
Abstract
Studies of the effects of intimate partner violence (IPV) on parenting have usually not examined the role of the maternal perceptions, either its stress or maternal satisfaction, on the mothers’ and children’s mental health functioning. The present study aimed to assess whether maternal satisfaction, parenting stress, and social support are significantly associated with women’s psychological functioning. The study also assessed whether maternal perceptions of the role of parenting were significantly associated with children’s emotional well-being and social behavior. The sample included 160 mothers, 79 (49.4%) who were living with the aggressors and 81 (50.6%) in shelters, and their children (n = 61). The findings suggested that high levels of maternal satisfaction and perception of social support were significantly negatively associated with women’s posttraumatic stress disorder (PTSD) symptoms and psychological distress, whereas parenting stress was significantly positively associated with these outcomes. Maternal satisfaction was the only parenting variable that predicted both maternal mental health and children’s emotional and behavioral problems, suggesting that it is a protective factor for both mothers and children. This study suggests that increasing maternal satisfaction with parenting and reducing parenting stress might promote better adjustment for both women and children victims of IPV.
The mental health effects of intimate partner violence (IPV) on women have been conceptualized within a traumatic response framework (Campbell & Lewandowski, 1997; van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005), thus extending beyond posttraumatic stress disorder (PTSD) to include other mental health concerns, such as depressive, anxious, and somatic symptoms and interpersonal problems (Herman, 1992; van der Kolk et al., 2005). Within this traumatic framework, the broad nature of the symptoms and the severity of the mental health conditions are explained by the chronic and severe nature of the trauma exposure (Astin, Lawrence, & Foy, 1993; Basile, Arias, Desai, & Thompson, 2004; Bonomi et al., 2006; Dutton, Kaltman, Goodman, Weinfurt, & Vankos, 2005; Herman, 1992; Pico-Alfonso, 2005; van der Kolk et al., 2005). In addition, contextual risk factors, such as poverty, young age, low socioeconomic status, and low education level, may increase the effects of the trauma exposure on women’s mental health symptoms (Capaldi, Knoble, Shortt, & Kim, 2012; L. A. Goodman, Smyth, Borges, & Singer, 2009). In addition to the impact on women, IPV can have a negative impact on children’s functioning, including internalizing and externalizing behaviors, and trauma symptoms (Bogat, DeJonghe, Levendosky, Davidson, & von Eye, 2006; Evans, Davies, & DiLillo, 2008; Levendosky, Lannert, & Yalch, 2012; Martinez-Torteya, Bogat, Von Eye, & Levendosky, 2009).
In contrast to contextual risk factors, women’s perception of social support has been established as a key factor in protecting women from the negative effects of IPV (e.g., Beeble, Bybee, Sullivan, & Adams, 2009; Coker et al., 2002; Coker, Watkins, Smith, & Brandt, 2003; Herman, 1992; Kamimura, Parekh, & Olson, 2013; Mburia-Mwalili, Clements-Nolle, Lee, Shadley, & Yang, 2010). This may be because women with supportive relationships perceive the stressful situation with their partners as less threatening (Cutrona & Russell, 1987; Liang, Goodman, Tummala-Narra, & Weintraub, 2005), improving ability to seek help from formal sources and subsequent capacity to stay safe (Liang et al., 2005). With regard to children, the healthy mother–child relationship has been identified as one of the most important protective factor to mitigate the negative impact of the IPV context (Graham-Bermann, Gruber, Howell, & Girz, 2009; Holt, Buckley, & Whelan, 2008; Letourneau, Fedick, & Willms, 2007; Levendosky & Graham-Bermann, 2001).
Although good maternal parenting can mitigate the effects of IPV on children’s functioning, few studies have found that women exposed to IPV generally parent well (Casanueva, Martin, Runyan, Barth, & Bradley, 2008; Kelly, 2009; Levendosky, Huth-Bocks, Shapiro, & Semel, 2003; Peled & Gil, 2011). In fact, mothers who experience IPV are likely to exhibit mental health problems (e.g., Gustafsson & Cox, 2012; Holmes, 2013; Miranda, de la Osa, Granero, & Ezpeleta, 2013), and maternal parenting stress (Huth-Bocks & Hughes, 2008; Taylor, Guterman, Lee, & Rathouz, 2009), which in turn negatively affects children’s adjustment (e.g., Holt et al., 2008; Huth-Bocks & Hughes, 2008; Levendosky, Leahy, Bogat, Davidson, & von Eye, 2006; Owen, Thompson, & Kaslow, 2006; Taylor et al., 2009). One theoretical explanation for these findings is the spillover hypothesis, which suggests that interparental hostility and conflict has negative effects on parent–child relationships (Erel & Burman, 1995). This is supported by several studies that find that mothers exposed to IPV are less available to their children, with lower warmth and maternal sensitivity, and higher levels of parenting stress, as well as harsh and punitive discipline (Bradford, Vaughn, & Barber, 2008; Krishnakumar & Buehler, 2000; Lannert, Levendosky, & Bogat, 2013; Lannert et al., 2014; Levendosky & Graham-Bermann, 2000; Levendosky et al., 2006; Sturge-Apple, Davies, Cicchetti, & Fittoria, 2014; Theran, Levendosky, Bogat, & Huth-Bocks, 2005).
However, given that most children exposed to IPV do not have either internalizing or externalizing behavior problems (Grych, Jouriles, Swank, McDonald, & Norwood, 2000; Martinez-Torteya et al., 2009), it may be that in many families exposed to IPV, the spillover hypothesis does not explain the functioning. Instead, the compartmentalization hypothesis may be relevant for these families. The compartmentalization hypothesis suggests that parents who experience elevated levels of interpartner conflict are able to continue to provide effective and responsive caregiving to their children (Bradford et al., 2008; Krishnakumar & Buehler, 2000) because they separate their conflicted marriage and associated negative feelings from their role as parents, establishing effective boundaries between these family systems (Krishnakumar & Buehler, 2000). Some mothers of children exposed to IPV may be warm toward their child as a compensation for exposure to violence in their parenting interactions (Letourneau et al., 2007), creating a buffer by preventing the abuse from affecting their functioning as mothers, and protecting their children from violence (Peled & Gil, 2011).
However, no studies have explored how parenting stress or satisfaction will differentially affect women’s mental health, and in turn, affect children’s adjustment. According to the compartmentalization hypothesis, it is possible that some mothers are satisfied with the maternal role, but it is unknown about how maternal satisfaction is associated to their own psychological functioning, and how it affects the children’s functioning. The present study aimed to assess whether maternal satisfaction, parenting stress, and social support are significantly associated with women’s psychological functioning, after adjusting for the type and severity of the IPV and socioeconomic variables. In addition, we intended to assess whether maternal satisfaction, parenting stress, and social support are significantly associated with children’s emotional well-being and social behavior, after adjusting for PTSD symptoms and psychological distress from mothers. Within a traumatic response framework, we chose to assess women’s psychological distress as well as their PTSD symptoms. We expected that women with high levels of maternal satisfaction and high levels of perception of social support would have less psychological distress and PTSD symptoms. In addition, we expected that high levels of maternal satisfaction and high levels of social support would be significantly associated with fewer emotional and behavioral problems in children. We expected high levels of parenting stress would be related to more psychological distress and PTSD symptoms and more emotional and behavioral problems in children.
Method
Participants
The present study is part of a larger research project funded by Fundação para a Ciência e Tecnologia (Foundation for Science and Technology—Portuguese and European funding) on the impact of IPV on women and children’s health carried out in Portugal. The study was approved by the National Commission for Data Protection (NCDP; authorization nº 7005/2016) and the ethics committees of both the University of Porto and the University of Lusófona of Porto.
To recruit the sample, 260 institutions that provide anonymous assistance to women victims of partner violence, including shelter residences, were contacted. One hundred seventeen agreed to collaborate in the study. Professionals of these institutions made the first contact with the participants, a general explanation of the study was provided to them, and then they were asked if they agreed to participate in the study. In total, 352 women were contacted and 160 women, including their children, obtained from 35 institutions, agreed to participate. The present study only included the children from whom researchers collected data from teachers. A questionnaire was sent by e-mail to the teacher of each child who participated (N = 160) and 61 (38.13%) were returned. The final sample included 79 (49.4%) mothers who were living with the aggressors and 81 (50.6%) in shelters. Of the 61 children included, 45 (73.8%) were living in home with mothers’ abusive intimate partner and 16 (26.2%) were living in shelters.
The inclusion criteria to participate in the study included women 18 years or older, and being mother of a child between 4 and 10 years old. The child had to be living with the mother, either at home with the abusive partner, or in the IPV shelter. When the mother had more than one child between 4 and 10 years, the older child was chosen for participation due to having spent more time in the context of violence. Finally, in order to be included in the study, the IPV had to have been reported to authorities, either the police department or an institution for victim support or be living in a domestic violence shelter. Exclusion criteria were receiving psychotherapy; having apparent psychosis, intoxication, and pregnancy; or having mental retardation, to ensure that informed consent could be given. In addition, children with any pervasive developmental disorder or severe medical condition were excluded.
The mothers’ ages ranged from 21 to 54 years (M = 36.39, SD = 7.64). In terms of marital status, 32 (20%) women were single, 57 (35.6%) married, 38 (23.8%) civil union, 32 (20%) divorced or separated, and one (0.6%) widowed. In terms of education, 22 (13.8%) participants had only 4 years, 63 (39.4%%) had completed 6 years, 58 (36.3%) had completed 9 years, 13 (8.1%) participants had completed the full compulsory education of 12 years, and 4 (2.5%) participants had obtained university degrees. The majority of women were unemployed (n = 116, 72.5%), 39 (24.4%) were employed, and five (3.1%) never worked. The children’s age on average was 7.08 years (SD = 2.07), ranged from 4 to 10, and 33 (54.1%) were females and 28 (45.9%) males.
Measures
Sociodemographic questionnaire
A sociodemographic questionnaire was used to collect information about age, gender, marital status, occupation, education, number of family members, living situation (i.e., either living in the shelter or with the aggressor), and length of time living in the shelter.
Revised Conflict Tactics Scales (CTS2)
The CTS2 (Straus, Hamby, Boney-McCoy, & Sugarman, 1996; Portuguese version by Paiva & Figueiredo, 2006) was used to measure psychological aggression, physical assault, and sexual coercion within couples whether they were dating, cohabiting, or in a marital relationship. Respondents reported on the frequency of abusive behaviors perpetrated by their current or most recent abusive partner within the previous 12 months on an 8-point scale (0 = this has never happened to 7 = more than 20 times in the past year). For the purposes of the current study, we used the chronicity score (continuous variable) that was calculated by determining the midpoint of the items as follows: this has never happened = 0, once in the past year = 1, twice in the past year = 2, 3 to 5 times in the past year = 4, 6 to 10 times in the past year = 8, 11 to 20 times in the past year = 15, and more than 20 times in the past year = 25. These midpoints of each item were then summed to obtain Psychological Aggression (eight items), Physical Assault (12 items), and Sexual Coercion (seven items) subscales (Straus, 2001). Psychological Aggression ranged from 0 to 220, Physical Assault ranged from 0 to 300, and Sexual Coercion from 0 to 175. Higher scores reflect higher frequency of the acts in each subscale. In addition, to describe how many women were victim of at least one act of each type of violence during the past year, we used the prevalence score, which indicates whether the respondent experienced one or more acts in each subscale (Straus, 2001). This measure is computed as a dichotomous variable (0 if there were no violent acts in the past year; 1 indicates one or more acts of violence in the past year). In the present study, the subscales presented good reliability: Sexual Coercion (α = .71), Psychological Aggression (α = .78), and Physical Assault (α = .89).
Brief Symptom Inventory (BSI)
The BSI (Derogatis, 1993; Portuguese version of Canavarro, 1999) is a well-established self-report instrument to assess psychological distress. The BSI comprises 53 items on a 5-point rating scale that ranges from 0 (not at all) to 4 (extremely). The inventory includes nine symptom dimensions: somatization, obsessive compulsivity, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. Mothers’ psychological distress was obtained by global severity index (GSI) that provides a global measure of current symptomatic state, combining information on the numbers of symptoms and the intensity of perceived distress. Higher GSI scores reflect higher global psychological distress. The GSI is computed by calculating the mean of all items. We also calculated the positive symptoms distress index (PSDI), which is the sum of all item values divided by the number of items endorsed with a positive response, to compute the cutoff score for clinical cases, which in the Portuguese version is ≥1.7 (Canavarro, 1999). The internal consistency for the present sample was .96.
PTSD Checklist–Civilian Version (PCL-C)
The PCL-C (Weathers, Litz, Herman, Huska, & Keane, 1994; Portuguese version of Marcelino & Gonçalves, 2012) is a checklist that includes 17 self-report items of symptoms of PTSD based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) B, C, and D criteria. It requires participants to rate the severity of each symptom during the previous 30 days on a Likert-type scale ranging from 1 (not at all) to 5 (extremely). The DSM-IV criteria for PTSD were met when a participant reported a moderate or higher level of at least one intrusion symptom, three avoidance symptoms, and two hyperarousal symptoms. In this study, participants were instructed to respond while thinking about the exposure to actual or threatened death or serious injury to meet DSM-IV A1 criteria. We also assessed DSM-IV A2 criteria by asking to participants if they recalled feeling terrified or helpless at the time of exposure. We also used a total PTSD score based on the sum of all symptoms, ranging from 0 to 85. Higher scores reflect higher levels of PTSD symptoms. The internal consistency for the present sample was .89.
Social Provisions Scale
Social Provisions Scale (Cutrona & Russell, 1987; Portuguese version of Moreira & Canaipa, 2007) is a scale that includes 24 self-report items to assess the degree to which a respondent’s social relationships provide various dimensions of social support. The respondent indicates on a 4-point scale the extent to which each statement describes her current social network. Responses range from 1 (strongly disagree) to 4 (strongly agree). The instrument contains six subscales as following: Attachment, Social Integration, Reassurance of Worth, Reliable Alliance, Guidance, and Opportunity for Nurturance. After reversal of negatively worded items, a total score may be computed by summing all items, ranging from 0 to 96. A high score indicates a greater degree of social support. The internal consistency for the overall items in the present sample was .95.
Parenting stress Index (PSI)
PSI (Abidin, 1990; Portuguese version of Santos, 1997) is a questionnaire that assesses stress in the parent–child system. Items are endorsed in a 6-point Likert-type scale ranging from (0) strongly agree to (5) strongly disagree. The measure yields subscale scores of two domains, as child domain (stress reflecting child characteristics that make it difficult to fulfill the parenting role) and parent domain (stress as a consequence of parental functioning). For the present study, maternal parenting stress was calculated from scores on the two subscales: Role Restriction of the parent domain and Demandingness of the child domain (e.g., Essex, Klein, Cho, & Kalin, 2002), and ranged from 0 to 75. Higher scores reflect higher levels of parenting stress. The Role Restriction means that mother expresses concerns regarding the loss of her personal identity, which sees herself as being controlled and dominated by her child’s needs and demands. Demandingness includes mother reports that child presents a number of demands for the parent’s attention, including crying, whining, and/or misbehaving. Adequate psychometric properties have been reported (e.g., Abidin, 1990; Solis & Abidin, 1991). In the current study, the internal consistency for the total score of both subscales was .74.
The Parenting Sense of Competence Scale
The Parenting Sense of Competence Scale (Johnston & Mash, 1989; Portuguese version of Ferreira, Veríssimo, Santos, Fernandes, & Cardoso, 2011) is a self-reported scale that measures maternal satisfaction and efficacy. In the present study, we used only the Maternal Satisfaction subscale that includes mothers’ anxiety, motivation, and frustration, which also includes nine items (e.g., “Being a parent makes me tense and anxious”) organized in a 6-point Likert-type scale ranging from 1 (strongly agree) to 6 (strongly disagree). For the present study, a total score was computed by summing the scores of the items, ranging from 0 to 54. Higher scores reflect higher levels of Maternal Satisfaction. Adequate psychometric properties have been reported (e.g., Johnston & Mash, 1989). The internal consistency of Maternal Satisfaction in the present study was .74.
Strengths and Difficulties Questionnaire–Teacher Version (SDQ)
SDQ (R. Goodman, 1997; Portuguese version of Fleitlich, Loureiro, Fonseca, & Gaspar, 2005; Marzocchi et al., 2004) was used to assess teachers’ perspective of children’s behaviors. The SDQ is a 25-item behavioral screening questionnaire for 4- to 16-year-olds that assesses children’s mental health problems, including emotional symptoms, conduct problems, hyperactivity/inattention, as well as peer relationship problems and prosocial behaviors. Each subscale is comprised of five items with a 3-point response scale (from not true to certainly true). For the present study, a total score was computed by summing the scores on the Emotional Symptoms, Conduct Problems, Hyperactivity-Inattention, and Peer Problems subscales (range = 0-40). We used the cutoff points published in the literature (R. Goodman, 1997), which are the same for the Portuguese version, to define “normal,” “borderline,” and “abnormal” punctuations. Previous studies have supported the psychometric properties of the instrument (e.g., R. Goodman, 2001). In the current study, the internal consistency was .70.
Procedure
Prior written informed consent was obtained from all participants. All mothers agreed to their children being assessed by researchers, including for the children’s teachers to be contacted to participate in the study. The mothers received vouchers from a local department store as a courtesy for participating in the study. Recruitments of women took place in the Portuguese Association for Victim Support (APAV), Child Protective Services, Domestic Violence Organizations and Shelter Residences from north to south of Portugal. The initial contact with the institutions was made by e-mail and then followed by telephone, where a face-to-face meeting was scheduled to present the study. The first contact with the participants was made by the professionals of the institutions and a general explanation of the purposes of the study, methods, and procedures was provided to them. After the participants agreed to participate, the researchers scheduled the interviews, in which more detailed information about the study and the informed consent was given. The questionnaires were administered by trained female psychologists either in the institutions’ facilities or in the shelters in a calm and private room. To evaluate the children’s emotional and behavioral problems, all children’s teachers were contacted by telephone and invited to participate in the study, and a questionnaire was emailed to them.
Data Analysis
Data analyses were carried out using the SPSS version 20 for Windows (New York, IBM Corporation). We calculated the effect sizes by using the post hoc power analyses of GPower 3.1 (Faul, Erdfelder, Buchner, & Lang, 2009). Descriptive statistics were calculated to characterize the study variables. Two hierarchical multiple regression analyses assessed the independent contributions of the perceived social support, perceived parental stress, and maternal satisfaction, to provide an estimate of incremental variance accounting for psychological distress and total score of PTSD symptoms, after adjusted for potential confounding variables, such as age, education, living with aggressor versus in shelter, chronicity, and type of IPV, as physical assault, sexual coercion, and psychological aggression. In addition, one hierarchical multiple regression analysis assessed the independent contributions of mother’s psychological distress and PTSD symptoms, maternal satisfaction, parenting stress, and social support, to provide an estimate of incremental variance accounting for children’s emotional and behavioral problems as outcome variable. Missing data occurred on the variable total score of psychological distress for 0.6% (n = 1), and PTSD symptoms as a continuous variable for 1.3% (n = 2) of the cases. Considering the low incidence of missing values, no correction was made for missing values in the reported analyses.
Results
Descriptive Information on IPV and Other Study Measures
Descriptive statistics of key measures are presented in Table 1. The results revealed that 152 (94.4%) women meet criteria for clinical values of psychological distress (PSDI ≥ 1.7), and 118 (72.8%) women meet criteria for probable PTSD. Considering the prevalence of each type of violence during the last year, 157 (96.9%) women experienced at least one act of physical assault, 161 (99.4%) women experienced at least one act of psychological aggression, and all the women (162) reported at least one act of sexual coercion. Regarding the children’s mental health problems, considering the normal, borderline, and abnormal ranges of the SDQ, 15 (24.2%) children scored in the normal range, three (4.8%) scored in the borderline range, and 44 (71%) scored in the abnormal range.
Means and Standard Deviations of Key Measures (n = 158-160).
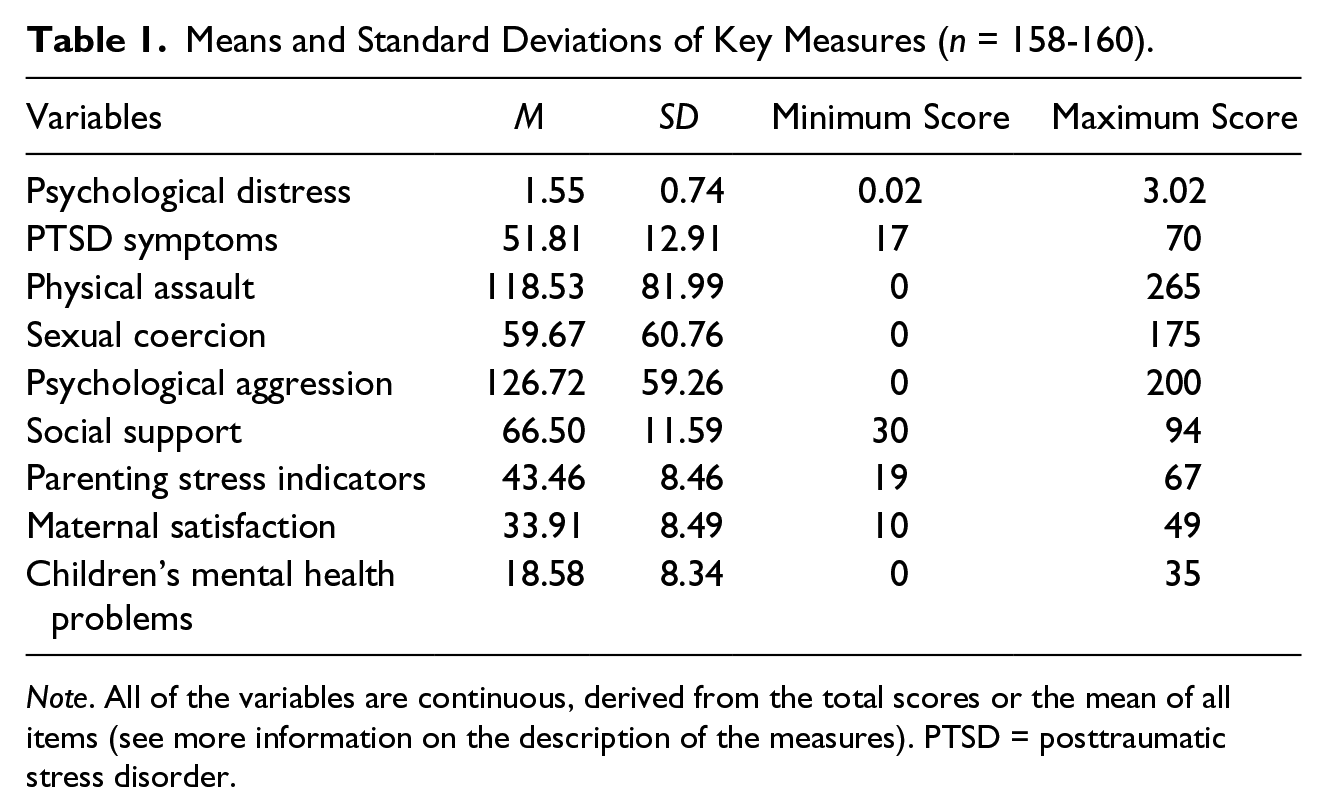
Note. All of the variables are continuous, derived from the total scores or the mean of all items (see more information on the description of the measures). PTSD = posttraumatic stress disorder.
Mother’s Outcomes
The results of hierarchical multiple regression analysis with psychological distress as outcome variable are shown in Table 2. The first block, including age, education, and location, did not significantly contribute to the regression model, F(3, 150) = 1.53, p = .21. Adding the physical assault, sexual coercion, and psychological aggression in the second block, the model became statistically significant, F(6, 147) = 6.12, p < .001, Cohen’s f2 = 0.21, contributing an additional 17% to the explained variance. Only physical assault was significantly correlated. Perceived parental stress was entered in the third step, and the model remained significant, F(7, 146) = 11.81, p < .001, Cohen’s f2 = 0.25, contributing an additional 16% to the explained variance. The perceived social support and maternal satisfaction were added in the final step, and the model remained significant, F(10, 143) = 12.41, p < .001, Cohen’s f2 = 0.19, contributing an additional 11% to the explained variance. The final model explained 47% of the variance, Cohen’s f2 = 0.89. Here, physical assault and parenting stress were positively associated with psychological distress; perceived social support and maternal satisfaction were negatively associated with psychological distress.
Hierarchical Regression With Psychological Distress as Outcome Variable (n = 154).
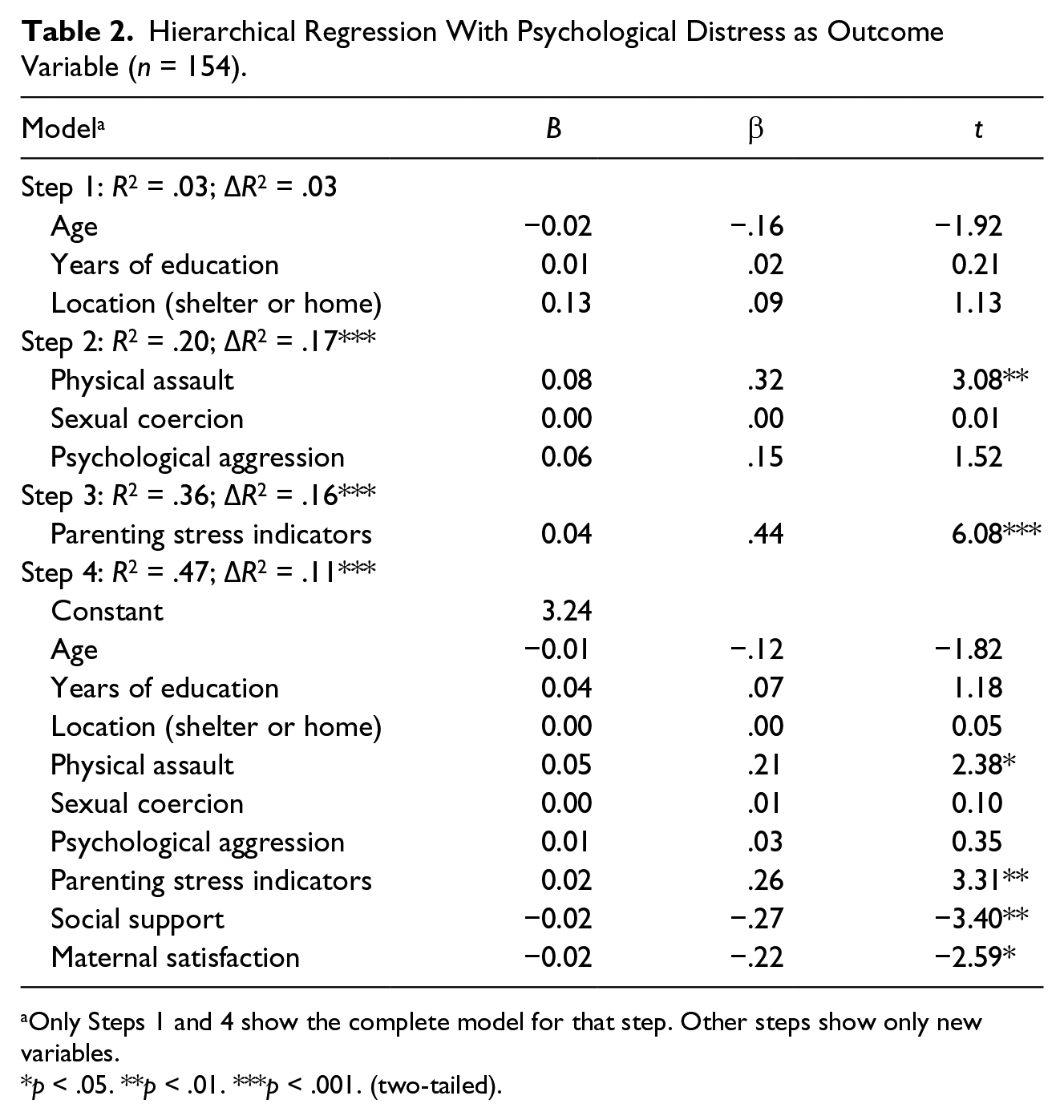
Only Steps 1 and 4 show the complete model for that step. Other steps show only new variables.
p < .05. **p < .01. ***p < .001. (two-tailed).
The results of hierarchical multiple regression analysis with total score of PTSD symptoms as outcome variable are shown in Table 3. The first block, including age, education, and location, did not significantly contribute to the regression model, F(3, 150) = 0.58, p = .63. Adding the physical assault, sexual coercion, and psychological aggression in the second block, the model became statistically significant, F(6, 147) = 9.01, p < .001, Cohen’s f2 = 0.36, contributing an additional 26% to the explained variance. Only physical assault was significantly correlated. Perceived parental stress was entered in the third step, and the model remained significant, F(7, 146) = 13.24, p < .001, Cohen’s f2 = 0.20, contributing an additional 12% to the explained variance. The perceived social support and maternal satisfaction were added in the final step, and the model remained significant, F(10, 143) = 12.55, p < .001, Cohen’s f2 = 0.15, contributing an additional 8% to the explained variance. The final model explained 47% of the variance, Cohen’s f2 = 0.89. Here, physical assault and parenting stress were positively associated with the PTSD symptoms; perceived social support and parental satisfaction were negatively associated with the PTSD symptoms.
Hierarchical Regression With PTSD Symptoms as Outcome Variable (n = 154).
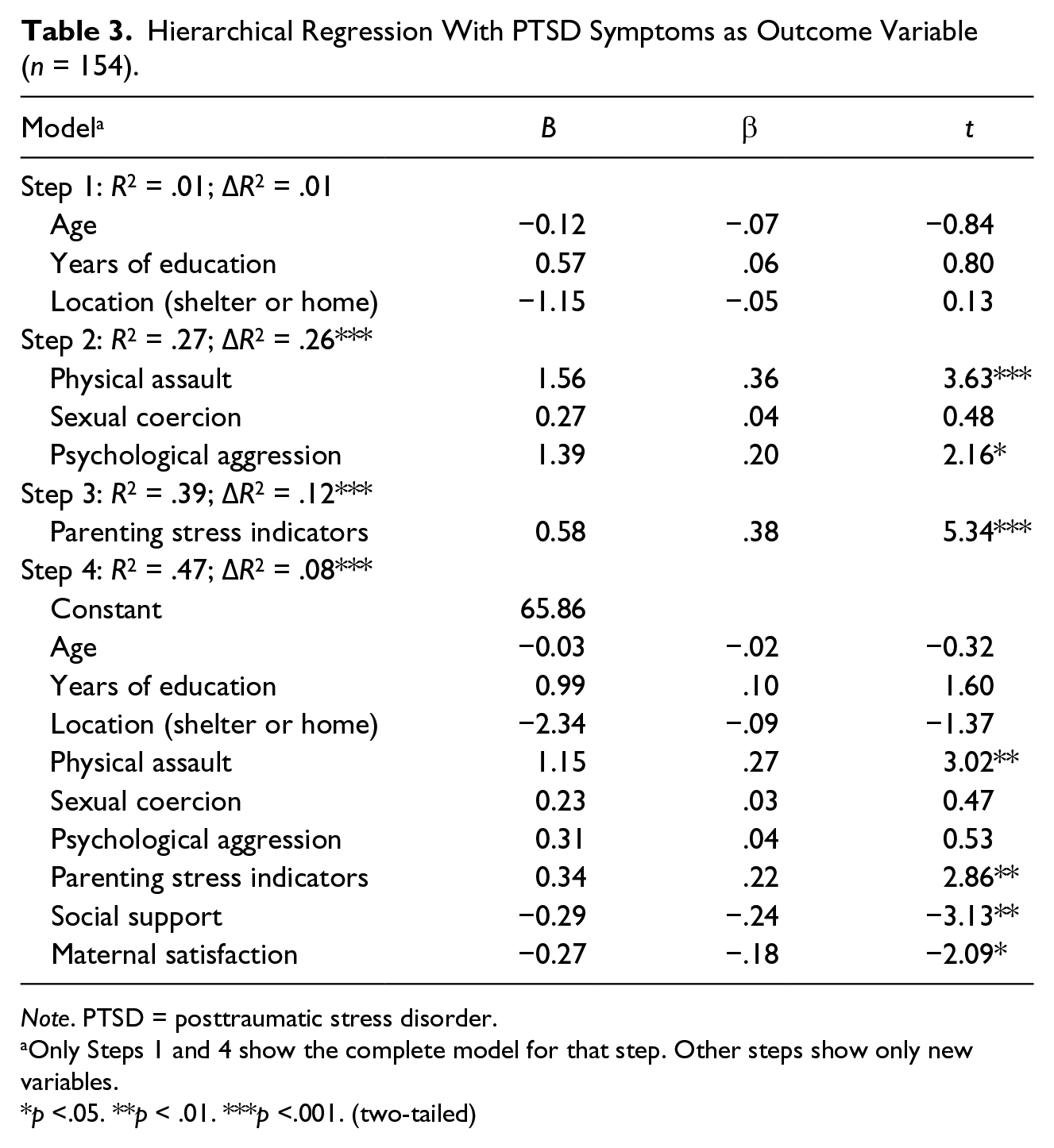
Note. PTSD = posttraumatic stress disorder.
Only Steps 1 and 4 show the complete model for that step. Other steps show only new variables.
p <.05. **p < .01. ***p <.001. (two-tailed)
Children’s Outcomes
The results of hierarchical multiple regression analysis with total score of children’s emotional and behavioral problems as outcome variable are shown in Table 4. The first block included mother’s psychological distress and PTSD symptoms and significantly contributed to the regression model, F(2, 57) = 8.46, p = .001, Cohen’s f2 = 0.30, explaining 23% of variance. Adding the maternal satisfaction, parenting stress, and mother’s social support in the second block, the model remained statistically significant, F(5, 54) = 5.45, p < .001, Cohen’s f2 = 0.17, contributing an additional 11% to the explained variance. Only PTSD symptoms and maternal satisfaction were significant correlates. The final model explained 34% of the variance, Cohen’s f2 = 0.52.
Hierarchical Regression With Total Score of SDQ Completed by Teachers as Outcome Variable (n = 60).
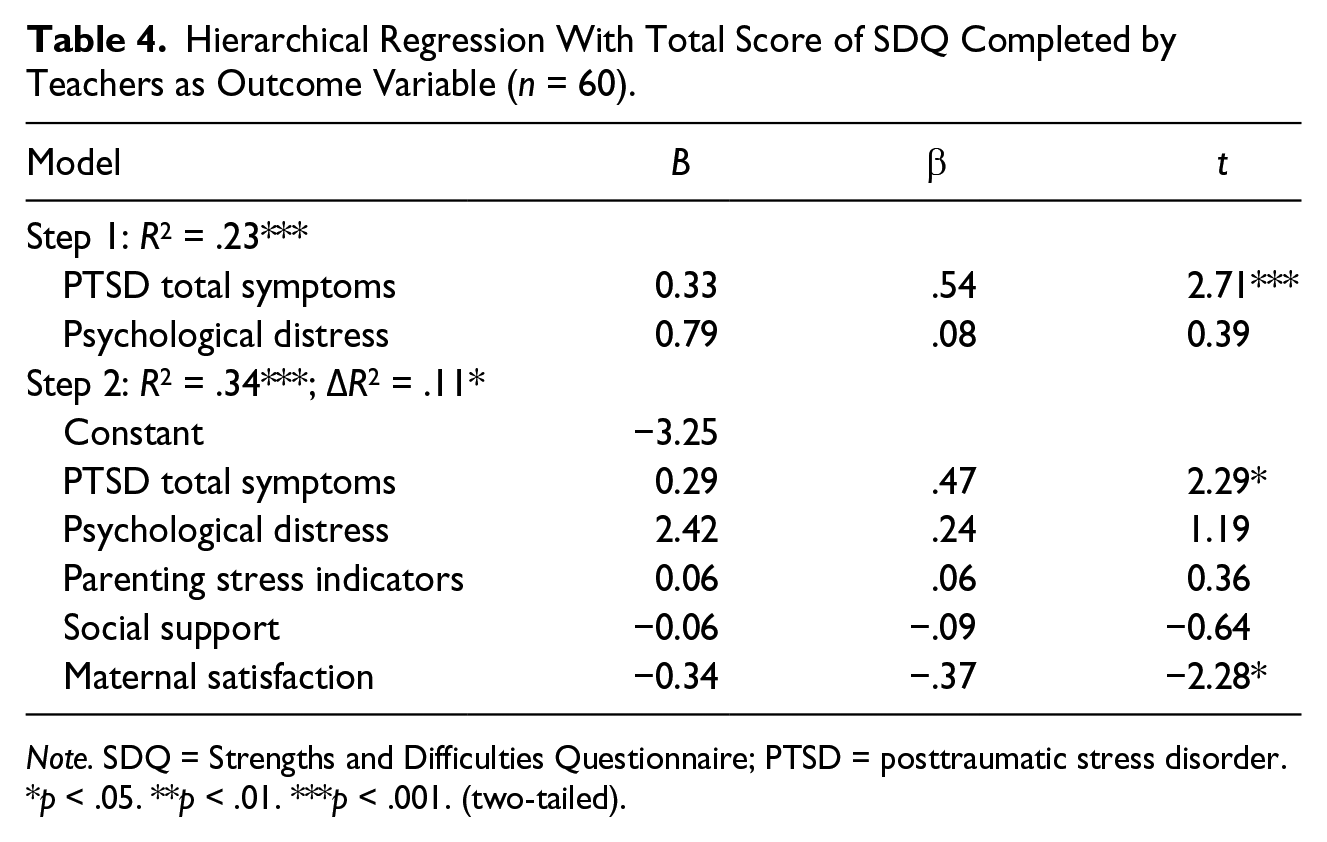
Note. SDQ = Strengths and Difficulties Questionnaire; PTSD = posttraumatic stress disorder.
p < .05. **p < .01. ***p < .001 (two-tailed).
Discussion
The present study aimed to examine the contribution of parenting stress, maternal satisfaction, and maternal social support to explain PTSD symptoms and psychological distress. In particular, we sought to test the independent contribution of these variables, after adjusting for characteristics of the IPV and socioeconomic variables. In addition, we examined how mother’s maternal satisfaction, parenting stress, and social support contributed to children’s emotional and behavioral problems.
As expected, because our sample only included women who had reported IPV to authorities, mothers reported experiencing high levels of physical assault, sexual coercion, and psychological aggression. In addition, they reported high levels of psychological distress and PTSD symptoms. In addition, teachers reported that more than two thirds of the children had abnormal levels of emotional and behavioral problems. This finding is consistent with the conceptual grounding of trauma and empirical evidence found in literature (e.g., Bogat et al., 2006; Levendosky & Graham-Bermann, 2001; van der Kolk et al., 2005).
As hypothesized, high levels of maternal satisfaction and perception of high levels of social support were significantly and negatively associated to the outcome variables for both models, and high levels of parental stress were significantly associated to high levels of PTSD symptoms and psychological distress. These significant associations were obtained after adjusting for other risk factors that increase the likelihood of women exposed to IPV will develop negative health outcomes, including the type and chronicity of the abuse (e.g., Basile et al., 2004; Bogat, Levendosky, Theran, Von Eye, & Davidson, 2003; Bonomi et al., 2006) as well as demographic risks, such as age and education level (Capaldi et al., 2012; L. A. Goodman et al., 2009). These findings are generally consistent with the traumatic framework (Herman, 1992; van der Kolk et al., 2005).
The finding that social support is related to lower levels of maternal distress is consistent with the literature that generally finds positive effects of social support among women exposed to IPV (Beeble et al., 2009; Coker et al., 2002; Coker et al., 2003; Herman, 1992; Kamimura et al., 2013; Mburia-Mwalili et al., 2010). For example, Levendosky et al. (2004) found that social support during pregnancy was related to higher self-esteem and less anxiety among mothers exposed to IPV. Similar findings were found later, where social support was directly and positively related to better maternal mental health, and an indirect effect on child externalizing behavior (Levendosky et al., 2006). Women with more social support may perceive the IPV as less threatening (Cutrona & Russell, 1987; Liang et al., 2005), increasing the ability to seek help from formal sources (Levendosky & Graham-Bermann, 2001; Liang et al., 2005). Social support helps mothers to accomplish the goals of motherhood (Belsky, 1984), but the IPV usually reduces the woman’s social relationships and reduces the sense of worth, value, or self-esteem, both of which are mutually reinforcing (Coker et al., 2002). Increasing social support may counter both of these characteristics in ways that increase coping skills to deal with violence as well as the creation of alternatives to the current abusive relationship (Coker et al., 2002; Levendosky & Graham-Bermann, 2001; Liang et al., 2005).
In the case of parenting stress, it was significantly associated to high levels of PTSD symptoms and psychological distress, even after adjusting for demographic and IPV variables. Maybe this finding is explained by the numerous internal and external demands associated with mothers exposed to IPV that go beyond the multiple roles that many women have between employment and family responsibilities, as worries about raising a child in a context of violence, and fears and anxiety about their own life and children’s life. The perception that the situation exceeds the person’s resources, and cannot accomplish the goals of motherhood, possibly increases the likelihood of experiencing psychological distress and PTSD. Contrary to a substantial amount of research associating parenting stress with increased internalizing symptoms and behavior problems (e.g., Huth-Bocks & Hughes, 2008; Levendosky & Graham-Bermann, 1998; Owen et al., 2006; Renner & Boel-Studt, 2013; Wolfe, Jaffe, Wilson, & Zak, 1985), we found that parenitng stress was not associated with child functioning. Maybe this finding is explained by the inclusion of both PTSD symptoms and parenting stress in the same model, which was not done in previous studies.
Maternal satisfaction was the only variable that resulted in reduced maternal psychological distress and PTSD symptoms as well as child emotional and behavioral problems, suggesting that it is a protective factor for both mothers and children. This is consistent with the compartmentalization hypotheses that support that it is possible to be satisfied with motherhood, despite the severe exposure to IPV, suggesting that some mothers are able to continue to provide effective and responsive caregiving to their children (Bradford et al., 2008; Krishnakumar & Buehler, 2000) and separate the violence victimization and associated negative feelings from their role as mothers (Krishnakumar & Buehler, 2000). The mothers who perceive the maternal parenting as more positive also have less psychological distress and PTSD symptoms. It is possible that parenting gives mothers a purpose and meaning in life, and satisfaction with this role, providing them with psychological resources to deal with the violence, as well as increasing their ability to attend to the children’s emotional and social needs. Parenting, for most individuals, is salient as a role in life that provides purpose and meaning. Purpose is a cognitive process that defines life goals and provides personal meaning (McKnight & Kashdan, 2009). Empirically, this sense of purpose is considered a powerful predictor of general life adjustment (Reker, Peacock, & Wong, 1987; Thompson, Coker, Krause, & Henry, 2003).
A few limitations must be considered when interpreting our results. This is a cross-sectional study, thus preventing determination of causality between variables. In addition, the scales for PTSD and psychological distress are symptom checklists, rather than diagnostic measures. Therefore, conclusions about diagnoses of mental disorders and comorbidity cannot be drawn. We had far fewer teachers’ reports of the children’s behaviors, thereby reducing the power to obtain statistically significant findings. Finally, another concern about the study was the high rejection rate of women and children. This rejection of the women to participate in the study may be because of embarrassment or fear of being identified. These feelings of embarrassment or fear were constant among all women contacted, whether they had participated or not in the study, considering that their partners often threatened many of them of death. With regard to the teachers, for some, the informed consent provided from the mother was enough to participate in the study and provide information about the child. However, for other teachers, they needed both informed consent from the mother and formal authorization of the school, and many of the schools did not provide the authorization at the time of data collection.
The sample for this study is more generalizable to the broader population of battered women than the usual samples studied in IPV research because it included both women and children in IPV shelters and those living with the abusive partner. Women’s mental health assessment was not limited to PTSD symptoms, consistent with a traumatic response framework, which considers other posttraumatic mental health symptoms, such as depression, anxiety, and somatization.
Future research should also address the possible contribution of the efficacy dimension of parental competence (parents’ competence, capability levels, and problem-solving abilities in their parental role) on both mothers’ victims of IPV and their children. In terms of clinical implications, our study suggests that increasing maternal satisfaction with parenting and reducing parenting stress, for example, through providing practical parenting support, might promote the resilience of both mothers and their children exposed to IPV.
Footnotes
Acknowledgements
The authors express appreciation to the Portuguese Association for Victim Support (APAV), Child Protective Services (CPCJ), Domestic Violence Organizations, and Shelter Residences from Portugal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors express appreciation to the Fundação para a Ciência e Tecnologia (research grant, FCT—EXPL MHC PED 1977/2013, Portuguese and European funding) for financing this project.