
Abstract
Intimate partner violence (IPV) is a significant public health problem. It has far reaching consequences such as social and economic costs, as well as a negative impact on women’s health outcomes. This study assessed the relationship between IPV and health risk factors, health behaviors, and poor mental health in Missouri women utilizing 2005 Missouri Behavioral Risk Factor Surveillance System (BRFSS) data (n = 3,110). Moderators (demographic indicators) of the relationship between IPV and health risk factors (high blood pressure, high cholesterol, and obesity) and health behaviors (physical inactivity, smoking, and binge drinking) were also examined. Women with a history of IPV were more likely to engage in health-compromising behaviors such as smoking and binge drinking, be obese, and report more poor mental health days compared with women without a history of IPV. Demographic variables moderated the relationship between IPV, obesity, smoking, high blood pressure, and high cholesterol. These findings underscore the importance that clinics, community, or other health care settings can play in identifying women who are victims of or have a history of IPV and provide them with appropriate resources as well as targeted interventions to reduce morbidity in this population.
In the United States, intimate partner violence (IPV) is a significant public health burden, affecting the quality of life of women of all ages and socioeconomic statuses (SESs). According to the National Intimate Partner and Sexual Violence Survey (NISVS; Black et al., 2011), 35.6% of women have experienced violence by an intimate partner, which includes rape, physical violence, and/or stalking. Given the prevalence and scope of impact of IPV, this study focused on exploring the association between IPV and multiple domains of women’s physical health.
IPV has far reaching consequences; there are social and economic costs, as well as negative impacts on women’s health outcomes (World Health Organization [WHO], 2005). Women who have experienced IPV are more likely to suffer from acute physical injuries and require medical care for their injuries (Black, 2011). They may also suffer from chronic physical conditions (e.g., frequent headaches, chronic pain, insomnia, gastrointestinal problems; Black et al., 2011; WHO, 2005) and mental health concerns and related disorders (e.g., depression, posttraumatic stress disorder, eating disorders, and suicide attempts; Dillon, Hussain, Loxton, & Rahman, 2013; WHO, 2005). Women with a history of IPV are also more likely to report overall poorer health and quality of life (WHO, 2005).
Experiencing IPV may lead to negative health outcomes through engagement in health-damaging behaviors such as smoking, substance use, physical inactivity, and high-risk sexual behaviors (Breiding, Black, & Ryan, 2008; Centers for Disease Control and Prevention [CDC], 2008). These health-compromising behaviors are known risk factors for many chronic illnesses such as cardiovascular disease, diabetes, and asthma (American Heart Association, 2012).
Many women with a history of IPV are also at risk for increased mental health problems. Numerous studies have found a relationship between a history of IPV and depression, anxiety, posttraumatic stress disorder (PTSD), suicide, and self-harm (Dillon et al., 2013). Health-compromising behaviors mediate the relationship between mental health conditions and adverse health outcomes (Kaysen et al., 2008). For example, those with symptoms of depression or PTSD may consume excessive amounts of alcohol or smoke cigarettes to cope with the emotional distress associated with their symptoms.
It is well established that health disparities exist in the United States and that lower SES is a predictor of poorer health. Those with higher SES are more likely to have access to health care and live in less impoverished neighborhoods where there is less violence or environmental pollution, variables that are risk factors for chronic illnesses (Adler & Newman, 2002; Henry J. Kaiser Family Foundation, 2007). Previous research has also found that the prevalence of IPV varies by socioeconomic indicators. According to the CDC, risk factors for IPV include younger age, lower educational attainment, low income, and unemployment (CDC, 2013a). Women of lower SES may be at an increased risk for IPV for various reasons, such as financial dependence on their abuser. These women are also more likely to have less education and may lack the resources to leave an abusive relationship. Given that SES is associated with health status and IPV victimization, the relationship between IPV and health outcomes may be moderated by SES (e.g., association between IPV and poor health may vary by level of educational attainment or employment status).
Given the disparities in health outcomes, the high prevalence of IPV and low SES as a risk factor for IPV and poorer health, it is important to examine the relationships among these factors. As previously stated, studies have found that IPV is associated with adverse health outcomes. However, many of these studies used clinical or community samples often of a smaller sample size, limiting generalizability of findings. Other studies utilized data from population-based health surveys such as the Behavioral Risk Factor Surveillance System (BRFSS) to examine the relationship between a lifetime history of IPV (physical and sexual violence), health behaviors, and health outcomes. These studies examined BRFSS data from multiple states or individual states (e.g., Breiding et al., 2008; Cloutier, Martin & Poole, 2002).
Given that populations vary by state, examining the impact of IPV on health outcomes at the individual state level is important to help local agencies develop and implement public health interventions that address the specific needs of the given population (Beitsch, Brooks, Grigg, & Menachemi, 2006). According to the CDC, state-level BRFSS data have provided state officials and policy makers with a better understanding of the scope of the problem of intimate partner and sexual violence in their states as well as information that may be used to guide public policy (CDC, 2014a). With regard to Missouri specifically, we have chosen to explore the association between IPV and health behaviors that carry a disproportionate health burden for this region. For example, obesity is a significant public health problem for the state as the number of obese individuals is slightly greater than the national average (CDC, 2015a). Furthermore, Missouri ranks no. 16 in the United States with regard to percentage of obese adults in the population. The number of smokers is also higher in Missouri compared with the national average (CDC, 2013b). Given that there has been previous research finding a relationship between obesity, smoking, and IPV, it is important to assess whether these relationships exists among Missouri women, and if so, developing targeted interventions to help these women is necessary. Poverty is also a significant problem in the state of Missouri with approximately 50 of the 114 counties (45%) having poverty rates between 19.7% and 36.3% (Missouri Census Data Center, 2015). Moreover, the number of reported violent crimes in the state (e.g., murder, robbery, aggravated assault) is slightly higher than the national average (U.S. Census Bureau, 2012). IPV is considered a violent crime, and lower SES (i.e., those who are poor or with lower education) is associated with increased risk for IPV (CDC, 2013a). Communities and individuals will need more resources to help stem these problems.
The goal of this study is to extend previous findings by describing the prevalence of IPV utilizing BRFSS data for the state of Missouri and examining the association within multiple domains of health. Specifically, we hypothesized the following:
Method
Data Collection and Participants
The 2005 BRFSS data for the state of Missouri were utilized for this secondary data analysis. The BRFSS is supported by the CDC and is an ongoing, cross-sectional, random-digit telephone survey collected at the state/territory level. It assesses health conditions, health behaviors, and behavioral risk factors among non-institutionalized adults over the age of 18. The BRFSS has a set of core questions that every state is required to ask; however, the questions regarding IPV are part of an optional module. Thus, only 16 states and 2 territories elected to administer this module in 2005, with Missouri as one of the states. Therefore, a comprehensive, national data set available to examine IPV and health outcomes does not exist for 2005 or in other years of the BRFSS. The data for Missouri include 5,164 respondents; however, analysis was restricted to females aged 18 to 89 (n = 3,110). The 2005 BRFSS data set was chosen because it was the only year in which IPV was assessed in the state of Missouri. The Saint Louis University Institutional Review Board provided a formal written waiver for the current study as a publicly available, anonymous, secondary data were used in the analysis which does not require IRB oversight.
Measures
Demographics
Demographic characteristics included age, race/ethnicity, marital status, education, annual household income, and employment status.
IPV
The BRFSS defines an intimate partner as a current or former spouse, boyfriend, or girlfriend. Women were identified as having a lifetime history of IPV if they ever experienced any of the following: threatened, attempted, or completed physical violence (which includes threatening to hit, slap, push, kick, or physically hurt them in any way) and/or unwanted sex by a current or former intimate partner.
Health risk factors
Health risk factors of interest included high cholesterol, high blood pressure, and overweight/obesity; each outcome was categorized as a dichotomous variable. All diagnoses were self-reported; participants were categorized as having the condition if they had ever been told by a doctor, nurse, or health professional that they had any of the above conditions. Overweight and obesity were previously determined in the BRFSS data set based on calculated body mass index (BMI), with 25 < BMI < 29.9 as overweight, and BMI ≥ 30 as obese.
Poor mental health
Poor mental health was determined based on responses to the question, “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” A response of 14 days or more was used to define poor mental health, consistent with prior research as well as diagnostic criteria for clinical depression and anxiety (CDC, 1998).
Health-compromising behaviors
Behaviors of interest were physical activity, binge drinking, and cigarette smoking.
Physical activity
The BRFSS previously calculated a dichotomous variable to assess whether participants met CDC recommendations for engaging in moderate or vigorous physical activity. Moderate activity includes brisk walking, bicycling, or anything else that causes an increase in breathing or heart rate, for ≥30 min per day for ≥5 days/week. Vigorous activity includes running, aerobics, or anything else that causes large increases in breathing or heart rate for ≥20 min per day on ≥3 days/week.
Binge drinking
Binge drinking was previously calculated in the BRFSS data set as a dichotomous variable that identifies participants who consumed ≥5 alcoholic drinks on at least one occasion in the 30 days prior to the survey.
Cigarette smoking
The BRFSS previously calculated a dichotomous variable to assess whether participants were current smokers. Cigarette smokers were identified as those who reported they have smoked at least 100 cigarettes in their entire life and currently smoke cigarettes daily or on some days. Those who never smoked cigarettes or who were former smokers are considered non-smokers by BRFSS.
Statistical Analysis
Data were analyzed utilizing SPSS v.20 statistical software. Because of the complex sampling method of the BRFSS, the SPSS Complex Samples module was utilized to account for sampling weights. More information regarding the SPSS Complex Samples module can be found on the IBM website (ftp://ftp.software.ibm.com/software/analytics/spss/documentation/statistics/20.0/en/client/Manuals/IBM_SPSS_Complex_Samples.pdf). The 2005 BRFSS used post-stratification to weight the data on age, race and ethnicity, sex, and geographic region. All analyses used α < .05 to determine statistical significance.
Chi-square analyses were utilized to assess for demographic indicators, health risk factors, and health behaviors associated with IPV. Logistic regression analyses examined the association between health risk factors, health behaviors, mental health, and IPV while adjusting for demographics (age, race/ethnicity, marital status, and employment status). Demographic indicators (age, race/ethnicity, marital status, and employment status) were then assessed as moderators of the relationship between a history of IPV and health risk factors and health behaviors.
Results
IPV and Demographic Characteristics
Differences in demographic characteristics were observed between women with and without a history of IPV. A greater portion of women with a history of IPV were younger (between 18 and 54 years), divorced, and unable to work compared with women without a history of IPV (Table 1).
Demographic Characteristics by History of IPV.
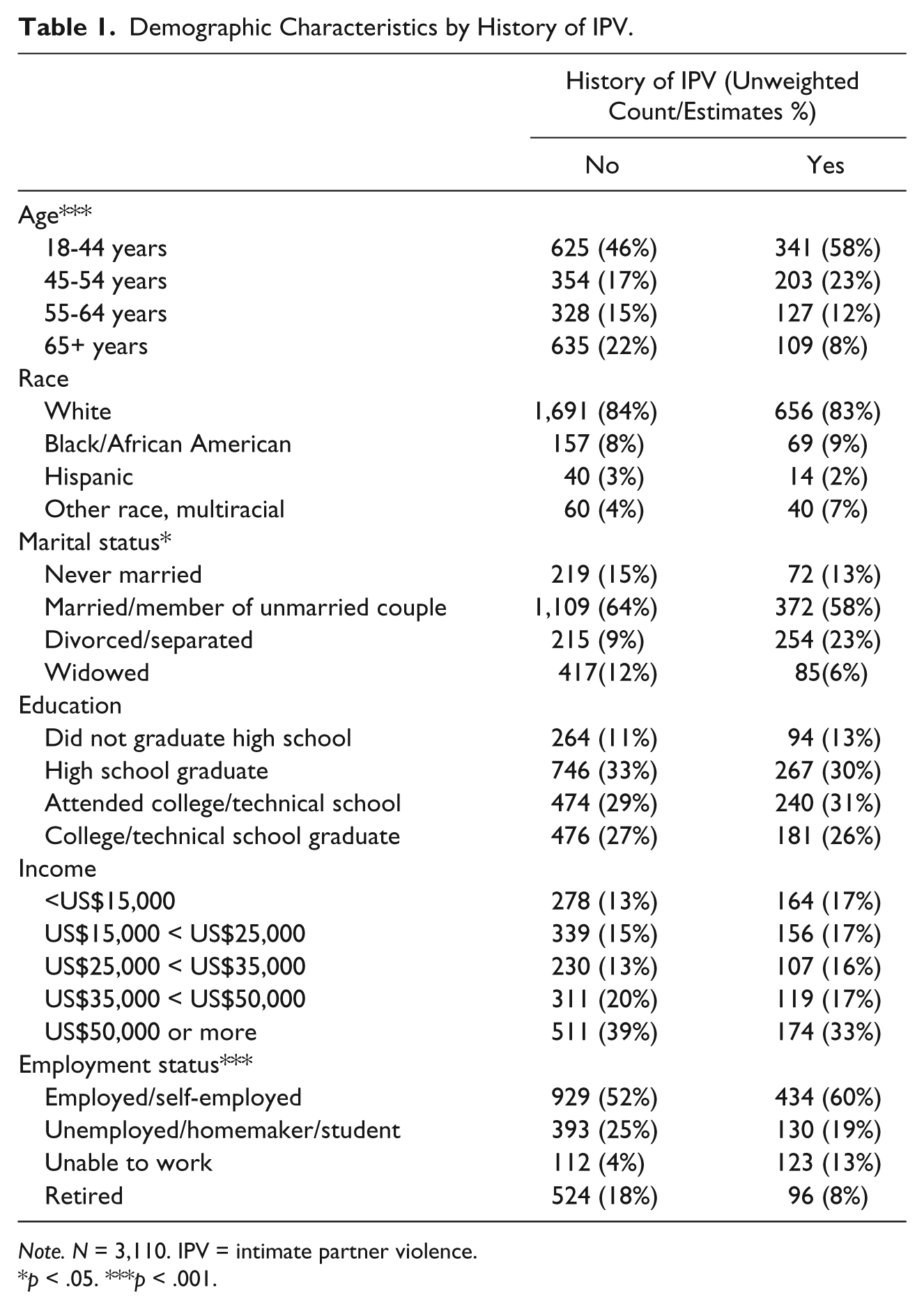
Note. N = 3,110. IPV = intimate partner violence.
p < .05. ***p < .001.
IPV and Health Outcomes and Health Behaviors
There were significant differences in health risk factors and health behaviors between women with and without a history of IPV. Those with a history of IPV were significantly more likely to be overweight, current smokers, binge drinkers, and report poor mental health (Table 2). Adjusted logistic regression models (Table 3) indicated that women with a history of IPV were approximately 2 times as likely to be current smokers, binge drinkers, and report poor mental health (p < .05). They were also 1.4 times as likely to be obese compared with women without a history of IPV (p < .05).
Health Risk Factors and Health Behaviors by IPV Status.
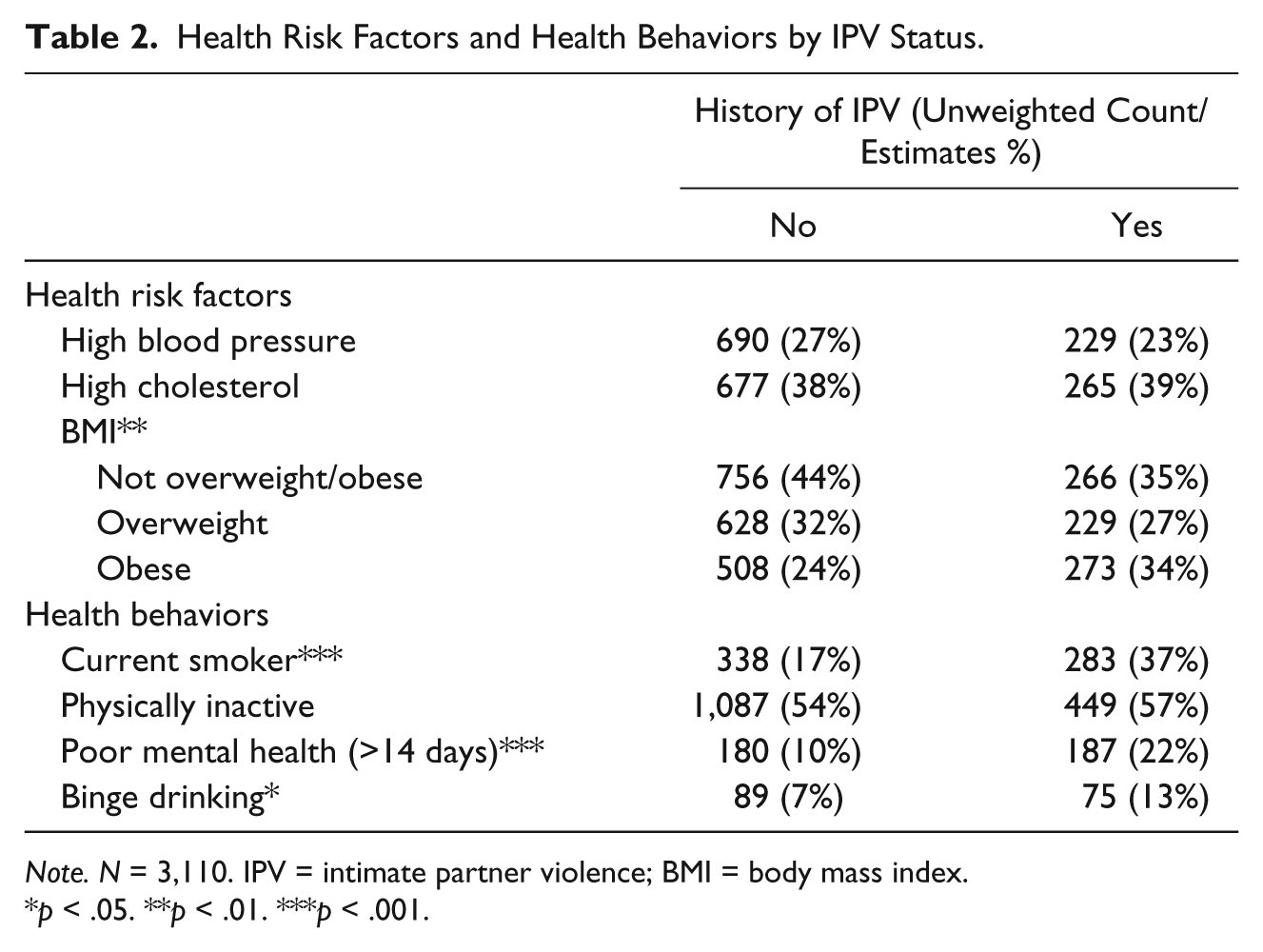
Note. N = 3,110. IPV = intimate partner violence; BMI = body mass index.
p < .05. **p < .01. ***p < .001.
Association Between Lifetime History of IPV and Health Risk Factors/Health Behaviors.
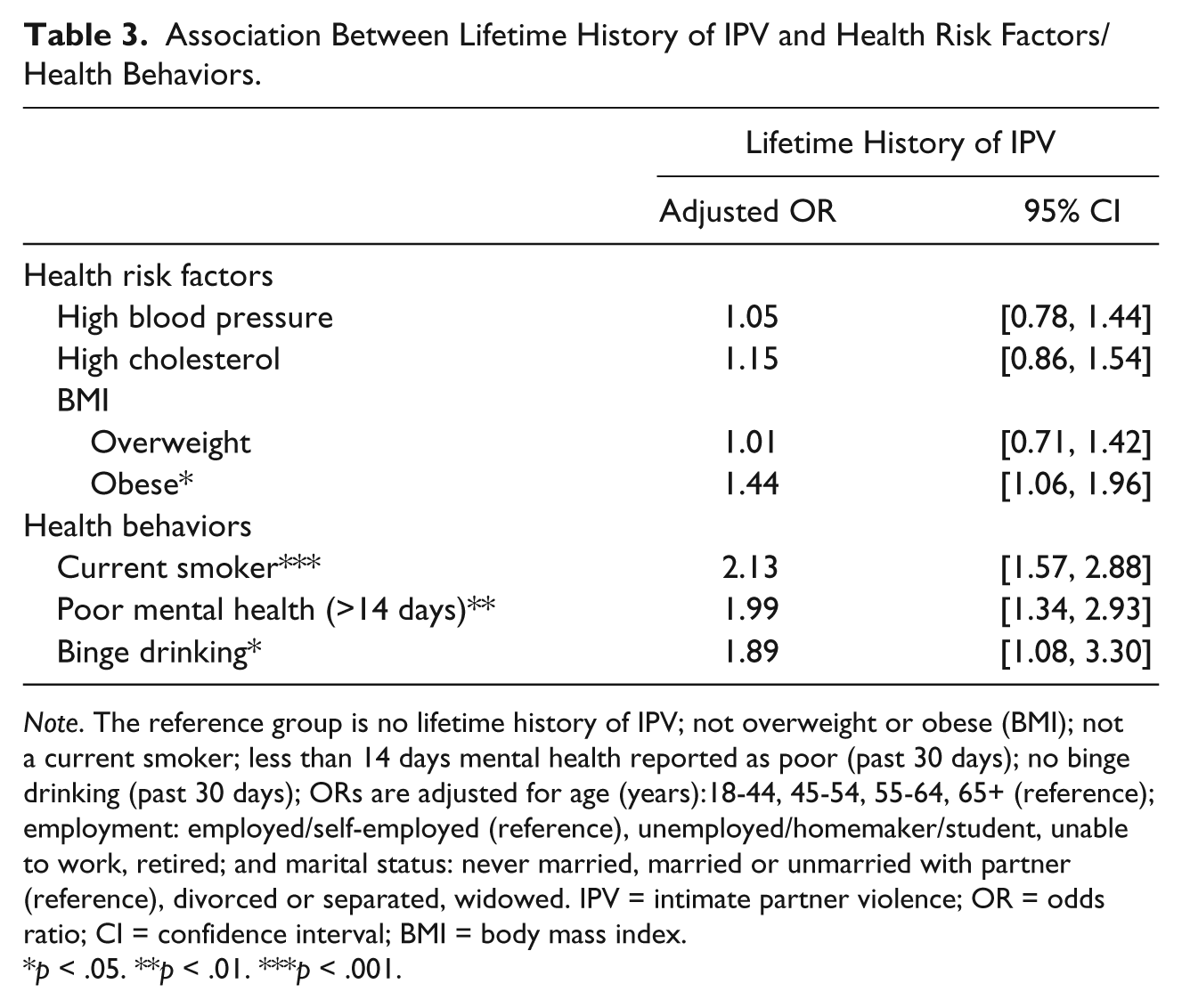
Note. The reference group is no lifetime history of IPV; not overweight or obese (BMI); not a current smoker; less than 14 days mental health reported as poor (past 30 days); no binge drinking (past 30 days); ORs are adjusted for age (years):18-44, 45-54, 55-64, 65+ (reference); employment: employed/self-employed (reference), unemployed/homemaker/student, unable to work, retired; and marital status: never married, married or unmarried with partner (reference), divorced or separated, widowed. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval; BMI = body mass index.
p < .05. **p < .01. ***p < .001.
Interactions
There were significant interactions between history of IPV and demographic variables for smoking, obesity, high cholesterol, and high blood pressure (Table 4). The interaction between history of IPV and employment status was significantly related to almost all health risk factors. Specifically, those who were unable to work with a history of IPV were approximately 3 times as likely to be diagnosed with high blood pressure and high cholesterol (p < .05) compared with those who were employed or self-employed with a history of IPV. Those with a history of IPV and unable to work were 2 times as likely to be obese (p < .05) compared with those who were employed or self-employed. There was also a significant interaction between younger age and a history of IPV and smoking status. Women between the ages of 18 and 54 with a history of IPV were about 4 times as likely to be current smokers (p < .01) than women over the age of 65 with a history of IPV. However, these women were less likely to be diagnosed with high blood pressure or high cholesterol (p < .01). Interactions of IPV and demographic variables for mental health and binge drinking were also examined and were significant but given the small sample sizes, they were not included in the models.
Adjusted ORs and 95% CIs of Significant Interactions Between History of IPV and Demographic Variables for Health Outcomes and Health Behaviors.

Note. All models adjusted for age, race/ethnicity, marital status, and employment status. Variables in the interaction term were not included separately in the respective model. OR = odds ratios; IPV = intimate partner violence; BMI = body mass index; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Discussion
The aim of this study was to examine the association between health risk factors and health behaviors in Missouri women with a history of IPV. Consistent with previous studies, history of IPV was significantly associated with obesity, smoking, binge drinking, and poor mental health (Breiding et al., 2008; Cloutier et al., 2002; Coker, Smith, Bethea, King, & McKeown, 2000). Unlike previous studies, no significant associations were found between IPV and high blood pressure and high cholesterol. However, the strong associations between IPV and obesity, smoking, binge drinking, and poor mental health may suggest that these women are engaging in health risk behaviors that are known risk factors for high blood pressure and high cholesterol (CDC, 2014b, 2015b). Therefore, although there was not a significant association between IPV and high blood pressure and high cholesterol in this sample, by continuing their engagement in health risk behaviors such as smoking, or being obese, women are increasing their risk for developing high blood pressure and high cholesterol, which can lead to other chronic health conditions. Importantly, obesity, smoking, binge drinking, and poor mental health are modifiable, and proper intervention (e.g., exercise, smoking cessation programs, or psychotherapy) can prevent the development of adverse health outcomes in women with a history of IPV.
The inability to work was a significant moderator of IPV and health risk factors. When the interaction of IPV and employment status was added to the model, significant relationships emerged between that interaction term and high blood pressure and high cholesterol. A greater proportion of women with a history of IPV (14%) reported that they were unable to work, compared with 3% of women in the sample without a history of IPV. Women with a history of IPV were more likely to report current activity limitations due to physical, mental, or emotional problems, which can consequently affect their ability to work (CDC, 2008). Other studies have found that women with a history of IPV had difficulty maintaining stable employment, and this was mediated by health outcomes (Staggs & Riger, 2005). The finding from the present study suggests that women with a lifetime history of IPV may be physically or mentally unable to work, which may be a sequela of the violence. Many women who experience IPV are also injured. Although rates of injury within the present study are unknown, studies have found that approximately 40% of women are injured as a result of IPV (Tjaden & Theonnes, 2000; WHO, 2013). The women in the present study may have received severe injuries or multiple, less severe injuries over time (Heise & Garcia-Moreno, 2002; Tjaden & Theonnes, 2000), which could lead to functional impairment, deeming them unable to work. It is also possible that aside from or in conjunction with physical injuries, these women are also struggling with mental health issues that are affecting their ability to obtain or maintain employment. Studies have found that women who have experienced IPV are 2 to 3 times more as likely to experience mental health disability, which affects their ability to perform their normal daily activities such as maintaining employment (Carbone-Lopez, Kruttschnitt, & Macmillan, 2006; Lindhorst, Oxford, & Gillmore, 2007). Given the cross-sectional nature of these data, it is also possible that women who are unable to work may be more vulnerable to experiencing IPV. Women who are unable to work may have disabilities that prevent them from being employed. Research examining the association between disability and IPV has found that those with a disability are more likely to report lifetime IPV, report poorer health status, and engage in more health risk behaviors (Mitra & Mouradian, 2014). The results for employment status moderating the relationship between IPV and health risk factors provide a clearer picture when examining outcomes that were not statistically significant in the logistic regression analyses without the interaction terms. It suggests that there could be other factors influencing the relationship between IPV and health outcomes. More specifically, these results illustrate the impact of IPV on multiple domains of women’s lives (i.e., physical, emotional, and social well-being). Furthermore, these findings are consistent with the idea that disease is multifactorial, that is, health conditions often have multiple risk factors. These risk factors interact in complex ways and may negatively affect one another as in the concept of risk factor caravans proposed by Layne, Briggs, and Courtois (2014). Risk factor caravans can be conceptualized as a constellation of risk factors that occur or co-occur, “travel” with the individual over time, and increase susceptibility to other adverse risk factors or adverse outcomes (Layne et al., 2014). For example, the relationship between smoking, obesity, binge drinking, and IPV have been found in numerous studies, including the present study. These health behaviors are also commonly the same constellation of risk factors for various chronic conditions such as diabetes or heart disease. The impact of these behaviors or risk factors can accumulate over time and, without proper intervention, will “travel” with the individual throughout the life span, which can lead to disease (Layne et al., 2014). As such, it is important for health care providers to be aware of the relationship between these risk factors and IPV, given that many women at risk for IPV and those who smoke are often younger; therefore, addressing these behaviors early on can play an important role in disease prevention.
Limitations
Despite the large sample size, this study has several limitations. The data are cross-sectional; therefore, causal relationships cannot be examined. It is unknown whether the negative health conditions and health behaviors preceded the IPV experiences or vice versa. Nonetheless, even if the health conditions or health behaviors preceded the IPV, these conditions may increase women’s vulnerability for staying with their abuser longer for various reasons such as economic dependence to receive medical care (e.g., health insurance), which may lead them to continue to engage in negative health behaviors to deal with the chronic stress of being in a violent relationship. Dealing with the chronic stress of IPV may contribute to even poorer mental health such as feelings of depression or anxiety (Dillon et al., 2013). These negative health behaviors and poor mental health may then lead to further health deterioration.
Another limitation of the study was that there were small sample sizes in some of the categories of interest, such as interactions between IPV and mental health and binge drinking. This yielded wide 95% confidence intervals (CIs), indicating that the point estimates were less precise. This, in turn, weakens any related conclusions. Thus, future studies may seek to examine these relationships with larger sample sizes (e.g., combining multiple BRFSS data sets across a number of years).
The BRFSS IPV questions did not gather information about severity, frequency, or duration of the IPV or the length of the relationship. These factors may influence health outcomes and behaviors. Also, the questions only captured physical and sexual violence and did not assess psychological violence. Psychological or emotional violence includes using threats or coercive tactics, controlling the victim’s activities, finances, or access to resources and isolating the victim from friends and family (Saltzman, Fanslow, McMahon, & Shelley, 2002). Psychological violence is also associated with negative health outcomes (Coker et al., 2002), and was found in one study to be a stronger predictor of depression and anxiety symptoms than physical IPV alone (Pico-Alfonso et al., 2006). Victimization in childhood was also not assessed, and women with a history of adverse childhood experiences are also at increased risk for IPV (Whitfield, Anda, Dube, & Felitti, 2003). There have also been significant associations between child physical and sexual abuse, and adverse health outcomes (Felitti et al., 1998); therefore, the relationship between IPV and adverse health outcomes may have been underestimated given that childhood victimization as well as all aspects of IPV were not assessed.
Despite the strong relationship between IPV and mental health problems, the way in which mental health was assessed by BRFSS may overestimate the prevalence of mental health symptoms. Unlike other measures of mental health problems in other BRFSS data sets where specific symptoms of depression and anxiety are assessed, the question assessing mental health in this data set was broad, asking respondents to think about their levels of “stress” and “problems with emotions.” Although those factors can contribute to mental health problems such as depression and anxiety, it may also capture women who may not meet criteria for these conditions at a clinically significant level.
Another limitation was that only individuals with land phone lines were included in the 2005 BRFSS. Women with only cell phones were not represented in the sample. These women tend to be younger and therefore at greater risk for IPV (CDC, 2013a; U.S. Census Bureau, 2013). The prevalence of IPV may therefore be an underestimate given exclusion of these women from the sample. Finally, despite our sample being representative of the racial/ethnic makeup of Missouri, it was predominantly White women; therefore, our findings may not generalize to women of another race or ethnic background.
Conclusion
This study supports other findings that suggest women with a history of IPV are more likely to report poor mental health and engage in health risk behaviors that put them at increased risk for various negative health outcomes. Given the recent changes in the U.S. health care system, with more emphasis on preventive care and inclusion of IPV screening as preventive services (Patient Protection and Affordable Care Act, 2010), assessment of health-compromising behaviors should be integrated with routine IPV screenings to underscore the health-related impact of IPV exposure and enhance relevance for discussion within a health care setting. These findings underscore the importance that clinics, community, or other health care settings have in identifying women who are victims of, or have a history of, IPV and providing them with appropriate resources (e.g., directing them to mental health clinics specializing in trauma-focused work) as well as targeted interventions (e.g., taking into account trauma history when working on smoking cessation) to reduce morbidity in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.