
Abstract
We investigated agency directors’ perspectives about how service goals should be prioritized for domestic violence and sexual assault service subtypes, including crisis, legal advocacy, medical advocacy, counseling, support group, and shelter services. A sample of 97 (94% response rate) North Carolina domestic violence and/or sexual assault agency directors completed a survey asking participants to rank the importance of service goals. Overall, participants considered emotional support provision to be a critical service goal priority across all service types. Social support and self-care service strategies were deemed less important. However, prioritization of other service goals varied depending on the service type. Statistically significant differences on service goal prioritization based on key agency characteristics were also examined, and agency characteristics were found to relate to differences in service goal prioritization.
Many partner and sexual violence survivors seek help from community-based domestic violence and sexual assault agencies (Hutchison & Hirschel, 1998; Ingram, 2007; Macy, Nurius, Kernic, & Holt, 2005) because survivors’ needs are often not met by health, human, and legal services (Campbell, 2006; Hazen et al., 2007; Kunins, Gilbert, Whyte-Etere, Meissner, & Zachary, 2007; McKie, 2003; Plichta, 2007; Tower, McMurray, Rowe, & Wallis, 2006). Thus, domestic violence and sexual assault agencies offer an important and unique human service. Regrettably, there is limited empirical evidence about the effectiveness of these services (Abel, 2000; Mears, 2003; Wathen & MacMillian, 2003; Whitaker, Baker & Arias, 2007). The lack of evidence-based domestic violence and sexual assault services is a worrisome knowledge gap that causes problems for practice, policy, and funding advancements (MacMillan et al., 2009; Moracco & Cole, 2009).
Evidence-Based Practices and Services for Violence Survivors
There is a growing consensus about the necessary steps for evidence-based practice development among intervention researchers (Carroll & Nuro, 2002; Fraser, Richman, Galinsky, & Day, 2009; Muser & Drake, 2005). Briefly, they include: (a) conceptualizing an intervention and designing a treatment manual, (b) conducting pilot and feasibility trials, (c) conducting randomized efficacy and then effectiveness trials, and (d) adapting the intervention for dissemination across diverse settings and communities. Even though there is widespread acceptance of this intervention research paradigm, few social and behavioral interventions could be considered a “gold standard” evidence-based practice.
Although domestic violence and sexual assault services are already well established and regularly delivered in communities throughout the United States, few of these programs have been rigorously documented or tested, though notable exceptions exist (e.g., Sullivan & Bybee, 1999). Work has been done to document recommended practices (for a comprehensive review of this literature, see Macy, Giattina, Sangster, Crosby, & Montijo, 2009), and preliminary, quasi-experimental evaluations have been conducted on domestic violence and sexual assault services (e.g., Edleson & Frick, 1997; Riger et al., 2002; Wasco et al., 2004). In light of the research paradigm described above, the state of knowledge about domestic violence and sexual assault services could be considered preliminary.
Unfortunately, for those wanting to conduct efficacy and effectiveness studies on domestic violence and sexual assault services, there are serious gaps in the work on conceptualizing domestic violence and sexual assault services (e.g., What are the theories of change that underlie these services? What are the services’ goals and delivery strategies?), as well as in the work to document these services into manuals. More specifically, there is little research about how these services should be delivered (Abel, 2000; Macy et al., 2009). Thus, the knowledge required for the first step in the development of an evidence-based practice (i.e., conceptualizing an intervention and designing treatment manual) is incomplete.
Even with literature describing how these services are best delivered, the current state of service delivery has been described as a “black box” because the inner workings of these services remain largely unknown. Furthermore, within the broad framework of domestic violence and sexual assault services, many service types are often (but not always) offered by providers. These service types, which include crisis, legal advocacy, medical advocacy, counseling, support groups, and shelter, are often delivered in different ways by different providers, including volunteers, advocates, and counselors. Furthermore, these services—both the services overall, as well as the various service types—differ across communities because of their grassroots beginnings (Koss & Harvey, 1991; Pfouts & Renz, 1981).
In summary, there is a literature describing how domestic violence and sexual assault services are best delivered, but there is little research about whether these recommended practices are used in community-based settings. To further complicate matters, there is considerable variability in how these services are delivered in practice because of differences in service types, providers, communities, as well as the grassroots nature of these services. In addition, little is known about what providers consider best practice strategies for each of the specific service types. Given that these services are grassroots and community-based and that the best practices literature has been largely developed by educators and researchers, evidence from providers about how these services should be delivered to best help survivors is critically important.
The Current Study
We investigated domestic violence and sexual assault agency directors’ opinions of how service delivery goals should be prioritized to ensure that survivors’ needs are met. Given their leadership positions in their agencies, directors are important informants concerning the service delivery strategies that work well for the survivors in their communities. However, there is little research about service delivery practices from directors’ points of view. We investigated directors’ opinions of how service delivery goals should be prioritized for the six service types that are often discussed in the domestic violence and sexual assault services literature (Macy et al., 2009). These six service types are as follows: (a) crisis services, (b) legal advocacy, (c) medical advocacy, (d) support group, (e) individual counseling, and (f) shelter. We wanted to better understand the extent to which service delivery goal priorities were similar and/or distinct across these six service types.
We also investigated the extent to which directors’ opinions about service delivery goals differed based on key agency characteristics, specifically: (a) the rural/suburban/urban location of their agencies and (b) the agency service focus (i.e., domestic violence, sexual assault, or both). Agencies may vary in their service delivery practices because of their service foci, their community-based nature, and their grassroots beginnings. Consequently, we posed this research question: To the extent that there are significant differences in how directors prioritize service delivery goals, does this variability relate to these differences in agency characteristics?
Agency characteristics
On the basis of the existing literature, we hypothesized that agency characteristics would relate to differences in service goal priorities. Research shows that survivors have different needs based on the types of communities in which they live. Vinton and colleagues (Vinton et al., 2007) identified 19 factors distinguishing rural survivors from their nonrural counterparts, such as geographic and social isolation, higher gun ownership, and lack of trained providers. Thus, providers from diverse agency locations (i.e., rural, suburban, urban) may prioritize service goals differently based on the needs of survivors in their locales.
We also posited that the focus of agency services (i.e., domestic violence only, sexual assault only, combined domestic violence and sexual assault) may relate to differences in directors’ perceptions for service goal priorities. Domestic violence and sexual assault services are often conceived of and described as distinct sets of services that are tailored to meet the needs of survivors who experienced either domestic violence or sexual assault. Moreover, questions are found in the literature regarding how combined agencies deliver services to survivors compared with single-focused agencies (Byington, Martin, DiNitto, & Maxwell, 1991; O’Sullivan & Carlton, 2001). Nevertheless, most sexual assault and domestic violence agencies in the United States and in North Carolina (where the study was conducted) provide both of these services and thus can be considered combined agencies (Bergen, 1996; Edmond, 2005). Consequently, we investigated differences in service goal priorities based on whether an agency delivered sexual assault services only, domestic violence services only, or delivered both of these services.
Method
Participants and Procedures
We developed our sampling frame by relying on the websites of the following organizations: (a) the North Carolina Council for Women/Domestic Violence Commission (NCCWDVC), (b) the North Carolina Coalition Against Sexual Assault (NCCASA), and (c) the North Carolina Coalition Against Domestic Violence (NCCADV). Using these sources, we created a database of all North Carolina domestic violence and sexual assault agencies and their executive directors. We used the list of directors (n = 103) as our sampling frame.
We conducted the survey over a 10-week period. Before survey administration, the study protocols were approved by the Institutional Review Board at our university. A paper version and an electronic version of the survey were made available. Typically, the agency executive director was the best person to respond to the survey. In some cases, however, associate directors or other staff members are in charge of overseeing agency services. Therefore, the cover letter accompanying the survey invited the directors to either complete the survey themselves or designate a staff member with the most knowledge of the agency’s services. To encourage survey participation, potential participants received multiple survey invitations via mail, e-mail, and telephone. Instructions for opting out of the study were also provided. There was a 94% (n = 97) response rate to the survey.
Instrument
Our research team developed the survey questions based on an extensive review of the literature and qualitative findings from in-depth interviews with North Carolina domestic violence and sexual assault agency directors about their services delivery practices (Macy et al., 2009; Macy, Giattina, Montijo, & Ermentrout, 2010; Macy, Giattina, Parish, & Crosby, 2010). Directors who participated in the interviews were also invited to participate in the survey, though a year passed between the interviews and the survey administration. After developing a draft survey instrument, two staff members at NCCADV, NCCASA, and the NCCWDVC, along with four persons who had previously delivered domestic violence and sexual assault services, piloted the survey (n = 10). No one who piloted the survey was a member of the survey sampling frame though all the pilot testers had experience delivering domestic violence and/or sexual assault services. The survey was finalized using pilot feedback.
Measures
Participants were asked their opinions about specific service delivery goals (e.g., emotional support, safety planning, help with social support, and community referrals) for six subtypes of domestic violence and sexual assault services: (a) crisis services, (b) legal advocacy, (c) medical advocacy, (d) support group, (e) individual counseling, and (f) shelter. For each of the service subtypes, participants were asked to rank the importance of specific service goals. Participants were asked to give the ranking of “1” to the item they felt was the most important for a survivor to receive from that service, “2” for the second most important, “3” for the third most important, and so on.
For each of the six service subtypes (crisis services, legal advocacy, medical advocacy, etc.), the survey included two-item types. First, the survey included goals that are common to all six service subtypes (e.g., emotional support, safety planning). Examples of these survey ranking items are as follows: (a) “Client received emotional support, such as kindness, caring, and empathy” for the emotional support item and (b) “Client received help with planning for safety, such as vary routine, plan for what to do if perpetrator becomes violent again, memorize emergency numbers” for the safety planning item. Such ranking items were listed with all six service subtypes.
Second, the survey included goals that are unique to service subtypes. For example, the service goal of legal accompaniment is only relevant to legal advocacy. Thus, to capture information about unique service goals, each set of survey ranking items for the six service subtypes (crisis services, legal advocacy, counseling, etc.) listed goals specific to that service. Examples of these survey ranking items are as follows: (a) “Client was accompanied to court, trials, and legal meetings” for the legal accompaniment item listed with legal advocacy; (b) “Client received information about medical options, as appropriate to advocacy role and not in conflict with advice of medical professionals” for the medical information ranking item listed with medical advocacy; and (c) “Client received a safe place to live free from violence” for the safe shelter ranking item listed with shelter services. Furthermore, instructions asked participants to answer questions only if their agencies provided that specific service. Some agencies, such as those that provide only sexual assault services, do not offer shelter services. Thus, the number of items ranked by each participant varied depending on the number of services their agency provided. The survey also included questions about agency and participant characteristics.
Analysis
First, frequencies and percentages were conducted on participant and agency characteristics. Then, to address the first aim, descriptive analyses were used to identify directors’ opinions about service goal priorities with medians and ranges. These finding are presented in Table 1. Table 2 shows the rankings of each service goal priority for the various service subtypes. Each service goal priority is ranked first (highest priority) to last (lowest priority) based on the overall medians in Table 1. Table 2 also shows the similarities and differences in service delivery priorities across the service subtypes for the overall sample. The second aim was to investigate to what extent service goal priorities differed based on specific agency characteristics. We used the Kruskal–Wallis test for these analyses because it is a nonparametric method for assessing the equality of population medians among groups. That is, the Kruskal–Wallis test uses the sum of the ranks for each group to calculate the test statistic. We tested for significant differences in rankings based on two agency characteristic groupings. Participants were grouped by (a) agency location: rural, urban/suburban, and both rural and urban/suburban and (b) agency service focus: domestic violence only, sexual assault only, and both domestic violence and sexual assault. Statistical analyses were then conducted in SPSS 18.0. All statistically significant findings are presented in Tables 3 and 4.
Rank-Order Descriptive Statistics for Service Goals Across Service Types (1 = Most Important; 10 = Least Important; n = 87 to 64 a )
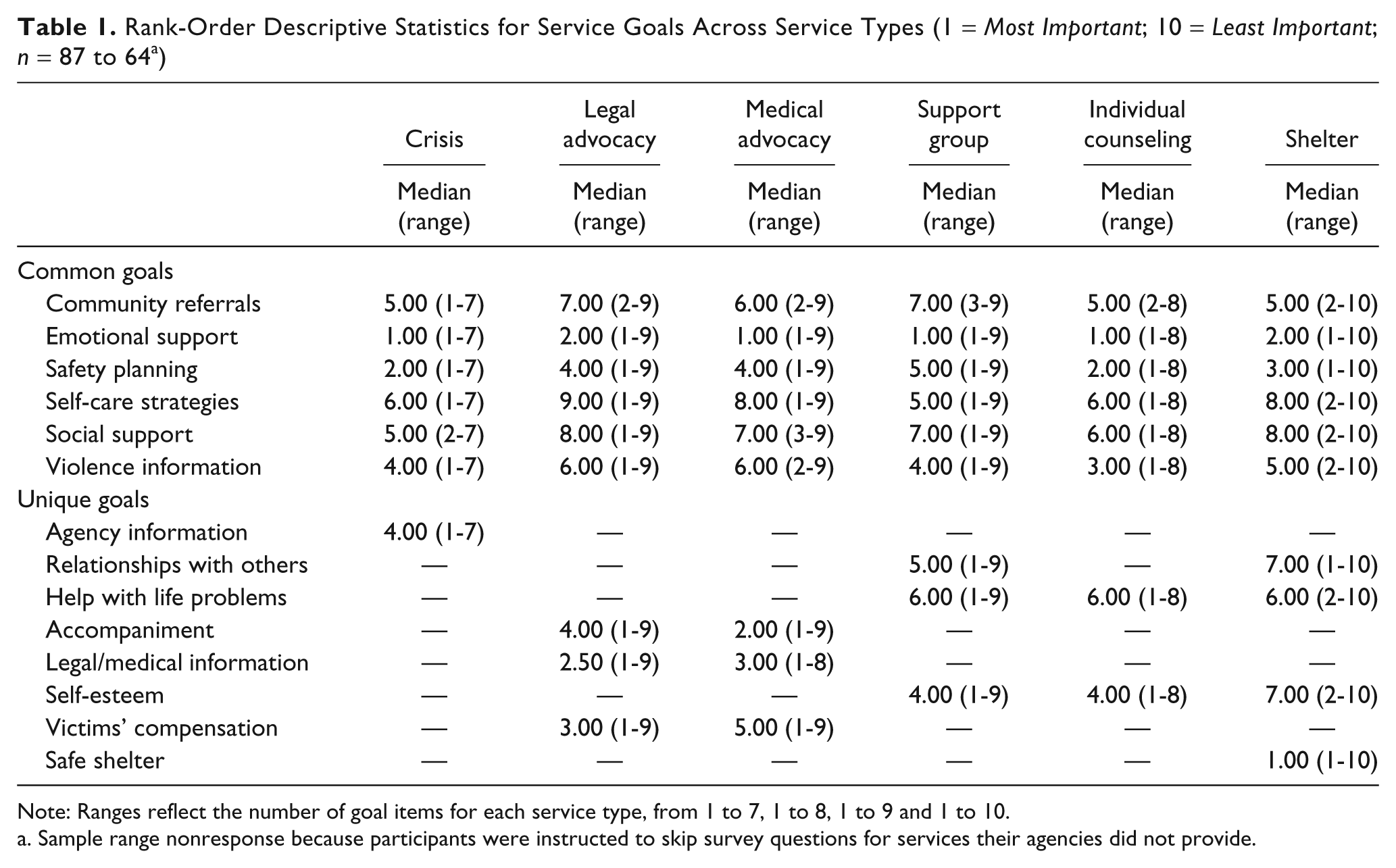
Note: Ranges reflect the number of goal items for each service type, from 1 to 7, 1 to 8, 1 to 9 and 1 to 10.
Sample range nonresponse because participants were instructed to skip survey questions for services their agencies did not provide.
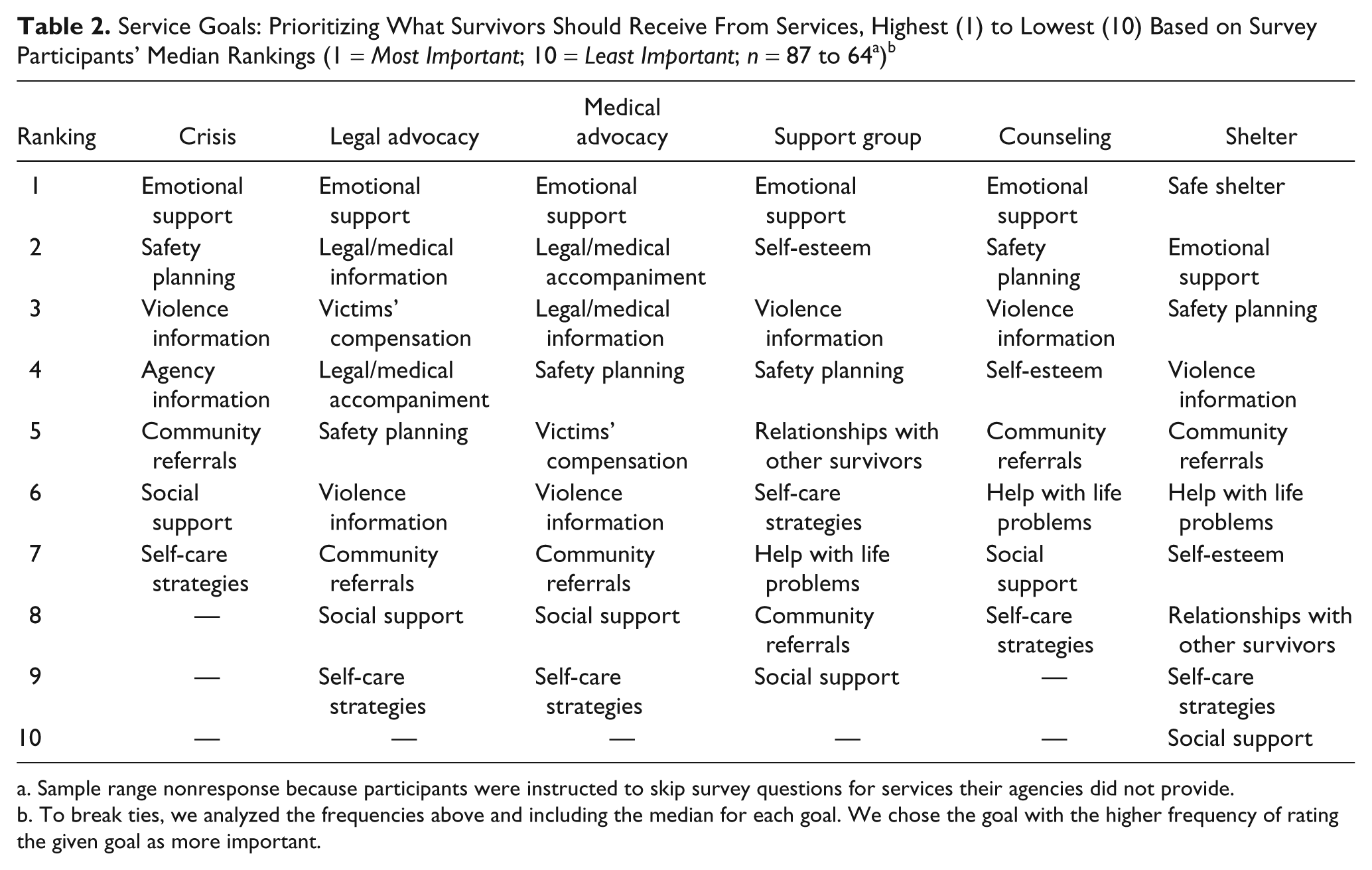
Sample range nonresponse because participants were instructed to skip survey questions for services their agencies did not provide.
To break ties, we analyzed the frequencies above and including the median for each goal. We chose the goal with the higher frequency of rating the given goal as more important.
Mean Ranks and Kruskal–Wallis Test for Crisis Service, Medical Advocacy, Support Group, and Counseling Goals by Agency Location
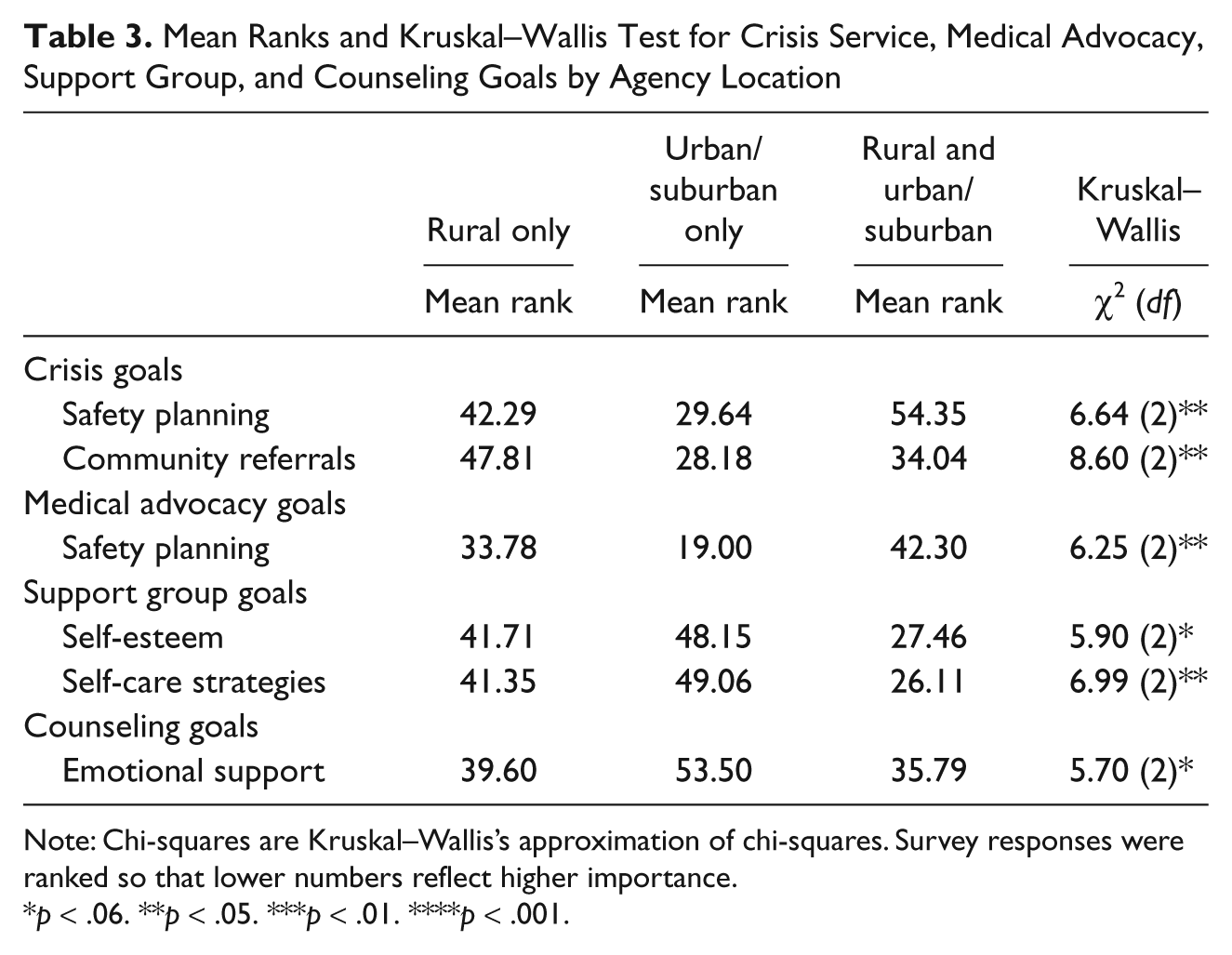
Note: Chi-squares are Kruskal–Wallis’s approximation of chi-squares. Survey responses were ranked so that lower numbers reflect higher importance.
p < .06. **p < .05. ***p < .01. ****p < .001.
Mean Ranks and Kruskal–Wallis Test for Crisis Service, Medical Advocacy, Support Group, and Counseling Goals by Agency Service Focus
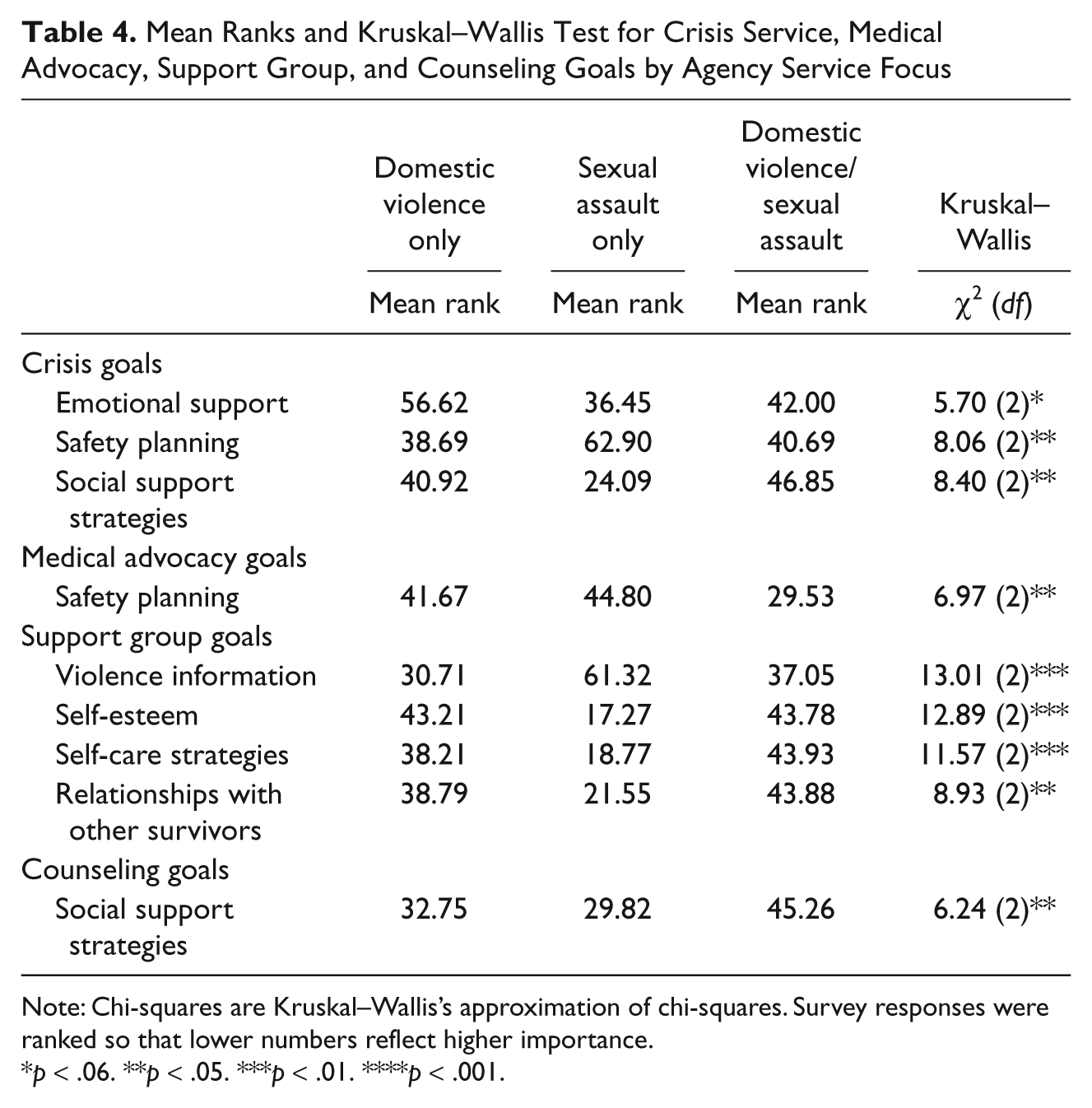
Note: Chi-squares are Kruskal–Wallis’s approximation of chi-squares. Survey responses were ranked so that lower numbers reflect higher importance.
p < .06. **p < .05. ***p < .01. ****p < .001.
Results and Discussion
Participant and Agency Characteristics
Most participants described themselves as a “director” (n = 80; 82.47%), with the remaining participants describing themselves as an “advocate” or “other.” Over half of the sample reported being employed in their current position for no more than 5 years (n = 52; 54.7%). However, 22 participants (23.2%) reported 6 to 10 years in their current position; 5 participants (5.3%) reported 11 to 15 years; and 16 participants (16.8%) reported 16 or more years. Most participants had completed either graduate degrees (n = 40; 41.2%) or 4-year college degrees (n = 32; 32.9%). Fourteen (14.4%) had completed community college or associate degrees, and 11 (11.3%) had completed high school and/or some college. On average, agencies had eight full-time employees and five part-time employees. However, staff numbers ranged from 1 to 100 full-time employees and from 0 to 20 part-time employees. Forty-three (44.3%) agencies had five or fewer staff members; 38 (39.2%) agencies had 6 to 10 staff members; 16 (16.5%) agencies had 11 or more staff members. Most participants came from combined agencies that provided both domestic violence and sexual assault services (n = 67; 69.8%), with 18 participants (18.8%) from agencies that provided domestic violence services only and 11 (11.5%) from agencies that provided sexual assault services only. Most participants came from agencies that provided their services to survivors only in rural communities (n = 66; 68.0%); 13 (13.4%) provided their services only in urban/suburban communities; and 16 (16.5%) provided their services in both rural and urban/suburban communities. We also conducted a chi-square analysis on the relationship between service foci and service geography. We determined that there was a significant relationship between these two agency characteristics (χ2 = 18.73, df = 4, p ≤ .001), with combined agencies being most often serving rural communities.
Next, we discuss the service goal results from the research. We present our results along with a discussion of the results due to the complex nature of the findings. We discuss the ways that each study finding is consistent with, or is not consistent with, the literature and research on domestic violence and sexual assault service delivery goals priorities.
Overall Service Delivery Goal Priorities
Common service goals
The first aim of this study was to identify directors’ overall opinions about service delivery goals among the various domestic violence and sexual assault service subtypes. Tables 1 and 2 show that on the whole, the directors in this sample highly ranked the provision of emotional support as an important goal across the different service subtypes. This finding is consistent with other research on the importance of emotional support for survivors. For example, Golding and colleagues (Golding, Wilsnack, & Cooper, 2002) noted the importance of emotional support for survivors of sexual assault because such support is associated with improved health. Likewise, research shows that increased emotional support may reduce the deleterious mental and physical health consequences associated with partner violence victimization (Coker, Watkins, Smith, & Brandt, 2003). This convergence of findings suggests that the provision of emotional support is a critical service delivery strategy.
Likewise, safety planning was also ranked as an important goal across the different service areas. In the literature, safety planning is a key recommended best practice that entails helping violence survivors to secure their safety by (a) determining escape routes at home, work, and school; (b) using legal remedies to address violence; (c) securing independent finances and economic resources; and (d) securing independent housing, as a few examples (Lindhorst, Nurius, & Macy, 2005; Roberts & Roberts, 2002). Consequently, our finding helps to substantiate safety planning as best practice recommendation consistent with the literature.
Remarkably, the provision of violence information as a service goal priority was only ranked as moderately important in this study, which is not consistent with the service literature. Rather, the literature recommends offering survivors a greater understanding of the effects of violence and trauma because providing information is an expression of the empowerment philosophy that is the foundation of domestic violence and sexual assault movements (Gilbert, 1994; McDermott & Garofalo, 2004; Roberts & Roberts, 2002; Tutty & Rothery, 2002; White Krees, Trippany, & Nolan, 2003). We speculate that the provision of information may not be considered an unimportant service strategy among these participants given its overall ranking as moderately important across service subtypes. Instead, this finding may reflect that the provision of information may not be as important as other service strategies, such as safety planning.
The study findings show that several goals were ranked consistently lower priorities across service subtypes, including the provision of community referrals, helping survivors with self-care strategies, and helping survivors with building social supports. Our findings regarding community referrals are notable because experimental research on domestic violence advocacy has determined greater access to community resources to be important (Bybee & Sullivan, 2002; Sullivan & Bybee, 1999). Also, the finding that self-care strategies were ranked as a lower service priority relative to other service goals was notable because this service strategy has been found to be a best practice in other research (Gorde, Helfrich, & Finlayson, 2004).
Our finding that directors rank social support strategies as less important relative to other service goals was also unexpected because social support has been identified as a factor associated with partner violence survivors’ resilience (Carlson, McNutt, Choi, & Rose, 2002). However, other research is mixed about the usefulness of social support for sexual assault survivors because of negative social reactions from friends, family, and providers (Ullman, 1996). Thus, this finding may reflect the uncertain nature of social reactions to violent victimization.
Unique service goals
This study’s findings about the differences in the rankings for the goals of legal and medical accompaniment, legal and medical information, and victims’ compensation shed light on the differences between the delivery of legal and medical advocacy in community-based practice among this sample of directors (see Tables 1 and 2). For medical advocacy, our findings show that medical accompaniment is the service strategy priority followed by the provision of medical information. For legal advocacy, the study findings show that the provision of legal information and help with victims’ compensation are clear priorities, though legal accompaniment is the next priority. Although the service strategy of helping survivors to improve their self-esteem is a recommended best practice in the domestic violence and sexual assault literature (Macy et al., 2009), it was only ranked as a moderate to low priority for support group, counseling, and shelter services in this study. Likewise, helping survivors with other life problems as needed was ranked a low priority by participants in our sample, even though a recommendation in the domestic violence literature is for providers to help survivors with safety by attending to their needs in holistic and individualized ways (Lindhorst et al., 2005).
Service Delivery Goal Priority Differences
Agency location differences
In this study, agencies that serve rural, urban/suburban, and both rural and urban/suburban locales were found to have statistically significant differences in prioritizing goals for crisis, medical advocacy, counseling, and support group services (see Table 3). In the context of crisis services, the findings show that the participants from agencies serving urban/suburban communities more highly prioritized the provisions of community referrals and safety planning, as well as safety planning in the context of medical advocacy, relative to participants from agencies that served rural locales in a dedicated way or as part of their service geography overall. We speculate that the emphasis on community referrals for urban/suburban providers in this study may reflect the reality that there are more services to which to refer in these communities relative to rural ones. The reasons why urban/suburban participants in this study placed a priority on safety planning is less apparent. However, these study findings may suggest a potentially important service provision difference for urban/suburban communities that future research should investigate to eliminate the possibility of a finding by chance. Likewise, our findings that urban/suburban directors prioritized the provision of emotional support in the context of counseling as less of a priority relative to other participants also requires additional research. One interpretation of these study findings is that participants in agencies serving rural/urban/suburban communities more highly prioritized self-esteem and self-care strategies for support groups to reflect a general service approach, which works well across all communities.
Agency services focus differences
We found in this study that agencies that are dedicated to domestic violence, dedicated to sexual assault, or provide both domestic violence and sexual assault services have significant differences in prioritizing crisis, medical advocacy, counseling, and support group service goals (see Table 4). In the context of crisis services, the participants from agencies dedicated to sexual assault services prioritized the provision of emotional and social support strategies more highly and the provision of safety planning less highly than participants from agencies that provide domestic violence services in either a dedicated or combined fashion. Though this finding was only marginally significant, it may reflect the importance of emotional support for sexual assault survivors in the immediate aftermath of violence. Given the mixed findings in the sexual assault literature regarding the usefulness of friends and family for social support (Ullman, 1996), it is notable that social support strategies were ranked in this study as more important in the context of crisis services among participants at agencies that focus on sexual assault. However, we speculate that our study findings suggest that planning for safety is considered a more important crisis service goal for participants from domestic violence agencies because many partner violence survivors needing crisis services may be still involved in dangerous situations.
Similarly for support group services, the participants from agencies dedicated to sexual assault services prioritized the provision of self-esteem, self-care, and the development of relationships with other survivors more highly than participants from agencies that provide domestic violence services. These study findings are consistent with the sexual assault services literature, which emphasizes the import of support groups for fostering self-esteem, promoting the development of relationships with others who survived similar experiences, and increasing self-care strategies (Koss & Harvey, 1991). Conversely, our findings showed that the participants from sexual assault agencies did not prioritize the provision of violence information as highly as the participants from agencies that provide domestic violence services. Thus, our study findings show that the provision of violence information may be a more important service goal for partner violence survivors relative to sexual assault survivors in the context of support group services.
Also in this study, participants from agencies with a combined focus tended to rank safety planning as a higher priority for medical advocacy than participants from agencies that provide a dedicated service, either domestic violence or sexual assault. In light of these findings, we posit that this service goal priority for directors from combined agencies may reflect a generic approach to medical advocacy for both survivors of partner violence and sexual assault. Alternatively, this finding may reflect the fact that directors of combined agencies know from experience that many violence survivors have experienced both domestic violence and sexual assault and that providing safety planning is especially helpful to survivors of multiple violent traumas in the context of medical advocacy. Future research should focus on how to tailor medical advocacy services to survivors of (a) partner violence, (b) sexual assault, and (c) both partner violence and sexual assault. Study participants from combined agencies also tended to rank social support strategies for counseling as a lower priority than participants from agencies that provide a dedicated service, either domestic violence or sexual assault. Given the mixed findings about social support in this study as well as the other literature cited earlier, we echo our recommendation that future research carefully investigate the utility of this practice for survivors of both partner violence and sexual assault.
Conclusions
Domestic violence and sexual assault agencies offer important and unique services for violence survivors. Unfortunately, limited evidence about service effectiveness poses a considerable barrier for practice, policy, and funding advancements. A key challenge to the development of an evidence-based practice research agenda for domestic violence and sexual assault services is the dearth of empirical information about the inner workings of these services. Though there is growing attention to domestic violence and sexual assault service evaluation and though there are articles, books, and manuals describing best practices, these streams of research have not been well integrated. Moreover, evidence about the ways that community-based providers deliver services in their everyday practice is needed, including how practices may vary because of agency differences.
With findings from a statewide survey of agency directors, this study provides information to help address these knowledge needs. More specifically, the study presents findings about service delivery goals for crisis, legal advocacy, medical advocacy, support group, individual counseling, and shelter. The literature concerned with the development of evidence-based practice manuals recommends the documentation and empirical verification of theories of change, service strategies, service formats, and service goals (Carroll & Nuro, 2002; Fraser et al., 2009; Saunders, Berliner, & Hanson, 2004). By helping to determine how those delivering these services think they are best delivered in their community-based settings, the findings from this research may be helpful in developing evidence-supported service manuals.
Some of the findings are consistent with the service recommendations found in the best practices literature (e.g., the importance of emotional support). However, the relatively low ranking of some service goals, such as the provision of community referrals, is not consistent with the literature. Such contradictory findings suggest the need for researchers to investigate effective service strategies while considering the realities of community-based practice. In addition, the different findings about the importance of social support service strategies point to the import of investigating the complex nature of social support for violence survivors.
This study also presents information about how service goal priorities differ based on agency characteristics. The findings regarding the differences in crisis and support group service goal priorities point to ways that these services may need to be differentiated between sexual violence and partner violence survivors, as well as tailored for delivery in urban/suburban areas. The findings regarding differences in combined services and services delivered by agencies that serve rural/urban/suburban areas may point to a general service strategy that is offered by these agencies. Such a general service strategy should be evaluated in future research efforts, including its helpfulness relative to tailored, specialized services.
Nonetheless, we note the relationship between the agency characteristics of service foci and geography. In light of this relationship, some of the common significant findings may be due to either or both of these characteristics. Unfortunately with this study, we are not able to determine which characteristic (or both) made the difference in some of the significant findings. Though it is not surprising that agencies in rural areas where there are fewer resources would provide both domestic violence and sexual assault services, future research should use larger, national samples to further investigate these agency characteristics and their relationships to service delivery practices.
We also note how few significant differences were determined based on the type of service provided either by agency or by the agency service locale. For example, it is striking that we did not find any significant differences in service goal priorities for legal advocacy among participants at dedicated domestic violence and sexual assault agencies or any significant differences for shelter services among participants at rural and urban/suburban agencies. Although there are statistically significant differences and these are worthy of consideration, we encourage readers to be mindful of our nonsignificant findings too. Domestic violence and sexual assault services are often described as distinct sets of services, and the practices of rural and urban agencies have been posited to be markedly different. However, our research findings suggest more service commonalities than differences on these agency characteristics.
Limitations
We also encourage readers to be mindful that a low priority ranking for a service goal does not imply that a goal is unimportant. Such findings only suggest that the service goal may be less important in a certain service context relative to other goals. The sample only included directors from North Carolina agencies, thereby limiting the generalizability of the results. However, the comprehensiveness of the sampling frame and high response rate (94%) provide assurance that the findings are representative of the state. We investigated directors’ opinions of how service delivery goals should be prioritized for the six service types that appear most often in the domestic violence and sexual assault services literature. However, there are other important domestic violence and sexual assault services (e.g., lethality risk assessment) that are worthy of investigation.
Another limitation is that these findings are based on directors’ opinions about service goal priorities. Thus, we recommend empirical testing of these service goal priorities especially in light of the dearth of evidence-based practices for domestic violence and sexual assault services. Given that the findings from this study help address the first step in the development of evidence-based domestic violence and sexual assault practices (i.e., conceptualizing an intervention and designing treatment manual), we encourage future research to investigate the efficacy and effectiveness of these services.
We also recommend an investigation of other agency staff members’ perspectives about helpful domestic violence and/or sexual assault services for survivors. Frontline staff members’ perspectives about services may vary in important ways from directors. An additional next step should include an investigation of what service strategies survivors find most helpful in securing safety and recovering from the trauma of violence. Such research should also investigate what service strategies survivors from diverse backgrounds deem as most helpful. Unfortunately, violence services have been largely developed and evaluated in “culturally neutral” ways (Bent-Goodley, 2005, p. 196), including this study. Thus, work is urgently needed to determine how domestic violence and sexual assault services are best delivered to diverse survivors from nonmajority cultures and groups.
Footnotes
Acknowledgements
We wish to acknowledge Lydian Altman-Sauer, Barry Bryant, Pam Dickens, Margaret Henderson, Carol Nobles, Leslie Starsoneck, Gordon Whitaker, the staff of the North Carolina Council for Women/Domestic Violence Commission, the staff of the North Carolina Coalition Against Domestic Violence, and the staff of the North Carolina Coalition Against Sexual Assault for their help with developing the survey instrument. We also wish to acknowledge Tamara Sangster for her contributions to this research, as well as Susan White and Diane Wyant for their comments on earlier drafts of this manuscript.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
This project was supported by Award No. 180-1-05-4VC-AW-463 awarded by the U.S. Department of Justice, through the North Carolina Department of Crime Control & Public Safety/Governor’s Crime Commission.