
Abstract
South African adolescents are exposed to high levels of violence and trauma, including community violence, abuse, and neglect. Violence and trauma are associated with negative mental health outcomes, including posttraumatic stress disorder (PTSD) and depression. Demographic characteristics, additional exposure to trauma, community violence, and types of childhood abuse and neglect may place adolescents at greater risk of developing PTSD. This study aimed to first assess the weighted contribution of demographic factors, trauma load, community violence, and types of abuse and neglect in predicting PTSD symptom severity. Second, we aimed to determine group differences in demographic factors, trauma load, community violence, and types of abuse and neglect among participants with no disorder, PTSD only, PTSD and depression, and depression only. Participants were 215 adolescents identified with emotional and/or behavioral problems and referred to an adolescent trauma clinic from schools in the Western Cape region of South Africa. Clinical assessments were undertaken to assess community violence exposure; physical, sexual, and emotional abuse; physical and emotional neglect; and a clinical diagnosis of PTSD and comorbidity. Trauma-exposed adolescents with PTSD and depression reported significantly higher levels of emotional abuse and community violence exposure in comparison with trauma-exposed adolescents without a disorder. Emotional abuse, community violence exposure, and female gender were significant predictors of PTSD in regression analysis. These findings underscore the contribution of different types of trauma in the development of PTSD. Interventions focused on preventing trauma, PTSD, and depression should be multifaceted and be targeted at various levels, for example, individual/interpersonal level (reduce abuse in the household and immediate environment) and community/societal level (reduce crime rates in communities and strengthen conviction policies). Traumatized youth should routinely be screened for a history of abuse and particularly exposure to community violence, given their strong association with PTSD.
Introduction
Posttraumatic stress disorder (PTSD) is one of the most common disorders that develops in the aftermath of trauma exposure (Acierno, Resnick, Kilpatrick, Saunders, & Best, 1999; Kilpatrick et al., 2003; Seedat, Nyamai, Njenga, Vythilingum, & Stein, 2004). Trauma exposure is high among South African youth with rates ranging from 73.8% to 83% (Seedat et al., 2004; Seedat, van Nood, Vythilingum, Stein, & Kaminer, 2000; Ward, Flisher, Zissis, Muller, & Lombard, 2001). South African adolescents are at increased risk of trauma exposure, driven by the high rate of violent crimes that are reported daily (Department of Social Development [DSD], Department of Women, Children and People With Disabilities [DWCPD], & United Nations Children's Fund [UNICEF], 2012; Richter & Dawes, 2008). Reported rates of violent crime perpetrated against children and adolescents in South Africa in 2012 included 793 cases of murder, 758 cases of attempted murder, 25,862 cases of sexual offenses, 12,645 cases of assault, and 10,630 cases of assault with grievous bodily harm (DSD, DWCPD, & UNICEF, 2012). Generally, the majority of trauma cases related to criminal offences are underreported to authorities, possibly due to fears of the perpetrator/s, feelings of guilt and shame associated with abuse, and a lack of confidence in the legal system (i.e., a belief that perpetrators will not be convicted). The actual number of violent crimes against children is, therefore, not known (Everson et al., 2008; Fergusson, Boden, & Horwood, 2008; Herrenkohl & Herrenkohl, 2007; MacMillan et al., 2001). Witnessing violence is also considered a traumatic event, but the number of children and adolescents exposed to witnessing violence is difficult to determine in the greater population, owing to the indirect nature of these events (DSD, DWCPD, & UNICEF, 2012). Previous research found that 90% of South African youth reported being a witness of physical violence in their neighborhood and 48% reported seeing at least one murder in their lifetime (Shields, Nadasen, & Pierce, 2008; Ward et al., 2001). PTSD prevalence among South African adolescent samples ranges between 3.5% and 5.8% in general community samples, but prevalence rates are relatively unknown among clinic samples (Calitz, de Jongh, Horn, Nel, & Joubert, 2014; Ward et al., 2001).
Trauma exposure may also lead to the development of psychiatric disorders other than PTSD, most commonly depression (Kolko et al., 2010; Macdonald, Danielson, Resnick, Saunders, & Kilpatrick, 2010; Ying, Wu, & Lin, 2012). Adolescents who experience a greater number of traumatic events are more likely to meet criteria for PTSD and depression compared with PTSD only (Macdonald et al., 2010). In one study, adolescents in a trauma-exposed clinic sample were also more likely to manifest with greater PTSD symptom severity if they met criteria for both depression and PTSD (Kolko et al., 2010). Ying et al. (2012) found that pretrauma depression may increase the risk of PTSD. They found a comorbidity rate between 16.5% and 19% over 24 months (Ying et al., 2012). PTSD and depression were highly correlated in their sample of adolescents and they noted that depression and PTSD were distinct disorders and that comorbidity was likely due to personality characteristics underlying the risk for both disorders (Ying et al., 2012). The question of whether PTSD precedes depression (or vice versa) or whether common symptom patterns underlie both disorders is still unclear (Levitan, Rector, Sheldon, & Goering, 2003; MacMillan et al., 2001).
Trauma exposure is a prerequisite for a diagnosis of PTSD, yet several factors other than the index trauma have been identified as risk factors for PTSD symptom severity (American Psychiatric Association [APA], 2013; Breslau, Chase, & Anthony, 2002). Certain demographic factors have been found to increase PTSD risk. Females are more likely to experience traumas associated with an increased risk for PTSD (Afifi et al., 2008; Hovens et al., 2010) and, as such, females are more likely to develop PTSD (Adams et al., 2014; Afifi et al., 2008; Amado, Arce, & Herraiz, 2015; Cougle, Timpano, Sachs-Ericsson, Keough, & Riccardi, 2010; Govender & Killian, 2001; Kilpatrick et al., 2003; Seedat et al., 2004; Suliman et al., 2009; Wolfe, Scott, Wekerle, & Pittman, 2001). Older age in adolescence is associated with greater trauma exposure and an increased risk for developing PTSD (Adams et al., 2014; Macdonald et al., 2010; Stein, Jaycox, Kataoka, Rhodes, & Vestal, 2003; Weist, Acosta, & Youngstrom, 2010). In addition poverty is associated with a greater risk of trauma exposure and PTSD (Nikulina, Widom, & Czaja, 2011; Richter & Dawes, 2008; Stein et al., 2003; Suliman et al., 2009; Wolfe et al., 2001).
Higher trauma load, defined as the number of traumas experienced, is associated with a higher risk of developing PTSD (Afifi et al., 2008; Fujiwara, Kawakami, & World Mental Health Japan Survey Group, 2011; Kingston & Raghavan, 2009; Suliman et al., 2009). Multiple trauma exposure during childhood is associated with a higher risk of revictimization in adolescence and adulthood, for example, childhood survivors of abuse are more likely to report multiple trauma exposure during their lifetime (Dong, Anda, Dube, Giles, & Felitti, 2003; Hovens et al., 2010; Widom, 1999). Prior victimization also increases PTSD symptom severity following revictimization (Tyler, 2002).
In addition to PTSD index trauma and trauma load, exposure to community violence may be considered to be a significant source of distress and may increase PTSD symptom severity (Shields et al., 2008). Injuries due to violence are the second leading cause of death in South Africa with males more often than females being the victim and/or perpetrator of violence (Govender & Killian, 2001; Seedat, van Niekerk, Jewkes, Suffla, & Ratele, 2009; Stein et al., 2003; Ward et al., 2001; Weist et al., 2010). Shields et al. (2008) found that the majority of children living in informal settlements in South Africa were exposed to community violence, including witnessing assault, gun violence, and murder (Shields, Nadasen, & Pierce, 2009). Gang violence is also common in informal settlements, and the majority of children know a family member who participates in gang activities (Shields et al., 2008). Exposure to community violence is significantly associated with the risk of developing PTSD and increased symptom severity (Barbarin, Richter, & de Wet, 2001; Martin, Revington, & Seedat, 2012).
Child abuse and neglect are other factors that contribute to the development of PTSD (Norman et al., 2012; Stoltenborgh, Bakermans-Kranenburg, van Ijzendoorn, & Alink, 2013). The link between sexual abuse, physical abuse, and PTSD is well established (Cougle et al., 2010; Libby et al., 2005; MacMillan et al., 2001; Norman et al., 2007; Tyler, 2002; Widom, 1999). Physical abuse has been associated with depression and suicidal behavior (MacMillan et al., 2001; Norman et al., 2012; Thornberry, Ireland, & Smith, 2001). The odds of developing PTSD following sexual abuse has been found to be higher compared with physical abuse (Hovens et al., 2010; Widom, 1999), and sexual abuse survivors are likely to be diagnosed with comorbid PTSD and depression (Kilpatrick et al., 2003).
Fewer studies have investigated the link between childhood physical neglect, emotional neglect, and emotional abuse, although these forms of neglect and abuse have been associated with an increased risk of developing PTSD and other psychiatric disorders (Herrenkohl & Herrenkohl, 2007; Lansford et al., 2002; Nikulina et al., 2011; Norman et al., 2012; Thornberry et al., 2001; Widom, 1999). Emotional neglect and emotional abuse, but not physical neglect have been found to be significantly associated with anxiety sensitivity (a trait related to risk of anxiety disorders) in a sample of South African adolescents (Martin, Viljoen, Kidd, & Seedat, 2014). Emotional neglect and abuse may occur simultaneously and frequently throughout childhood, rather than occasionally, with parents the perpetrators in the majority of the cases (Hovens et al., 2010). Childhood physical neglect is also associated with internalizing problems, for example, social withdrawal, sleeping problems, and irritability which is related to anxiety disorders and depression, in adolescence (Thornberry et al., 2001).
Mental health care facilities are often severely overburdened in low-income countries, and access to these services is limited to individuals displaying severe symptoms (Mayosi et al., 2012; Petersen, Lund, Bhana, & Flisher, 2012). Physical abuse, sexual abuse, trauma load, and exposure to community violence have been found to increase risk for PTSD in general community samples. Increased trauma load and different forms of abuse and neglect have also been linked to PTSD symptom severity and PTSD + depression comorbidity in general community samples. However, less is known about PTSD risk (specifically risk related to physical neglect, emotional neglect, and emotional abuse) and comorbidity in clinic samples in low- and middle-income countries, where trauma load is often high and the type of exposure diverse. Identifying the contribution of various risk factors in PTSD symptom severity and comorbidity is important for determining the allocation of limited mental health care resources (Macdonald et al., 2010). It may also inform interventions aimed at reducing relapse and lessening PTSD symptom severity.
First, we aimed to determine the weight of risk factors (trauma load, community violence, emotional abuse, emotional neglect, sexual abuse, physical abuse, and physical neglect) in relation to PTSD symptom severity, while adjusting for the influence of depression and demographic factors on PTSD severity. Based on previous findings, we hypothesized that trauma load, community violence, sexual abuse, and physical abuse would predict PTSD symptom severity. Too little is known about emotional neglect, physical neglect, and emotional abuse to make any firm predictions. Second, we aimed to determine group differences in gender status, age, ethnicity, trauma load, community violence, emotional abuse, emotional neglect, sexual abuse, physical abuse, and physical neglect in four groups of adolescents: (a) trauma exposed with no disorder, (b) trauma exposed with PTSD only, (c) trauma exposed with PTSD and depression, and (d) trauma exposed with depression only. We hypothesized that participants with comorbid PTSD and depression would have a higher trauma load and greater exposure to community violence, sexual abuse, and physical abuse.
Method
Participants
Participants comprised 215 adolescents between 12 and 18 years of age. The majority of adolescents were female (60.9%) and of mixed ethnicity (80.3%). These adolescents were referred to an adolescent trauma research clinic (Department of Psychiatry, Stellenbosch University, Cape Town, South Africa) by schoolteachers or community/social workers for trauma-related emotional and/or behavioral problems. Participants were included in the study if they had been exposed to at least one Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) qualifying PTSD traumatic event, were proficient in English or Afrikaans, and resided in the Cape Town metropolitan area. Exclusion criteria included evidence of intellectual disability (based on a prior assessment of cognitive delay and adaptive functioning), current use of sedative psychotropic medication, history of a traumatic brain injury, and current illicit substance abuse (e.g., participants who were in urgent need of admission or were under the influence of substances during assessments). Referred participants were telephonically screened for inclusion and exclusion criteria. Alternative mental health resources were suggested if participants did not meet the criteria for this study.
Study Design, Procedure, and Ethical Considerations
The study followed a cross-sectional design. Ethical approval to conduct the study was obtained from the Health Research Ethics Committee at Stellenbosch University. Approval was also obtained from the Western Cape Department of Education. Schools, clinics, and nongovernmental organizations working with community development and trauma were informed of the study and asked to refer willing participants who had experienced trauma and presented with emotional and/or behavioral problems secondary to traumatic exposure. Following referral, participants were telephonically screened for potential eligibility. Eligible participants were invited to attend an appointment at the clinic. Written informed consent was obtained from participants aged 18 years and older. Participants under 18 years provided informed assent and a parent or legal guardian provided informed consent. A clinical psychologist evaluated participants with a semistructured diagnostic interview to determine their PTSD status and to assess for other psychiatric disorders. The diagnostic interview was followed by completion of self-report measures of trauma exposure and psychopathology. Efforts were made to minimize missing data, for example, completed questionnaires were checked by a member of the research team and participants were encouraged to complete all items. Participants who were in need of treatment were referred as appropriate. Participants were reimbursed for their travel expenses.
Measures
All measures were translated from English into Afrikaans. The translated Afrikaans versions were then independently back-translated into English and the back-translated versions were compared with the original versions. Adjustments were made, based on the back-translation, to assure the quality of the translation. The following measures were used in this study.
The Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS-PL)
The K-SADS-PL is a semistructured interview used to assess current and lifetime history of psychiatric disorders, as well as symptom severity, in children and adolescents (Kaufman, Birmaher, Brent, Rao, & Ryan, 1997). The K-SADS-PL assesses psychiatric disorders based on DSM-IV criteria. Disorders covered by the K-SADS-PL include anxiety disorders, mood disorders, psychotic disorders, eating disorders, substance abuse, adjustment disorders, and so on. Trauma load was determined by the Traumatic Events subscale of the K-SADS-PL. Traumatic events covered by this subscale include car accidents, other serious accidents, fire, witness of a natural disaster, witness of a violent crime, confronted with traumatic news, witness to domestic violence, physical abuse, and sexual abuse. The K-SADS-PL has shown excellent interrater reliability and concurrent validity in a previous study (Kaufman et al., 1997). Kaufman et al. (1997) found that children meeting criteria for current depression had significantly higher scores on the Beck Depression Inventory (BDI), the Children’s Depression Inventory (CDI), and the internalizing subsection of Child Behavior Checklist (CBCL). Children meeting criteria for attention deficit hyperactivity disorder or other behavioral disorders scored significantly higher on the Conner’s Parent Rating Scale (CPRS) and the externalizing subsection of the CBCL, respectively. Children meeting criteria for any anxiety disorder scored significantly higher on the Screen for Child Anxiety Related Emotional Disorders (SCARED). Interrater reliability for current and lifetime disorders equated to 98% agreement with a range of 93% to 100% in a previous study (Kaufman et al., 1997). Interrater reliability, in this study, was established through uniform training and observation of clinical psychologists in the administration of the K-SADS-PL.
The Child PTSD Checklist (CPC)
The CPC is a 28-item, self-report questionnaire used to measure PTSD symptom severity in accordance with the DSM-IV symptoms of PTSD (Amaya-Jackson, McCarthy, Newman, & Cherney, 1995). The CPC has been used in various trauma populations and has shown acceptable psychometric properties (Esterhuyse, Louw, & Bach, 2007; Lipschitz, Grilo, Fehon, McGlashan, & Southwick, 2000). The CPC has been correlated (r = .64) with the Clinician Administered PTSD Scale for Children and Adolescents (CAPS-CA), and an alpha coefficient of .82 was found for the total CPC in a sample of African adolescents (Esterhuyse et al., 2007; Lipschitz et al., 2000). The CPC (α = .94) showed good to excellent internal consistency in this study.
The Childhood Trauma Questionnaire (CTQ)
The CTQ is a 28-item, retrospective, self-report questionnaire (Bernstein & Fink, 1998). Participants respond to items related to abuse and neglect before the age of 18, on a 5-point Likert-type scale, ranging from “never true” to “very often true.” Scores range from 25 to 125 for the entire scale and between 5 and 25 for each of the five subscales (i.e., Sexual Abuse, Physical Abuse, Emotional Abuse, Physical Neglect, and Emotional Neglect). The CTQ has shown high internal consistency for the entire scale in previous studies (α = .91) and acceptable to excellent internal consistency for the subscales: Sexual Abuse (α = .94), Physical Abuse (α = .69), Emotional Abuse (α = .83), Physical Neglect (α = .58), and Emotional Neglect (α = .85) (Scher & Stein, 2003; Villano et al., 2004). The CTQ showed good internal consistency (α = 0.86) in this sample. The CTQ Sexual Abuse subscale showed excellent internal consistency (α = .90), followed by the Emotional Neglect (α = .79), Physical Abuse (α = .78), and Emotional Abuse (α = .74) subscales that showed acceptable internal consistency. The Physical Neglect (α = .52) subscale showed poor internal consistency.
The Child Exposure to Community Violence Checklist (CECV)
The CECV is a 39-item, self-report questionnaire used to measure exposure to violence in participants’ communities, including hearing about, witnessing, and experiencing community violence (Amaya-Jackson, 1998). Responses to items are measured on a 5-point Likert-type scale ranging from “never” to “more than 10 times.” Scores range between 0 and 156. The CECV has shown excellent internal consistency (α = .90) in a previous study (Martin et al., 2012). The CECV (α = .89) showed good to excellent internal consistency in this study.
Data Analysis
Descriptive statistics were computed for demographic variables. Data were missing at random. Missing data were replaced using maximum likelihood estimates through expectation maximization (EM). ANOVAs were used to compare the following groups on a number of continuous variables (i.e., sexual abuse, physical abuse, emotional abuse, physical neglect, emotional neglect, exposure to community violence, number of traumas, and age): adolescents with no disorder, those with PTSD only, those with depression only, and those with comorbid PTSD and depression. Levene’s test was used to determine homogeneity of variance. Games–Howell post hoc analysis was used if equal variance was not assumed, and Least Squares Mean (LSM) post hoc analysis was used if equal variance was assumed. Bonferroni corrections were used in post hoc analyses to avoid Type I errors caused by an inflated p value due to multiple comparisons. Chi-square tests were used for categorical variables (i.e., gender and ethnicity). Correlations between variables were investigated, and variables significantly correlated with PTSD were included as predictors in a stepwise hierarchical multiple regression model. Depression status was entered into the first block as a covariate. Age, gender, and ethnicity were added in the second block. Trauma load was added into the third block. Community violence was added into the fourth block. Emotional abuse, sexual abuse, physical abuse, and physical neglect were added in the final block. Cronbach’s alpha scores were calculated for the CPC, CTQ, and CECV.
Results
Prevalence of Trauma, PTSD, and Depression
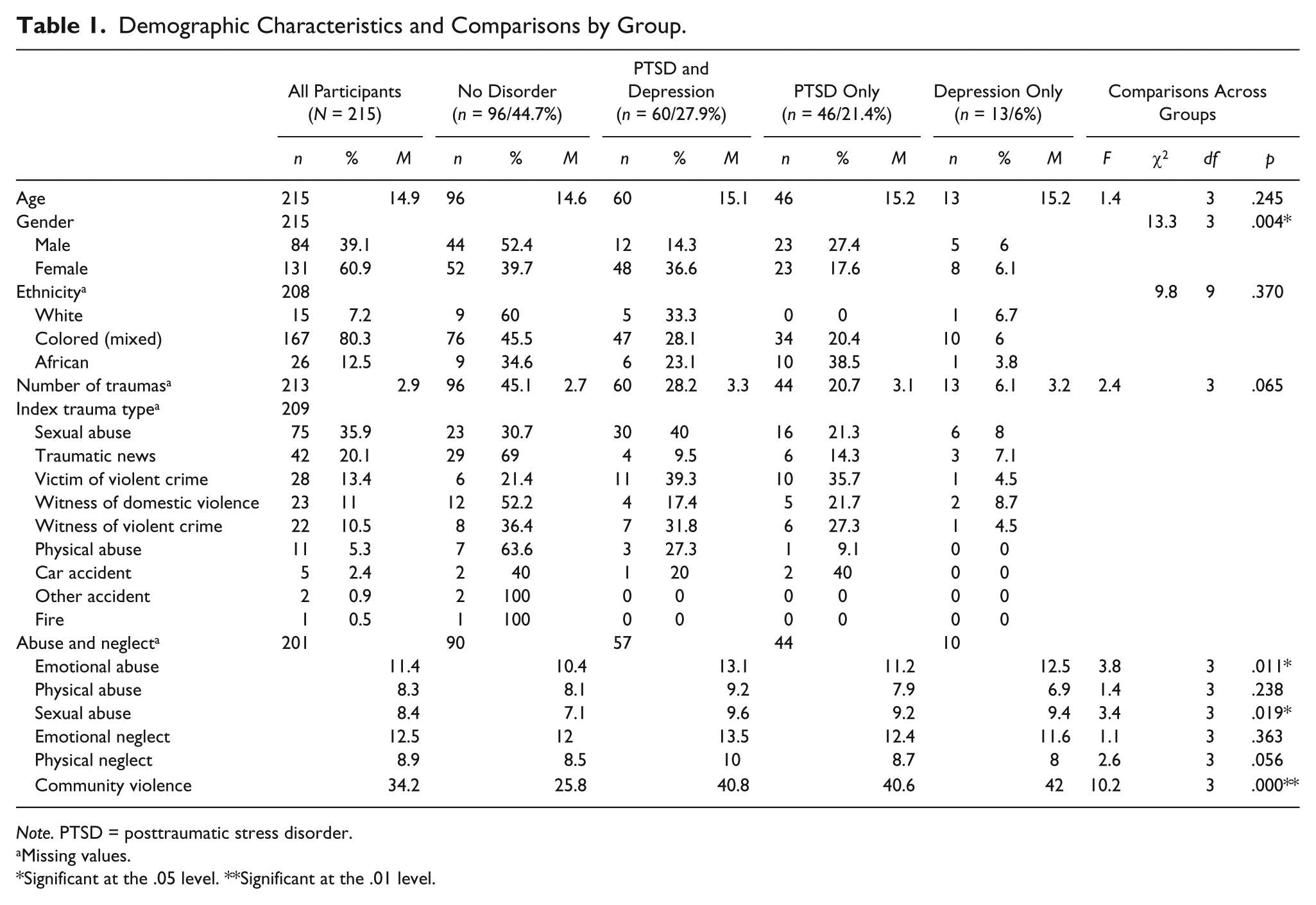
Ninety-six adolescents did not meet criteria for PTSD or depression (44.7%), 60 adolescents met criteria for both PTSD and depression (27.9%), 46 met criteria for PTSD only (21.4%), and 13 met criteria for depression only (6%). Approximately half the sample (49.3%) qualified for a PTSD diagnosis, and 34% met criteria for depression when taking the overlap between the comorbidity group, PTSD only group, and depression only group into account. The majority of the participants had at least one psychiatric disorder (55.3%). PTSD + depression comorbidity, in terms of those meeting criteria for PTSD, was 56.6%. The most commonly reported index trauma was sexual abuse (35.9%), followed by confronting traumatic news (20.1%), being a victim of a violent crime (13.4%), witnessing domestic violence (11%), witnessing a violent crime (10.5%), physical abuse (5.3%), car accident (2.9%), other accidents (0.9%), and exposure to fire (0.5%). A mean of 2.94 traumatic events (range = 1-7) were reported by adolescents in this sample. Demographic characteristics, index traumas, and the comparison between subgroups are presented in Table 1.
Demographic Characteristics and Comparisons by Group.
Note. PTSD = posttraumatic stress disorder.
Missing values.
Significant at the .05 level. **Significant at the .01 level.
Differences Between Groups
A comparison of adolescents with no disorder, PTSD only, depression only, and comorbid PTSD and depression revealed significant group differences for emotional abuse, F(3, 197) = 93.36, p = .011; sexual abuse F(3, 197) = 274.15, p = .019; and exposure to community violence, F(3, 193) = 10.23, p < .000. Post hoc comparisons using the LSM with Bonferroni corrections indicated that the mean score for community violence was significantly higher in participants with depression only (M = 42.04, SD = 16.33, d = .93, p = .049), PTSD only (M = 40.61, SD = 22.64, d = .71, p < .000), and comorbid PTSD and depression (M = 40.85, SD = 16.97, d = .81, p < .000) compared with participants with no disorder (M = 25.78, SD = 18.66). LSM analysis also indicated that the mean score for emotional abuse was significantly higher in participants with comorbid PTSD and depression (M = 13.12, SD = 5.14, d = .55, p = .007) compared with participants with no disorder (M = 10.36, SD = 5.08). Games–Howell post hoc analysis indicated that the mean score for sexual abuse was significantly higher in participants with comorbid PTSD and depression (M = 9.57, SD = 5.97, d = .49, p = .034) compared with participants with no disorder (M = 7.07, SD = 4.18).
There were significant gender differences in the rates of PTSD and depression determined (χ2 = 13.3, p = .004). The majority of males (52.4%) and 39.7% of females did not meet criteria for PTSD or depression. Females were more likely to meet criteria for both PTSD and depression (36.6%) compared with PTSD only (17.6%) and depression only (6.1%). Males were more likely to meet criteria for PTSD only (27.4%) compared with both PTSD and depression (14.3%) or depression only (6%). There were no significant differences in the rates of these disorders for ethnicity (χ2 = 9.8, p = .370); age F(3, 224) = 1.4, p = .245; or trauma load (F = 2.4, p = .065).
Relationship Between Variables
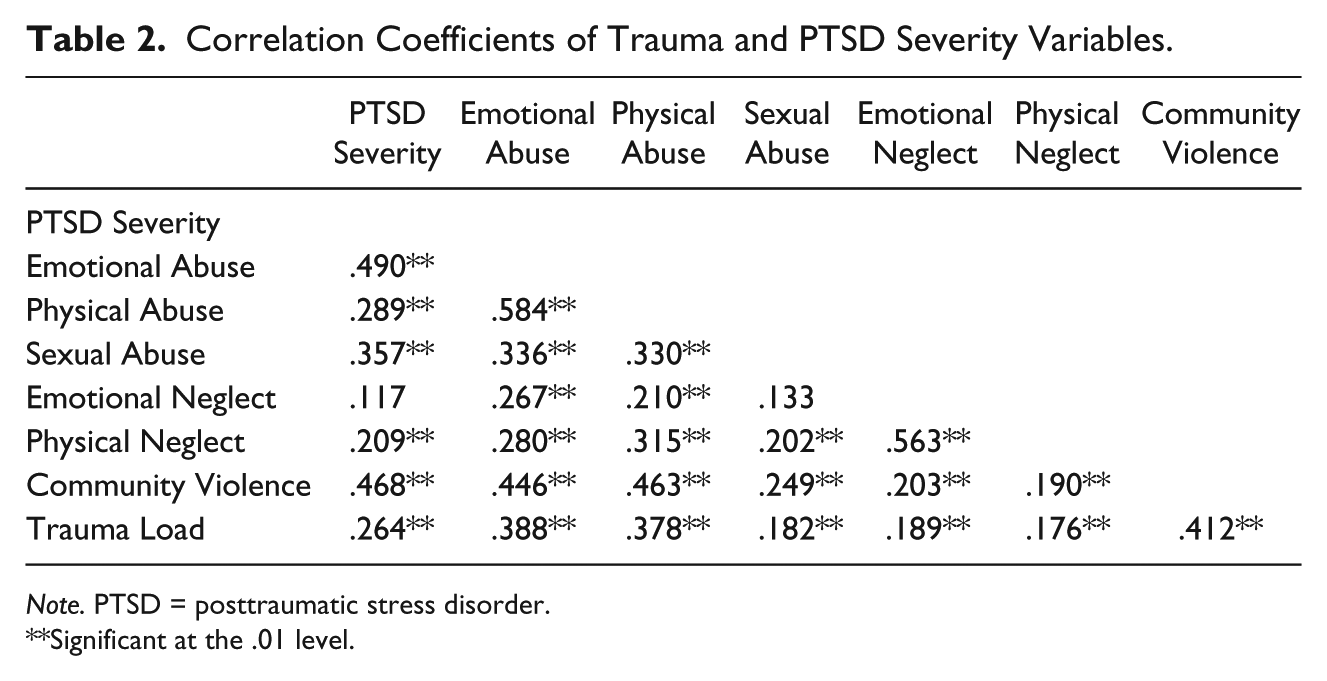
Correlation coefficients between variables are presented in Table 2. Significant positive correlations were found between PTSD severity and emotional abuse (r = .490, p < .01), physical abuse (r = .289, p < .01), sexual abuse (r = .357, p < .01), physical neglect (r = .209, p < .01), community violence (r = .468, p < .01), and trauma load (r = .264, p < .01). The relationship between PTSD severity and emotional neglect (r = .117, p >.05) was not significant.
Correlation Coefficients of Trauma and PTSD Severity Variables.
Note. PTSD = posttraumatic stress disorder.
Significant at the .01 level.
Predictors of PTSD
Tables 3 and 4 present the summary statistics of the regression analysis. Depression status was entered into the first block of the regression analysis as a covariate. The model significantly explained 22.5% of the variance in PTSD symptom severity, F(1, 181) = 53.96, p < .000. Depression was a significant predictor of PTSD symptom severity, β = 2.48, t(1, 181) = 7.35, p < .000.
Parameters for Multiple Regression Models Predicting PTSD Severity.
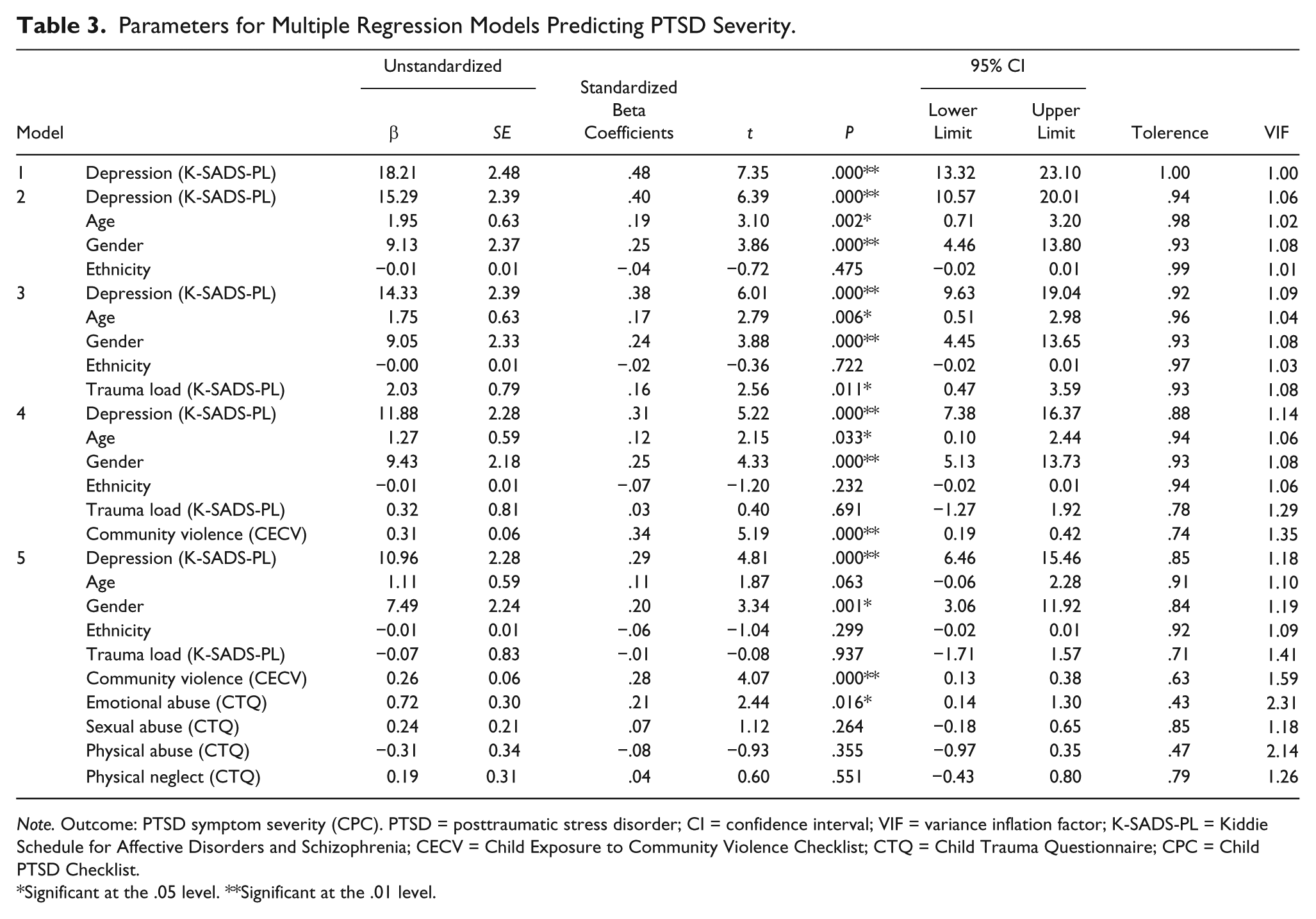
Note. Outcome: PTSD symptom severity (CPC). PTSD = posttraumatic stress disorder; CI = confidence interval; VIF = variance inflation factor; K-SADS-PL = Kiddie Schedule for Affective Disorders and Schizophrenia; CECV = Child Exposure to Community Violence Checklist; CTQ = Child Trauma Questionnaire; CPC = Child PTSD Checklist.
Significant at the .05 level. **Significant at the .01 level.
Model Summary for Multiple Regression Models Predicting PTSD Severity.
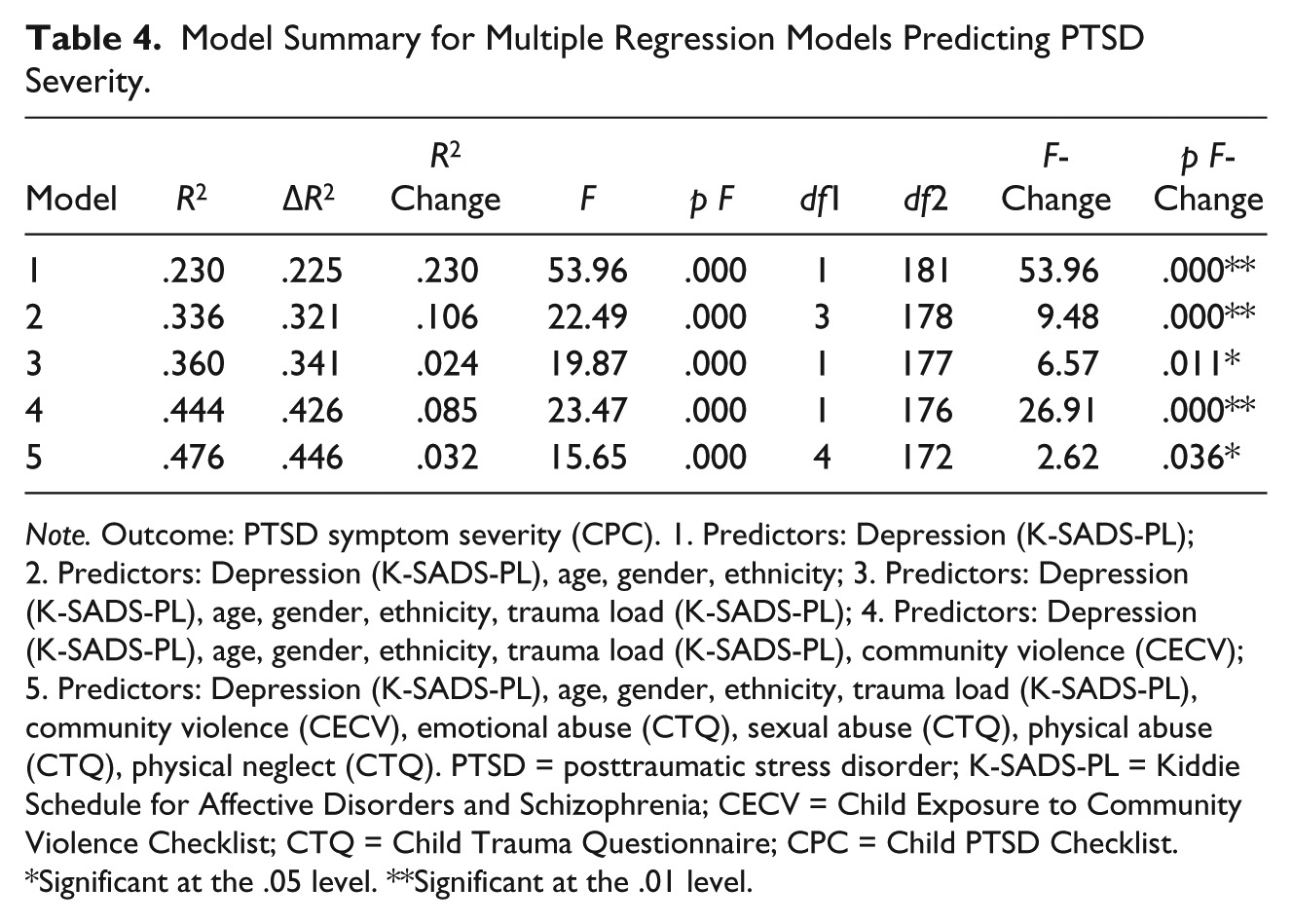
Note. Outcome: PTSD symptom severity (CPC). 1. Predictors: Depression (K-SADS-PL); 2. Predictors: Depression (K-SADS-PL), age, gender, ethnicity; 3. Predictors: Depression (K-SADS-PL), age, gender, ethnicity, trauma load (K-SADS-PL); 4. Predictors: Depression (K-SADS-PL), age, gender, ethnicity, trauma load (K-SADS-PL), community violence (CECV); 5. Predictors: Depression (K-SADS-PL), age, gender, ethnicity, trauma load (K-SADS-PL), community violence (CECV), emotional abuse (CTQ), sexual abuse (CTQ), physical abuse (CTQ), physical neglect (CTQ). PTSD = posttraumatic stress disorder; K-SADS-PL = Kiddie Schedule for Affective Disorders and Schizophrenia; CECV = Child Exposure to Community Violence Checklist; CTQ = Child Trauma Questionnaire; CPC = Child PTSD Checklist.
Significant at the .05 level. **Significant at the .01 level.
Age, gender, and ethnicity were entered into the second model. The model significantly explained 32.1% of the variance in PTSD symptom severity. The addition of age, gender, and ethnicity significantly increases the variance explained by 10.6%, F-change(1, 181) = 9.48, p < .000. Age, β = 0.63, t(3, 178) = 3.10, p = .002, and gender, β = 3.86, t(3, 178) = 3.86, p < .000, were significant predictors of PTSD symptom severity, but ethnicity was not significant, β = 0.01, t(3, 178) = −0.72, p = .475. There was no indication of multicollinearity in this model (tolerance range = .93-.99; variance inflation factor [VIF] range = 1.01-1.08).
Trauma load was added into the third model. The model significantly explained 34.1% of the variance in PTSD symptom severity. The addition of trauma load significantly increased the variance explained by 2.4%, F-change(1, 177) = 6.57, p = .011. Age, β = 0.63, t(1, 177) = 2.79, p = .006; gender, β = 2.33, t(1, 177) = 3.88, p < .000; and trauma load, β = 0.79, t(1, 177) = −2.56, p = .011, were significant predictors of PTSD, but ethnicity was not significant, β = 0.01, t(1, 177) = −0.36, p = .722. There was no indication of multicollinearity in this model (tolerance range = .92-.97; VIF range = 1.03-1.09).
Community violence was included in the fourth model. The model significantly explained 42.6% of the variance in PTSD symptom severity. The addition of community violence significantly increased the variance explained by 8.5%, F-change(1, 176) = 26.91, p < .000. Age, β = 0.59, t(1, 176) = 2.15, p = .033; gender, β = 2.18, t(1, 176) = 4.33, p < .000; and community violence, β = 0.06, t(1, 176) = 5.19, p < .000, were significant predictors of PTSD symptom severity, but ethnicity, β = 0.01, t(1,176) = −0.07, p = .232, and trauma load, β = 0.81, t(1, 176) = 0.40, p = .691, were not significant. There was no indication of multicollinearity in this model (tolerance range = .74-.94; VIF range = 1.06-1.35).
Emotional abuse, sexual abuse, physical abuse, and physical neglect were introduced in the final model. The model significantly explained 44.6% of the variance in PTSD symptom severity. The addition of abuse and neglect variables significantly increased the variance explained by 3.2%, F-change (4, 172) = 2.62, p = .036. Gender, β = 2.24, t(4, 172) = 3.34, p = .001; community violence, β = 0.26, t(4, 172) = 4.07, p < .000; and emotional abuse, β = 0.30, t(4, 172) = 2.44, p = .016, were significant predictors of PTSD symptom severity. Age, β = 0.59, t(4, 172) = 1.87, p = .063; ethnicity, β = 0.01, t(4, 172) = −1.04, p = .299; trauma load, β = 0.83, t(4, 172) = −0.08, p = .937; sexual abuse, β = 0.21, t(4, 172) = 1.12, p = .264; physical abuse, β = 0.34, t(4, 172) = −0.93, p = .355; and physical neglect, β = 0.31, t(4, 172) = 0.60, p = .551, were not significant in the final model. There was no indication of multicollinearity in this model (tolerance range = .74-.94; VIF range = 1.09-2.31). Emotional abuse had the lowest tolerance score and highest VIF score.
Discussion
Overall, the rate of clinician-diagnosed PTSD was high in this group, with almost half (49.3%) of the adolescents meeting criteria for PTSD and the vast majority experiencing multiple traumas (85%). The rate of depression (34%) was also high. PTSD + depression comorbidity, in terms of those meeting criteria for PTSD, was 56.6%, which is comparable with previous findings from clinical settings (APA, 2013). The high prevalence of PTSD underscores the vulnerability to trauma, community violence, abuse, and neglect among South African adolescents as well as the mental health consequences resulting from trauma and the need for early intervention (Lalor, 2004; Richter & Dawes, 2008).
In terms of relationships between variables and PTSD, first, depression was entered as a covariate in the regression model and significantly explained 23% of the variance in PTSD symptom severity. Comorbid PTSD and depression are common among survivors of trauma (Acierno et al., 1999; Kilpatrick et al., 2003; Plichta & Falik, 2001; Ullman & Brecklin, 2002). Previous studies have found that abused and neglected children are likely to develop depression secondary to PTSD (Kilpatrick et al., 2003; Levitan et al., 2003; MacMillan et al., 2001). However, temporal causality cannot be inferred in this study because of the cross-sectional design. Comorbidity is also prevalent in adolescent samples exposed to community violence (Jaycox et al., 2002). However, it is not clear whether comorbidity represents distress experienced as a result of PTSD status, a common emotional and biological susceptibility to mental disorders, an additional symptom cluster of PTSD, or whether depression precedes PTSD or vice versa (Breslau et al., 2002; O’Donnell, Creamer, & Pattison, 2004).
Second, age, gender, and ethnicity significantly explained 10.6% of the variance in PTSD symptom severity. Gender was a significant predictor of PTSD in the final model, and females were more likely to be diagnosed with comorbid PTSD and depression. Age and ethnicity were not significant predictors, and no significant group differences were found. Various previous studies have found that females are more likely to develop psychiatric disorders following trauma (Afifi et al., 2008; Cougle et al., 2010; Govender & Killian, 2001; Kilpatrick et al., 2003; Seedat et al., 2004; Suliman et al., 2009; Wolfe et al., 2001). Older adolescents are also more likely to qualify for a PTSD diagnosis (according to the group comparison); however, this finding could be attributed to the effect of time (i.e., more years for potential exposure; Stein et al., 2003; Weist et al., 2010).
Third, trauma load explained 2.4% of the variance in PTSD symptom severity. The amount of variance explained was small, but significant. However, there was no significant difference in trauma load between groups, and trauma load was not a significant predictor of PTSD symptom severity in the final model. Although previous studies have found that adolescents exposed to multiple traumas report significantly higher rates of PTSD symptomatology and are significantly more likely to meet criteria for PTSD (Afifi et al., 2008; Kingston & Raghavan, 2009; Resnick, Kilpatrick, Dansky, Saunders, & Best, 1993; Suliman et al., 2009), the results of this study suggest that trauma type is more likely to predict PTSD status and symptom severity than trauma load. The nonsignificant finding may also be due to limited variance in trauma load between groups.
Fourth, exposure to community violence was a strong predictor of PTSD symptom severity in the final model and significantly explained 8.5% of the variance. Adolescents with PTSD only, PTSD and depression, and depression only also had significantly higher levels of exposure to community violence compared with those without a disorder. Our findings are consistent with previous findings. Exposure to community violence is significantly associated with PTSD and emotional distress (Barbarin et al., 2001; Martin et al., 2012; Shields et al., 2008). South Africa has very high rates of rape, gang involvement, and interpersonal violence (Jewkes et al., 2006; R. Norman et al., 2007). In 2011, 9.1% of all deaths from census figures in South Africa were due to unnatural causes, and the prevalence of unnatural deaths is highest among adolescents between 15 and 19 years old with 39.4% of all deaths in this age group due to unnatural causes (Statistics South Africa, 2014). The number of deaths due to injury in South Africa is twice that of the global average (Seedat et al., 2009). Many of these deaths are due to community violence. Children are often exposed to burglaries, witnessing physical assault and injury, hearing gunshots, awareness of gangs, all of which occur in their neighborhood and immediate surroundings (Martin et al., 2012). Prolonged fear and anxiety due to unsafe living environments in childhood increases the risk of developing anxiety disorders (Heim & Nemeroff, 2001; Pynoos, Steinberg, & Piacentini, 1999).
Fifth, the addition of abuse and neglect variables significantly explained 3.2% of the variance in PTSD symptom severity. Emotional abuse was the only significant predictor of PTSD symptom severity in the final model. We also found significant group differences in emotional abuse with participants with comorbid PTSD and depression endorsing the highest levels of emotional abuse. Emotional abuse is commonly reported among individuals diagnosed with mood and anxiety disorders and have been linked to an increased risk for suicidal behavior and the development of PTSD (Hovens et al., 2010; Norman et al., 2007; Norman et al., 2012). Emotional abuse in childhood may affect a wider range of developmental and functional entities, compared with other forms of abuse, and include impairment in emotional state, behavior and cognitive development, positive peer relationships, physical development, and sexual risk behavior (Glaser, 2002; Norman et al., 2012). Emotional abuse also hinders the development of various factors associated with resilience, including an extraverted nature, self-efficacy, self-esteem, hope, control, a sense of belonging, and secure attachment (Herman et al., 2011). Insecure attachment has far-reaching consequence. Insecure attachment and mistrust of others compromise the development of positive peer relationships and intimate relationships throughout the life span and, in turn, compromise social support, which is another important resilience factor (Margolin & Gordis, 2000). A low level of resilience, withdrawal, and poor social support due to emotional abuse leaves the individual vulnerable for the development of anxiety, depression, suicide, drug abuse, sexual risk behavior, and general poor mental health (Norman et al., 2012).
Sixth, sexual abuse was not significantly associated with PTSD after accounting for associations of other forms of abuse, neglect, community violence, demographics, and depressive symptoms. However, significant group differences in sexual abuse scores were found in group comparisons. Participants with PTSD only, PTSD and depression, and depression only had significantly higher sexual abuse scores compared with participants with no disorder. The nonsignificant finding in the regression analysis may be due to collinearity with emotional abuse. Multicollinearity was not a significant problem on statistical analysis, but emotional abuse did have the lowest tolerance score and the highest VIF, which indicates that collinearity may have been present. This may indicate that emotional abuse commonly co-occurs with sexual abuse and other forms of abuse and neglect, and that other forms of abuse and neglect therefore share a portion of the variance explained by emotional abuse (Dong et al., 2003; Trickett, Mennen, Kim, & Sang, 2009).
Previous studies have found a strong association between sexual abuse and PTSD (Cougle et al., 2010; Fergusson et al., 2008; Kingston & Raghavan, 2009; Libby et al., 2005; MacMillan et al., 2001; Norman et al., 2007; Tyler, 2002; Widom, 1999). Survivors of sexual abuse are more likely to develop PTSD compared with victims of physical abuse and other trauma types and are also more likely to dissociate during abuse (Arata, 2002; Hetzel-Riggin & Roby, 2013; Hovens et al., 2010; Widom, 1999). The high rate of sexual abuse in South Africa has been attributed to various factors. For example, South Africa has a very high rate of HIV, and a common myth related to HIV is that sex with a virgin can prevent or cure the disease (Jewkes, Penn-Kekana, & Rose-Junius, 2005; Lalor, 2004; Madu & Peltzer, 2001; Richter, 2003). South Africa has a history of hegemonic masculinity where men assume a dominant social position and women assume a subordinate position (Morrell, Jewkes, & Lindegger, 2012). This may contribute to an assumption that women should attend to men’s sexual needs, leaving women with limited choice in participating in sexual activities and often taken advantage of (Richter & Dawes, 2008). Poverty is also widespread in South Africa, and a consequence of such poverty is that children sleep in close proximity to their parents and other adults, increasing their exposure to adult sexual activity and the risk of sexual abuse (Lalor, 2004; Richter & Dawes, 2008). High rates of alcohol and substance abuse among the South African population may also lead to high rates of sexual abuse (Jewkes & Abrahams, 2002).
Seventh, physical abuse was not a significant predictor of PTSD, with no significant group differences in the level of physical abuse. Previous studies have found a significant relationship between childhood physical abuse and PTSD (Afifi et al., 2008; Cougle et al., 2010; Fergusson et al., 2008; Lansford et al., 2002; Libby et al., 2005; Norman et al., 2012; Widom, 1999). High rates of physical abuse are also common in South Africa. This may, again, be attributed to men assuming the dominant social role and a history of violence as a means to resolving conflict in South Africa (Morrell et al., 2012; Richter & Dawes, 2008). A longstanding history of violence also contributes to a cycle of abuse where adults abused as children are more likely to become abusers in adulthood (Coohey, 2004; Maker, Shah, & Agha, 2005; Seedat et al., 2009). Poverty, unemployment, substance abuse, and a norm of physical punishment also increases the risk of physical abuse among South African youth (Berger, 2005; Maker et al., 2005; Richter & Dawes, 2008).
Last, we did not find a significant relationship between physical and emotional neglect and PTSD. We also did not find significant group differences in levels of physical and emotional neglect. Emotional neglect may be common among South African adolescents due to the limitations that poverty places on parents (e.g., a high number of single-parent households, long commutes to work, and long working hours), with children left unsupervised and emotionally unattended to for long periods of time (Lalor, 2004; Richter & Dawes, 2008). Parents may also struggle with processing their own experiences of trauma and abuse, which can hinder their mental ability to attend to their children’s emotional needs (Hornor, 2010). Physical neglect, similar to emotional neglect, may be consequent to basic financial and community resources associated with poverty in South Africa (Richter & Dawes, 2008). Physical neglect can be defined as the failure to provide adequate food, shelter, clothing, and medical care, often due to financial constraints (Nikulina et al., 2011). Further research is needed to explore the relationship between physical neglect, emotional neglect, and PTSD. However, it may be hypothesized that common experiences of emotional and physical neglect may lead to adolescents not perceiving these forms of neglect as traumatic and turning to other sources (e.g., friends and extended family) to fulfill their emotional needs.
A few limitations deserve mention. Abuse and neglect were measured retrospectively, and recall bias may have influenced the reported severity. The sample was not homogeneous with regard to index trauma type, and participants were exposed to diverse trauma types. This did, however, allow us to compare outcomes of the various trauma types. Poverty, a previously found predictor of abuse, neglect, and exposure to violence, was not measured in this study. However, participants were predominately recruited from low income communities, consisting largely of informal settlements. PTSD status was determined using DSM-IV criteria as this study was initiated prior to the publication of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Although this may limit cross-comparability with more recent studies that have applied DSM-5 criteria, studies in adolescent and adult samples have reported small differences (between 1% and 2.3%) in PTSD diagnosis using DSM-IV criteria compared with DSM-5 criteria (Carmassi et al., 2013; Hoge, Riviere, Wilk, Herrell, & Weathers, 2014; Kilpatrick et al., 2013). The subscale Physical Neglect showed poor reliability, and interpretation of the findings of the regression analysis relating to this subscale should be cautiously approached. Concordance between raters was not determined statistically for the K-SADS-PL, and clinical judgment may have biased the outcome. However, raters received uniform training and were observed by the trainer to identify and rectify inconsistencies in the administration of this diagnostic interview. The study also followed a cross-sectional design, which limits casual inferences.
Several strengths of the study should also be highlighted. PTSD and depression status were ascertained using a clinician-administered interview; thus, the possibility of elevated rates due to self-report measures was avoided. The sample size (N = 215) was adequate for statistical analysis and allowed for comparison of groups of adolescents with PTSD, depression, and their co-occurrence. The trauma types reported are highly representative of the trauma types generally reported in low-income South African populations. Most prior research has focused on childhood abuse, neglect, and exposure to violence as a predictor of adult psychopathology. This study focused specifically on childhood abuse and neglect as predictors of PTSD and depression in a clinic sample of adolescents. We also reported the prevalence of PTSD, which is relatively unknown in clinic samples located in low- and middle-income countries.
Implication of Findings
In conclusion, we found that the prevalence of PTSD was high among traumatized adolescents, with comorbidity often present. Exposure to community violence was highly predictive of a PTSD diagnosis, and adolescents with PTSD only, PTSD and depression, and depression only reported significantly higher levels of exposure to community violence compared with those without a disorder. Community violence also explained a large portion of the variance in PTSD symptom severity. Emotional abuse was the only form of abuse that significantly predicted PTSD symptom severity, and participants with PTSD only, PTSD and depression, and depression only, had significantly higher levels of emotional abuse. However, the possible influence of collinearity cannot be excluded. Females were more likely to have a comorbid PTSD and depression diagnosis, and demographic variables, specifically gender, contributed a large portion of the variance in PTSD symptom severity. These findings suggest that interventions focused on preventing trauma and PTSD should be multifaceted, assess for emotional abuse, and be targeted at various levels, for example, individual/interpersonal level (prevent emotional abuse in households and immediate environment) and community/societal level (lower crime rates in communities and strengthen conviction policies). They also suggest that youth, particularly females, should routinely be screened for a history of abuse and exposure to community violence and should receive appropriate care to minimize the effects of abuse and prevent future victimization in their communities. Mental health resources should be directed toward community violence reduction and female mental health, given the large impact these factors have on PTSD symptom severity. However, male mental health should not be overlooked. School-based interventions should focus on reducing future gang involvement, community violence, and interpersonal violence. Clinical interventions should not only address the PTSD index trauma but should also consider the effects of abuse, neglect, gender, and community violence, to prevent relapse. Parental interventions may also be beneficial in reducing emotional abuse and enhancing positive parenting techniques. Symptoms of depression should be evaluated along with symptoms of PTSD, and both conditions should be addressed if present.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the South African Research Chair in posttraumatic stress disorder (PTSD) hosted by Stellenbosch University, funded by the Department of Science and Technology (DST) and administered by the National Research Foundation (NRF), and the Medical Research Council (MRC) Unit on Anxiety and Stress Disorders.