
Abstract
To engineer a porous nanohydroxyapatite/polyphosphoester-amino acid composite bone graft substitute (nHA/PPE-AA) in granular form and evaluate its reparative efficacy and in vivo safety in a rabbit femoral condyle critical-sized defect (CSD) model. Porous nHA/PPE-AA granules were fabricated using polyphosphoester-amino acid copolymer (PPE-AA) as the organic matrix and nanohydroxyapatite (nHA) as the inorganic phase. Material characteristics were examined by scanning electron microscopy, X-ray diffraction, and Fourier-transform infrared spectroscopy. A rabbit femoral condyle CSD model (10 × 10 × 10 mm3) was randomly assigned to nHA/PPE-AA, positive control (calcium sulfate), and blank groups. Bone repair was assessed by gross inspection, serum bone turnover markers, digital radiography (G/N ratio), micro-computed tomography, sequential fluorochrome labeling, histology, interfacial SEM, and BMP-2 mRNA expression. Safety was evaluated by ESR, WBC, CRP, and histology of major organs and peri-implant tissues. The nHA/PPE-AA composite exhibited an interconnected porous granular structure (35%–55% porosity, 3–7 MPa compressive strength). XRD and FTIR confirmed stable coexistence of nHA and PPE-AA. Gross and imaging analyses demonstrated progressive defect repair, with higher G/N ratios and more trabecular regeneration in the nHA/PPE-AA group. Fluorochrome labeling and histomorphometry indicated accelerated mineralization and shorter lag time. Histology and SEM confirmed mature neobone formation and superior bone-material integration. RT-qPCR showed sustained BMP-2 upregulation from 1 to 3 months, peaking at 3 months. Safety assessments revealed only transient changes in ESR, WBC, and CRP, with no significant organ pathology. Porous nHA/PPE-AA granules provide interconnected porous structure, moderate mechanical support, osteogenic activity, and good in vivo biocompatibility. In a rabbit femoral condyle CSD model, they promoted new bone formation, accelerated mineralization, and improved bone-material interface, highlighting their potential as a translationally relevant bone void filler.
Introduction
Bone defects caused by trauma, tumors, infection, osteoporosis, and related conditions remain a major challenge in orthopaedic practice.1,2 Against the backdrop of rapid population aging in China, the burden of osteoporosis and fracture-related disorders continues to rise, driving an increasing clinical demand for effective bone defect reconstruction.3,4 Although autologous bone grafting is still regarded as the gold standard for bone repair, its clinical utility is inherently constrained by limited graft availability and donor-site morbidity.1,5 Allogeneic bone grafts partially address the issue of tissue supply, yet they are still compromised by the risks of immune rejection and disease transmission.6–8 Consequently, there is an urgent need to develop novel bone substitute materials that combine excellent biocompatibility, appropriate mechanical competence, and robust bone-regenerative capacity. 2
Despite substantial progress in biomaterials research, currently available materials remain far from ideal. Bioactive ceramics exhibit favorable osteoconductivity and biological activity; however, their intrinsic brittleness and proneness to fracture severely limit their applicability, particularly in mechanically demanding settings.9,10 Polymeric materials, by contrast, offer improved processability and compositional tunability, yet they often suffer from inadequate surface wettability, suboptimal cell adhesion, and insufficient osteogenic activity. More importantly, their degradation behavior frequently fails to match the pace of tissue regeneration, while the resulting degradation by-products may disturb the local microenvironment and even provoke inflammatory responses.11–13 Metal implants provide structural support, but are fundamentally limited by stress shielding effects and poor intrinsic bioactivity.14,15 Taken together, neither inorganic nor organic materials alone can fully satisfy the complex requirements of bone defect repair. This limitation strongly underscores the need for composite bone substitutes that integrate the complementary advantages of both material classes. 16
Hydroxyapatite is a classic bioceramic that has been extensively used in bone repair because of its close compositional resemblance to the mineral phase of native bone, and it has been consistently shown to possess favorable biocompatibility and osteogenic potential.17,18 Importantly, nanoscale hydroxyapatite can further enhance osteogenic bioactivity by better recapitulating the nanostructural features of natural bone.19,20 Polyphosphoesters (PPEs), which share structural similarities with nucleic acids and phosphate-containing biomolecules, exhibit high biocompatibility, cellular affinity, and permeability. Their phosphoester backbones are susceptible to hydrolytic and/or enzymatic degradation under physiological conditions, generating phosphorus-containing small molecules that are theoretically amenable to metabolic clearance in vivo.21–23 Polyamino acids, composed of natural α-amino acids and non-α-amino acids, degrade into low-molecular-weight amino acid derivatives and have been widely recognized for their favorable biocompatibility and hydrophilicity; accordingly, they have been explored in artificial skin, controlled drug delivery, and bone repair biomaterials.24–27 Caprolactam-related structures have also found applications in the biomedical field. 28
On the basis of these material attributes, we proposed a strategy for developing a porous granular composite bone substitute by combining an organic matrix with an inorganic reinforcing phase. Specifically, a polyphosphoester-amino acid copolymer (PPE-AA) was constructed via in situ polymerization/copolymerization as the organic phase, and nanohydroxyapatite (nHA) was introduced as the inorganic component. Previous studies have suggested that the incorporation of amide bonds can strengthen hydrogen-bonding interactions and improve mechanical performance. 29 Therefore, caprolactam-related chain segments were deliberately introduced in the present design with the aim of enhancing both strength and toughness, thereby overcoming the brittleness that has long restricted conventional bioceramics under load-bearing conditions. At the same time, the synergy between amino acid monomers and PPE segments was expected to improve surface hydrophilicity and cellular compatibility, while allowing tunable degradation behavior through adjustment of the copolymer composition.30,31 We further postulated that the resulting nHA/PPE-AA porous granular bone substitute could mimic the biphasic “organic-inorganic” nature of native bone at both the structural and compositional levels. 16 In addition, the release of Ca and P ions, together with organic degradation products during degradation/dissolution, may collectively establish a microenvironment conducive to mineralization and bone regeneration, 32 thereby promoting new bone formation while enabling a more favorable coupling between material degradation and defect healing.
To test these hypotheses and to evaluate the translational potential of this material, we established a rabbit femoral condyle critical-sized defect model and performed a systematic, multiscale assessment of its reparative performance. Using gross observation, X-ray imaging, micro-computed tomography (micro-CT), histological analysis, sequential fluorochrome labeling, and RT-qPCR analysis of BMP-2 mRNA, we evaluated the feasibility and osteogenic efficacy of this material for the repair of critical-sized bone defects across multiple dimensions, spanning macroscopic appearance, radiographic reconstruction, microstructural regeneration, dynamic mineralization, and molecular expression.
Materials and methods
Preparation and characterization of nHA/PPE-AA
The nanohydroxyapatite/polyphosphoester-amino acid (nHA/PPE-AA) bone-filling material was developed by collaborating institutions. The preparation procedure was as follows.
4-Aminocaproic acid, 6-aminobutyric acid, and caprolactam were weighed and dissolved in deionized water at a mass ratio of 2:1:1, and the solution was transferred into a reaction kettle (Weihai, Shandong, China). A 50% (w/w) phosphoric acid solution was added as the catalyst, and the mixture was stirred under nitrogen protection at 150–200°C to remove water. The temperature was then increased to 210°C, and melt copolymerization was conducted for 2.5 h. Subsequently, 2.5%–10% cyclic phosphate ester (molar fraction) was added, and the reaction was continued for 0.5 h. After cooling, crude PPE-AA was obtained.
The PPE-AA was then crushed and transferred into an automatically controlled reaction kettle. Subsequently, nHA was added to achieve a mass fraction of 30 ± 5% in the system, followed by the addition of an appropriate amount of purified water for mixing. The mixture was stirred at 210 ± 5°C for 2.5 h. Cyclic phosphate ester (molar fraction, 2.5%) was subsequently added, and the reaction was continued for 1 h. After cooling, a semi-finished nHA/PPE-AA product was obtained. The semi-finished product was extrusion-molded using a twin-screw extruder (SHJ-20; Nanjing, China) at a gradient extrusion temperature decreasing from 160°C to 110°C and a screw speed of 30–50 Hz. The extrudate was pelletized and sieved to obtain irregular granules with particle sizes ranging from 300 to 5000 μm.
The positive control material was a medical-grade calcium sulfate artificial bone graft (Osteoset® pellets, without DBM; Wright Medical, USA), which was processed into 2–4 mm granules before implantation. Calcium sulfate was selected as the positive control because it is a clinically used, commercially available, resorbable bone void filler with established biocompatibility and osteoconductive properties. All implant materials were sterilized with ethylene oxide, fully aerated, and stored in sealed packages until use.
For material characterization, morphology was observed by scanning electron microscopy (SEM; S-3400, HITACHI, Japan). Phase composition was analyzed by X-ray diffraction (XRD; D8 ADVANCE, Bruker, Germany; Cu Kα radiation; 2θ = 10°–80°). Functional groups were examined by Fourier-transform infrared spectroscopy (FTIR; Nicolet iS10, Thermo Fisher Scientific, USA; 4000–400 cm−1). Porosity was determined by the Archimedes drainage method. Pore size distribution was measured statistically from SEM images. Compressive strength was determined by compression testing and reported as a range.
Animal model and surgery procedures
Thirty-six healthy adult New Zealand White rabbits of either sex, weighing 2.5–3.0 kg, were included in this study. All procedures involving animals were approved by the Institutional Animal Ethics Committee ([Information blinded for peer review]) and conducted in accordance with institutional and national guidelines for the care and use of laboratory animals. All efforts were made to minimize animal suffering and the number of animals used.
All animals underwent routine physical examination upon arrival. Normal food intake, mental status, activity, urination, and defecation were confirmed. The coat was smooth, with no evidence of trauma or infection. Routine blood tests and serum biochemistry showed normal liver and kidney function. After 2 weeks of acclimatization without abnormalities, the animals were enrolled in the experiment.
The rabbits were randomly assigned to three groups (n = 12 per group). A critical-sized bone defect measuring 10 × 10 × 10 mm3 was created in the femoral condyle of each rabbit. In the experimental group, the defect was filled with nHA/PPE-AA granules; in the positive control group, the defect was filled with calcium sulfate granules; and in the blank control group, no material was implanted after defect creation. Animals were euthanized at 1, 2, 3, and 6 months postoperatively for sample collection (n = 3 per group at each time point).
Food was withheld for 8 h before surgery. General anesthesia was induced by intravenous injection of 3% sodium pentobarbital (0.03 g/kg) through the marginal ear vein. A longitudinal incision approximately 3 cm in length was made on the medial side of the knee, and the medial femoral condyle was exposed layer by layer. Under saline irrigation, the defect was created using an orthopedic drill and curette until only the anterior and posterior cortices, the articular cartilage surface, and the subchondral bone were preserved. After irrigation, nHA/PPE-AA granules were tightly packed into the defect in the experimental group, and calcium sulfate granules were implanted in the positive control group. No implant was placed in the blank control group. The wound was closed in layers, and the animals were allowed unrestricted activity after surgery. Penicillin was administered intramuscularly at 40,000 U/day for 3 consecutive days postoperatively to prevent infection.
Macroscopic observation and serum markers of bone metabolism
At 1, 2, 3, and 6 months after surgery, three rabbits from each group were randomly selected for cardiac blood collection to measure bone-specific alkaline phosphatase (B-ALP) and N-terminal midfragment osteocalcin (N-MID). After euthanasia, femoral condyle specimens were harvested, and the degradation of implanted materials and filling of the defects by newly formed tissue were recorded and photographed.
DR imaging evaluation and G/N radiopacity ratio
Anteroposterior and lateral radiographs of the operated femur were obtained using digital radiography (DR). Radiopacity values were measured in the grafting area and the adjacent non-grafting normal bone area using Siemens imaging software. The grayscale ratio (G/N) was then calculated, with the normal bone area defined as G/N = 1.0. Because nHA is inherently radiopaque, the G/N ratio was interpreted as a composite radiographic parameter reflecting both residual implanted material and newly mineralized bone. Therefore, longitudinal changes in G/N over time, rather than the absolute value at a single time point, were used as supportive evidence of progressive mineralization. These radiographic findings were further interpreted together with micro-CT, fluorochrome labeling, and histological results.
Micro-CT scanning
After X-ray examination, the femoral condyles were harvested and scanned using a micro-computed tomography system (Quantum GX, PerkinElmer, USA) under the following conditions: 57 min per specimen, slice interval 50 μm, scanning range 20 × 25 × 25 mm, 90 kV, and 88 μA. The scans were used to evaluate bone density, new bone formation, and the distribution of osteoid/high-density signals within the defect region. Residual material and newly formed bone were differentiated mainly according to the morphology and distribution of high-density signals. Residual material was identified as discrete irregular granular signals, whereas newly formed bone was identified by interconnected trabecular architecture continuous with the adjacent host bone.
Sequential fluorochrome labeling and dynamic histomorphometry
Fourteen days and 3 days before euthanasia, calcein (15 mg/kg) and alizarin red (30 mg/kg), respectively, were injected into the gluteus maximus muscle. After specimen collection, fluorescence imaging was performed using an upright two-photon laser confocal fluorescence microscope. Calcein was excited at approximately 470 nm and detected at approximately 516 nm, showing green fluorescence, whereas alizarin red was excited at approximately 543 nm and detected at approximately 600 nm, showing red fluorescence. Images were acquired at a thickness of 5–10 μm, with 50–100 images collected per specimen.
The images were imported into NIS-Elements Analysis 4.50.00.64 software for reconstruction and quantitative analysis. The following parameters were calculated: (1) Interlabeled width (IL.WI), defined as the mean distance from the inner edge of the inner label to the inner edge of the outer label within the same trabecular structure, representing the thickness of mineralized bone formed during the interval between the two administrations. (2) Mineral apposition rate (MAR), defined as the amount of bone mineralization per unit time and calculated as MAR = IL.WI/labeling interval, reflecting osteoblastic activity and daily mineralization rate. (3) Mean osteoid seam width (MOSW), defined as the average width of unmineralized osteoid at bone-forming sites, namely the distance from the mineralization front to the marrow-side surface, reflecting the degree of osteoid mineralization. (4) Mineralization lag time (MLT), defined as the time required for osteoid to undergo mineralization after formation and calculated as MLT = MOSW/MAR.
Histological evaluation
Specimens were fixed in 10% neutral formalin for 48 h and decalcified in 10% EDTA for 4–8 weeks, with the decalcifying solution changed weekly. After gradient ethanol dehydration and paraffin embedding, serial sections of 5 μm thickness were prepared. The sections were stained as follows: (1) Hematoxylin and eosin (H&E) staining was used to evaluate inflammatory response, morphology of newly formed bone, and material degradation. (2) Masson’s trichrome staining was used to assess collagen deposition and bone matrix maturation. Stained sections were examined under an Olympus CX31 light microscope.
SEM observation
After fixation in 10% formaldehyde solution, the specimens were dehydrated in graded ethanol, air-dried, and sputter-coated with gold by ion sputtering. Bone-material interfacial integration was examined by SEM (HITACHI S-3400N, HITACHI, Japan).
Quantitative RT-PCR analysis of BMP-2 mRNA expression
Primer sequences and annealing temperatures used in RT-qPCR.
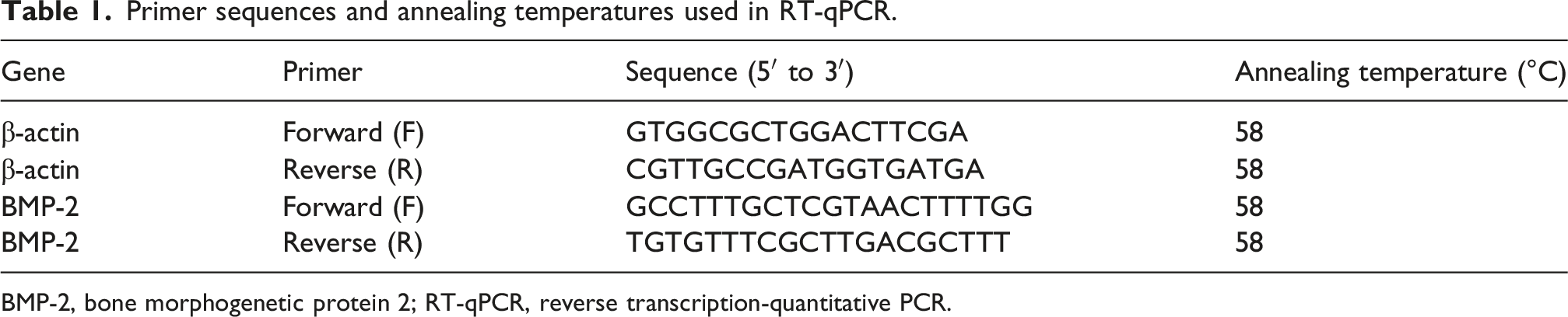
BMP-2, bone morphogenetic protein 2; RT-qPCR, reverse transcription-quantitative PCR.
Material safety evaluation
At 6 months after surgery, the liver, lung, kidney, brain, heart, and implant-related tissues (femoral condyle implantation site and intramuscular implantation site) were harvested for H&E staining. In addition, Masson’s trichrome staining was performed for the femoral condyle implantation site. Blood samples were collected at 1 day, 3 days, 7 days, 2 weeks, 1 month, 3 months, and 6 months postoperatively for measurement of erythrocyte sedimentation rate (ESR), white blood cell count (WBC), and C-reactive protein (CRP).
Statistical analysis
Quantitative data are presented as mean ± standard deviation. Statistical analyses were performed using SPSS 19.0 software (SPSS Inc., Chicago, IL, USA). At each time point, one-way analysis of variance (one-way ANOVA) was used to compare the experimental, positive control, and blank groups, followed by pairwise comparisons. A value of p < 0.05 was considered statistically significant.
Results
Characterization of nHA/PPE-AA porous granules
As shown in Figure 1, PPE-AA copolymer was successfully synthesized and combined with nHA to form a composite system. The nHA/PPE-AA material appeared as gray-white irregular granules with particle sizes of approximately 300–5000 μm (Figure 1(b)). SEM revealed a distinct porous architecture, with rough pore walls and interconnected pores. The pore size was mainly distributed within the range of 20–500 μm, and the initial porosity of the material was 35%–55% (Figure 1(c)). Preparation and characterization of the nHA/PPE-AA composite material. (a) Schematic illustration of the synthetic route of PPE-AA. (b) Gross morphology of the nHA/PPE-AA porous granules, showing irregular particles with diameters of approximately 300–5000 μm (scale bar = 1000 μm). (c) SEM image of the porous nHA/PPE-AA structure, showing rough pore walls and an interconnected porous architecture; pore sizes ranged from approximately 20 to 500 μm (scale bar = 20 μm). (d) XRD patterns of PPE-AA, nHA, and nHA/PPE-AA. PPE-AA exhibited a broad diffuse peak at approximately 2θ = 20.32°. The composite retained the characteristic diffraction peaks of nHA, including the peak cluster near 2θ = 31.84°, indicating successful incorporation of nHA while preserving its crystalline features. (e) FTIR spectra of PPE-AA, nHA, and nHA/PPE-AA. nHA showed an -OH absorption band at 3573.3 cm−1 and characteristic PO43- vibration bands at 1095.2, 1041, 993.7, and 962.3 cm−1. PPE-AA exhibited a -CH2- stretching vibration band at 2922.7 cm−1, a carbonyl band at 1730 cm−1, and amide-related bands at 1649.6 and 1541.1 cm−1. The composite exhibited characteristic bands from both phases, confirming the coexistence of inorganic nHA and organic PPE-AA within the nHA/PPE-AA system.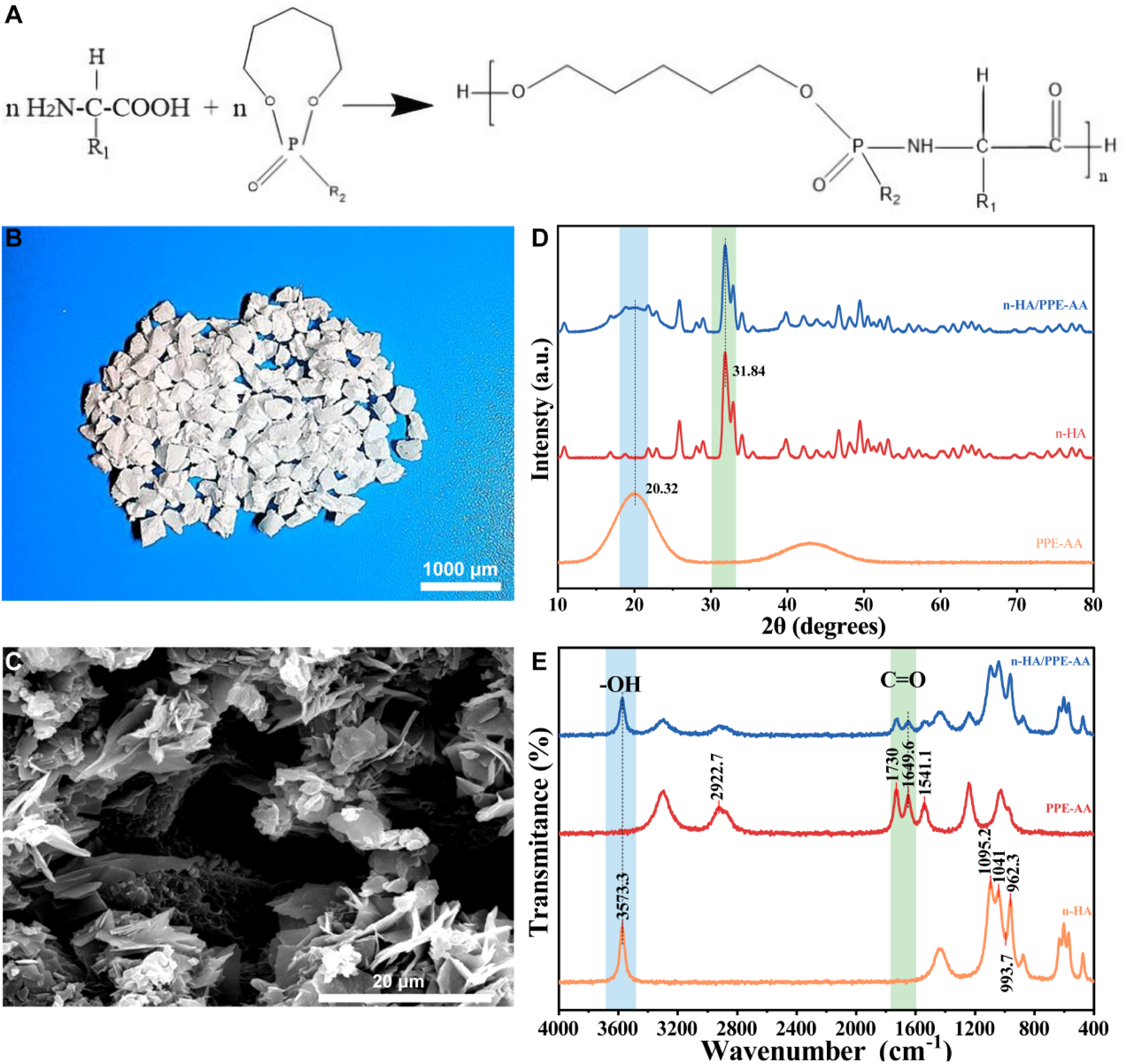
XRD analysis showed a broad diffuse peak for PPE-AA at approximately 2θ = 20.32°, indicating that the polymer was predominantly amorphous. nHA exhibited characteristic crystalline diffraction peaks, particularly a prominent peak cluster around 2θ = 31.84°. In the nHA/PPE-AA composite, the characteristic diffraction peaks of nHA, including the peak cluster at 31.84°, were retained together with the amorphous background of PPE-AA, indicating that nHA was successfully incorporated into the PPE-AA matrix without disruption of its major crystalline phase. No additional strong diffraction peaks were detected, suggesting that no detectable new crystalline impurities formed during composite fabrication (Figure 1(d)).
FTIR further confirmed the coexistence of the two components in the composite system. nHA showed a characteristic -OH absorption peak near 3573.3 cm−1 and multiple characteristic phosphate vibration peaks at approximately 1095.2, 1041, 993.7, and 962.3 cm−1 (Figure 1(e)). PPE-AA exhibited an aliphatic -CH2- stretching vibration peak at 2922.7 cm−1, together with clear absorption peaks in the carbonyl- and amide-related regions at 1730 cm-1 (C = O) and 1649.6 and 1541.1 cm−1 (amide-related peaks). In the nHA/PPE-AA composite, characteristic absorption peaks from both the inorganic and organic phases were present simultaneously, indicating the stable coexistence of nHA and PPE-AA within the composite material (Figure 1(e)). Compression testing showed that the compressive strength of the material ranged from 3 to 7 MPa.
Postoperative general condition
All animals in the three groups resumed feeding and drinking after recovery from anesthesia. As the surgical incisions healed, daily activity gradually returned to normal. The animals maintained good appetite and general condition, and body weight increased progressively. All incisions healed by primary intention, with no necrosis, infection, suppuration, material rejection, or material exposure observed. No postoperative complications, including swelling, joint effusion, deformity, dislocation, or fracture, were detected in the operated knees (Figure 2). Establishment of the rabbit femoral condyle critical-sized defect model and implantation conditions in each group. (a–c) Creation of a critical-sized defect (10 × 10 × 10 mm3) in the medial femoral condyle. (d) Experimental group: implantation of nHA/PPE-AA granules into the defect site. (e) Positive control group: implantation of calcium sulfate artificial bone granules into the defect site. (f) Blank control group: the defect was left unfilled and the wound was closed directly.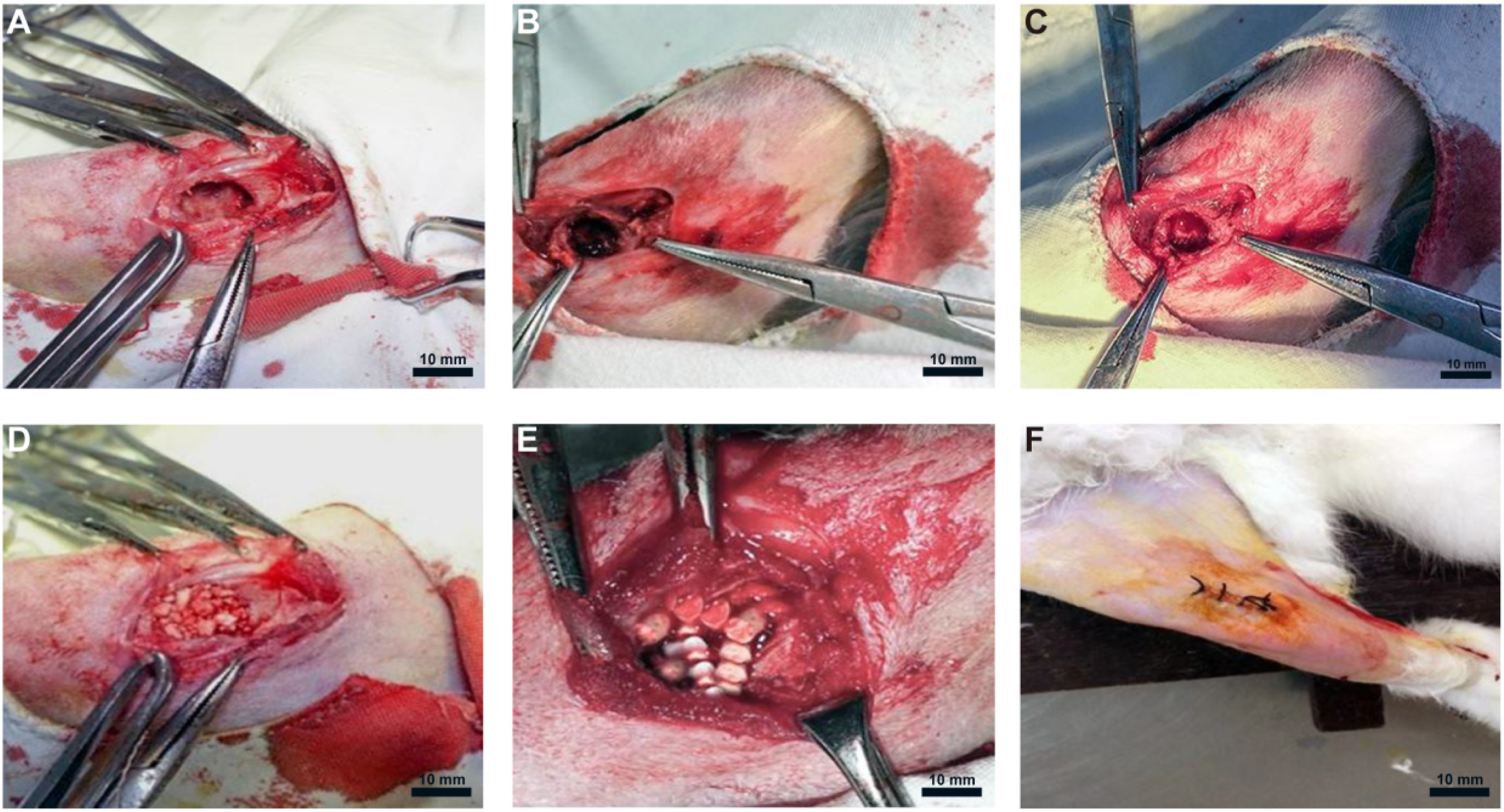
Gross repair status and changes in serum bone metabolism
Gross specimens are shown in Figure 3(a)–(f). In the experimental group, fibrous callus formation covering the implant surface was observed at 1 month postoperatively, and the bone callus progressively covered the defect surface over time (Figure 3(a)). At 6 months, the implanted region was grossly similar to normal bone tissue, the defect surface was covered by cortical bone, and the contour of the femoral condyle had been restored (Figure 3(b)). Gross postoperative findings and changes in serum bone metabolism markers. (a) Gross specimen from the experimental group at 1 month postoperatively. (b) Gross specimen from the experimental group at 6 months postoperatively. (c) Gross specimen from the positive control group at 1 month postoperatively. (d) Gross specimen from the positive control group at 6 months postoperatively. (e) Gross specimen from the blank group at 1 month postoperatively. (f) Gross specimen from the blank group at 6 months postoperatively. (g) Serum B-ALP levels in the three groups at 1, 2, 3, and 6 months postoperatively. (h) Serum N-MID levels in the three groups at 1, 2, 3, and 6 months postoperatively. Data are presented as mean ± standard deviation, *p < 0.05, **p < 0.01, ***p < 0.001.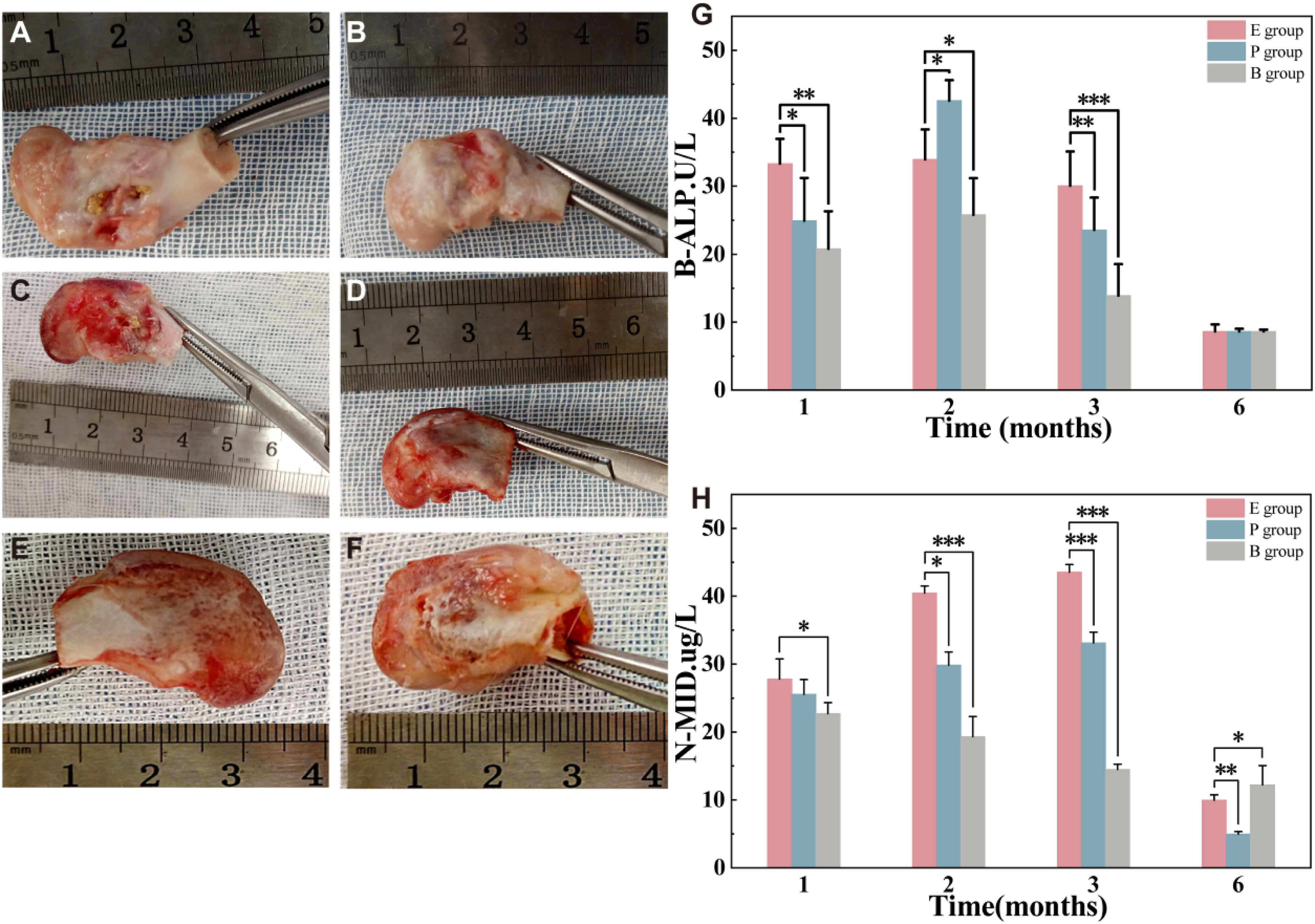
In the positive control group, the defect was enclosed by fibrous callus at 1 month, and the implanted material was prone to detachment on sectioning (Figure 3(c)). At 6 months, the defect had also undergone repair, and cortical continuity was largely re-established; however, the surface morphology remained slightly irregular (Figure 3(d)). In the blank group, fibrous tissue ingrowth was evident within the defect at 1 month (Figure 3(e)), and incomplete repair was still observed at 6 months, with the defect area being occupied predominantly by fibrous scar tissue (Figure 3(f)).
Serum bone metabolic markers were measured at each postoperative time point. In all three groups, an active osteogenic phase was observed after implantation. B-ALP increased during the early postoperative period, peaked at 2 months, and then gradually declined. At 1 month, the B-ALP level in the experimental group was significantly higher than those in the positive control and blank groups (Figure 3(g)). N-MID peaked at 3 months, and the level in the experimental group was significantly higher than those in the other two groups (Figure 3(h)), suggesting that nHA/PPE-AA promoted bone matrix formation and maturation.
X-ray observation and detection of G/N ratio
DR images showed a time-dependent increase in radiographic density within the defect area in all groups. In the experimental group, the defect area had already shown an increase in radiographic density at 1 month postoperatively (Figure 4(a)). At 6 months, the density had increased further and approached that of normal bone (Figure 4(b)). The positive control group also exhibited a gradual increase in density over time, but the overall density at 6 months remained lower than that in the experimental group (Figure 4(c) and (d)). In the blank group, the defect area remained markedly radiolucent at 1 month (Figure 4(e)). By 6 months, only mild density increase was observed at the defect margins, whereas repair of the central defect area remained limited (Figure 4(f)). Digital radiographic (DR) images of the femoral condyle defect area and grayscale ratio (G/N) after surgery. (a) DR image of the experimental group at 1 month postoperatively. (b) DR image of the experimental group at 6 months postoperatively. (c) DR image of the positive control group at 1 month postoperatively. (d) DR image of the positive control group at 6 months postoperatively. (e) DR image of the blank control group at 1 month postoperatively. (f) DR image of the blank control group at 6 months postoperatively. (g) Grayscale ratio (G/N) between the defect area and the adjacent normal bone. The G/N ratio in the positive control group was lower than that in the experimental group at 2 and 3 months postoperatively (p = 0.037 and 0.041, respectively), whereas the experimental group showed higher G/N ratios than the blank group at all time points (all p < 0.001).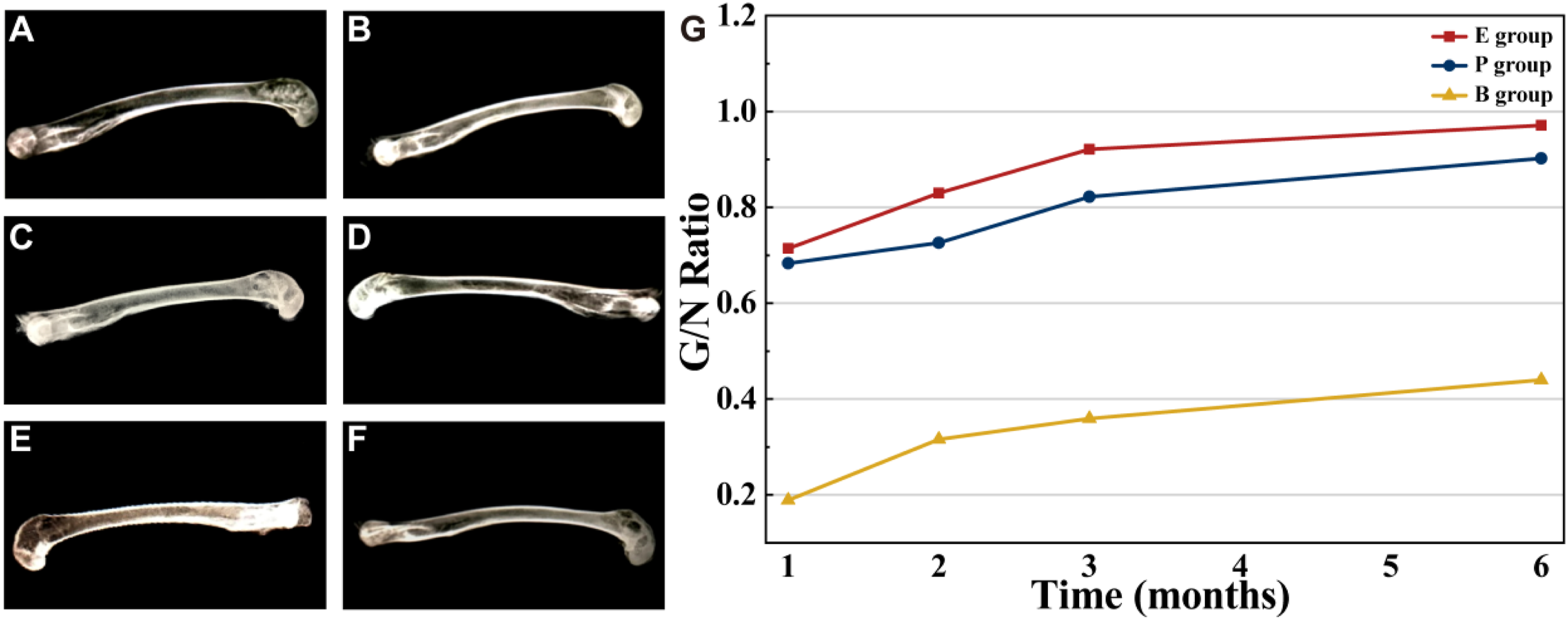
To quantify radiographic changes within the defect area, the grayscale ratio between the defect area and adjacent normal bone (G/N) was calculated. Because both nHA/PPE-AA granules and calcium sulfate are radiopaque, the G/N ratio was interpreted as a composite radiographic parameter rather than a direct stand-alone measure of newly formed bone. The G/N ratio increased progressively over time in both the experimental and positive control groups, suggesting increased mineralized tissue within the defect region when interpreted together with micro-CT, fluorochrome labeling, and histological findings. In the intergroup comparison, the G/N ratio in the positive control group was significantly lower than that in the experimental group at 2 and 3 months postoperatively (p = 0.037 and p = 0.041, respectively). In addition, the G/N ratio in the experimental group was significantly higher than that in the blank group at all time points (all p < 0.001).
Micro-CT evaluation of bone regeneration
Micro-CT demonstrated marked differences in new bone formation and defect repair among the three groups. In the experimental group, a high-density signal was visible in the defect area at 1 month, with a clear bone-material interface, although the defect area was still dominated by low-density signals and trabecular structures were not yet evident (Figure 5(a)). At this stage, the high-density signal was mainly interpreted as residual nHA/PPE-AA material because it appeared as discrete irregular granular signals. At 3 months, trabeculae had increased in number and become thicker, extending into the defect in a woven network-like pattern (Figure 5(b)). The interconnected trabecular architecture continuous with adjacent host bone supported progressive new-bone formation rather than residual material signal alone. At 6 months, cortical continuity was largely restored, and the trabecular structure became denser and more clearly defined, with progressive integration of bone and material (Figure 5(c)). Micro-CT images of the defect area in each group after surgery. (a–c) Micro-CT images of the experimental group at 1, 3, and 6 months postoperatively. (d–f) Micro-CT images of the positive control group at 1, 3, and 6 months postoperatively. (g–i) Micro-CT images of the blank control group at 1, 3, and 6 months postoperatively.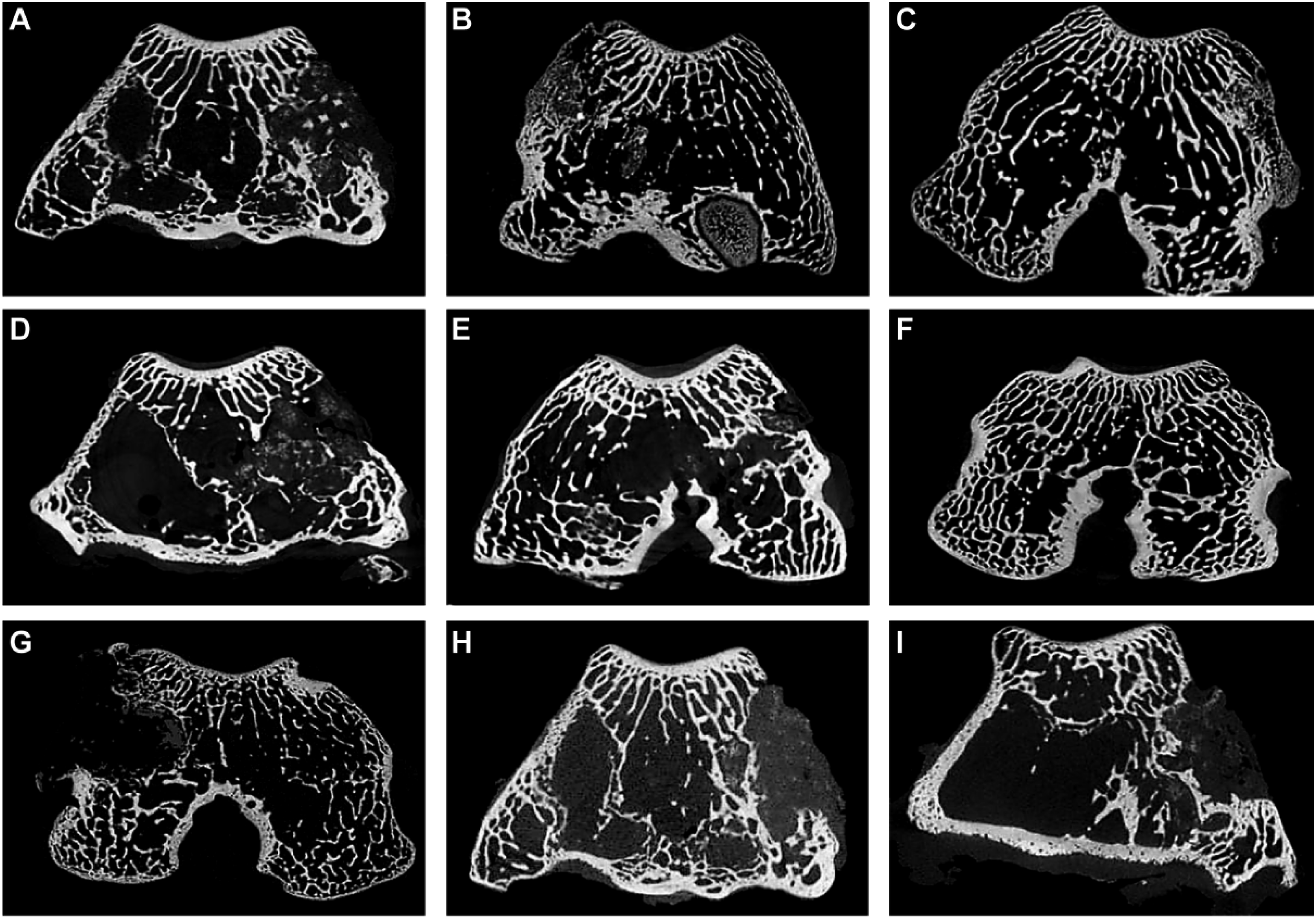
In the positive control group, high-density signals corresponding to residual calcium sulfate granules were observed in the defect area at 1 month, and trabecular structures were not obvious (Figure 5(d)). At 3 months, trabeculae extended toward the center of the defect, while the high-density signal had markedly decreased, consistent with calcium sulfate resorption and progressive tissue/bone replacement within the defect region (Figure 5(e)). At 6 months, cortical continuity was restored, and the trabecular structure became relatively clear (Figure 5(f)).
In the blank group, only marginal changes were observed at 1 month (Figure 5(g)). At 3 months, sclerosis gradually developed at the defect margins, whereas the defect area remained predominantly occupied by soft tissue (Figure 5(h)). At 6 months, the defect remained incompletely healed, cortical continuity was not restored, and low-density soft tissue-like regions were still visible within the defect (Figure 5(i)).
Fluorochrome labeling and dynamic mineralization
Sequential fluorochrome labeling showed distinct double labeling with red and green fluorescent bands in both the experimental and positive control groups. These bands gradually extended from the defect margins toward the center and became increasingly continuous over time. In contrast, fluorescence signals in the blank group were weak and failed to form continuous bands (Figure 6). Fluorescence labeling results and quantitative parameters of new bone formation. (a–d) Fluorescence images of the defect area in the experimental group at 1, 2, 3, and 6 months postoperatively. (e–h) Fluorescence images of the defect area in the positive control group at 1, 2, 3, and 6 months postoperatively. (i–l) Fluorescence images of the defect area in the blank control group at 1, 2, 3, and 6 months postoperatively. (m) Mean interlabel width of double fluorescence labeling in the bone defect area in the experimental and positive control groups (IL.WI, μm). (n) Mineral apposition rate in the bone defect area in the experimental and positive control groups (MAR, μm/d). (o) Mean osteoid seam width in the bone defect area in the experimental and positive control groups (MOSW, μm). (p) Mineralization lag time in the bone defect area in the experimental and positive control groups (MLT, d). Data are presented as mean ± standard deviation. *p < 0.05, **p < 0.01, ***p < 0.001.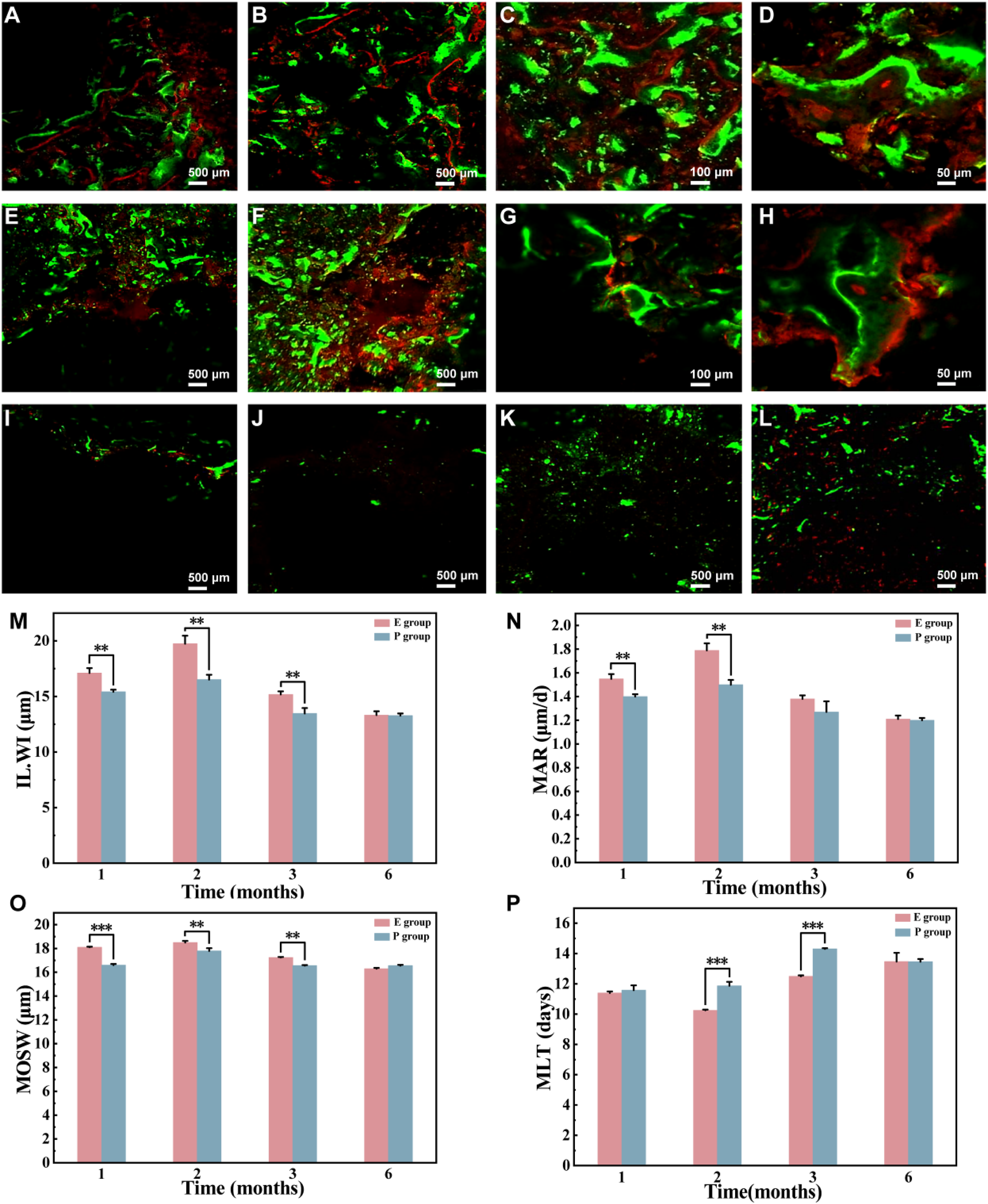
In the experimental group, abundant red and green fluorescent bands were observed at 1 month along the defect margins and the bone-material interface, with signal intensity gradually decreasing toward the center of the defect (Figure 6(a)). At 2 months, the number of fluorescent bands increased, and the bands became thicker and broader, extending further toward the center of the defect (Figure 6(b)). At 3 months, the bands exhibited a woven distribution, and fluorescence signals were also visible in the center of the defect. At higher magnification, trabecular structures with osteoblast attachment could be observed (Figure 6(c)). At 6 months, fluorescent labeling was distributed more uniformly throughout the defect area, and although the bands were relatively fewer, the structure was clearer (Figure 6(d)).
In the positive control group, fluorescent bands also gradually increased from 1 to 3 months and extended toward the defect center; however, their overall continuity and uniformity were inferior to those in the experimental group, with varying degrees of interruption still present (Figure 6(e)–(g)). At 6 months, extensive fluorescent bands and concentric ring-like structures were observed within the defect area (Figure 6(h)). In the blank group, only a small number of scattered fluorescence signals were observed at 1 month (Figure 6(i)). At 2, 3, and 6 months, the field was dominated by a dark background with scattered punctate red and green fluorescence, without obvious continuous bands (Figure 6(j)–(l)).
Dynamic histomorphometric analysis showed that IL.WI, MAR, and MOSW were all at relatively high levels in both the experimental and positive control groups during the first 1–2 months after surgery, and these values were significantly higher in the experimental group than in the positive control group, indicating more active bone formation and mineral apposition during the early and middle stages of repair in the experimental group (Figure 6(m)–(o)). MLT was shorter in the experimental group than in the positive control group, and the differences reached statistical significance at 2 and 3 months postoperatively (Figure 6(p)). After 3 months, these parameters generally declined or stabilized. By 6 months, no obvious differences in IL.WI, MAR, MOSW, or MLT were observed between the two groups, suggesting that osteogenic activity had gradually entered a plateau phase during late-stage repair.
Histological results
Experimental group: At 1 month postoperatively, osteoid tissue and/or trabecula-like structures were already observed interwoven with the surrounding tissue in the defect area (Figure 7(a)). Masson’s trichrome staining showed predominantly blue-stained collagenous matrix, with focal areas of red-stained bone matrix (Figure 8(a)). At 3 months, trabeculae were increased in number and became more continuous (Figure 7(b)). Correspondingly, Masson’s staining showed a marked increase in red-stained bone matrix with greater continuity, whereas the proportion of blue-stained matrix decreased (Figure 8(b)). At 6 months, the bone tissue became denser and showed a remodeling trend (Figure 7(c)), and Masson’s staining was dominated by extensive red-stained bone matrix (Figure 8(c)). H&E staining of the femoral condyle defect area. (a–c) H&E staining results of the experimental group at 1, 3, and 6 months postoperatively. (d–f) H&E staining results of the positive control group at 1, 3, and 6 months postoperatively. (g–i) H&E staining results of the blank control group at 1, 3, and 6 months postoperatively. Scale bar = 100 μm. Masson’s trichrome staining of the femoral condyle defect area. (a–c) Staining results of the experimental group at 1, 3, and 6 months postoperatively. (d–f) Staining results of the positive control group at 1, 3, and 6 months postoperatively. (g–i) Staining results of the blank control group at 1, 3, and 6 months postoperatively. Scale bar = 100 μm.

Positive control group: At 1 month, scattered irregular osteoid tissue and/or fine trabeculae were observed in the defect area (Figure 7(d)), and Masson’s staining showed a relatively high proportion of blue-stained matrix with only focal red-stained areas (Figure 8(d)). At 3 months, trabeculae increased, but a considerable amount of stromal/fibrous tissue was still interspersed (Figure 7(e)). Masson’s staining showed mixed red and blue areas, with increased red-stained bone matrix but insufficient continuity (Figure 8(e)). At 6 months, the bone tissue became more mature and tended to be continuous (Figure 7(f)), and the extent of red staining further increased (Figure 8(f)).
Blank group: At 1 month, the defect area was dominated by fibrous/granulation-like tissue, with limited mineralized bone structure (Figure 7(g)). Masson’s staining showed predominantly blue-stained loose matrix (Figure 8(g)). At 3 and 6 months, the defect area still consisted mainly of fibrous connective tissue, without formation of continuous trabecular structures (Figure 7(h) and (i)). Red-stained bone matrix remained sparse and lacked broad continuous distribution on Masson’s staining (Figure 8(h) and (i)).
SEM results
Experimental group: At 1 month, abundant tissue-/matrix-like deposits were observed on the material surface and in the interfacial region, extending inward along the pore walls, with interfacial gaps still visible (Figure 9(a)). At 2 months, the coverage of these deposits increased, more continuous deposition was observed within the pores, and the interfacial gaps were reduced (Figure 9(b)). At 3 months, interfacial deposits became more abundant and denser, the interface boundary became less distinct, and focal fragmentation-like changes were observed in the pore walls of the material (Figure 9(c)). At 6 months, extensive tissue-/matrix-like filling was observed within the pores, and the bone tissue was more tightly apposed to the material surface, forming a continuous interfacial transition (Figure 9(d)). SEM findings at the bone-material interface. (a–d). SEM images of the experimental group at 1, 2, 3, and 6 months postoperatively. (e–h). SEM images of the positive control group at 1, 2, 3, and 6 months postoperatively. Scale bars: a and d = 500 μm; b, c, and g = 50 μm; e, f, and h = 100 μm.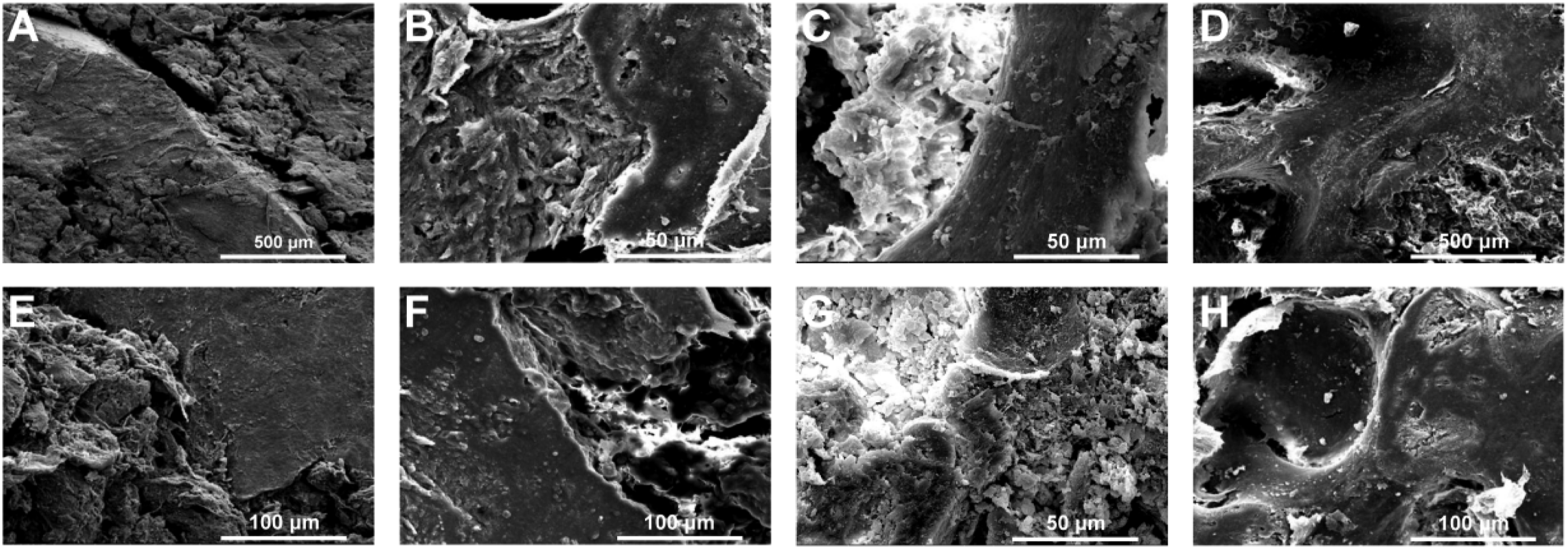
Positive control group: At 1 month, tissue-/matrix-like deposits were observed on the material surface and within the pores, and interfacial gaps were present (Figure 9(e)). At 2 months, the material surface appeared more fragmented than before, and the integrity of the pore structure was reduced, although the area covered by deposits had increased (Figure 9(f)). At 3 months, the interface boundary became less distinct, and deposition increased with a trend toward relative continuity (Figure 9(g)). At 6 months, the interfacial surface morphology became denser and smoother (Figure 9(h)).
BMP-2 mRNA expression (RT-qPCR)
RT-qPCR showed that the relative expression of BMP-2 mRNA in both the experimental and positive control groups was significantly higher than that in the blank group at 1–3 months postoperatively (Figure 10). In the experimental group, BMP-2 expression increased over time and reached its highest level at 3 months, at which point it was significantly higher than that in the positive control group (Figure 10). By 6 months, BMP-2 expression had declined to a low level in all three groups, with no obvious intergroup differences (Figure 10). Relative BMP-2 mRNA expression after surgery, as determined by RT-qPCR (2^-ΔΔCT). Relative BMP-2 expression in both the experimental group and the positive control group gradually increased during the first 2 months after surgery. In the experimental group, expression peaked at 3 months and then gradually declined, reaching a lower and more stable level by 6 months postoperatively. Data are presented as mean ± standard deviation. *p < 0.05, **p < 0.01, ***p < 0.001.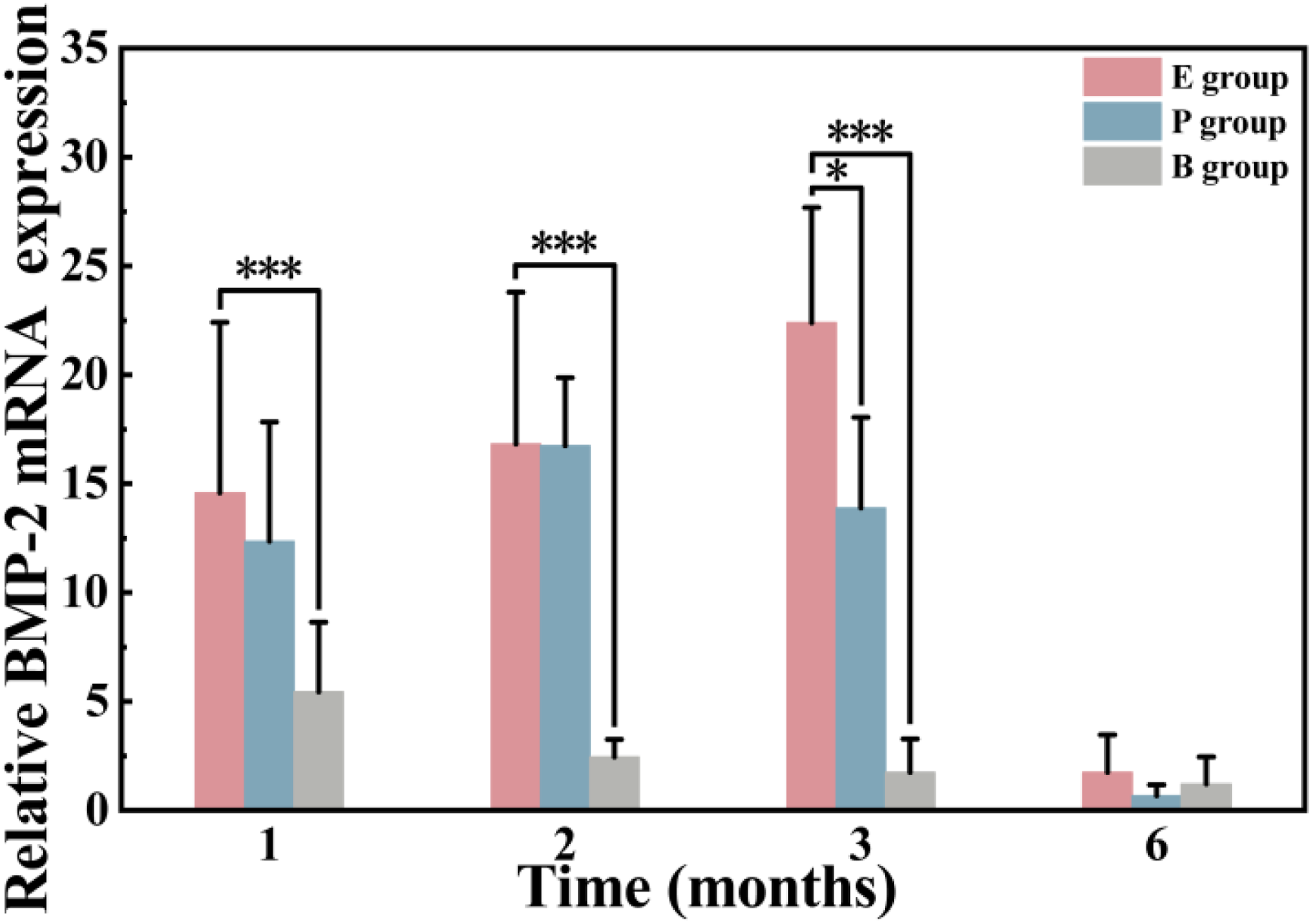
Safety results
At 6 months postoperatively, H&E staining showed intact tissue architecture in the liver, lung, kidney, brain, and heart of the experimental group, without obvious necrosis, hemorrhage, or marked inflammatory cell infiltration (Figure 11(a)–(e)). In the femoral condyle implantation area, trabecular remodeling was observed; partial collapse of the material pore structure was accompanied by tissue ingrowth, and the trabeculae were in close contact with the material (Figure 11(f)). Masson’s staining showed increased collagen deposition and improved tissue maturation (Figure 11(g)). In the intramuscular implantation area, local calcium salt deposition and osteoid-/trabecula-like tissue formation were observed, without obvious myocyte lysis or necrosis (Figure 11(h)). Safety evaluation after material implantation. (a–e) H&E-stained sections of the liver, lung, kidney, brain, and heart from the experimental group at 6 months postoperatively. (f) H&E staining of the femoral condyle implantation site in the experimental group at 6 months postoperatively. (g) Masson’s trichrome staining of the femoral condyle implantation site in the experimental group at 6 months postoperatively. (h) H&E staining of the intramuscular implantation site in the experimental group at 6 months postoperatively. (i–k) Time-course changes in peripheral inflammatory markers in the experimental, positive control, and blank groups at 1 day, 3 days, 7 days, 2 weeks, 1 month, 3 months, and 6 months postoperatively: erythrocyte sedimentation rate (ESR), white blood cell count (WBC), and C-reactive protein (CRP). All three markers peaked at postoperative day 3, and no statistically significant differences were observed between the experimental group and the blank group (WBC: p = 0.134; ESR: p = 0.473; CRP: p = 0.162). Scale bar = 100 μm.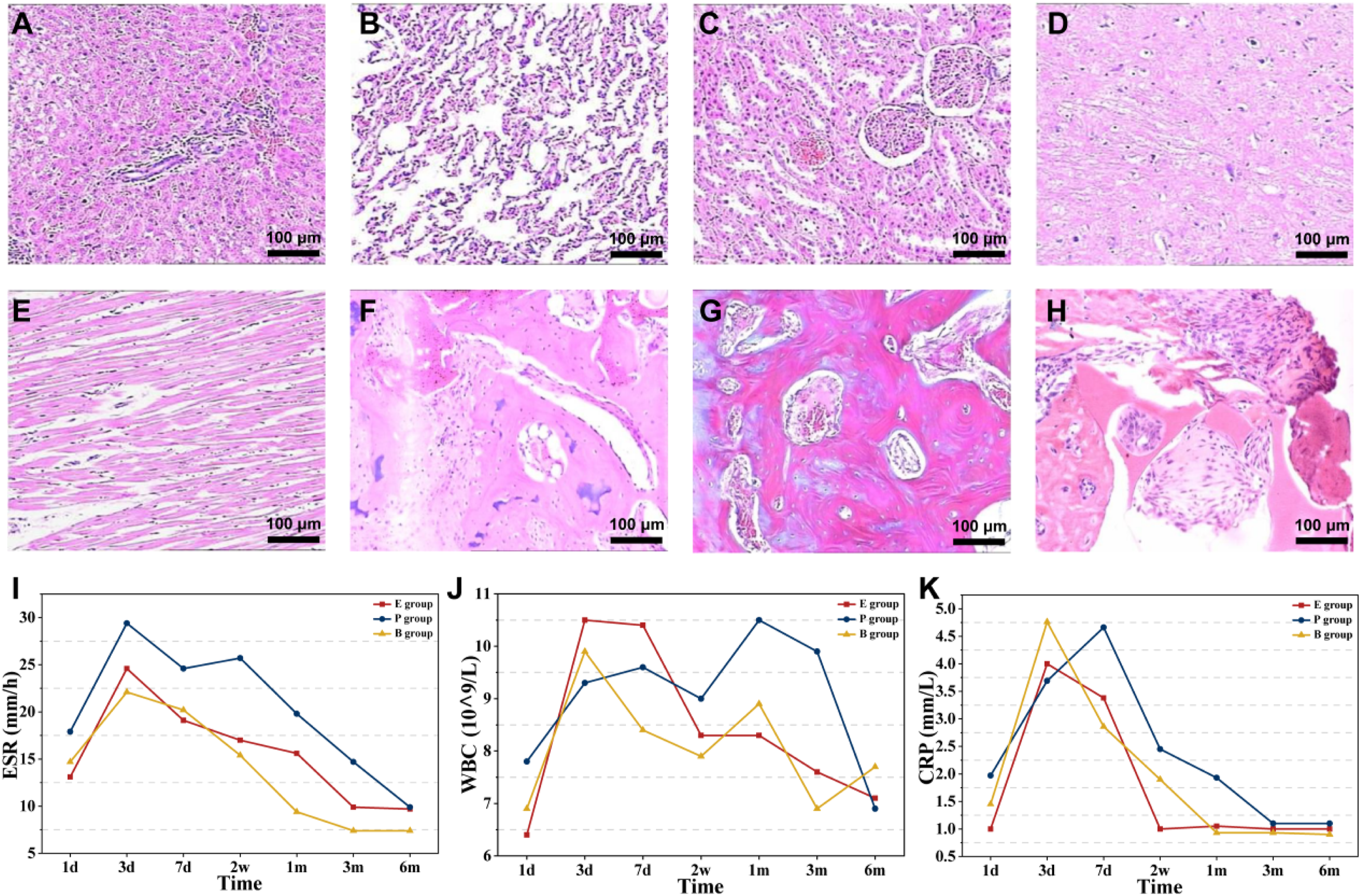
With respect to inflammatory blood markers, ESR, WBC, and CRP showed transient elevations in all three groups during the early postoperative period, peaked at postoperative day 3, and then gradually declined (Figure 11(i)–(k)). The peak ESR, WBC, and CRP values in the experimental group did not differ significantly from those in the blank group (p = 0.473, 0.134, and 0.162, respectively) (Figure 11(i)–(k)).
Discussion
This study established a rabbit femoral condyle critical-sized defect model to systematically evaluate the osteogenic repair performance of nHA/PPE-AA composite material from multiple perspectives, including macro-imaging, microstructure, dynamic mineralization, molecular expression, and safety. The results demonstrated that nHA/PPE-AA effectively promoted new bone formation and trabecular reconstruction in the defect area, with superior performance compared to calcium sulfate (positive control) in the early-to-mid-stage repair process. Importantly, no significant systemic or local adverse reactions were observed, indicating good bioactivity and in vivo safety of the material.
Critical-sized bone defects typically do not heal spontaneously, making them ideal models for assessing the regenerative potential of bone substitutes. 33 In the blank control group, no continuous cortical structure was formed after 6 months, with the defect area primarily filled with fibrous tissue, validating the efficacy of the model. In contrast, the experimental group showed bone callus formation as early as 1 month postoperatively, with a significant increase in trabeculae and network-like reconstruction by 3 months. At 6 months, cortical continuity was largely restored, and trabecular structure became more compact, closely resembling normal bone. Although the positive control group also showed signs of bone repair, the osteogenic rate and mineralization degree were generally lower than those observed in the experimental group during the early and middle stages. The differences in the G/N ratio from DR imaging, micro-CT, and histological analysis further supported this finding, suggesting that nHA/PPE-AA exhibited more favorable osteogenic performance during bone repair.
The difference in particle-size distribution between the nHA/PPE-AA granules (300–5000 μm) and calcium sulfate control granules (2–4 mm) should be considered when interpreting the group comparisons. This discrepancy may affect packing density, surface-area-to-volume ratio, material–tissue contact, and tissue ingrowth. Therefore, calcium sulfate served as a clinically relevant reference material rather than a particle-size-matched control, and future studies using size-matched controls are warranted.
An inherent limitation of evaluating nHA-containing bone graft substitutes by radiography or micro-CT is that nHA itself is radiopaque; therefore, early high-density signals may partially reflect residual material rather than newly mineralized bone. To reduce this bias, the G/N ratio was interpreted longitudinally rather than as a single absolute value. Micro-CT morphology, H&E and Masson’s trichrome staining, and fluorochrome labeling were used as complementary evidence to distinguish residual material from regenerated bone. Future studies using material-specific labeling or calibrated micro-CT analysis may allow more precise separation of material and biological mineralization signals.
Material structure and composition are critical factors influencing bone regeneration. The nHA/PPE-AA granules possess a connected porous structure (20–500 μm), which is optimal for facilitating the migration of blood vessels and osteoblast-related cells into the material, thereby promoting tissue ingrowth.34,35 The approximately 30% nHA content provides a mineralized core and maintains structural stability. The material’s compressive strength ranges from 3 to 7 MPa, comparable to that of trabecular bone (approximately 4–7 MPa), indicating that it possesses adequate mechanical support in load-bearing environments.36–38 Compared to single-phase inorganic materials, the PPE-AA organic matrix imparts toughness and interfacial stability to the composite, making it structurally and compositionally more akin to the “organic-inorganic” biphasic nature of native bone, which facilitates the formation of a more stable bone-material integration interface. 35
Sequential fluorochrome double labeling further revealed the material’s impact on the mineralization process. In the experimental group, IL.WI, MAR, and MOSW were higher than those in the positive control group during the early-to-middle stages (1–2 months), and MLT was shorter, suggesting more active mineralization and higher mineralization efficiency in the early and middle phases. After 3 months, these parameters generally decreased and stabilized, indicating that bone formation gradually entered a more stable remodeling phase. This dynamic trend aligns with the expression patterns of BMP-2 mRNA: RT-qPCR showed that BMP-2 levels in the experimental group were high between 1 and 3 months, peaking at 3 months, and were significantly higher than those in the positive control group at 3 months. By 6 months, BMP-2 expression decreased to low levels in all groups. BMP-2, a classic osteoinductive factor,39,40 showed a peak expression pattern coinciding with the active osteogenesis phase, suggesting that nHA/PPE-AA may promote bone regeneration by enhancing local osteogenic signaling. However, only BMP-2 mRNA was evaluated in this study; therefore, the osteogenic molecular mechanism should be interpreted cautiously, and additional markers such as Runx2, OCN, COL-I, and OSX should be assessed in future studies.
Interface observations also support these conclusions. SEM results showed that tissue/matrix-like coverage at the interface in the experimental group increased over time, and interfacial gaps gradually reduced. By 6 months, the interface exhibited more intimate attachment and continuous transition. In contrast, in the positive control group, the material surface showed more fragmentation at 2–3 months. Calcium sulfate degrades relatively quickly and provides short-term filling and support; however, its ability to maintain structural integrity is limited.41,42 In comparison, nHA/PPE-AA exhibited progressive structural changes, with localized collapse of the pore walls accompanied by tissue ingrowth, suggesting that material remodeling and structural changes may be coordinated with new bone formation. However, these observations provide only indirect morphological evidence and do not constitute quantitative degradation data. This remodeling pattern may help maintain mechanical stability in the defect area and reduce the risk of early collapse. Serum and histological safety results further support the biocompatibility of the material in vivo. Elevated B-ALP and N-MID in the early-to-middle stages suggested active bone formation. ESR, WBC, and CRP showed transient increases in the early postoperative period, which gradually subsided, with no significant difference between the experimental and blank groups at peak levels, indicating that the material did not induce excessive inflammation. At 6 months, histological examination of the major organs revealed no significant pathological abnormalities. No obvious necrosis or inflammatory reactions were observed in the intramuscular implantation area, although local calcium salt deposition and osteoid-like structure formation were seen, suggesting that the material may have an inductive effect on mineralization even in non-bone environments. Previous studies have shown that sustained release of Ca/P ions and regulation of the local microenvironment can promote mineral deposition and influence bone regeneration. 43 Therefore, this phenomenon may be related to the Ca/P ion release from nHA and the degradation products of PPE-AA, which work synergistically to modulate the microenvironment. This mechanism warrants further investigation in future studies.
In summary, nHA, as the inorganic phase, provides a mineralization core and a source of Ca/P ions; the degradation products of PPE-AA, containing phosphorus, may influence the local microenvironment. The amino acid segments contribute to increased hydrophilicity and cell adhesion. The interconnected porous structure facilitates cell migration and vascularization.34,35 These structural and compositional factors may work synergistically through the “spatial scaffold effect + biochemical signal regulation” to enhance osteogenic-related molecular expression and drive the bone regeneration process. The multi-dimensional results from imaging, histology, dynamic mineralization, and molecular analysis provide relatively comprehensive evidence for the bone repair capacity of this composite material.
However, this study has some limitations. First, the sample size was limited, and the follow-up period did not exceed 6 months. Second, only BMP-2 was assessed as a molecular indicator of osteogenic activity, whereas other osteogenesis-related markers, such as Runx2, OCN, COL-I, and OSX, were not included. Third, changes in the material’s mechanical properties over time in vivo were not systematically evaluated. Fourth, quantitative degradation kinetics of nHA/PPE-AA were not directly measured, and the proposed coupling between material degradation/remodeling and bone regeneration remains a qualitative inference based on morphological observations. Future studies should include quantitative degradation assays, broader osteogenic marker profiling, long-term follow-up, mechanical loading models, and large-animal experiments to further validate the repair efficacy and translational feasibility of nHA/PPE-AA.
Conclusion
This study successfully developed a novel nHA/PPE-AA composite porous bone-filling material, which exhibits an irregular granular morphology, interconnected porous structure, and appropriate mechanical strength, providing a structural foundation for tissue ingrowth and defect space maintenance. In the rabbit femoral condyle critical-sized defect model, implantation of nHA/PPE-AA promoted new bone formation and trabecular reconstruction, with both imaging and histological results demonstrating superior repair performance compared to the positive control material. Early-to-mid-stage dynamic fluorochrome labeling indicated more active mineral deposition and shorter mineralization lag time. RT-qPCR analysis revealed elevated BMP-2 mRNA levels between 1 and 3 months post-surgery, peaking at 3 months, providing molecular evidence supporting enhanced osteogenic signaling. Safety evaluation confirmed the material did not induce sustained systemic inflammation, and no significant pathological changes were observed in major organs or implanted tissues at 6 months, indicating excellent biocompatibility and in vivo safety. Overall, nHA/PPE-AA shows promising potential as a bone substitute material for further translational research; however, further validation in larger samples, longer follow-up studies, and large animal models is warranted.
Footnotes
Ethical considerations
All procedures involving animals in this study were reviewed and approved by the Animal Ethics Committee of West China Hospital, Sichuan University (Approval Number: 20230227016). The research was conducted strictly in accordance with institutional and national guidelines for the care and use of laboratory animals. All efforts were made to minimize animal suffering and reduce the number of animals used.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National 863 Program (Grant No. 2015AA033605) and the National Natural Science Foundation of China (Grant Nos. 31070834 and 10402025).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The results in this study are available from the corresponding author on reasonable request.
Material statement
The nanohydroxyapatite/polyphosphoester-amino acid (nHA/PPE-AA) bone-filling material used in this study was jointly developed by the Laboratory of Physics and Physical Technology, Sichuan University, and Sichuan Guona Technology Co., Ltd.