
Abstract
Advocacy intervention has been shown to be efficacious at reducing depressive symptoms in women who suffer from intimate partner violence (IPV). However, the intervention effect among abused immigrant women has not been well studied. This study compares the demographic and psychosocial characteristics between abused immigrant and nonimmigrant women, and evaluates the impact of immigration status on the efficacy of an advocacy intervention in reducing depressive symptoms and improving perceived social support. Two hundred abused Chinese women recruited from a local community center in Hong Kong were randomized to receive either the advocacy intervention or usual care. The advocacy intervention was found to be effective at reducing depressive symptoms and improving social support for abused Chinese nonimmigrant women, but the same effects were not seen for abused immigrant women. The findings provide essential insights into the need for developing targeted and efficacious advocacy interventions for abused immigrant women. Effective services to address abused immigrant women’s needs were also suggested.
Keywords
Background
Intimate partner violence (IPV) is a serious public health problem. As reported in 48 population-based surveys worldwide, the lifetime prevalence of IPV against women ranges from 10% to 69% (Krug, Dahlberg, Mercy, Zwi, & Rafael, 2002). There is abundant evidence in the literature that IPV is detrimental to physical and mental health (Campbell, 2002) and increases medical utilization and costs (Ulrich et al., 2003). For example, depression is one of the most serious mental health problems among abused women. A meta-analysis found that the pooled prevalence of depression among abused women was 47.6%, which is much higher than the lifetime rate of 18.6% in the general population (Golding, 1999). Further, a more recent study has also shown the risk of depression in abused women was three times of that in nonabused women (Bonomi et al., 2009).
In this article, we use the term “Chinese immigrants” to represent legal immigrants from Mainland China to Hong Kong, that is, those living in Hong Kong for fewer than seven years, while “Chinese nonimmigrants” refers to ethnically Chinese who were born in Hong Kong or who have lived in Hong Kong for at least seven years. Note that the laws of Hong Kong stipulates the official period of living in Hong Kong should be at least seven years to obtain full legal residency. Moreover, “Chinese community” represents all ethnic Chinese residents in Hong Kong, while “immigration status” refers to the status of being a legal resident or being in the process of obtaining full legal residency.
Abused Chinese immigrant women in Hong Kong have been found to have high levels of depressive symptoms (Wong, Tiwari, Fong, Humphreys, & Bullock, 2011). The effects of IPV do not fade even after these women have obtained Hong Kong residency or have stayed in Hong Kong for at least seven years. This motivates the need of investigating the relation between immigration status and IPV.
Hong Kong is a geographically small but densely populated special administrative region of China that had over seven million inhabitants in 2011 (Hong Kong Census and Statistics Department, 2011). Since the First Opium War in 1839, a large number of immigrants have arrived in Hong Kong. Most of them came from Mainland China constituting approximately 30% of the overall population. After the handover of Hong Kong to China in 1997, Article 24(2)(3) of the Basic Law has made people of Chinese nationality born outside Hong Kong to permanent Hong Kong residents entitled to permanent residency in Hong Kong. Moreover, Mainland mothers can also claim residency with their dependent children born from their Hong Kong fathers. Such family reunions have resulted in an influx of immigrants from the Mainland under a quota of 55,000 people each year. According to official statistics, the number of immigrants in Hong Kong increased from 28.5% in 2006 to 37% in 2010 (Home Affairs and Immigration Department, 2011). In particular, the proportion of Chinese immigrants who were young to middle aged women and married in Hong Kong increased from 80% in 2006 to 84% in 2010 (Home Affairs and Immigration Department, 2011).
The rising rate of immigrants has drawn great attention to their needs. Although Chinese immigrants are unable to access the same formal help-seeking opportunities and support services as can local people in Hong Kong including social security assistance, financial assistance for education, and government subsidies for medical fees, the government provides other kinds of formal assistance and support including medical, housing, employment, welfare, and education services. Nevertheless, 59% of new immigrants still find it difficult to adjust to life in Hong Kong and suffer from problems related to employment, living environment, and language barrier (Home Affairs and Immigration Department, 2011). Language can be a particular problem for Chinese immigrants. Even though over 70% of Chinese immigrants understand and speak Cantonese, the primary language in Hong Kong, there remain differences in dialect, pronunciation, slang, and written characters between Mainland Chinese and Hong Kong Chinese (Mo, Mak, & Kwan, 2006).
Being an immigrant has been found to be associated with an increased risk of IPV (Dutton, Orloff, & Hass, 2000). Abused immigrant women’s use of formal help-seeking opportunities, such as police, shelter, and medical services has been found to be lower than that for abused nonimmigrant women (Brabeck & Guzmán, 2009; Rodríguez, Sheldon, Bauer, & Pérez-Stable, 2001). Lack of social support has been identified as being common among immigrants of different ethnicities (Raj & Silverman, 2002; Yoshioka, Gilbert, El-Bassel, & Baig-Amin, 2003). In addition, perpetrators often use the immigration status as a threat to control the women (Dutton et al., 2000). In the United States, the lifetime prevalence of IPV among Chinese immigrant women ranged from 14% (Hicks, 2006) to 61% (Yoshihama, 1999). However, no similar figure has been reported in the general Chinese population.
In the United States, an advocacy intervention was developed and has shown to be effective at reducing abuse (McFarlane, Soeken, & Wiist, 2000; Parker, McFarlane, Soeken, Silva, & Reel, 1999), promoting safety behavior (McFarlane et al., 2002), and improving social support (Sullivan, Tan, Basta, Rumptz, & Davidson, 1992). Building on this success, Tiwari and colleagues (2010) conducted a randomized controlled trial to test the efficacy of the advocacy intervention with an aim to reduce depressive symptoms in abused women living in a Chinese community. The study reported a statistically significant reduction of 2.66 units in Beck Depression Inventory-II (95% CI [0.26, 5.06) in abused women who received the intervention more than those who did not. Although this difference may not have reached a clinically meaningful level, the advocacy intervention does have reduced depressive symptoms in this group of vulnerable women. Moreover, a significantly more improvement in perceived social support was also observed in the intervention group.
While the effects of advocacy interventions in reducing depressive symptoms among abused women of different races and ethnicities have been recognized, there has not been any consideration on its effects on abused immigrant women who have more demanding needs. Wong et al. (2011) found that abused immigrant women are more likely to suffer from depressive symptoms and perceived social support is a protective factor in preventing these depressive symptoms. The World Health Organization has made a lot of attention on preventing violence against women but not much has been done on immigrant abused women. Moreover, the review conducted by Yoshihama’s (2008) concluded that the evaluation of intervention programs for abused immigrant women was seriously lacking. Further research to develop better target future interventions for immigrants is worth carrying out.
In light of the paucity of research on IPV in immigrants, the present study examines the clinical differences between immigrant and nonimmigrant women who suffer from IPV. In addition, it also evaluates the impact of immigration status on the efficacy of an advocacy intervention in reducing depressive symptoms and enhancing perceived social support in community-dwelling abused women by conducting a secondary analysis of a randomized controlled trial (Tiwari, et al., 2010). We hypothesize that the advocacy intervention can reduce the depressive symptoms of both abused Chinese immigrant and abused Chinese nonimmigrant women.
Method
Design
This study was a secondary post hoc analysis of data from a randomized controlled trial conducted between February 2007 and June 2009 (Tiwari, et al., 2010), which supplements the findings of the original study.
Setting and Participants
The study was carried out in a local community center in Hong Kong. This community center is located in a district of the third highest number of residents with the least education and lowest household income, and the fourth highest prevalence of IPV in Hong Kong during the study period (“Population and Household Statistics,” 2008). The inclusion criteria for participating in this study were Chinese women (a) with a history of abuse as identified by the Chinese Abuse Assessment Screen (C-AAS; Tiwari, et al., 2007); (b) aged 18 or older; and (c) able to communicate in Cantonese or Mandarin. Written consent was obtained from those eligible and agreed to participate. The study was approved by the Institutional Review Board of the primary investigator’s institution. A total of 200 women were recruited as planned in the primary study (Tiwari, et al., 2010).
Advocacy Intervention
The intervention employed for this study aims to empower abused women and link them to available community services. Trained research assistants who were licensed social workers acted as the advocates to empower the abused women with ongoing support and informal counseling. The intervention consists of one 30-min face-to-face empowerment training session followed by 12 weeks of telephone social support. The design of the empowerment training was originally developed by Parker and colleagues (1999) and is based on Dutton’s (1992) empowerment model that includes protection and enhanced choice-making and problem-solving. The aim of empowerment training is to increase women’s safety through the recognition of increased danger, paired with a safety plan developed for individual use. In addition, it provides information about the cycle of violence, facts, and options regarding partner violence, legal protection orders, filing for criminal charges, and community resources for abused women. This information gives women options from which they can make their own decisions about relationships. Each woman was given an empowerment pamphlet to reinforce the information delivered. The empowerment protocol has been tested in a previous study and found to be efficacious at reducing IPV and postnatal depression in Chinese mothers (Tiwari et al., 2005).
The telephone social support was based on Cohen’s (1988) Social Support Theory and modified from that of Bullock, Browning, and Geden’s (2002) to enhance the cultural congruence with respect to addressing the cultural difference between abused Chinese women and abused women in Western countries. It aims to provide tangible and perceived social support through social relationships to promote health and well-being. This telephone social support program was conducted through 12 scheduled weekly phone calls. The 12 telephone sessions were decided after due consideration of a balance between the maximum number that would not overwhelm the participants, and the minimum number needed for sufficient social support based on the experience of the investigator team. The telephone social support included the provision of a nonjudgmental listening ear, discussion with the women about their needs, the offer of information when requested, and referrals to other professionals (health/social services) and/or agenes (voluntary/statutory) when appropriate. Each telephone call lasted about 15 to 20 min. To ensure consistency in the responses to expressed needs, a protocol listing the possible responses was made available to the research assistants providing the telephone sessions.
In the present study, empowerment training was conducted in a private area within the community center by research assistants trained by two study investigators. The training consists of five sessions including information on how to implement the intervention in a culturally appropriate manner, how to be nonjudgmental and empathetic, empowerment training protocol and telephone social support protocol. In addition, 15% of the telephone logs were randomly checked for adherence to the intervention protocol. Retraining and observation would be conducted if adherence was unsatisfactory.
A detailed description of the advocacy intervention can be found in Tiwari et al. (2010).
Measurements
IPV
The Chinese version of the Abuse Assessment Screen (C-AAS) was used to screen potential participants for the trial. This scale addresses physical, psychological, and sexual abuse and it has been validated and shown to demonstrate satisfactory accuracy in screening a Chinese population with satisfactory specificity, sensitivity, and predictive values (Tiwari et al., 2007).
History of abuse
To gain a deeper understanding of the abuse history, the Revised Conflict Tactics Scales (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) were used, as they provide information about the frequency of the behavior used by the perpetrator during IPV over the past year. The CTS2 contain 27 items, from which the frequency score for psychological aggression ranges from 0 to 200, physical assault from 0 to 300, and sexual coercion from 0 to 175. The higher the score, the higher is the frequency.
Depressive symptoms
The Chinese version of the Beck Depression Inventory Version II (C-BDI-II; Beck, Steer, & Brown, 1996) was used to measure the depressive symptoms of participants. The Chinese version has been validated and verified as demonstrating good psychometric properties in Chinese populations (Byrne, Stewart, & Lee, 2004). It is a 21-item questionnaire with a total score ranging from 0 to 63. A higher score indicates more depressive are the symptoms reported by the participants.
Social support
Perceived social support was measured using the Interpersonal Support Evaluation List-12 (ISEL-12; Cohen, Mermelstein, Kamarck, & Hoberman, 1985), which has established psychometric properties and good internal consistency (Cronbach’s α = 0.88). The 12-item questionnaire measures three subscales: appraisal, belonging, and tangible support, which provides a total score ranging from 0 to 36. The higher the score, the more the participant perceived that they received social support.
Demographics
Demographic data such as age, place of birth, years of living in Hong Kong, educational level, marital status, immigration status, employment status, receiving social security, and self-perceived financial difficulties were collected.
Data Collection and Procedures
Data were collected by a research assistant in a private room, who first explained the study purpose, potential risks and benefits, instruments, administration time and follow-up schedules. Informed consent was obtained if the women were willing to participate. The above measurements including the CTS2, C-BDI-II, ISEL, and demographic questionnaire were administered (a) on entry to the study, (b) 3 months after enrolment, and (c) 9 months after enrolment.
Statistical Analysis
Secondary analyses were performed using SPSS Version 18 (SPSS, Inc., Chicago, United States). Three women who had immigrated from Mainland China declined to report the number of years they had lived in Hong Kong, hence the sample size for data analysis was 197. Baseline comparisons between the immigrant women and nonimmigrant women were performed using the Fisher’s exact test, the χ2 test and the Mann-Whitney U test for dichotomous, nondichotomous categorical, and continuous characteristics, respectively. A linear mixed effects model was then used to examine the impact of immigrant status on the intervention effects of depressive symptoms and perceived social support. Specifically, the intercept was taken as random to account for the extra-covariance among the repeated measurements over time. The C-BDI-II and ISEL baseline scores, study group, and time of measurement were considered to be independent variables in the model.
The impact of immigration status on intervention effect was first assessed if it changed from 3 to 9 months by incorporating a third order interaction—grouped by immigration status and time. If this interaction was found to be significant, the impact of immigration status on intervention effect was estimated separately by time. If this was found to be insignificant, the overall impact of immigration status between 3 and 9 months was reported. The random effects as well as the residuals were checked for the adequacy of normality and potential outliers. A 5% level of significance was used in all significance tests.
Results
Immigrants and Nonimmigrants
Among the 197 women included in this study, all either lived or worked in the catchment area of the community center. Their mean age was 38 (SD = 7.19), and most (72.5%) had at least grade 7 education. The majority of the women (n = 176, 89.5%) were married or cohabiting. More than half (n = 124, 62%) were born in Mainland China. One third of the women (n = 60, 30.5%) did not have permanent residency in Hong Kong and were considered to be immigrants for this study.
Table 1 compares immigrant (n = 60) with nonimmigrant (n = 137) abused women. Immigrant women were much younger (mean age = 35.6, SD = 4.8, p = 0.001), had lower employment status (n = 11, 18.3%, p = 0.012), and had more children (p = 0.003) compared with nonimmigrant women. There was also a significant difference in the marital status of these women. Immigrant women were more likely to stay married or continue to cohabit with their partners (n = 58, 97.7%, p = 0.001). The baseline levels of depressive symptoms of immigrant and nonimmigrant women were not statistically significant (p = 1.151). Moreover, immigrant women had lower perceived social support (mean score = 4.3, SD = 5.5, p = 0.006).
Descriptive Characteristics for Comparing the Abused Immigrant Women and Abused Nonimmigrant Women in Intervention Group and Control Group (n = 197).
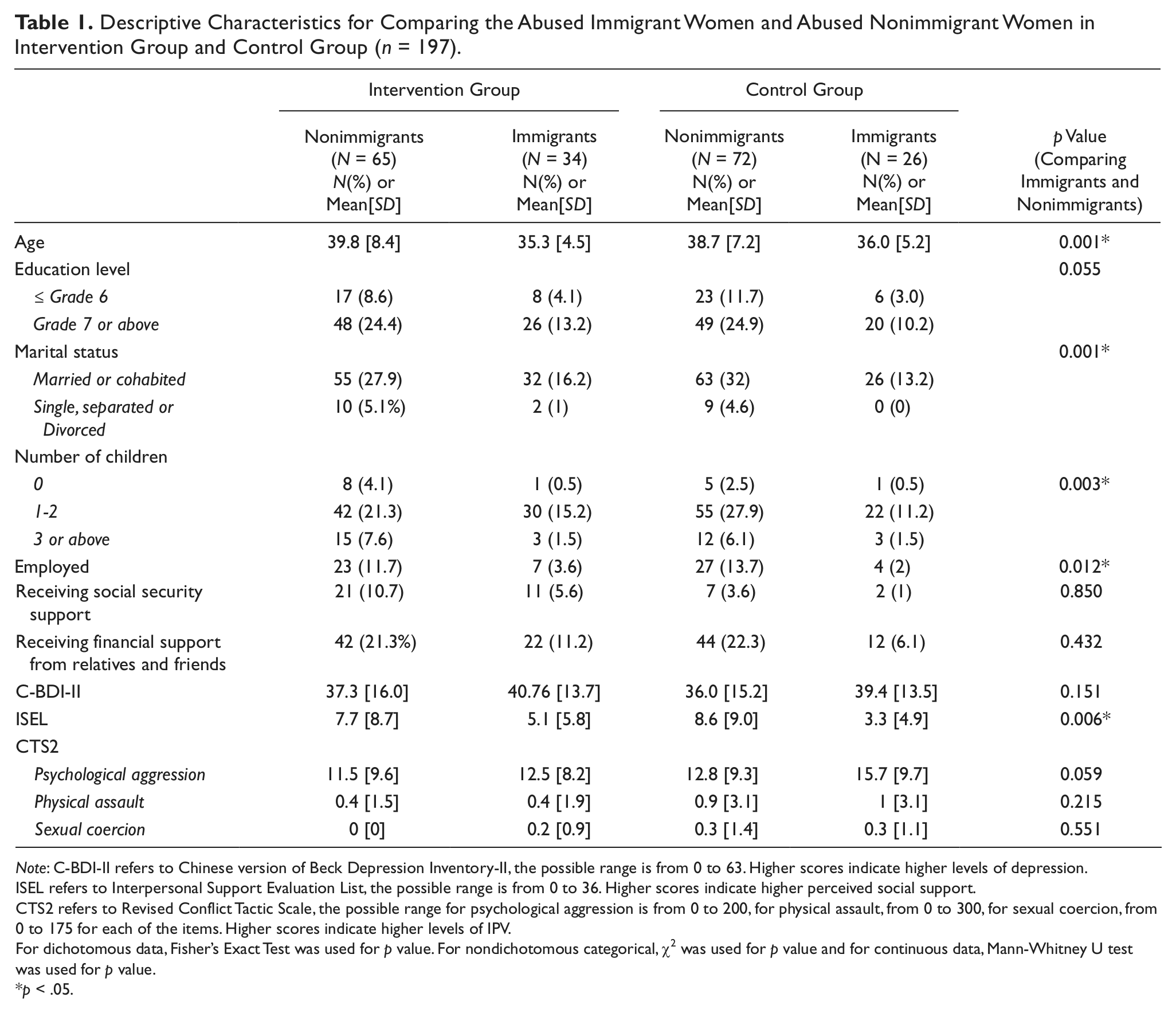
Note: C-BDI-II refers to Chinese version of Beck Depression Inventory-II, the possible range is from 0 to 63. Higher scores indicate higher levels of depression.
ISEL refers to Interpersonal Support Evaluation List, the possible range is from 0 to 36. Higher scores indicate higher perceived social support.
CTS2 refers to Revised Conflict Tactic Scale, the possible range for psychological aggression is from 0 to 200, for physical assault, from 0 to 300, for sexual coercion, from 0 to 175 for each of the items. Higher scores indicate higher levels of IPV.
For dichotomous data, Fisher’s Exact Test was used for p value. For nondichotomous categorical, χ2 was used for p value and for continuous data, Mann-Whitney U test was used for p value.
p < .05.
Impact of Immigration Status on the Effect of Advocacy Intervention in Reducing Depressive Symptoms
Figure 1 shows the mean C-BDI-II score of abused Chinese immigrant and nonimmigrant women by their study group at baseline, 3 months, and 9 months follow-up. Among the immigrant women, the mean C-BDI-II score in the intervention group was higher than that in the control group at baseline. However at the 9-month follow-up, the mean C-BDI-II score in the intervention group was lower than that in the control group.
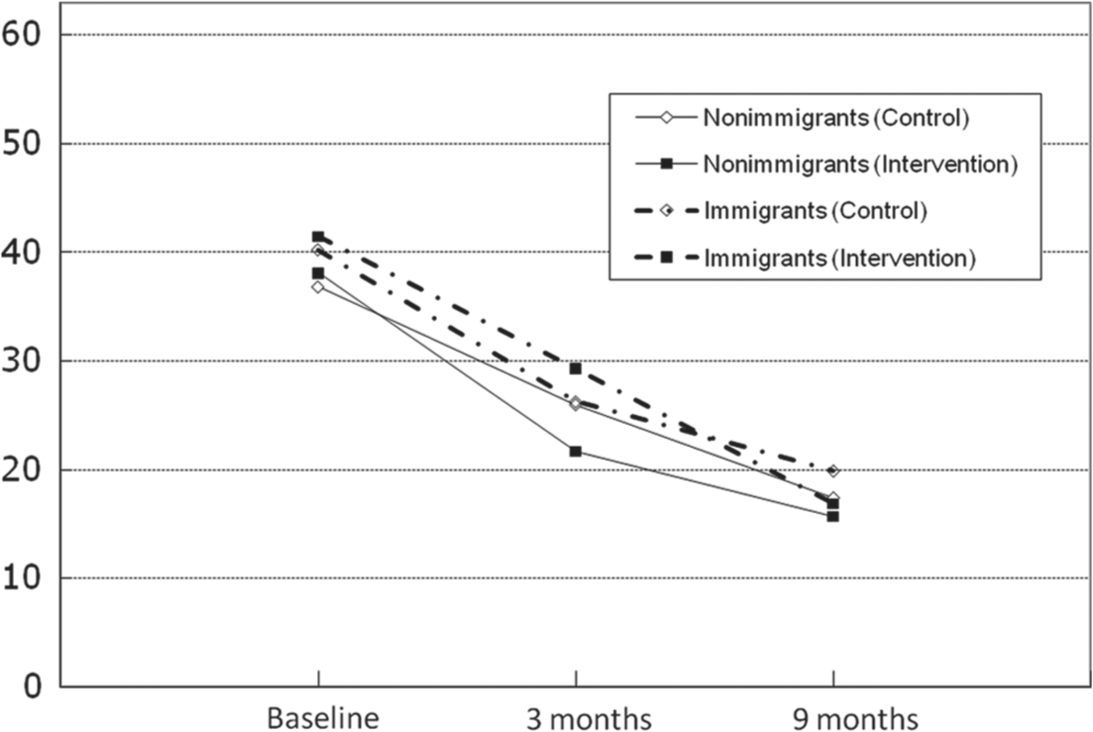
The mean scores of Beck Depression Inventory (C-BDI-II) of Chinese abused immigrant women and abused nonimmigrant women in intervention group and control group.
Table 2 shows the results of the linear mixed effects model, which highlights the significant impact of immigration status on the intervention effect between three and nine months (p = 0.014). Thus, the impact of immigration status on the effectiveness of the advocacy intervention at reducing depressive symptoms at 3 months and 9 months was reported separately. Immigration status influenced the intervention effect at 3 months (p = 0.02), but not at 9 months (p = 0.74). At 3 months, the advocacy intervention reduced depressive symptoms significantly more in the intervention group than it did in the control group among nonimmigrant women (Estimate = −4.9, 95% CI [−8.38, −1.41], p = 0.006), but no significant effect was found among immigrant women (Estimate = 2.7, 95% CI [−2.65, 7.99], p = 0.325). One outlier in the control group was identified who had a substantial reduction of depression symptoms during follow-up when compared with other women in the control group. However, after removing this outlier and adjusting for the clinical characteristics that were significantly different between immigrants and nonimmigrants (i.e., age, marital status, number of children, employment, and ISEL baseline score), the results remained the same.
The Impact of Immigration Status on the Effect of Advocacy Intervention in Reducing Depression Among Abused Chinese Women at 3 Months and 9 Months (n = 197)
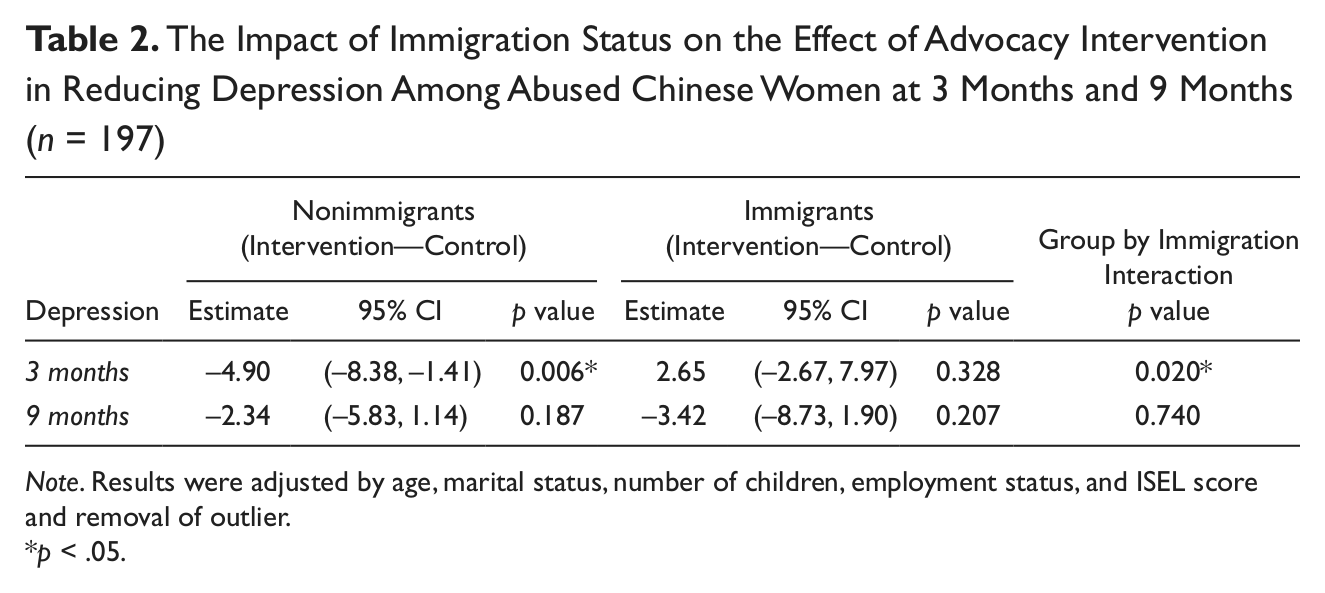
Note. Results were adjusted by age, marital status, number of children, employment status, and ISEL score and removal of outlier.
p < .05.
Impact of Immigration Status on the Effect of Advocacy Intervention in Enhancing Perceived Social Support
Figure 2 shows the mean ISEL score of abused Chinese immigrant and nonimmigrant women by study group at baseline, 3 months, and 9 months. Table 3 shows the overall intervention effect on perceived social support between 3 and 9 months. Advocacy intervention significantly increased perceived social support for nonimmigrant women (Estimate = 2.74, 95% CI [0.66, 4.82], p = 0.01) but not for immigrant women (Estimate = 0.62, 95% CI [–2.54, 3.79], p = 0.698) between 3 and 9 months. Furthermore, the impact of immigration status on the intervention effect was not significantly different at 3 months and 9 months follow-up (p = 0.677). Again, there was no difference in the findings after adjusting the factors that were significantly different between immigrants and nonimmigrants (i.e., age, marital status, number of children, employment, ISEL baseline score), and removing the outlier.
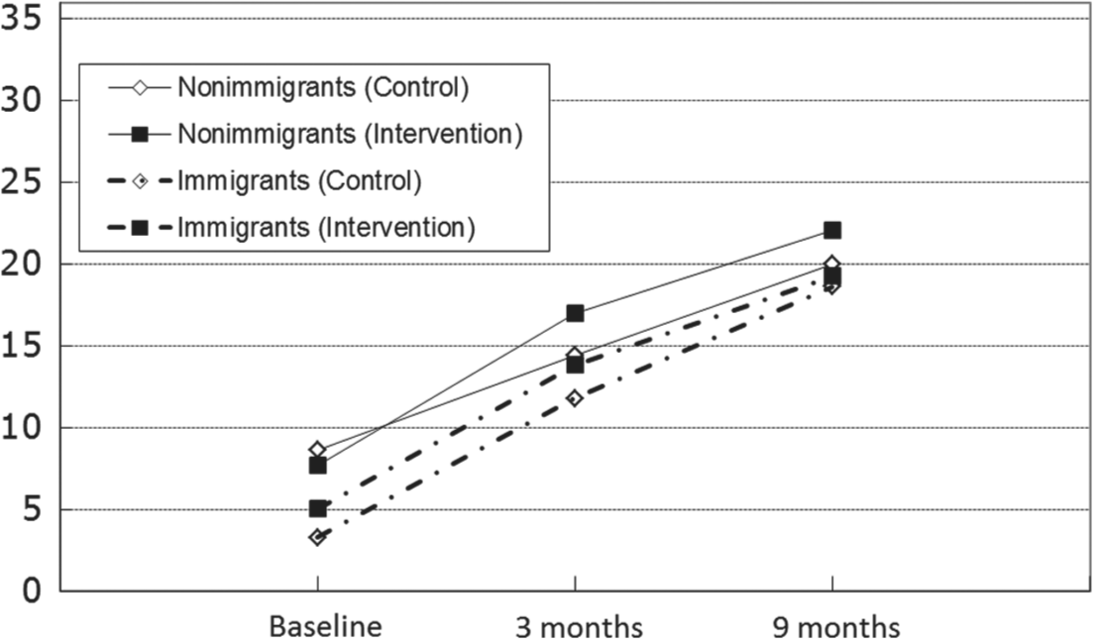
The mean scores of Interpersonal Support Evaluation List (ISEL) of Chinese abused immigrant women and abused nonimmigrant women in intervention group and control group.
The Impact of Immigration Status on the Overall Effect of Advocacy Intervention on Improving Social Support Among Abused Chinese Women (n = 197)
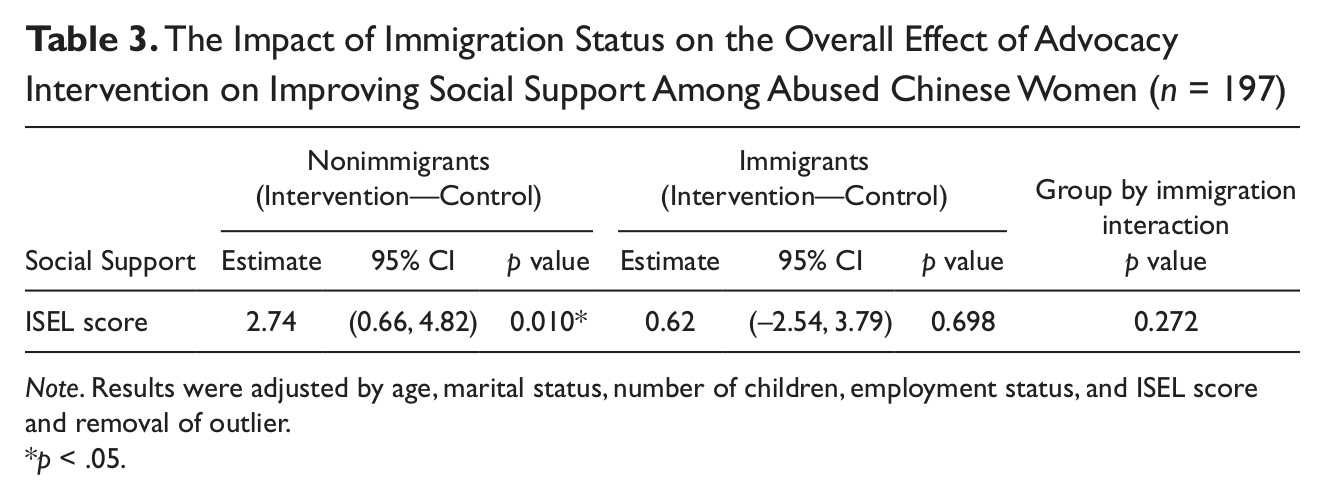
Note. Results were adjusted by age, marital status, number of children, employment status, and ISEL score and removal of outlier.
p < .05.
Discussion
This is the first study to investigate the differential effect of an advocacy intervention for abused immigrant and nonimmigrant women in the Chinese community. Immigrants present themselves as a group of individuals with special needs different from residents in a local setting. This implies the need of interventions tailored to the needs of abused immigrant women. Moreover, this study raises the importance of cautious interpretation when assessing an intervention in a sample composed of both immigrants and non-immigrants in whom the intervention may exhibit different effects.
In our women suffering from IPV in Hong Kong, those immigrants from Mainland had lower perceived social support than the nonimmigrants. This could be contrary to the belief of similar experiences with IPV and the corresponding health impact between the two groups of Chinese because they share the similar culture. Nevertheless, our result is in line with the findings of previous studies, which indicate that abused immigrant women experience obstacles to accessing formal or informal resources because of different cultural norms, language barriers, immigration status, lack of familiarity with existing service systems (Lee & Hadeed, 2009; Raj & Silverman, 2002; Xu, Campbell, & Zhu, 2001), as well as the fear of deportation (Bauer, Rodriguez, Quiroga, & Flores-Ortiz, 2000; Dutton et al., 2000). Immigrant women may face many unmet needs with very limited social network. The social isolation may then develop the feeling of poor social support. Some studies have suggested that immigrant women experience greater social isolation because of unfamiliar environments (Lee & Hadeed, 2009; Yoshioka, et al., 2003; Song, 1996), which may necessitate their dependency on the perpetrators of IPV. The perpetrators may make use of immigration status to control the women from legal and financial resources, as well as emotional support services, which enhance the unmet needs of the immigrant women (Dutton et al., 2000). On the other hand, the observed difference may also be attributed to any differentials in IPV experience between immigrants and non-immigrants. However, the CTS2 scores at baseline were not statistically different between the two groups of abused women, and thus the observed difference would more likely be a result of immigration.
The immigrant women had unexpectedly no significant difference from the nonimmigrants in their mean scores of depressive symptoms measured by the C-BDI-II. However, among Asian American and Chinese American immigrants, their prevalence of depressive symptoms was generally higher than that in the general populations (Lee, Pomeroy, & Bohman, 2007;Hicks & Li, 2003; Hicks, 2006; Yick, Shibusawa, & Agbayani-Siewert, 2003). In the Chinese cultural context, developing and maintaining family harmony is a woman’s responsibility. Therefore, abused Chinese immigrant women may feel as though they bear the responsibility for the abuse or are even at fault for it, resulting in shameful emotions. Furthermore, some Chinese immigrant women might have moved to Hong Kong because of their poor living conditions in Mainland and their family members would expect immigrant women to be materially and emotionally rewarded after their marriage in Hong Kong (Chin, 1994). The abused immigrant women would rather not to seek help or even inform their family members in Mainland of their unpleasant experience. The resultant shameful emotions (Tiwari et al., 2009) and the feeling of learned helplessness (Bargai, Ben-Shakhar, & Shalev, 2007) might have led to more depressive symptoms. Nevertheless, the lack of such difference in depressive symptoms between immigrants and nonimmigrants in our study may due to two possible reasons. First, the level of depressive symptoms in this study was generally severe at baseline for both groups of women because of IPV. The ceiling effect may have limited difference between the two groups. Second, previous studies examined Chinese immigrants in America with a non-Chinese culture, whereas the present study assessed Mainland immigrants in Hong Kong, a place sharing similar Chinese culture with Mainland. Chinese Americans may suffer from additional stress because of acculturation and language differences compared with Chinese immigrants in the present study. Thus, difference of depressive symptoms between immigrant and non-immigrant women in Hong Kong may not be as large as those previously reported.
The linear mixed effects analysis showed that the advocacy intervention was effective at reducing the depressive symptoms in abused nonimmigrant women but not in abused immigrant women at 3 months. However, the impact of immigration status did not sustain at 9 months. The duration of the advocacy intervention appears to be an important factor. Yakushko and Chronister (2005) pointed out that communication with immigrant women begins with establishing rapport for understanding their mental health needs, and time is vital for establishing the rapport. Our social support intervention lasted for 12 weeks only, which may not be long enough to sustain the support to the abused women beyond the 3 months period. Moreover, the C-BDI-II may not be a comprehensive instrument for measuring the efficacy of advocacy intervention, as level of depressive symptoms does not directly lead to the adoption of safety behaviors with regard to IPV. In other words, the stress of both abusive relationships and immigration may not be expected to change dramatically in 3 or even in 9 months, but perhaps women behaved differently, such as in seeking formal help for IPV, as a result of the intervention. A longer follow-up time will be helpful to assess the long-term effect of the intervention.
In addition, advocacy intervention was found to be efficacious at enhancing the perceived social support of nonimmigrant but not in immigrant women, regardless of the time period. Although the advocacy intervention in the present study has been delivered in a culturally appropriate manner, such as avoid demanding verbal emotional disclosure which is not part of the Chinese culture, it was not sufficiently tailored to address the specific and complex needs of immigrant women. Also, the interventionists were trained to have a good understanding of IPV but not specifically of immigration issues. Modifications addressing the unmet needs of abused Chinese immigrant women are thus strongly recommended. Specifically, attention should be focused on (a) strengthening the capacity of these women to adjust for cultural differences, (b) providing survival tips to meet typical challenges, for example, parenting issues, employment opportunities and language learning, (c) enhancing their knowledge of the Hong Kong legal system, (d) relieving their fear of deportation, and (e) making referrals to community resources in Hong Kong.
Despite the efforts made to ensure the validity of the analysis by checking of various assumptions and assessing the robustness to outliers, this study bears several limitations. First, it is a secondary analysis using a design and sample size not initially planned for this purpose. The findings remain exploratory and need to be confirmed by a prospective study designed for the purpose. However, the significant impact of immigrant status on the effects of the advocacy intervention is unlikely as a result of insufficient sample size. In addition, the new findings of this study supplement the findings of the parent study conducted by Tiwari et al., (2010). Second, this study relied on self-reported data for assessing depressive symptoms and perceived social support. This may bring concerns on the reliability of the responses. However, the recruited women were not under any special care of our study team and were informed of no rewards for participating in our study. Hence, they would unlikely provide unreliable responses. Third, the 9-month follow-up period may be too short to examine the efficacy of the advocacy intervention on immigrant women. Further studies with a longer follow-up period are recommended. Finally, we have not assessed the association between IPV and depression. However, IPV has been a known risk factor of depression (Golding, 1999), which is the rationale the advocacy intervention was developed for reducing depression in abused women. It is nevertheless difficult to assess the association between the changes of IPV and depression in our study because of the expected confounding effect from the intervention.
Notwithstanding these limitations, this study provides important clinical implications for community service providers. A tailor-made advocacy intervention program should be developed for abused immigrant women in the community. Such interventions should ensure good rapport between immigrant women and service providers, and address immigrant women’s needs, including language learning, employment training, and parenting skills. Furthermore, service providers may also consider to enhance the support networks of abused women, including emotional support and tangible resources. In addition, under the current policy of open door immigration to Hong Kong from Mainland China, the increase of immigrant women from the Mainland would be continued. Policymakers should not underestimate the manifestations of both the social and the health-related problems of immigrant women. Continual support programs and public services to help immigrant women, especially the vulnerable group of abused women, are essential.
Conclusion
IPV among immigrant women is a complicated issue involving cultural, societal, legal, and interpersonal considerations. Even under a similar cultural setting, abused Chinese immigrant women had lower perceived social support compared with abused nonimmigrant Chinese women. Current interventions for reducing depressive symptoms of abused women may be efficacious to nonimmigrants but the effects may not be necessarily carried to immigrants. There is an urgent need to design strategies and interventions specific to the unmet needs of immigrants to reduce their depressive symptoms and enhance their social support.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.