
Abstract
Osteoarthritis is a degenerative condition that is highly prevalent and primarily affects the joints. The knee is the most commonly affected site, impacting the lives of over 300 million individuals worldwide. This study presents a potential solution to address the unmet need for a minimally invasive technique in the treatment of osteoarthritis: a biocompatible, injectable, and thermoresponsive hydrogel. In comparison to commercially available products such as lyophilized platelets, dextrose, and triamcinolone, the thermoresponsive hydrogel exhibits significantly superior performance in dynamic behaviors, including print area, stability, and step cycle, when tested on rats with knee osteoarthritis. However, it demonstrates similar treatment efficacy to these products in static behaviors, as observed through histopathological and immunohistochemical analysis. Therefore, the thermoresponsive hydrogel holds promise as an effective alternative therapy for osteoarthritis. Moreover, by blending the hydrogel with drugs, controlled and sustained release can be achieved, thereby facilitating the long-term management of osteoarthritis symptoms.
Introduction
Osteoarthritis (OA) is a prevalent degenerative joint disorder that primarily affects the knee in approximately 85% of cases, impacting the lives of over 300 million people worldwide.1,2 The growing burden of knee OA, exacerbated by an aging population and rising obesity rates, underscores the urgency to effectively address this condition. 3 The pathogenesis of OA is complex and not fully understood; however, it is characterized by progressive cartilage degradation, osteophyte formation, and subchondral bone sclerosis, accompanied by biochemical changes. 4 Cartilage degradation is a critical aspect of OA, and severely damaged cartilage has limited self-repair capacity due to the absence or limited presence of nerves and blood vessels. 5 Consequently, healthcare systems worldwide are facing increasing strain as the demand for joint replacement surgeries rises in response to the escalating burden of OA. 6 In light of this situation, it remains crucial to assess the effectiveness of current treatments and explore the development of innovative approaches to address this pressing issue.
Despite extensive research on knee OA, there is still a significant gap in its treatment options. The available interventions primarily focus on managing symptoms rather than modifying the disease, highlighting the need for innovative therapeutic strategies. While non-pharmacological approaches, such as exercise, weight management, and physical therapy, play a crucial role in knee OA management, 7 their implementation and adherence rates remain suboptimal. Additionally, pharmacological therapies like nonsteroidal anti-inflammatory drugs (NSAIDs) and analgesics offer only temporary pain relief and come with notable adverse effects, including cardiovascular, renal, and gastrointestinal complications, limiting their long-term use.8,9 Although total knee arthroplasty, a surgical intervention, is highly effective for advanced knee OA cases, its high cost makes it suitable only for patients with severe functional impairment. As a result, there is an urgent need to develop minimally invasive procedures that bridge the gap between invasive treatments like joint replacement and non-invasive approaches such as rehabilitation programs and pain relief medications.
In the treatment of OA, intra-articular injections of hyaluronic acid and corticosteroids, specifically triamcinolone, are considered micro-invasive procedures. However, these treatments provide limited pain relief and fail to effectively halt the progression of the disease. 10 Consequently, alternative options like dextrose prolotherapy, platelet-rich plasma, or lyophilized platelets have emerged.11,12 Nevertheless, their suitability for chronic diseases is impeded by their limited duration in the affected area and the short release of growth factors from platelet-rich plasma or lyophilized platelets. 13 Therefore, there is an urgent need for a micro-invasive technique that does not require skin incisions while improving treatment acceptability for OA patients. 14
The objective of this study was to address the unmet need for a micro-invasive technique in the treatment of OA by introducing a biocompatible, injectable, and thermoresponsive hydrogel. Upon injection, the hydrogel undergoes a liquid-to-gel transition at physiological temperatures, enabling it to remain in the target site (in situ). This unique characteristic makes it particularly advantageous for clinical procedures, especially in knee joints with irregular-shaped cavities and high activity requirements. In this study, using a rat knee OA model, we formulated a hypothesis that the injection of the hydrogel would lead to a superior improvement in gait pattern compared to injections of triamcinolone, lyophilized platelets, and dextrose.
Materials and methods
Materials and instruments
Animals
The use of rats in this study was granted ethical approval by the ethics committee of the Laboratory Animal Center at National Taiwan University College of Medicine (Approval No. 20200222). Female Sprague Dawley rats (SD) aged 8 weeks were obtained from the National Laboratory Animal Center (Taipei City, Taiwan) for the in vivo studies conducted between 8 and 16 weeks of age.
Bio- and chemical materials
Lyophilized porcine platelets were customized from Spirit Scientific Co. LTD. (Taipei city, Taiwan). Dextrose was purchased from Taiwan Biotech Co., LTD. (Taoyuan city, Taiwan). Triamcinolone was purchased from Tai-Yu chemical & pharmaceutical Co., LTD. (Hsinchu County, Taiwan). Isotonic sodium chloride solution (0.9% Saline) was provided by Taiwan Biotech Co., Ltd. (Taoyuan, Taiwan) and was sterile filtered through a 0.22 μm polyethersulfone membrane (Millipore syringe filter) from Polyplus-transfection (Illkirch, France). Collagen I antibody (GTX20292) was purchased from GeneTex Inc. (CA, USA). Monosodium Iodoacetate (MIA, I2512), Toluidine blue (89,640), and collagen II antibody (MAB1330) was purchased from Merck KGaA (Darmstadt, Germany). Collagen X (ab49945) and Sox 9 (ab185230) antibodies were purchased from Abcam PLC (Cambridge, UK). Thermoresponsive hydrogels (mPEG-PLGA-BOX block copolymer) here were synthesized by our previous research.15,16
Instruments and devices
The matrix isoflurane vaporizer (VIP 3000) was acquired from Midmark Corp. (Ohio, US). The Catwalk gait analysis system (XT) was purchased from Noldus Information Technology bv. (Wageningen, Netherlands). The incapacitance tester (Singa 1) was obtained from Singa Technology Co. (Taipei, Taiwan). The digital microscope camera system (RT-KE Color 3-shot, SPOT) and its software (SPOT advanced) were purchased from Diagnostic Instruments, Inc. (Sterling Heights, US).
Rat osteoarthritis model and treatments
Rat osteoarthritis model
After 7 days of catwalk gait and incapacitance tester training, the animals were anesthetized using a 2% isoflurane-O2 mixture. Following surgical preparation, a single intra-articular injection of 2 mg of MIA in 50 μL of saline was administered through the infrapatellar ligament of the right knee using a 31 G, 0.5-inch needle mounted on a 0.5 mL syringe. The OA rat model was considered fully established 2 weeks after the intra-articular injection of MIA, as illustrated in Figure 1.17,18 The experimental protocol involved sacrificing the rats at two time points: 14 days (E1) and 49 days (E2) after the MIA intra-articular injection. This was done to assess the damages induced by MIA in the right leg knee and evaluate the efficacy of treatments including lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel. Catwalk (CW) and incapacitance tester (IT) were used to evaluate the outcomes.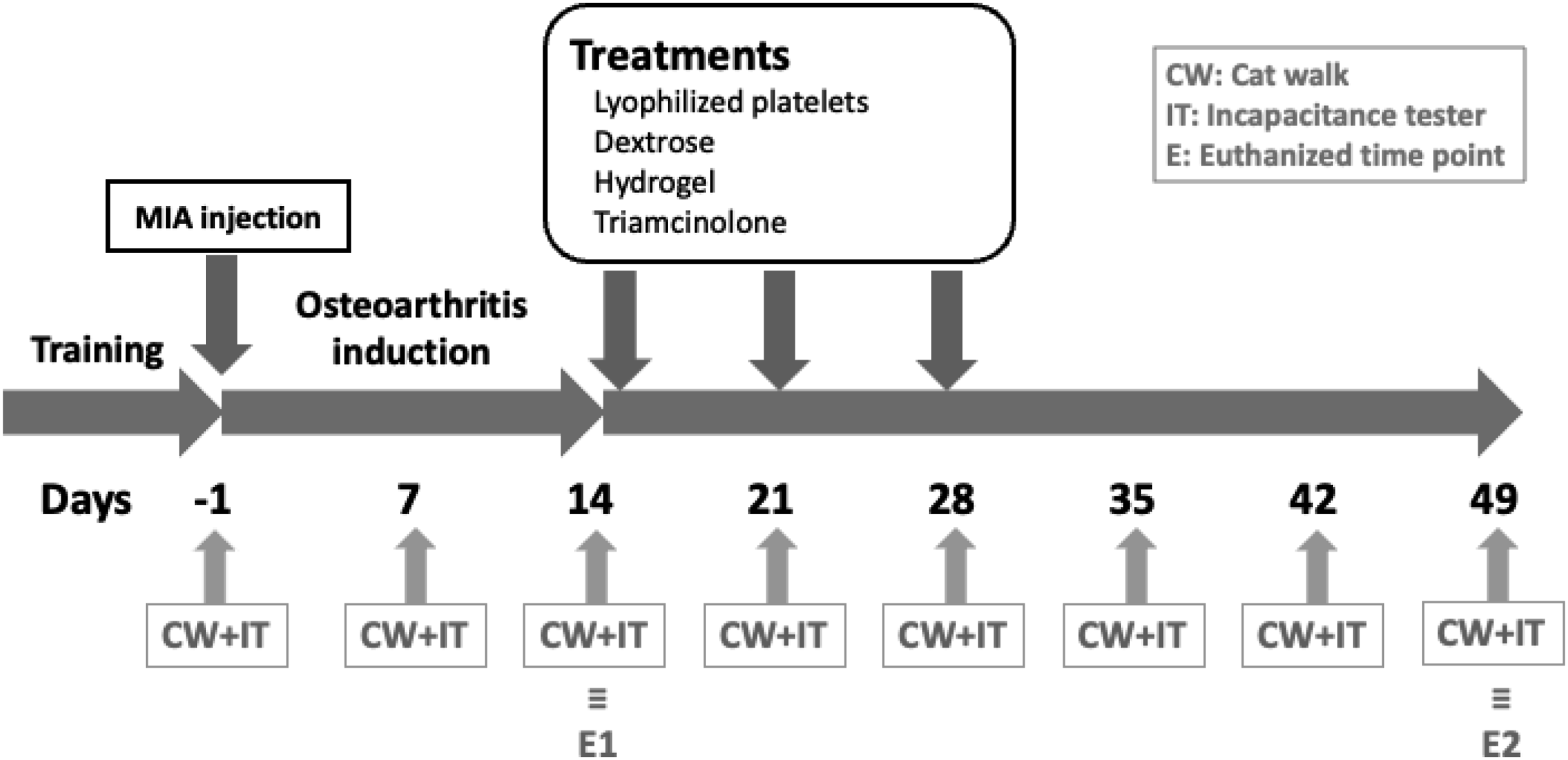
Treatment by lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel
After 14 days of the MIA intra-articular injection, the treatments involving lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel were consecutively administered over a period of 3 weeks on days 14, 21, and 28, as depicted in Figure 1. During this phase, the animals were anesthetized using a 2% isoflurane-O2 mixture. Following surgical preparation, a single intra-articular injection of 50 μL of 0.5% lyophilized platelets (in 0.9% saline), 25% dextrose (in 0.9% saline), 4 mg/ml triamcinolone (in 0.9% saline), and thermoresponsive hydrogel was administered through the infrapatellar ligament of the right knee using a 31 G, 0.5-inch needle mounted on a 0.5 mL syringe.
Animal behaviors
Throughout the entire experimental period, the rats were tracked weekly using the catwalk and incapacitance tester to assess the damages induced by MIA in the right leg knee, as well as to evaluate the efficacy of treatments including lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel.
Incapacitance tester
The distributions of static weight bearing through the right and left leg knees were assessed by incapacitance tester. The force exerted by each leg was measured and analyzed in grams, but reported in percentage of total body weight (% BW) to normalize the data. Rats were allowed to acclimate to the testing apparatus, and when stationary, readings were taken over a 3 s period. Triplicates were taken simultaneously for each leg at each time point.18,19
Catwalk
The catwalk system comprises an illuminated-walkway glass floor and a high-speed video camera equipped with a wide-angle lens (6.0 mm). The camera was positioned underneath the walkway, at a distance of 56 cm, to capture the paw prints. The Catwalk XT 10.6 software automatically recorded the paw prints when the animals crossed the pathway in a 20 × 10 cm calibrated lane. The glass floor created a contrast for the animal steps using a green LED combined with a red-illuminated background.20,21 The Catwalk analysis was depicted in Supplementary Figure 1. The Catwalk XT system was used to detect all dynamic behavioral indicators by tracking changes in paw prints.
Histopathologic sections and immunohistochemistry
To verify the presence of OA in the rat knee and assess the therapeutic effect, the knees of the rats were extracted 14 and 49 days after MIA-induced OA. The knee fillets were then immersed in a 10% formaldehyde solution for 24 h. Afterwards, the specimens were decalcified and embedded in paraffin for histopathological and immunohistochemical analysis. All slides were examined using a Ventana Dp200 slide scanner along with its software, Ventana Image Viewer v3.2 advanced.
Histopathologic analysis
The paraffin-embedded sections underwent H&E staining and Toluidine blue assay, as described in previous publications.22,23 H&E staining was employed to examine the cell and tissue morphologies and distributions of rat knees. This staining technique utilizes hematoxylin and eosin, where the cell nuclei appear blue-purple, and the cartilage matrix exhibits a pink color with a blue hue in areas containing high levels of proteoglycans. Conversely, Toluidine blue, a small, weakly hydrophilic cationic dye, was used to intensely stain proteoglycans and glycosaminoglycans, thereby elucidating the cartilaginous matrix of rat knees.
Immunohistochemical analysis
The paraffinized sections were treated with various antibodies to perform specific staining. Connective tissues were stained using an anti-Collagen I antibody (GTX20292, GeneTex), chondrodysplasia was identified with an anti-Collagen II antibody (MAB1330, Millipore), mineralized hyaline cartilage was detected using an anti-Collagen X antibody (GTX37732, GeneTex), and chondrogenesis was visualized through an anti-Sox nine antibody (ab185230, abcam). The staining procedures followed the official protocols provided by the respective manufacturers. The detection of labeled sections was carried out using the Elite ABC kit (PK-6100) and ImmPACT™ DAB (SK-4105), as recommended by the manufacturer, Vector Laboratories. To enhance contrast, all sections were counterstained with hematoxylin in Ventana reagent.
Statistics
The statistical analysis was conducted using SPSS version 26. All data were presented as the mean ± standard deviation (SD) of a minimum of five independent samples (N). Group comparisons were assessed using one-way ANOVA followed by post-hoc analysis using the Least Significant Difference (LSD) test. A p-value less than 0.05 was considered statistically significant.
Results
Validation of rat osteoarthritis model
Incapacitance tester and catwalk
The incapacitance tester (Figure 2(a)) and catwalk (Figure 2(b)–(f) and supplementary Figure 2(a)–(d)) were widely employed indicators for static and dynamic behavioral evaluation in animal models of OA. These tools were utilized to confirm the successful establishment of the disease model in behavioral science. As shown in Figure 2(a), it can be observed that in terms of static behavioral evaluation, the MIA-induced OA group exhibited a statistically significant difference compared to both the control and sham groups after 7 days of MIA intra-articular injection (p < .01). The evaluation of the MIA-induced OA rat model was conducted on various behavioral indices on the 14th day. These included: (a) static weight bearing measured using the incapacitance tester; (b) print area; (c) swing; (d) duty cycle; (e) step cycle; and (f) stand assessed through the catwalk system. The experimental groups were as follows: control, representing the non-treatment group; Sham, representing the normal saline group; and MIA, representing the MIA-induced OA group. Statistical analysis was performed using one-way ANOVA with the LSD post hoc test, and significance was indicated as ααp and ββp < .01 and αp < .05, respectively, when compared to the control and sham groups. The total number of samples used in the study was n = 6.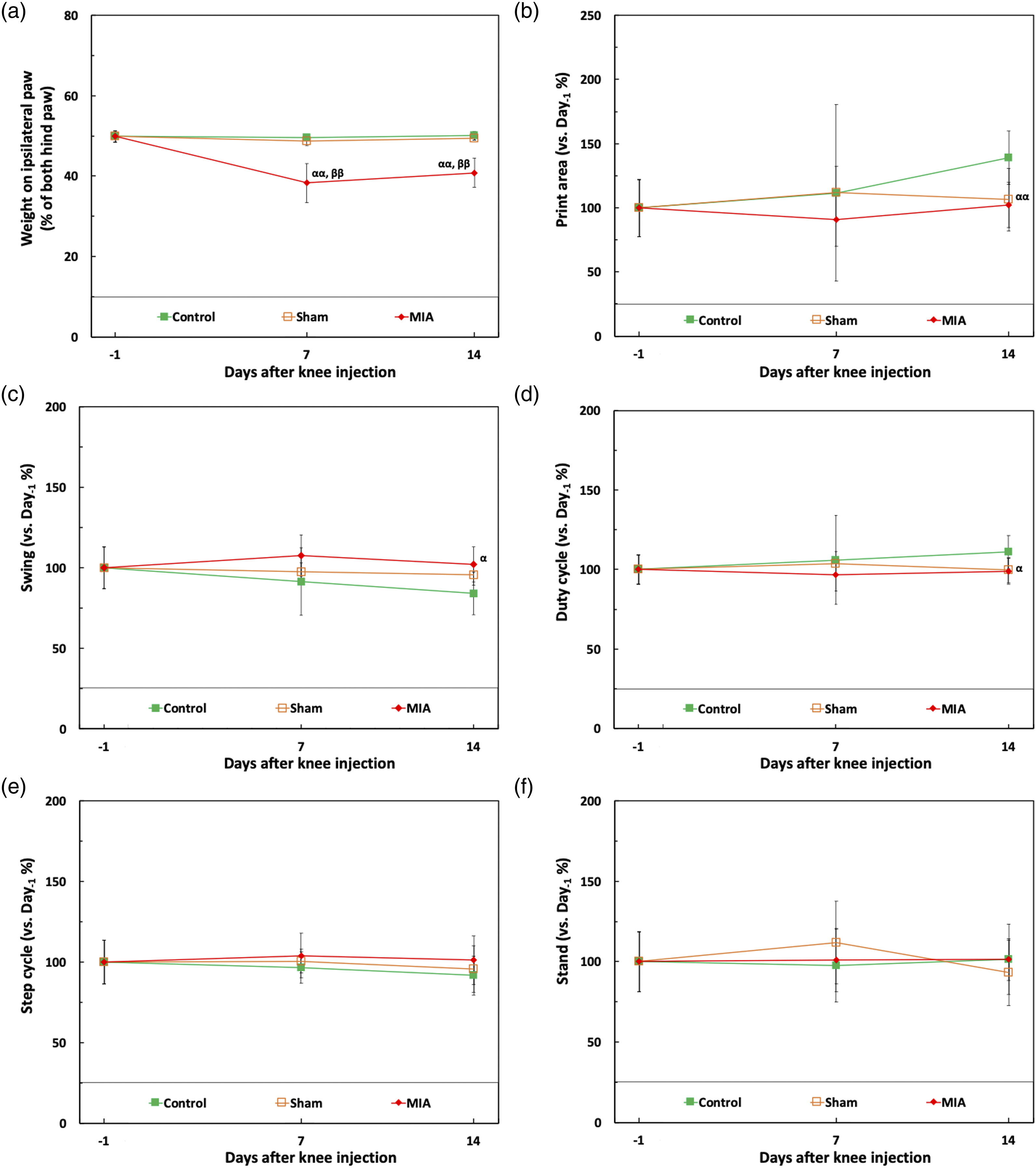
Figure 2(b)–(f) reveals that the MIA-induced OA group exhibited a statistically significant difference in print area (p < .01) and swing duty cycle (p < .05) compared to the control group after 14 days of MIA intra-articular injection. In conclusion, considering both static and dynamic behaviors, the MIA-induced OA model employed in this study can be considered representative for establishing animal behavior models to a certain extent.
Histopathologic analysis
After discussing the animal behavior, the histopathologic sections of the control, sham, and MIA groups were analyzed. Among them, Figure 3(a) and (b) depict the H & E and Toluidine blue stains, respectively, of the control, sham, and MIA groups. Figure 3(c)–(e) present the femur, patella, and femur-patella thickness data for these three groups. The histopathologic section data in Figure 3(c)–(e) clearly indicate that the MIA groups exhibit statistically significant differences in femur, patella, and femur-patella thickness compared to the control and sham groups. Therefore, based on the discussion of animal behavior and histology in sections incapacitance tester and catwalk and histopathologic analysis of results, it can be confirmed that the MIA intra-articular injection method employed in our study successfully establishes the MIA-induced OA model on the 14th day following MIA injection. The histopathologic analysis of the MIA-induced OA rat model was performed on the 14th day. The evaluation included: (a) H & E stain, (b) toluidine blue stain, (c) femur thickness, (d) patella thickness, and (e) femur-patella thickness. The experimental groups consisted of: control (non-treatment group), Sham (normal saline group), and MIA (MIA-induced OA group). Statistical analysis was conducted using one-way ANOVA with the LSD post hoc test, and significance levels were set at αp and βp < .05 for comparisons against the control and sham groups, respectively. The sample size for each group was n = 6.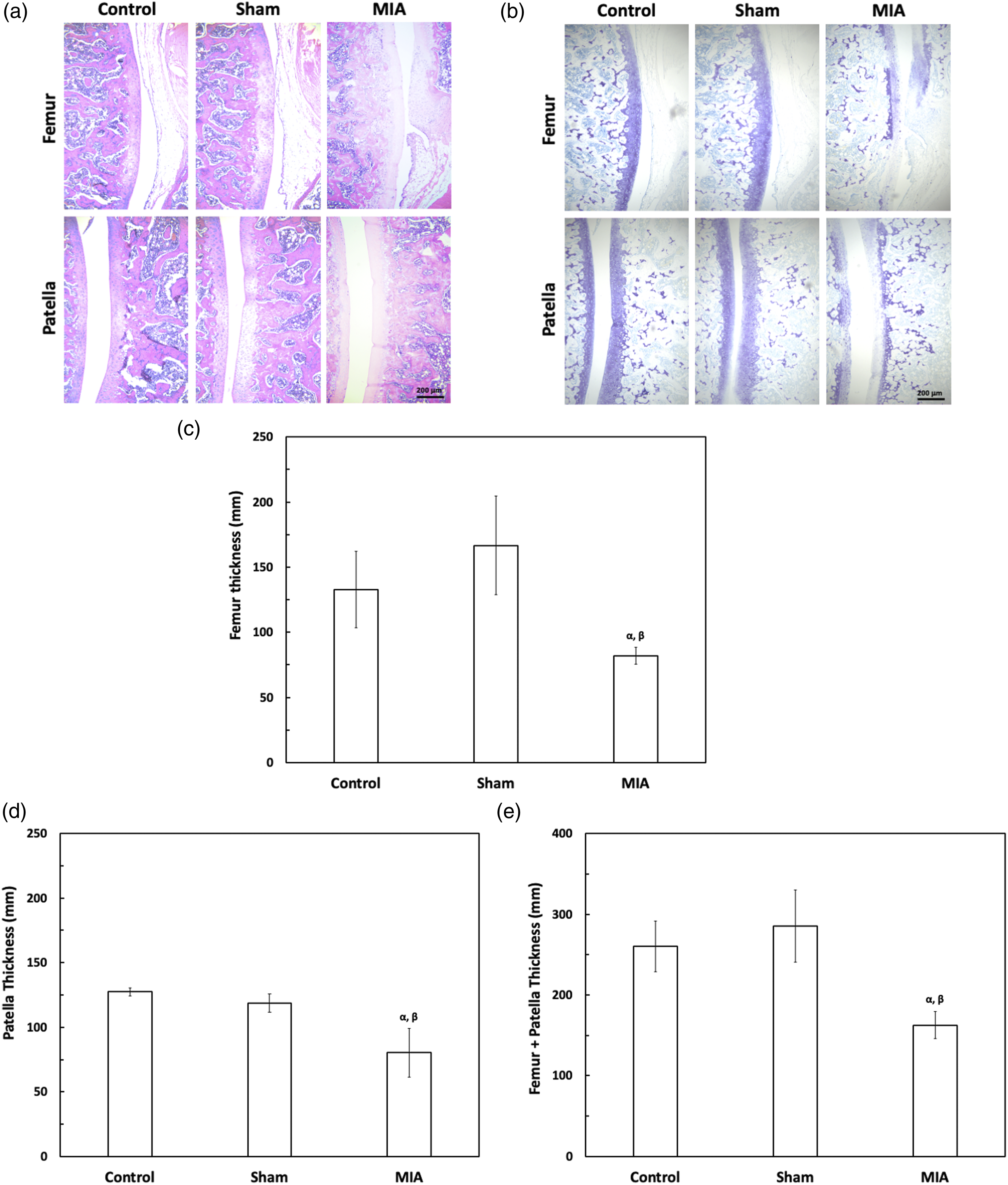
Comparisons of treatment efficacy on osteoarthritis rat model
Incapacitance tester and catwalk
From this section onwards, we would discuss and compare the treatment effects of lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel after the successful induction of MIA-induced OA. The intervention therapies were administered at the 14th, 21st, and 28th days after MIA injection, and the therapeutic outcomes were assessed up to day 49, as depicted in Figure 1.
Regarding static behavior, there was no statistically significant difference observed in the incapacitance tester between the groups injected with MIA, irrespective of whether they received interventional therapy or not (Figure 4(a)). However, concerning dynamic behavior (Figure 4(b)–(f) and supplementary Figure 3(a) to 3(d)), the thermoresponsive hydrogel treatment group exhibited statistically significant differences compared to the MIA group in terms of print area (D28, p < .05) and stand (D28, p < .01). The treatment efficacy of different interventions on the MIA-induced OA rat model was compared across various behavior indexes on the 49th day. The evaluated indexes included: (a) static weight bearing measured using an incapacitance tester, (b) print area, (c) swing, (d) duty cycle, (e) step cycle, and (f) stand analyzed through the catwalk system. The experimental groups consisted of: control (non-treatment group), Sham (normal saline group), MIA (MIA-induced OA group), MH (MIA-induced OA with thermoresponsive hydrogel treatment group), MP (MIA-induced OA with lyophilized platelets treatment group), MD (MIA-induced OA with dextrose treatment group), and MT (MIA-induced OA with triamcinolone treatment group). Statistical analysis was performed using one-way ANOVA with the LSD post hoc test, and significance levels were set at ααp, ββp < .01; αp, βp, γp, and δp < .05 for comparisons against the control, sham, MIA, and thermoresponsive hydrogel treatment groups, respectively. The sample size for each group was n = 6.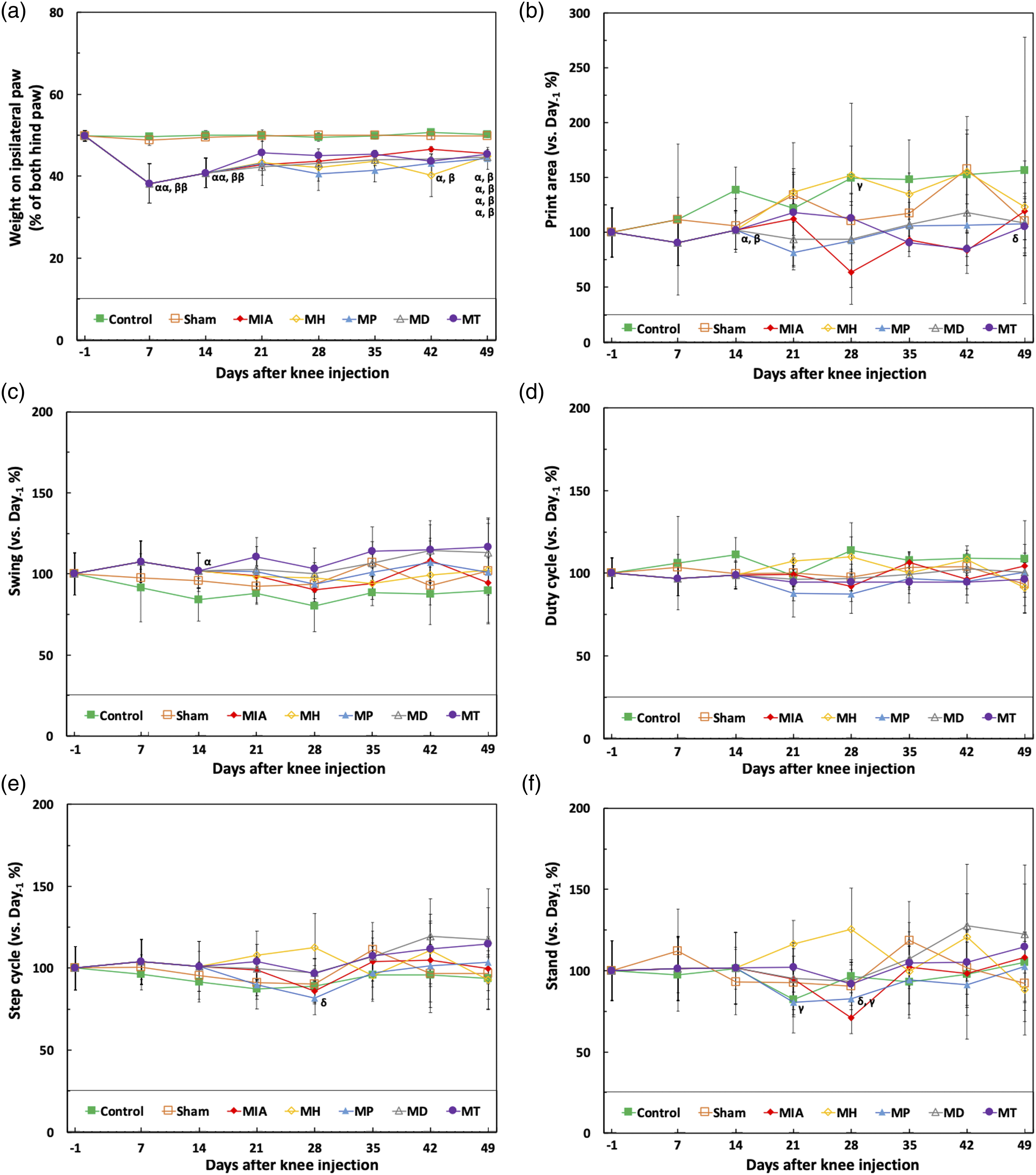
Additionally, the thermoresponsive hydrogel treatment group showed statistical differences compared to the triamcinolone treatment group in print area (D42, p < .05) and compared to the lyophilized platelets treatment group in stand (D21, p < .01; D28, p < .01) and step cycle (D28, p < .05). In summary, among the therapies involving lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel, only the thermoresponsive hydrogel treatment group demonstrated behavioral performance closer to that of the control and sham groups, with statistically significant differences observed in print area and stand.
Histopathologic analysis
Histopathologic sections were analyzed for the effects of lyophilized platelets, dextrose, triamcinolone, and thermoresponsive hydrogel therapies on the 49th day. Figures 5(a) and (b) present the H&E and Toluidine blue stains, respectively, of all the groups. It was evident that in all the groups injected with MIA, there was noticeable thinning of the femur and patella, as well as severe joint cavity lesions, when compared to Figure 3(a) and (b). Figure 5(c)–(e) display the femur, patella, and femur-patella thickness data for all groups. Overall, there were no statistically significant differences observed in the femur and patella thickness among the MIA-injected groups, regardless of whether they received interventional therapy or not. The treatment efficacy on the MIA-induced OA rat model was compared through histopathologic analysis on the 49th day. The comparisons included: (a) H&E stain, (b) toluidine blue stain, (c) femur thickness, (d) patella thickness, and (e) femur-patella thickness. The experimental groups consisted of: control (non-treatment group), Sham (normal saline group), MIA (MIA-induced OA group), MH (MIA-induced OA with thermoresponsive hydrogel treatment group), MP (MIA-induced OA with lyophilized platelets treatment group), MD (MIA-induced OA with dextrose treatment group), and MT (MIA-induced OA with triamcinolone treatment group). Statistical analysis was conducted using one-way ANOVA with the LSD post hoc test, and significance levels were set at ααp, ββp < .01 and αp, βp < .05 for comparisons against the control and sham groups, respectively. The sample size for each group was n=6.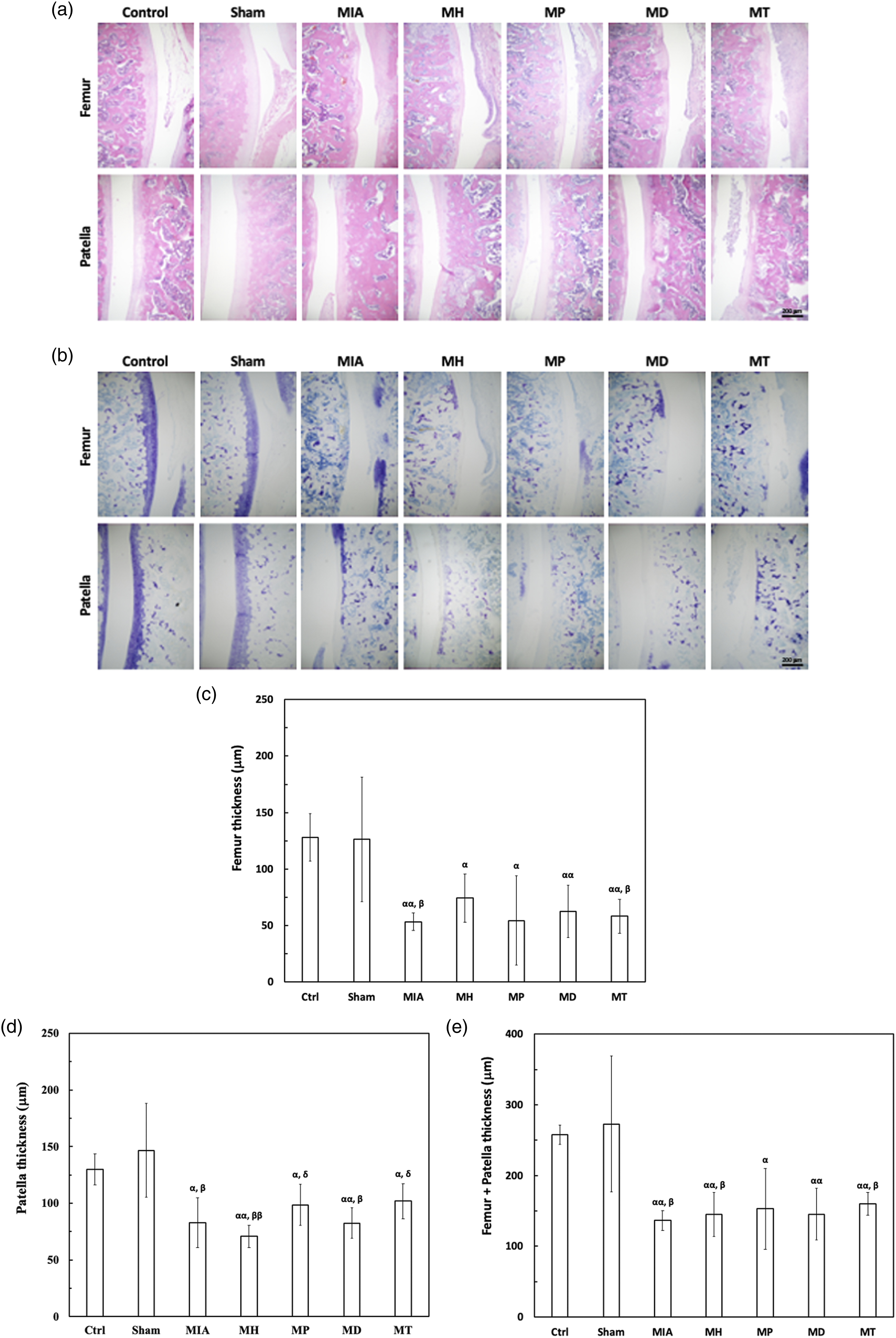
Immunohistochemical analysis
After the discussion of histopathologic analysis, we would proceed to perform immunohistochemical analysis on various tissues. Specifically, we analyzed connective tissues using Collagen I stain (Figure 6(a)), chondrodysplasia using Collagen II stain (Figure 6(b)), mineralized hyaline cartilage using Collagen X stain (Figure 6(c)), and chondrogenesis using Sox nine stain (Figure 6(d)). The treatment efficacy on the MIA-induced OA rat model were compared through immunohistochemical analysis on the 49th day. The comparisons were involved: (a) collagen I stain, (b) collagen II stain, (c) collagen X stain, and (d) Sox nine stain. The experimental groups consist of: control (non-treatment group), Sham (normal saline group), MIA (MIA-induced OA group), MH (MIA-induced OA with thermoresponsive hydrogel treatment group), MP (MIA-induced OA with lyophilized platelets treatment group), MD (MIA-induced OA with dextrose treatment group), and MT (MIA-induced OA with triamcinolone treatment group).
Regarding connective tissues, Figure 6(a) illustrates that both the control and sham groups exhibited superior connective tissue integrity in the femur and patella compared to all the MIA-induced OA groups. However, no significant difference was observed in the connective tissue performance among the MIA-induced OA groups, irrespective of the specific treatment received.
As for chondrodysplasia, Figure 6(b) reveals that the degree of normal cartilage in both the control and sham groups was lower compared to all the MIA-induced OA groups, whether in the femur or patella. However, it was noteworthy that regardless of the specific treatment received, none of the MIA-induced OA groups were able to effectively improve the level of chondrodysplasia.
Furthermore, let us delve into the analysis of mineralized hyaline cartilage. Figure 6(c) illustrates that the level of mineralized hyaline cartilage in both the control and sham groups was lower compared to all the MIA-induced OA groups, whether in the femur or patella. However, it was important to note that regardless of the specific treatment received, none of the MIA-induced OA groups were able to effectively reduce the level of mineralized hyaline cartilage.
Lastly, let us focus on the analysis of chondrogenesis. Figure 6(d) reveals that both the control and sham groups exhibited better chondrogenesis compared to all the MIA-induced OA groups, irrespective of whether it was observed in the femur or patella. However, it was noteworthy that regardless of the specific treatment received, none of the MIA-induced OA groups were able to effectively reduce chondrodysplasia.
Discussions
In this study, a knee OA rat model was successfully established in female mice by intra-articular injection of MIA. Within this model, the thermoresponsive hydrogel exhibited notably superior performance in dynamic behaviors, specifically in terms of print area, stability, and step cycle, when compared to commercially available products such as lyophilized platelets, dextrose, and triamcinolone.
Currently, robust animal models serve as indispensable tools for fundamental research into novel therapeutic approaches. Considering that approximately 70% of the patients affected by OA are female, our study specifically focuses on female rats as the target subjects. Although existing OA animal models possess certain advantages, none of them comprehensively represent all the pathologies, behaviors, and mechanisms associated with OA. Taking into account the clinical requirements for pain management and rehabilitation interventions, we have ultimately chosen the MIA-induced OA model.
The injection of MIA into the knee joint induces a gradual degradation of cartilage, leading to the development of pain-like behaviors. The MIA model of OA holds promise for studying new treatments targeting OA-associated pain and assessing pharmacological effects for several reasons. Firstly, the pathological changes triggered by MIA closely resemble those observed in human OA, encompassing cartilage loss and subchondral bone alterations.24–26 This model has been extensively utilized in fundamental research due to its ability to replicate the time course, histopathological changes, and pharmacological characteristics associated with OA-related pain. Additionally, the severity of pathological progression can be controlled by adjusting the MIA concentration in the control group. Moreover, compared to other OA models, MIA can rapidly induce pain-related manifestations, thereby reducing the cost of screening potential therapies. Consequently, this model may offer greater predictability for evaluating the clinical effectiveness of novel pharmacological agents compared to chronic or acute OA models. 27
At day 21 (D21), the triamcinolone treatment group exhibited relatively better performance compared to the other treatment groups; however, no statistically significant difference was observed in terms of pain suppression efficacy (Figure 5(a)). This finding aligns with the clinical treatment approach of administering triamcinolone during the acute phase of OA pain. Overall, based on the results presented in Figures 5 and 6, it can be inferred that none of the treatments employed in this study had an impact on the degree of knee cartilage lesions. This was primarily attributed to the limited regenerative capacity of cartilage, which lacks nourishing pathways (such as blood vessels, nerves, and lymph) and consists of chondrocytes with low proliferative activity. 28 Consequently, once damaged, cartilage faces significant challenges in self-repair, leading to the results depicted in Figures 5 and 6.
Currently, treatment methods for cartilage defects mainly involve autologous cartilage transplantation, microfracture (bone marrow stimulation), and autologous chondrocyte transplantation. 29 Although these methods demonstrate certain therapeutic effects, they also possess drawbacks such as donor site damage, inconsistency between the repaired area and surrounding cartilage characteristics, and poor interface healing. 30 Consequently, enhancing the implementation of clinical guidelines, including weight loss and rehabilitation programs, as well as effective pain control, was considered a crucial aspect for improving the quality of life and functionality of individuals with OA. 6
In our research, static and dynamic behavioral analysis has been widely recognized as a valuable reference for assessing pain control, quality of life, and functional abilities in individuals with OA. Clinical assessments of the effectiveness of OA therapeutics often focus on their palliative effects. By evaluating weight bearing during stance, mechanical hyperalgesia, mechanical allodynia, and altered gait, the pain and disease progression status of OA rats can be further assessed. 31 It was worth noting that in dynamic behavioral analysis, larger error bars were commonly observed in small animal experiments, particularly those involving pain-related modes.17,18,20,21
In terms of the trend observed in the thermoresponsive hydrogel treatment group from D42 to D49 in Figure 4 and supplementary Figure 3, it can be noted that the favorable therapeutic outcome was no longer evident. This observation could be attributed to the degradation period (approximately 14 days) of the thermoresponsive hydrogel, as reported in previous studies. 16 Hence, in future joint-related therapeutics, it may be necessary to consider reapplying the thermoresponsive hydrogel every 2 weeks to maintain its efficacy.
Compared to lyophilized platelets, dextrose, and triamcinolone therapies, the thermoresponsive hydrogel therapy employed in this study exhibited statistically superior effects on behavioral evaluation indicators, specifically in terms of print area, stand, and step cycle. This notable improvement can be attributed to the prolonged retention and gradual degradation of the thermoresponsive hydrogel within the affected area. These characteristics are particularly advantageous for joints with high mobility requirements, as they enable sustained therapeutic action.15,16 In contrast, treatments involving lyophilized platelets, dextrose, and triamcinolone may result in the displacement or degradation of the treatment agents due to the intense joint activity, limiting the possibility of long-term efficacy. 13
Since the selected therapies in this study did not exhibit significant therapeutic efficacy on the MIA-induced OA model, this outcome can be attributed to the model's classification as a robust and rapid pain phenotype. At this stage, the OA model can be divided into two categories: spontaneous and non-spontaneous. However, the spontaneous OA model was often challenging to precisely control the disease progression, and the process itself was time-consuming and costly, resulting in a relatively low utilization rate. 32 The non-spontaneous model primarily encompasses chemically-induced OA using MIA and surgically-induced OA through anterior cruciate ligament (ACL) transection. However, this model was not chosen for this study due to its aggressive nature, rapid cartilage degeneration, and slow and inconsistent development of pain-related behaviors. 27 Nonetheless, this model has the potential to induce lesions that resemble the progression of post-traumatic human OA, thus offering a non-acute and pain-based model for investigation. 33 Future studies that focus on comparing treatments in the ACL-OA state may provide a better understanding of the long-term differences between various therapeutic approaches.
Conclusions
In this study, we successfully established a knee OA rat model in female mice by performing intra-articular injection of MIA. We conducted comprehensive investigations to evaluate the therapeutic effects of lyophilized platelets, dextrose, triamcinolone, and the thermoresponsive hydrogel. These investigations included assessments of static and dynamic animal behavior, histopathology, and histoimmunology. Comparable results were observed among the four treatments in terms of static animal behavior, histopathology, and histoimmunology, with no significant differences.
However, in terms of dynamic behavior, the group treated with the thermoresponsive hydrogel exhibited superior behavioral performance compared to the groups treated with lyophilized platelets, dextrose, and triamcinolone. This finding highlights the suitability of the thermoresponsive hydrogel, developed by our research institute, for further integration with effective non-pharmacological treatments for OA, such as weight loss and exercise programs. Furthermore, when combined with relevant therapeutic drugs for long-acting sustained-release therapy in the future, this technology holds promise as a novel approach to OA treatment.
Supplemental Material
Supplemental Material - Potential of thermoresponsive hydrogel as an alternative therapy for rat knee osteoarthritis
Supplemental Material for Potential of thermoresponsive hydrogel as an alternative therapy for rat knee osteoarthritis by Yi Kung
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Taiwan University Hospital (NTUH 109-M4670), National Taiwan University Hospital Hsinchu Branch (110-BIH009, 111-HCH003) and the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-002-045-MY3, MOST 110-2314-B-002-070, MOST 111-2314-B-002-164-MY2).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.