
Abstract
Unfortunately, the number of bank robberies is increasing and little is known about the subsequent risk of posttraumatic stress disorder (PTSD). Several studies have investigated the prediction of PTSD through the presence of acute stress disorder (ASD). However, there have only been a few studies following nonsexual assault. The present study investigated the predictive power of different aspects of the ASD diagnosis and symptom severity on PTSD prevalence and symptom severity in 132 bank employees. The PTSD diagnosis, based on the three core symptom clusters, was best identified using cutoff scores on the Acute Stress Disorder scale. ASD severity accounted for 40% and the inclusion of other risk factors accounted for 50% of the PTSD severity variance. In conclusion, results indicated that ASD appears to predict PTSD differently following nonsexual assault than other trauma types. ASD severity was a stronger predictor of PTSD than ASD diagnosis.
The number of bank robberies is increasing in Denmark and most of the Western world, which places the employees at increased risk of exposure to one or multiple robberies (Gilioli, Campanini, Fichera, Punzi, & Gassitto, 2006; The Danish Bankers Association, 2011). During a bank robbery, the employees are threatened with violence and/or held at gun point while being told to hand over cash. Research on the psychological sequelae of robberies at the workplace (Elklit, 1999, 2002; Richards, 2000) and particularly research on bank robberies is limited (Hansen & Elklit, 2011; Miller-Burke, Attridge, & Fass, 1999). However, the few existing studies generally show that robberies at the workplace seem to be a traumatic event associated with both immediate and long-term posttraumatic symptoms. Despite this knowledge, only a few studies have sought to identify victims of bank robberies at risk of developing posttraumatic stress disorder (PTSD; Kamphuis & Emmelkamp, 1998; Miller-Burke et al., 1999), and thereby facilitate early treatment and a reduction in the large costs associated with PTSD (Litz & Maguen, 2007). The acute stress disorder (ASD) diagnosis was introduced into the Diagnostic and Statistical Manual of Mental Disorders (4th ed. [DSM-IV]) with the purpose of recognizing posttraumatic stress occurring within the 1st month after a trauma and identifying victims at risk of developing PTSD (American Psychiatric Association, 1994). Like PTSD, ASD is defined in the DSM-IV as a disorder that follows experiencing, witnessing, or being confronted with an event that involves death, physical injury, or a threat to the physical integrity of self or others (criterion A1), in which the individual reacts with feelings of fear, helplessness, and intense horror (criterion A2). The main difference between the ASD and the PTSD diagnostic criteria besides from duration of disturbance, is that the ASD diagnosis requires three dissociative symptoms (criterion B), whereas the PTSD diagnosis does not. Like PTSD, the ASD diagnosis also involves reexperiencing (criterion C), avoidance (criterion D), and arousal (criterion E) symptoms. However, as pointed out by Bryant and Harvey (1997), these ASD symptom clusters differ from the PTSD symptom clusters in several ways. In contrast to the PTSD diagnosis, the ASD diagnosis does not require that reexperiencing causes or involves involuntary distress. In relation to arousal and avoidance, the ASD diagnosis only states a diffuse requirement of marked arousal and avoidance, whereas a PTSD diagnosis requires the presence of at least three symptoms of avoidance and two symptoms of arousal. Furthermore, both the PTSD and ASD diagnoses require functional impairment (criterion F).
According to Bryant’s (2011) systematic review, 22 studies have investigated the ability of ASD to predict the development of PTSD in terms of sensitivity, specificity, and positive and negative predictive power following different types of traumatic exposure. However, none of these studies were conducted following a bank robbery. Bryant’s (2011) review showed that there was variability in the predictive power of the ASD diagnosis across trauma types and that the studies varied in inclusion and assessment criteria, which may have biased the results. However, the majority of studies generally found high negative predictive power (NPP; i.e., most participants without ASD did not develop PTSD) and specificity (i.e., most participants without PTSD did not initially meet criteria for ASD). Furthermore, most of the studies found that at least half of the trauma victims suffering from ASD developed PTSD (i.e., high positive predictive power; PPP). However, most of the studies showed that the majority who developed PTSD did not initially suffer from ASD (i.e., low to moderate sensitivity; Bryant, 2011). According to Bryant’s (2011) review, seven of the studies indicated that the low sensitivity was attributed to a high percentage of victims suffering from subclinical ASD (i.e., an ASD diagnosis without dissociation). The predictive power of the ASD diagnosis in terms of sensitivity therefore appears to be limited by the dissociation criterion. Bryant (2011) concluded that if the goal is to identify victims who will benefit from treatment then the present definition of ASD is overly restrictive. This is because the presence of three rather than four symptom clusters, in acute distressed victims, identifies more victims who develop PTSD. Notably however, Bryant’s (2011) review mainly included studies of motor vehicle accidents (MVA), injury, and disaster.
Bryant’s (2011) review only included two studies of nonsexual physical assault (Brewin, Andrews, Rose, & Kirk, 1999; Elklit & Brink, 2004) and one study of sexual assault (Elklit & Christiansen, 2010). Ozer, Best, Lipsey, and Weiss’s (2003) and Brewin, Andrews and Valentine’s (2000) meta-analyses of risk factors of PTSD showed that the ability of several different investigated risk factors to predict PTSD varies between trauma types. Therefore, it may make little sense to compare studies of victims of nonsexual assault with victims of sexual assault. Indeed, studies have shown that there are different PTSD risk factors in female victims of sexual and nonsexual assault (Acierno, Resnick, Kilpatrick, Saunders, & Best, 1999). This also seems to hold for the predictive power of ASD, because in contrast to Elklit and Christiansen’s (2010) rape study, both studies of nonsexual assault (Brewin et al., 1999; Elklit & Brink, 2004) found that combinations of the ASD symptom clusters, including dissociation, improved the prediction of PTSD. Furthermore, in contrast to Bryant’s (2011) review the two studies of nonsexual assault found high sensitivity and high PPP. According to Brewin et al. (1999) the best overall classification of PTSD was obtained by a combination of the A2, B, C, D, E, and F ASD symptom clusters with both sensitivity and PPP of 57%. Contrary to Brewin et al. (1999), Elklit and Brink (2004) found that the A2 and F criteria did not improve correct PTSD classification, and that the overall best model of correct PTSD classification was obtained by the combination of the four ASD symptom clusters (B, C, D, and E) with high PPP (52%) and high sensitivity (80%). Combined, the two studies of nonsexual assault suggest that ASD may be a better predictor of PTSD following nonsexual assault compared with sexual assault, MVA, injury and disaster. The results of both Elklit and Brink’s (2004) and Brewin et al.’s (1999) study may, however, be biased by the lack of a reliable ASD measurement. Indeed, both studies assessed ASD using PTSD measures. At the same time, it is unknown whether the results can be generalized to workplace violence.
To summarize, research indicates that ASD predicts PTSD differently across trauma types. Thus, it seems that the ASD diagnosis cannot identify victims at risk of developing PTSD following all traumatic exposure as proposed in the DSM-IV. However, ASD does appear to predict PTSD relatively well following nonsexual assault, but this has not been investigated in relation to violence at the workplace. The present proposal for ASD in the DSM-5, states that ASD should be limited to describing severe acute stress responses independently of PTSD (Bryant, Friedman, Spiegel, Ursano, & Strain, 2011). Despite this proposal it is important to thoroughly investigate how well ASD predicts PTSD after nonsexual assault. Important, as it appears that ASD may still be useful for identifying victims at risk of developing PTSD following nonsexual assault.
The aim of the present study was to explore the prevalence of PTSD following bank robbery and to assess the predictive power of different aspects of the ASD diagnosis on the PTSD prevalence. To more fully explore the nature and strength of the relationship between ASD and PTSD following bank robbery, we also wanted to explore how well ASD severity predicts PTSD severity before and after controlling for other known PTSD risk factors. The risk factors were selected based on previous studies of robberies and nonsexual assault (Brewin et al., 2000; Elklit, 1999, 2002; Hansen & Elklit, 2011; Kamphuis & Emmelkamp, 1998; Miller-Burke et al., 1999; Ozer et al., 2003). The selected pretrauma risk factors were gender, age, prior traumatic exposure, and prior robberies. The selected peri-trauma risk factors were presence during the robbery, perceived helplessness, and perceived life threat. The selected posttrauma variables were perceived social support, and perceived safety.
Based on the existing studies of nonsexual assault (Brewin et al., 1999; Elklit & Brink, 2004), we hypothesized the following. The combination of the four ASD symptom clusters (B, C, D, and E) would result in better classification of PTSD compared with other combinations of the B, C, D and E ASD symptom clusters. It is unknown whether the A2 criterion and the use of Bryant and Harvey’s (2002) cutoff scores will improve the predictive power of ASD on PTSD. Furthermore, we hypothesized that the PPP, the NPP, the sensitivity, and the specificity of ASD on PTSD would be high. In addition, due to existing research in relation to risk factors of PTSD, we expected younger age, female gender, prior traumatic exposure, prior robberies, presence during the robbery, perceived helplessness, perceived life threat, and ASD severity to be positively associated with PTSD severity. We expected perceived social support and perceived safety to be negatively associated with PTSD severity. We also expected ASD severity alone to be a significant predictor of PTSD severity, and that the best model explaining PTSD severity would be a combination of risk factors and ASD symptom severity. However, it was unknown whether ASD severity would be a significant predictor of PTSD, when the other variables are controlled for.
Method
Participants and Procedure
The present study is a follow-up study of Hansen and Elklit’s (2011) bank robbery study. A total of 132 bank employees, employed at 28 different banks, that were exposed to bank robberies filled out two questionnaires between 48 hr to 1 week after a robbery (T1) and at 6 months after the robbery (T2). At T1, all employees (N = 199) received the questionnaire, and 76.4% of the employees filled out the questionnaire (N = 152). At T2, 86.8% of the 152 participants from T1 (n = 132) filled out the questionnaire. A total of 94 participants (71.2%) were present during the robbery, 22 participants (16.7%) were at work during the robbery, and 16 participants (12.1%) were not at work during the robbery. As argued in Hansen and Elklit (2011) we assume that the stressor criterion A1 is met during a bank robbery, because a bank robbery involves actual or threatened death or serious injury or a threat to the physical integrity of self or others. Furthermore, we argue that the A1 criteria is met regardless of the whereabouts of the participants during the robbery, because the participants experienced, witnessed, or were confronted with the robbery through colleagues who directly experienced a bank robbery (A1). In addition, about half of the participants (54.5%, n = 72) received psychological debriefing the same day or the day after the robbery. The debriefing was not part of the present study. For more details about the design of the study, please see Hansen and Elklit (2011).
Measures
The questionnaire included questions related to demographic factors. The experience of perceived helplessness, fear of dying, and perceived life threat during the robbery were assessed dichotomously (yes or no) at T1. This measurement has been used previously (cf. Elklit, 1999; Elklit & Christiansen, 2010). Presence during the robbery was assessed dichotomously at T1 by asking the participants, if they had been present during the robbery (yes or no). Perceived safety was assessed at T1 by asking the participants, in the immediate aftermath of the robbery, if they had feared for their own safety during the robbery. Answers were scored on a 7-point Likert-type scale (1 = no, not at all, 7 = yes, very much). Thus, a high score indicated low perceived safety. The scores on perceived safety were reversed in the analyses to simplify the results. Prior traumatic exposure was assessed at T1 by asking the participants whether they had experienced 14 different kinds of traumas applied in the U.S. National Comorbidity Survey (cf. Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995) with a separate scoring of prior robberies.
ASD severity was assessed at T1 using the Danish version of the Acute Stress Disorder scale (ASDS; Bryant, Moulds, & Guthrie, 2000). The ASDS was developed to identify ASD and predict PTSD. The ASDS includes 19 items with four subscales assessing the four separate ASD symptom clusters of dissociation, reexperiencing, arousal, and avoidance. These are the present subscales employed in the DSM-IV. Responses are scored on a 5-point Likert-type scale (1 = not at all, to 5 = very much). The Cronbach’s alpha values were satisfactory (subscales = .84-.92, total score = .95). ASD was assessed according to the DSM-IV in the following ways. The subjective stressor criterion A2 was met if the participants reported fear of dying or helplessness during the robbery. The ASD symptom clusters were met if the participants reported at least one reexperiencing symptom, one avoidance symptom, and one arousal symptom in addition to at least three dissociative symptoms—indicated by item scores ≥3 on the ASDS. This procedure has been used previously (cf. Elklit & Christiansen, 2010). Furthermore, ASD was assessed using Bryant and Harvey’s (2002) recommended cutoff scores. According to Bryant and Harvey (2002) the cutoff scores for diagnosing ASD from the ASDS is scores ≥9 on the dissociation subscale total and ≥28 on the total scores for reexperiencing, avoidance and arousal. The recommended optimal cutoff scores for predicting PTSD from the ASDS are scores ≥56 (Bryant & Harvey, 2002).
PTSD severity was assessed at T2 using the Danish version of the Harvard trauma questionnaire part IV (HTQ; Mollica et al., 1992). The HTQ was developed to identify PTSD based on all 17 items assessing the three PTSD symptom clusters (intrusion, arousal, and avoidance) in the DSM-IV. The answers are scored on a 4-point Likert-type scale (1 = not at all, to 4 = all the time) with item scores ≥3 indicating symptom presence. The Danish version of the HTQ has been used in a wide range of Danish trauma populations with reports of good reliability and validity (cf. Bach, 2003; Elklit & Brink, 2004; Elklit & Christiansen, 2010). The Cronbach’s alpha values were satisfactory (subscales = .84-.89, total score = .94). The HTQ was also used to diagnose PTSD by following the DSM-IV’s diagnostic criteria. The diagnosis for PTSD was met if the participants reported at least one intrusion symptom, three avoidance symptoms, and two arousal symptoms. This procedure has been used previously (cf. Elklit & Christiansen, 2010).
Perceived social support was assessed at T1 using the Danish version of the Crisis Support scale (CSS; Joseph, Andrews, Williams, & Yule, 1992) which is comprised of seven items. The first five items are related to positive social support, item six is related to feeling let down by others, while the last item assesses social support satisfaction. The answers are rated on a 7-point Likert-type scale (1 = never, to 7 = always on the first six items, and 1 = very unsatisfied, to 7 = very satisfied on the last item). A total score was calculated by adding scores on all seven items. The CSS has been shown to have good reliability and validity (Elklit, Pedersen, & Jind, 2001; Joseph et al., 1992). The Cronbach’s alpha value was satisfactory (total score = .75).
Results
Prior to data analysis the data was screened for errors. The percentage of missing values was small (0.8%-4.5%). Thus, the missing data was imputed with the expectation maximization (EM) algorithm. The EM algorithm is a demonstrated effective method of dealing with missing data (Bunting, Adamson, & Mulhall, 2002).
Descriptives
A χ2 test of independence was conducted to explore the difference between the three groups of participants (Group 1: present during robbery, Group 2: at work but not present during the robbery, Group 3: not at work) on estimated ASD and PTSD prevalence. There were no significant differences between the three groups and estimated PTSD prevalence, χ2 (2, 132) = .89, p = 1.000. However, there was nearly a significant difference between the three groups and estimated ASD prevalence, χ2 (2, 132) = 6.15, p = .054. A further investigation revealed that the difference between the three groups was due to the difference between Group 1 and 3, χ2 (1, 110) = 2.40, p = .069, and not a difference between Group 2 and 3, χ2 (1, 38) = .00, p = 1.000, or Group 1 and 2, χ2 (1, 116) 1.81, p = .118. Thus, the difference between the three groups and estimated ASD prevalence was not as close to being significant as first assumed (p = .069 and p = .054, respectively). However, to fully assess homogeneity between the three groups and estimated ASD prevalence, we conducted all analyses including the estimated ASD prevalence with all three groups and only Group 2 and 3. This only meant minor differences in the statistical analyses and had no impact on the interpretation, discussion, or conclusion of the results. Thus, the full sample was used. Furthermore, one-way between-groups analysis of variance showed that Group 1 had significantly higher scores on the ASDS (M = 39.02, SD = 15.42) and the HTQ total scores (M = 26.45, SD = 8.77) than Group 2 (ASDS, M = 30.68, SD = 12.88, HTQ, M = 20.95, SD = 5.79) and Group 3 (ASDS, M = 25.88, SD = 11.45, HTQ, M = 19.75, SD = 5.98) respectively, F(2, 131) = 7.28, p = .001 and F(2, 61) 12.11, p < .001. There were no significant differences between Group 2 and 3. Thus, Group 1 could not be treated as being homogenous to Group 2 and 3. Therefore, we assessed and controlled for the effect of being present during the robbery in further analyses concerning ASD and PTSD symptom severity. Only 7 participants (5.3%) feared that they were going to die during the robbery and therefore fear of dying was only used in relation to the A2 criterion in the further analyses.
Furthermore, differences between the debriefed and nondebriefed participants in relation to probable PTSD status and severity were investigated. No significant difference was found in relation to PTSD status, χ2 (1,132) = 1.00, p = 1.000. However, the debriefed participants had significant higher scores on the HTQ (M = 26.40, SD = 8.21) compared with the nondebriefed participants (M = 22.70, SD = 8.38), t(130) = 2.56, p = .012. This difference could reflect a harmful effect of debriefing but is more likely to indicate the tendency of very affected participants to take part in the voluntary debriefing. Thus, distinguishing between the debriefed and nondebriefed participants in any of the further analyses would therefore make little sense and may even bias the results.
Sample Characteristics, ASD, and PTSD Prevalence
Table 1 shows the sample characteristics.
The estimated ASD rate, including the presence of stressor criterion A2, was 14.4% (n = 19) according to the DSM-IV diagnostic criteria and as measured by the ASDS. Table 2 shows the number and percentage of participants meeting the different ASD symptom clusters alone and combined in subclinical ASD (i.e., as meeting only three of the four symptom cluster) and meeting cutoff scores of the ASDS.
Sample Characteristics of Pre-, Peri-, and Posttrauma Variables, and Significance Test of Differences Between the PTSD and the Non-PTSD Group
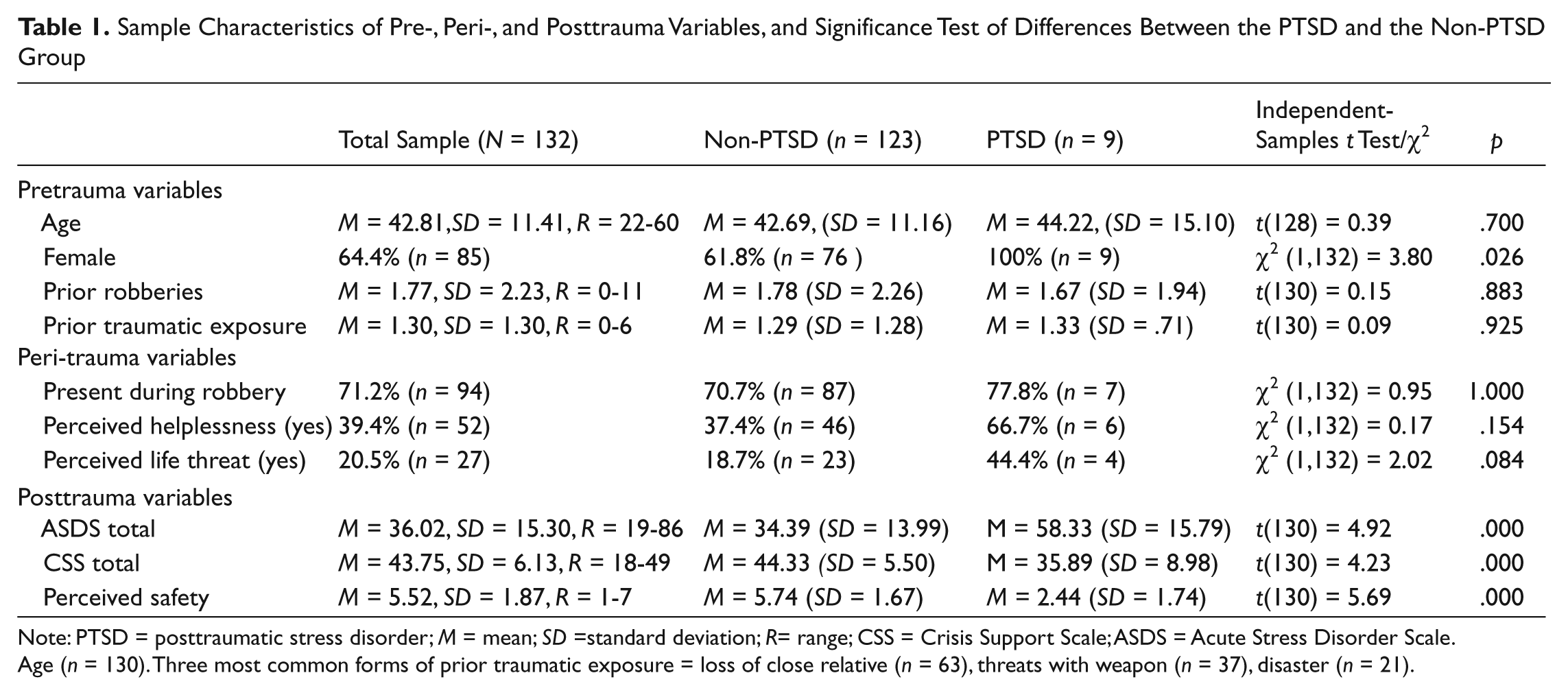
Note: PTSD = posttraumatic stress disorder; M = mean; SD =standard deviation; R= range; CSS = Crisis Support Scale; ASDS = Acute Stress Disorder Scale. Age (n = 130). Three most common forms of prior traumatic exposure = loss of close relative (n = 63), threats with weapon (n = 37), disaster (n = 21).
Classification of PTSD With Different Combinations of the ASD Symptom Clusters, and Cutoff Scores on the ASDS
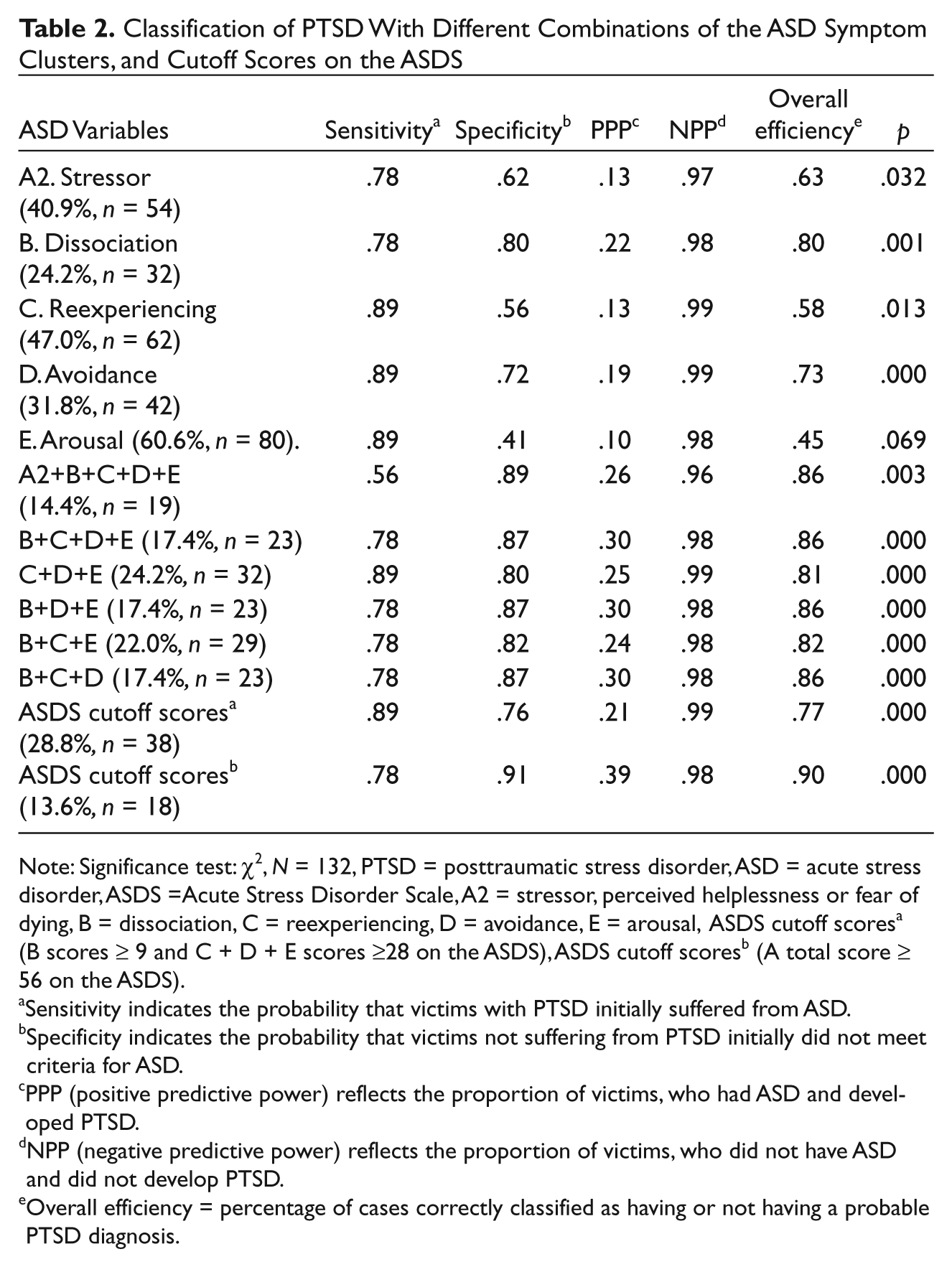
Note: Significance test: χ2, N = 132, PTSD = posttraumatic stress disorder, ASD = acute stress disorder, ASDS =Acute Stress Disorder Scale, A2 = stressor, perceived helplessness or fear of dying, B = dissociation, C = reexperiencing, D = avoidance, E = arousal, ASDS cutoff scoresa (B scores ≥ 9 and C + D + E scores ≥28 on the ASDS), ASDS cutoff scoresb (A total score ≥ 56 on the ASDS).
Sensitivity indicates the probability that victims with PTSD initially suffered from ASD.
Specificity indicates the probability that victims not suffering from PTSD initially did not meet criteria for ASD.
PPP (positive predictive power) reflects the proportion of victims, who had ASD and developed PTSD.
NPP (negative predictive power) reflects the proportion of victims, who did not have ASD and did not develop PTSD.
Overall efficiency = percentage of cases correctly classified as having or not having a probable PTSD diagnosis.
The estimated PTSD rate was 6.8% (n = 9) according to the DSM-IV as measured by the HTQ. Table 1 shows significance tests of differences between the PTSD and non-PTSD participants on pre-, peri-, and posttrauma variables and the ASDS.
Predictors of PTSD
Predicting PTSD from ASD
The performance of the different combinations of ASD symptom clusters and ASDS cutoff scores was assessed in terms of PPP, NPP, sensitivity, specificity and overall efficiency (Baldessarini, Finklestein, & Arana, 1983). Overall efficiency was measured in terms of the percentage of cases correctly classified as having or not having a probable PTSD diagnosis. Significance was established by the χ2 test. Table 2 shows to which extent the different combination of the ASD symptom clusters and the cutoff scores on the ASDS predicted PTSD.
Table 2 generally shows high sensitivity in all the different combinations of ASD symptom clusters and cutoff scores (.56-.89). Specificity varied between moderate and high (.42-.91), whereas NPP was high in all combinations of ASD symptom clusters (.97-.99). PPP tended to be low to moderate (.10-.39). The different combinations of ASD symptom clusters correctly classified more PTSD cases than any of the symptom clusters alone. However, overall correct classification was higher in combinations including the dissociation and avoidance symptom cluster and excluding the A2 criteria. The overall best model for classification of PTSD cases from ASD was obtained with the use of Bryant and Harvey’s (2002) recommended cutoff score for predicting PTSD from the ASDS (sensitivity = .78, specificity = .91, PPP =. 39, and NPP = .98, overall efficiency = .90).
Predicting PTSD severity from ASD severity and pre-, peri-, and posttrauma variables
Preliminary analyses were performed prior to testing the model for predicting PTSD symptom severity. The mutual relationships of the independent variables were investigated in correlation analyses and in relation to the HTQ total score.
Table 3 shows correlation analyses between the pretrauma, peri-trauma, posttrauma variables, the ASDS total score, and the HTQ total score.
Correlations Between Pretrauma, Peri-Trauma, Posttrauma Variables, the ASDS Total, and the HTQ Total Score (Pearson’s r)
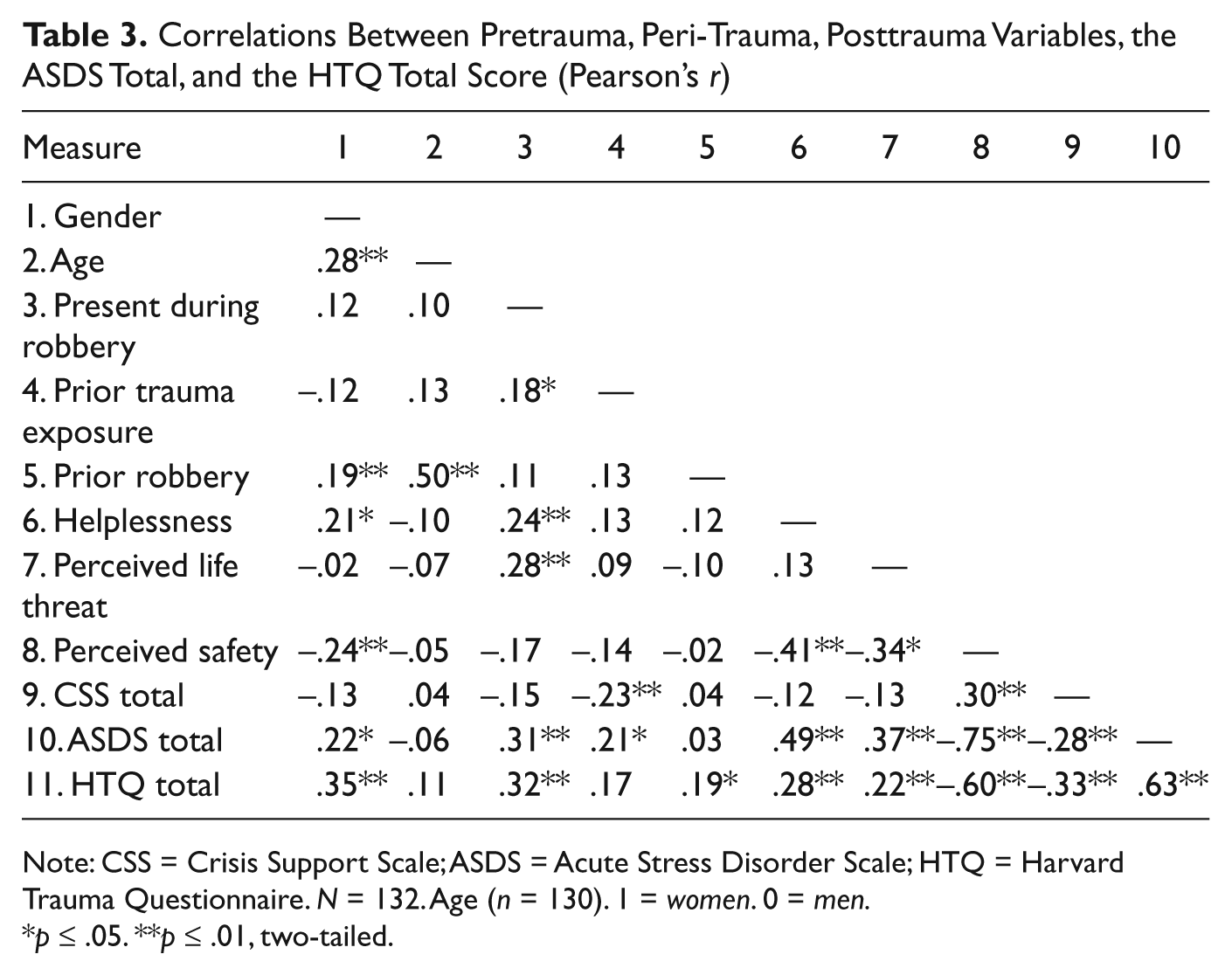
Note: CSS = Crisis Support Scale; ASDS = Acute Stress Disorder Scale; HTQ = Harvard Trauma Questionnaire. N = 132. Age (n = 130). 1 = women. 0 = men.
p ≤ .05. **p ≤ .01, two-tailed.
The distribution of HTQ scores was a close approximation to a normal distribution and thus did not give cause for concern in conducting the regression analysis. Furthermore, there were no problems with multicollinearity (all tolerance values > .10; all VIF values < 10).
Table 4 shows a hierarchical multiple regression analysis of the prediction of the HTQ total score from the ASDS total score and the nine other risk factors. The ASDS total was entered separately at the first step of the model to show its unique contribution.
Hierarchical Multiple Regression Analysis Predicting the HTQ Total Score After Bank Robbery
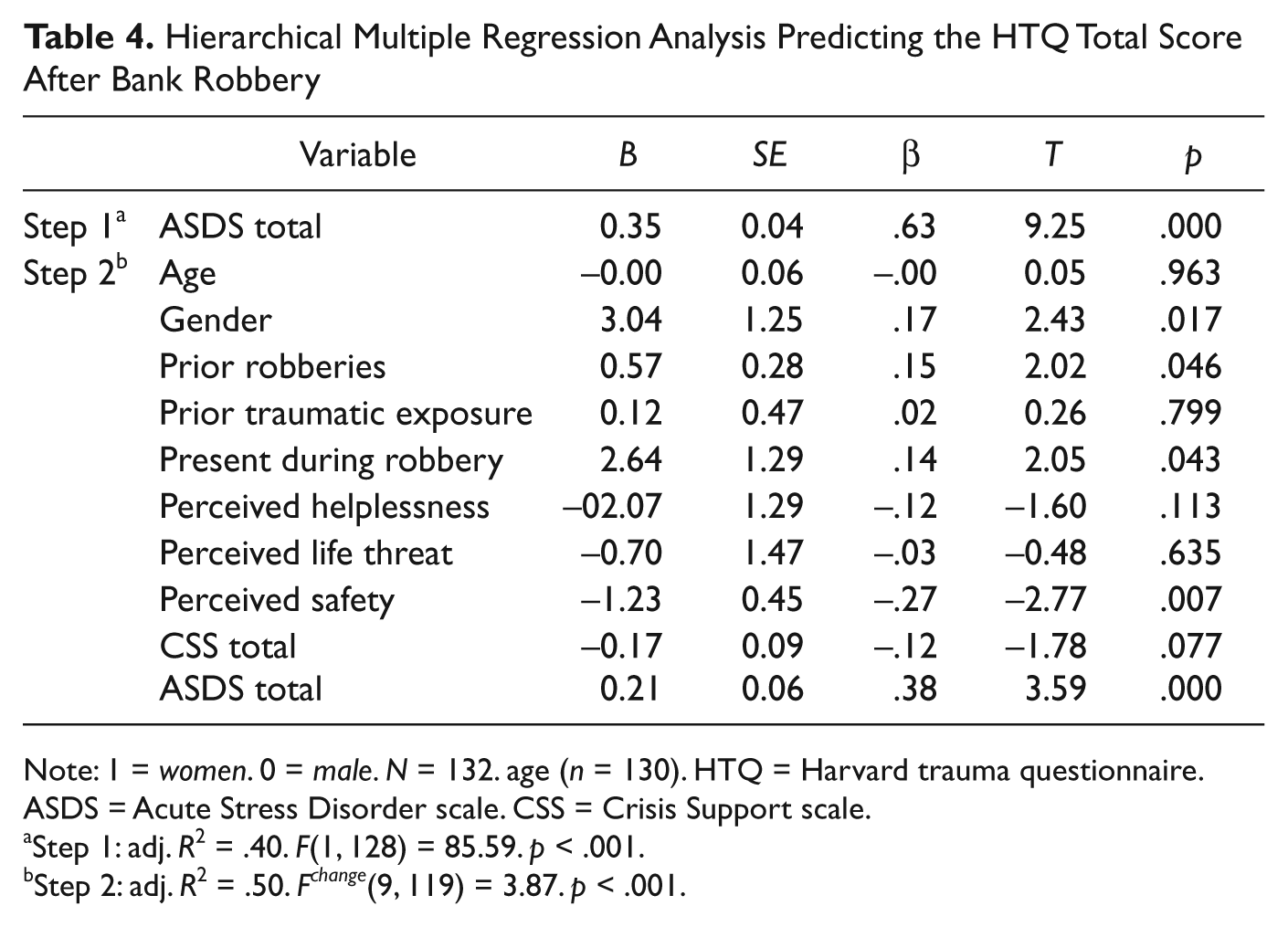
Note: 1 = women. 0 = male. N = 132. age (n = 130). HTQ = Harvard trauma questionnaire. ASDS = Acute Stress Disorder scale. CSS = Crisis Support scale.
Step 1: adj. R2 = .40. F(1, 128) = 85.59. p < .001.
Step 2: adj. R2 = .50. F change (9, 119) = 3.87. p < .001.
Table 4 shows that the ASDS total score alone explained 40% of the variance in the HTQ total score. At the final step of the regression analysis 50% of variance in the HTQ total score was explained by female gender, prior robberies, presence during the robbery, low perceived safety, and a high ASDS total score. The ASDS total score was the strongest predictor (β = .38, p < .001).
Discussion
Estimated PTSD Prevalence
The estimated prevalence of PTSD (6.8%) found in the present study is lower than the PTSD prevalence rates of 20% to 30% found in other studies of robberies and other forms of nonsexual assault (Brewin et al., 1999; Elklit, 1999; Elklit & Brink, 2004). There are several possible explanations for the lower prevalence of PTSD found in the present study. First, bank employees are a special trauma population, as they score relatively low on avoidance symptoms. Attributable to the fact that they have difficulty avoiding the place of the traumatic event (they return to work the day after) as well as difficulty avoiding talking and thinking about the robbery (they are constantly confronted with the robbery from the debriefing and their colleagues etc.). Second, differences in prevalence may be due to the heterogeneity in measurements. Third, it is possible that the differences in ASD and PTSD prevalence may be attributed to the index trauma. Experiencing a bank robbery may be less traumatizing than other forms of nonsexual assault, because violence during a bank robbery is instrumental in being directed toward achieving money and is rarely personally directed toward the employees. Fourth, the low prevalence rates and the decrease in posttraumatic symptomatology could reflect a positive effect of debriefing, because decreases in posttraumatic symptomatology of this size are not found in other studies of nonsexual assault (Brewin et al., 1999; Elklit, 1999, 2002; Elklit & Brink, 2004). Of course, normal remission of posttraumatic symptomatology cannot be ruled out.
Predicting PTSD From ASD
As expected and in accordance with previous studies of nonsexual assault (Brewin et al., 1999; Elklit & Brink, 2004) the combination of the four ASD symptom clusters resulted in a higher correct classification of PTSD compared with the separate symptom clusters. However, combinations of symptom clusters including the dissociation and the avoidance symptom cluster achieved the same PTSD classification as the four ASD symptom clusters combined. The results are mainly in contrast to Bryant’s (2011) review, which concluded that the dissociation symptom cluster limited the predictive power of ASD on PTSD in terms of sensitivity. The removal of the dissociation symptom cluster in the present study improved sensitivity, but at the same time, specificity and PPP were reduced. The DSM-IV definition of ASD may be, as suggested by Bryant (2011), too restrictive in identifying victims at risk of PTSD. However, the present study suggests that this is in relation to the A2 criterion rather than dissociation. Contrary to Brewin et al.’s (1999) study and in accordance with Elklit and Brink’s (2004) study, the A2 symptom cluster did not improve correct PTSD classification in the present study. At the same time, the A2 criterion was weakly associated with the HTQ total score and could not predict the HTQ total score when the other variables were controlled for. Similarly, several studies of various trauma types have suggested that the A2 criterion in ASD does not improve the prediction of PTSD, thus it is recommended that it is removed from the present proposed diagnostic criteria for ASD in the DSM-5 (Bryant et. al., 2011). However, Hansen and Elklit’s (2011) bank robbery study showed that the A2 criterion predicted ASD severity when other variables were controlled for. The A2 criterion therefore seems to serve a function in relation to acute symptomatology but not in relation to long-term symptomatology.
Contrary to our expectations, the different combinations of ASD symptom clusters and cutoff scores resulted in only low to moderate PPP (10%-39%), whereas sensitivity, NPP and specificity were generally high as expected. This means that 61% to 90% of the participants who had ASD would not develop PTSD, whereas the majority of participants with PTSD had suffered from ASD. At the same time, the majority of participants not suffering from PTSD initially tested negative for ASD and the majority of participants without ASD were correctly diagnosed as not having PTSD. The low PPP is likely the result of the low estimated PTSD prevalence rate. It is impossible to achieve high sensitivity, high specificity, high NPP and high PPP, when the prevalence is low (Baldessarini et al., 1983). It is in the best interest of the victims to be offered needed treatment (i.e., high sensitivity). However, in terms of mental health costs it is problematic if too many victims are identified and offered treatment if not needed (i.e., the moderate PPP). Offering too many victims early treatment may, however, still be the most cost-efficient model. Even though many participants did not develop PTSD, the subclinical ASD prevalence rates and the ASDS total score reflect high levels of distress and so early treatment may accelerate their return to normal functioning. In relation to productivity in the bank sector, it therefore seems more profitable to offer too much rather than too little help.
Surprisingly, the overall best correct PTSD classification was achieved using Bryant and Harvey’s (2002) recommended cutoff scores for predicting PTSD from the ASDS. A total severity score of ASD therefore appears to be a better predictor of ASD than differentiation between the symptom clusters. In other words, it appears that when the participants experience a certain symptom level, meeting the individual symptom clusters becomes less important. At the same time, the results indicate that all four symptom clusters need to be represented in the ASD total severity score. This result may not be in contrast to Brewin et al.’s (1999) and Elklit and Brink’s (2004) studies of nonsexual interpersonal assault, because neither of them applied the ASDS and they were therefore not able to assess the cutoff scores. Paradoxically, the results suggest that the present proposal of ASD in the DSM-5, where eight symptoms need to be present, will result in a better prediction of DSM-IV PTSD, even though ASD is proposed as a diagnosis independent of PTSD (Bryant et al., 2011).
Predicting PTSD Severity From ASD Severity and Pre-, Peri-, and Posttrauma Variables
As expected female gender, presence during the robbery, prior robberies, perceived helplessness, perceived life threat, and ASD severity were significantly and positively associated with PTSD severity, whereas perceived social support and perceived safety were significantly and negatively associated with PTSD severity. Contrary to our expectations, age and prior traumatic exposure were not associated with PTSD severity. Furthermore, as expected, ASD severity was a significant predictor of PTSD. However, it was surprising that the ASDS total score alone accounted for 40% of the variance in the HTQ total score. Furthermore, the inclusion of the nine risk factors only improved the explanation of the variance in HTQ total score by 10%. In addition, the ASDS total score uniquely contributed to the explanation of the HTQ total score and was the strongest predictor of the HTQ total score, when all other variables were controlled for. The strong relationship between ASD severity and PTSD severity is in accordance with Bryant and Harvey’s (2002) recommend cutoff scores being the best model for predicting PTSD from ASD in the present study. Both results indicated that the relationship between ASD and PTSD is strong following bank robbery and that ASD severity may be a better predictor of PTSD than the ASD diagnosis.
It is beyond the purpose of this article to thoroughly address the results in relation to the pre-, peri- and posttrauma variables, but some of the results need to be acknowledged and discussed. It is important to note that all the PTSD cases were female. In general, the effect of gender in the prediction of PTSD is found to be small when other risk factors have been controlled for (Brewin et al., 2000; Ozer et al., 2003), but gender can indirectly bias the results by affecting the other risk factors. ASD is found to be a more accurate predictor of PTSD and so showing higher PPP in women. This may be due to dissociation being a more significant predictor of PTSD in women rather than men (Bryant & Harvey, 2003). However, PPP was low in the present study and the ASDS total score uniquely contributed to the explanation of the variance in the HTQ total score when gender was controlled for. Gender may have influenced perceived helplessness, which was the only factor that was significantly correlated with gender and the HTQ total score and was not a significant predictor when gender was controlled for.
The lack of a significant association between prior traumatic exposure and the HTQ total score is likely to be attributed to the fact that the most common prior traumatic exposure in the present study, besides from robberies, was the loss of a close relative. According to Ozer et al. (2003) all trauma types are not necessarily equal in their effect, and therefore the loss of a close relative may often not be as traumatizing as experiencing a robbery in terms of developing PTSD.
The correlation analysis showed a high correlation between the ASDS total score and perceived safety (r = .75, p < .01). However, there were no problems with multicollinearity and both variables uniquely accounted for the HTQ total score when the other variables were controlled for. As argued by Hansen and Elklit (2011), the high correlation does not seem to indicate similarity between the perceived safety item and the ASDS items, because ASD concerns traumatization, whereas perceived safety concerns the sense of present threat.
Limitations
The present study has several limitations. First, the results are based on a convenience sample of bank employees associated with a particular crisis aid service, which may create problems with validity and reliability. Second, there were only a few PTSD cases and all cases were female, which may also have biased the results. Furthermore, the classification of PTSD from the different combinations of ASD may have been affected by the low estimated PTSD prevalence. Third, half of the participants were debriefed, which may have affected the employees’ recovery process either negatively or positively and thus may affect the prevalence rates. Fourth, both the ASD and the PTSD diagnosis were based on self-report measures rather than clinical interviews. Despite both self-report measures being standardized scales assessed according to the DSM-IV, the estimated ASD and PTSD prevalence rates may be biased. Fifth, it was not possible to fully assess the A2 criterion (i.e., intense horror or fear rather than fear of dying), which may have biased the results regarding the role of the A2 criterion. However, studies generally find that only perceived helplessness is associated with PTSD (Bryant, 2011). Finally, the DSM-IV ASD criteria F and H were not assessed and their role in predicting PTSD is therefore unknown.
Conclusion
The present study investigated the role of ASD in predicting PTSD from multiple perspectives. Although ASD does not seem to be able to predict PTSD following all traumatic exposures, as proposed in the DSM-IV, the results suggest that ASD predicts PTSD in a different way following bank robbery than following sexual assault, MVA, injury, and disaster. Despite its limitations, the present study is the only study of bank robberies and nonsexual assault investigating the ASD symptom clusters, cutoff scores, and ASD severity with the use of a reliable ASD measure. The prevalence of ASD was 14.4% and the prevalence of PTSD was 6.8%. The best PTSD classification model was obtained with Bryant and Harvey’s (2002) cutoff score for predicting PTSD from the ASDS with high NPP, sensitivity, specificity, and overall efficiency but moderate PPP. Combined, the results suggest that ASD severity predicts PTSD better than the ASD diagnosis. At the same time, the results suggest that the A2 criterion does not improve correct classification. Thus, the proposed removal of the A2 criterion in the DSM-5 ASD diagnosis (Bryant et al., 2011) does not seem to affect the predictability of ASD on PTSD. Despite the moderate PPP, the ASDS is recommended for screening for PTSD following bank robbery, given that many victims suffering from full or subclinical ASD who exhibit high levels of distress may benefit from early treatment. Future research will need to shed more light on whether the results also hold for other types of nonsexual assault.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.