
Abstract
In this study we estimated the combined effects of violence experiences, parenting processes, and community poverty on sexual onset, alcohol or other drug (AOD) use at last sex, multiple sex partners, and prior pregnancy in a sample of 7th-, 9th-, and 11th-grade adolescents (n = 7,891), and the subsample of sexually experienced adolescents (n = 2,108). Multilevel multivariate logistic regression analyses revealed that having experienced any interpersonal violence, and low levels of perceived parental warmth and parental knowledge predicted sexual onset. Adult sexual abuse or peer sexual coercion increased the odds for AOD use at last sex and having multiple sexual partners. When demographic, violence experiences and parenting behaviors were accounted for, poverty was not associated with sexual onset, AOD use at last sex, or multiple sex partners. Results suggest prevention efforts to reduce teen dating violence may be especially important to diminish sexually risky behaviors among adolescents.
Recent attention to adolescents’ experiences of violence demonstrates the importance of exposure to violence on teens’ developing sense of healthy intimate relationships (Banyard, Cross, & Modecki, 2006). Nineteen percent (19.4%) of teens, ages 14 to 17, have reported physical abuse and 3.9% have reported sexual abuse by an adult within their lifetime (Finkelhor, Turner, Ormrod, & Hanby, 2009). National data indicate that 7.7% of 14- to 17-year-olds have been sexually assaulted by a peer, 8.8% have experienced dating violence within their lifetime (Finkelhor et al., 2009), and 1 in 10 sexually experienced adolescents has experienced physical violence in his or her most recent sexual relationship (Eaton, Davis, Barrios, Brenner, & Noonan, 2007).
Sexual and physical abuse are among the top three types of child abuse reported by 48 states in 2008 (U.S. Department of Health and Human Services, Administration on Children, Youth, and Families [DHHS_ACYF], 2008). Physical abuse is most often perpetrated by family members (DHHS_ACYF, 2008), whereas comparatively fewer sexual assaults on children and teens occur by a family member (10%; Finkelhor, Hammer, & Sedlak, 2008). Between 2004 and 2007, adolescent females, age 15 to 17 and 18 to 19, received medical care for injury from sexual assault at rates of 152.6 and 163.7 per 100,000 respectively (Morbidity and Mortality Weekly Report [MMWR], Vol. 58, SS-6, 2009). According to a U.S. Office of Justice report, one in four perpetrators of sexual assault on children and adolescents is a youth aged 13 to 17; perpetrators are more often male, and victims of sexual assault are more often female (Finkelhor et al., 2008).
These data suggest that adolescents experience violence, and in particular sexual violence, at alarming rates. Interpersonal violence in the form of physical or sexual abuse by an adult, and teen sexual coercion (including penetration) has been associated with risk-taking behaviors that are known to increase risk for sexually transmitted diseases, pregnancy, and HIV among women and adolescent girls. Intimate partner relationship violence (Manlove, Ryab, & Franzetta, 2004) and child sexual abuse (Parillo, Freeman, Collier, & Young, 2001) have been linked to failure to use contraception. In other research, adolescents who reported child sexual abuse were at increased odds of using substances prior to sex, having more than one sexual partner, and having sex without a condom (Voisin, 2005). Similarly, women who experienced child sexual abuse involving penetration reported more sex partners than those with no history of childhood sexual assault (Parillo et al., 2001). In a sample of urban Black youth, sexual victimization was associated with sexually transmitted infections (STIs) for girls and self-reported pregnancy among both girls and boys (Trent, Clum, & Roche, 2007). Eaton et al. (2007) found that adolescent girls and boys who were sexually experienced and had multiple sexual partners were at increased risk for dating violence victimization in the past year. Taken together, these studies suggest that interpersonal violence is a context within which other risk behaviors occur. Experiences of interpersonal violence increase adolescents’ risk for negative outcomes across a variety of indicators including sexual risk and substance use (Eaton et al., 2007; Parillo et al., 2001; Spano, Vazonyi, & Bolland, 2009; Voisin, 2005).
As policy makers and practitioners work to reduce sexual risk-taking among adolescents (U.S. Department of Health and Human Services [DHHS], 2007, Healthy People 2010 Midcourse Review), it is prudent to examine more closely adolescents’ experiences of violence as a context that may contribute to increasing teens risk for sexually transmitted diseases or pregnancy. Recent national research suggests that an estimated 3.2 million adolescent females in the United States (26%) have contracted at least one STI (Centers for Disease Control, 2008). U.S. teens have the highest rate of unplanned pregnancies than any other industrialized nation (Alan Guttmacher Institute, 2004; Panchaud, Singh, Feivelson, & Darroch, 2000; Santelli, Morrow, Anderson, & Lindberg, 2006). In addition, national data indicate that living in a poor community is predictive of more frequent sex, a greater number of sexual partners, and failure to use contraception among adolescents, even after accounting for family characteristics and potential mediating parenting variables (Baumer & South, 2001). Dupere, Lacourse, Willms, Leventhal, and Tremblay (2008) reported with a national Canadian sample, that for most adolescents in their study, living in a poor neighborhood did not increase the odds of sexual onset over time. Among 12- to 13-year-old girls, however, living in a poor neighborhood and having a history or conduct problems predicted early sexually activity.
The role of parents in reducing adolescents’ sexual risk is well established in research. There is empirical evidence that a warm supportive parent–adolescent relationship is associated with delay of sexual debut, having less frequent sex, having only one sexual partner, and consistent use of contraception (DiClemente et al., 2007; Miller, Benson, & Galbraith, 2001). Across diverse samples and study designs, parental knowledge has demonstrated strong effects on reduced sexual risk taking. Student reports of parents’ knowledge and solicitation of their whereabouts and behaviors has been associated with having one sexual partner (versus multiple partners) and using contraception (Huebner & Howell, 2004; Rodgers, 1999; Whitaker, Miller, & Clark, 2000). Among African American youth who reside in low-income urban neighborhoods, adolescent reports that their parents knew where they went and with whom they spent their time outside of the home significantly reduced the odds of being diagnosed with an STI (Bettinger et al., 2004; Crosby, DiClemente, Wingood, Lang, & Harrington, 2003) and having multiple sexual partners (DiClemente et al., 2007).
Parents can also mediate the effects of violence exposure on adolescents. In a 3-year longitudinal study of African American youth living in poor communities, adolescents living in poor communities who were exposed to violence at time one were at increased risk for becoming perpetrators 3 years later (Spano et al., 2009). In addition, parents’ efforts to mediate the effect of violence exposure on violent behavior through monitoring and rule setting were less effective when adolescents were exposed to violence at Time 1. This suggests that parenting processes known to typically protect teens against risks may be compromised within the context of a poor neighborhood where violence and social norms compete with parental control attempts.
These trends prompt us to explore two research questions. First, in what way are experiences of violence (physical and sexual abuse and teen sexual coercion), parenting practices, and living in a poor community related to (a) having had sexual intercourse, (b) having used alcohol or other drugs (AOD) at last sexual intercourse, (c) having more than one sexual partner, and (d) having a history of pregnancy? Each of these behaviors is known to increase teens’ risk for pregnancy or STIs. Second, are factors within these contexts differentially predictive of these risky behaviors? These questions help to expand current literature by examining the independent contribution of physical and sexual victimization and parenting processes to behaviors that place adolescents at risk of negative sexual outcomes within the context of community poverty. They can also help direct prevention efforts to reduce adolescent pregnancy and STIs.
A goal of this study is to concurrently examine the effects of individual, family, and community contexts specific to sexually linked behavioral risks among teens. In doing so, we can parcel out effects of interpersonal violence, parenting behaviors, and community poverty for specific behaviors that can increase teens’ risk for STIs or pregnancy. To this end, we propose the following:
Hypothesis 1: Adolescents living in poorer communities will have more personal and family risk factors (interpersonal violence experiences, low parental warmth, and knowledge) and will more likely engage in sexually risky behaviors than youth who live in communities with less poverty.
Hypothesis 2: Adolescents who have experienced interpersonal violence, who have family risk factors, and who live in higher poverty communities will more likely engage in sexually risky behaviors than youth without these risk factors.
Method
Sample
We use a sample of 7th-, 9th-, and 11th-grade adolescents from 26 middle and high schools that participated in a large community-based health assessment in a southeastern city and surrounding rural and suburban areas. Students were anonymously surveyed by trained data collectors during one classroom hour. A passive parental consent procedure was used; 95% of students who were present on the day of surveying gave their assent to participate (n = 9101). Three percent of students declined to participate and 5% of surveys were unusable because of obvious patterning or response bias leaving a usable data set of 8,373. Procedures were approved by the Washington State University Institutional Review Board.
Study sample and sexually active subsample
A study sample of 7,891 students who lived with two first-married parents, a single parent, or in a remarried or cohabiting family, and had complete data on the included predictor variables were selected out to examine correlates of onset of sexual intercourse. Using this same selection criterion, a subsample of 2,108 sexually experienced adolescents was also selected to examine correlates of risk-taking behaviors and outcomes that can only be measured among sexually active youth (drug or alcohol use during sex, number of partners, and experience of a pregnancy). Table 1 presents descriptive information on the study sample and subsample. As can be seen in the table, in both samples there was an even gender distribution and the majority of students were White. Compared with the larger study sample, the sexually active sample had more adolescents who resided in a single or remarried family, were older and had slightly fewer mothers who had completed some college education.
Sample Characteristics: Demographics, Context Variables, and Outcomes
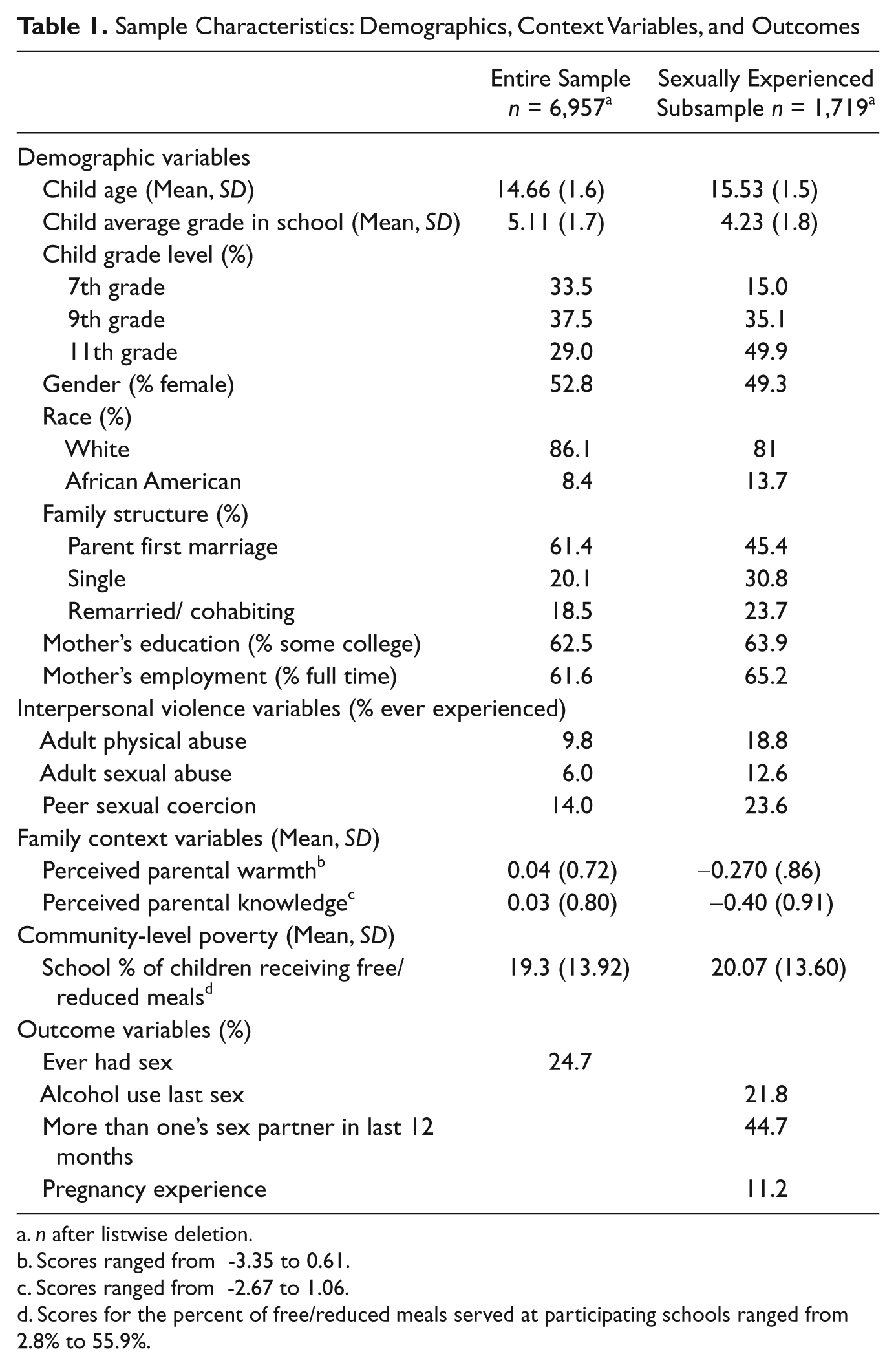
n after listwise deletion.
Scores ranged from -3.35 to 0.61.
Scores ranged from -2.67 to 1.06.
Scores for the percent of free/reduced meals served at participating schools ranged from 2.8% to 55.9%.
Measures
Sexual behavior and risk taking
Four sexual behavior variables were assessed with one question each; responses were dichotomized with one indicating a positive response to each behavior and zero indicating a negative response. Adolescents reported (a) if they had experienced first intercourse, (b) if they had ever been pregnant or caused a pregnancy, (c) whether they or their sexual partner had used alcohol or other drugs (AOD) at last sexual intercourse, and (d) the number of sexual partners within 12 months of surveying. For parsimony, we dichotomized the last variable: 0 = lower sexual risk (0-1 partners within the last year) and 1 = higher sexual risk (2 or more partners within the last year). See Table 1 for descriptive statistics (percentages, means, standard deviation scores) for this variable and those described below.
Violent relational contexts
One item asked participants if they had experienced adult physical abuse; one item asked participants if they had experienced adult sexual abuse. Definitions were provided on the survey for sexual and physical abuse “(sexual abuse is when someone in your family or another person does sexual things to you or makes you do sexual things to them;” physical abuse “(e.g., beat up, hit with an object, kicked, or some other form of physical force.)” A third item asked participants if they had experienced peer sexual coercion “Have you ever been made to do something sexual that you didn’t want to do by another teenager?” Response choices described types of coercive behavior ranging from never (0), unwanted kissing (1), unwanted kissing and touching (2), to unwanted kissing, touching, and sexual intercourse (3). For the multivariate analyses, each measure was dichotomized (0 = never, 1 = current or past experience).
Parenting processes
Parental warmth was assessed with a three-item measure of adolescents’ perception of their relationship with each parent (e.g., my mother/father is there when I need her/him, my mother/father cares about me, my father/mother trusts me) adapted from Armsden and Greenberg’s (1987) Parent–Adolescent Attachment Inventory. Responses ranged from 0 (never) to 4 (very often). Items were z scored and summed, with higher scores representing a higher level of perceived parental warmth (α = .86 for mothers and fathers together; nonstandardized scale scores ranged from 0 to 4, M = 3.32, SD = .83.) Four items assessed adolescents’ perception of how well their parent(s) know what they were doing after school, how they spent their time, where they were when out at night, and the parents of their friends (parental knowledge, α = .84). Responses on a 5-point scale from 0 (never) to 4 (always) were standardized and then summed, with higher scores indicating higher levels of knowledge (nonstandardized scale scores ranged from 0 to 4, M = 2.91, SD = .90).
Community-level poverty
Community poverty was calculated as the percentage of children who received free and reduced lunch at each participating school. Percentages were derived from school district reports by school for the year of surveying. Because the school breakfast and lunch program is a means-tested program based on family income level, and because schools are nested within communities, the economic demographics of a school population is a proxy measure of the level of poverty within the community. Community poverty is the only variable assessed at the school level, and is entered into the hierarchical model as a Level 2 predictor.
Control variables
Demographic variables known to be associated with both the predictors and the outcomes were controlled for in the multivariate analyses. Most variables were dummy coded with scores of 1 indicating a participant was positive for that characteristic. Family structure (single parent, and step or cohabiting parents), race (African American), mother’s education (some college) and gender (female) were entered into the multilevel logistic regression equations as categorical variables. First married, White, and having less than some college education were the comparison groups. Students reported their age in years and reported their average academic grade (see Table 1).
Analyses
To provide an overall picture of associations we first ran Pearson’s correlations and Chi-square analyses. We conducted t test to test Hypothesis 1 that differences in risk factors and risky behaviors would differ by community poverty level. To test Hypothesis 2, that risk factors of interpersonal violence, ineffective parenting, and higher community poverty would be associated with increased sexual-risk behavior, we utilized multilevel modeling with the MPLUS data analysis program. This allowed us to examine the relative contributions of school-level poverty as well as individual- and family-level factors (experiences of violence and parenting), in predicting the probability of onset of sex (entire sample), and use of alcohol during sex, number of partners, and experience of pregnancy (sexually active subsample). Individuals were clustered by schools, and the variability between schools was first estimated and then predicted with school-level poverty (see Table 3, row 2). Analyses of individual predictors for the sexual outcomes all controlled for the variability between schools and the levels of poverty at each school. We used multivariate logistic regression to account for the binomial outcome variables (alcohol before sex, multiple sex partners, pregnancy). For each logistic regression, the Level 2 predictor was community poverty. Level 1 variables included our demographic control variables, the interpersonal violence variables (adult physical abuse, adult sexual abuse, and teen sexual coercion), and family context variables (parental warmth and knowledge). Level 1 variables were entered in one block.
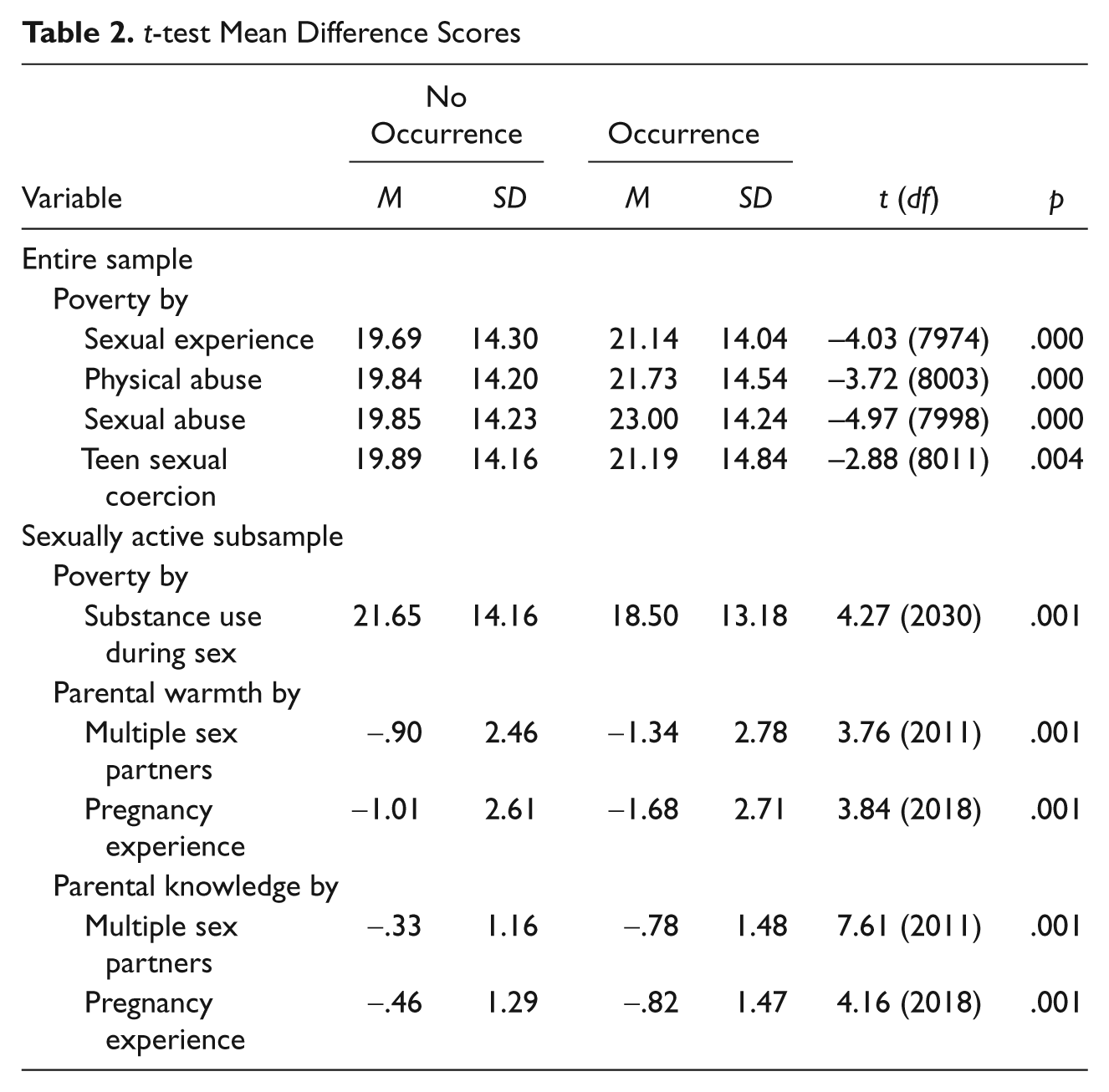
t-test Mean Difference Scores
Multilevel Predictors of Sexual Risk-Taking Behaviors
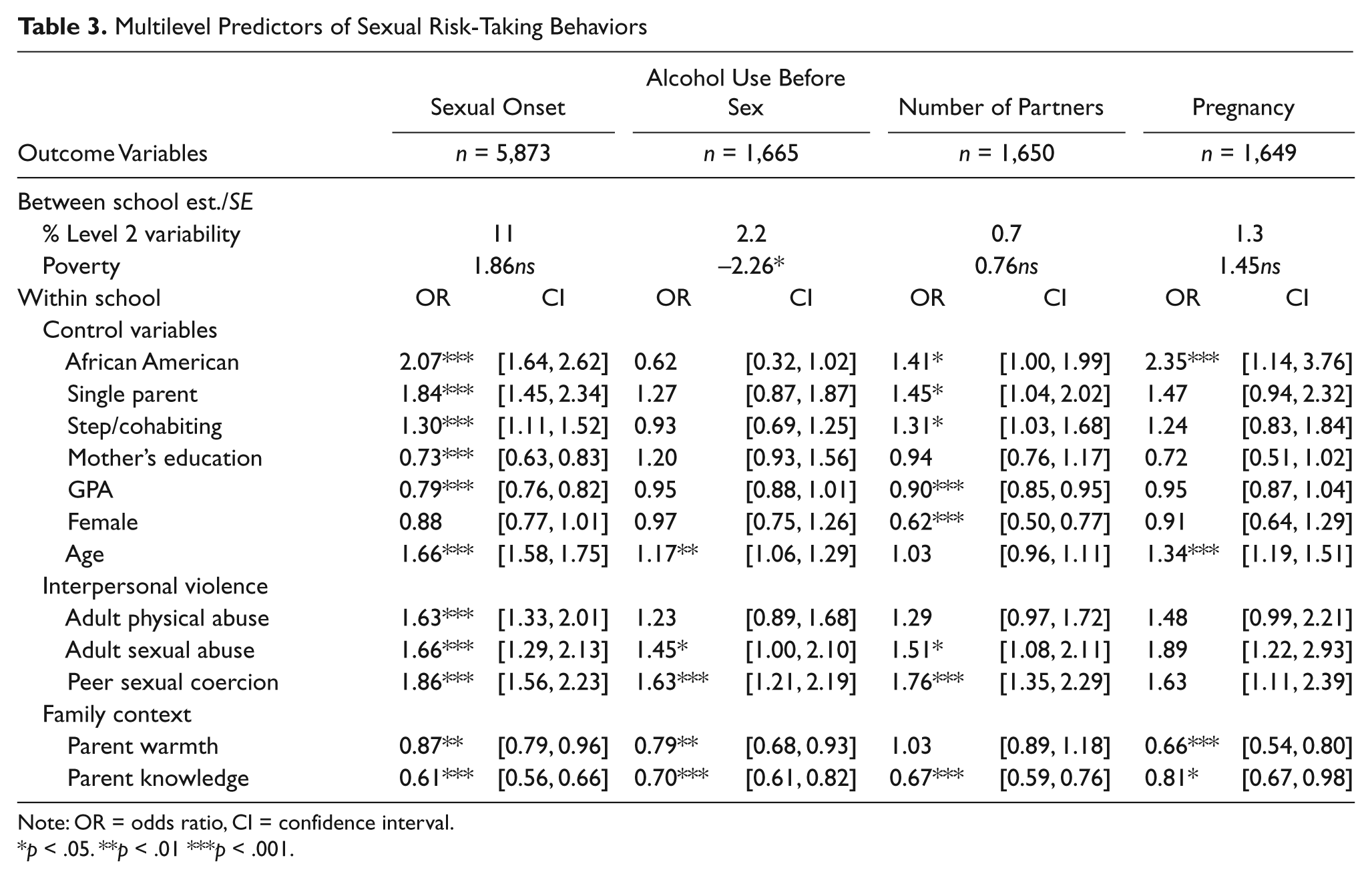
Note: OR = odds ratio, CI = confidence interval.
p < .05. **p < .01 ***p < .001.
Results
Bivariate correlations run with the entire sample revealed a strong positive association between parental knowledge and parental warmth (r = .46, p < 001), and a weak correlation between parental warmth and community-level poverty (r = –.11, p < .001).
Chi-square tests revealed significant associations among types of violence experiences: students who had experienced one type were more likely than expected to report each other type. Associations for all combinations of the three types of violence were significant and ranged from χ2(7,972-7,989) = 125 to 242, with all p < .001. Types of risk outcomes were also associated: students who had experienced one type were more likely than expected to report each other type of risk behavior. Associations for all combinations of the three types of sexual risk were significant and ranged from χ2 = 62 to 295, with all p < .001. All three types of violence were associated with all three types of risk taking. In each case, reporting any type of violence was associated with more than expected report of any type of risk behavior. Physical and sexual abuse and sexual coercion were associated with increased likelihood of AOD use during sex, having more than one sex partner, and having had or caused a pregnancy. Associations for all combinations of the three types of risk behaviors were significant and ranged from χ2 = 15 to 110, with all p < .01.
The t tests conducted with the entire sample revealed that adolescents who attended schools with a higher percentage of poor students were more likely to be sexually experienced and to have experienced any form of personal violence (see Table 2). Within the sexually active subsample, t tests revealed differences in sexual risk taking and family variables among youth who attended schools with a higher versus lower percentage of poor students (i.e., higher versus lower community poverty). Among sexually experienced youth, those living in poorer communities reported fewer instances of substance use during sex; sexually experienced teens who perceived parents to be less emotionally warm and less knowledgeable about their behaviors reported having more sexual partners and a prior pregnancy (see Table 2).
The multilevel intraclass correlations for each of the risk behavior variables revealed that Level 2 variability was strongest for onset of sexual intercourse at 11%. The risk behaviors among sexually experienced youth accounted for less variability at Level 2, in part because the threshold of onset of intercourse had to be met before individuals were included in analyses about other risk behaviors. For number of sex partners in the last 12 months, 7% of variability was accounted for at Level 2; for AOD use during sex 2.2% was accounted for at Level 2, and for pregnancy 1.3% was accounted for at Level 2. Although the percents were low for sexual risk variables, because they were significant for AOD use and onset of intercourse, we retained community poverty as a Level 2 predictor of sexual risk taking in subsequent analyses.
The multilevel multivariate logistic regression analyses revealed that, after controlling for demographic variables, community poverty at Level 2 negatively predicted AOD use during sex only (see Table 3). For onset of sexual intercourse, almost all Level 1 control variables were significant in the direction expected. An odds ratio greater than 1 indicates a greater risk of onset associated with higher levels of the given predictor variable. An odds ratio of less than one indicates a lower risk of onset associated with greater levels of the predictor variable. For example, African Americans were twice as likely to have experienced onset of intercourse as Whites while controlling for all other factors. The control variables marginally predicted the risk behavior variables but were still generally in the expected direction. The exception was in the case of number of partners, where most of the control variables were significant in the expected direction.
As seen in Table 3, the odds of having initiated intercourse increased for youth who experienced any form of interpersonal violence. The odds of having used substances at last sex or having multiple sexual partners significantly increased with a history of adult sexual abuse or peer sexual coercion. Individuals with stronger family contexts generally reported less risky behaviors. Greater parental warmth and parental knowledge reduced the odds of onset of sexual intercourse, AOD use during sex, and pregnancy history. Greater parental knowledge also reduced the odds of having multiple sexual partners.
Discussion
In conducting this research, we were interested to know how experiences of interpersonal violence, parenting, and community poverty independently and collectively contribute to adolescent behaviors that put teens at risk for STIs or pregnancy. Our findings support the proposed hypotheses and suggest the relative importance of violence experiences and parenting over community poverty as predictors of sexual risk taking. Efforts to reduce pregnancy and sexually transmitted infections among adolescents have tended to focus on proximal indicators of sexual risk taking such as building specific skills (e.g., use of condoms) and sexuality knowledge (Kirby et al., 2007). The results from our study suggest that interventions to prevent interpersonal violence and improve parenting may be particularly useful to reduce sexually risky behavior among adolescents. Such efforts include educating preteens and adolescents to identify and disavow sexual coercion within romantic relationships as well as increased efforts and vigilance to reduce child abuse. Given the prevalence of dating violence among teens (Eaton et al., 2007; Finkelhor et al., 2009; Young & Furman, 2008) programs to reduce dating violence can be especially useful to reduce negative sexual outcomes and thus promote resiliency of youth from all communities, including those in who live in poverty. Alcohol and other drug prevention programs are also important for increasing teens’ awareness of sexual risks by emphasizing increased risk for sexual violence and loss of sexual agency when alcohol and other substances are used.
As was similarly reported in earlier research (Parillo et al., 2001; Trent et al., 2007; Viosen, 2005), our results indicate that interpersonal violence experiences were strongly predictive of behaviors that increase teens risk for STIs or pregnancy, even after accounting for poverty, demographic variables, and parenting processes. For most outcomes, experienced violence increased the odds of sexual risk taking by 150% to 200%. It is plausible that adolescents who have experienced abuse may look to sexual partners for intimacy (Young & Furman, 2008) or may use alcohol or other drugs to self medicate. Either of these coping strategies can increase the vulnerability of youth who have experienced sexual violence for health-compromising sexual behaviors. Alternatively, it is possible that our risk behavior outcomes may be a function of sexual coercion by peers. As noted by other researchers, use of alcohol or other drugs or having multiple sexual partners increased the odds of adolescent dating victimization, particularly for girls (Eaton et al., 2007; Grover, 2004). In all likelihood, these processes of violence and risk are mutually influencing and require long-term longitudinal data to tease apart.
Consistent with other research, adolescents’ perceptions of parents as warm and knowledgeable were associated with taking fewer sexual risks, even when accounting for the effects of community poverty, demographics, and violence experiences (e.g., Crosby et al., 2003; DiClemente et al., 2007; Huebner & Howell, 2004). These findings lend support to the value of positive parenting in promoting adolescent sexual health. Regardless of community income levels, youth who have warm and knowledgeable parents are less likely to engage in risk behaviors that increase their odds for STIs or a first or second pregnancy.
Finally, community poverty was associated with sexual onset in bivariate analyses, but contrary to previous research (e.g., Baumer & South, 2001), the multivariate analyses revealed no direct association between community poverty and sexual onset, having multiple sexual partners or pregnancy. Our results are consistent with recent research (Dupere et al., 2008) in that poverty itself was not the most important contributing factor to sexual onset or other sexual risk behaviors. Counterintuitively, living in a poor community predicted fewer episodes of substance use at last sex. This may be in part because youth in poor communities may have less disposable income to spend on alcohol or other substances.
Accounting for community poverty at Level 2 (the school level) is important to understand how proximal and distal factors within the social ecology can influence sexual risk taking. Unfortunately, the relatively young age of our sample and the behavioral risk outcomes (which are developmentally advanced) contributed to a washout of Level 2 effects among sexually experienced adolescents. A wider array of community-level poverty measures or an older age range of youth might alleviate this problem in other samples.
Because our data are crossectional, readers are cautioned against making causal inference from the results. Reporting of sexual or nonsexual abuse is retrospective and may therefore be biased. Other scholars have argued, however, that youth are unlikely to forget traumatic violent events (Trent et al., 2007). There is also the possibility that reported peer sexual coercion could inflate the sexual risk outcomes. To test for this, we conducted crosstabs analyses (peer sexual coercion X multiple sexual partners and occurrence of pregnancy). Of the 957 sexually experienced adolescents who indicated they had two or more sexual partners in the last year, 137 (14%) also reported peercoerced sexual intercourse. Among the 277 sexually experienced adolescents who reported experiencing pregnancy, 61 (22%) also reported peercoerced sexual intercourse at some time. Thus the majority of students (78%-86%) did not experience multiple partners or pregnancy resulting from peer sexual coercion. Our measure of sexual onset was indicated by “voluntary” sex. We are therefore confident that most reports of onset did not coincide with adolescent sexual coercion. Longitudinal research is needed to fully determine the directionality of adult abuse and teen sexual coercion and the sexual risk taking outcomes, but our findings are one step toward better understanding these associations.
Our measure of poverty has both strengths and weaknesses. Because we do not measure poverty at the individual level (e.g., personal/family poverty), we cannot make inferences about how personal experiences of poverty relate to interpersonal violence, family processes, or sexual risk. We are however, able to examine individual and family risk and protective factors within a broader context of poverty—that which is indicated by the degree of poverty within the school that youth attend daily. We assume that the percentage of poor youth within a school reflects the social context of their community.
Few studies of violence and sexuality among teens account for broad-level community factors using a nested design (Level 2 modeling). This series of analyses suggests that the context of community poverty is important to onset of sexual intercourse, but that once youth have crossed the threshold of virginity, other factors such as parenting practices, and violence experiences especially, contribute to sexual risk-taking behaviors more so than poverty itself. Reduced exposure to violence and improved parenting strategies are two important avenues to address concerns about adolescent sexual risk taking. Parents who know their child’s behaviors and whereabouts, and who can maintain a relationship that is perceived by teens as supportive can be better prepared to protect their children from violence experiences and risky sexual behavior. Prevention programs that enhance parenting skills and work to reduce violence experiences can complement current school-based sexuality education programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.