
Abstract
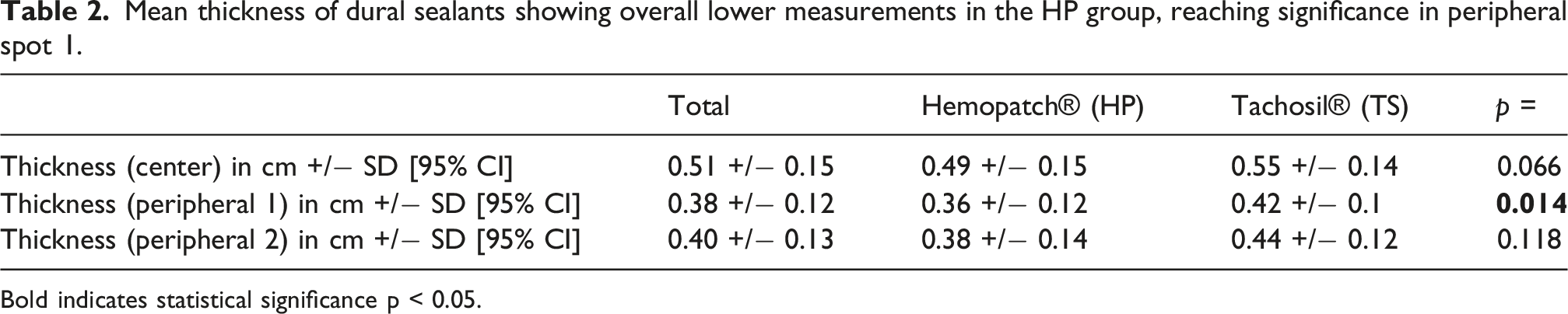
This study compares the in vivo behavior (epidural thickness and complication rate including the development of cerebrospinal fluid fistula, CSF-fistula) of the newer dura sealant HEMOPATCH® (HP) with that of the well-established patch TACHOSIL® (TS) in early postoperative magnetic resonance imaging (MRI) and during the clinical course after supratentorial cranial surgery. This retrospective cohort study included 58 patients with complete datasets (HP group n = 39, TS group n = 19). Inclusion criteria were supratentorial surgery, use of one dura sealant (HP or TS), re-implantation of the bone flap, and MRI within 3 months after surgery. We measured the thickness of the used dura sealant in axial T1-weighted sequences of postoperative MRI on the area of suture (central) and on two peripheral spots. Additionally, we examined the incidence of surgical revisions due to hemorrhage, infection, and wound healing disorders. The mean central thickness of HP and TS were 0.49 cm and 0.55 cm, respectively. This difference in size was not statistically significant (p = 0.066). The peripheral epidural thickness of HP (d = 0.36 cm) was significantly smaller than of TS (d = 0.42 cm; p = 0.014) in one of two points of peripheral measurement. Similarly, the two groups did not differ significantly in the complication rate needing surgical revision, including CSF fistula (HP 3/39 vs TS 3/19; p = 0.34). The biological behavior in terms of growth, swelling, induction of wound healing disorders, hemorrhage, and development of CSF-fistula showed no statistically significant difference within this small descriptive cohort.
Introduction
Watertight dural closure after craniotomy is an important principle in neurosurgery, as it prevents cerebrospinal (CSF) fistula, wound-healing disorders, and postoperative wound infections, thereby actively reducing the rate of surgical revision. 1 In addition to autologous tissues such as galea-periost flaps, muscle, fatty tissue, or fascia lata, artificial substitutes that allow immediate sealing of the sutured dura are widely used.1–4 This avoids additional remote trauma due to autologous tissue harvesting.
A variety of sealants have been approved by the Federal Drug Administration (FDA) and the European Medicines Agency (EMA). One of the most frequently applied dural sealants is the bioabsorbale fibrin sealant Tachosil® (TS) (Corza Medical, Westwood, MA, USA), a dural onlay that was designed as a sealant and hemostatic product. As TS has been used worldwide for many years, its safety and efficacy have been repeatedly evaluated.5–8 Recently, the new dural sealant Hemopatch® (HP) (Baxter Healthcare SA, Zurich, Switzerland) has been introduced, which has also been designed as a topical hemostat.
TS is an equine collagen sponge coated with an active side of human fibrinogen and thrombin, that is activated by forming a stable fibrin clot after dissolution of the added fibrinogen after contact to body fluids. 9 HP consists of a bovine collagen pad coated with polyethylene glycol-coated (PEG-coated) matrix. It activates via a combination of collagen’s intrinsic clotting properties and the PEG’s ability to bind to tissue proteins and accelerate clot formation. 10
A recent review has shown a significant benefit of both patches as augments of dural suture in preventing CSF leaks. 11
HP has already been evaluated in several laboratory investigations and clinical studies of various surgical disciplines.12–15 In neurosurgery, the use of HP is already well established.16,17 We previously evaluated the feasibility of HP as a dural sealant in 22 and 123 patients with cranial disorders, and in 24 patients with spinal disorders.17,18
A study comparing HP to TS in liver surgery has shown similar properties of the two patches in controlling intraoperative bleeding. 19 In infratentorial neurosurgery, a comparison between HP and TP showed no significant difference in the development of CSF fistula. 20
However, these two add-ons have not yet been compared in a clinical study as dural sealants in supratentorial neurosurgery. Data regarding the epidural morphology of both are lacking.
Therefore, we retrospectively evaluated the two sealants for their efficacy in preventing CSF fistula and examined the epidural extension visible on postoperative magnetic resonance imaging (MRI). In addition, we focused on any sealant-related morbidity, such as local infection or epidural hemorrhage requiring surgical revision. To the best of our knowledge, no data are available so far that compare the material changes and complication rates of these dural sealants in neurosurgery.
Material and methods
We retrospectively evaluated the data of consecutive patients treated at our department between January 2017 and January 2023. Inclusion criteria were age older than 18 years, elective supratentorial surgery with consecutive postoperative gadolinium-enhanced MRI within 3 months of surgery, primary dural suture with no gap larger than 3 mm, absence of other bioabsorbable substitutes such as fibrin glue or second patches, re-insertion of the autologous or allogenic bone flap, and epidural application of either HP or TS. Patients with incomplete datasets and other indication for dural sealing patch use than dural suture augmentation were excluded. The decision on sealant use was at the surgeons discretion.
Both dural sealants are applied on top of the dural suture to completely cover the sutured rims of the dura with no gap larger than 3 mm (see Figure 1). There is no difference in preparation of the dural sealing. The sealants were trimmed to fit the area of craniotomy. TS is applied after immergence in irrigation fluid and gently pressed onto the dura with a moistened surgical gauze for three to 5 min. HP is applied dry to the dura and held in place with dry gauze for 2 min. Epidural onlay on top of the dural suture. 1: Bone; 2: Dural sealant; 3; Dura; 4: Brain parenchyma; 5: Dural suture; 6: Area of peripheral measurement; 7: Area of central measurement. With kind approval by Baxter International.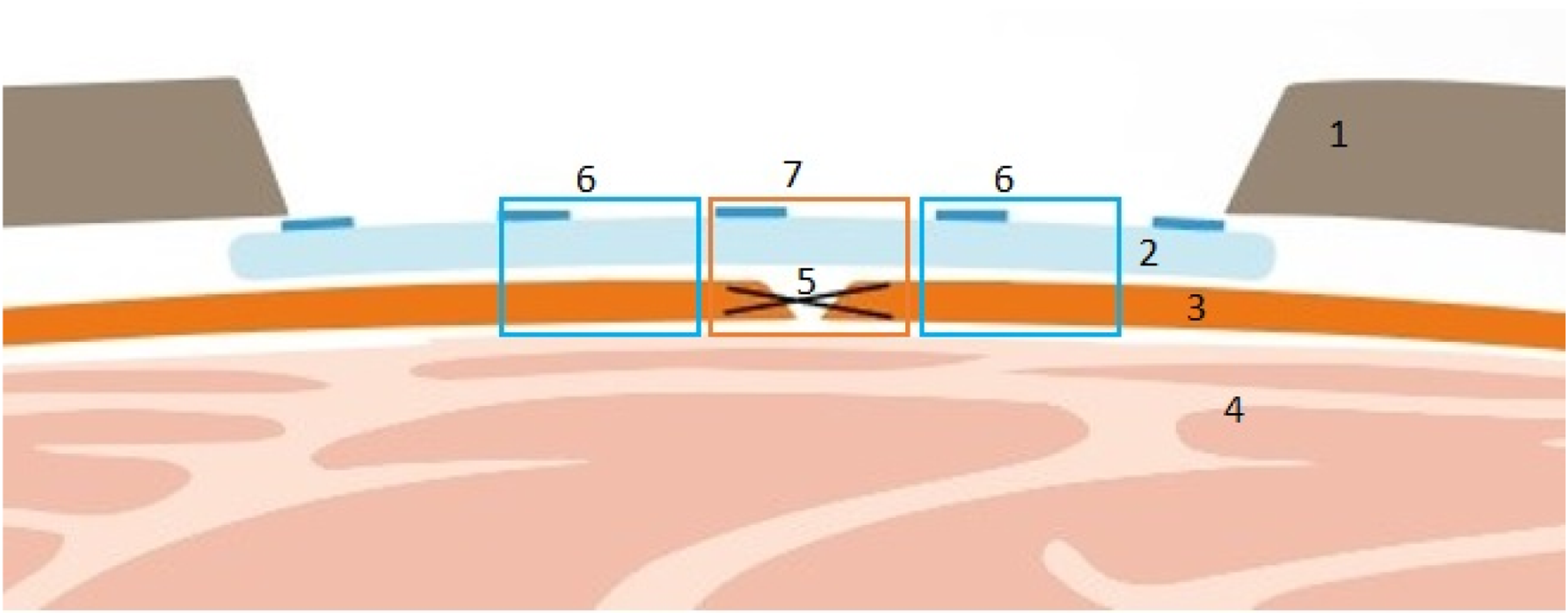
Baseline data of included patients and histological diagnoses.
Furthermore, we evaluated the (gadolinium-enhanced) T1-sequences of all available postoperative MR images made within 3 months of surgery. Imaging data was acquired on a Siemens Skyra 3-Tesla full-body scanner (MAGNETOM Skyra; Siemens, Erlangen, Germany). A neuroradiologist blinded to the sealants used manually measured the central and peripheral epidural thickness of the implanted dural sealants. Central thickness measurement included the underlying dural tissue, the suture, and the sealing patches, peripheral only dura and sealant (see Figure 2). Measurement of the thickness (white = central diameter, black = peripheral diameter) on an early axial T1 MRI scan on the first postoperative day after right frontal craniotomy.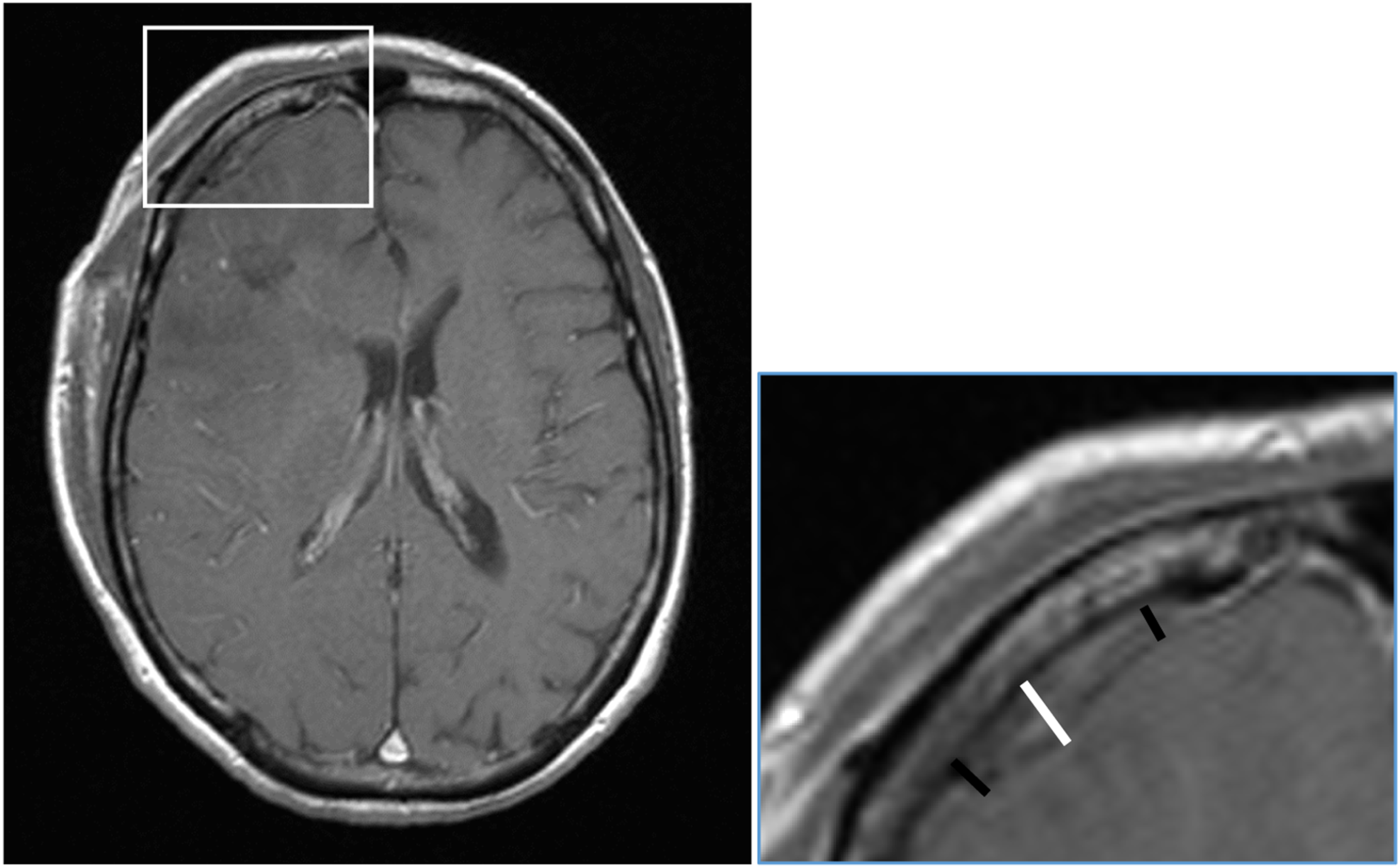
Thickness of HP and TS was compared on the central and two peripheral sites of measurements. Since baseline pathology varied significantly between the groups, a subgroup analysis was performed to determine the potential impact.
To address the temporal imbalance between groups, a subgroup analysis restricted to early imaging (within 28 days) was performed.
Correlation between age and dural sealant thickness as well as between timing of MRI and thickness was calculated. Additionally, correlation between sealant thickness and complications was calculated.
Statistical analysis was computed with SPSS 27 (IBM, Armonk, New York, USA). Significance was set at p < 0.05. The Kolmogorov-Smirnov test and the Shapiro-Wilk test did not show normal distribution in all groups. Comparison of means were calculated with the Mann-Whitney-U test. Effect sizes (r) were calculated according to Cohen’s benchmarks, where values greater than 0.1, 0.3 and 0.5 represent small, medium, and large effects, respectively. Categorical variables were compared with the Chi-Square test. Selected variables were tested for correlations using Spearman’s correlation. Spearman’s Rho (rs) and p-values are reported in these analyses.
Results
58 patients (22 women, 36 men; mean age 60 years, range 22 to 86 years) were included in the analysis; 39 patients had received HP and 19 patients TS.
Dural sealant thickness measurements were performed on 68 MR images (47 HP, 21 TS). 52 scans were obtained within 28 days (32 HP, 20 TS) and 16 scans within 3 months of surgery (15 HP, 1 TS).
Mean thickness of dural sealants showing overall lower measurements in the HP group, reaching significance in peripheral spot 1.
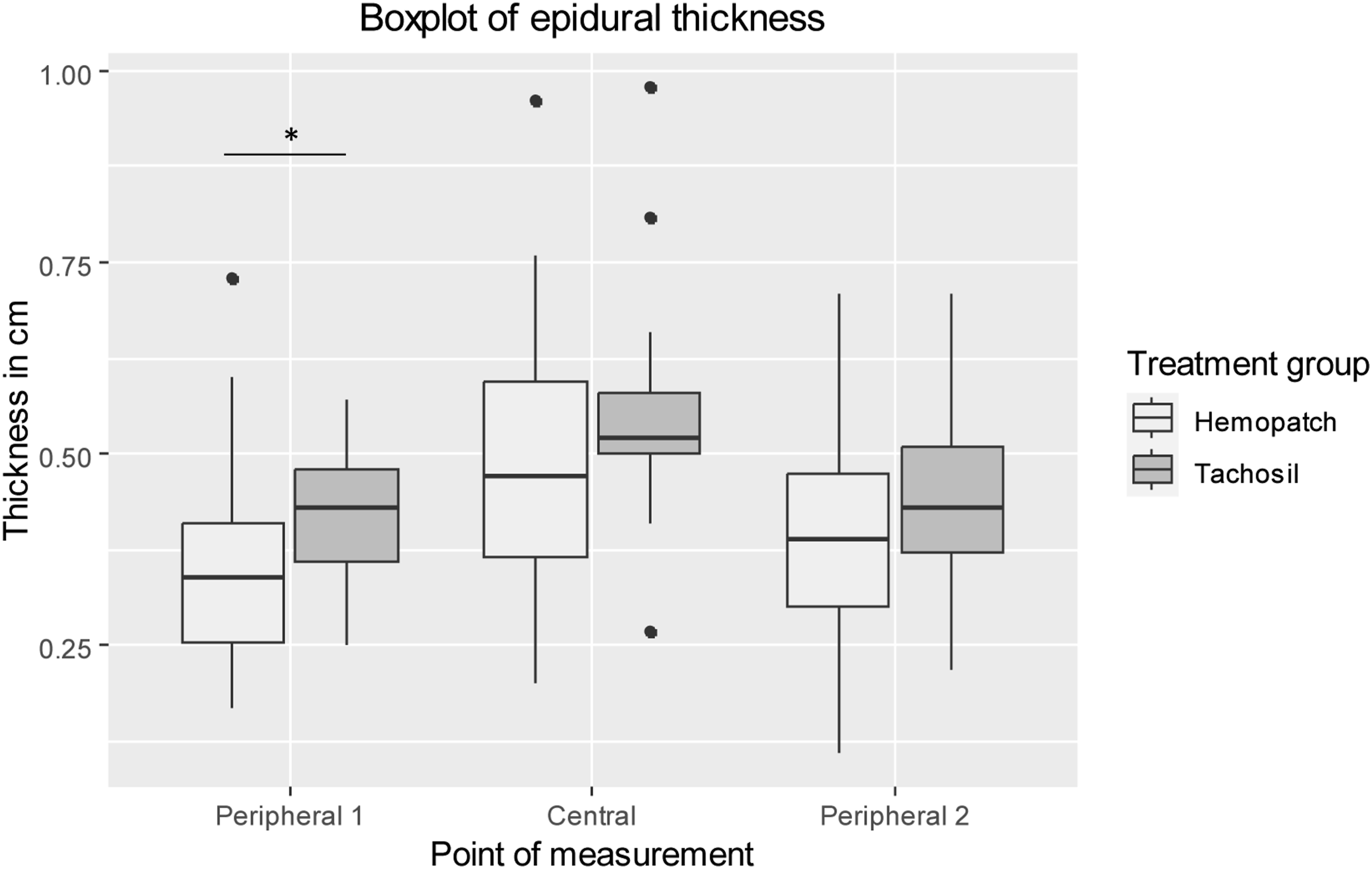
Boxplot of epidural thickness of patches in cm at all points of measurement. Significant smaller diameter was shown for the HP group compared to the TS group in peripheral diameter 1 (p = 0.014). Outliers are shown as dots. Significance is shown by “*”.
When comparing tumor patients, the difference in dural sealant thickness remained significant for one of the peripheral sites (p = 0.012; r = 0.31), and without significance in the central (p = 0.052; r = 0.24) and other peripheral site (p = 0.072; r = 0.22). Comparison of only glioma patients produced similar results (p (per1) = 0.033; p (cent) = 0.91; p (per2) = 0.108).
Within the early MRI group (within 28 days), there was no significant difference in distribution, with a trend towards lower thickness in the HP group (d (per1) = 0.37 +/− 0.13; d (cent) = 0.51 +/− 0.15; d (per2) = 0.40 +/− 0.13) compared to the TS group (d (per1) = 0.42 +/− 0.10; p (per1) = 0.06; r (per1) = 0.26; d (cent) = 0.56 +/− 0.14; p (cent) = 0.22; r (cent) = 0.17; d (per2) = 0.44 +/− 0.12; p (per2) = 0.35; r (per2) = 0.17).
Timing of MRI showed no significant correlation with dural sealant thickness (rs (per 1) = −0.13, p = 0.38; rs (cent) = −0.18, p = 0,24; rs (per 2) = −0.22; p = 0.13). There was no correlation between age and dural sealant thickness (rs (per1) = 0.002, p = 0.99; rs (cent) = -0.04, p = 0.74; rs (per2) = −0.07, p = 0.57). No correlation was observed between complications and sealant thickness (rs (per1) = 0.026, p = 0.834; rs (cent) = −0.106, p = 0.388; rs (per2) = 0.095, p = 0.442).
Complications requiring surgical revision showing no significant differences.

Discussion
To the best of our knowledge, no studies have yet compared radiographic morphologic changes due to the use of epidural TS and HP after supratentorial craniotomy. Furthermore, we identified the rate of procedure-related complications in terms of infection, CSF fistula, and hemorrhage. Our study showed no significant difference in rate of surgical complications. The thickness of HP was lower than of TS at all three sites of measurement, but reached only statistical significance at the peripheral position 1 (p = 0.014). After adjustment for early MRI (within 28−days), no significant difference could be observed.
Overall epidural diameter
The mean central epidural diameter of all used dural sealants was 0.51 +/− 0.15 cm. This measurement includes the dural tissue, the suture, and the dural sealing patch (see Figure 1). On average, the dura measures approximately 0.11 cm. 21 Our standard dural suture is a Terylene 4.0 suture with a minimum diameter of 0.15 mm. So far, there is no reliable research on the thickness of TS, especially after compression and contact with CSF or blood.
According to the manufacturer, dry and uncompressed TS has a thickness of 0.5 cm. In-vitro measurement of thickness with a caliper showed HP to measure 0.2 cm in thickness when dry and uncompressed. However, uncompressed patches had a mean thickness of 2.5 mm after 24 h of immersion in human citrated plasma, with a maximum measured thickness of 2.8 mm. 10 The results suggest a difference in the behavior of TS and HP on live dural tissue after suture and contact to the patients homeostasis. Further scientific research on the different biological behavior of dural sealants when getting in contact with blood, air, and CSF is still lacking.
The two mean peripheral thicknesses were 0.38 +/− 0.12 cm and 0.40 +/− 0.14 cm, which is in line with the measurements of the dura and the known diameters of the sealants. This is relevant for neuroradiological differentiation. Knowing the expected postoperative range for intact sealants helps the clinician rule out unintended mass effect, like epidural hematoma or infectious fluid collections on postoperative imaging, preventing anxiety driven follow-up imaging or revision surgery.
Difference in thickness between the sealants
Our data showed a significant lower thickness in one of the two peripheral sites. The other sites and subgroup analysis of early MRI showed lower diameters, although without statistical significance.
The difference of the uncompressed sealants in vitro partially explains the lower measurements of HP. A further mechanism could be the compression to the surgical field and soaking of body fluids or saline. In addition, imperfect pressure distribution after application to the surgical field could explain the difference between the two peripheral spots.
Influence of MRI timing and biomaterial degradation
A critical factor in the evaluation of thickness of bioabsorbable dural sealants is their time-dependent degradation and swelling, which is driven by enzymatic cleavage and fluid absorption of the underlying collagen matrices.22–24To eliminate the potential bias derived from difference in timing between the groups, we conducted a subgroup analysis restricted to early imaging (within 28 days). Within this early cohort, the significant difference in peripheral thickness was attenuated (p = 0.06). However, the calculated effect size remained medium (r = 0.26), indicating a relevant descriptive trend towards a lower peripheral thickness in the HP group even in the early postoperative phase.
Furthermore, our correlation analysis demonstrated that timing of MRI did not significantly correlate with measured sealant thickness. Together, these findings suggest that the variations in MRI timing within the 3-months window did not act as a profound confounding variable in our thickness measurements.
Difference in procedures
The subgroup analyses of all tumor patients and Glioma patients showed results similar to the total analysis. While the baseline pathology varied significantly, the underlying surgical principle of applying the dural sealant over a primary suture line remains technically identical across all procedures, reducing the impact of the diagnosis on localized sealant thickness measurements.
Difference in biological origin
Both sealants use animal product, which could increase the risk of infectious disease and immunologic reactions. HP consist of a collagen pad derived from bovine dermis. This inherits a risk of bovine spongiform encephalopathy. Since the bovine materials are sourced from countries with negligible risk according to the classification of the WHO, and there has not been any reports of encephalopathy after use, the overall risk is low. 10 TS, formerly also using bovine collagen, has replaced it with equine collagen, which overall has a low likelihood of immunologic reactions. 25 Although the fibrinogen in TS is from thoroughly tested humans, the use of TS is not recommended in pregnant women due to the potential theoretical risk of Parvovirus B19. 9
There have not been any recorded cases of Parvovirus B 19 or transmission of prions by manufactured plasma products. 9 The overall low infection rate in our dataset seems to rather contradict the reported risks.
Complications
Although this work is underpowered to reliably depict complication rates, there was no statistically significant difference in the complication rate between the HP group (3/39 = 7.7%) and the TS group (3/19 = 15:8%; p = 0.34), and no record of fistula in the HP group. Nowak et al. showed similar results for posterior fossa surgery: fistula occurred in 6.2% of patients receiving TS and in 1.4% of patients receiving HP. 20
The rate of wound infection in the HP group (2/39 = 5.1 %) is within the range of 0.8-7.0% postoperative wound infection reported in previous studies. 26 There were no infections in the TS group.
The percentage of postoperative hemorrhage (HP: 1/39 = 2.6%; TS: 1/18 = 5.6%) is comparable to the percentage of 1.9% found in other recent analyses. 27
Our data did neither show an increase in post-operative complications, nor a correlation between complications and thickness. Hence, there is no hint towards a potential harm through the difference in epidural thickness.
Dural sealants as surgical adjuncts
The debate over the need for expensive dural sealants remains controversial, despite the proven need for watertight dural closure to reduce morbidity and mortality. 3 Barth et al. did not find any significant improvement in surgical revision rates for CSF leakage in 137 patients solely treated with watertight dural sutures compared with patients treated with additional dural sealants and with patients solely treated with loose dural sutures. 28 On the contrary, according to Hutter et al., the need for dural sealants to achieve watertight dural closure was an independent risk factor for CSF leakage, but dural sealants also shortened the mean time on the intermediate care unit of patients undergoing supratentorial craniotomy. 29 In favor of dural sealants, the latest meta-analysis by Shah et al. showed a benefit of dural sealants as reinforcement of dural suture in reducing CSF leakage. 11
Regardless of this debate, the use of dural sealants is widely accepted, and the efforts to find the best way of how to seal dural tissue after craniotomy are ongoing.2,4,30
Limitations
The limitations of this work are the small number of patients, the retrospective study design and the monocentric data collection, although allowing for significant results, not allowing for generalizability of the data. This work is also underpowered to allow a meaningful comparison of complication rates. Selection bias is introduced by group allocation at the surgeons’ discretion. The different sample sizes and the uneven distribution of sex and diagnoses are potential sources of bias. While these baseline imbalances could constrain internal validity of our comparison, the identical surgical technique used for sealant application across the different diagnoses and the subgroup analysis mitigate a profound confounding effect on thickness measurements. Nonetheless, these factors limit the external validity of our data. An even distribution and bigger sample would allow for more significant conclusions.
A prospective multi-arm RCT comparing dural suture alone against suture plus several dural sealants could overcome these limitations and help to determine the best technique for dural closure after craniotomy to improve patient outcomes.
Conclusion
Comparing the epidural thickness HP and TS, we found an overall lower diameter with a significant smaller epidural diameter in HP in one of the two peripheral sites. In our small observational cohort, we did not find any evidence for harm of either sealant in terms of complications or a clinical advantage related to the diameter.
Footnotes
Acknowledgements
The authors would like to thank Gerhard Moersdorf (Medical Affairs), Baxter International Inc. for support with Hemopatch data.
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the internal review board (Ethics Committee of the University of Regensburg, 21-2907-104).
Consent to participate
The need for patient consent was waived by the ethics committee due to the retrospective nature of this work.
Author contributions
Jakob Rossmann – Writing – original Draft, Formal Analysis, Software. Andreas Schicho – Investigation. Julius Höhne - Validation. Johannes Falter- Writing – Review & editing. Thomas Eibl - Writing – Review & editing. Eduard Yakubov - Writing – Review & editing. Nils Ole Schmidt - Resources. Karl-Michael Schebesch – Conceptualization, Writing – Review & editing. Methodology, Supervision, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author and Karl-Michael Schebesch have received research support for the conduct of this study by Baxter Deutschland GmbH, Germany.
Declaration of conflicting interests
The corresponding author, Karl-Michael Schebesch, and Julius Höhne declare honoraria and travel grants from Baxter Deutschland GmbH, Germany. All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work. All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.