
Abstract
To investigate the clinical results of treating Kummell’s Disease by using mineralized collagen modified polymethyl methacrylate bone cement, 23 cases (23 vertebras) who sustained Kummell’s Disease treated with mineralized collagen modified polymethyl methacrylate bone cement from July 2017 to February 2019 were reviewed retrospectively. The visual analogue scale, vertebral body height, Cobb angle, CT values pre-operation and post-operation as well as incidence of complications were observed. All the patients were successfully followed up with an average period of 11.3 months (ranging from 6 to 12 months). The patients could ambulate on the second day after the operation. The visual analogue scale scores significantly decreased from two days after the operation to the last follow-up compared with that before the operation (p < 0.05); the average vertebral height and local Cobb angle had significant recovery (p < 0.05); the CT value of the treated vertebra significantly increased compared with that before the operation (p < 0.05). Bone cement leakage occurred in one case, anterior edge leakage occurred in one case, and no clinical symptoms caused by bone cement leakage occurred. No re-fracture of the treated vertebral body or adjacent vertebral bodies were observed in the follow-ups. With good osteogenic activity and degradable absorption characteristics, mineralized collagen was compounded with the existing polymethyl methacrylate bone cement to reduce its strength in the vertebral body and enhance biocompatibility, the incidence of adjacent vertebral fractures and re-fractures within the injured vertebrae is significantly reduced, and good clinical results are obtained, which is worthy of popularization.
Introduction
With the increasing aging in China and the continuous improvement of clinical imaging diagnostic technology, the occurrence of Kummell’s disease, which was considered to be less frequent in the past, has been increasing year by year.1–5 Kummell’s disease was first proposed and defined by German doctor Kummell in 1895, that is, posttraumatic vertebral column collapse, 6 which is characterized by the appearance of “intravertebral vacuum cleft” (IVC) signs in the vertebrae, many secondary in elderly patients with osteoporotic vertebral compression fractures, approximately 10% of clinical osteoporotic vertebral compression fractures. 7
For patients with Kummell’s disease without spinal cord compression, surgical treatment is mainly given by percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP), which can effectively relieve patients’ pain and re-store the height of vertebral body in time and correction of kyphosis.8–10
Polymethylmethacrylate (PMMA) is a commonly used bone cement for PVP or PKP, which has a strong hardness and biological inertness. Such properties were considered as one of the major factors inducing the postoperative fracture rate of adjacent vertebral bodies and incidence of re-fractures in the treated vertebra. 11 In order to overcome these disadvantages of existing PMMA bone cement, a biomimetic mineralized collagen (MC) bone graft substitute, which is a type I collagen/hydroxyapatite composite material, has been used as an additive for PMMA bone cement. MC has orderly arranged type I collagen and nano-sized hydroxyapatite, which is similar to the natural bone matrix in terms of composition and microstructure.12–14 Therefore, MC could be degraded and induce bone regeneration as bone graft substitute.15–17 The objective of such modification by adding MC into PMMA bone cement was to down-regulate compressive modulus of the cement, as well as improve osteointegration between bone and the cement.18–20 Previous studies showed an obvious down-regulation of compressive modulus, without affecting strength of the bone cement. 19 Osteointegration improvement was also demonstrated via animal experiments.20,21 Now, such modification of PMMA bone cement has been widely accepted by spine surgeons. Safety and effectiveness have been verified by tens of thousands of cases with beneficial outcomes. Some typical cases were reported by our own and other researchers and surgeons.19,20,22–24 In the current study, MC modified bone cements were used to treat patients with Kummell’s disease without spinal cord compression, This work was feasible and obtained good clinical results.
Clinical date and methods
Clinical data
From July 2017 to February 2019, 23 patients with osteoporotic single vertebral compression fracture with Kummell’s disease, underwent percutaneous unilateral vertebroplasty using MC-modified PMMA in our department. The patients had 8 males and 15 females, the age ranging from 65 to 88 years, with an average age of 76.81 years. All the patients had varying degrees of thoracolumbar back pain and kyphosis deformity, a slight history of trauma or no obvious history of trauma. According to the phases of Kummell’s disease, we chose the patients from the phase IV, during which the patients sought treatment for repeating and serious pain in their fractures. The course of disease lasted from 2–10 months, with an average of 6.3 months. There were 3 cases of thoracic 11 vertebral body, 6 cases of thoracic 12 vertebral body, 8 cases of lumbar 1 vertebral body, and 5 cases of lumbar 2 vertebral body. All the patients are required to do the bone mineral density test before operation.
All patients underwent chest and/or lumbar spine X-ray, CT and MRI examinations to confirm that a single vertebral compression fracture was accompanied by vertebral fissure signs, except those with vertebral bone kyphosis occupying the spinal canal compressing the spinal cord and vertebral body metastases and occupying lesions.
Surgical techniques
The patient was placed in a prone position with the abdomen suspended, and electrocardiographic monitoring and oxygen inhalation were given during the operation. According to the preoperative physical examination and imaging data, the doctor selected the side of the patient with more pain or the side with large “vacuum” signs in the vertebral body as the needle insertion point for unilateral percutaneous puncture, and under projection, the doctor marked the injured vertebral pedicles disinfected and a sterile surgical drape is laid.
After local anesthesia with lidocaine hydrochloride infiltration, a working channel was established by premarking one side of the pedicle puncture under the guidance of a C-arm machine X-ray, and the puncture work was ensured on the positive side under the C-arm machine X-ray perspective. The channel entered the “vacuum” fissure sign area of the compression fracture, the working channel on the lateral slice reached the depth of the front of the fissure sign, and the positive slice avoided the puncture working channel passing the midline of the spinous process. After confirming that the puncture working channel was in a correct position, the needle core was removed. The modified bone cement was prepared according to the preproportioned bone cement (produced by Heraeus Medical, Germany) and type I collagen/hydroxyapatite composite material, namely, mineralized collagen (produced by Allgens Medical Technology Corporation, China). As described by previous published research papers, the mixing ratio of MC was 15 wt% of the powder part of PMMA bone cement. Oscillator or any other devices for mixing are not essential, the PMMA bone cement was regularly prepared with a simple additional step of adding MC into the slurry immediately after mixing powder and liquid parts of the cement together. The modified bone cement was then prepared to the "drawing stage" of the viscous state under the C-arm X-ray machine perspective and the modified bone cement was slowly injected in the vacuum fracture cavity of the vertebral body to disperse it uniformly, fully filled it, and infiltrated the edge of the cavity along the trabecular bone until the burr shape stopped the injection; after the bone cement becomes hard, pull out the working channel and push rod. After observing no abnormality for 10 minutes or so, the operation can be ended.
Postoperative treatment
Patients were given bed rest after surgery and calcium and vitamin D; then they were supplied with electrocardiographic monitoring to monitor postoperative vital signs such as postoperative fever and bone cement allergic reactions. Those who didn’t have any adverse reactions postoperatively were given zoledronic anti-osteoporosis treatment on the second day and were instructed to get out of bed.
Postoperative follow-up
The patients were followed up two days, three months, six months and one year after operation to review the injured vertebrae X-ray and CT film, and the doctor measured the Cobb angle before and after each follow-up visit;the doctor observed the modified bone cement dispersion in the injured vertebra coupling with the surrounding trabecular bone, and measured the CT value of the trabecular bone around the modified bone cement, using visual analogue scale (VAS) score to evaluate the postoperative pain relief of the patient and observing what the adjacent vertebral fracture happened.
Statistical analysis
The data are expressed as mean ± standard deviation, and statistical analysis was performed using SPSS 19.0 software. The comparison of the data before and after the follow-up was performed by paired t-test. P < 0.05 was considered statistically significant.
Results
All patients successfully completed the operation, one case of intervertebral disc bone cement leakage, one case of anterior vertebral body leakage, no clinical symptoms caused by bone cement leakage, no bone cement allergy after operation, and no bone cement leakage into the spinal canal caused symptoms of spinal nerve root compression. The average operation time was (28.5 ± 8.2) minutes. All 23 patients were followed up for 6–12 months, with an average follow-up of 11.3 months. There were no re-fracture of the injured vertebral bodies and fractures of adjacent vertebral bodies in each follow-up operation.
The VAS score of patients before and after each follow-up was statistically significant (p < 0.05), and the VSA score of patients after each follow-up was significantly improved compared with that before operation (p < 0.05); the height of injured vertebra and Cobb angle of patients before and after each follow-up were measured, and statistical analysis showed that the height of injured vertebra and Cobb angle of patients after each follow-up were significantly improved compared with that before operation (p < 0.05); there was no significant difference in the height of the injured vertebrae and Cobb angle (p > 0.05). The CT value of the trabecula around the fracture sign in the injured vertebrae before operation and the trabecula around the modified cement were measured and compared with each other. It was found that the CT value of the injured vertebrae after operation did significantly increase compared with that before operation (p < 0.05). There was no significant difference between the CT values at each follow-up (p > 0.05). See Table 1 for specific data and Figure 1 for typical cases.
The average VAS score, the average height of the vertebral, Cobb angle and the T value of CT before and after surgery (

aCompared with the preoperative values, p < 0.05.
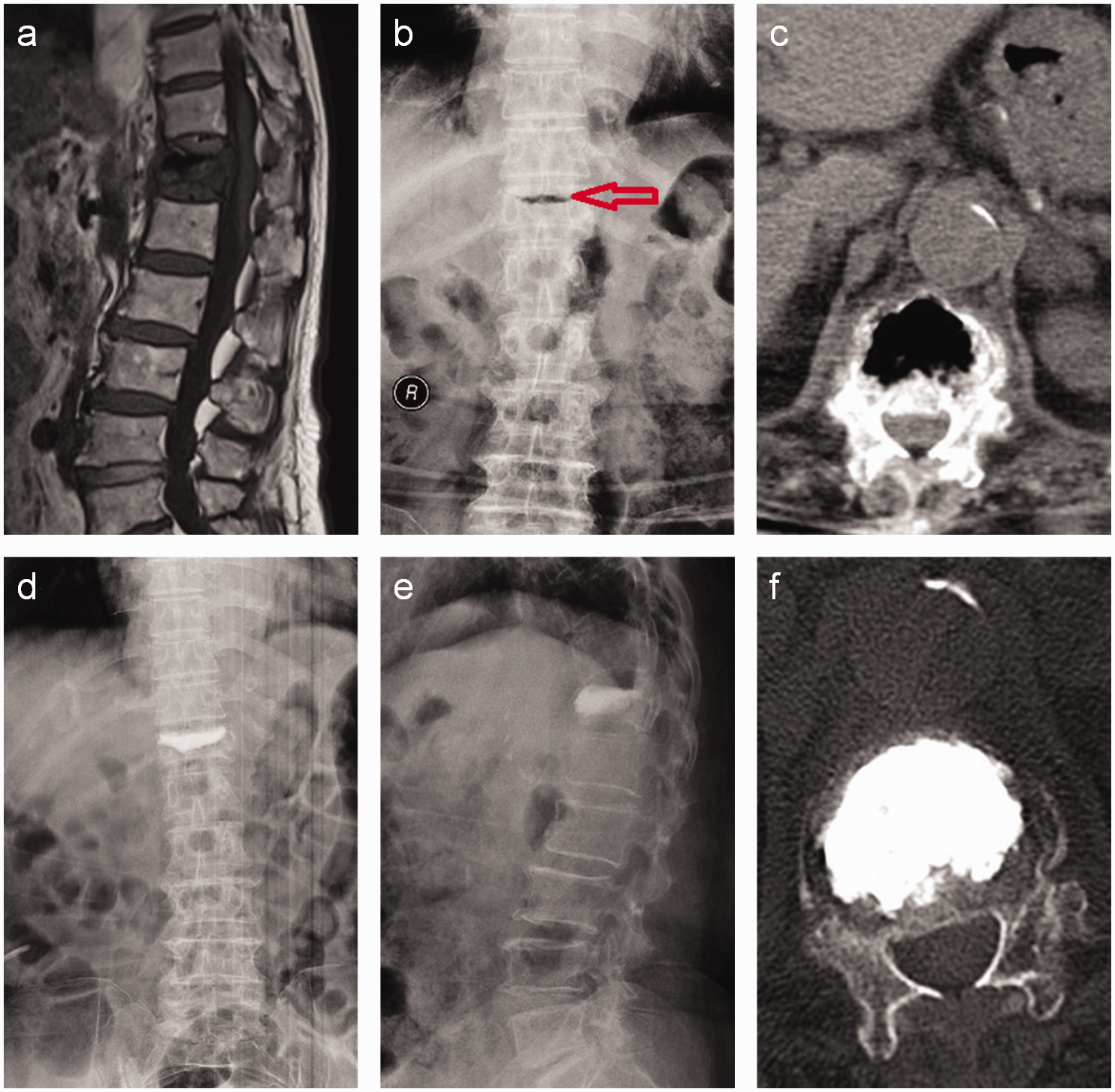
Female, 83 years old, admitted to the hospital for more than three months after minor trauma with persistent pain in the thoracolumbar segment. In the figure (a), preoperative MRI indicated Kummell’s disease of the thoracic 12 vertebral body; in the figure (b), X-ray in the anterior position, the red arrow is the fracture sign; the figure (c) shows the fracture sign in the CT of the vertebral body with peripheral hyperosteogeny and sclerosis; the figure (d) to (f) show the X and CT re-examination after the operation. It can be seen that the PMMA modified by MC diffuses evenly and stably in the vertebral body, the height of the vertebral body partially recovers, and no cement leakage is found.
Discussion
Since Kummell’s disease was put forward and defined by Kummell, clinical workers have been improving their understanding of the disease and staging it during the development process of the disease. Benedek divided Kummell’s disease into five stages 25 : stage I is the early stage of the disease, which can be asymptomatic after trauma, and X-ray can be free of abnormal manifestations; In stage II, the patients survive mild thoracolumbar and back pain, but their daily walking activities are not affected. The stage III? is the incubation period, during which the patients don’t show any obvious clinical symptoms, but which can last for several months to several years; the stage IV is the repeated pain at the fracture site, and the pain is gradually aggravating; the stage V is the end stage, during which the patients survive the persistent pain with kyphosis or spinal nerve root compression. It can be seen that the patients with this disease have a small history of trauma. In the early and middle period after injury, there may be no obvious symptoms of thoracolumbar and back pain, even without any neurological symptoms. However, with the development of the disease, the pain symptoms will gradually be aggravated, and it is difficult for the fracture to heal itself. If not treated in time, the kyphosis and local pseudarthrosis caused by the collapse caused by the avascular necrosis of the vertebral body can be found in the later stage. In severe cases, the spinal cord can be compressed with obvious neurological symptoms.26–28
The patients who came to see the doctor were mostly in stage IV, mainly because they can't bear repeated pain in the chest, waist and back. The surgical treatment was mainly minimally invasive vertebroplasty, which can immediately and effectively relieve the pain, stabilize the injured vertebra, and correct kyphosis by filling the vertebra with bone cement.1,10
Because of the poor hardness and biocompatibility of PMMA, it has a high incidence of adjacent vertebral body and intravertebral fracture after operation for the treatment of osteoporotic vertebral body fracture in the elderly. 11 When the traditional bone cement is directly injected into the fracture space of the injured vertebral body of patients with Kummell’s disease, it is easy to form an independent mass structure. Because of its poor biocompatibility and strong inertia, it is easy to form an independent mass structure in the later stage, and it is easy to loosen or even slip in the vertebral body. 29 We used MC to modify the existing PMMA, because the composition and microstructure of MC are similar to the natural bone matrix, it can be phagocytized and degraded by osteoclasts in the vertebral body, and it has good osteogenic activity and degradability.12,21,22 When being properly mixed with specific PMMA bone cements, it can effectively reduce hardness and improve biological compatibility of the PMMA cements. 30 Moreover, the MC itself has been used in the clinical treatment of elderly patients with osteoporotic vertebral compression fracture. In the postoperative follow-ups of previous studies for the treatment of normal osteoporotic vertebral compressive fractures, we found that the incidence of adjacent vertebral body and intravertebral fracture was significantly reduced. 31
In order to reduce the incidence of fracture in adjacent vertebrae and injured vertebrae of Kummell’s disease after operation, we also used MC to modify the existing PMMA, which achieved good clinical effect. In this study, 23 patients were not found any fracture in adjacent vertebrae during the follow-up, which was far lower than that of patients using ordinary PMMA operation. The reduced strength of cement can effectively reduce the incidence of fracture in adjacent vertebrae rate:the height and Cobb angle of the injured vertebrae at each follow-up after operation were significantly improved compared with those before operation, and the difference was statistically significant, indicating that the PMMA hardness after MC modification was reduced, but it could still recover the injured vertebrae height and correct kyphosis of vertebrae, and the strength after modification could fully meet the clinical use; most patients with Kummell’s disease were the elderly people, and the degree of osteoporosis was serious. The CT value measured in the injured vertebrae before operation was lower, and the CT value around the modified cement was significantly improved after two days of operation. The difference was statistically significant. Our analysis suggested that it was related to the increase of the density of the bone trabeculae around the cement by pushing and squeezing the cement into the vertebrae, but the CT value gradually increased after three months, six months and one year of follow-up, suggesting that the MC on the surface of PMMA after the modification was degraded by itself. 21 It has good histocompatibility and certain osteogenic activity.
From our point of view, the treatment strategy of the present study is not recommended for those young adult patients with kummel’s disease. Because young adults possess good bone healing ability (except those with special diseases of bone metabolism), kyphosis could be well treated by transpedicular bone grafting augmentation within the vertebral body, followed by screw-rod internal fixation. Such transpedicular bone grafting and screw-rod fixation keeps local strong stability, and helps rapid healing of the injured vertebrae.
To sum up, this study uses mineralized collagen modified bone cement to treat Kummell’s disease through percutaneous one-sided vertebroplasty, which has a good clinical effect and is worthy of further clinical application. However, due to the small number of cases and short follow-up time in this study, a long-term follow-up study with large sample size is needed to provide more reliable and accurate follow-up data for clinical reference.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was in part supported by the project support of Jiangsu University clinical medicine science and Technology Development Fund (JLY20180155), Research Fund for Jiangsu Provincial Commission of Health and Family Planning (H201559), the Haiyan Project of Lianyungang (KD2019lyghy001) and the National Key R&D Program of China (2020YFC1107600).