
Abstract
The first year of parenthood can be a stressful time, especially for high-risk couples. Symptoms of posttraumatic stress (PTS) have been associated with decreased intimacy, communication, and relationship adjustment, yet there is a lack of research on how PTS symptoms might affect couples in early parenthood. Furthermore, there is little evidence regarding the way in which PTS symptoms may affect couples above and beyond known risk factors such as intimate partner violence (IPV) and harmful alcohol use. The current study investigated how PTS symptoms were related to new parents’ relationship satisfaction in the context of IPV and harmful drinking. Ninety-eight heterosexual couples filled out questionnaires 1 year after the birth of their first child. Hierarchical multiple regression analyses indicated that, for men, PTS symptoms predicted lower relationship satisfaction over and above IPV victimization and harmful drinking. However, for women, psychological IPV victimization was the only significant multivariate predictor. In addition, for men, PTS symptoms interacted with harmful drinking to predict poorer relationship satisfaction. The results suggest that women’s relationship satisfaction is particularly linked to psychological IPV victimization during early parenthood, whereas men’s relationship satisfaction is particularly associated with their own harmful drinking and PTS symptoms. Implications are discussed.
The first year of parenthood can be a stressful life event for couples, with relationship satisfaction often declining after the first child is born (e.g., Doss, Rhoades, Stanley, & Markman, 2009; Mitnick, Heyman, & Smith-Slep, 2009; Neff & Broady, 2011). In turn, low relationship satisfaction during this pivotal developmental period is associated with other relationship outcomes, such as perceived unfairness of labor division (e.g., Grote & Clark, 2001), work–family conflict, and lower satisfaction with parent–child interactions (e.g., Shreffler, Meadows, & Davis, 2011). Perceptions of stress tend to peak around a year after the child is born, particularly for those parents with preexisting mental health vulnerabilities (Perren, von Wyl, Bürgin, Simoni, & von Klitzing, 2005). Previous research illustrates that couples that either have no previous experience managing stressful situations (e.g., Neff & Broady, 2011) or couples who experience significant additional stressors (such as intimate partner violence [IPV] and alcohol abuse) (Charles & Perreira, 2007) are at a higher risk for relationship discord and maladaptive relationship behaviors during the first few years of parenthood.
Specifically, IPV (e.g., Coker et al., 2002), drug and alcohol abuse (e.g., White & Widom, 2003), and posttraumatic stress (PTS) symptoms (e.g., Monson, Fredman, & Adair, 2008) have been identified as risk factors for relationship discord, increased conflict, and poor mental health (e.g., depression in one or both partners). However, we know less about how these risk factors operate during times of stress and developmental changes, such as the first year of parenthood. Indeed, most studies to date have examined the link between PTS symptoms and relationship satisfaction in discrete populations such as men who are veterans of military combat (Taft, Watkins, Stafford, Street, & Monson, 2011). Furthermore, we know little about how these risk factors affect relationship satisfaction in combination with one another, and particularly the extent to which PTS symptoms might further affect the relationship above and beyond experience of IPV and substance misuse. The overarching goal of the current study was to understand the additive and interactive role of harmful drinking, IPV victimization, and PTS symptoms in predicting relationship satisfaction in a sample of first-time parents.
IPV During Pregnancy and Early Parenthood
The annual prevalence rate of physical aggression in the general population is 10% to 12%, and the prevalence of psychological aggression is much higher, often 75% or above (e.g., Archer, 2000; Coker et al., 2002). IPV prevalence rates during pregnancy range from 8% to 11% (Stampfel, Chapman, & Alvarez, 2010), but can be as high as 30% in high-risk samples (i.e., families with substance-misuse issues; Charles & Perreira, 2007). Although some studies have found that IPV decreases during pregnancy (Charles & Perreira, 2007), others have found an increase in IPV during pregnancy (Stampfel et al., 2010). Moreover, couples who experience multiple risks (e.g., poverty, substance abuse) may experience a temporary decline in IPV during pregnancy, followed by an increase in IPV after the child’s birth (e.g., Charles & Perreira, 2007). IPV in couples has been associated with decreased relationship satisfaction (e.g., Falconier & Epstein, 2010), decreased trust and affection between partners, increased conflict, and continued/escalated IPV for both partners (e.g., Monson, Langhinrichsen-Rohling, & Taft, 2009), in addition to mental health difficulties, such as depression (e.g., Beach et al., 2004). However, we know very little about how IPV affects the relationship satisfaction of new parents. Women in community samples tend to engage in similar or slightly higher rates of physical and psychological IPV than men (Archer, 2000) and such IPV tends to be largely bidirectional between partners (Langhinrichsen-Rohling, Misra, Selwyn, & Rohling, 2012). Studies of bidirectional violence during pregnancy and early parenthood also provide mixed results. For example, studies with women who access mental health care during pregnancy have found that this group of women is more likely to be victimized during pregnancy (e.g., Charles & Perreira, 2007). However, such studies do not always ask about women’s perpetration of violence. More comprehensive studies on bidirectionality of IPV during early parenthood are needed.
Harmful Drinking as a Risk Factor for IPV
In couples, harmful drinking often co-occurs with IPV. For instance, rates of alcohol consumption before episodes of IPV range from 20% to 50% (e.g., Stalans & Ritchie, 2008). Men and women presenting for treatment of alcohol disorders are six to eight times more likely to engage in IPV toward their partner (Fals-Stewart, 2003; O’Farrell & Murphy, 1995). The combination of harmful drinking and IPV may place couples at higher risk for further relationship problems, such as poor communication (White & Widom, 2003), as well as personal problems, such as depression and anxiety (Forgey & Badger, 2010). However, much of the research that examines the link between IPV and harmful drinking has been done with men, and few studies have examined the relationship between women’s drinking and aggression (or victimization, for example, Parks, Hsieh, Bradizza, & Romosz, 2008). Even more importantly, few studies have investigated how IPV and harmful drinking relate to the functioning of couples during the first year of parenthood, a time in which the negative effects of IPV and harmful drinking may extend to the well-being of young children.
Men and women tend to reduce overall rates of alcohol use during early parenthood (e.g., Neve, Lemmens, & Drop, 2000). There is some evidence, however, that alcohol abuse, or a pattern of drinking that causes negative consequences, increases significantly for men and women after childbirth (Richman, Rospenda, & Kelley, 1995).
The Role of PTS in Relationship Satisfaction
PTS symptoms show a robust association with relationship dissatisfaction (e.g., Cook, Riggs, Thompson, & Coyne, 2004; Dekel, Enoch, & Solomon, 2008; Monson et al., 2008), even after controlling for known risk factors such as depression (O’Donnell, Cook, Thompson, Riley, & Neria, 2006). For example, trauma survivors who experience PTS symptoms or clinical PTS disorder (PTSD) often have difficulties with communication, sexual intimacy, and boundary setting in relationships (Najavits, Sonn, Walsh, & Weiss, 2004). Such difficulties can engender dysfunctional relational dynamics. For instance, if the trauma survivor appears distant and irritable, his or her partner may feel frustrated and react by being psychologically or physically aggressive. In addition, trauma survivors with active PTS symptoms are at higher risk for entering abusive relationships, where they are at risk of being retraumatized and experiencing an escalation in their PTS symptoms or other symptomatology (Najavits et al., 2004; Seedat, Stein, & Forde, 2005). PTS symptoms in one or both partners can present the couple with a continuous stressor. Individuals who are already at high risk for poor relationship satisfaction (e.g., individuals experiencing IPV and harmful drinking), are likely to experience this additional stressor more acutely and subsequently engage in further maladaptive coping strategies, such as escalating levels of harmful drinking (Monson et al., 2008).
IPV, harmful drinking, and PTS symptoms tend to be related in such a way that they are likely to maintain one another (e.g., Dekel et al., 2008). For instance, alcohol use can provide temporary relief from acute PTS symptoms, but create a dependence that is associated with other costs (e.g., Monson et al., 2008). Alternatively, IPV in the relationship can be a significant stressor in a person’s life, possibly leading to the development of PTS symptoms (Evans, McHugh, Hopwood, & Watt, 2003). We do not know how PTS symptoms affect new parents in the presence of IPV and substance misuse, although it is likely that such stressors may pose additional obstacles to couples’ relational functioning.
PTS symptoms (psychological dysregulation) may contribute to development of a dyadic environment that is more susceptible to behavior dysregulation, including IPV and alcohol misuse. We applied the framework of the vulnerability-stress-adaptation (VSA) theory of relationship satisfaction (Karney & Bradbury, 1995) to conceptualize the relationship between PTS symptoms, IPV, and harmful drinking. In such a framework, PTS symptoms are considered a vulnerability that elevates the couple’s risk for maladaptive behavioral responses (such as IPV and harmful drinking) to stressful events. Although the effects of PTS symptoms are hypothesized to interact with effects of IPV and harmful drinking, previous literature has shown that PTS symptoms have a unique association with relationship dissatisfaction, even in presence of other risk factors (e.g., Lambert, Engh, Hasbun, & Holzer, 2012; Nelson Goff & Smith, 2005).
Depression as a Complex Risk Factor
PTS symptoms are highly comorbid with symptoms of depression (Blasco-Ros, Sanchez-Lorente, & Martinez, 2010). The relationship between PTS and depressive symptoms is complex. For example, a person may experience emotional numbing, but it may be difficult to tell whether this is a symptom of depression or PTSD per se. Depressive symptoms also have a complex relationship with harmful drinking, such that harmful drinking can predict increases in depression and vice versa (Labbate, Sonne, Randal, Anton, & Brady, 2004). Finally, depression can either precede or follow IPV (Blasco-Ros et al., 2010). Thus, any study that examines PTS symptoms, harmful drinking, and IPV must control for potential effects of depressive symptoms.
Purpose of the Study
The purpose of this study was to examine how PTS symptoms relate to relationship satisfaction in new parents in the presence of IPV and harmful drinking. As a vulnerability factor, PTS symptoms were hypothesized to account for unique variance in relationship satisfaction, over and above harmful drinking and IPV. Our goal was to examine whether the presence of any PTS symptoms have a unique association with relationship dissatisfaction, even in the presence of known problem behaviors, such as IPV and harmful drinking. We hypothesized (a) that the presence of PTS symptoms would predict lower relationship satisfaction for men and women, even above and beyond the effects of harmful drinking and IPV victimization, (b) that IPV victimization, harmful drinking, and PTS symptoms would interact to predict the greatest risk for relationship dissatisfaction during early parenthood, and (c) that these associations will continue to be significant after controlling for symptoms of depression.
Method
Participants
The 88 women and 79 men who participated in this study were part of a larger longitudinal project of 100 couples who were originally recruited during the third trimester of pregnancy. The current study analyzed data from the second wave of data collection, which occurred approximately 1 year after the child’s birth. The couples participating in the study were recruited from a mid-sized city in British Columbia, Canada, by placing advertisement brochures in the offices of midwives, maternity doctors, and maternity stores. Researchers also conducted presentations about the study at prenatal classes. To be eligible to participate in the original study, the couples had to be pregnant with their first child, be living together, and be more than 17 years of age. Participants were offered a US$25.00 honorarium for completing the questionnaires at the postnatal assessment. The dropout rate between the prenatal and postnatal assessments was 7%, which is consistent with attrition rates of 6% to 7% in other longitudinal studies (e.g., Doss et al., 2009). The only significant demographic difference between participants and dropouts was the number of years the couple had lived together, t(165) = −2.12, p < .04). Surprisingly, participants who dropped out of the study reported living with their partner for significantly more years (7 vs. 4.5); however, this trend was skewed by several couples who have lived together for more than 10 years.
At the postnatal assessment, participants were between 18 and 48 years of age. The mean age was 34 (SD = 4.90) for men and 31 (SD = 5.00) for women. Mean annual income for women was US$27,000 (SD = 23,621) and for men was US$49,700 (SD = 26,740). Approximately 11% of the participants identified themselves as a visible minority (men: 4% Asian, 2% First Nations, 1% each Latin American, Portuguese, and Sikh; women: 3% First Nations, 6% Asian, 1% each African, East Indian, Filipina, and Latin American). The constitution of the sample is representative of the ethnic constitution of the recruitment area (Statistics Canada, 2006).
Procedures
One year after the child was born, participants were contacted by phone and/or email and asked if they were interested in continuing their participation in the study. Participants were given their own individual code and password to access the online questionnaires and were encouraged to complete the questionnaires separately from their partners. Participants filled out validated questionnaires regarding PTS symptoms, experiencing and perpetrating IPV, harmful drinking, depression, and relationship satisfaction, among others. Once the participants completed the survey, they were mailed a US$25 honorarium.
Measures
IPV
The Conflict Tactics Scale Revised (CTS-R; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) contains questions about experiencing and engaging in various conflict tactics in the past year. For example, a question about psychological aggression, such as, “Have you insulted or sworn at your partner?” is also asked as, “Has your partner insulted or sworn at you?” In the current study, the Psychological (8 items) and Physical Aggression (12 items) subscales were used. Responses for each subscale range from “never” to “more than 20 times,” and a higher score indicates greater use of aggression (Straus et al., 1996).
To minimize the problem of underreporting of aggression (e.g., Heyman & Schlee, 1997), the higher of the two partners’ reports were used to calculate each individual’s levels of psychological and physical aggression when possible. This is the standard procedure that is used in other studies of IPV (e.g., Heckert & Gondolf, 2000), because it corrects for possible underreporting of violence by either partner. While the procedures used in this study minimize underreporting, participants may still underreport their own aggression. The Psychological and Physical Aggression subscales demonstrated satisfactory reliability, measured separately for men and women (Cronbach’s alphas were .61 and .88). According to the couples’ reports, 81.8% of women and 87.5% of men were the victims of at least one act of psychological aggression by their partner, whereas 20.5% of women and 28.4% of men were the victims of at least one act of physical aggression by their partner. Means and SDs are reported in Tables 1 and 2.
Summary of All Intercorrelations for Men (N = 79, Unless Specified Otherwise).
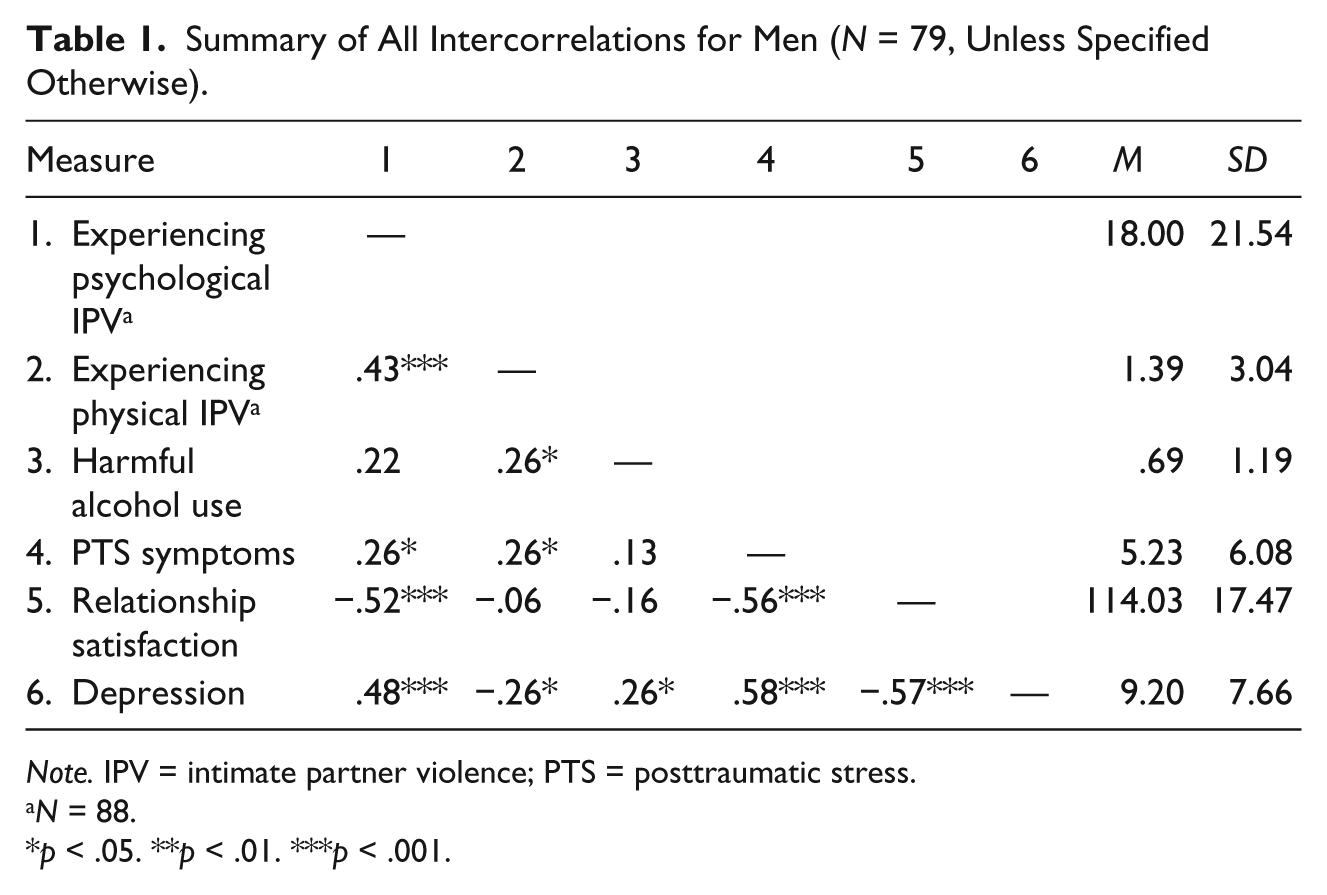
Note. IPV = intimate partner violence; PTS = posttraumatic stress.
N = 88.
p < .05. **p < .01. ***p < .001.
Summary of All Intercorrelations for Women (N = 88, Unless Specified Otherwise).
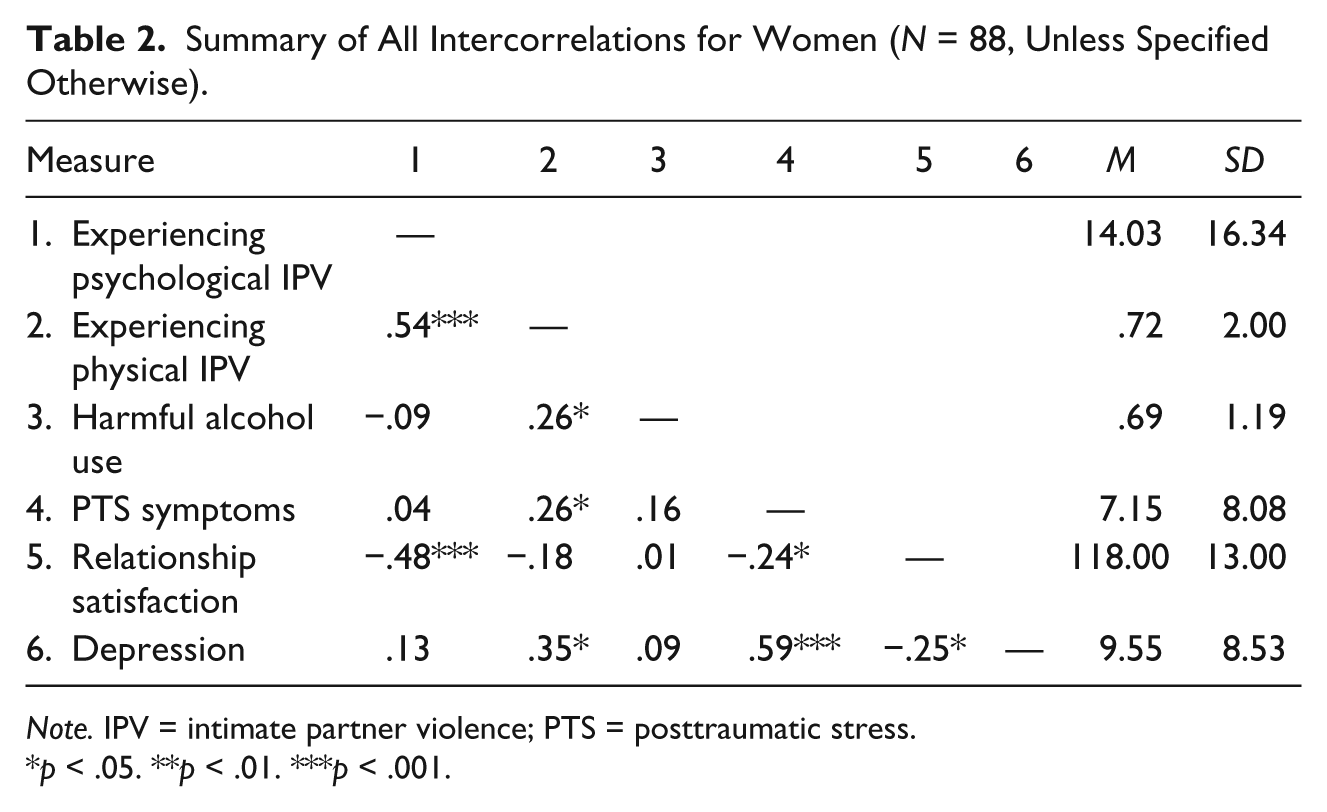
Note. IPV = intimate partner violence; PTS = posttraumatic stress.
p < .05. **p < .01. ***p < .001.
Harmful drinking
The Alcohol Use Disorders Identification Test (AUDIT) was used to assess harmful drinking patterns (Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). The AUDIT comprises 10 items that assess four domains: drinking behavior, alcohol consumption, adverse psychological reactions, and alcohol-related problems. The response options range from “never” to “daily or almost daily.” The original version of AUDIT had poor reliability for women in the current study. Therefore, an amended version of the AUDIT was created in which several items with zero variance for women were deleted. The revised AUDIT showed excellent reliability for men (Cronbach’s alpha = .83) and satisfactory reliability for women (Cronbach’s alpha = .58). Only 4% of men scored at or above the cutoff of 8 on the AUDIT (which represents problematic drinking) and 8% of men scored in the borderline range (i.e., 6-7). None of the women scored above the cutoff or in the borderline range. However, these cutoffs were computed using the modified version of the AUDIT and, therefore, may slightly underestimate the extent of harmful drinking in this sample.
Relationship satisfaction
The Dyadic Adjustment Scale (DAS) is a 32-item questionnaire that measures relationship satisfaction (Spanier, 1976). A score in the range of 90 to 100 indicates average or moderate relationship satisfaction. A score of 50 or below indicates very low relationship adjustment (Spanier, 1976). The DAS had excellent reliability in the current study (men: Cronbach’s alpha = .93; women: Cronbach’s alpha = .88). In terms of relationship satisfaction, 15.5% of men and 16.6% of women reported average relationship satisfaction (represented by scores in the 90-110 range), 10.3% of men and 3.6% of women reported below average relationship satisfaction (DAS < 90), and 74.2% of men and of 79.8% women reported above-average relationship satisfaction (DAS > 110).
PTS symptoms
To assess PTS symptoms, the PTSD checklist (PCL) was used (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). The PCL is a 17-item scale that measures symptoms of PTSD as they are outlined in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnostic category. The symptom clusters include hyperarousal, re-experiencing, and avoidance/numbing. Each item asks the participant to what degree they have been bothered by a particular symptom in the past month; items are scored on a scale of 1 to 5, with 1 meaning “not at all” and 5 meaning “extremely.” The reliability for the PCL in this study was excellent: Cronbach’s alpha = .85 (men) and Cronbach’s alpha = .91 (women). See Table 3 for types of traumatic events endorsed and Table 4 for correlations between the PCL total and the events endorsed by participants.
Endorsement of THQ items for Men and Women (Lifetime).
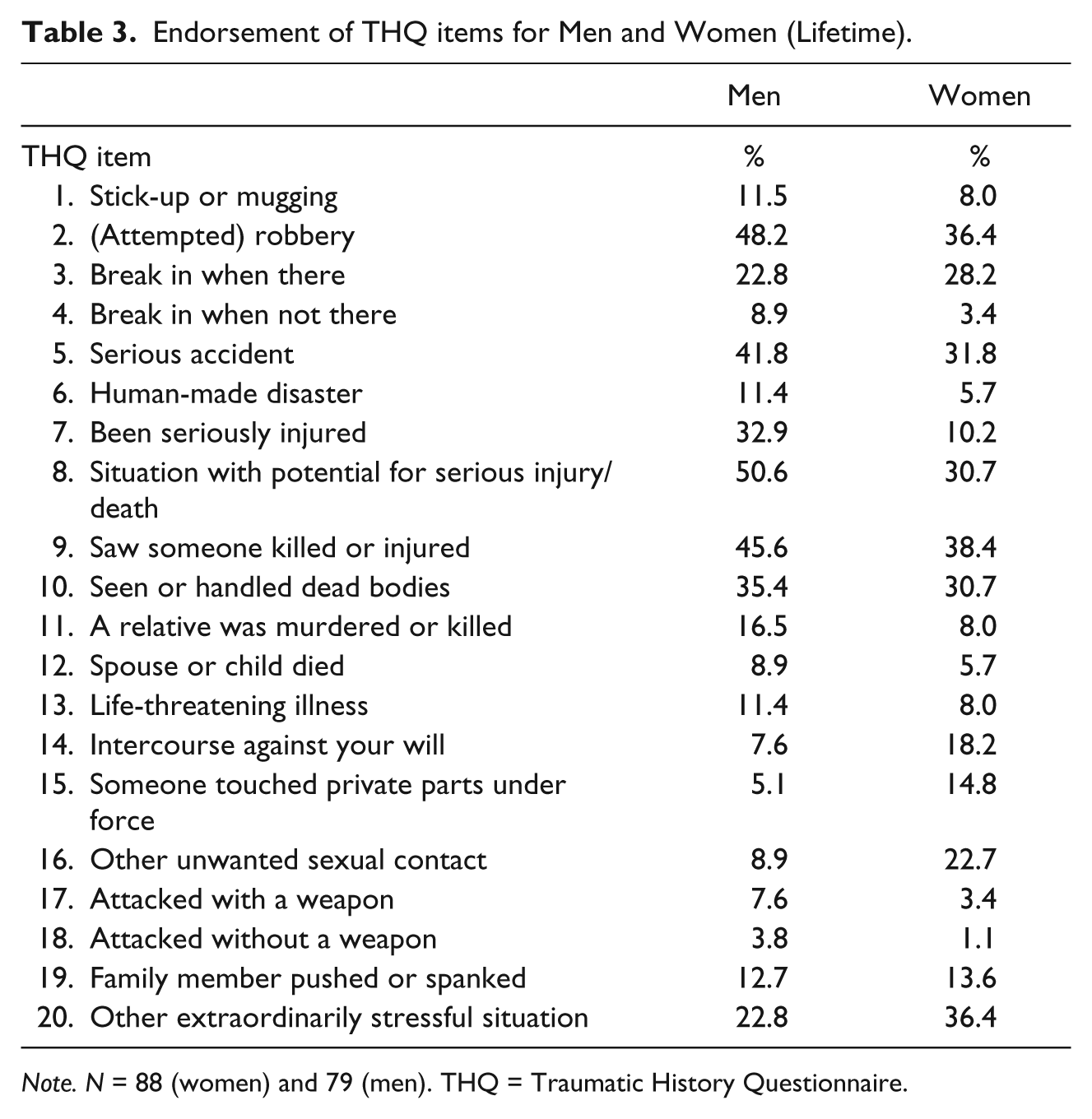
Note. N = 88 (women) and 79 (men). THQ = Traumatic History Questionnaire.
Correlations Between THQ Items and PCL Total.
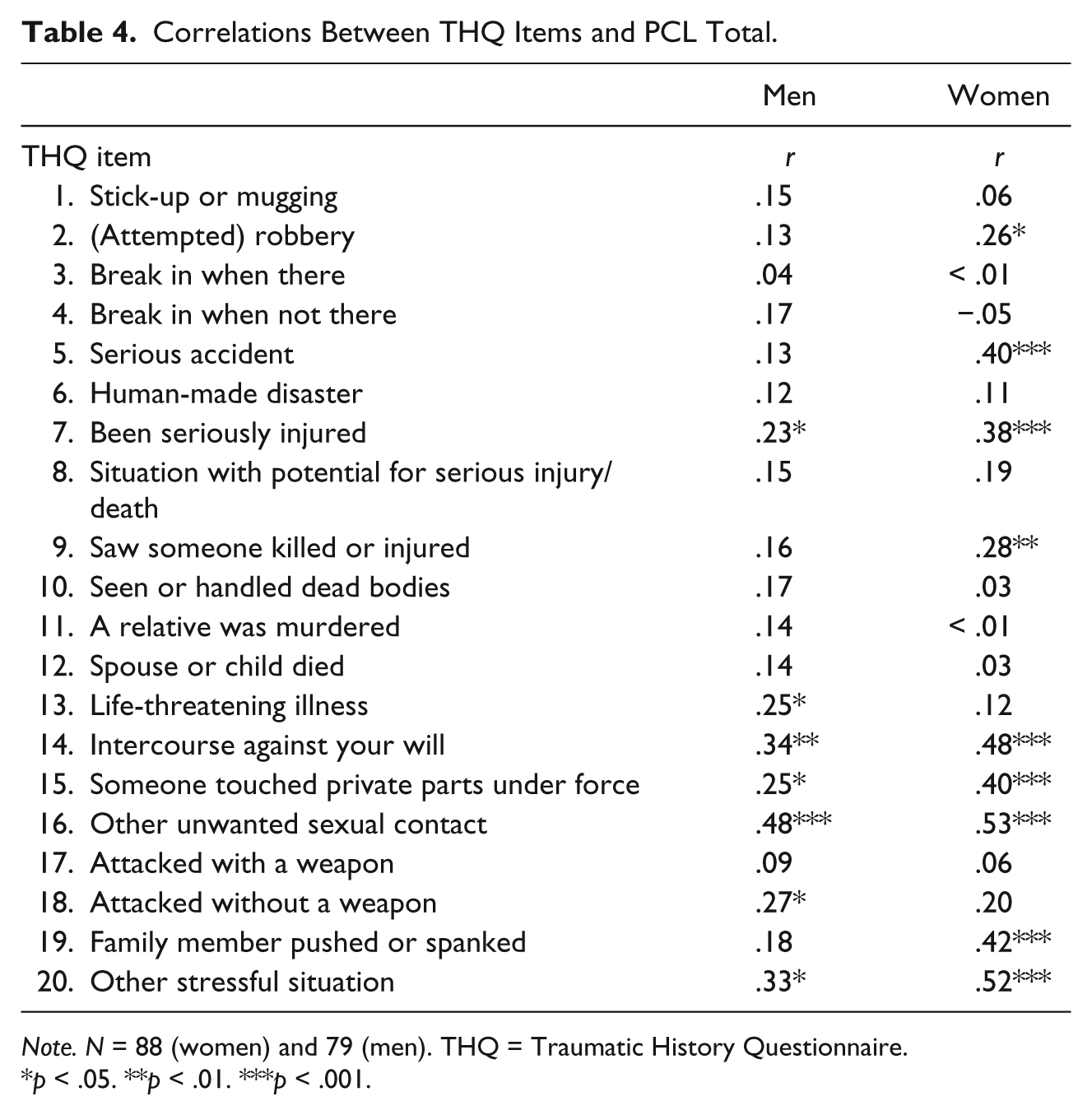
Note. N = 88 (women) and 79 (men). THQ = Traumatic History Questionnaire.
p < .05. **p < .01. ***p < .001.
Depression
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) was included as a covariate in the current study because PTS symptoms are often comorbid with depression (e.g., Labbate et al., 2004). The CES-D measures individuals’ depressive symptoms in the past week. The CES-D contains 20 items and each item is scored on a scale from 0 to 3, representing the frequency of each symptom experienced (Radloff, 1977). Some examples of the items on the CES-D are, “I felt hopeful about the future,” and “I felt that everything I did was an effort.” In the current study, the CES-D displayed excellent reliability, indicated by Cronbach’s alpha of .87 for men and .90 for women. Means and SDs are displayed in Tables 1 and 2; 16.5% of men and 14.8% of women scored above the cutoff score of 16 on the CES-D. The suggested cutoff of 16 reflects a potentially clinical level of depression, although this scale was designed to measure depression symptoms in the general population rather than to provide a definite diagnosis (Radloff, 1977).
Infant health and care
Infant health and care was measured by the Infant Health and Care Arrangements Scale (IHC, Punamäki et al., 2006). This is an 11-item measure that asks questions about health and care practices in the first year of parenthood, such as whether the baby was breastfed at 6 months of age and frequency of common infections in the first year of life. Some questions from the IHC were used in post hoc analyses to examine the association between breastfeeding and alcohol use in women.
Results
Prior to conducting analyses, diagnostics were performed on all measures, including checking for outliers, missing data, and abnormal kurtosis and distribution. Several variables were significantly positively skewed, and contained outliers more than two standard deviations from the mean. To improve the normality of these skewed variables, significant outliers were recoded to be one unit larger than the next largest response (Tabachnick & Fidell, 2007).
Next, the associations between the outcome variable (relationship satisfaction) and possible demographic covariates (i.e., age, income) were tested through bivariate correlations and one-way ANOVA. No demographic variables were significantly related to relationship satisfaction. Relationship satisfaction during pregnancy (collected during the previous wave of data collection) was originally included as covariate in the model, but was not significant in multivariate analyses. Thus, it was removed from the model. The only covariate included in this study was depression, measured by CES-D.
As expected, preliminary zero-order correlations (Tables 1 and 2) demonstrated that PTS symptoms for men and women were associated with a greater likelihood of a history of trauma as well as more current symptoms of depression. Also as expected, PTS symptoms were associated with higher rates of experiencing physical IPV for men and women, and with greater experiencing of psychological IPV for men only. An unexpected finding, however, was that PTS symptoms were not significantly associated with levels of harmful drinking for either gender. However, women’s rates of drinking were quite low. We examined the association between alcohol use and breastfeeding via a question on the Infant Healthcare Arrangement measure (Punamaki et al., 2006), which asked whether or not the women breastfed at 6 months postpartum. The alcohol use was not related to this measure. Finally, PTS symptoms and experiencing psychological IPV were significantly negatively related to the outcome variable of relationship satisfaction for men and women, whereas harmful drinking was not.
The Link Between PTS Symptoms and Relationship Satisfaction
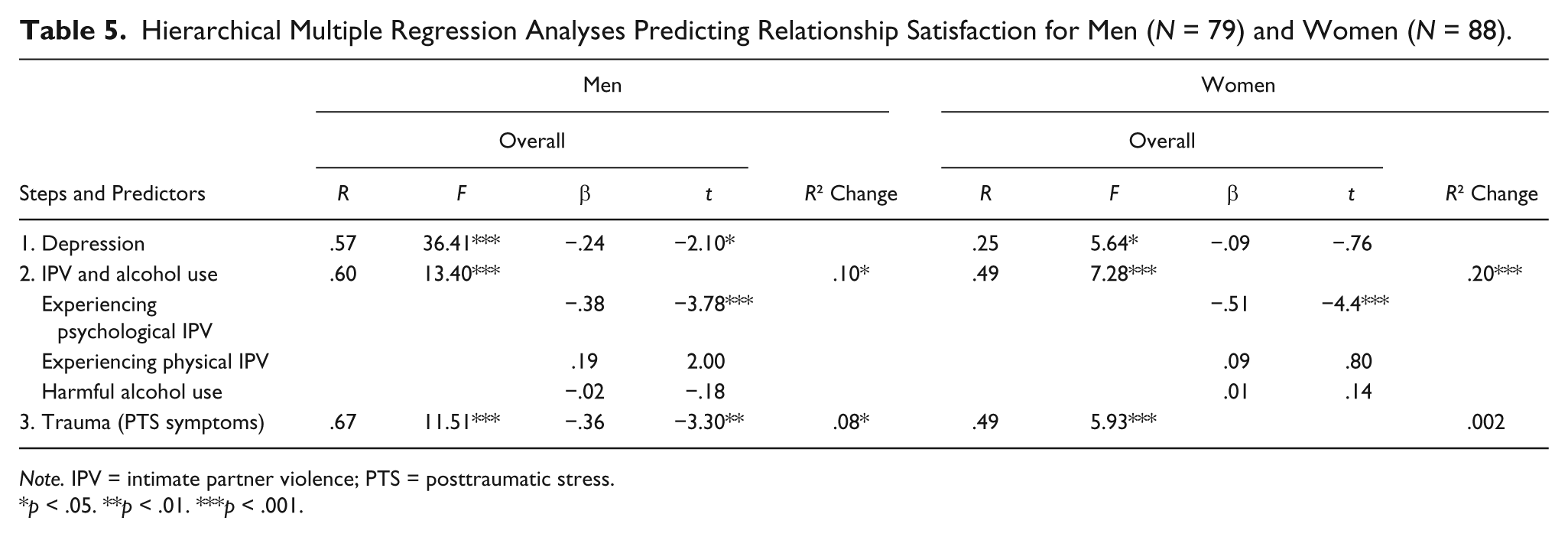
To test the first hypothesis that PTS symptoms would be associated with relationship satisfaction above and beyond the influence of experiencing IPV and harmful drinking, and after controlling for symptoms of depression, separate hierarchical multiple regressions were performed for each gender with relationship satisfaction as the outcome variable (see Table 5). From here on, when we refer to IPV, we are referring to the participants’ experience of IPV, not perpetration of IPV. Depression was entered in the first block. Harmful drinking, experiencing psychological IPV, and physical IPV were entered in the second block; and PTS symptoms were entered in the third block.
Hierarchical Multiple Regression Analyses Predicting Relationship Satisfaction for Men (N = 79) and Women (N = 88).
Note. IPV = intimate partner violence; PTS = posttraumatic stress.
p < .05. **p < .01. ***p < .001.
For men, PTS symptoms accounted for significant additional variance in relationship satisfaction (β = −.40, p < .001) above and beyond depression, IPV, and alcohol use (R2Δ = .10, p < .05; see Table 5). Depression and experiencing psychological IPV also remained significant predictors of self relationship satisfaction with PTS symptoms included in the model (β = −.24, p < .05 and β = −.38, p < .001, respectively). This suggests that PTS symptoms, depression, and experiencing psychological IPV are all uniquely associated with men’s relationship satisfaction.
For women, the results did not support the first hypothesis (see Table 5). PTS symptoms did not predict women’s relationship satisfaction when experiencing IPV and harmful drinking were controlled for (β = −.51, p < .001) and the R2 change was not significant in the third block. In contrast, experiencing psychological IPV was the most robust multivariate predictor of women’s relationship satisfaction. A nonsignificant post hoc t test conducted between men and women, t(165) = −1.72, p > .05, suggested that gender differences in PTS symptoms cannot explain these results.
The Interaction Between Risk Factors and Relationship Satisfaction
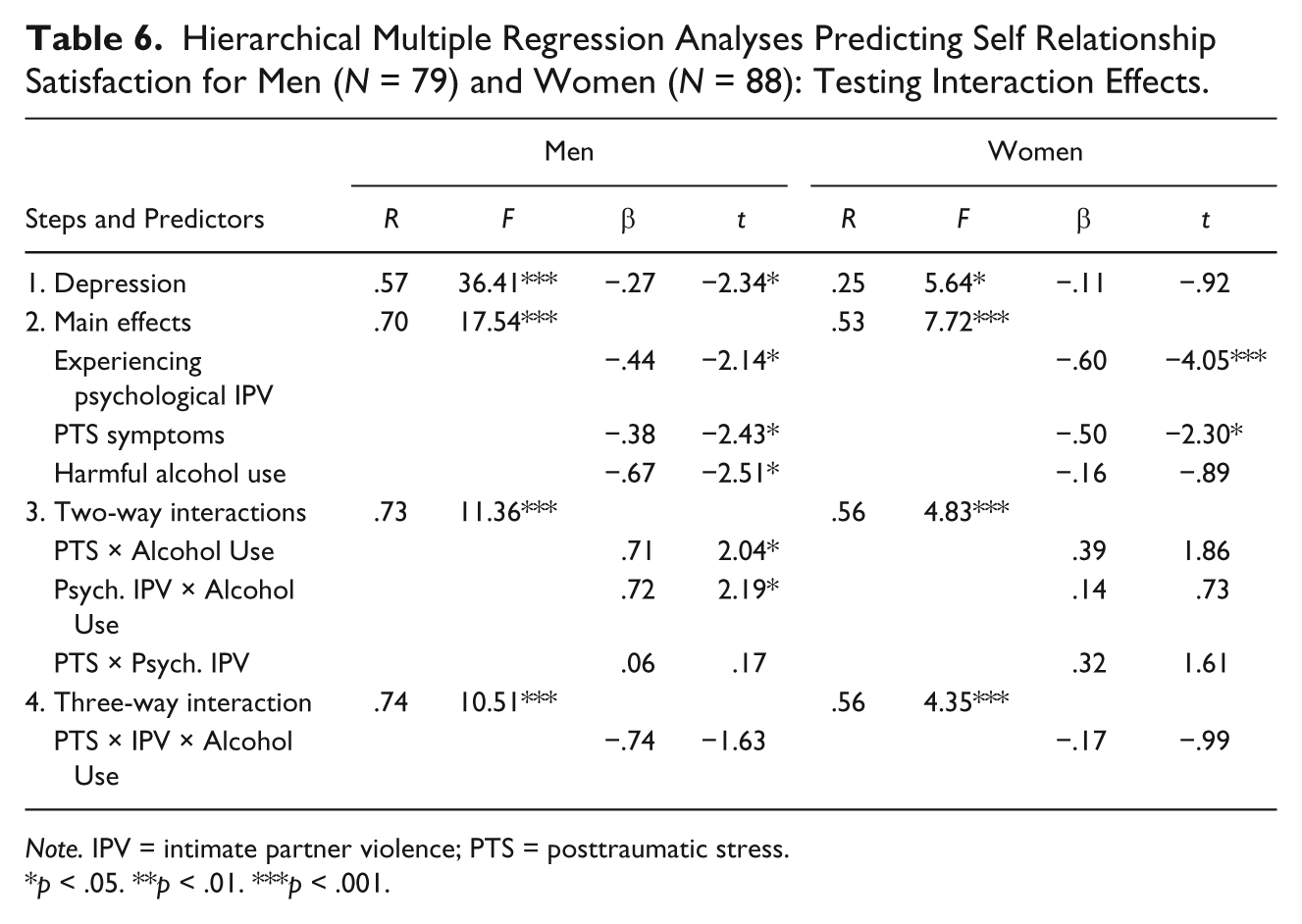
To investigate the second hypothesis that experiencing IPV, harmful drinking, and PTS symptoms will interact to predict lower relationship satisfaction, all two-way and three-way interaction terms were tested in separate regression analyses for each gender. Because experiencing physical IPV was not related to relationship satisfaction for either men or women, only psychological IPV was examined in the moderation analyses.
For men, the three-way interaction term was not statistically significant (Table 6). There were, however, two significant two-way effects involving the interaction between harmful drinking and PTS symptoms as well as the interaction between harmful drinking and experiencing psychological IPV. An examination of the simple means indicated that the combination of high PTS symptoms and high harmful drinking was associated with particularly low relationship satisfaction, as was the combination of experiencing high levels of psychological IPV and high harmful drinking. Thus, for men, the second hypothesis was partially supported in that harmful drinking in particular appeared to exacerbate the risk of relationship dissatisfaction in combination with either PTS symptoms or experiencing psychological IPV.
Hierarchical Multiple Regression Analyses Predicting Self Relationship Satisfaction for Men (N = 79) and Women (N = 88): Testing Interaction Effects.
Note. IPV = intimate partner violence; PTS = posttraumatic stress.
p < .05. **p < .01. ***p < .001.
For women, none of the two-way or three-way interaction terms were statistically significant (Table 6). Instead, psychological IPV victimization was the strongest multivariate predictor of women’s relationship satisfaction.
Discussion
To our knowledge, this is the first study to test the direct and interactive associations between relationship satisfaction and harmful drinking, experience of IPV, and PTS symptoms during the first year of parenthood. As such, this study provides new information about this unique period in the lifespan. The results support some of the existing literature and provide novel information, especially with regard to gender differences in how men’s and women’s relationship satisfaction is affected by PTS symptoms and harmful drinking.
In the current study, men’s and women’s PTS symptoms were associated with their own lower relationship satisfaction, which is consistent with previous literature (e.g., Parfitt & Ayers, 2009). Indeed, men’s PTS symptoms continued to be related to lower relationship satisfaction even after controlling for symptoms of depression and experiences of psychological IPV. This is a noteworthy and novel finding, and suggests that men’s perceptions of their intimate relationships may be particularly vulnerable to experiences of PTS. The research literature on how PTS symptoms affect men is often restricted to veteran populations or examines the effects that PTS symptoms have on individual functioning, such as physical and mental health, rather than relationship functioning (e.g., Taft, Street, Marshall, Dowdall, & Riggs, 2007).
In contrast, the finding that women’s satisfaction in this study appeared to be primarily related to experiencing psychological IPV was an unexpected finding, but is consistent with past research indicating that psychological IPV is one of the most robust predictors of relationship satisfaction, over and above substance misuse (e.g., Taft et al., 2006). Furthermore, experiencing psychological IPV may be particularly detrimental to women’s overall well-being (e.g., Blasco-Ros et al., 2010). However, this result contradicts the research literature that asserts that women are more negatively affected by PTS symptoms than men (e.g., Ditlevsen & Elklit, 2010). As there was no statistically significant difference between overall PTS symptoms for men and women, this gender difference is likely not to be due to simple differences in amount or severity of PTS symptoms between, but is possibly a result of a different interpretation of or threshold for such symptoms by, men and women. It is possible that, in relation to satisfaction in one’s intimate relationship, men may be more negatively affected by PTS symptoms than women. For example, there may be a difference in the way men and women cope with sexual trauma. Considering the lack of research, information, and services about men’s sexual trauma in particular (Monson et al., 2009), it is possible that it is more difficult for men to cope with PTS symptoms related to sexual rather than physical or psychological trauma. However, such explanations need to be tested in future research.
For men, PTS symptoms also interacted with harmful drinking to predict particularly low relationship satisfaction, which is a novel finding. Specifically, these results suggest that men’s relationship satisfaction may be especially susceptible to the negative effects of PTS symptoms if the men are also misusing alcohol. There are several reasons why the link between PTS symptoms and harmful drinking can be particularly detrimental to intimate relationships. For example, individuals with PTS symptoms are at particular risk for harmful drinking because one or two alcoholic drinks can actually temporarily decrease anxiety-related PTS symptoms (e.g., Savage, Quiros, Dodd, & Bonavota, 2007). If individuals experience this relief and believe that it is due to alcohol, then they are likely to keep drinking. However, having two or more drinks has been associated with an increase of PTS symptoms, such as flashbacks and feelings of guilt (e.g., Savage et al., 2007). Many people may not realize the complexity of the relationship between the amount of alcohol consumed and PTS symptoms, and may continue to use alcohol to cope with PTS, thus creating a habit or dependence on a substance that can actually exacerbate their mental health symptoms and general well-being. When considering prevention and intervention efforts with new fathers, it may be particularly important to pay attention to how they may be coping with prior experiences of trauma and/or symptoms of PTS, to help them develop and maintain healthy coping strategies while preventing harmful drinking.
Strengths and Limitations
This study’s focus on the first year of parenthood is a particular strength, as most of the research conducted with couples does not include couples who have young children or does not focus exclusively on couples who are new parents. Furthermore, this study examined reports from both partners, which enhances the validity of the data as it minimizes the issue of underreporting. Finally, this study builds on previous research by examining the link between PTS symptoms and relationship satisfaction in the context of other possibly interrelated risk factors. Several theoretical models of relationship functioning (which includes relationship satisfaction) posit that individual vulnerabilities (e.g., PTS) likely interact with dyadic functioning (e.g., IPV) to influence relationship outcomes (e.g., the VSA Model; Karney & Bradbury, 1995), however, this is the first study that we know of that has explicitly examined the interaction between PTS symptoms and other individual and dyadic characteristics. For an illustration of the VSA model, see Figure 1.
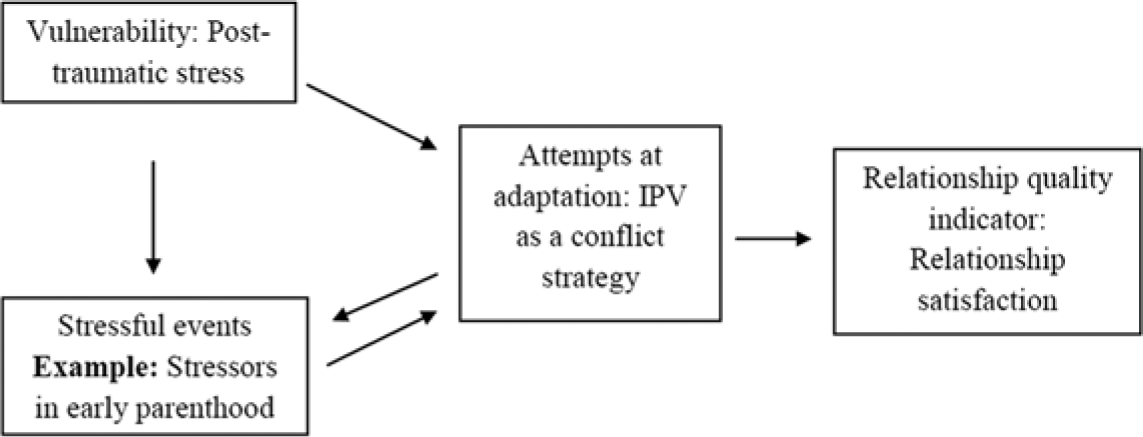
Vulnerability-stress-adaptation model.
This study also contains a number of limitations. First, the cross-sectional design does not permit us to analyze how relationship satisfaction may be affected over time and future research is needed to understand the longitudinal and possible reciprocal influences between PTS symptoms and relationship satisfaction. The cross-sectional design of this study precludes conclusions about causation. Second, our focus on the first year of parenthood may have affected the psychometric properties of some of the measures, most notably AUDIT for women. This did not appear to be related to whether women were breastfeeding at the time. It is possible that harmful drinking may be an important interactive factor for women at other points in the lifespan. In addition, the prevalence and range of physical IPV was substantially lower and associated with a more narrow range when compared with psychological IPV, which may have been an artifact of the developmental period. Although other studies have found a similar pattern of results with regard to how physical versus psychological IPV affects relationship satisfaction (e.g., Moore, Elkins, McNulty, Kivisto, & Handsel, 2011), this difference in incidence and range may have affected the study results. Third, we were not able to measure sexual IPV or history of sexual trauma due to the low reliability of the measures. Fourth, there were also a number of limitations associated with the trauma-related measures used in this study. For instance, there was no way to determine which event(s) the participants referred to when they filled out the PCL or whether PTS symptoms were related to current IPV, which precludes conclusions about what type of traumatic events are more likely to be associated with PTS symptoms or relationship discord. In addition, the PCL was the only measure of PTS symptoms, thus limiting the study’s conclusions about clinical levels of PTS symptoms or presence of PTSD diagnosis. Considering these limitations, the results may not generalize to persons experiencing severe PTS symptoms or complex PTSD. Finally, our sample was composed of largely middle-class couples and the rate of education attainment was high. Although the ethnic diversity of our sample reflected the diversity of the geographical area where the data were collected, the results of this study may not generalize to couples and families in poverty or with lower overall educational attainment.
Implications for Research and Intervention
Such research can further our understanding of how specific combinations of risk factors can be addressed with tailored, evidence-based prevention and intervention strategies. There is research showing success in using prevention techniques specific to the population instead of relying on techniques that buffer relationship satisfaction only (e.g., Monson et al., 2008; Rynerson & Fishel, 1993). Furthermore, tailoring interventions to specific populations, such as couples in which at least one partner has been diagnosed with PTSD, can improve the results of the intervention because it allows the service providers to address issues that are unique to a particular population (Monson et al., 2008). In addition, the results of this research can be used to help identify couples and families at highest risk for severe mental health and relational difficulties. Identifying at-risk couples and families in an accurate and timely fashion would allow for early intervention and would perhaps prevent escalation of certain mental health problems, such as harmful drinking.
In conclusion, this study opens many new avenues for future research. Studies that examine sexual aggression in new parents are needed, as sexual trauma and violence are phenomenologically different from psychological or physical traumas and violence (even though various forms of violence often co-occur), yet reliable measures of sexual trauma and sexual violence in intimate relationships are few. Longitudinal research that combines quantitative and qualitative methodology would be best suited to explaining the complex dynamics between partners’ alcohol misuse, experience of IPV, PTS symptoms, and relationship satisfaction. A particularly important finding of this study is that the relationship satisfaction of men and women in the same couple is related to different, albeit related, risk factors. The results strongly suggest that practitioners working with couples during the transition to parenthood need to adopt a gender-sensitive, yet comprehensive approach. Part of this approach would be to explore what risk factors are present in the relationship and how they are affecting each partner. Most importantly, it is imperative not to assume that partners of either gender will or will not have symptoms of PTS, or that partners of either gender will be more or less affected by PTS symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by Master’s Fellowship awarded by IMPART, CIHR to the first author.