in length was then created at 1 cm from the head of the penis, and the urethra was exposed. The proximal end of the catheter was transected, and the distal catheter was pulled out through the incision and inserted with a 2c stent. The proximal segment of the urethra was transected, and approximately 2 cm of normal urethra was removed. The synthetic scaffold was interposed between the two cut ends of the urethra and anastomosed with 6/0 bioabsorbable poly sutures. The catheter was passed from the proximal end of the scaffold to the distal end of the urethra. Finally, the incision was closed, and the tourniquet was removed. The average operation time was 35 ± 10 min. All animals were treated with metronidazole orally for 2 weeks, and the catheter was retained for 2–4 weeks.
Retrograde computed tomography (CT) urethrograms after operation
A retrograde CT urethrogram was performed 1 month after the operation, under general anesthesia with pentobarbital sodium. A 6 F catheter was placed through the distal end of the urethra. Meglumine diatrizoate was injected to permit visualization of the entire urethra. CT scans and three-dimensional reconstructions were performed.
Histological assessment
All animals were euthanized 3 months after the operation. The penis of each dog was dissected, and the reconstructed urethras were removed. The reconstructed urethral tissues were fixed with formalin, embedded with formaldehyde, and serial sections of 5 µm thickness were obtained. Tissue sections were then deparaffinized and hydrated, and α-SMA immunohistochemical staining was performed. The sections were stained with hematoxylin–eosin (H&E) and Masson staining to compare the histological structure of the proximal end, midpoint, and distal end of the reconstructed urethras. The tissues were incubated overnight at 4 °C with primary antibody Anti-alpha smooth muscle Actin mouse mAb (α-SMA; Servicebio, Wuhan, China) and subsequently incubated with anti-mouse IgG-HRP (Servicebio, Wuhan, China) for 1 h. Sections were observed under the microscope, and pictures were collected.
Results
Fabrication of PLGA and PLGA/gelatin scaffolds
Both PLGA and PLGA/gelatin scaffolds were made using electrospinning. SEM showed that the electrospun PLGA and PLGA/gelatin scaffolds had a disorderly arrangement of fibers with a uniform diameter, a multi-voided structure, and a porosity greater than 85% (Figure 1(a) to (d)). The mean diameter (Figure 1(e)) and pore size (Figure 1(f)) of the PLGA scaffolds were 716.15 ± 264.85 and 017.82 ± 661.87 nm. The mean diameter (Figure 1(g)) and pore size (Figure 1(h)) of the PLGA/gelatin scaffolds were 1085.77 ± 294.08 and 4935.31 ± 1702.14 nm. Then the mechanical properties were tested and the results showed that the tensile strength was decreased whereas the tensile deformation and suture retention strength was increased in PLGA/gelatin scaffolds compared to that in PLGA scaffolds (Figure 1(i)).
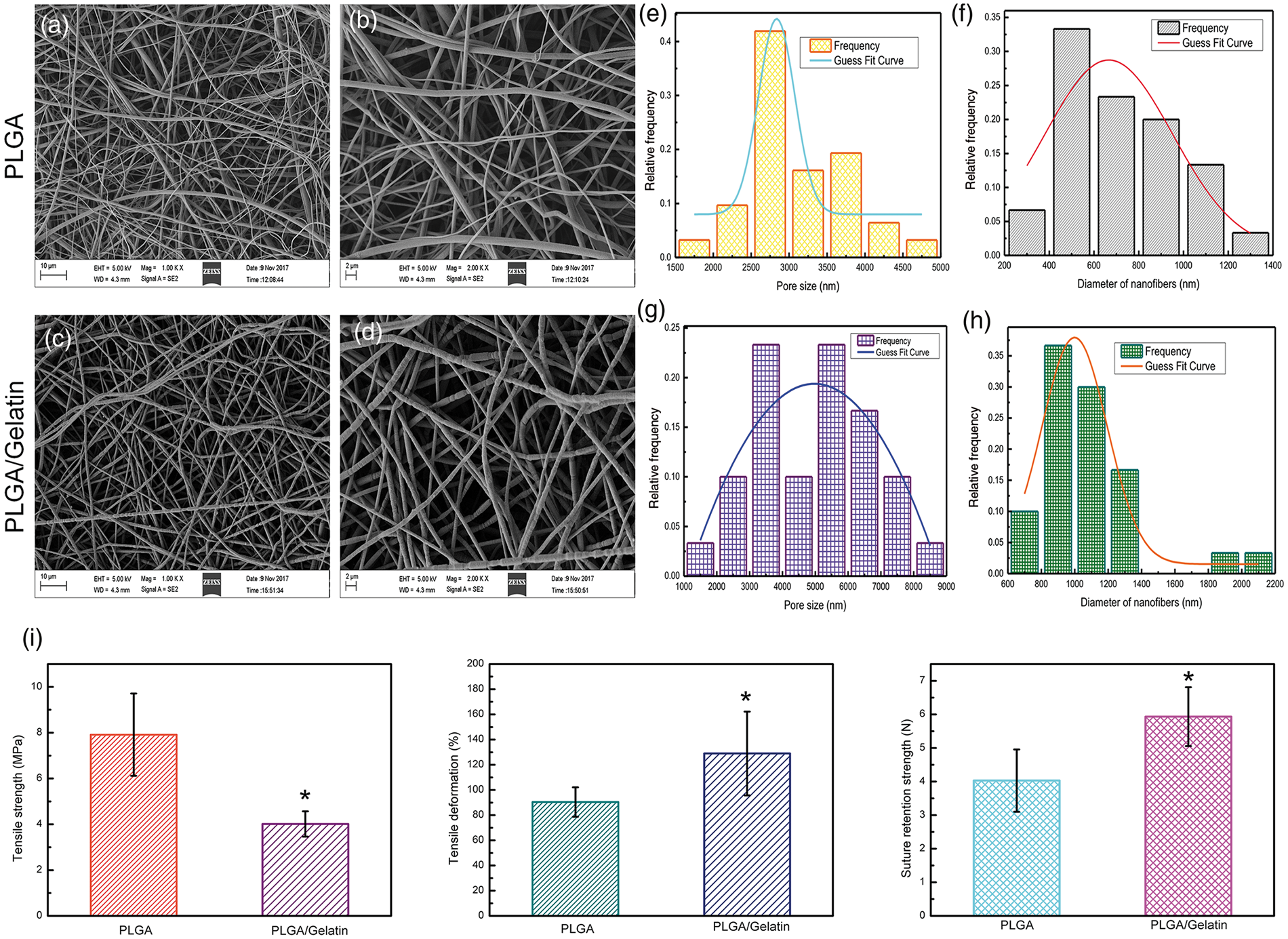
SEM image and mechanical properties of PLGA and PLGA/gelatin scaffolds. SEM image of electrospun PLGA scaffolds, scale bar length 10 μm (a) and scale bar length 2 μm (b). Mean pore size (e) and mean diameter (f) of electrospun PLGA scaffolds. SEM image of electrospun PLGA/gelatin scaffolds, scale bar length 10 μm (c) and scale bar length 2 μm (d). Mean pore size (g) and mean diameter (h) of electrospun PLGA/gelatin scaffolds. (i) The mechanical properties of PLGA and PLGA/gelatin scaffolds including tensile strength, tensile deformation, and suture retention strength. *, P < 0.05.
Cellular adhesion and proliferation
Human urothelial cells were seeded on PLGA and PLGA/gelatin membranes. Cell attachment was examined by SEM after seeding for 4, 8, 12, and 72 h. After 4 h (Figure 2(a) and (b)), SEM showed that scattered human urothelial cells, of polygonal or elliptical shape, developed with pseudopodia and adhered tightly to the surface of the scaffolds. After 8 h (Figure 2(c) and (d)) and 12 h (Figure 2(e) and (f)), the number of adherent cells was significantly increased. And after 72 h (Figure 2(g) and (h)), increasing numbers of adherent cells fused into pieces and secreted more matrix particles. So we selected 12 h urothelial cell-seeded membranes for further confocal analysis. Results showed that urothelial cell grew evenly on the surface of the two scaffolds and showed good cell activity (Figure 2(i)).
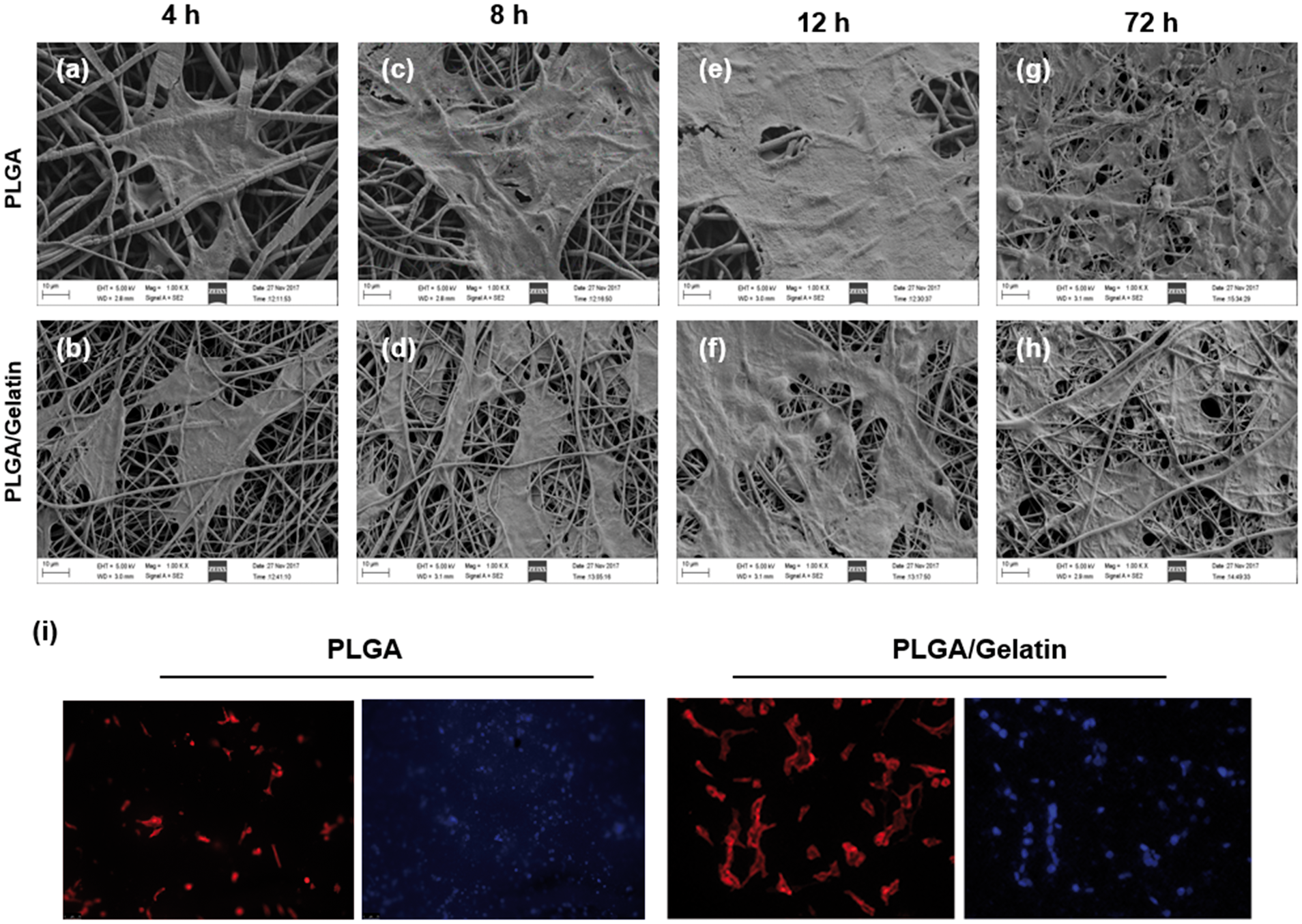
SEM and confocal images of urothelial cell attachment on PLGA and PLGA/gelatin scaffolds. Cells were seeded and cultured with PLGA scaffold for 4 h (a), 8 h (c), 12 h (e), and 72 h (g). Cells were seeded and cultured with PLGA/gelatin scaffolds for 4 h (b), 8 h (d), 12 h (f), and 72 h (h). Cell attachment was examined using SEM images, scale bar length 10 μm. (i) The urothelial cell activity at 12 h cultivation on the PLGA and PLGA/gelatin scaffolds was also detected using confocal analysis after rhodamine-conjugated phalloidin and DAPI staining, scale bar length 75 μm.
Surgical outcome and radiological assessment
To evaluate the suitability for tubular urethral replacement in the canine model, approximately 2 cm of normal urethra was removed (Figure 3(a)). The synthetic scaffold was interposed between the two cut ends of the urethra and anastomosed with 6/0 bioabsorbable poly sutures (Figure 3(b)). Dogs in both the PLGA and PLGA/gelatin groups recovered well, with no deaths. All dogs received metronidazole orally for 1 week after the surgery. There was a dog accidentally lost the catheter 26 h after the surgery in the PLGA group, so it was re-catheterized with a 6 F catheter under general anesthesia, which was left in place for 15 days after re-catheterization. While the other dogs in the PLGA group, the catheters was left in place 2–4 weeks. Although the dogs urinated spontaneously, CT urethrograms and three-dimensional reconstructed images showed that all dogs from both the PLGA (Figure 3(c) and (e)) and the PLGA/gelatin groups (Figure 3(d) and (f)) suffered from varying degrees of urethral stricture. One dog from the PLGA group developed penile–urethral incision infection, leading to infection and necrosis of the penile head. No infection was observed in the other dogs. One dog from each group developed a urethral fistula.
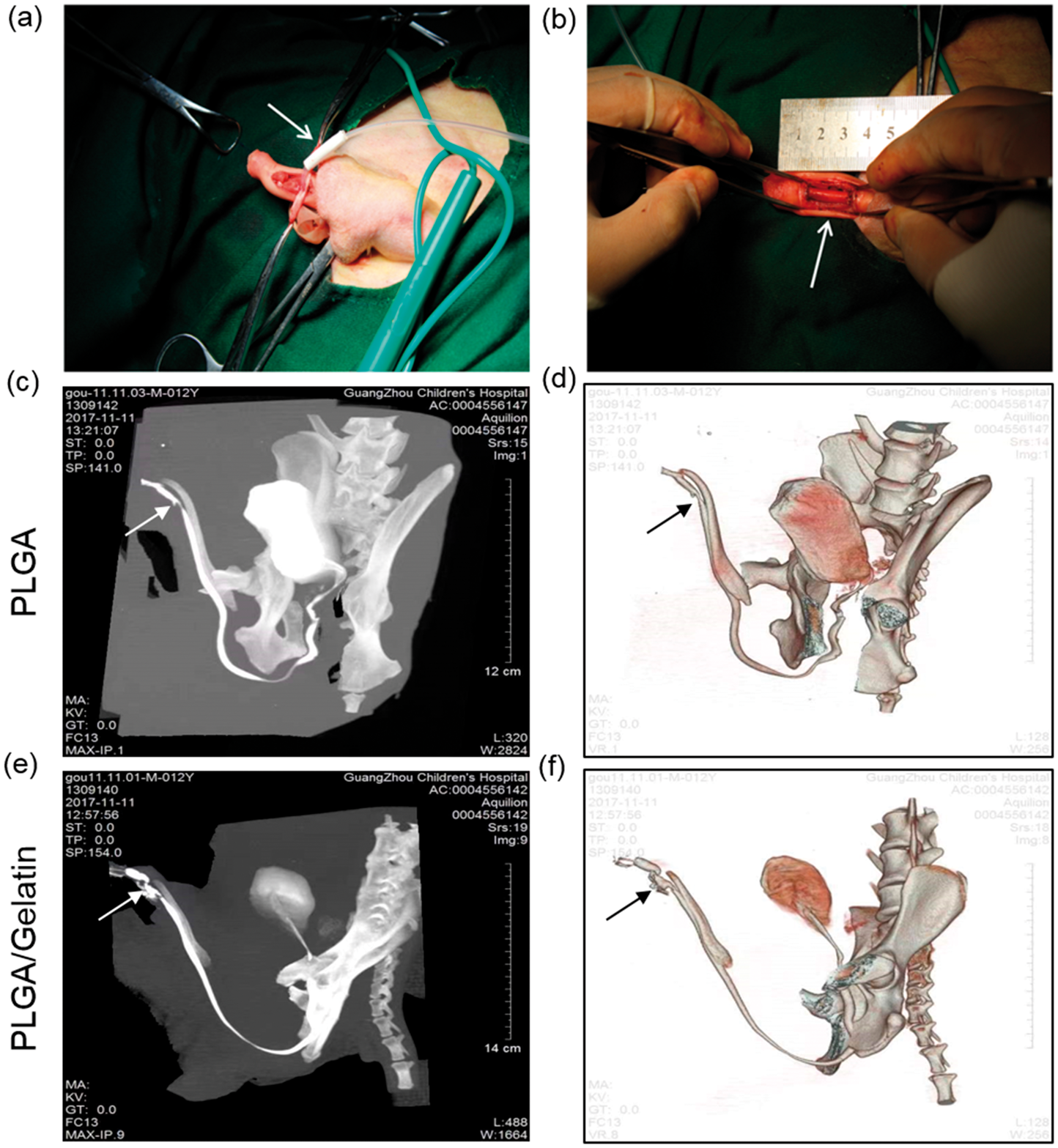
(a, b) Images of tubular urethral replacement in the canine model. All animals showed strictured urethra using two-dimensional computed tomography (CT) urethrocystography (c, d), three-dimensional reconstructed images (e, f) obtained at postoperative day 30 (bottom arrow).
Histological assessment
Dogs were euthanized 3 months after the surgery. Complete penises were obtained from each dog in the PLGA (Figure 4(a)) and PLGA/gelatin groups (Figure 4(b)), and the reconstructed urethras were dissected. Extensive scar tissue was observed in both groups, which formed strictures, although the reconstructed urethras were unobstructed. H&E staining was conducted at the proximal, midpoint, and distal segments of the reconstructed urethras. Multilayered urothelial cells were formed in the proximal (Figure 4(c) and (d)) and distal segments (Figure 4(g) and (h)) in the two groups but did not persist. There was a small amount of smooth muscle tissue and vasculature under the epithelium. H&E staining of the midpoint segment (Figure 4(e) and (f)) showed that the regenerative urothelial cells were not continuous, and a large amount of lymphocyte infiltration was observed under the epithelium.
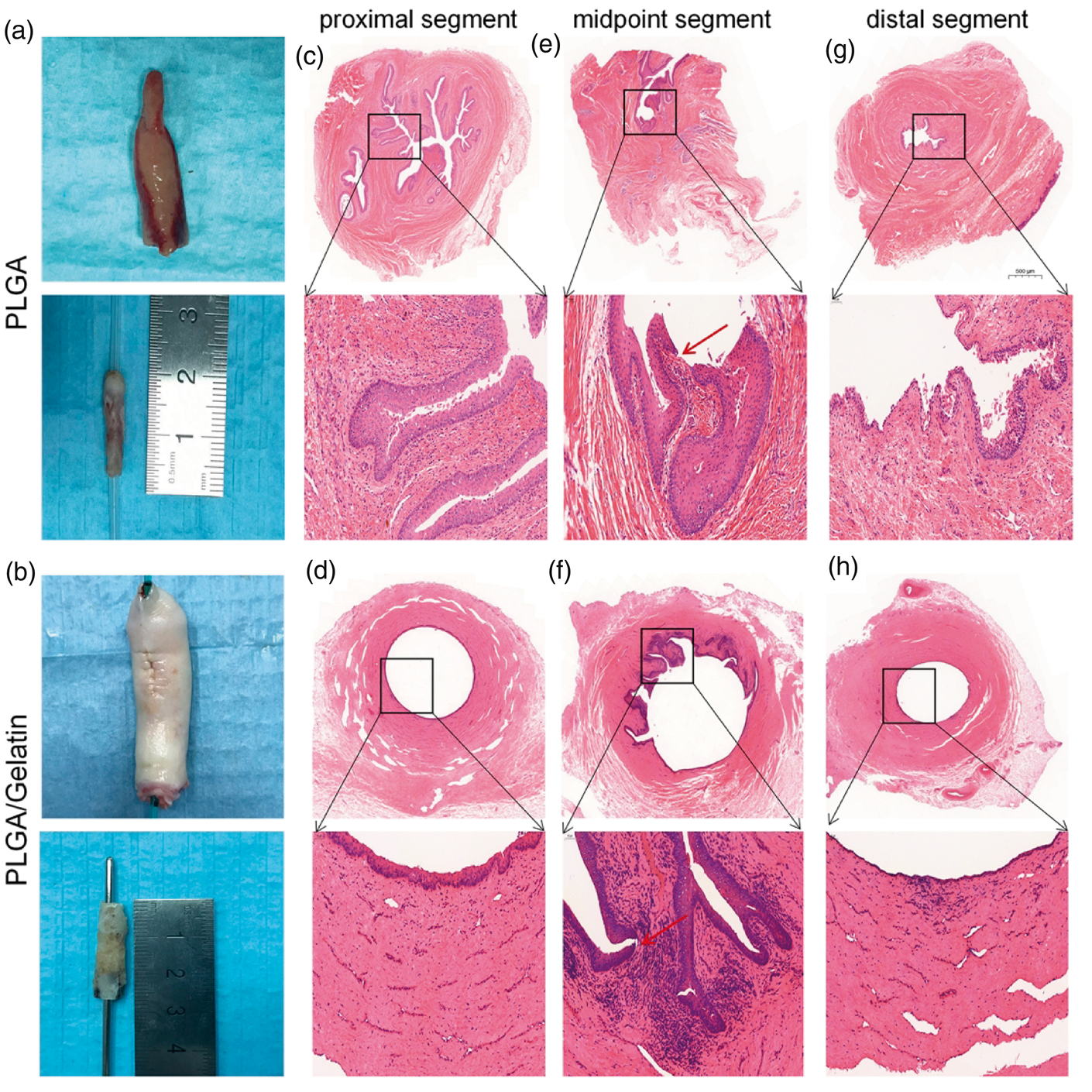
Macroscopic examination of the penis and retrieved urethra at 3 months after urethral reconstruction (a, b). Hematoxylin–eosin (H&E) staining of the urethra: proximal segment (c, d), midpoint segment (e, f), and distal segment (g, h) of the reconstructed urethras: appearance of hypersia of urethral epithelia. The red bottom arrow indicates that the epithelium is continuous. The scale bar at the top of each group is 500 µm. The scale bar at the bottom of each group is 50 µm.
Masson staining at the midpoint of the reconstructed urethras further revealed the proliferation of urothelial cells, some of which were multilayered but discontinuous. A large amount of collagen was deposited under the epithelium, resulting in scar tissue (Figure 5(a) and (b)).
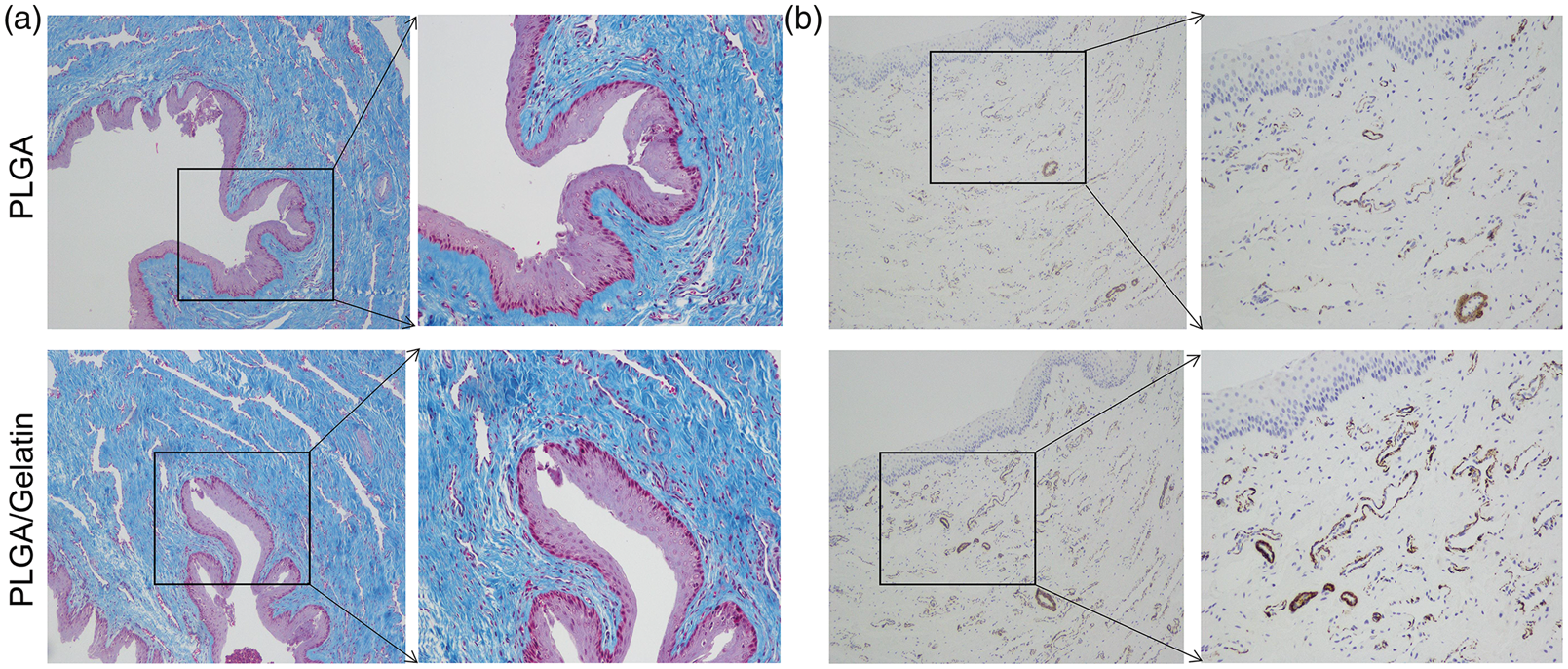
Masson trichrome staining (a) and α-SMA immunofluorescence analysis (b) in the PLGA and PLGA/gelatin groups to assess the urothelium, and smooth muscle of scaffold sites after operation.
Discussion
There are several different surgical approaches to the treatment of urethral stricture and hypospadias. For the reconstruction of short urethral segments, the most common approach is to tubularize auto-foreskin, oral mucosa, or bladder mucosa to construct a new urethra. 8 For the reconstruction of long segments of urethra, however, autologous grafts are not sufficient to achieve entire urethral reconstruction; even when compulsorily reconstructed, the failure rate of surgeries is as high as 50%, and those surgeries are highly susceptible to complications such as infection, urethral strictures, and fistula formation. 9 Patients who suffer from urethral stricture after repeated surgeries can no longer achieve urethral reconstruction simply involving autologous grafts. 10
Tissue engineering technology should theoretically be able to provide nonurological grafts for urethral reconstruction, overcoming the challenge of shortage of source material. At present, there are three types of urothelial tissue engineering material. Membranes or scaffolds may be constructed by in vitro culture of autologous urothelium or smooth muscle cells. Simple cell scaffolds are easily collapsed because of poor mechanical properties and therefore cannot meet the requirements of urethral reconstruction and are therefore rarely used in surgeries. Decellularized scaffolds may be used. These are acellular scaffolds, including those of biological origin such as SIS 11 or BAMG, 12 and synthetic scaffolds. It is also possible to use complexes of scaffolds and cells.3,13 With this approach, electrospun synthetic scaffolds are the most promising for tissue engineering, because they have an adjustable microstructure, good mechanical strength, and a relatively low degradation rate. Sartoneva et al. used poly (l-lactide-co-e-caprolactone) membrane to replace a 1 × 2 oval defect in rabbit urethra. After 16 weeks, no severe strictures were identified using urethrography; only mild fibrosis and inflammation were observed upon histological examination. These results indicate that electrospun scaffolds are suitable for urethral reconstruction. 14
Although most studies using decellularized scaffolds for patchy defect reconstruction achieved promising results, these studies did not involve complete removal of segments of the urethra. Onlay repair, in which about half of the strictured portion of the tubular urethra is replaced with a tissue graft, is often used to repair damaged urethras that have a healthy urethral bed. 15 Most studies using decellularized scaffolds to reconstruct segmental urethral defects reported the occurrence of urethral strictures and fistulas formation after the surgeries. Orabi et al. 16 applied porcine acellular bladder matrix to reconstruct a 6 cm-long section of urethra in a canine model. Their results showed that all animals developed urethral strictures within 3 months of implantation. Dorin et al. 17 used acellular matrices of bladder submucosa to reconstruct segments of urethra of varying lengths of male rabbits (0.5, 1, 2, and 3 cm). Urethrograms showed that only the 0.5 cm graft reconstructions had no strictures within 4 weeks of the surgery. Histological examination further indicated that the 1, 2, and 3 cm grafts showed ingrowth and normal cellular regeneration only at the anastomotic edges, with increased collagen deposition and fibrosis toward the center by 2 weeks and dense fibrin deposition throughout the grafts by 4 weeks. Therefore, the maximum defect distance for normal tissue formation using acellular grafts that rely on native cells for tissue regeneration appears to be 0.5 cm.
There are two major reasons why acellular decellularized scaffolds are not suitable for urethral segment reconstruction. First, the decellularized scaffold is relatively soft and must be tubularized into a tube and anastomosed with the urethra during urethral segment reconstruction. However, the urethra loses support and collapses once the catheter is removed, resulting in urethral stricture and surgery failure. Second, scaffolds will be exposed to urine during the remodeling of the urothelium, leading to repeated infections and the formation of scar tissue at the reconstructed area. 16
Synthetic scaffolds, including electrospun PLGA, PLGA, and PTMC, can be directly shaped into tubular scaffolds because of their adjustable mechanical strength and rate of degradation, which means that they can support the regenerative urethra before degradation. However, few studies have investigated the maximum length of segments of urethral defects that can be replaced by acellular electrospun scaffolds. In this study, PLGA, one of the most common synthetic tissue engineering materials, was selected for the construction of tubular scaffolds, at a thickness of 0.3 mm, using electrospun technology. We also added gelatin to adjust the hydrophilicity of the scaffolds in the control group. The internal diameter of the scaffold was 3 mm, a diameter which can easily accommodate a 6 F single-lumen catheter. All animals were able to urinate spontaneously after the removal of the catheter. Urethrography examination showed urethral strictures 1 month after the surgery, but no urethral collapse was observed at the reconstructed area. No urinary retention caused by urethral collapse developed after the reconstruction.
Although the problem of urethral collapse has been solved, varying degrees of urethral strictures were evident in both groups within 1 month after surgery. Histological examination 3 months after surgery showed that the coverage of urothelial cells, as well as the integrity of the urothelium, was unsatisfactory, especially in the midpoint of the reconstructed urethra. Additionally, acute inflammation and dense fibroblast proliferation were observed. No obvious scaffold was found in examination three months after surgery, indicating that the scaffold had degraded. Although an unobstructed lumen of the urethra had formed, urethral stricture still developed, because of the proliferation of scar tissue. Our results are consistent with previous studies using non-synthetic scaffolds such as BAMG and SIS for urethral reconstruction, which showed varying degrees of urethral strictures, inflammation, and fibroblast proliferation. 16 However, seeding scaffolds with cells to form scaffold cell complexes has contributed to reducing the formation of scar tissue. Lv et al. 18 used PLLA/PEG scaffolds seeded with human amniotic mesenchymal stem cells to reconstruct a urethra with a 2 × 1.5 cm defect. These researchers compared cell-seeded PLLA/PGE with non-cellular PLLA/PGE grafts and observed that in the non-cellular group, no epithelial cells were present until 12 weeks after surgery. However, in the cell-seeded group, the PLLA/PGE scaffolds partially degraded, and a layer of epithelial cells was observed on the surface of the scaffolds; the cellular layer increased over time.
Orabi 16 compared acellular collagen matrices and collagen matrices seeded with cells for the reconstruction of segments of urethra measuring 1–6 cm. Their results indicated that collagen matrices seeded with cells formed normal urethral tissue, which can be used for tubular replacement, whereas tubular collagen matrices without cells lead to poor tissue formation and the development of strictures. It is hypothesized that, after seeding with cells, the rapid development of a urothelial barrier along the luminal surface of the urethra may prevent urine leakage into the suburothelial tissue and the subsequent development of fibrosis. We will further investigate this hypothesis in future studies. Methods for culturing cells in tubular scaffolds and maintaining the physical properties of cell-seeded scaffolds also need further investigation.
Conclusion
In conclusion, an electrospun tubular scaffold can provide mechanical support during urethral reconstruction, avoiding the formation of strictures due to the collapse of the regenerative urethra. However, acute inflammation reactions, fibroblast deposition, and scar tissue proliferation after urethral reconstruction lead to a poor long-term effect. Therefore, acellular electrospun PLGA and PLGA/gelatin scaffolds are not suitable for urethral segment reconstruction. Reducing the extent of the inflammatory reaction and promoting the rapid coverage of epithelial cells are the key challenges that need to be overcome to produce effective synthetic materials for urethral reconstruction.
Footnotes
Authors’ contributions
HX and WJ conceived and designed the study, and critically revised the manuscript. JH and BA performed the experiments, analyzed the data and drafted the manuscript. SZ and ZW participated in study design, study implementation and manuscript revision. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Guangzhou Women and Children’s Medical Center (GCP-2018-006); and Guangzhou Medical and Health Science and Technology Research (2016A010031).
Ethical statement
The animal experiments were approved by the Institutional Animal Care and Use Committee of Guangzhou Medical University, Guangzhou, PR China. The study was performed following the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996).