
Abstract
This study explored the prevalence of violent behaviors in patients who are addicted to drugs. A sample of 252 addicted patients (203 male and 49 female) who sought outpatient treatment was assessed. Information on violent behaviors, sociodemographic factors, consumption factors (assessed by the European version of the Addiction Severity Index [EuropASI]), psychopathological factors (assessed by Symptom Checklist–90–Revised [SCL-90-R]), and personality variables (assessed by Millon Clinical Multiaxial Inventory [MCMI-II]) was collected. Drug-addicted patients who were associated with violent behaviors were compared on all variables with patients who were not associated with violent behaviors. The rate of drug-addicted patients with violent behaviors in this sample was 39.68% (n = 100). There were significant differences between the numbers of patients who did and did not demonstrate violence on some variables. Patients with violence problems were younger than those without violence problems and were more likely to report having been a victim of abuse. Moreover, they were significantly more likely to have experienced an overdose and showed a significantly higher score on several EuropASI, SCL-90-R and MCMI-II variables. According to these results, patients with violence control problems present with both a more severe addiction and several comorbid problems. The implications of these results for further research and clinical practice are discussed.
Introduction
Concern about the relationship between drug abuse and the development of violent behavior and criminal acts has increased in recent years. Some authors posit that violence is a major cause of morbidity and mortality among drug-addicted patients, especially in patients who are addicted to illegal substances (Marshall, Fairbairn, Li, Wood, & Kerr, 2008). Several studies have shown evidence regarding high rates of physical violence among addicted patients (Clements & Schumacher, 2010; Fernández-Montalvo, López-Goñi, & Arteaga, 2011; Moore et al., 2008). These studies have analyzed the violence both from a general perspective and from the specific perspective of gender violence.
Regarding gender-based violence, research has consistently shown evidence of a high presence of alcohol and/or drug abuse among men who batter (Murphy & Ting, 2010). For example, research has shown that approximately 48% of perpetrators of gender violence have problems with alcohol abuse or dependence and almost 20% demonstrate problems with drug consumption (Fernández-Montalvo & Echeburúa, 1997, 2005). The same relationship is observed when analyzing the problem from the opposite perspective. Recent studies show that between 40% and 60% of drug-dependent patients who live with their partners have been perpetrators of violence against their partners during the year before beginning treatment for addiction (Easton, Swan, & Sinha, 2000; Fals-Stewart, Golden, & Schumacher, 2003; O’Farrell & Murphy, 1995). This had led to increasing concern about the relationship between intimate partner violence and drug abuse in recent years (Moore et al., 2008).
Substance abuse also appears to be related to violent behavior against society and to the commission of criminal acts. In a study by Colasanti et al. (2008), which evaluated a sample of 350 psychiatric patients, 45% of patients reported aggressive behavior and 33% of patients demonstrated violent behavior. In addition, violent behaviors were associated with alcohol and drug abuse. Similar data have been obtained in other studies. In a sample of 1,114 drug users, Marshall and colleagues (2008) found that 70% of women and 66% of men reported some form of aggression in a 5-year follow-up period. Similarly, Mericle and Havassy (2008) found that 41% of the sample studied had been involved in violent behaviors during the month prior to the study. Moreover, drug abuse was a factor in 40% of the detected incidents.
A similar pattern has been shown for the relationship between the commission of criminal acts and drug consumption. Both international studies (Bennett & Holloway, 2005) and those carried out in Spain (Santamaría & Chait, 2004) show a relationship between drug use and numerous criminal acts.
Due to the findings described above, researchers have begun to believe that drug treatment programs may be an appropriate context to identify the presence of general violent behaviors and partner-specific violence. Identifying behaviors and studying their impact on therapy progress will help clinicians treat both problems simultaneously and thus could help improve the results of existing treatment programs.
The link between drug abuse, alcohol abuse, and violence remains unknown today. Although there is some evidence about the influence of certain drugs in the development of violence behaviors (Marshall et al., 2008; Martin & Bryant, 2001), the connection between substance use and violent behavior is complex and is suggestive rather than conclusive (Boles & Miotto, 2003; Fagan, 1993). Moreover, most data have been obtained from alcohol abuse, and there is little research with other drugs. There is insufficient research toward the specific causal role that substances play in the perpetration of violence.
One of the most commonly used frameworks developed to explain the relationship between drugs, alcohol, and violence was proposed by Goldstein (Goldstein, 1985, 1989). According to this framework, three categories are used to describe the factors that link drugs and violence: (a) pharmacological (pharmacological effects of substances enhance violent behavior, and individuals under the influence of drugs are less aware of their surroundings, making them vulnerable to violence), (b) economical (engagement in economically oriented violent crime to sustain drug-use behaviors), and (c) systemic (the endemic nature of violent interactions within the system of drug distribution and use). However, only limited empirical evidence supports all three components of this conceptual model (Boles & Miotto, 2003; Marshall et al., 2008; Martin & Bryant, 2001). Increased evidence regarding the relationship between violence and substance abuse underscores the fact that more research is needed to address the nexus between substance abuse and violence and to understand the psychological profile of substance abusers with violence problems.
The present study examined the prevalence rate of violent behaviors in a sample of drug-addicted patients. The main purposes of this study were to assess the specific characteristics of drug-addicted patients with associated violence problems, to identify the differential profiles of patients who do and do not demonstrate violence problems, and to determine the relationship between violence problems and treatment retention and dropout.
Method
Participants
The initial sample consisted of 314 consecutive addicted patients who sought outpatient treatment at the Proyecto Hombre addiction treatment program in Pamplona, Spain from October 2008 to July 2010.
The current study’s admission criteria were that the patients had to (a) meet the diagnostic criteria of substance dependence according to the DSM-IV-TR (American Psychiatric Association, 2000), (b) be between 18 and 65 years old, (c) give their informed consent to participate in the study, and (d) complete the three assessment sessions.
Sixty-two (19.8%) of the 314 initial participants did not meet the criteria mentioned above. Therefore, the final sample was composed of 252 participants.
The mean age of the individuals included in the study was 37.6 years (SD = 9.5); the sample included 203 (80.6%) men and 49 (19.4%) women. The socioeconomic level was middle to lower middle class. The main substances that motivated treatment were cocaine (49.6% of the sample) and alcohol (43.3% of the sample), followed by other substances (e.g., heroin, cannabis, amphetamine, etc.) in smaller numbers (7.1% of the sample).
Assessment Measures
The EuropASI (Kokkevi & Hartgers, 1995) is the European version of the Addiction Severity Index (ASI; McLellan, Luborsky, Woody, & O’Brien, 1980). This interview assesses the need for treatment in the following six areas: (a) general medical state, (b) labor and economic situation, (c) drug consumption (alcohol included), (d) legal problems, (e) family and social relationships, and (f) psychiatric state. In this study, we have used the “composite scores” (CS) of the EuropASI. The composite scores were developed for research purposes; they are arithmetically based indicators of current (last 30 days) problem severity and range between 0.00 and 1.00, with higher values denoting higher degrees of severity. The composite scores have been calculated according to the proposal by Koeter and Hartgers (1997). The Spanish version of the EuropASI was used in this study (Bobes, González, Sáiz, & Bousoño, 1996).
The Symptom Checklist–90–Revised (SCL-90-R; Derogatis, 1992; Spanish version by González de Rivera, 2002) is a self-administered general psychopathological assessment questionnaire. It consists of 90 questions that are answered on a 5-point Likert-type scale, ranging from 0 (none) to 4 (very much). The questionnaire aims to assess the respondent’s psychiatric symptoms. The SCL-90-R has been shown to be sensitive to therapeutic change and thus may be used for either single or repeated assessments. The SCL-90-R measures nine areas of primary symptoms: somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. It also provides three indices that reflect the participant’s overall level of severity.
The Millon Clinical Multiaxial Inventory (MCMI-II; Millon, 1997) is a self-report questionnaire with 175 true/false items. It was designed to identify clinical states and personality disorders that are similar to those contained in the DSM-IV-TR. The MCMI-II contains eight basic personality scales: (a) Schizoid-Asocial, (b) Avoidant, (c) Dependent-Submissive, (d) Histrionic-Gregarious, (e) Narcissistic, (f) Antisocial-Aggressive, (g) Compulsive-Conforming, and (h) Passive-Aggressive. In addition to the basic personality patterns, there are three pathological personality scales: Schizotypal (S), Borderline (B), and Paranoid (P). The nine symptom scales of the MCMI-II were not taken into account in this study as they are not relevant to the purposes of our research. According to the conservative criteria of Weltzer (1990) regarding the MCMI-II, a base rate score above 84 for the personality scales is considered to be significant for the existence of a personality disorder.
Procedure
Once the clinical sample was selected using the previously described criteria, the assessment of the sample was carried out in three sessions before beginning the treatment. Each session took place once a week for 3 weeks; the time interval between sessions was the same for each participant. In the first session, data related to sociodemographic characteristics and drug consumption were collected using the EuropASI. In the second session, the presence of psychopathological symptoms was assessed using the SCL-90-R. Finally, in the third session, the prevalence of personality disorders was assessed using the MCMI-II.
After the assessment sessions, patients began the standard treatment of Proyecto Hombre for addiction. Outpatient treatment at this program consists of a cognitive-behavioral intervention aimed at abstinence from substances. The treatment lasts an average of 9 months with a subsequent follow-up period of 12 months.
Data Analysis
Descriptive analyses were conducted for all variables. Bivariate analyses were employed using χ2 or t test statistics, depending on the nature of the variables studied. A difference of p < .05 was considered significant. Statistical analyses were carried out using SPSS (version 15.0 for Windows).
Results
Prevalence of Drug-Addicted Patients With Violent Behaviors
The rate of drug-addicted patients with violent behaviors in this sample was 39.68% (n = 100). Each of these patients reported that they could not control violent impulses in different settings whether with family, friends, or drug-abuse partners. Moreover, in some cases, violence emerged in crime settings to obtain money for buying drugs (e.g., pickpocketing, shoplifting, robbery, drug dealing, etc.).
Comparison Between Drug-Addicted Patients With and Without Violent Behaviors
Sociodemographic and consumption variables
Regarding the sociodemographic variables that were assessed, the only statistically significant difference was found for age. On average, patients associated with violence problems were younger than those without violence problems (Table 1).
Comparisons in Sociodemographic and Drug Abuse Characteristics
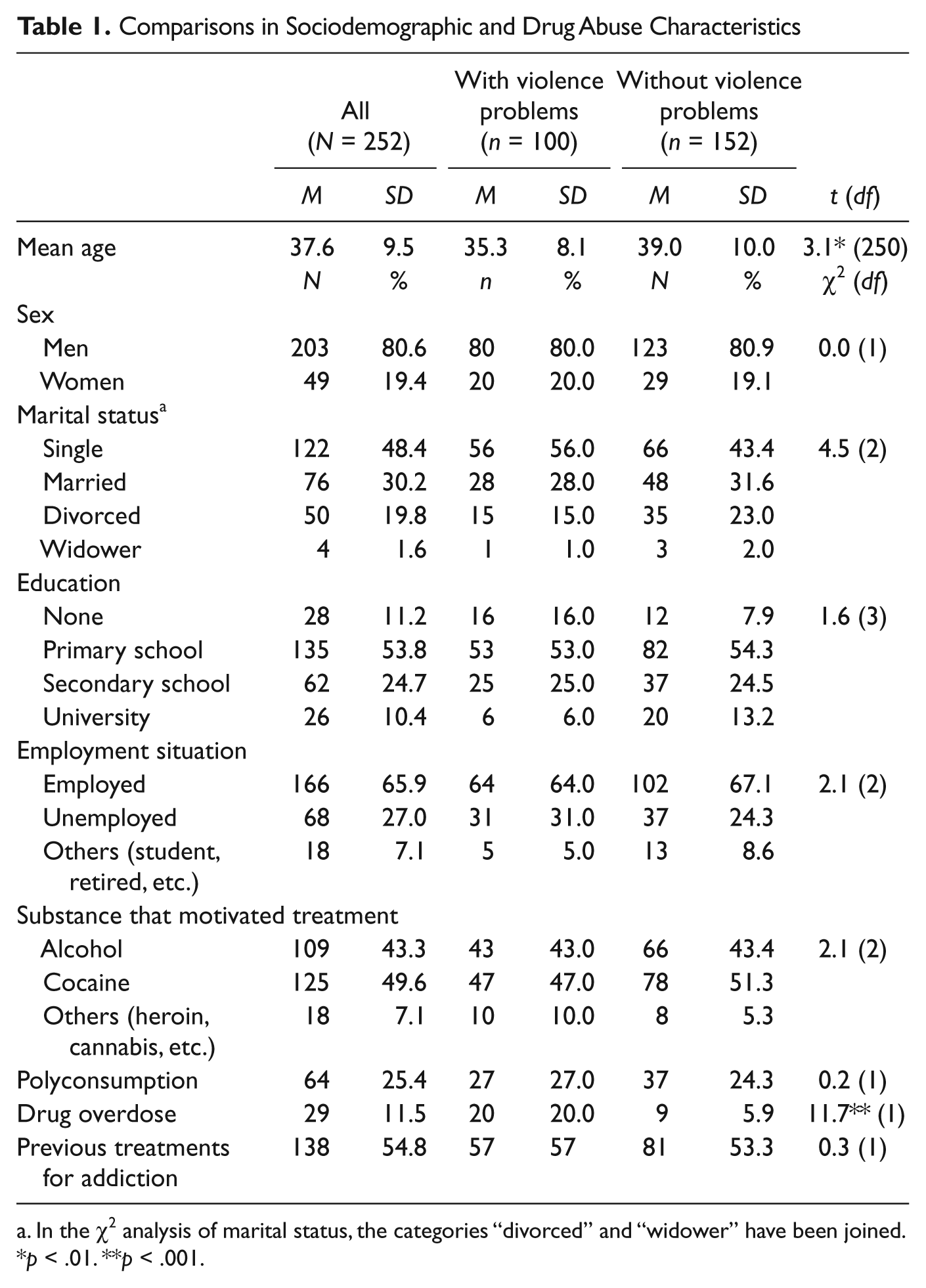
In the χ2 analysis of marital status, the categories “divorced” and “widower” have been joined.
p < .01. **p < .001.
The addicted patients with violence problems were also more likely to have experienced an overdose. Overall, 11.5% of the sample had ever experienced a drug overdose. However, addicted patients with violence problems experienced an overdose significantly more frequently (20% of the sample) than those without violence problems (5.9% of the sample).
Regarding areas of the EuropASI, patients with violent behaviors had significantly higher scores on variables related to legal situation, social relationships, and need for psychiatric treatment (Table 2). The mean composite scores in these areas show a great need for treatment to resolve the patients’ problems.
Comparisons in Clinical Variables
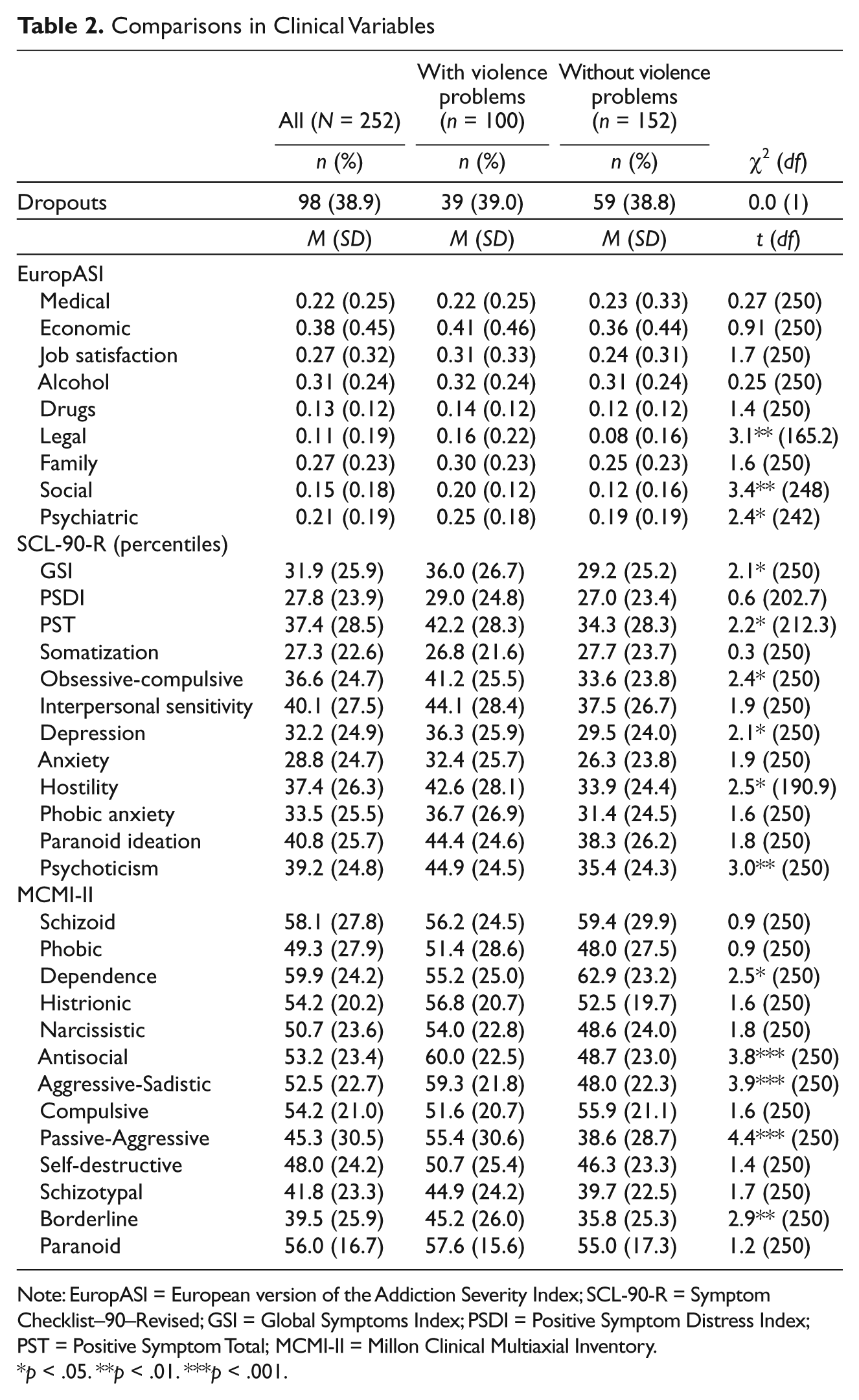
Note: EuropASI = European version of the Addiction Severity Index; SCL-90-R = Symptom Checklist–90–Revised; GSI = Global Symptoms Index; PSDI = Positive Symptom Distress Index; PST = Positive Symptom Total; MCMI-II = Millon Clinical Multiaxial Inventory.
p < .05. **p < .01. ***p < .001.
Psychopathological variables
Regarding psychopathological variables, the results of the SCL-90-R symptoms inventory show that only a moderate level of psychopathological symptoms in the participants was found (Table 2). In fact, overall, their score is positive in 37 of the 90 items contained in the inventory (Positive Symptom Total = 37.4). Furthermore, according to the Global Symptoms Index (GSI; X = 31.9), symptoms do not appear in this sample with any great degree of intensity as the cutoff point is not exceeded for any of the overall indices or any of the specific dimensions.
In terms of differentiating between the two subgroups in the areas assessed by the SCL-90-R, significant differences were found in two overall inventory indices (GSI and Positive Symptoms Total [PST]) as well as in the obsessive-compulsive, depression, hostility, and psychoticism dimensions. Although neither of the subgroups exceeded the cutoff point for these dimensions, the patients with violence problems present with significantly more symptoms than those without violence problems.
Personality variables
Drug-addicted patients who were associated with violence problems showed a higher score in four scales of the MCMI-II; the scales were the Antisocial, Aggressive-Sadistic, Passive-Aggressive, and Borderline scales. Patients who were not associated with violence problems scored significantly higher on the MCMI-II Dependence Personality Disorder Scale (Table 2).
The overall prevalence rate in this sample for at least one personality disorder was 46.8% (n = 118; Table 3). The most prevalent disorders were dependence personality disorder and passive-aggressive personality disorder, which affected 11.5% and 11.1% of the sample, respectively.
Comparison in the Rate of Personality Disorders
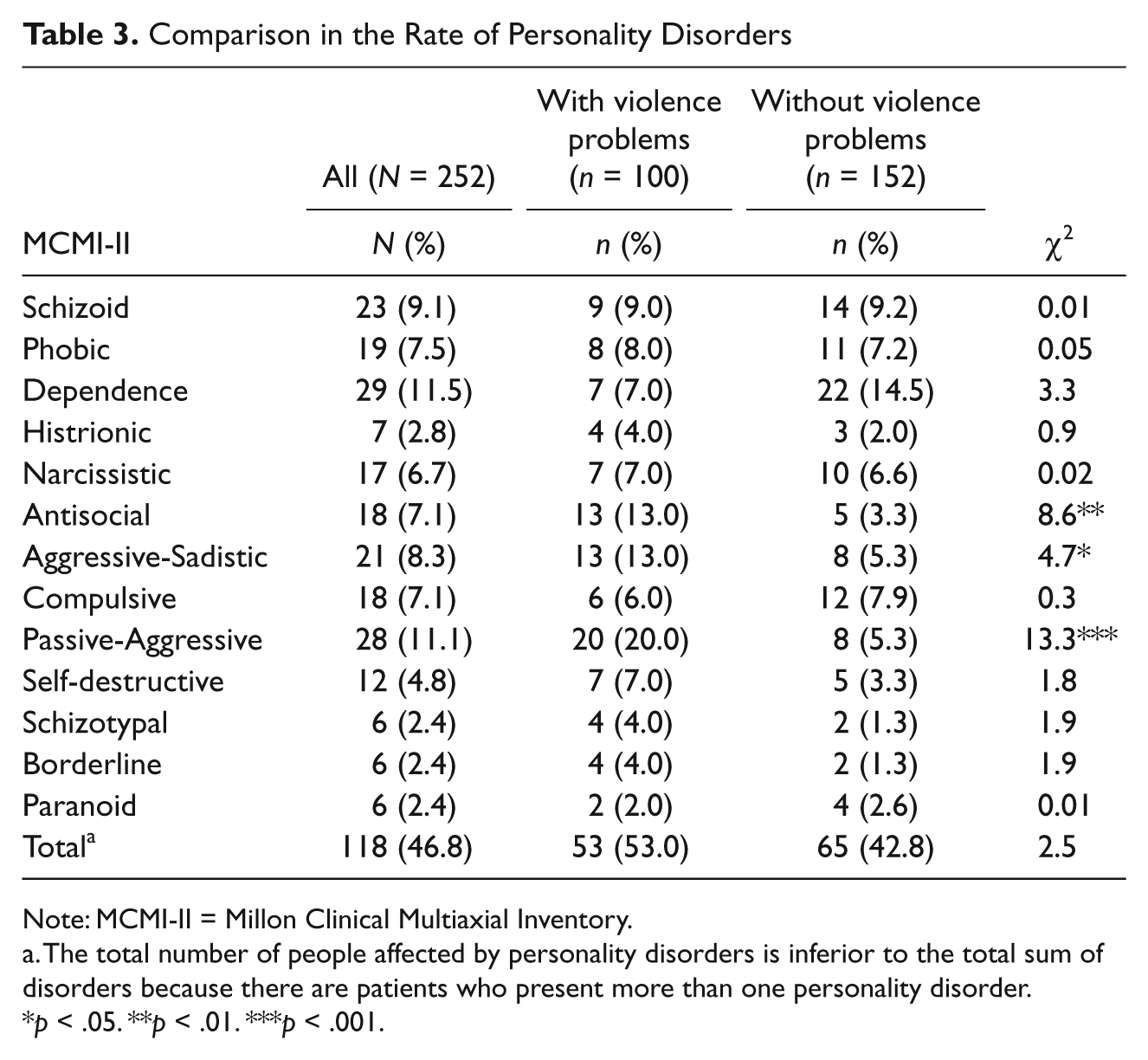
Note: MCMI-II = Millon Clinical Multiaxial Inventory.
The total number of people affected by personality disorders is inferior to the total sum of disorders because there are patients who present more than one personality disorder.
p < .05. **p < .01. ***p < .001.
No statistically significant differences were found between groups regarding the overall prevalence rate of personality disorders. The most prevalent personality disorder among the patients associated with violence problems was passive-aggressive personality disorder (20%), followed by antisocial and aggressive-sadistic personality disorders (13% each). Each of these disorders was significantly more prevalent in patients with violence problems than those without. The most commonly diagnosed personality disorder in patients without violence was the dependence personality disorder, although this difference was not statically significant.
Maladjustment variables
Comparisons of some of the maladjustment variables are shown in Table 4. As can be seen, the patients with violence problems showed more adjustment difficulties with family (especially parents, brothers, and sisters) and social (friends and colleagues) domains.
Comparison in Maladjustment Variables
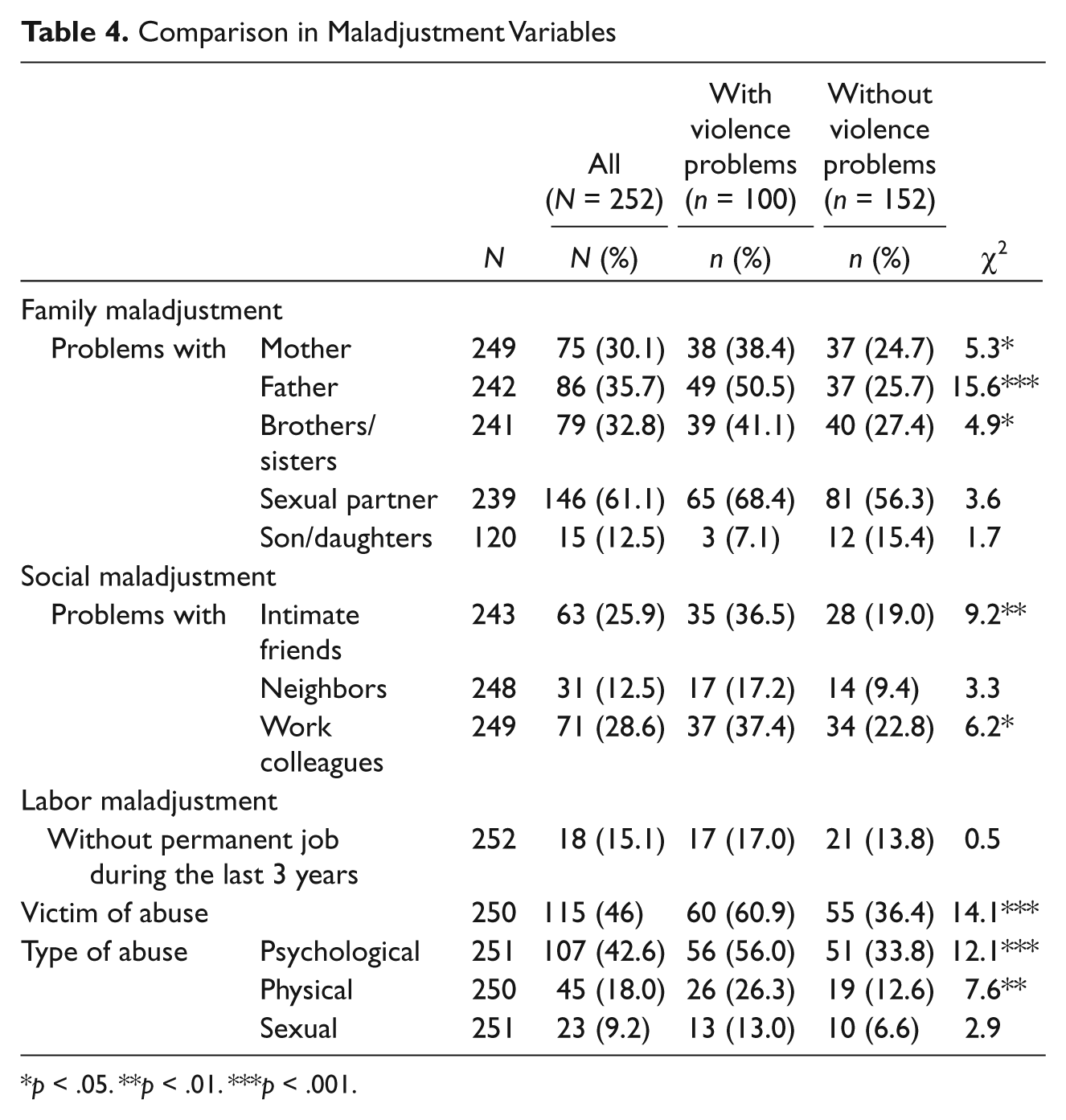
p < .05. **p < .01. ***p < .001.
It is important to note that 46% of the patients studied had been victims of different kinds of abuse. This level for the overall sample is worrisome; even so, patients with violence problems were more likely to report any kind of abuse (60.9%) than patients without violence problems (36.4%). Statistically significant differences were found between the groups in the categories of psychological and physical abuses.
Discussion
The results of this study indicate that violent behaviors are quite frequent in addicted patients. According to this study, 39.68% of the sample had experienced problems related to violence control. These problems were closely associated with drug consumption and were mainly directed at family, friends, and drug-abuse partners or executed to obtain money for buying drugs. These results are consistent with data obtained in the few studies that were carried out to date in this field (Boles & Miotto, 2003; Marshall et al., 2008; Mericle & Havassy, 2008).
These results are very relevant because interpersonal violence can interfere with therapy progress and with maintaining abstinence from substances (Schneider & Timko, 2009). Encountering interpersonal problems is well known to predict relapse in addicted patients (Fernández-Montalvo, López-Goñi, Illescas, Landa, & Lorea, 2007; Marlatt & Gordon, 1985). Thus, violent behaviors are an important domain to account for when assessing and treating addicted patients.
Comparisons between addicts with and without associated violence problems showed statistically significant differences in sociodemographic, psychopathological, personality, and adjustment variables. According to these results, patients with violence control problems presented with both more severe addictions and with more comorbid problems.
The profile of drug-addicted patients with violence problems as compared with nonviolent drug-addicted individuals reflected a younger patient who had experienced risk situations related to drug consumption more frequently (e.g., drug overdose) and who demonstrated a greater need for help in important domains, as assessed by the EuropASI, including legal situation, social relationships, and psychiatric state. Furthermore, the results showed an increased presence of psychopathological comorbidity in violent drug-addicted patients, as reflected by SCL-90-R and MCMI-II scores. It is noteworthy, however, that nonviolent patients scored significantly higher on the Dependent Personality Scale. This is consistent with other results as the presence of violent behavior is clearly inconsistent with the typical traits of a dependent personality.
Regarding maladjustment variables, patients who were associated with violence showed more maladjustment issues in some family, social, and labor variables. Problems in these domains could also interfere seriously with the progress of addiction treatment (Fernández-Montalvo, López-Goñi, Illescas, Landa, & Lorea, 2008; López-Goñi et al., 2011).
One surprising and worrisome piece of data obtained in this study is the high rate of patients who had been victims of different kinds of abuse (46% of the whole sample), especially for drug-addicted patients who were associated with violent behaviors (more than 60% of this group). Although few studies have examined risk factors for violence among substance users, the prevalence of abuse among this population has been found to be strikingly high in numerous studies, with some studies showing rates above 50% in drug-addicted samples (Chermack, Walton, Fuller, & Blow, 2001; Finlinson et al., 2003; Marshall et al., 2008). Nonetheless, the rate of abuse found in drug-addicted patients in this research was higher than expected. Additional studies are needed to validate these findings and explore potential explanations for this phenomenon.
Our results suggest that individuals with violence problems showed a more severe profile of addiction. Because of this, some authors have recommended that violent patients with a substance use disorder must be provided with additional, targeted intervention to promote violence-free outcomes (Schneider & Timko, 2009). When violent and nonviolent patients with a substance use disorder receive comparable treatments, the violent group tends to have poorer substance use–related outcomes at follow-ups (Fernández-Montalvo et al., 2011). However, few studies have focused on this aspect and more research in this area is needed.
The present study has a number of limitations. First, the exploratory and descriptive nature of this study means that the specific causal role that substances play in the perpetration of violence remains unknown. The configuration of the sample itself is another issue that should be taken into account. As few women were included in the sample, the results obtained can mainly be generalized to male addicted patients. It is true that almost all studies about drug dependence include largely male samples, but it should nevertheless be taken into account when generalizing the obtained results. Third, the assessment of the sample was carried out in three sessions, each of which took place once a week. Hence, the final sample may be biased because all clients had to attend three consecutive measurements during a 3-week period. The patients who dropped out before all of the measurements were completed were not included in the study. This methodological problem might influence the findings and must be considered in further research.
In summary, the present study investigated the prevalence rate of violent behaviors in drug-addicted patients as well as the differential profiles of patients with and without violence problems. This study forms part of a wider research base that is focused on understanding factors related to violence and addictions. From a clinical perspective, this is an important goal because violence interferes with the course of the therapeutic evolution of addicted patients.
Footnotes
Acknowledgements
The authors would like to thank the “Proyecto Hombre de Navarra” program staff for their help with assessing the clinical sample and Octavio Díaz for help with managing the data.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (code PSI2009-08500) from the “Ministerio de Ciencia e Innovación” of the Spanish Government.